
Abstract
We use data from the 2014 China Longitudinal Aging Social Survey to examine the effect of attitudes toward aging on quality of life among older adults in China. We find that older people who experience psychosocial loss may be less satisfied with their life, and have more feelings of depression and loneliness. Compared to older women, older men have lower life satisfaction, and more depression and loneliness, though psychosocial loss has less of an effect on them. Older women who experience psychosocial loss are more likely to be dissatisfied with their life and feel more depressive and lonelier than their male counterparts. Among those who experience psychosocial loss, older people living in rural communities have a higher level of life satisfaction, while living in urban areas may counteract some of the positive impact of psychological growth on reducing the frequency of feeling depressed and lonely. Social policy can play a role in shaping constructive social/community environments to build more positive attitudes toward aging.
China has the largest older population and fastest aging speed in the world (Qin & Wang, 2017). In response to population aging, China abolished the one-child policy and permitted each couple to have two children in 2015, but the effect of this policy change remains to be seen (Chen, Alston, et al., 2019). Low fertility and ever-increasing life expectancy make aging a prominent public policy and public health issue. Exploring factors affecting older people’s capacity to live a long, high-quality life is a pressing issue in China (Chen, Guo, et al., 2019). Quality of life (hereafter, QoL) measurements include both subjective and objective dimensions. QoL usually refers to the many different positive and negative evaluations that people make of their own lives (Diener, 2006). These evaluations typically focus on subjective measurements of life satisfaction, as well as the objective presence or absence of psychological symptoms such as loneliness, depression, anxiety or low self-esteem, which are also well-accepted indices of health status in the Western world (Gana et al., 2013).
A positive attitude can be viewed as an important step toward enhancing QoL. Research has shown that older individuals who endorse more positive attitudes toward aging may live longer and healthier lives and have a higher QoL (e.g., Kerschner & Pegues, 1998). However, in view of the cultural differences between west and east, Chinese attitudes toward aging might be complex and may differ from those found in other contexts. On one hand, aging could be associated with fear of death, anxiety, stereotypes, and physical disabilities, which lead to negative attitudes toward aging, like in some western countries (Nelson, 2005; Vasil & Wass, 1993). On the other, Chinese tradition and culture often place a strong emphasis on respecting and valuing the contributions of elders because they are experienced, knowledgeable, and wise (Laidlaw et al., 2010). These cultural norms lead people to conclude that older people are highly valued and are viewed as important in Chinese society (Mok et al., 2007). These opinions form the basis for Chinese older adults’ attitudes toward aging and affect their life satisfaction and mental health. However, values are changing in contemporary Chinese society and positive attitudes toward aging are on the decline. Laidlaw et al. (2010) conducted a cross-sectional study of attitudes to aging in three different groups: older Chinese immigrants in the UK, older Chinese adults living in Beijing, and UK-born older adults living in Scotland. They found that both the Chinese-immigrant and UK-born participants reported more positive attitudes toward aging than the Beijing-Chinese participants.
Hence, for practitioners and policy-makers alike, it is imperative that we improve our understanding of how Chinese older people’s views of aging affect their QoL, while also taking their health-related circumstances into account. One way to build such knowledge is to examine older people’s attitude toward their own aging and explore its effects on their QoL in the Chinese context.
Literature Review
Attitudes Toward Aging from the Perspectives of Older People
Social psychological research has historically focused on attitudes. An attitude can be defined as a belief that has an “evaluative component” (Bryant et al., 2012), or as the “evaluation of a stimulus as reflected in our affective, cognitive, and behavioral responses to it” (Hess, 2006, p. 379). These evaluations and our responses to them may be part of a conscious process, as individuals consider information about the “attitude object” (i.e. aging), and then formulate their response to it (Glasman & Albarracin, 2006). How people feel about getting older and the age at which they consider themselves to be “old” are thought to become salient from midlife onward, triggered by signs of physical aging, role transitions, menopause, possible health issues, and the loss of parents, which can cause people to question their own mortality (Levy et al., 2009). Most of this research has followed a model of attitude measurement prevalent in social psychology: respondents are shown a set of Likert-type opinion statements with which they are instructed to agree or disagree. Although there is no standard method of measuring attitudes toward aging (Kalfoss et al., 2010), the Attitudes to Aging Questionnaire (AAQ) represents one commonly-used approach, and was developed as part of a larger 3-year international project on the QoL of older adults in collaboration with the WHO (Power et al., 2005).
Attitudes toward aging have been found to be largely negative (e.g., Bennett & Eckman, 1973; Holroyd et al., 2009), with older people often holding the most negative attitudes (e.g., Thorpe, 2015). In addition, a systematic review of the literature on attitudes toward aging found that negative views among older people might reinforce similar views in the young, resulting in a feedback loop that further reinforces negative views of aging in both young and old. It can also lead to the neglect and rejection of older adults and an inability or unwillingness to plan for one’s own later years (Thorpe, 2015). Based on the premise that attitudes affect behavior and knowledge acquisition, other scholars have further examined and found that attitudes toward one’s own experiences of aging influence and shape health and well-being among older adults (Brown et al., 2016). Research has also found that positive attitudes are associated with better engagement with healthy behaviors (Levy & Myers, 2004) and enhanced well-being among older adults (Bryant et al., 2012), which helps to explain how and why attitudes to aging exert these powerful effects (Levy, 2009).
Quality of Life from the Perspective of Older People
Abrams (1973) defined QoL as the degree of satisfaction or dissatisfaction felt by people with different aspects of their lives, and Andrews (1974) related it to the extent to which pleasure and satisfaction characterize human existence. However, in social gerontology and social indicators research, one commonly-cited definition of QoL comes from George and Bearon’s (1980) work, which describes four underlying dimensions to the concept. Two of these dimensions are objective: general health/functional status and socioeconomic status; and two reflect the personal judgment of the individual: life satisfaction and self-esteem (Farquhar, 1995). Since QoL consists of a potentially infinite number of aspects, these four dimensions are central to, but cannot fully assess QoL (George & Bearon, 1980). In addition, QoL was first conceptualized in political and philosophical thought as dictated by people’s religious principles, rational thought and modern economic thinking (Diener & Suh, 1997). Previous research suggests that QoL reflects both macro-societal and socio-demographic influences on people, as well as individuals’ personal characteristics and concerns. There is arguably a common core of values influencing overall QoL within societies as QoL is subjective; however, QoL is equally dependent on individual interpretations, perceptions, and experiences (Ziller, 1974). If a person experiences their life as good, we assume this to be the case. This approach therefore prioritizes, factors like feelings of contentment, joy, and life satisfaction (Moons et al., 2006). This way of defining QoL is most associated with the subjective well-being tradition in behavioral sciences.
The World Health Organization QoL (WHOQOL) Group defined QoL as individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns (The WHOQoL Group, 1993). It is a broad concept encompassing a person’s “physical health, psychological state, level of independence, social relationships, and relationships with salient features of his or her environment” (Bodur & Cingil, 2009, p. 652). Although the WHOQoL were developed based on a sample in which 50% of participants were under 45 and 50% were over 45, there has been no subsequent examination of how the tools that were developed reflect older people’s evaluations of QoL (Hendry & McVittie, 2004). It therefore seems important to balance this perspective by focusing on older people’s own views of their QoL. Some studies have also indicated that growing old may provoke a shift in which domains are perceived to be important for QoL (Bowling & Windsor, 2001; Browne et al., 1994). Using a national survey of QoL of 999 people aged over 65, who lived in private households in Britain, Gabriel and Bowling (2004) found that the central elements of QoL consisted of: social relationships, roles, and activities; social capital; psychological wellbeing; independent hobbies and activities; and health and functional abilities. Borglin et al.(2005) conducted in-depth interviews with six women and five men (aged 80+) living in their own homes in Sweden. Using an interpretative hermeneutic phenomenological analysis, they found that QoL in older age was related to the preservation of a sense of self and meaning in life, and that family-oriented care, alongside helping older people remain in their own homes may enhance their QoL.
Association between Attitudes toward Aging and Quality of Life among Older Adults
As other authors have argued, “subjective perceptions of physical, cognitive and social aging have been found to influence mental health in terms of symptoms of depression, self-esteem and morale” (Low et al., 2013, p. 2). An extensive body of literature has found that specific dimensions of attitudes toward aging (e.g. physical changes and psychological growth) were significantly related to QoL among older adults in some western countries (Low et al., 2008; Top et al., 2013).
Mock and Eibach (2011) have confirmed that those who report feeling relatively older in middle-age and older adulthood had lower life satisfaction and lower self-esteem than those who feel younger relative to their chronological age. Across 20 country samples, Low et al. (2013) investigated how men’s and women’s attitudes toward their own aging affect their QoL between ages 60 and 100. They found that older people’s attitudes toward their own aging with respect to “physical changes,” feelings of “psychosocial loss,” and “psychological growth” were related to QoL regardless of participant age or gender.
Study Aims
Despite the fact that attitudes toward aging are thought to be significant predictors of older adults’ QoL (Top et al., 2013), the associations between these factors among older adults in the Chinese context have not been well addressed. Therefore, our aim in this study is to assess attitudes toward aging from the perspective of the older population itself, as older individuals are most capable of informing researchers about the experience of aging. Given the gender gap and urban-rural dual division system in China, there might be some heterogeneity of aging attitudes between genders and across urban-rural settings, moderating the relationship between attitudes and QoL. Thus, we examine the association between attitudes toward aging and QoL and clarify the extent to which the effects of aging attitudes determine variations in QoL across gender and urban-rural community settings, among older adults aged 60 years and over in China.
Method
We obtained data from the 2014 China Longitudinal Aging Social Survey (CLASS 2014), a project aimed at understanding various problems and challenges that Chinese people face during the aging process, including the Attitudes to Aging Questionnaire (AAQ), and evaluating the real effects of various social security policies, e.g. on improving the older population’s quality of life. CLASS 2014 is a large-scale nationwide social survey directed by National Survey Research Center (NSRC) at Renmin University of China. It employed a stratified, multi-stage sampling method: county-level regions were selected as the Primary Sampling Unit (PSU) and villages/communities were selected as the Secondary Sampling Unit (SSU), aiming to collect social and economic data on the Chinese aging population at both the individual- and community-level. Respondents to the survey were Chinese citizens aged 60 or above and the data were collected through face-to-face interviews conducted in their own homes. In the 2014 baseline survey, CLASS finished a survey of 11,511 older people lived in 476 villages/communities across mainland China. Although it was designed as a longitudinal survey, CLASS has so far only conducted two pilot surveys (in 2011 and 2012), and one baseline survey, in 2014. 1 In this study, we focused exclusively on the 2014 CLASS, treating it as cross-sectional data during the analysis.
Setting and Sample
Because of our study’s focus on the relationship between older people’s attitudes to aging and their QoL, and given that older respondents answered these questions themselves, participants scoring <3 on five cognitive questions (drawn from the Mini-Mental State Examination, MMSE by Folstein et al., in 1975) were excluded from the study (n = 2,790). Participants who had not completed the aging attitudes, depression, and loneliness questionnaires (n = 1,257) were removed. The cases with missing data for one or more covariates are about 789, in which the highest proportion of values missing is monthly income (554 cases, 7.5% of total). To reduce sample attrition, we used regression to impute the missing data of monthly income (analysis variables including age, gender, years of education, hukou status, and ethnic minority). The final simple consisted of 7,229 participants (M = 68.99 years, SD = 7.40; 45.84% female, 54.16% male).
The Dependent Variable
Quality of life (QoL)
The structure of QoL consisted of two major components: one emotional or affective, and the other a judgmental or cognitive component (Diener, 1984). The latter was also conceptualized as life satisfaction (Andrews & Withey, 1976). Thus, life satisfaction, depression, and loneliness were employed as measurements of QoL in this study. The measure of life satisfaction was extracted from the subjective, self-reported question of “Do you feel satisfied with your present life in general?” The options to this question took discrete values from 1 to 5, ranging from “very unsatisfied” to “very satisfied.” Depressive symptoms were measured using a shortened version of the CES-D (Center for Epidemiologic Studies–Depression Scale, developed by Radloff in 1977) with nine items, as revised by Santor and Coyne in 1997. The CES-D has been shown to be a valid and reliable instrument for measuring depression among older Chinese individuals (Cheng & Chan, 2005). Questions like “Do you feel sad?” and “Was your sleep restless?” were asked. Loneliness was measured using the three-item Loneliness Scale developed by Hughes et al. (2004), an abbreviated version of the 20-item revised UCLA Loneliness Scale (Russell et al., 1980), consisting of feelings of lacking companionship, being left out, and isolation from others. Options on the nine-item CES-D and three-item Loneliness Scale were both coded as “1” for rarely or none of the time, “2” for sometimes, and “3” for often. Scores were summed (range: 9–27 for the depression scale; 3–9 for the loneliness scale, separately) and a higher score indicated greater symptoms of depression and loneliness.
The Key Explanatory Variable
Aging attitudes
Participants’ attitudes toward the aging process were measured using a short version of AAQ (Laidlaw et al., 2007). The AAQ comprised a 24-item questionnaire including three subscales for: psychosocial losses; physical change; and psychological growth, each of which had eight items. The AAQ’s structure has been established in 15 countries including China (Guangzhou), using both classical and modern psychometric methods. Given that CLASS chose seven items from the AAQ (mainly from the psychosocial losses and psychological growth subscales), we constructed two indicators to measure aging attitude: psychosocial loss and psychological growth. Psychosocial loss was based on agreement with the following four statements: “I feel old”; “I see old age mainly as a time of loss”; “As I get old I find it more difficult to make new friends”; and “I feel excluded from things because of my age.” Psychological growth was based on agreement with three additional statements: “As people get older they are better able to cope with life”; “Wisdom comes with age”; and “There are many pleasant things about growing older.” Responses to these questions were coded using a 5-point scale, from 1 “totally disagree” to 5 “totally agree.” Total scores for all options were calculated (ranging from 4 to 20 for psychosocial loss and 3 to 15 for psychological growth, respectively).
Control Variables
Our regression models considered a number of demographic and socio-economic factors as control variables. These include economic and sociological variables like age, gender (0 = female, 1 = male), marital status (0 = unmarried, 1 = married), ethnic minority status (0 = no, 1 = yes), religious believer (0 = no, 1 = yes), monthly income (thousand yuan) as a range of covariates. Based on previous studies, we further selected years of education (Lai, 2009), physical activities of daily living (PADL, if the participants need help with dressing, bathing, eating, etc.), instrumental activities of daily living (IADL, if the participants need help with cooking, shopping, doing housework, etc.) (Hellström & Hallberg, 2001), number of living children (Tajvar et al., 2018), participation in social activities (Chiao et al., 2011), and community character (urban vs. rural) (Lau & Morse, 2008) as control variables.
Analysis
We used STATA (Version 14.0) for statistical analyses. Because the data were clustered and individuals were nested within communities, we used multilevel regression models instead of single-level multivariable analyses (Rabe-Hesketh & Skrondal, 2008). We first present descriptive statistics for all variables by gender. ANOVA and Chi-squared tests were used to assess the differences for continuous and categorical variables, respectively. Correlations between aging attitudes, covariates, and subjective well-being were tested. After preliminary analysis using variance component models, we examined the association between aging attitudes and QoL using hierarchical regression. In the subsequent hierarchical regressions, interaction terms between aging attitudes and gender and community urban-rural character (gender × aging attitudes and urban community × aging attitudes) were entered to identify whether there were moderating effects. Robust standard errors (SE) were calculated. The Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and log likelihood tests were used to assess model fit across nested models. As suggested by Monte Carlo simulation studies, lower AIC, BIC, and log likelihood values indicate that the model fits the data better (Nylund et al., 2007).
For hierarchical regression, we define Yij as the score of self-reported life satisfaction/ depression/ loneliness of older people i living in community j. Yij can be modeled using a regression approach. Thus, the two-level random-intercept model can be expressed as in Equation (1).
where β and γ are the coefficients of the individual-level and community-level variables, respectively, γ00 is the intercept, which is allowed to vary by community, u 0j are residual error terms at the community level, and ε ij is the usual residual error term.
For testing the interaction effect, interaction items of gender × psychosocialloss, gender × psychosocialgrowth, urban × psychosocialloss, and urban × psychosocialgrowth were also added. A significant p-value of interaction effect meant that simple slope of psychosocial loss or psychosocial growth was significantly different across gender or rural-urban settings. Given that our main concerns were the simple slopes of regression of Y on psychosocial loss and psychosocial growth, we calculated the coefficients of psychosocial loss, psychosocial growth and corresponding interaction items when we interpreted the interaction effects (Preacher et al., 2006).
Findings
Descriptive Statistics
Table 1 presents descriptive statistics for each variable (mean and standard deviation (SD) for continuous variables, frequency and percentage for categorical variables, respectively) and difference test results comparing male and female gender groups. The results regarding QoL–life satisfaction, depression, and loneliness–show that there are significant differences in depression and loneliness between older men and women, except for life satisfaction. Older women’s higher scores for depression and loneliness show their poorer status, compared to older men. Regarding attitudes to aging, there are no significant differences in the distributions of psychosocial loss and psychosocial growth across gender groups.
Descriptive Characteristics of the Study Sample and Bivariate Analyses by Gender.
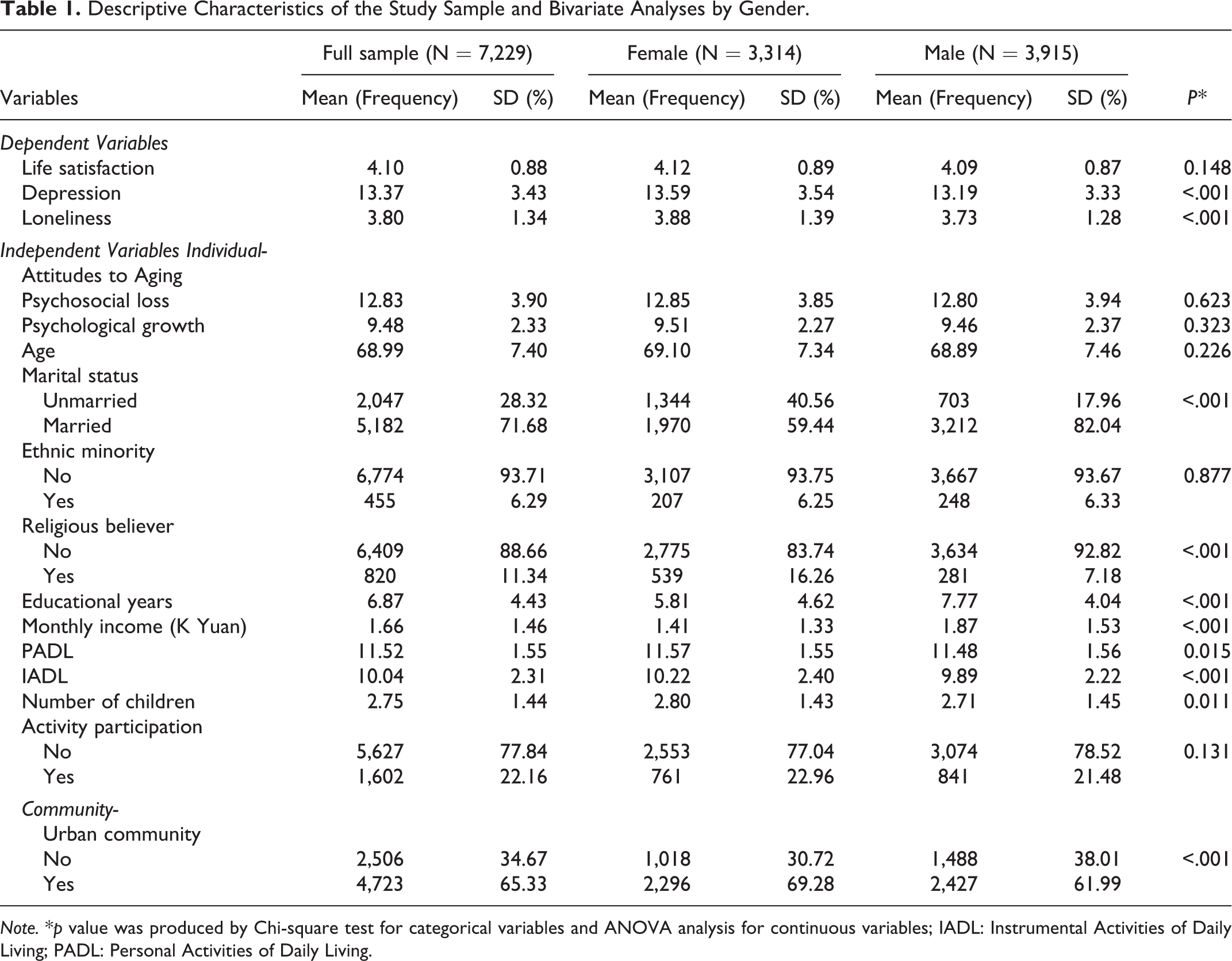
Note. *p value was produced by Chi-square test for categorical variables and ANOVA analysis for continuous variables; IADL: Instrumental Activities of Daily Living; PADL: Personal Activities of Daily Living.
Nearly half (45.84%) of respondents are female, and the sampled women’s mean age was 69.10 years (SD = 7.34), compared to 68.89 (SD = 7.46) for men. With respect to marital status, 59.44% of women and 82.04% of men were married. Women are more likely be religious believers than men. Older men have higher levels of education (mean = 7.77 years, SD = 4.04) and a higher monthly income (mean = 1.87 (thousand yuan), SD = 1.53) than older women (mean = 5.81 years of education, SD = 4.62; mean = 1.41 (thousand yuan), SD = 1.33). Older women’s higher PADL and IADL scores indicate that their health status is worse than men’s. Regarding community character, 30.72% of older females and 38.01% of older males live in rural communities.
Bivariate Correlation
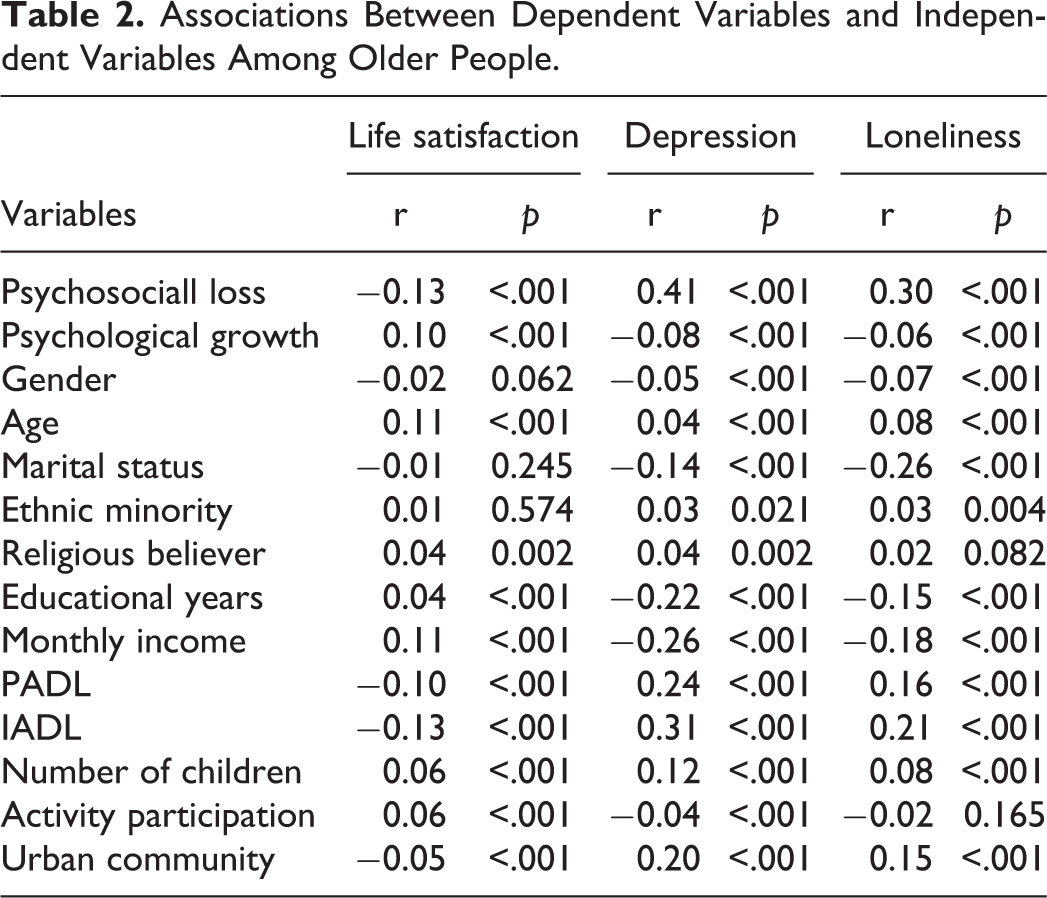
Table 2 displays the correlations and p-values of significance tests for the relationship between dependent and independent variables. Psychosocial loss is negatively associated with life satisfaction and positively associated with depression and loneliness (r = −.13, p < .001; r = .41, p < .001; r = .30, p < .001, respectively). Psychological growth is positively associated with life satisfaction (r = −.10, p < .001) and negatively associated with depression and loneliness (r = −.08, p < .001; r = −.06, p < .001, respectively). Older males experience less depression and loneliness than females (r = −.05, p < .001; r = −.07, p < .001). Older people who live in urban communities are less satisfied with life (r = −.05, p < .001) and more likely be depressive and lonely (r = .20, p < .001; r = .15, p < .001, respectively).
Associations Between Dependent Variables and Independent Variables Among Older People.
Hierarchical Linear Regression Analysis
The results of the analysis of variance component models show that communities may account for a considerable proportion of total variance. The ICCs (intra-class correlation coefficient) for life satisfaction, depression, and loneliness are .09, .13, and .08, respectively. Table 3 presents the results of hierarchical regressions addressing QoL among older people. Older people who experience feelings of psychosocial loss may be less satisfied with their life and have a higher frequency of feeling depressed and lonely. The covariates selected based on the previous literature (gender, age, marital status, monthly income, IADL, number of children, and community character) all exhibited associations with QoL in some way.
Effect of Aging Attitude on QoL Among Older People.
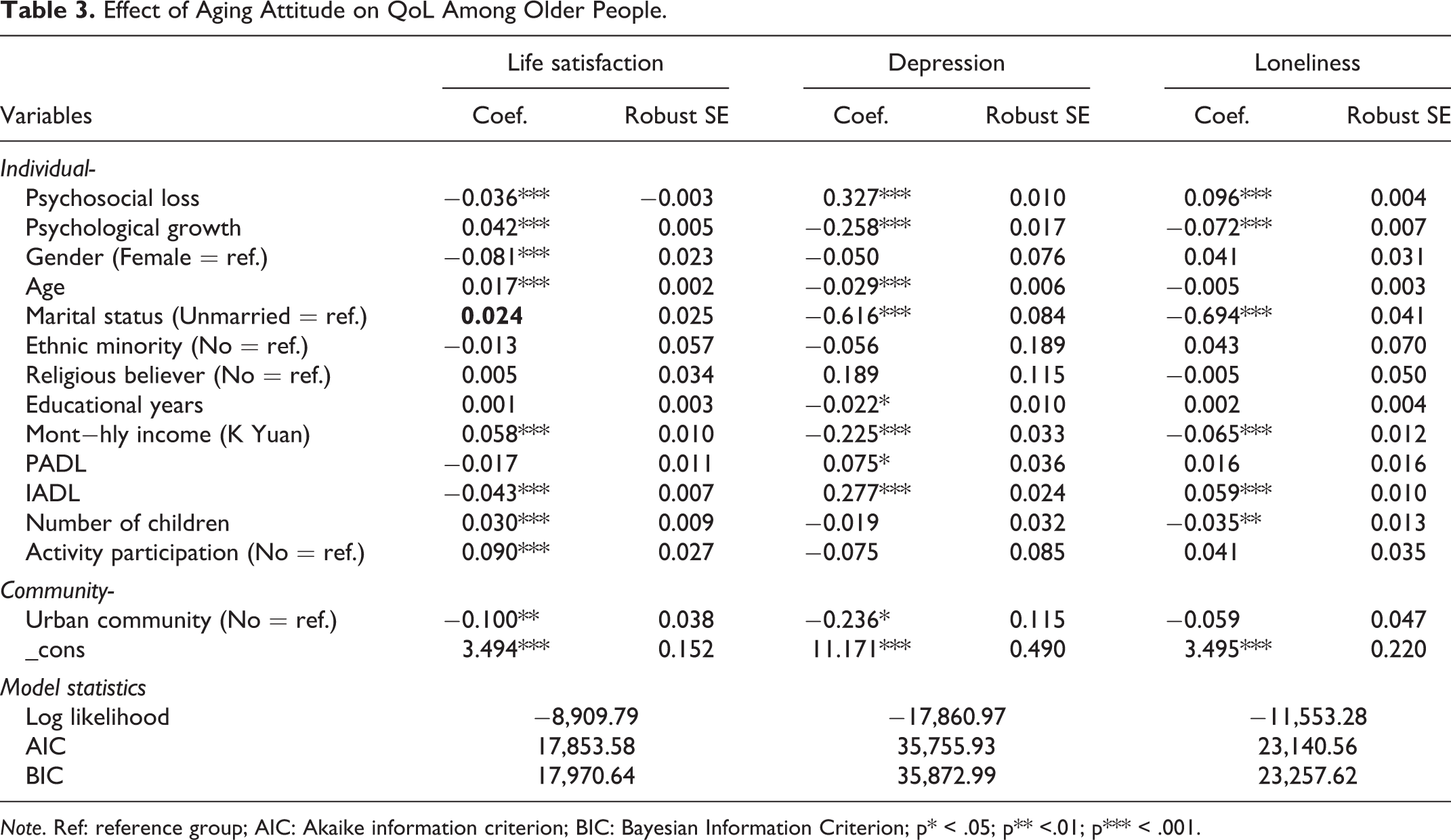
Note. Ref: reference group; AIC: Akaike information criterion; BIC: Bayesian Information Criterion; p* < .05; p** <.01; p*** < .001.
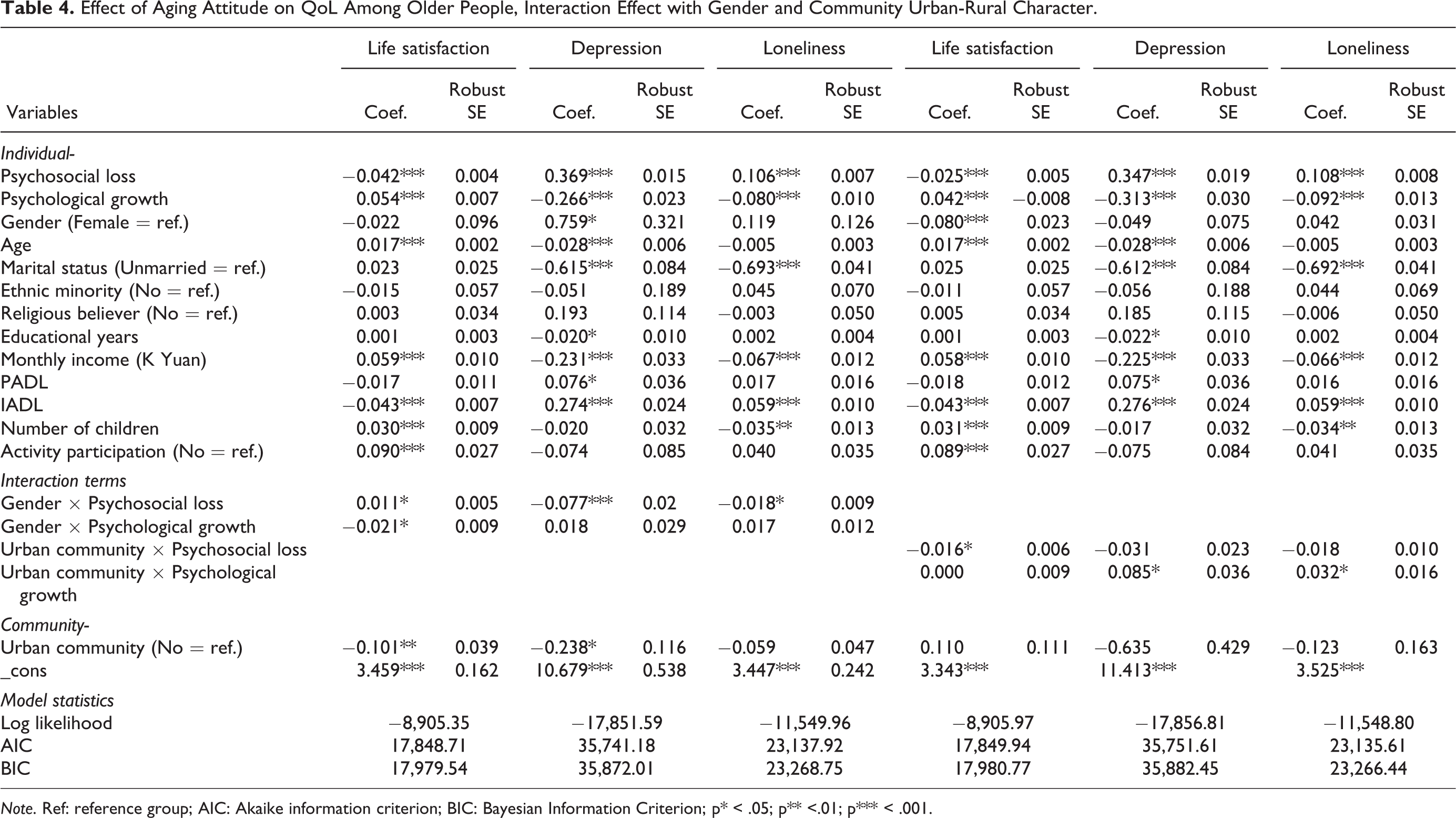
Table 4 presents the results of analyses examining whether the association between aging attitude and QoL is moderated by gender and community character. The results show that the impact of psychosocial loss on life satisfaction, depression, and loneliness is significantly different for older women and men. Psychosocial loss has less of effect on older men. The marginal effects of psychosocial loss on life satisfaction are −0.042 for women and −0.031 (−0.042 + 0.011) for men. The associations between psychosocial loss and depression are 0.369 among older women and 0.292 (0.369–0.077) among older men. The associations between psychosocial loss and loneliness are 0.106 among older women and 0.088 (0.106–0.018) among older men. Regarding psychological growth, the associations with depression and loneliness exhibit no significant differences between older men and women. However, the relationship between psychological growth and life satisfaction does vary among gender groups (0.054 for older women and 0.033<0.054–0.021> for older men). More psychosocial growth will bring more benefit for female elderly’s life satisfaction.
For older people experiencing feelings of psychosocial loss, those who live in rural communities might feel less affected on their life satisfaction than their urban counterparts (−0.025 for rural older adults and −0.041<−0.025−0.016> for urban older adults). Similarly, living in urban communities may counteract some of the positive impact of psychological growth on reducing the frequency of feeling depressed (−0.313 for rural older adults and −0.228<−0.313 + 0.085> for urban older adults) and lonely (−0.092 for rural older adults and −0.06 <−0.092 + 0.032> for urban older adults), meaning that the situation of older men and women who have experienced psychological growth is worse in urban than in rural communities.
Effect of Aging Attitude on QoL Among Older People, Interaction Effect with Gender and Community Urban-Rural Character.
Note. Ref: reference group; AIC: Akaike information criterion; BIC: Bayesian Information Criterion; p* < .05; p** <.01; p*** < .001.
Discussion
This study focused on two themes: first, it examined the association between attitudes toward aging and QoL; second, it clarified the extent to which the effects of attitudes toward aging determine variations in QoL across urban-rural community settings and between older men and women in the Chinese context. The findings of this study contribute to the growing literature demonstrating that older people who experience psychosocial loss might be more dissatisfied with their life, and experience more feelings of depression and loneliness (Lai, 2009). As other scholars have found, “Attitude is the central issue that predicts, explains and continuously influences behavior and determines emotion, thought and behavioral style” (Kim et al., 2004, in Suh et al., 2012, p. 97). This indicates that older people with a positive attitude about themselves are better able to adapt to the aging process and, accordingly, that positive attitudes toward aging might enhance older people’s QoL. Therefore, in more developed areas of China, communities could be built around the expansion and strengthening of older adults’ networks, in which an educational program, such as socialization groups based on a role theory perspective, could be incorporated to facilitate constructive adaptation to the psychosocial challenges faced by older people, to help them develop positive attitudes and see themselves as valuable. This could help promote higher QoL among older adults. The government could also institutionalize initiatives such as “Silver Hair Action” Program, which was previously launched to mobilize retired people with different professional expertise to go to less developed areas of China and provide these communities with needed intellectual and practical support (Mui, 2010). This could further aid older adults with worse psychological health in less developed areas of China.
In this study, we also examined how older peoples’ gender and community characteristics moderated the relationship between their attitudes toward their own aging and QoL. Older women who experience psychosocial loss are more likely to feel unsatisfied with their life, more depressive, and lonelier than their male counterparts. Attitudes are affected by social cognition (Greenwald & Banaji, 1995). Older Chinese women usually have lower levels of education, alongside poorer cognitive and economic resources (Lei et al., 2012), which in turn affects their attitudes toward aging. Therefore, if older women experience psychosocial loss, it will have a greater impact on their QoL. Wang et al. (2009) found that, among older people in China, gender differentials in many health indicators increased with age, generally disadvantaging women. In an aging society, and due to their longer life expectancy, older women will live without their husbands for many of their later years. Psychosocial loss may be even more critical for older Chinese women than men (Lei et al., 2012). Considering that living with a spouse has a direct influence on older women’s QoL (Suh et al., 2012), it is also important to encourage those women without a spouse to engage in economic and social activities that can help them take care of their psychological well-being.
Working in two Chinese provinces, Strauss et al. (2010) found that, for many dimensions of health outcomes, unmeasured community influences are highly important, much more so than one usually finds in this context. As shown in our study, among older people experiencing feelings of psychosocial loss, living in rural communities might have a lesser impact on their life satisfaction than living in urban communities. The basic reasons why most rural-dwellers are happier despite their relative income poverty and lower socio-economic status probably relate to having limited information sets and narrower reference groups. Additionally, their own income has risen in recent years and they expect it to rise in the future, and they place a high value on personal and community relationships. Moreover, in China’s traditional rural areas, people live in a social context which is highly stable. This situation likely offsets the negative impact of social and psychological losses on the QoL of rural older people. In China, peasant families appear to be more traditional than others, and people in rural areas usually have more respectful attitudes toward older adults, which allows older adults with a positive attitude toward aging to gain more social support and recognition, thereby improving their QoL.
Meanwhile, living in urban communities may counteract some of the positive impact of psychological growth on reducing the frequency of feeling depressed and lonely, making the situation of older urban-dwellers who experienced psychological growth worse than that of their rural peers. This result suggests that urban communities and rural villages are important social and economic entities that have a collective impact on their residents. In addition, this finding is similar to those of a previous study in China, showing that standards of living are substantially lower in rural areas, and suggesting that, while the financial needs of older adults in rural areas may be greater, community-based programs are more abundant in urban areas (Guo et al., 2019). We think that social policy that promotes age-friendly and community-based health care programs for older people are important for maintaining their physical and psychological well-being and promoting healthy aging in China. Here, “healthy aging” means not only that older adults live in good physical/mental health and participate in social activities, but also that Chinese society would benefit from implementing sound policies and intervention programs for older adults, to support this.
The limitations of this study deserve discussion and suggest directions for future research in this area. The causal relationship between aging attitudes and the QoL of the older adults in this analysis is assumed to be unidirectional (with positive attitudes toward aging thought to influence QoL positively). However, because this analysis relies on cross-sectional data, we are unable to model the dynamic correlation between aging attitudes and QoL among older Chinese adults. Other limitations relate to the measures used in this study. The measurement of aging attitudes and QoL limits our ability to capture these variables in a more multidimensional and nuanced way.
Conclusion
Despite these limitations, the results of our analysis have raised some intriguing questions with regard to the wellbeing of older adults in China and have implications for elder care policy in China. Although family support for elders is deeply rooted in Chinese tradition and promoted by government policies, current demographic and social patterns suggest that families’ capacity and willingness to provide care for older adults may be diminishing. Our findings show that there is a need for developing community-focused intervention programs, using community resources that are directed toward China’s older population. A follow-up study that focuses on community capacity building, and which includes integrated, high-quality health care and social welfare services for older men and women will contribute to the development of healthy aging in China. Moreover, over the past several months, both the number of people with 2019 novel coronavirus disease (COVID-19) and the number of deaths associated with this new illness have been increasing, particularly affecting older adults (Yang et al., 2020). In 2017, older adults aged 60 years and above constituted 17.3% of China’s total population, of whom around 19% required long-term care due to disabilities and 14% were the oldest-old (aged over 80) (Han et al., 2020). Loneliness and social isolation are known to be associated with negative physical and mental health outcomes, including increased symptoms of depression and anxiety (Morrow-Howell et al., 2020). Therefore, Chinese central and local governments should focus on the inequalities experienced by disadvantaged older people who urgently need long-term care due to disabilities or who are living alone during this crisis, and bring a stronger commitment to improving their QoL both now and into the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Fund of China (NSSFC) under Grant No. 20VYJ039, the National Natural Science Foundation of China under Grant No. 71921003, and Shandong Provincial Social Science Planning Project under Grant No.20CRK01. Dr. Wei Guo would like to convey the deep feeling of missing his beloved maternal grandparents, Mr. Chao Wang and Mrs. Zequn Ma, who have gone to heaven from their rural village in western China where aging support systems have been structurally fragile many years ago, through remaining true to his original aspiration of writing and publishing research papers on Aging, Health and Well-being (AHW) in China.