
Abstract
The Healthy Brain Initiative: National Public Health Road Map to Maintaining Cognitive Health (2007) called on the research community to disseminate its work on cognitive aging and cognitive health. The purpose of this scoping review was to (1) identify terminology that cognitive, social, and behavioral scientists use to describe cognitive aging and cognitive health, in association with dementia and Alzheimer’s disease, among older adults; (2) demonstrate how such terms are defined; and (3) illustrate how these constructs are measured in research settings. Empirical studies published 2007–2018 were examined for terminology, definitions, disciplinary orientation, and measurement mechanisms. Analysis of the corpus and a detailed review of the terms “cognitive impairment” and “mild cognitive impairment” reveal that formal definitions are provided infrequently and measurement of constructs ranges widely. Overall, the variability in terminology, definitions, and measures reflects a need for greater specificity in research communication, such that cross-disciplinary collaboration can be facilitated.
Two important calls for enhancing communication about cognitive aging and cognitive health have been issued in recent years. In 2007, The Healthy Brain Initiative: National Public Health Road Map to Maintaining Cognitive Health (The Road Map, 2007) was issued jointly by the Centers for Disease Control and Prevention (CDC) and the Alzheimer’s Association and called on researchers to disseminate critical findings about cognitive health. More recently, the Institute of Medicine (IOM, 2015) issued its report, Cognitive Aging: Progress in Understanding and Opportunities for Action, and included recommendations for improving communication on the concept of cognitive health, especially with respect to the public. To fulfill the mandates of these efforts, research on cognitive aging is being shared across disciplines, put into clinical practice, and used in public health messaging. However, this widespread dissemination has increased the opportunity for ambiguity and misinterpretation of terminology.
Disciplinary assumptions, whether epistemological, ethical, ideological, theoretical, or methodological, exist and influence terminology used to describe phenomena of study (Szostak, 2014). When terms are employed across disciplinary boundaries or translated into clinical practice, confusion, misunderstanding, and misinterpretation can occur (Koskan et al., 2010). Often, terminology does not translate easily. In cross-disciplinary contexts, researchers from various disciplines may attach different meaning to the same terms due to the inherent ambiguity in language. Though such ambiguity can be a positive force by stimulating curiosity and leading to new research directions, it can also be negative, masking logical or theoretical inconsistencies (Griffiths & Stotz, 2014; Szostak, 2011). Scholarly attention to the use of terminology in the study of cognitive science is limited, despite its relevance to interdisciplinary research efforts on cognitive aging and cognitive health.
In an effort to highlight ways in which further clarification of terminology might be relevant to research dissemination efforts, this review aims to (1) identify the shared terminology found in medical, nursing, and social science research literature to describe cognitive aging and cognitive health specifically in conjunction with dementia and Alzheimer’s disease among older adults; (2) demonstrate how such terms may be defined; and (3) illustrate the range of construct measurement practices being employed in research settings. We conclude with a practical call to provide evidence to support the adoption of common data elements and to develop interdisciplinary consensus around application of terms both clinically and in research, along with recommendations for future research.
Background
Prior to 2007, the burden of cognitive decline, in terms of care-related costs and health disparities, was rapidly rising, despite growing scientific evidence that healthy behaviors may reduce risk and the rate of decline. In response, CDC (2007) and the Alzheimer’s Association released The Road Map, the first nationally coordinated effort to promote cognitive health as a public health issue. Recommendations contained in The Road Map placed emphasis on research dissemination, translation into clinical practice, and policy implementation, among other factors. It set the goal of developing strategies to increase cognitive health awareness among providers, public health professionals, and service providers. While it did not provide a formal definition for the term “cognitive health,” The Road Map called for standardized mechanisms for the measurement of neurological and behavioral health.
The National Alzheimer’s Project Act (2011) prompted the development of a federal coordination strategy to address the burden of Alzheimer’s disease and other dementias. The National Plan to Address Alzheimer’s Disease (U.S. Department of Health and Human Services, 2012), first published in 2012 and updated annually through 2017, focused on prevention and research but also on building public awareness and monitoring progress to drive improvement, prioritizing the role of communication as key for success, especially to enhance awareness of cognitive aging to health care practitioners, public health professionals, service providers, and the public. Little attention has been given, however, to the ways in which concepts of cognitive health are communicated among researchers, despite the inherent interdisciplinary nature of this work.
Interdisciplinary Communication
Interdisciplinary approaches are growing more common as a heuristic mechanism for scientific progress (Porter & Rafols, 2009). Interdisciplinary research promotes innovation by developing new lines of questioning and expanding problem definitions (Frost & Jean, 2003). Linking fields of study enables researchers to more fully address critical questions (Aboelela et al., 2007) and builds common knowledge and methodologies to solve complex problems (Newhouse & Spring, 2010). However, communication beyond individual disciplines is complicated, as each relies on methodologies and terminology used within its boundaries (Frost & Jean, 2003). Although scholars tend to agree that there is no formal definition of “interdisciplinary communication,” it is a practice aimed at achieving some kind of reciprocal comprehension, or shared knowledge, among researchers from different disciplines (Holbrook, 2013).
Researchers use dialects that are specialized to their discipline (Wear, 1999). This creates translational difficulty between natural science fields, between natural and social science fields, and between qualitative and quantitative social and behavioral scientists (Bruce et al., 2004). Different disciplines can use the same word to mean different things (Szostak, 2014), and words that are used in everyday discourse by nonexperts, particularly contributes to misunderstanding (Bracken & Oughton, 2006). An example of this may be found in terms such as “memory” and “recall,” which may seem to suggest equivalent concepts. The former often refers to a passive ability to retain information and the latter often refers to an active ability to retrieve information, yet these terms are frequently used interchangeably. Translation of terminology into clinical practice presents additional opportunities for misinterpretation. Groups of differing socioeconomic status or geographic proximity attach meaning to convey concepts commonly encountered by the group (Hebert et al., 2009), and these meanings may differ or conflict with meaning attached by other groups and/or researchers.
In health care, members of various disciplines may use the same words; however, subtle conceptual interpretations can lead to misunderstanding (Bonis, 2013). As an ideal, terminology enables a common understanding of concepts. In practice, however, this ideal often fails because (a) in a scientific context, not every term is defined and assumptions are made about existing knowledge or (b) terms, even when clearly defined, pick up connotations in usage that “gradually separate its fine-grained meaning into potentially incompatible submeanings” (Wray, 2017, p. 82).
Further complications to achieving a common understanding arise in cross-language and/or cross-cultural research settings. Cross-translations of research instruments and research reports may not adequately capture subtle nuance and cultural connotation with precise equivalency across languages (Shklarov, 2007). Moreover, cultural contexts shape the semantic meaning of terminology (Goddard, 2014), even among a shared, common language. For example, although English is common to both the United States and England, the equivalency of patient-supplied terms and responses can vary between these contexts; differing health care systems, private and socialized, may influence the readiness of patients to admit to health problems, patient satisfaction, or compliance with medical regimens (Hunt & Bhopal, 2004). Thus, comparability of data sets across languages and cultures is not always achievable, as concepts around health often are influenced by disparate expectations and cultural values (Hunt & Bhopal, 2004).
Terminology related to cognitive aging, specifically, presents challenges to interdisciplinary work, as the presentation of symptoms related to cognitive aging is highly variable. For example, the terms “dementia” and “mild cognitive impairment” (MCI) are often used to represent a syndrome of maladaptive behaviors related to cognitive health, which vary both in the type of behavior (e.g., memory loss, sleep disturbance) and in the behaviors that occur together. Clinical practitioners may use a variety of measures in practice to render diagnosis of these conditions, as such variety helps to illuminate and differentiate gradation and progression. In scientific research settings, however, such variability is far less desirable, as its presence diminishes the ability to reproduce and compare findings. Inconsistent definitions and measurement mechanisms can limit the interpretability of research results and impede the potential for interdisciplinary research progression.
Given the emphasis placed on communication in both The Road Map (2007) and the IOM (2015) Report, identification of basic concepts, terminology, and measurement practices related to cognitive aging may serve to overcome potential cross-disciplinary communication challenges and foster greater research collaboration. To assist in this process, we examined the terminology used by researchers in reporting their work on cognitive aging and cognitive health that specifically related to dementia and Alzheimer’s disease. We address the questions, “What are the basic concepts relied on by cognitive, social, and behavioral scientists to describe cognitive aging and cognitive health in their work on dementia and Alzheimer’s among older adults?” “How are such terms being defined, if at all?” and “How are these constructs being measured?” By demonstrating how such terms are defined by researchers and by illustrating the range of construct measurement practices being employed in research settings, we aim to highlight potential research terminology that might benefit by greater definitional clarity and thereby enhance the potential for its use in interdisciplinary research settings.
Method
Scoping reviews enhance conceptual clarity about a specific topic or field of evidence (Davis et al., 2009). They differ from systematic reviews in their emphasis on mapping a field of study and do not evaluate the quality of the underlying literature (Levac et al., 2010); yet by utilizing the techniques of systematic reviews, scoping reviews offer rigorous and transparent methods to identify and analyze relevant literature pertaining to a research question (Pham et al., 2014). This review examines peer-reviewed literature published between January 2007 and July 2018 to scope research nomenclature relating to cognitive aging and cognitive health and specifically concerning dementia and Alzheimer’s disease among older adults. This selected period coincides with the publication of The Road Map (2007), which called for greater critical research dissemination on cognitive health.
Conceptual Criteria
Search terms and targeted databases were determined by consensus and developed with the assistance of a health sciences librarian. The research team consisted of experts in nursing, social work, communication, psychology, gerontology, and public health. Embase, CINAHL, PsycINFO, and MEDLINE were searched using the parameters summarized in Online Appendix 1 to search title, abstract, subject terms, and key words. In addition to terms related to cognitive aging and health, supplementary terms related to public health were included to maintain a focus on research aligned with disease prevention and early diagnosis, consistent with The Road Map’s aim of promoting cognitive health as a public health issue. This concentrated the data set on studies that focused on the health of populations, outside of clinical settings, to capture the broad range of ways in which dementia occurs in the community.
Inclusion/Exclusion Screening
After reviewing for duplicates, 3,714 articles were selected for further screening of abstract and title information to ensure that articles met inclusion and exclusion criteria. To be included in the database, articles covered primary research, included terminology used by researchers and others related to dementia, Alzheimer’s disease, cognitive aging, and cognitive health, and were published between January 2007 and July 2018. Reasons for exclusion included, for example, case studies, study protocols, and pharmaceutical studies. Studies performed outside of the United States were excluded in an effort to enhance the conceptual clarity of terminology being used in the research and to eliminate challenges associated with cross-language and cross-cultural contexts (Hunt & Bhopal, 2004). In an effort to maintain a focus on public health research, studies on basic science (e.g., biological studies) were excluded, along with studies that did not align with the focus of this review, such as cost of care studies and study proposals and study protocols. An illustration of the screening processes is provided in Figure 1, and the full list of inclusion/exclusion criteria is detailed in Table 1.
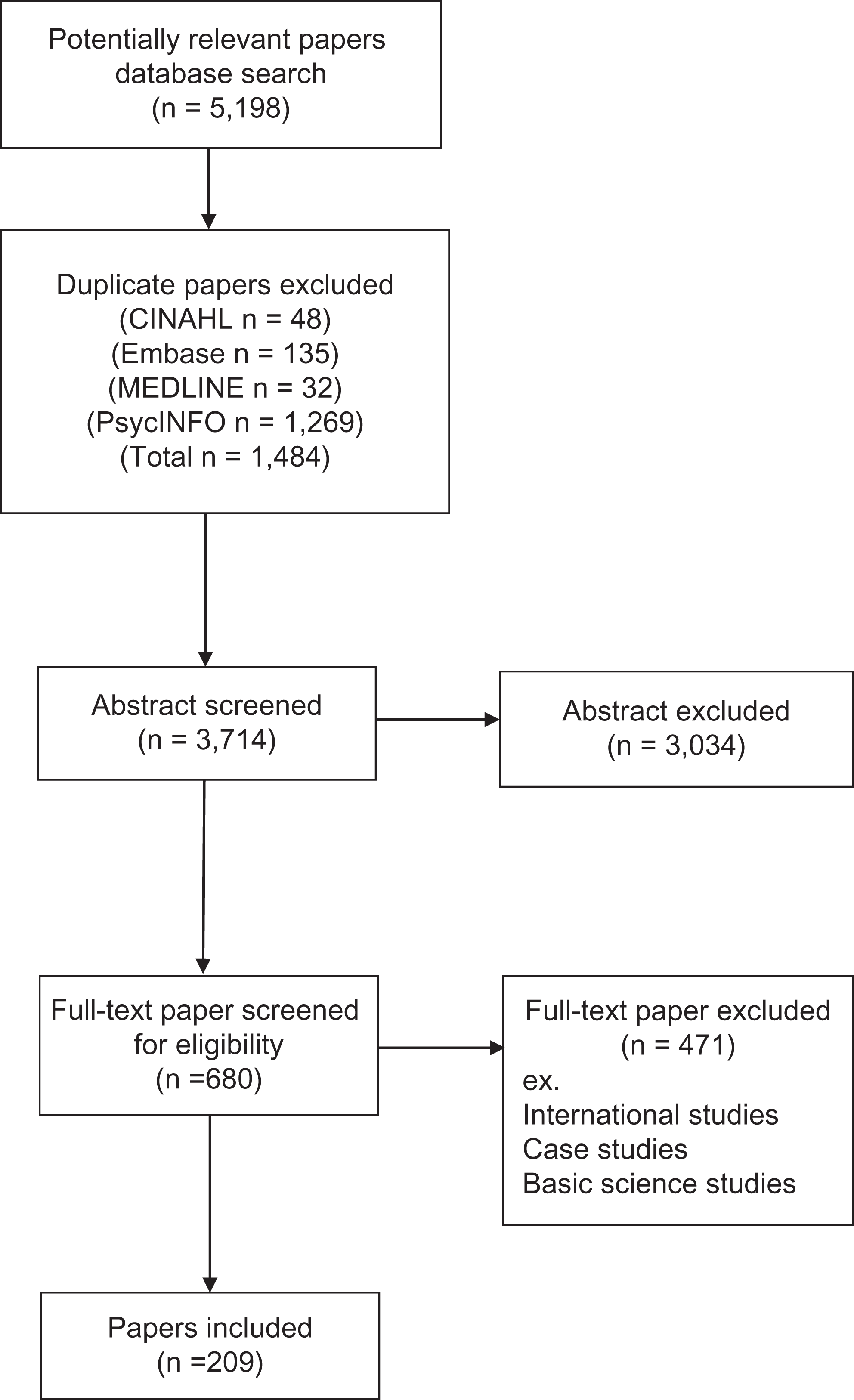
Screening process flowchart.
Inclusion and Exclusion Criteria.
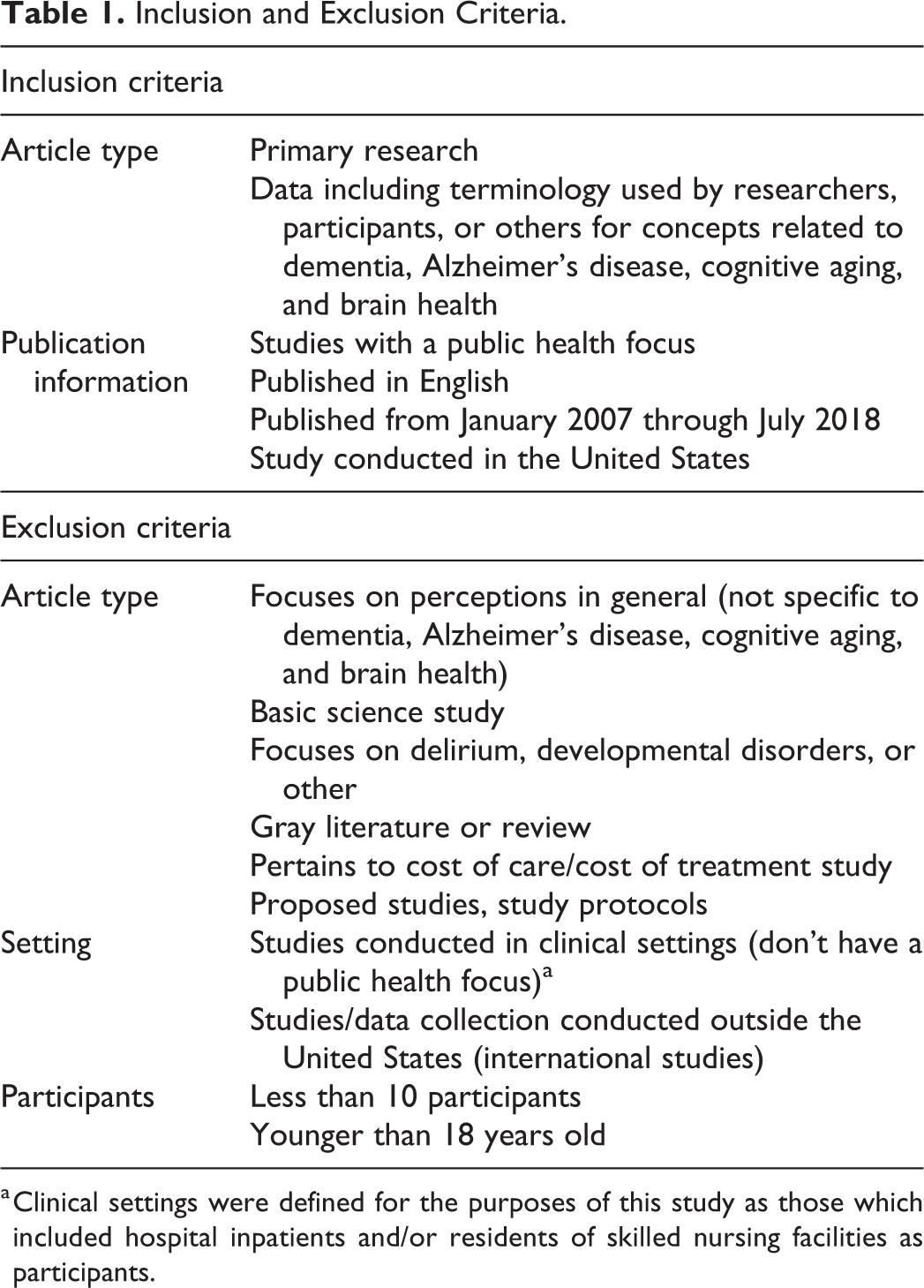
a Clinical settings were defined for the purposes of this study as those which included hospital inpatients and/or residents of skilled nursing facilities as participants.
Screening was conducted using the Covidence platform (www.covidence.org), a web-based tool developed for systematic reviews that enable a blind, random assignment of articles to the reviewer team. To ensure accuracy and consistency among reviewers, every article was screened by at least two team members, and all reviewers formally revisited inclusion/exclusion criteria after screening approximately every 50 articles. Two designated team members resolved conflicts in the screening process. In all, 3,034 studies were excluded in the abstract/title screening phase, leaving 680 articles available for data extraction.
Data Charting
Once the initial screening process was completed, each article was obtained and distributed to team member dyads, or pairs of research team members, for data charting. Data were collected and managed using REDCap electronic data capture tools (Harris et al., 2009). Each dyad reviewed the full text of between 50 and 120 articles, with each member of the dyad charting information independently. Members of each dyad reconciled the charted data with one another after completing approximately 25–50 articles, with reconciliation events varying between one and four per dyad in total. Another 471 articles were excluded in this phase: 341 reported on international study populations, 33 reported on basic science (animal studies, neuroimaging, etc.), 21 articles were considered gray literature, 26 articles related to instrument testing, 14 articles were letters to the editor or opinion essays, and 36 articles were excluded for miscellaneous reasons (e.g., case studies, cost of care studies, focus on delirium; one unobtainable article and one duplicate). The following information was charted from the remaining 209 articles (see Online Appendix 3 for a complete listing): study type; study purpose; descriptive sample data; specific use of the terms dementia, cognitive impairment, mild cognitive impairment, cognitive decline, and cognitive change; definitions for specified terms, applicable citations for specified terms, and measurement of specified terms; other relevant terms related to cognitive health and/or cognitive aging, along with definitions, citations, and measurement processes; measurement instruments used in the study; and any other relevant conclusions, citations, and research recommendations related to terminology.
As a final step, the disciplinary orientation for each of the remaining 209 articles was assigned by examining the National Library of Medicine catalog entry for the Broad Subject Terms assigned to the publishing journal of each article.
Results
The following analysis provides descriptive information about the 209 articles in the data set. We then offer a more detailed analysis of two specific terms, “cognitive impairment” and “mild cognitive impairment,” as these were commonly employed throughout the literature. Descriptive information on the data set is summarized in Table 2.
Descriptive Summary of Data Set.
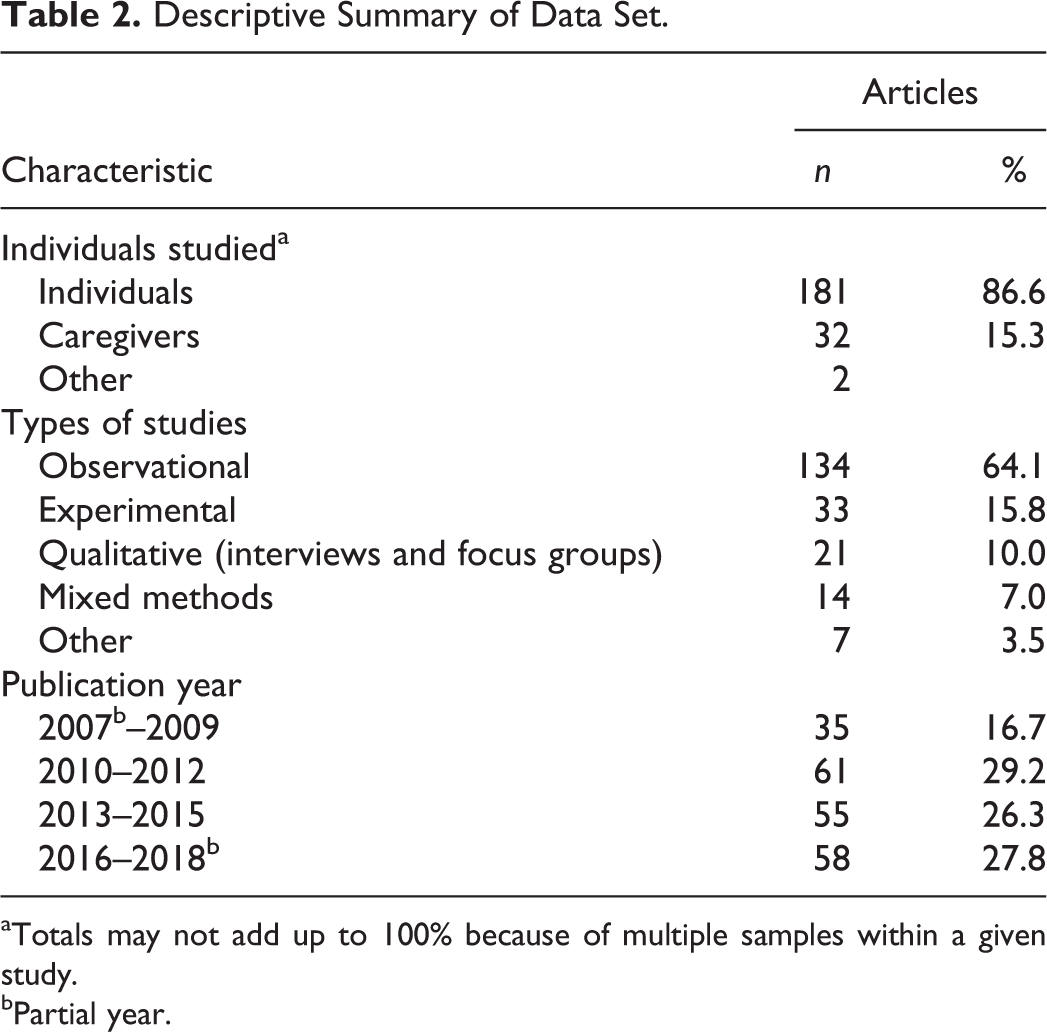
aTotals may not add up to 100% because of multiple samples within a given study.
bPartial year.
We first note the significant acceleration in published literature regarding cognitive health over the period of review. Ten articles were included in the data set for 2007 (a partial year) and 13 articles for 2008. By comparison, 25 articles were published in 2017 (the latest complete year), with another 17 articles published in the first 7 months of 2018. This significant rise in published literature demonstrates the increased attention to this field, likely in response to the calls of The Road Map and the IOM report.
Types of Studies
The majority of studies in the data set were observational in nature (n = 134, 64.1%) and included longitudinal studies on neuropsychological measures and cognitive performance, and studies of the predictive power of performance on these types of measures (e.g., tests of executive function, visuospatial tests) and cognitive condition. A number of studies examined the relationship between physical behaviors and characteristics (e.g., sleep patterns, physical activity levels, body mass index, lower extremity function), psychological factors (e.g., apathy, pain reports, agitation, anxiety), or other health conditions (e.g., kidney or cardiovascular disease, anemia, presence of dental care) and cognitive health. The role of caregiving for persons with cognitive impairment also received attention, with several observational studies examining caregiver burden and the role of patient behaviors, the prevalence of anticipatory grief, and the reliability of caregiver reports on patients’ cognitive state.
Experimental research (n = 33, 15.8%) included studies on the efficacy of a variety of psychosocial interventions such as interaction strategies, hypnosis, and support groups on memory and recall. Some studies also examined interventions aimed at preserving cognitive function such as caregiver-supported in-home cognitive and mindfulness training. A third line of research encompassed the role of physical activity to cognitive health, comparing groups with and without structured physical activity programs.
The prevalence of qualitative protocols (n = 21, 10.0%) was much more limited and centered on the ways in which narratives arise around cognitive decline and Alzheimer’s disease, how partners navigate intimate relationships in the face of cognitive loss and the experiences of caregivers and their quality of life. A few qualitative studies examined the ways in which diagnoses are obtained from both the perspectives of the caregiver and primary care provider. Mixed methods research (n = 14, 7.0%) examined differences in mechanisms for reporting health information, the characteristics of caregivers, and cultural differences in common beliefs about memory loss and Alzheimer’s disease.
Sample Data
The majority of articles (n = 181, 86.6%) centered on older community-dwelling adults as the subject of study. About 15.3% (n = 32) of the articles concerned caregivers including family members, spouses, and clinicians. Two studies examined document content such as death certificates and advertisements. Somewhat surprisingly, over 12% (n = 25) of the studies did not report age and/or gender information about the study sample and 35.4% (n = 74) failed to report race and/or ethnicity information. Only 12 studies (6.0%) reported information about the duration or onset of cognitive decline and/or impairment.
Disciplinary Representation
Disciplinary analysis was conducted on the data set by examining “broad subject terms” listed in the National Library of Medicine catalog record for each article’s publication. In all, the data set represented research in 31 disciplines as noted in Table 3. Many journal titles are cross-disciplinary in nature: Two disciplines were listed for about half of the articles in the data set (n = 101), one discipline was listed for 74 articles, three disciplines were listed for 15 articles, and 11 articles had no disciplinary information listed. Despite the interdisciplinarity of the underlying research, the majority of the articles in the data set were published in journals circulated among geriatrics (n = 95), neurology (n = 81), psychiatry (n = 65), and to a lesser degree, psychology (n = 30). Other disciplines that might be expected to contribute, such as nursing and public health (n = 6 and n = 4, respectively), had substantially lower levels of research reporting on the topics. Fewer than six articles were represented by any other field. The majority of the articles appeared in journals devoted to geriatrics, neurology, and psychiatry are perhaps unsurprising. More notable is the absence of work in other relevant areas such as social work and sociology.
Disciplinary Representation.
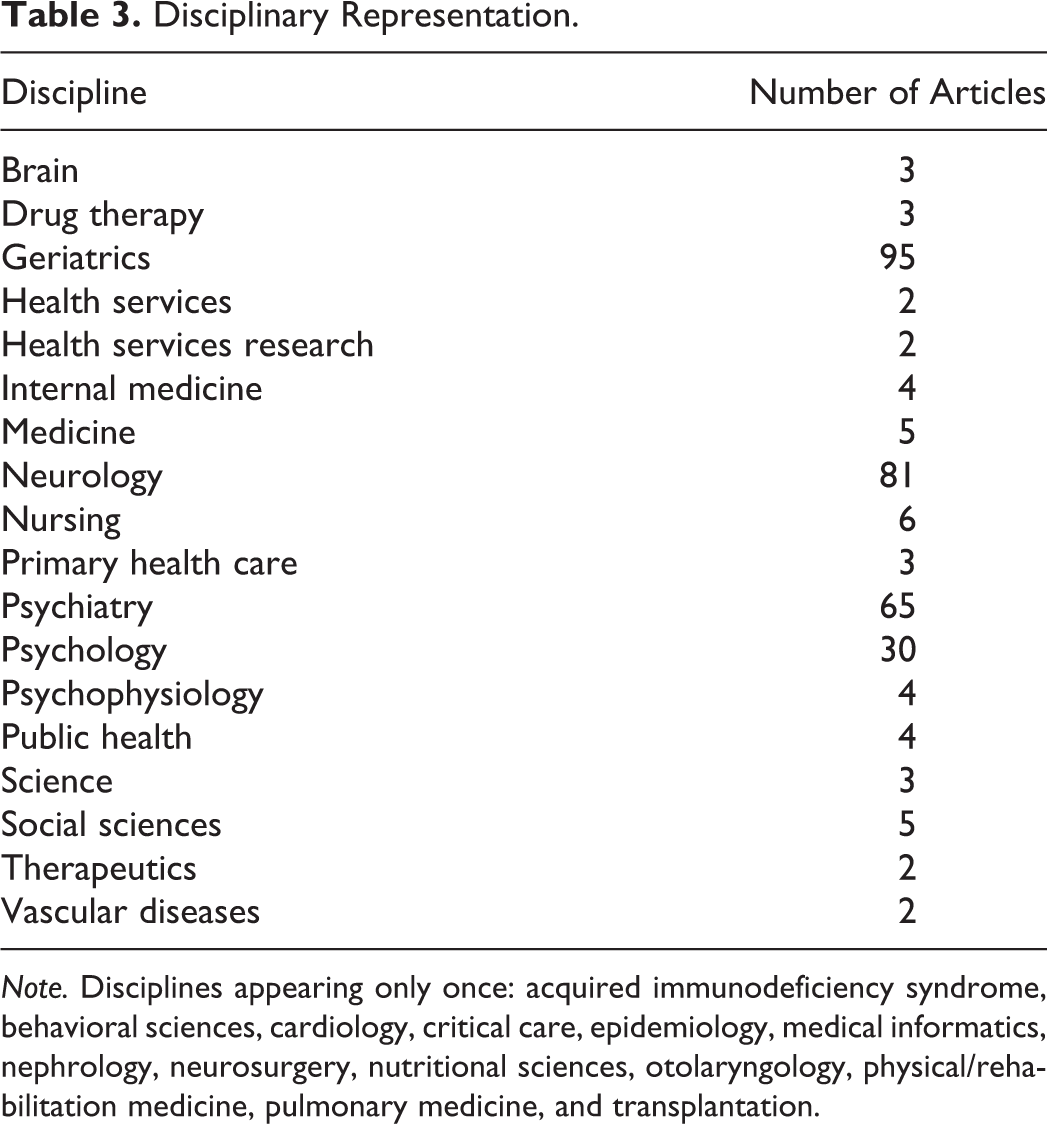
Note. Disciplines appearing only once: acquired immunodeficiency syndrome, behavioral sciences, cardiology, critical care, epidemiology, medical informatics, nephrology, neurosurgery, nutritional sciences, otolaryngology, physical/rehabilitation medicine, pulmonary medicine, and transplantation.
Measurement Tools
By far, the most frequently used measurement tool for assessing cognitive status was the Mini-Mental State Examination (MMSE; Folstein et al., 1975). In its various forms (modified, revised, the Consortium to Establish a Registry for Alzheimer’s Disease adaptation), the MMSE was used in n = 120 (57.4%) of the 209 studies in the data set. Other tools used to assess cognitive function included the Clinical Dementia Rating (CDR) Scale and its variants (n = 35, 16.7%) and a variety of phone or practitioner assessments. Tests of executive function included the trail making test (n = 39, 18.7%), the digit span forward and backward test (n = 26, 12.4%), and a variety of the Wechsler Adult Intelligence Scale subtests (n = 22, 10.5%).
Terminology
A variety of terminology was used to describe cognitive health and cognitive aging, though most of the terms extracted from the articles reflected cognitive deficiency. The full list of terms is cataloged in Online Appendix 2 and includes 1,160 references to cognitive function and cognitive health. For analysis purposes, the terms were loosely grouped by topic; these centered on terms describing Alzheimer’s disease and related disorders, dementia, cognitive impairment, MCI, cognitive change and decline, cognition and cognitive function, memory, executive function, and cognitive aging. There were few references to cognitive health or cognitive improvement.
Within each of these categories, terms that described related concepts were grouped. For example, the group surrounding “memory” also included phrases such as “memory complaint,” “memory loss,” and “subjective memory impairment.” Frequently, definitions of such terms were not included in the research report. For example, of the 158 (75.6% of the data set) articles that mentioned dementia, only 12 (8.0% of the dementia articles) articles defined the term. Measurement of constructs, similarly, was poorly outlined and, if a measurement mechanism was offered, varied widely among articles. Again, using the term dementia as an example, measurement was described in a scant 33 articles (20.9% of the dementia articles) and varied widely between use of the MMSE, the National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association criteria, a participant’s “prior diagnosis of dementia,” the CDR, or by a participant’s “subjective memory complaint in the absence of functional impairment” (Koppel et al., 2012).
To offer a more nuanced perspective on this wide-ranging nomenclature and the ways in which terms are defined and measured, the terms cognitive impairment and mild cognitive impairment are offered as detailed examples, as these were two frequently used terms.
Cognitive impairment
The term cognitive impairment was used in a majority (n = 132, 63.2%) of the articles. However, out of these, only one article defined the term as, “a spectrum of conditions ranging from MCI to full dementia” (Gurgel et al., 2014). Frequently, researchers used measurement instrument scale readings to define cognitive impairment within their studies, but these more quantitatively oriented definitions varied widely in both the instruments that were used and the cut points were employed to determine an impaired cognitive status.
The measurement tools used as proxies for definitions of cognitive impairment included more widely employed instruments such as the MMSE, Montreal Cognitive Assessment, the Blessed Orientation Memory and Concentration (BOMC) Test (Katzman et al., 1983), the CDR, and Cumulative Illness Rating Scale for Geriatrics (Miller et al., 1992), and researcher-improvised mechanisms. These improvised mechanisms ranged widely. Researchers used interviews (Rovner et al., 2012), devised their own batteries of neuropsychological measures such as language, executive function, praxis, and reading ability to assess participant’s cognitive impairment (e.g., K. H. Lee et al., 2015), or considered participants cognitively impaired when they “failed” a screening test (Bailey & Arab, 2012). One study used performance difficulty on items such as tracking current events, paying attention, and remembering people and addresses (Bass et al., 2012) to determine cognitive impairment. Researcher-improvised assessments, while likely providing valid indication of impairment, may be unhelpful for cross-disciplinary use, as the outcomes of study may necessarily be tied to levels of impairment that cannot be reliably assessed in other settings.
Some studies attempted to employ more universal mechanisms, such as by defining cognitive impairment as falling at least 1.5 standard deviations (SDs) below available age-corrected normative data in a standard neuropsychological test battery (Eggermont et al., 2010). Yet these too can make comparison more challenging because of varying assessment mechanisms, despite such comparison’s importance to cross-disciplinary work.
Even when more conventional tools were used, relevant cut points to demonstrate cognitive impairment deviated broadly between studies. For example, as shown in Table 4, the MMSE was frequently employed as an instrument to measure cognitive function, but scores to designate cognitive impairment ranged widely. One study defined cognitive impairment as participant scores of between 20 and 30 (Beard et al., 2012), while other studies considered participants to have significant cognitive impairment with MMSE scores of less than or equal to 23 (Clarke et al., 2010) or less than 19 (Morrow et al., 2009). Other, widely available tools, such as the CDR and the BOMC, evidenced similar discrepancies.
Assessment Tools Used to Define Terms.
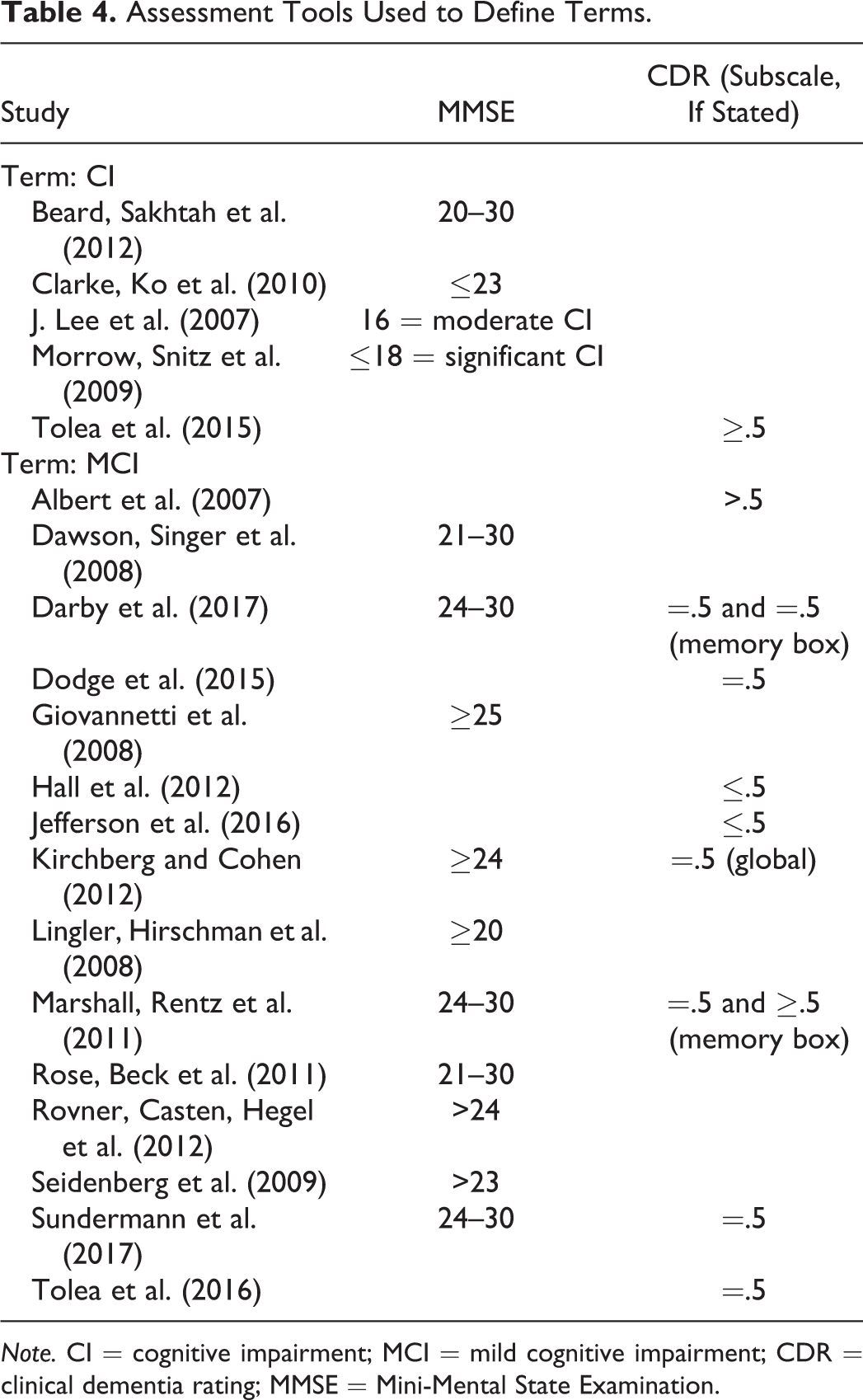
Note. CI = cognitive impairment; MCI = mild cognitive impairment; CDR = clinical dementia rating; MMSE = Mini-Mental State Examination.
MCI
A total of 131 articles (62.7%) used the term, mild cognitive impairment. Definitions for this term were more prevalent in these articles than in those that used the term cognitive impairment, but still meager, with only 33 articles (25.1%) providing any kind of definition. Similar to cognitive impairment, there was a wide variety in definitions provided. MCI is well-established as a precursor to dementia (Petersen, 2004) and is seen as a clinical syndrome that may intercede in the neuropathological progression between normal aging and Alzheimer’s disease (Pertersen et al., 1999).
Citation analyses of terms revealed many (n = 15, 45.5%) of these definitions were based on Petersen and colleagues’ (1999, 2001, 2004, 2009) work, which evolved from the work of Braak and Braak (1991, 1995). Other definitions included MCI as “an initial state of [Alzheimer’s disease] or prodromal [Alzheimer’s disease]” (Tappen & Hain, 2014) and “a transition state between normal aging and dementia and predicts progression to dementia, particularly [Alzheimer’s disease]” (e.g., Lingler et al., 2016), or a disorder often thought to be a transitional phase between cognitive health and Alzheimer’s disease (e.g., Kirchberg et al., 2012). People with MCI have subjective concerns about cognition and perform poorly on cognitive tests (Winblad et al., 2004) and/or experience impaired test performance (Plassman et al., 2011). Mild difficulties in complex everyday tasks can commonly be seen among people with MCI (Giovannetti et al., 2008); however, they are able to perform and preserve their normal activities of daily living skills and, therefore, do not meet the criteria for dementia disorders (Petersen et al., 2001).
Measurement of MCI, like that of cognitive impairment, varied among a number of instruments, both single and in combination. The MMSE was the most frequently used instrument (n = 14, 16.0%) and was often used in tandem with the CDR (e.g., Kirchberg et al., 2012) or Dementia Rating Scale–2 (Jurica et al., 2001; e.g., Seidenberg et al., 2009; Tremont & Alosco, 2011). While the CDR was used as a stand-alone assessment in some studies (e.g., Albert et al., 2007), others used a standard battery of neuropsychological tests, such as tests of memory and executive function (Hall et al., 2012), or the presence of subjective memory complaint (Koppel et al., 2012).
Cut points to define MCI again varied widely and are shown in Table 4. For example, two studies defined participants with MCI as having MMSE scores between 21 and 30 (Dawson et al., 2008; Rose et al., 2011), while others used cut points of a score of 20 or higher (Lingler et al., 2008), 24 or higher (Kirchberg et al., 2012), and 25 and higher (Giovannetti et al., 2008). In some cases, the MMSE was used to assign gradations of cognitive impairment such as for making distinctions between MCI and moderate or severe cognitive impairment (Rose et al., 2011). When using the CDR, researchers were similarly inconsistent in their determinations: Some used a defining score of 0–0.5 (Hall et al., 2012) and others a score of greater than 0.5 (Albert et al., 2007). Comparison to normed data was also employed, consistent with the Petersen definitions, using 1.5 SD units below that of individuals with comparative age and education (e.g., Kirchberg et al., 2012).
Discussion
Multiple specific clinical diagnoses fall under the umbrella of dementia, but all clinical representations indicate maladaptive behaviors and deficits in cognition. A challenge of dementia and cognitive decline is the insidious nature of its onset. Its early stages are where researchers and clinicians frequently grapple to define terminology and employ measurement tools to capture the variability of symptoms present in patients. Under such circumstances, it is understandable that variation in expression arises. Terminology changes over time as well, perhaps in response to more nuanced grappling. Yet the deliberate development of common vocabulary and corresponding operationalization is essential to interdisciplinary research efforts, and even efforts within disciplines, to solve the complex problems presented by dementia and cognitive decline.
Our review of terminology used to describe cognitive aging and cognitive health among older adults (see Online Appendix 2) demonstrates wide variation in what is employed in a research reporting context. To date, studies which examine these discrepancies have been limited, despite the importance of language to advancing interdisciplinary research efforts. Research on dementia and MCI is extensive and ongoing, and yet many studies offer limited opportunity for comparability or interpretation in the collective because of the ways in which terminology and measurement tools are utilized. This review highlights some ways in which further clarification of language might be relevant to enhancing research endeavors.
Six terms stand out as most frequently used: dementia (n = 158), cognitive impairment (n = 132), mild cognitive impairment (n = 131), Alzheimer’s disease (n = 57), cognitive decline (n = 55), and cognitive deficit(s) (n = 55). The prominence of these terms signals not only their significance to research efforts but also that a shared, common understanding of these terms is imperative. Other scoping reviews research indicate similar findings and recommendations. Friedman and colleagues (2015) examined risk and protective factors for Alzheimer’s disease and related disorders and found several definitions; however, there was a lack of common definitions, measures, and instruments across studies. Given that work in this area is so vast in nature, it is recommended that a next step could be establishing an interdisciplinary task force of investigators in key areas, where this work is being published (geriatrics, neurology, psychiatry, and psychology) to discuss how to proceed with the study of these key areas through a common lens. The field would benefit from clear specification of these terms to better communicate within and across disciplines.
Closer examination of the terms cognitive impairment and mild cognitive impairment reveals that such common understanding does not yet exist. Our review uncovered that when using these terms, few authors offered definitions. When definitions appeared, there was no consistent application across studies or, more surprisingly, within disciplines. Furthermore, it was common for researchers from various disciplines to have technically distinct definitions of terms, especially when the terms were used in the vernacular. In the articles we reviewed, there was more clear and consistent terminology used, once a specific etiology was confirmed.
In addition, there was substantial variation in the measurement tools used to quantify participants’ level of cognitive impairment and MCI and inconsistency in interpreting results of these tools, especially with respect to various stages of cognitive decline. For example, the MMSE was the most used measurement tool to identify cognitive impairment. Yet the MMSE is a screening tool and not intended for diagnosis (Monroe & Carter, 2012). The widespread, individualized interpretation of MMSE scores by researchers highlights the limited utility of this tool to capture the early spectrum cognitive impairment.
Part of our assessment of methodological rigor in this review was to determine whether standard demographic information was reported in the articles in our data set. We found inconsistent reporting on race and ethnicity, gender, income level, and time since diagnosis. When data were collected about ethnicity and race, the data sets revealed a lack of ethnic and racial diversity in the samples. Because not all studies included this information, it is unclear whether they indeed lacked diversity; however, such information is essential to understand the broader patterns of social determinants of health as they relate to cognitive aging. Moreover, universally collecting and reporting demographic information is critical to producing credible research and drawing appropriate conclusions.
Finally, based on journal classifications, research from a variety of disciplines was represented in our data set, with geriatrics, neurology, and psychiatry featured prominently. Less represented were journals specific to the disciplines of social work, nursing, and sociology. Because of the significance of cognitive aging and cognitive health as key public health issues, readers of all health-related professional journals would benefit from articles on these topics.
Suggestions Going Forward
Findings from this scoping review have important research and practice implications and indicate the importance of moving toward agreed upon definitions and measurement for cognitive disorders impacting older adults. First, researchers should include a definition and citation for the term(s) used for cognitive health description (Petersen et al., 2014), as such precision will aid in the ability to compare, reproduce, and interpret results. Moreover, more research is needed to uncover whether consistency in terminology exists within disciplines such as geriatrics, neurology, and psychiatry, as inconsistent use of terminology can hinder communication within disciplines as well. If such consistency is present, researchers should state the disciplinary-specific definition and its measurement for the benefit of those working in other disciplines. Second, journals should consider promoting consistent usage and definitions of cognitive health terms. This scoping literature review highlights the need for future research, such as use of the Delphi method, to establish definitions of these terms. Third, well-established and psychometrically strong measurement tools should be developed and used in ways that enable consistent interpretation of results across studies. As noted in our findings, screening tools such as the MMSE have limited utility for capturing the spectrum of cognitive impairment, especially in its early stages. Finally, it is also important for the field to identify common data elements to be reported in all research studies about these topics, including demographic information of samples. Such standards would help ensure scientific rigor and transparency as multiple disciplines join together to improve the cognitive health of older adults.
Governmental funding research mechanisms, professional associations, and publishers can play a key role in this effort by providing authorship guidance that aims for greater consistency in research language and reporting requirements. Substantial efforts have been made in this direction with the 2011 update of clinical guidelines for diagnosis, which have more clearly delineated the clinical differences that exist on the cognitive continuum (e.g., Albert et al., 2011; McKhann et al., 2011). In clinical practice, having clearer and agreed upon definitions of cognitive impairment and MCI may help facilitate diagnosis and treatment. Additionally, discussing terms with consistency might serve to legitimize the subjective experiences of individuals in the early stages of cognitive change.
There were several limitations of this scoping review. Due to the nature of the search strategy, the data set may have inadvertently excluded some articles due to the specific nature of the search terms and inclusion/exclusion criteria. The review was limited to studies conducted in the United States due to an effort to preserve conceptual clarity. We anticipate that an analysis incorporating international research reporting might surface additional deviations in language and terminology, due to the introduction of translational and cultural influences. In addition, basic science articles were excluded from the data set because of a focus on public health, yet extensive research on dementia and Alzheimer’s disease is being conducted in this area, along with research in areas related to cognitive training and intervention. Future studies might expand inquiry into each of these directions. Our search was reliant on the indexing of the four databases employed, Embase, CINAHL, PsycINFO, and MEDLINE. Also, our approach did not include a review of author disciplines, only the discipline of the journal in which a study was published, thereby limiting the view of the disciplinary representation of research.
We found few terms describing research on healthy cognitive status; rather, most of the terminology focused on cognitive decline, and many of the identified terms had negative valence. This absence of terminology surrounding positive cognitive outcomes of aging suggests an important area for future research. Further work could also include additional analytical strategies, such as semantic network analysis or automated forms of topic modeling of the corpus of articles, to further expand on the variety of terminology and themes used in describing research on these topics. Likewise, an analysis of how terminology has changed over time may be a fruitful avenue for exposing the nuanced and positive changes that have occurred in response to more detailed studies of cognitive aging. In addition, researchers could examine other terms related to cognitive health and cognitive aging (see Online Appendix 2), beyond that of cognitive impairment and MCI, and terminology employed in other settings such as clinical and caregiving settings.
Conclusion
In sum, with society’s aging population, work on understanding and improving cognitive health is of utmost importance, and researchers from across disciplines have joined this mission. Although some ambiguity can be helpful to research innovation, the disparities in definitions of cognitive impairment and MCI ultimately hinder cross-disciplinary communication. This limits opportunities for broader research collaboration to meet the challenges of cognitive aging and impedes dissemination of research on a wider scope. If researchers aim to make progress toward improving cognitive health among all older adults, it would be helpful to have more specificity and clarity around definitions, along with greater consistency in the use of measurement tools to assess the conditions of study.
Supplemental Material
Supplemental Material, Appendix_1 - Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review
Supplemental Material, Appendix_1 for Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review by Kelly Quinn, Christina E. Miyawaki, Raina Croff, Mia T. Vogel, Basia Belza, Anita M. Souza, Minhui Liu, Valerie J. Edwards and Daniela B. Friedman in Research on Aging
Supplemental Material
Supplemental Material, Appendix_2 - Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review
Supplemental Material, Appendix_2 for Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review by Kelly Quinn, Christina E. Miyawaki, Raina Croff, Mia T. Vogel, Basia Belza, Anita M. Souza, Minhui Liu, Valerie J. Edwards and Daniela B. Friedman in Research on Aging
Supplemental Material
Supplemental Material, Appendix_3 - Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review
Supplemental Material, Appendix_3 for Terms and Measures of Cognitive Health Associated With Dementia and Alzheimer’s Disease: A Scoping Review by Kelly Quinn, Christina E. Miyawaki, Raina Croff, Mia T. Vogel, Basia Belza, Anita M. Souza, Minhui Liu, Valerie J. Edwards and Daniela B. Friedman in Research on Aging
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: South Carolina Department of Health and Human Services (A20190088), Aljoya Endowed Professorship in Aging, National Center for Advancing Translational Sciences (award number UL1 TR002319), Oregon Alzheimer’s Disease Center of Oregon Health Sciences University (NIA grant #AG08017), and Centers for Disease Control and Prevention Alzheimer’s Disease and Healthy Aging Program (Cooperative Agreement Number U48DP005013).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.