
Abstract
This research examines whether unobserved time-stable influences confound the association between chronic pain and psychological distress in older adults as well as how race and ethnicity combine with subjective social status (SSS) to modify the association. In a nationally representative longitudinal survey, holistically controlling for unobserved time-stable influences using fixed-effects models substantially reduces the pain–depression relationship and eliminates the overall pain–anxiety relationship. The association with depression is stronger for Black and Hispanic elders, illustrating a process of double-jeopardy. Black elders with severe pain experience lower anxiety, as do Black elders with moderate pain and low SSS, which we suggest may be due to the enervating effects of undermanaged pain. Black elders at high SSS experience greater anxiety with moderate pain. This research suggests that undermanagement of chronic pain among racial and ethnic minorities differentiates the association between pain and distress in late life and especially creates stronger associations with depression.
This research examines the association between chronic pain and psychological distress in older adults. The consequences of pain are important to examine in older adults because the risk of experiencing chronic pain increases with age (Johannes, Le, Zhou, Johnston, & Dworkin, 2010). Pain can be quite stressful, as research shows that chronic pain is associated with psychological distress (Bierman, 2011; Castillo et al., 2013; Gayman, Brown, & Cui, 2011), which is often characterized as symptoms of depression and anxiety (Mirowsky & Ross, 2003). Examining symptoms of both depression and anxiety is useful for understanding the overall consequences of pain for mental health because symptoms of depression and anxiety often reflect a range of psychiatric disorders (Kessler et al., 2002). Moreover, research has tended to focus on depression far more than anxiety (Gureje et al., 2008), with the result that previous studies may be overlooking how pain is associated with one of the major indicators of mental health problems.
Despite evidence supporting an association between pain and psychological distress, previous research may have overstated this association by failing to adequately account for time-stable factors that act as confounders. A time-stable factor is any “attribute that does not change over time” Page 595. (Bierman, 2011, p. 595), regardless of whether the factor is directly measured. A confounder is a factor that influences both a putative causal agent and an outcome, thereby falsely creating the appearance of an association between the agent and outcome (Weinberg, 1993). There is a diverse set of time-stable factors that may influence both the experience of pain and psychological distress. For example, both pain responses and symptoms of distress have substantial heritability factors (Demirkan et al., 2011; Norbury, MacGregor, Urwin, Spector, & McMahon, 2007), leading to common genetic and biological pathways that could confound their association (Gambassi, 2009). On a broader level, adversities earlier in the life course are associated with mental health problems and heightened stress responses as well as the experience of pain (Jones, Power, & Macfarlane, 2009; Patten et al., 2015; Pieritz, Rief, & Euteneuer, 2015). Failing to completely rule out the influence of these time-stable factors may therefore falsely create the appearance of an association between pain and psychological distress. Previous research has statistically removed—or “controlled”—the influence of time-stable factors using observed measures (e.g., Castillo et al., 2013; Gayman et al., 2011), but it is unlikely that analyses will be able to control for the breadth of the potential time-stable confounders through observed measures alone. In addition, time-stable components of depression and anxiety may have led reverse causation to be a factor in some previous studies, as research suggests that trait components of anxiety and depression can influence the experience of pain (Sullivan, Thorn, Rodgers, & Ward, 2004; Tang & Gibson, 2005; Vossen, van Os, Hermens, & Lousberg, 2006). Ruling out time-stable influences can therefore also provide more robust support for pain as a causal factor in psychological distress in late life by eliminating the influence of dispositional tendencies toward distress on pain.
As an alternative to previous analyses that have relied on observed measures to control for time-stable confounders, in this research, we employ an econometric approach called “fixed-effects models” (Allison, 2009). The fixed-effects model holistically controls for all time-stable factors—meaning that the influence of all possible unchanging sources of confounding are statistically removed, even if these sources are not directly observed. Thus, the first contribution of this research is in examining whether the association between pain and symptoms of both depression and anxiety in a nationally representative sample of older adults holds when time-stable confounders are holistically controlled. We hypothesize that pain will be associated with psychological distress in late life when statistical controls are based only on observed measures, but we also hypothesize that the association between pain and psychological distress will be substantially reduced when all time-stable sources of confounding are controlled through the application of fixed-effects models.
Double-Jeopardy of Minority Race and Ethnicity
Research on aging and mental health suggests, however, that the consequences of aging may be especially detrimental for racial and ethnic minorities, in what has been called a process of “double-jeopardy” (Carreon & Noymer, 2011). The question of double-jeopardy is likely to be particularly relevant when examining the consequences of pain because of a well-documented pattern in which pain among racial and ethnic minorities is less likely to receive adequate management from health-care providers (Heckman & Britton, 2015; Shavers, Bakos, & Sheppard, 2010). As a result, pain may have greater detrimental consequences among racial and ethnic minorities. Although research has not consistently supported the double-jeopardy hypothesis as it pertains to mental health (Barry et al., 2014; Liang, Xu, Quiñones, Bennett, & Ye, 2011; Spence, Adkins, & Dupre, 2011), this research has not tended to focus on differences in the effects of stressful experiences that occur in late life, such as chronic pain. Therefore, a second important contribution of this research is examining race and ethnic differences in the association between chronic pain and symptoms of distress in older adults. Specifically, we hypothesize that, after time-stable confounders are holistically controlled, the association between chronic pain and psychological distress will be stronger for older adults who are racial and ethnic minorities as compared to White older adults.
Differences Due to Subjective Social Status (SSS)
Sociological perspectives on mental health suggest that socioeconomic status (SES) may also modify the consequences of stress exposure (Pearlin & Bierman, 2013). An individual’s subjective ranking of social standing, called “subjective social status,” may especially be important as a measure of SES in studies of older adults because more objective indicators of SES become less relevant as careers are ended and incomes are curtailed (Demakakos, Nazroo, Breeze, & Marmot, 2008; Wright & Steptoe, 2005). Furthermore, the potential importance of SSS as a stress buffer is suggested by research showing SSS is inversely associated with biological markers of stress responses, such as inflammation, waking cortisol, and health shock proteins (Derry et al., 2013; Muscatell et al., 2016; Saban, Hoppensteadt, Bryant, & DeVon, 2014; Wright & Steptoe, 2005). SSS may buffer the effects of stressors, such as chronic pain, because individuals with high levels of SSS have a greater reliance on active forms of coping that more efficaciously address problems (Adler, Epel, Castellazzo, & Ickovics, 2000; Derry et al., 2013). Moreover, as a broad reflection of one’s overall social standing, SSS likely denotes degree of access to a range of resources that may aid in coping with the experience of pain (Chen, Covinsky, Stijacic Cenzer, Adler, & Williams, 2012). Therefore, an important additional contribution of this research is in examining whether SSS modifies the association between pain and psychological distress in older adults. We hypothesize that, after time-stable confounders are holistically controlled, the association between pain and psychological distress among older adults will be weaker at higher levels of SSS.
Diminishing Returns on SSS
The racial–ethnic background of seniors and their SSS may intersect to shape the association between pain and psychological distress. The “diminishing returns” hypothesis suggests that, due to structures of discrimination, higher levels of SES may not convey as strong of physical and mental health advantages for racial and ethnic minorities as for Whites (Farmer & Ferraro, 2005; Hudson et al., 2012). This argument is supported by studies showing that socioeconomic attainment is more weakly associated with well-being particularly among African Americans and also that these differences increase with age (Farmer & Ferraro, 2005; Shuey & Willson, 2008). More specific to pain, Black individuals are more likely to prematurely terminate headache treatment regardless of SES, while Whites with higher SES have the lowest risk of premature termination (Heckman et al., 2008). These findings demonstrate how higher SES may convey advantages in addressing pain, but more for White than ethnic and racial minority seniors. The final contribution of this research is therefore in examining whether SSS intersects with the race and ethnicity of seniors to jointly modify the association between pain and psychological distress. We hypothesize that, after time-stable confounders are holistically controlled, SSS will more strongly buffer the association between pain and psychological distress among White older adults than for older adults who are racial and ethnic minorities.
Method
Data
This study utilizes data from the Health and Retirement Study (HRS), an ongoing survey of adults aged 51 and over from the United States (Sonnega et al., 2014). In 2006 and 2008, a psychosocial and lifestyle questionnaire was added to the HRS, with half of the core HRS respondents receiving the questionnaire in 2006 and the second half receiving the questionnaire in 2008 (Smith et al., 2013). There were 7,167 respondents with valid values for the psychosocial subsample survey weight in 2006 and 6,177 in 2008, for a total of 13,344 respondents. Ninety-two respondents were subsequently dropped from analyses due to the use of proxy responses, producing an overall sample size of 13,252. Because there were a small number of respondents who were not White, Black, or Hispanic, seniors of other races or ethnicities were not included in the analyses, reducing the analytic sample to 12,988. The subsamples were surveyed a second time 4 years later, with the 2006 subsample resurveyed in 2010 and the 2008 subsample resurveyed in 2012. Of the original 2006 sample, 6,128 respondents completed the pain follow-up in 2010 (for an 85.5% retention rate), and of the 2008 sample, 5,624 respondents completed the pain follow-up in 2012 (for a 91% retention rate). Analytic approaches that address sample attrition and item nonresponse are addressed below. Respondents for the 2006 and 2008 psychosocial subsamples were combined to create a Time 1 observation point, and responses to the 2010 and 2012 psychosocial subsamples were combined to create a Time 2 observation point 4 years later. Subsequent waves of the HRS did not include the anxiety measure that is of focal interests in this study. All analyses are computed with Stata Version 14.2 and utilize sampling weights to account for differential probabilities of selection and response; information on clustering and sampling design is also utilized in the estimation of standard errors and significance tests.
Focal Measures
Distress
Symptoms of depression at each wave were measured using an 8-item version of the Center for Epidemiological Studies–Depression Scale that has been validated for use in older adults (Karim, Weisz, Bibi, & Rehman, 2015): felt depressed, everything you did was an effort, sleep was restless, you were happy (reverse coded), felt lonely, enjoyed life (reverse coded), felt sad, and could not get going. Responses were a yes or no checklist as to whether each symptom had been experienced in the previous week, and in keeping with common practice in studies of the depression using the HRS, positive responses were summed to create a measure of depressive symptomology ranging from 0 to 8 (Cronbach’s α = .80–.81). Anxiety was measured at each wave using 5 items adapted from the Beck Anxiety Inventory (Beck, Epstein, Brown, & Steer, 1988): fear of the worst happening, nervous, felt my hands trembling, had a fear of dying, and felt faint. Respondents indicated experiences of these symptoms in the past week on a scale of 1 (never) to 4 (most of the time). The Beck Anxiety Inventory “has been shown to distinguish symptoms of anxiety from depression and to be valid for use in older populations” (Smith et al., 2013, p. 46). To further demonstrate validity of this measure, we performed a principal axis factor (PAF) analysis on a polychoric correlation matrix of responses to the anxiety items in the HRS. At each wave, the PAF analysis indicated one factor with an eigenvalue above 1 that accounted for over 60% of the variance in the items, with the next factor having an eigenvalue of approximately 0.3. When the first factor was extracted, loadings were approximately 0.73–0.84 for all items, generally providing strong evidence that these questions are similarly reflective of the same underlying construct. The mean of responses was therefore used as the indication of anxiety (Cronbach’s α = .81 at both waves).
Chronic pain
Chronic pain was measured using the combination of two questions. First, respondents were asked, “Are you often troubled with pain?” Individuals responding in the affirmative were then asked, “How bad is the pain most of the time: mild, moderate, or severe?” Because preliminary analyses did not indicate strong discrimination between mild and moderate, responses to these two categories were combined and a set of dichotomous variables was created: moderate (mild/moderate) and severe, with no chronic pain used as the reference. Although brief, this measure has frequently been used in previous research on pain in older adults (e.g., Covinsky, Lindquist, Dunlop, & Yelin, 2009; Reyes-Gibby, Aday, Todd, Cleeland, & Anderson, 2007).
Race and ethnicity was based on codings of White, Black, and Hispanic, in which a set of dichotomous variables for Black and Hispanic were compared to White. There were a small number of cases who overlapped in Black and Hispanic (n = 24), and because minority race is more likely to be immediately visibly ascertained, these respondents were coded as Black.
SSS
SSS was measured using the MacArthur Scale of SSS, in which respondents are presented with the image of a ladder and told, Think of this ladder as representing where people stand in our society. At the top of the ladder are the people who are the best off—those who have the most money, most education, and best jobs. At the bottom are the people who are the worst off—who have the least money, least education, and the worst jobs or no jobs. The higher up you are on this ladder, the closer you are to the people at the very top and the lower you are, the closer you are to the people at the very bottom.
Observed Control Measures
Observed control measures are based on chronic health conditions that may engender pain and also affect distress as well as fundamental social statuses that are associated with stress exposure and mental health (Aneshensel, Phelan, & Bierman, 2013). Chronic health conditions were based on a summative count of seven conditions: cancer of any kind (excluding skin), high blood pressure or hypertension, diabetes or high blood sugar, chronic lung disease such as chronic bronchitis or emphysema, heart condition (heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems), stroke, and arthritis or rheumatism. Core social statuses include age, gender, and marital status as well as alternative dimensions of SES. Age was measured in years at baseline. Gender was coded 0 = men, 1 = women. Marital status was measured based on a set of dichotomous variables—divorced, widowed, and never married—with the married as reference. Alternative components of SES were controlled using multiple measures. First, education was based on two dichotomous variables—less than a high school degree and high school degree—with greater than a high school degree as reference. Second, because income tends to be less useful as a measure of SES in late life, we used self-assessed difficulty paying bills, which is a common indicator of economic hardship (Mirowsky & Ross, 2003). For this measure, some difficulty and very/complete difficultly contrasted with none/not very difficult. Third, individuals reported at each wave whether they were currently employed, and this variable was coded so that the higher value indicated currently working.
Methods of Analyses
Analyses are based on random- and fixed-effects models. A random-effects model is useful in longitudinal analyses because standard errors are adjusted for repeated observation, but confounding is still addressed based only on the observed measures that are included as controls (Wooldridge, 2010). A fixed-effects model is similar to a random-effects model, but controls for all time-stable confounds, even if these time-stable influences are not observed (Allison, 2009). Comparing the random- and fixed-effects models therefore indicates the extent to which analyses may be biased when only the observed controls are included in the model.
Random- and fixed-effects models are estimated through structural equation modeling (SEM; Allison, 2009). In this procedure, the outcome across time points is used as an indicator for a latent variable called α. α represents the influence of all time-stable factors on the outcome, and the factor to indicator paths are set to 1 to represent the consistent influence of these time-stable factors. When α is allowed to covary with the time-varying predictors, the result is fixed-effects coefficients, and when this covariance is disallowed, the result is random-effects coefficients. In addition, time-stable predictors can be retained in the model to produce random-effects coefficients by disallowing covariance between α and the predictors. Interactions between time-stable predictors and the time-varying predictors can also be allowed to covary with α and produce fixed-effects coefficients.
An additional advantage of the SEM approach to random- and fixed-effects models is that these models can be estimated through full information maximum likelihood (FIML) estimation. FIML estimation integrates all information available from each case, thereby providing less biased analyses when sample attrition occurs than methods using list-wise deletion, and estimates are identical to those created by multiple imputation with the same model and data (Allison, 2003; Collins, Schafer, & Kam, 2001). FIML assumes that data are missing at random, meaning that missing data can be predicted by other variables included in the model and are not due to values on the missing data (Enders, 2010). Because we include multiple strong indicators of mortality, such as education and chronic conditions, it is likely that we are accounting for the major cause of sample attrition in terms of mortality. Furthermore, even when data are not missing at random, methods that assume data are missing at random produce better estimates than more conventional estimation techniques (Allison, 2003).
Results
Sample Characteristics
Table 1 presents weighted descriptives for the study measures and sample characteristics. The baseline mean age of the sample is 66, and the sample has a slightly higher percentage of women than men. About 30% of the sample has more than a high school degree, and a little over 16% has less than a high school degree. In terms of the focal measures, race is treated as time stable in the model, and at baseline the sample is composed of approximately 9% Black seniors and 7% Hispanic seniors. Both pain and the measures of psychological distress are time varying. At each wave, seniors reported an average of just under two symptoms of depression and a relatively low mean level of anxiety of just over 1.5 on a scale of 1–4. Furthermore, about 6% of the sample at each wave experienced severe chronic pain, and about 30% of the sample experienced moderate pain. SSS is also time varying, but since SSS was centered over a value of 6, means for SSS indicate deviations above or below this value. Thus, means of 0.459 at Wave 1 and 0.383 at Wave 2 for SSS indicate that mean SSS is about 6.5 at Wave 1 and about 6.4 at Wave 2.
Study Descriptives.

Note. N = 12,989. Descriptives are weighted and calculated through full information maximum likelihood estimation.
Depression
Table 2 presents models of the association between pain and depression. Model 1 presents a random-effects model and shows that seniors with both moderate and severe levels of pain have significantly higher mean levels of depressive symptoms than seniors who do not report chronic pain. However, these models do not take all time-constant sources of spuriousness into account, and Model 2 achieves this through the use of a fixed-effects model. Both comparisons also remain significant in Model 2, but the comparison for moderate pain is reduced over 60% from Model 1, while the comparison for severe pain is reduced over 50%. These results therefore indicate that conventional analyses using standard observed controls tend to substantially overestimate the association between chronic pain and depression in older adults.
Chronic Pain and Depressive Symptoms Among Older Adults.
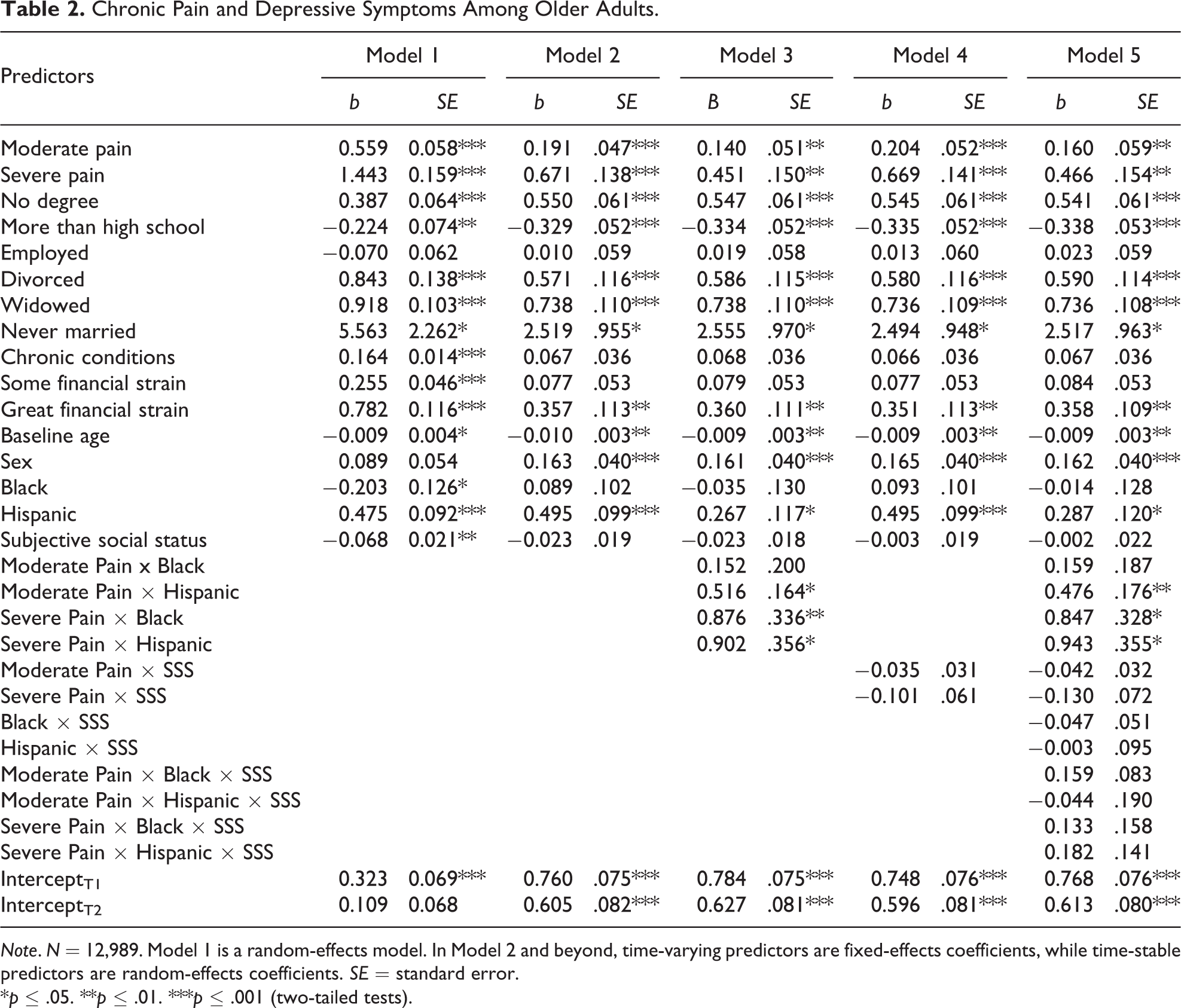
Note. N = 12,989. Model 1 is a random-effects model. In Model 2 and beyond, time-varying predictors are fixed-effects coefficients, while time-stable predictors are random-effects coefficients. SE = standard error.
*p ≤ .05. **p ≤ .01. ***p ≤ .001 (two-tailed tests).
Model 3 examines how the association between pain and depression varies by race and ethnicity by testing interactions between the indicators for Black and Hispanic with the pain indicators. For moderate levels of pain, the interaction with Hispanic is significant, while for severe pain interactions with both Black and Hispanic are significant. Figure 1 illustrates the meaning of these interactions by using Model 3 to depict the predicted mean level of depression at each level of pain for each racial–ethnic group. Figure 1 shows that racial and ethnic minorities with severe chronic pain experience a substantially greater level of depression than racial and ethnic minority seniors without pain; conversely, White elders with severe pain experience a much less dramatic difference when compared to White elders without pain. However, additional analyses did not support the role of SSS as a modifier of the pain–depression association: Interactions between the pain indicators and SSS (Model 4), as well as tests of whether these interactions differed by race and ethnicity (Model 5), were not significant.
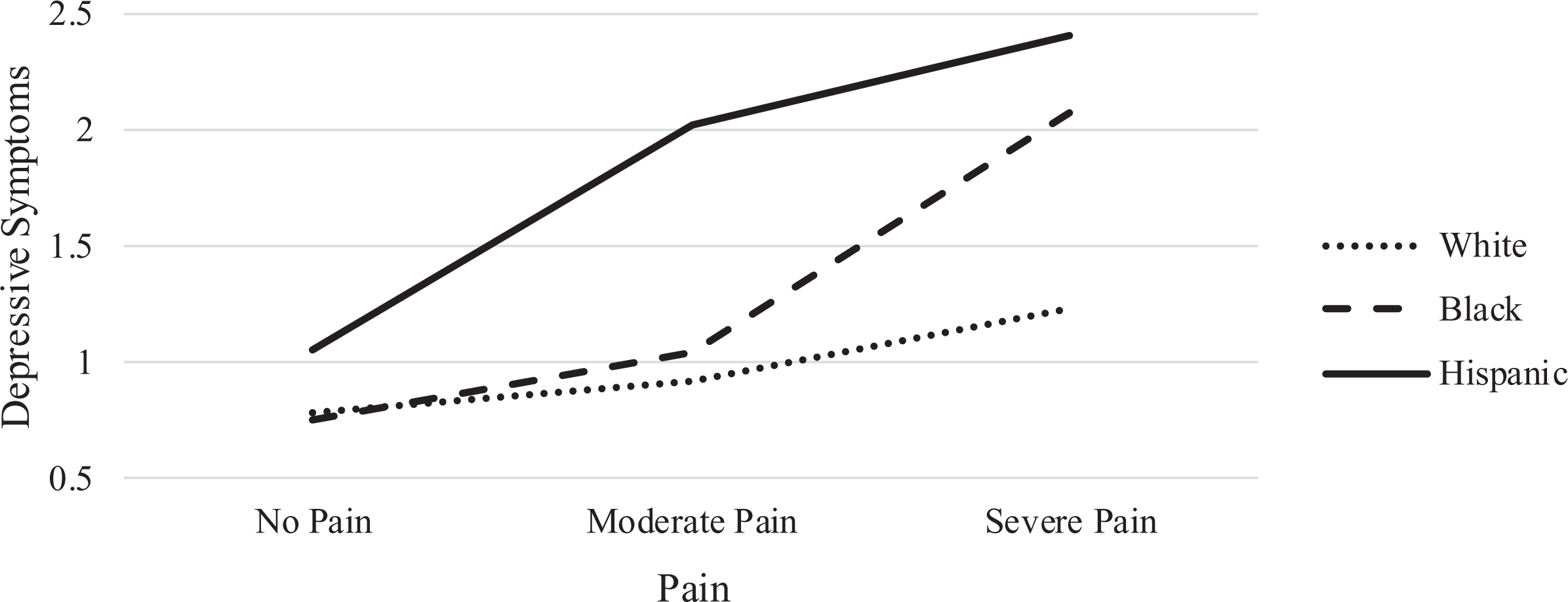
Pain and symptoms of depression.
Anxiety
Table 3 displays the analyses of anxiety. Model 1 shows that, with a standard set of time-stable and time-varying controls, individuals with both moderate and severe pain report significantly higher levels of anxiety than individuals who do not report chronic pain. Model 2 shows that, in a fixed-effects model, the comparison for severe pain is essentially reduced to nil and is no longer significant. Furthermore, the comparison for moderate pain is reduced almost 75% and, since the scale of the anxiety measure is 1–4, the practical significance of a difference in anxiety of 0.03 (b = 0.029, p < .05) is negligible. When all time-stable confounders are controlled, then, the association between pain and anxiety is largely obviated.
Chronic Pain and Anxiety Symptoms Among Older Adults.
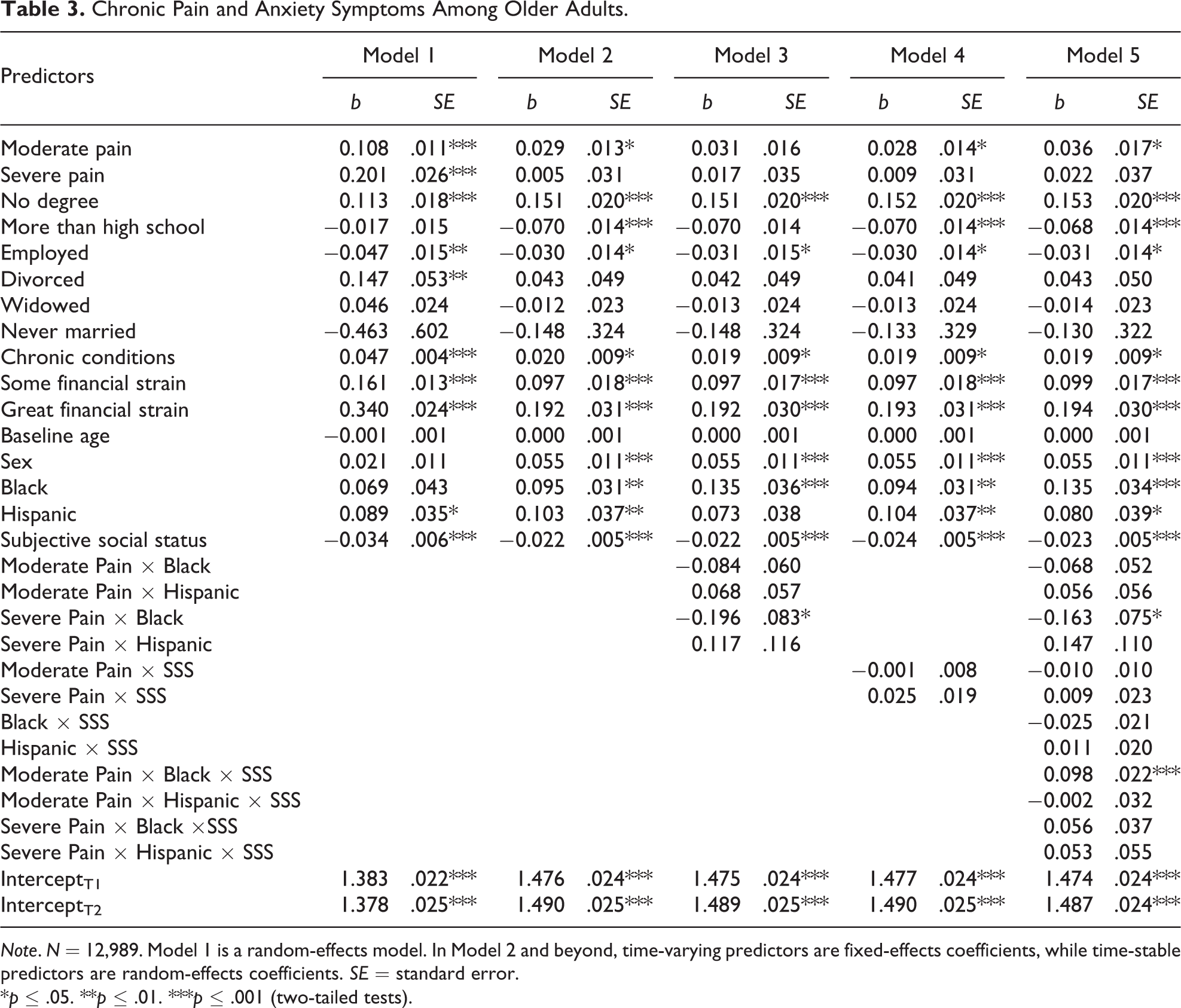
Note. N = 12,989. Model 1 is a random-effects model. In Model 2 and beyond, time-varying predictors are fixed-effects coefficients, while time-stable predictors are random-effects coefficients. SE = standard error.
*p ≤ .05. **p ≤ .01. ***p ≤ .001 (two-tailed tests).
Model 3 examines whether race and ethnicity modify the association between pain and anxiety, and only the interaction between the indicators for Black and severe pain is significant. Race-specific ancillary analyses indicated that, for White elders, severe pain was not associated with a significantly different level of anxiety (b = 0.005, p > .10), but Black seniors with severe pain reported significantly lower anxiety than Black seniors without pain (b = −0.169, p < .05).
In addition, although interactions between the pain indicators and SSS in Model 4 were not significant, Model 5 shows that a three-term interaction between the indicators of pain, racial–ethnic background, and SSS is significant for Black seniors with moderate levels of pain. Figure 2 illustrates the meaning of this interaction by using Model 5 to depict the association between pain and anxiety for Black and White seniors at high and low levels of SSS. For Black seniors at high levels of SSS, anxiety is significantly higher at moderate levels of pain. However, for Black seniors at low SSS, anxiety is lower when moderate pain occurs. In total, the analyses of anxiety show an unexpected pattern in which Black seniors with severe pain report lower anxiety, as do Black seniors who combine moderate pain with low levels of SSS, although anxiety is higher in Black seniors with moderate pain and high SSS. We describe potential reasons for these unexpected findings in the Discussion section.
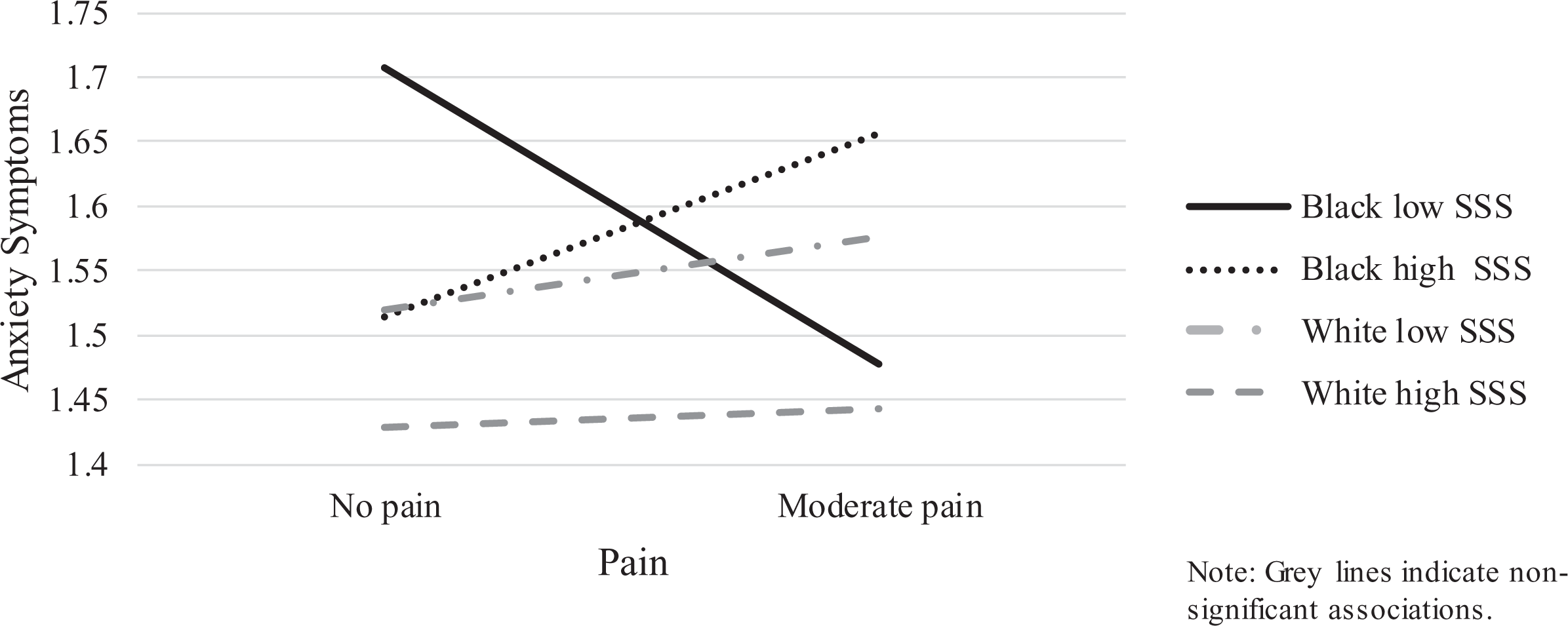
Moderate pain and symptoms of anxiety.
Discussion
The current research uses a nationally representative sample of older adults followed over 4 years to examine the association between chronic pain and symptoms of psychological distress. The analyses supported the first two hypotheses: Chronic pain was associated with measures of depression and anxiety when only standard controls were included in the models, but these associations were substantially reduced through the application of fixed-effects models, which eliminate all time-stable sources of confounding. Eliminating the influence of all time-stable confounders essentially ruled out the overall association with anxiety, although pain continued to be significantly associated with depressive symptomology.
This pattern of findings suggests that research on pain and mental health in older adults should look skeptically on studies which rely only on observed measures to rule out spuriousness. The association between pain and psychological distress may be especially disposed to confounding in older adults because there are a large number of life-course factors that can affect both pain and psychological distress, and it is difficult to sufficiently address the breadth of this array through observed measures alone. Furthermore, taking time-stable confounders into account also helps to address reverse causation by ruling out the influence of trait anxiety and trait depression on experiences of pain. It is likely that the fixed-effects models negated the overall association between pain and anxiety in part because this analytic approach eliminated the influence of trait anxiety on pain. Future research on pain and psychological well-being should therefore more commonly utilize methods of analyses that better control for unobserved confounding in this association, such as fixed-effects models, or risk confounding by reverse causation and a host of life-course influences. By the same token, that the association between pain and depression remains even when stable dispositions toward depression are taken into account lends greater confidence to the view that this is evidence of the consequences of pain for depression. That pain remains associated with depression is therefore in concordance with the “emerging consensus that persistent pain is more likely to lead to depression than vice versa” (Campbell, Clauw, & Keefe, 2003, p. 399).
We hypothesized that the association between pain and distress would be stronger for racial and ethnic minorities in late life in a process of “double-jeopardy.” We found partial confirmation of this hypothesis, as particularly severe pain was associated with greater risk of depressive symptoms more strongly among Black and Hispanic than White seniors. Severe chronic pain among Black and Hispanic seniors was associated with an average of over a symptom more of depression compared to racial and ethnic minorities without pain. Because a sum of four symptoms on the 8-item depression measure indicates clinical relevance (Steffick, 2000), this difference will not result in clinical depression in isolation of additional depressive factors. Yet, if racial and ethnic minorities in late life already experience elevated symptomology due to various stressors accrued throughout the life course, the addition of severe pain will likely serve as a crucial tipping point into clinical depression. Thus, one clear practical application of these results is that they suggest unmet needs among racial and ethnic minorities in regard to palliative pain management. These unmet needs may be due to the well-documented increased barriers to pain care that racial and ethnic minorities often face (Shavers et al., 2010). Addressing these structural deficiencies may therefore be a key way of reducing risks for depression experienced by racial and ethnic minority individuals in late life, especially since individuals are at greater risk for chronic pain as they age (Johannes et al., 2010).
The increased risk for depression that racial and ethnic minorities face due to severe chronic pain is particularly important in the context of larger questions of double-jeopardy in the aging process. The focus of studies examining the double-jeopardy hypothesis has largely been on whether the association between age and heath is more detrimental for racial and ethnic minorities, but this hypothesis has generally not been supported when psychological distress has been examined as an outcome. The results of the current research suggest that the question of double-jeopardy may not be whether age in and of itself is associated with mental health, but instead whether the stressors experienced as individuals age are differentially associated with mental health across race and ethnicity. A potentially fruitful area of future research on the double-jeopardy hypothesis is to shift to examining whether stressors that are prevalent when aging occurs are more likely to affect the mental health of racial and ethnic minorities.
Results were surprisingly contrary for anxiety, though. At severe levels of pain, levels of anxiety were lower for Black elders than when Black elders did not report chronic pain. The small inverse association may be due to the role of anxiety as an indicator of “agitation,” whereas symptoms of depression are much more passive, in terms of indicating lethargy and malaise (Mirowsky & Ross, 2003; Ross & Mirowsky, 2009). Because chronic pain is an enervating experience, undermanaged pain may leave Black seniors less liable to express active signs of distress.
Associations with anxiety were also found once we took differentiation by SSS into account. Although we predicted that SSS would weaken the association between chronic pain and psychological distress, we also proposed a diminishing returns hypothesis, which predicted that SSS would be less protective for racial and ethnic minorities than for White elders. These results did not support the general role of SSS in weakening the association between pain and psychological distress but did provide partial support for the diminishing returns hypothesis. SSS did not buffer the association between pain and depression for any group examined in this research and also did not differentiate the association between pain and anxiety for White and Hispanic elders. However, Black seniors at low levels of SSS experienced lower anxiety when moderate pain occurred, while Black seniors at high SSS experienced greater anxiety. The combination of disadvantage in both race and social status likely accentuates the risk of undertreatment, leading low SSS Black seniors to be especially subject to the draining effects of moderate pain. Conversely, higher levels of SSS may have provided some protection from the draining effects of pain for Black elders, particularly when pain was only at moderate levels, but at the same time moderate pain may have been a substantial threat because of the combination of risk it posed for progressing to serve pain, and the tendency of the medical establishment to undertreat pain in Black elders. Consequently, for Black elders at high SSS, moderate pain was an anxiety-inducing experience.
Care should also be taken to avoid overemphasizing associations with anxiety. The anxiety measure ranged from 1 to 4, with a standard deviation of approximately 0.60 at both waves. Conversely, absolute differences in anxiety for Black elders were less than 0.25 in all cases, indicating at best a small practical difference in anxiety even when statistically significant. This pattern of results therefore suggests that, once time-stable confounders are taken into account, older adults are more likely to respond to pain with depression than anxiety, most likely due to the enervating effects of pain. The differences in the extent to which pain was associated with depression and anxiety underscore the importance of examining how pain is associated with multiple mental health outcomes. Had we examined only depression, we might have extrapolated a broader set of mental health repercussions for pain than actually exists.
Overall, then, we do not see strong or consistent evidence to support the diminishing returns hypothesis because there was little protective effect of SSS to differentiate. Although previous research on SSS supports its association with health, the results of this research suggest that an important limiting factor for the benefits of SSS may be that more objective measures of social status are better for predicting differentiation in the effects of stress in late life. However, Lee and Bierman (2016) recently found that SSS buffered the effects of perceived discrimination in older adults. This pattern of findings suggests that SSS may buffer some stressors more than others among older adults, and additional research is needed to delineate the contours of these buffering properties.
An important weakness that should be noted in this research is that we have access only to self-rated measures of pain. Moreover, these measures of pain are quite general, in that they ask individuals only to rate the overall severity of their pain. Although these measures have been used among older adults in previous research (e.g., Covinsky et al., 2009; Reyes-Gibby et al., 2007), other research on older adults is more specific in terms of asking about pain experienced in specific sites of the body (e.g., Bierman, 2011). Additional research on older adults should therefore examine more detailed measures of pain, while including substantial samples of ethnic and racial minorities. This also touches on an additional weakness of this study, in that we examined ethnic and racial minorities only in terms of Hispanic and Black elders. Sample sizes precluded the study of additional minority groups, but attention to additional groups such as Asian and Middle Eastern seniors is especially important for furthering understanding of the consequences of pain in late life. In addition, the measure of anxiety dealt with general symptoms of anxiety but did not address worries or concerns in regard to specific areas of life. For example, if older adults are still employed, pain may threaten potential earnings or financial security, particularly if older adults work in physically demanding occupations or if pain restricts physical movement. This in turn may create financial anxieties that are not reflected by the general measure of anxiety. Examining domain-specific worries, and the mechanisms through which pain may affect these domains, is also an important area for future research.
Conclusion
This research indicates that the association between chronic pain and psychological distress is likely to be substantially overestimated in analyses that depend only on observed controls, especially for the association between chronic pain and anxiety. Further, in a demonstration of double-jeopardy, racial and ethnic minorities appear to be especially subject to increases in depression associated with severe pain. This research therefore suggests that ethnic and racial minorities continue to experience unmet needs in regard to pain management, and the result is a substantial degradation in quality of life, as indicated by greater depressive symptomology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.