
Abstract
Research indicates that childhood adversity is associated with poor mental health in adulthood. The purpose of this study is to examine whether the deleterious long-term effects of childhood adversity on adult mental health are reduced for individuals who are involved in religious practices. Using longitudinal data from a representative sample of American adults (N = 1,635), I find that religious salience and spirituality buffer the noxious effects of childhood abuse on change in positive affect over time. By contrast, these stress-buffering properties of religion fail to emerge when negative affect serves as the outcome measure. These results underscore the importance of religion as a countervailing mechanism that blunts the negative impact of childhood abuse on adult mental health over time. I discuss the theoretical implications of these findings for views about religion, childhood adversity, and mental health.
Childhood adversity involves stressful events and conditions that a child may experience, including emotional and physical maltreatment, problems in childhood family structure (e.g., parental death or divorce), and low socioeconomic status during childhood (Schafer & Ferraro, 2013). Childhood adversity has enduring effects on a host of adult outcomes, including life evaluations, sense of control, and physical health (Hayward & Gorman, 2004; Irving & Ferraro, 2006; Schafer, Ferraro, & Mustillo, 2011). In particular, numerous studies link childhood adversity to mental health (Greenfield & Marks, 2010a; Horwitz, Widom, McLaughlin, & White, 2001; Schilling, Aseltine, & Gore, 2008; Shaw & Krause, 2002). Although some research suggests that adverse experiences in childhood might spur positive growth (Bonanno & Mancini, 2008), the bulk of evidence confirms that adults who had the experience of childhood adversity demonstrate worse mental health on average than adults who did not. Despite this knowledge, little is known about why some individuals with a history of childhood adversity have poor psychological well-being in adulthood whereas others report relatively better mental health. Based on previous evidence regarding the role of coping resources in moderating the effects of stress on mental health (Pearlin, 1989), I propose that this differential long-term mental health effect of childhood adversity can be explained by the use of compensatory mechanisms that mitigate the adverse effects of early disadvantage.
Among a broad array of countervailing mechanisms, I focus on religion because of its utility as a coping resource: People often turn to religion as a way of dealing with stressful conditions (Pargament, 1997; Park, 2008). However, only a few empirical studies have explored the intersection between childhood adversity, religion, and mental health (Dervic, Grunebaum, Burke, Mann, & Oquendo, 2006; Gall, Basque, Damasceno-Scott, & Vardy, 2007). For example, Gall and her colleagues (2007) found that relationship with a benevolent God is associated with less negative mood among a sample of 101 men and women survivors of childhood sexual abuse. Similarly, analyzing a sample of 119 depressed inpatients who reported childhood abuse, Dervic and her colleagues (2006) found that religious beliefs have an inverse correlation with suicidal ideation. Nonetheless, this oversight is noteworthy because (a) religion is still salient in the United States; (b) religion is especially helpful for dealing with stressors such as childhood adversity that cannot be altered, avoided, or easily resolved (Gottlieb, 1997); and (c) a substantial amount of research and theory has been predicated on the notion that religion is particularly influential among economically and socially deprived individuals, by extension, among individuals who had adverse childhood experiences (Pargament, 1997; Schieman, Bierman, & Ellison, 2010; Weber, 1922/1964). While turning to religion in response to stressors might foster negative beliefs about the self and the world, religious coping tends to help individuals reconcile life’s adversities and view the stressful situation in a positive light (Exline & Rose, 2005; Park, 2008).
The central research question in this study is whether religion in adulthood buffers the noxious effects of childhood adversity on change in adult mental health over time. The current study contributes to the literature by addressing three key limitations in prior work on the interface of childhood adversity, religion, and mental health. First, an important caveat of the previous scholarship is the use of convenience sampling that is not representative. Second, prior studies rely on cross-sectional data, which prevent the establishment of temporal order among focal variables. Third, previous works employ limited measures of religiosity. This study is designed to address these limitations by incorporating various, previously unexplored measures of religiosity (e.g., religious attendance, religious salience, and spirituality) in a longitudinal study of a nationally representative sample of adults. Hence, the current study provides a firmer ground for the generalization of the findings, illuminates the causal nature of empirical relationships involving the stress-moderating effects of religion, and documents the roles of multiple dimensions of religiosity in this area. In this endeavor, I use data from the National Survey of Midlife Development in the United States (MIDUS), a panel survey of a representative sample of American adults in 1995 and 2005. This data set is ideal for addressing the main research question because it has a rich battery of questions concerning childhood adversity, religion, and mental health.
Theoretical and Empirical Background
Childhood Adversity, Adult Mental Health, and Countervailing Mechanisms
The life-course perspective provides an important insight into the association between childhood adversity and adult mental health. It suggests that early disadvantages accumulate across the life course, placing individuals on a trajectory of disadvantage leading to additional risks that can ultimately harm adult mental health (Dannefer, 2003). In stress research, this reflects a process of “stress proliferation” in which new or secondary stressors follow on the heels of primary stressors to which people are initially exposed (Pearlin, Aneshensel, & LeBlanc, 1997). In the context of the current study, these theoretical perspectives assert that exposure to childhood adversity sets in motion a chain of subsequent stressors, some of which may persist over time and contribute to poor mental health in adulthood (Pearlin, 2010). In specifying the nature of these processes, scholars theorize that childhood adversity is associated with poor mental health outcomes among children. In turn, poor mental health during childhood increases the risk of suffering subsequent stressors such as divorce and unemployment, which can be detrimental to adult mental health (Horwitz et al., 2001). Further, adverse experiences in childhood can strain family relationships and damage a successful transition to adulthood, which can also jeopardize mental health in adulthood (Schilling et al., 2008; Shaw & Krause, 2002). Among multiple indicators of early adversity that affect adult mental health, prior evidence suggests that childhood abuse is very important (Schafer & Ferraro, 2013; Schilling et al., 2008).
Yet, scholars have called for more attention to processes that can turn off the influence of accumulated risks on mental health (Pearlin, 1989; Schafer et al., 2011). The stress process model provides a rich foundation for understanding how events and experiences in later stages of life can moderate the influences of childhood experiences on adult mental health (Wheaton, 1985). The stress process model is a conceptual framework that analyzes the processes through which stressors exert noxious effects on mental health and people respond to these stressors based on social and personal resources available to them (Pearlin, 1989). In particular, it posits that stress proliferation is subject to countervailing mechanisms that impede its progression. Put differently, exposure to one stressor does not invariably lead to exposure to other stressors. In elaborating on this view, the stress process model underscores the role of psychosocial resources as moderators that modify the extent to which a primary stressor generates additional stressors, thereby blunting the otherwise damaging impact of the primary stressor on mental health. In support of this theoretical perspective, prior studies have identified some of the resources in adulthood (i.e., social support, self-esteem, and sense of community) that can protect against the long-term mental health effects of childhood adversity (DuMont, Widom, & Czaja, 2007; Greenfield & Marks, 2010b; Jonzon & Lindblad, 2006).
The Role of Religion
Although certain facets of religiosity (e.g., conservative religious beliefs) may have deleterious consequences for health and well-being, a wealth of research and theory has suggested that religiousness tends to be positively associated with psychological well-being (Koenig, King, & Carson, 2012). Further, religion provides cognitive, personal, and social resources that are particularly important during time of stress. Stress research highlights a process often referred to as buffering, where the detrimental effects of stressors on mental health are reduced for individuals who have resources to deal with them (Wheaton, 1985). Although some studies find that religion exacerbates the harmful effects of stress on mental health, a growing literature documents stress-buffering effects of religion (see Schieman, Bierman, & Ellison, 2013). Given that religion is a complex, multidimensional construct (Stark & Glock, 1968), the current study examines three important dimensions of religiousness: (a) religious attendance, (b) religious salience, and (c) spirituality. In the following, I outline theoretical views about the ways that multiple aspects of religious involvement mitigate the harmful effects of childhood adversity on adult mental health.
First, organizational religious involvement often measured by frequency of religious attendance can serve as a buffer for childhood adversity. Religious congregations provide unique opportunities for the exchange of social support for church members (Ellison & George, 1994). Church-based assistance can take a variety of forms. For example, tangible assistance such as financial aid and information provided both formally (via church programs) and informally (via informal networks) can be a valuable source of comfort and hope for victims of childhood adversity who suffer from economic hardship and physical illness. In particular, socioemotional aid (i.e., expressions of caring and love) exchanged among fellow church members is beneficial for the recipient, because psychological literature on social identity argues that individuals derive greater benefits from social support when provided by someone who shares common cultural values and social identity (Haslam, Jetten, Postmes, & Haslam, 2009). Indeed, the members of religious congregations tend to have a shared set of religious discourses concerning human suffering. Further, if coreligionists have similar adverse childhood experiences to share, socioemotional support provided by them in the form of healing words and consolation may hold particular psychological benefits for the recipient.
Religious salience may also be beneficial in a number of ways. Most religions encourage believers to develop an optimistic and positive outlook on both inner and outer reality (Koenig et al., 2012). Thus, individuals for whom religion is important are likely to affirm and internalize religious teachings that promote a positive interpretation of life events, including adverse experiences in childhood. This would help individuals reframe their early hardships into divine purposes, so that they are seen as an opportunity for personal or spiritual growth, rather than as a misfortune and threat (Idler, 1995). Such reframing makes early disadvantages less threatening to their core identities. In addition, given that most major world religions promote a value of caring for others, individuals who consider religion as important in their lives are likely to provide support for others in need (Putnam & Campbell, 2012). If religious persons with histories of childhood adversity help others and make a difference in the lives of others, they can gain a heighted sense of mattering, an important antecedent of psychological well-being (Pearlin & LeBlanc, 2001). Moreover, religious salience can promote more constructive responses (e.g., forgiveness) to negative experiences, enabling individuals to let go of feelings of anger, betrayal, and shame arising from adverse childhood experiences (Krause & Ellison, 2003).
Spirituality can help fend off the detrimental effects of childhood adversity on adult mental health. Although a clear distinction between spirituality and religiosity is elusive, spirituality can be characterized by its connection to the mystical, the supernatural, and the transcendent (Koenig et al., 2012). Thus, individuals with a high level of spirituality may benefit from a strong feeling of connection with a perceived divine other (e.g., God). Given that many religious traditions portray a divine other as loving and caring, individuals who view life as connected to a higher power can derive comfort, solace, and strengths from divine relations (Bradshaw, Ellison, & Marcum, 2010). This, in turn, may produce feelings of dignity and worth. Further, they may see their lives as imbued with spiritual power, which helps them successfully deal with stressful conditions in the long run. This may contribute to feelings of personal empowerment because people gain greater confidence that they can manage life stresses by virtue of the divine power (Schieman, Pudrovska, & Milkie, 2005). Overall, these feelings of self-worth and competence may be valuable to those who had considerable childhood adversity because early misfortune tends to promote feelings of hopelessness and helplessness that undermine self-perception (Irving & Ferraro, 2006). Moreover, individuals who are spiritual may perceive that there is an underlying order to life experiences and that these experiences fit into a larger scheme of things (Petersen & Roy, 1985). In turn, these beliefs help individuals create a framework of meaning with which to understand adverse experiences in childhood, which may lessen the potency of childhood adversity.
Taken as a whole, these theoretical and empirical arguments lead to the central hypothesis in this study that religious involvement (e.g., religious attendance, religious salience, and spirituality) may buffer against the deleterious effects of childhood adversity on adult mental health over time. Moreover, based on prior evidence that religiosity serves as a protective factor for individuals with reported childhood abuse (Dervic et al., 2006), I hypothesize that the stress-buffering effects of religion would be more pronounced in the context of childhood abuse relative to other types of childhood adversity.
Data and Method
Sample
This study uses two waves of data from the MIDUS study. The MIDUS study is a nationally representative survey of noninstitutionalized, American adults aged 20–74 with an oversampling of older males between 65 and 74. The first wave of data was collected in 1995. Data collection was carried out in two parts. Initially, respondents were contacted by phone through random digit dialing and asked to participate in a 30-min telephone interview. The response rate for these initial telephone interviews was 70%. Following this, respondents who participated in the telephone interview were mailed a more detailed, self-administered questionnaire (86.8% response rate). A total sample of 3,034 respondents completed both the telephone and mail interviews at the baseline with an overall response rate of 60.76% (.70 × .868 = .6076). Ten years later, participants in the first wave were recontacted for a follow-up survey. Of the 3,034 participants at the first wave, 1,748 individuals completed both the telephone interview and self-administered surveys at the second wave.
Of the 1,748 participants, 113 respondents (6.5%) did not have complete data across all of the variables. I used listwise deletion to handle missing data on account of item nonresponse. To assess the robustness of the results derived from listwise deletion, I employed multiple imputation in Stata 13 to handle missing values and estimated models. The findings from listwise deletion were fully consistent with the findings from multiple imputation. In the current study, I report the results based on listwise deletion. Hence, a final analytic sample consists of 1,635 respondents who participated in both waves of the MIDUS study and had complete information for all study variables. In terms of poststratification sample weights, the current study does not use them, because most of the variables used to construct the poststratification weights are included in the analytic models (Winship & Radbill, 1994).
Measures
Negative and positive affect
The dependent variables in this study consist of negative and positive affect that were used to measure mental health. Because prior research suggests that mental health is a multidimensional construct and that mental well-being is not necessarily identical to mental ill-being, it is useful to examine both positive and negative mental health outcomes (Huppert, 2009). These two variables were measured at both Wave 1 and Wave 2. In this study, negative affect is measured with an index composed of the mean value from the 6 items of distress such as “hopeless,” “nervous,” “restless or fidgety,” “so sad nothing could cheer you up,” “that everything was an effort,” and “worthless.” Respondents reported how often in the past 30 days they had experienced each of these symptoms on a 5-point scale (1 = none of the time, 2 = a little of the time, 3 = some of the time, 4 = most of the time, and 5 = all of the time). The Cronbach’s α for this scale is .85 for Wave 1 and .86 for Wave 2. Similarly, positive affect is measured with a 6-item mean index using questions that asked respondents how much of the time during the past 30 days they felt: “calm and peaceful,” “cheerful,” “extremely happy,” “full of life,” “in good spirits,” and “satisfied.” Respondents reported their experiences with each of these on a scale of 1 (none of the time) to 5 (all of the time). The Cronbach’s α for this index is .91 for both Wave 1 and 2.
Childhood adversity
One of the key independent variables is childhood adversity that comes from questions at Wave 1. Drawing from prior literature and available MIDUS questions on childhood (Schafer & Ferraro, 2013), I used 14 different indicators to generate three summary scores that encompass different domains of childhood adversity. These 14 indicators include physical abuse at the hands of a mother, father, siblings, or other person; emotional abuse by any of the same parties; parental divorce; lack of a male in the household; death of a parent; receipt of welfare; report of being “worse off” than other families; and less than a high school education for father (or mother in households where father was not present). Some of these measures were not initially coded as binary variables, so I recoded them as a dichotomous variable indicating experience of the given adversity. For example, in the case of both physical and emotional abuse, respondents who reported experiencing abuse “sometimes” or “often” from mother, father, siblings, or other were coded as 1 whereas experiencing abuse “never” or “rarely” from any of the same parties was not considered a report of abuse (coded as 0). Next, I divided the 14 adversity measures into three conceptual categories: abuse (both physical and emotional maltreatment), family instability (divorce, lack of male in household, and parental death), and financial strain (welfare, worse off than others, and low education for father or mother). These categories may be useful in advancing our knowledge about the unique effect of different types of early adversity on adult mental health.
Religious involvement
This study focuses on three aspects of religious involvement that were measured via the Wave 1 interview. First, the frequency of religious attendance is measured using responses to the following question: “How often do you usually attend religious or spiritual services?” Response categories include 1 = never, 2 = less than once a month, 3 = 1–3 times a month, 4 = about once a week, and 5 = more than once a week. Second, I measured religious salience using answers to the following 6 items: (a) “How religious are you?” (b) “How important is religion in your life?” (c) “How important is it for you—or would it be if you had children now—to send your children to religious or spiritual services for instruction?” (d) “How closely do you identify with being a member of your religion?” (e) “How much do you prefer to be with other people who are the same religion as you?” and (f) “How important do you think it is for people of your religion to marry people who are the same religion?” Response options include 1 = not at all, 2 = not very, 3 = somewhat, and 4 = very. The scale consists of the mean of the 6 items (Cronbach’s α = .88). Third, spirituality is measured with a mean index of 2 items: (a) “How spiritual are you?” and (b) “How important is spirituality in your life?” Response categories for each item range from (1) not at all to (4) very (Cronbach’s α = .89).
Control measures
I control for several demographic variables measured at Wave 1 that prior research found to be related to focal variables in the study (Bradshaw & Ellison, 2010; Krause, 2009). These variables include age (continuous), gender (1 = female and 0 = male), race (“White” is contrasted with “Black” and “others”), marital status (“married” is contrasted with “divorced/separated,” “widowed,” and “never married”), educational attainment (from 1 = no school/some grade school to 12 = PhD, EdD, MD, DDS, LLB, LLD, JD, or other professional degree), and household income (logged).
Analytical Strategy
The current study estimates a series of ordinary least squares (OLS) regression models to address its research question. The central question in the study focuses on whether the deleterious effects of childhood adversity on adult mental health become progressively weaker at successively higher levels of religious involvement. Two steps were taken to deal with this question. In the first step, I used OLS regression to model change in mental health, regressing mental health outcomes at Wave 2 on key independent variables (W1), control measures (W1), and mental health scores at Wave 1. The analytical models incorporate change in mental health because prior theory and evidence suggests that both positive and negative affect change over the life course (Carstensen, 1995; Charles, Reynolds, & Gatz, 2001). Using this lagged dependent variable model enables us to examine how childhood adversity exerts additional influence on mental health over time net of the baseline levels. In addition, this model helps prevent endogeneity bias due to any change in religious involvement brought about by mental health. In the second step, the multiplicative terms assessing the interaction between childhood adversity and religious involvement were added to the equation. These multiplicative terms were created by multiplying each domain of childhood adversity (e.g., childhood abuse, family instability, and financial strain) by each category of religious involvement (e.g., religious attendance, religious salience, and spirituality) at Wave 1. I use these multiplicative terms to test for the proposed interaction effect between childhood adversity and religious involvement on change in mental health. I centered the variables prior to creating interaction terms, which diminishes multicollinearity between the interaction coefficients and lower order terms (Aiken & West, 1991). The variance inflation factors for all regression models are within conventional standards (i.e., below 2.5), which indicates that multicollinearity does not affect the results (Allison, 2012).
A common problem with using panel data is that sample attrition can bias the results. To address this issue, I employ Heckman’s (1979) selection bias models to adjust for nonrandom selection effect. I first estimated a probit model to differentiate respondents who participated at the follow-up interview from those who did not. I subsequently estimated the selection instrument (λ) based on the inverse Mills ratio that represents the likelihood of remaining in the study. I included this selection instrument (λ) in the substantive regression models. Additional analyses not shown here reveal that results do not differ when I do not correct for selection.
Results
Table 1 shows descriptive statistics for all study variables. Mean levels of negative affect were low and showed a modest, but nonsignificant decline between waves, with the average respondent experiencing negative affect somewhere between none of the time and a little of the time. Levels of positive affect were moderate and showed a slight, but nonsignificant increase between waves. On average, respondents experienced positive affect somewhere between some of the time and most of the time. With respect to childhood adversity, the most prevalent of the three categories of childhood adversity was childhood abuse (64.3%) whereas the least prevalent category was family instability (18.8%). On average, respondents reported “often” or “sometimes” experiences of nearly two types of childhood abuse, whereas they experienced less than one form of financial strain. In addition, average respondents rarely experienced family instability during childhood. In terms of religious involvement, average respondents attended religious services almost 1–3 times a month. On scales of 1–4, mean levels of religious salience and spirituality were 2.753 and 3.084, respectively, showing that respondents have a slightly higher level of spirituality than religious salience.
Descriptive Statistics for All Study Variables.
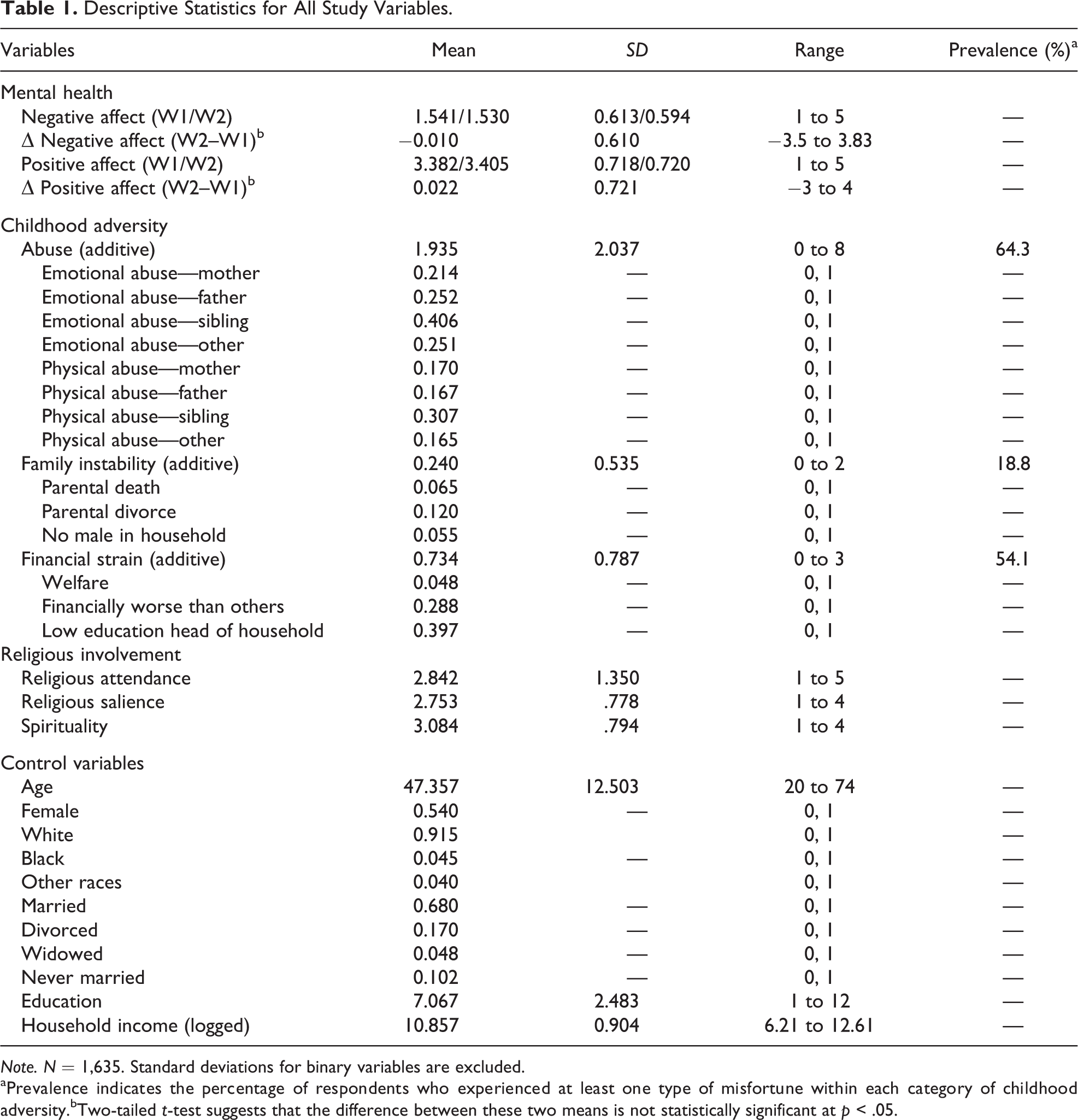
Note. N = 1,635. Standard deviations for binary variables are excluded.
aPrevalence indicates the percentage of respondents who experienced at least one type of misfortune within each category of childhood adversity.bTwo-tailed t-test suggests that the difference between these two means is not statistically significant at p < .05.
Table 2 shows the results of OLS regression analyses that are designed to examine whether religious involvement moderates the effects of childhood adversity on change in negative affect over time. In Model 1, the results seem to indicate that more severe childhood adversity does not lead to a greater increase in negative affect over time. Moreover, none of the religious involvement variables has a statistically significant effect on change in negative affect. In addition, the findings obtained estimating Models 2 through 4 suggest that there is no significant interaction effect between childhood adversity and religious involvement on change in negative affect across the two waves of data.
OLS Regression of Negative Affect (W2) on Negative Affect (W1), Childhood Adversity (W1), Religious Involvement (W1), and Interactions.
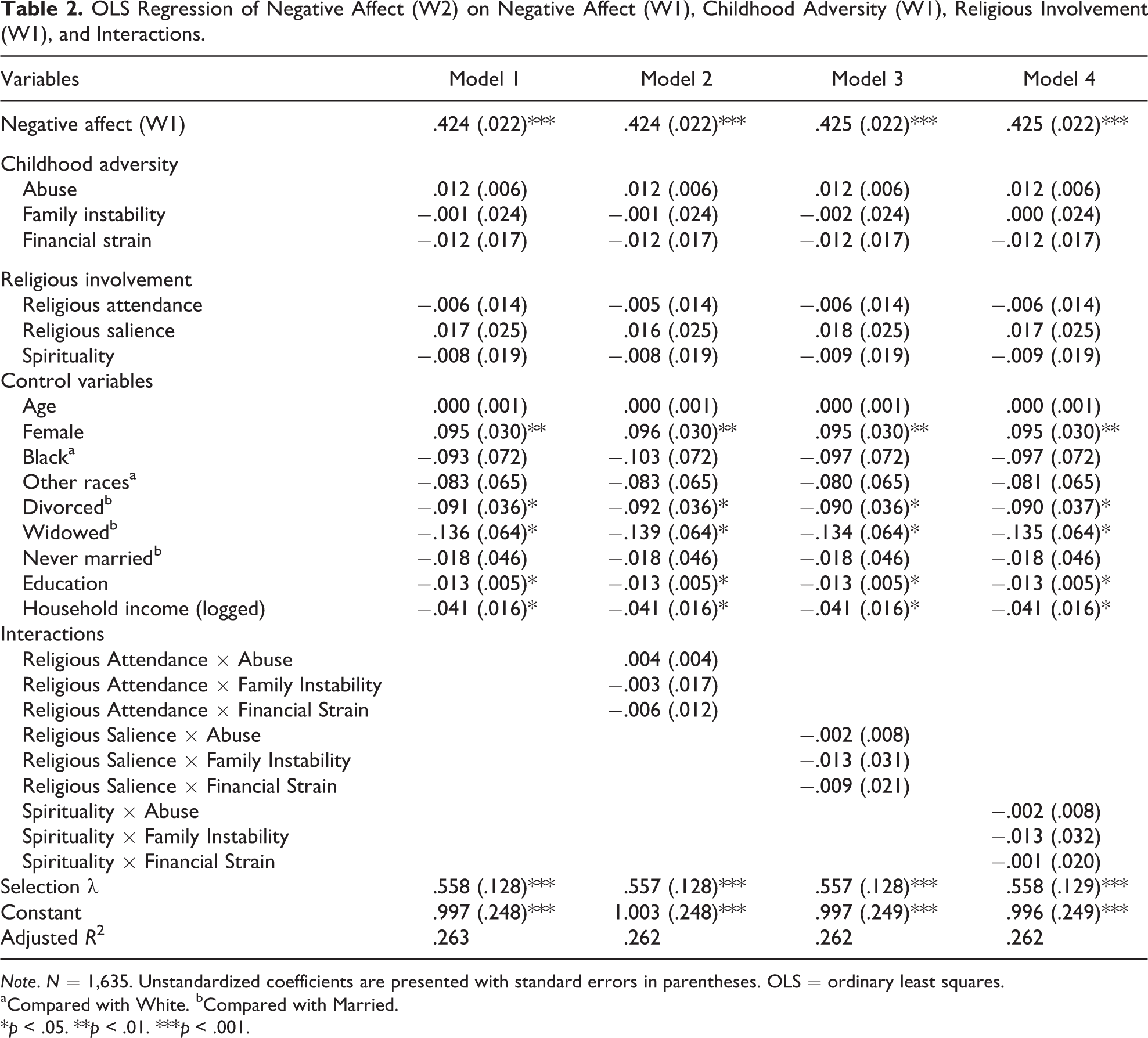
Note. N = 1,635. Unstandardized coefficients are presented with standard errors in parentheses. OLS = ordinary least squares.
aCompared with White. bCompared with Married.
*p < .05. **p < .01. ***p < .001.
Table 3 replicates the analyses above for positive affect. Model 1 reveals that among measures of childhood adversity, only childhood abuse has a significant effect on change in positive affect (b = −.020, p < .05). This observation indicates that individuals who experienced more severe childhood abuse report greater decreases in positive affect over time. In terms of religious involvement, none of the indicators of religious involvement has a significant effect on change in positive affect. Further, Model 2 suggests that a significant interaction effect between childhood adversity and church attendance fails to emerge from the data. On balance, these findings may create the impression that positive affect is not substantially affected by either childhood adversity or religious involvement. However, the results shown in Models 3 and 4 provide a different picture.
OLS Regression of Positive Affect (W2) on Positive Affect (W1), Childhood Adversity (W1), Religious Involvement (W1), and Interactions.
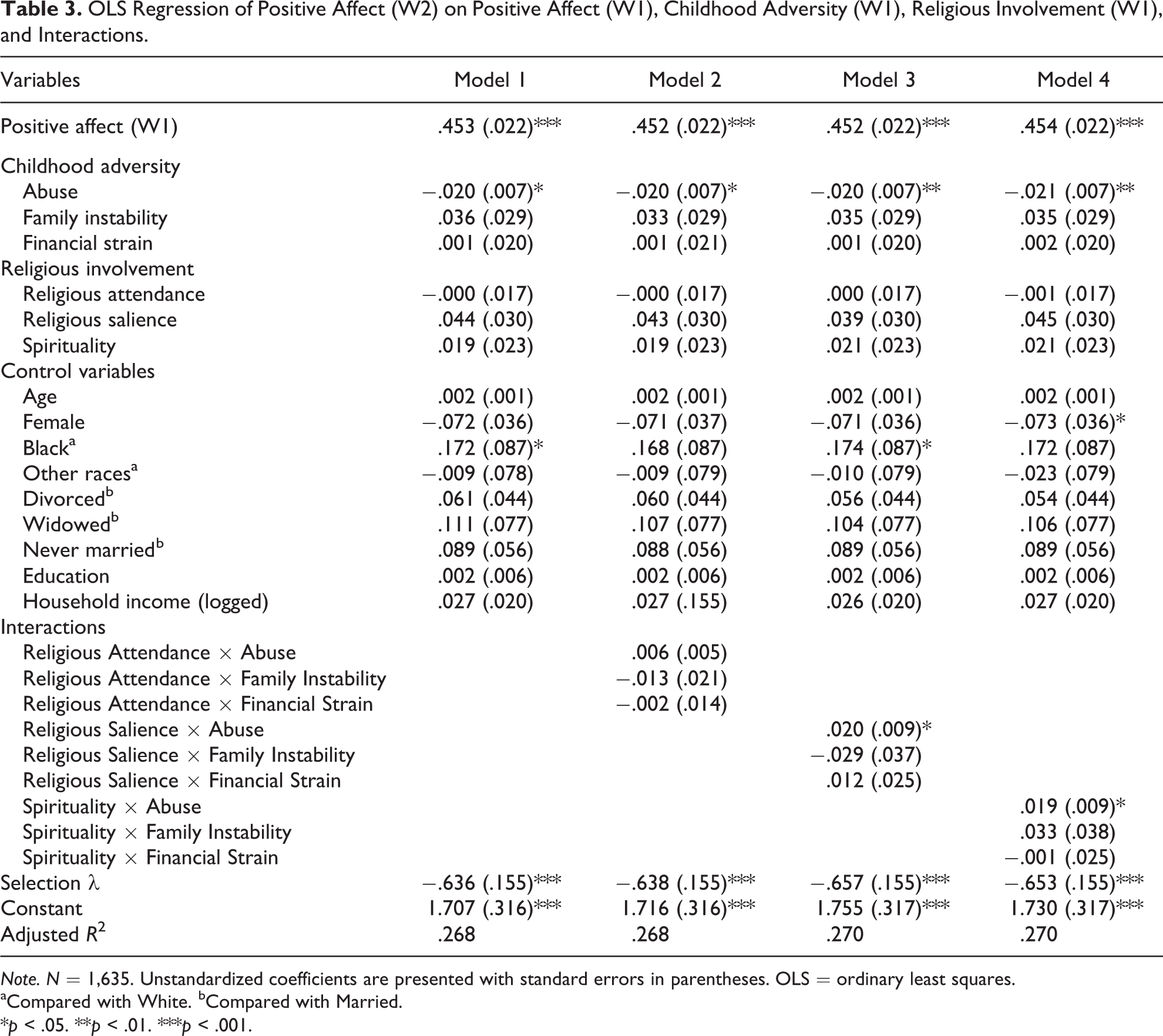
Note. N = 1,635. Unstandardized coefficients are presented with standard errors in parentheses. OLS = ordinary least squares.
aCompared with White. bCompared with Married.
*p < .05. **p < .01. ***p < .001.
Model 3 demonstrates that religious salience significantly interacts with childhood adversity to influence change in positive affect over time. Specifically, the coefficient for the interaction term between childhood abuse and religious salience is positive (b = .020, p < .05). In order to assess the direction of this interaction effect, I use formulas provided by Aiken and West (1991) to estimate the effects of childhood abuse on change in positive affect at select levels of religious salience. Panel A of Table 4 provides the findings from these additional analyses. It shows that childhood abuse is associated with a decrease in positive affect (b = −.036, p < .01) for individuals who have lower levels of religious salience (e.g., 1 standard deviation below the mean). However, the undesirable impact of childhood abuse on change in positive affect over time is entirely offset (b = −.004, ns) for individuals who have higher levels of religious salience (e.g., 1 standard deviation above the mean). These observations suggest that the detrimental effects of childhood abuse on positive affect become progressively weaker at successively higher levels of religious salience. Taken together, these analyses reveal the stress-buffering benefits associated with religious salience.
The Effects of Childhood Abuse (W1) on Positive Affect (W2) at Each Level of Religious Salience and Spirituality.
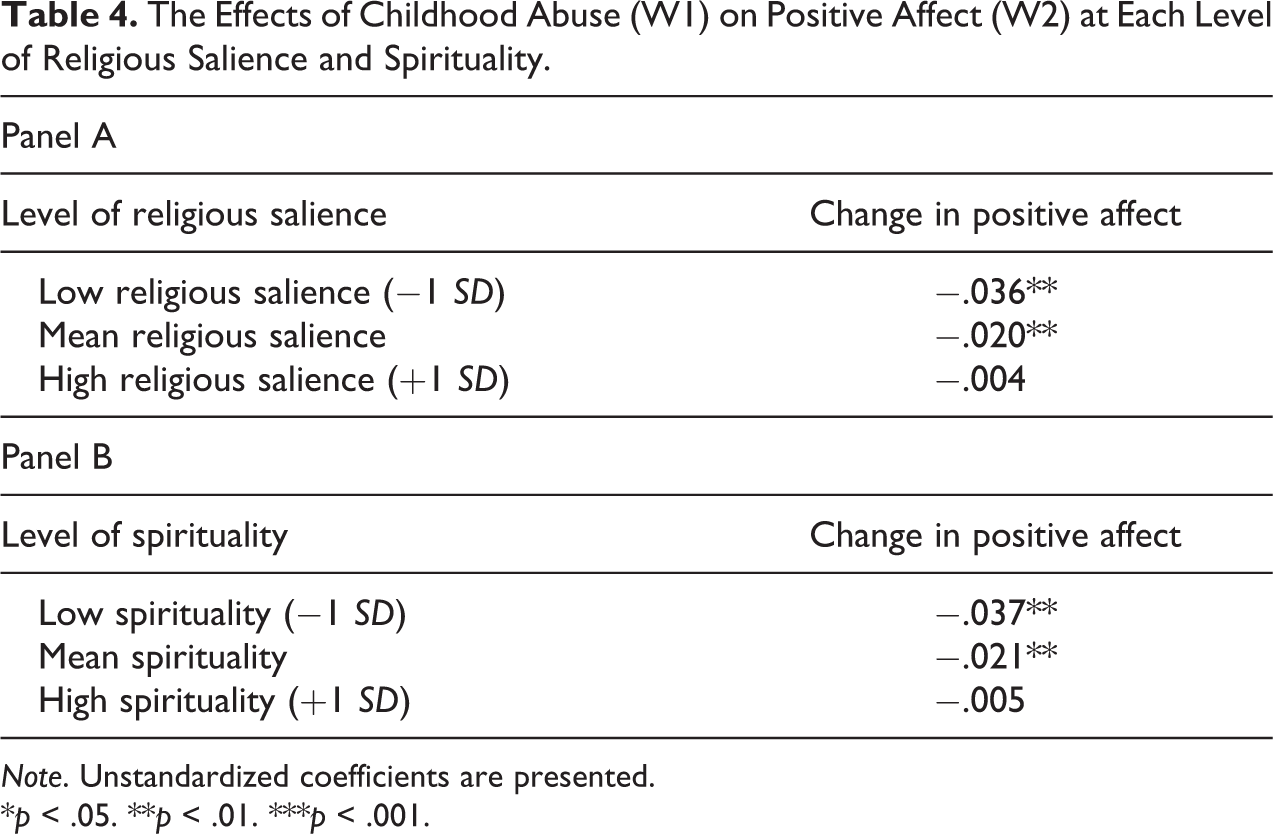
Note. Unstandardized coefficients are presented.
*p < .05. **p < .01. ***p < .001.
Model 4 in Table 3 displays a similar pattern. The cross-product term between childhood abuse and spirituality is significant and positive (b = .019, p < .05), suggesting that spirituality mitigates the noxious effect of childhood abuse on change in positive affect over time. Panel B of Table 4 illustrates this pattern. The additional calculations based on Aiken and West (1991) indicate that childhood abuse is associated with a decrease in positive affect (b = −.037, p < .01) for individuals who have lower levels of spirituality (e.g., 1 standard deviation below the mean). However, childhood abuse fails to exert a harmful effect on change in positive affect (b = −.005, ns) for individuals who have higher levels of spirituality (e.g., 1 standard deviation above the mean). Collectively, these observations suggest that the pernicious effects of childhood abuse on positive affect are less severe for individuals who are committed to spiritual life.
Discussion
It is well established that childhood adversity represents a prominent stressor that has noxious mental health consequences in adulthood. However, little is known about the role of religion as a moderating influence in the association between childhood adversity and adult mental health. Using the stress process model as a guiding framework, the current study examines how religious involvement in adulthood moderates (i.e., buffers) the effects of childhood adversity on change in negative and positive affect in adulthood. The analyses in the study find that religious salience and spirituality buffer the harmful effects of childhood abuse on change in adult positive affect over time. However, no stress-buffering effects involving religious attendance surface. Further, the analyses reveal no evidence that the deleterious effects of childhood adversity on change in adult negative affect are reduced for individuals who are deeply involved in religious activities.
Several contributions emerge from the present analysis. First, the current analysis shows that childhood abuse matters more than other types of early adversity. Specifically, childhood abuse is damaging for positive affect over time, while early socioeconomic strain and family instability fall short of generating a marginal decline for positive affect beyond baseline levels. Childhood abuse leaves an enduring mark on the victim over the life course, interrupting various aspects of adult life including mental health (Greenfield & Marks, 2010a). Of particular note, childhood abuse may affect stress-related biological systems during critical developmental period, which can have long-standing damaging influences on mental health over the life span (Putnam & Trickett, 1997). This process tends to be triggered by extremely severe experiences such as childhood abuse, which early financial strain and family instability may fail to accelerate.
Second, the current study provides some evidence that adult religious involvement serves as a protective factor against the long-term negative psychological effects of childhood adversity. This observation is consistent with the stress process proposition that personal resources modify the effects of stressors (Pearlin, 1989). Broadly speaking, this evidence reinforces prior research that found mental health benefits of religious involvement, particularly during times of stress (Koenig et al., 2012). Specifically, my findings suggest that religious salience and spirituality mitigate the noxious effects of childhood abuse on change in positive affect over time. Compared to other types of early adversity, childhood abuse can be thought of as a chronic stressor that is difficult to control, something that cannot be altered or reconciled easily. Thus, the role of religion may become more relevant for childhood abuse (Gottlieb, 1997). Religious salience and spirituality are beneficial for dealing with childhood abuse because they may promote a sense of peaceful acceptance among the victims, which helps reduce the effects of childhood abuse. Further, individuals who are highly religious or spiritual tend to view their lives as a part of a divine master plan, such that they may let go of hurt by reframing their early adversities as positive opportunities for religious and spiritual growth (Idler, 1995).
Third, this study finds that religious attendance does not provide a buffering effect. One possible explanation for this pattern may involve religious doubt (Krause & Ellison, 2009). Religious individuals who have been victimized by early misfortune may come to perceive life to be unjust or unfair, questioning the benevolence of God (Bierman, 2005). Having troubled relationships with God, these religious people may fall into religious doubt, a specific instance of cognitive dissonance. Given that religious scriptures sometimes condemn those who entertain doubt, religious doubt may carry stigma within religious congregations. Moreover, individuals with significant doubts tend to have religious views that differ from those embraced by their fellow coreligionists. This may prevent individuals with doubts from interacting frequently with members of their congregations, which in turn deprives them of a potentially valuable source of spiritual and social support. Yet, this line of explanation is speculative. Further analysis with richer measures of religious doubt and congregational life would expand our understanding of this pattern.
Fourth, this study finds that religiosity buffers the effects of childhood adversity only for positive affect; the stress-buffering properties of religion are not observed with negative affect. Ancillary analyses not shown here reveal that the stress-buffering effects of religion fail to emerge when depression serves as the outcome measure. Perhaps these patterns indicate that religion tends to influence more positive aspects of mental health, instead of improving negative and positive facets of mental health together. In some sense, being more distressed by childhood adversity may appear to be more serious and detrimental than decreases in well-being. Hence, it may be that religion helps protect individuals from less pernicious effects of childhood adversity on mental health, the ability of childhood adversity to make people less happy and satisfied. Future investigations can examine more closely why religion is a protective factor only for the effects of childhood adversity on positive affect.
Fifth, unlike most studies that examine the link between religion and mental health, the current study capitalizes on longitudinal analyses to establish clear temporal ordering among focal measures, an important precondition for causality. One of the shortcomings of previous scholarship on the stress-buffering effects of religion is that it uses cross-sectional data and cannot rule out the possibility that those who have better mental health may be more likely to participate in religious practices (Bradshaw & Ellison, 2010). In order to control for this possibility and perform more rigorous tests of religion’s moderating effects, the current study conducts longitudinal analyses to examine whether more religious persons exhibit better mental health following childhood adversity over time. This study finds that adults report a smaller decrease in positive affect across two waves of data following childhood abuse if they report higher levels of religious involvement in adulthood. These findings are notable because this study appears to be the first time that the interface between childhood adversity, religion, and mental health has been assessed with data gathered at more than one point in time.
Several study limitations should be noted. First, childhood adversity is a retrospective measure that is subject to potential recall bias. For example, individuals who have poor mental health may retroactively interpret life experiences in more negative terms and thus report more severe childhood adversity. While this may be a problem, prior research shows that the ability to recall significant experiences and events is relatively stable (Hardt & Rutter, 2004). Second, although this study assesses the role of multiple facets of religiosity in mitigating the psychological effects of childhood adversity, it is also possible that other aspects of religiosity may provide a buffering effect. For example, prayer and belief in an afterlife can be promising candidates. Recent investigations highlighted the mental health benefits associated with prayer and beliefs in an afterlife, which make stressful conditions less distressing (Bradshaw & Ellison, 2010; Krause, 2009).
Third, even though this study finds that childhood adversity interacts with religion to affect adult mental health, it fails to specify the intervening variables linking these constructs. For example, I mentioned the possibility that religion may provide a buffering effect by bolstering self-esteem and perceived control, but no effort was made to empirically evaluate these linkages. Thus, additional studies are necessary to advance our knowledge of these linkages. Fourth, despite this study’s evidence for religion as a protective factor against the harmful psychological effects of childhood adversity, it is still unclear when these stress-buffering effects of religion emerge across the life course. Accordingly, future investigations can shed light on the processes through which religion protects mental health following childhood adversity at diverse ages throughout adulthood.
Conclusion
The current study makes a significant contribution to the literature by documenting the role of religion in buffering the deleterious mental health effects of childhood adversity. The findings in the study indicate that the noxious effects of childhood abuse on positive affect are reduced for adults who have high levels of religious salience and spirituality over time. A more refined understanding of the interrelationships among childhood adversity, religion, and mental health would have both theoretical and practical benefits. In sum, this study finds that adverse childhood experiences do not necessarily lead to poor mental health in adulthood. Rather, religion acts as a countervailing mechanism that may cushion the effects of early misfortune later in the life course.
Footnotes
Acknowledgements
The author thanks Hyoyoup Shim, Daniel V.A. Olson, Daniel Winchester, Kenneth Ferraro, Shawn Bauldry, Joe Marshall, Fanhao Nie, Tyler Anderson, and Shirley Olson for their suggestions and help as well as the editor and anonymous reviewers for their valuable comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.