
Abstract
While the health implications of intergenerational caregiving have been broadly investigated in the aging literature, less is known about caregivers in four-generation families and their living arrangements. Using 2011 and 2013 waves of China Health and Retirement Longitudinal Study (N = 12,914 obs.), we document enhanced life satisfaction of grandchild caregivers and sandwich caregivers caring for both grandchildren and parents than non-caregivers. When further taking living arrangements into consideration, we find that parent caregivers also benefit from care provision when not living with their parents and sandwich caregivers only have an advantage when co-residing with care recipients with adult children present in households. By contrast, grandchild caregivers living with grandchildren show substantially higher life satisfaction no matter adult children are present or not. The subgroup comparison suggests that females and rural residents enjoy psychological advantages over their male counterparts and urban counterparts in grandparenting within skipped-generation households and sandwich caregiving.
Introduction
The health implications of caregiving activities have been extensively studied in the social science literature. Existing studies under the Western context often treat caregiving activities as a chronic stressor that elicits detrimental effects on physical and mental health (Chen et al., 2015; Pearlin et al., 1990; Pinquart & Sörensen, 2003a). However, competing theoretical perspectives and mixed empirical evidence exist, depending on the type of caregiving, the level of intensity, and the national setting (Arpino et al., 2018). For example, in the context of China, where filial piety and reproductive obligation of Confucianism still prescribe substantial caregiving responsibilities and strong intergenerational bonds (Chen & Liu, 2009; Xu, 2019), the normative expectation of care for parents or grandchildren may translate into emotional rewards for middle-aged and older adults. Moreover, recent evidence shows that intensive care provision to parents (Cheng et al., 2020) or grandchildren (Pan et al., 2020) usually leads to stress for caregivers. However, a lighter load of care may not be harmful and may even provide health benefits, particularly when it comes to grandparents caring for grandchildren (Chen & Liu, 2012).
The purpose of this study is to investigate the implications of intergenerational caregiving, defined as parental care and care for grandchildren, for the life satisfaction of adults in mid and later life in China. Existing literature on the health consequences of care for grandchildren and aging parents often do not overlap. However, we argue it is important to integrate these two types of care in contemporary China. In the Western context, increasing attention has been paid to the sandwiched generation, those who are caught between childcare and parent care responsibilities, driven mainly by delayed fertility (Miller, 1981). In the context of China and in this study, we refer to the sandwich caregivers as those who are shouldering the responsibilities of care for grandchildren and their parents simultaneously. As a result of prolonged life expectancy and declined child mortality (Feng, 2011), more and more individuals live to become grandparents while their parents are still alive, giving rise to the prevalence of four-generation families. We witness the primary caregiving responsibilities increasingly fall onto middle-aged and older adults. Care for aging parents is considered their filial duties, as institutional care is still largely stigmatized in China. At the same time, due to the extremely high labor force participation rates among young adults and the lack of formal childcare facilities, grandparents are often considered the default alternative childcare providers. Thus, compared to the younger generation, caregivers in their middle and later life are more vulnerable to intensive caregiving loads, but they may also be more likely to acquire an enhanced sense of self-fulfillment from these caregiving activities. After all, “four generations living under the same roof (Si Shi Tong Tang)” is considered a cultural ideal in China, historically only within reach of the richest families.
Are these “sandwich caregivers” suffering from competing demands from multiple care recipients? Or, do the benefits of caregiving outweigh the adverse effects? Additionally, the care setting also matters. Does living with parents or grandchildren (or both) translate into a higher caregiving load and therefore take a toll on life satisfaction? Or, could the multigenerational living arrangements be culturally preferred and therefore enhance family support? We maintain that we should answer these questions in consideration of China’s unique normative and cultural context. Using the 2011 and 2013 waves of China Health and Retirement Longitudinal Study (CHaRLS), we examine the implications of caring for aging parents only, caring for dependent grandchildren only, and caring for both generations for life satisfaction, with specific attention paid to the influence of multigenerational living arrangements. Further, we compare the subgroups of male and female caregivers and rural and urban caregivers to investigate the potential heterogeneities of caregiving’s psychological effects.
Role Strain or Role Enhancement? The Health Implications of Caring for Grandchildren and Older Parents
The stress process model and role enhancement assumption serve as competitive theoretical perspectives regarding the caregiving’s health implications in demographic and aging literature. The stress process model argues that caregivers are exposed to hardships directly related to caregiving activities, such as ADL dependencies, financial strains, and relational deprivation, and intrapsychic strains and the strains brought by roles and activities outside caregiving involving self-concepts diminishment (Pearlin et al., 1990). By contrast, the role enhancement hypothesis regards the pile-up of multiple roles as an opportunity for achieving self-actualization and self-fulfillment (Doress-Worters, 1994) given that the increased social support and social integration have the potential to offset the risks of role strain. It is also recognized by the stress process model that social support could act at multiple points as a moderator between caregiving and stress outcomes (Pearlin et al., 1990).
The tendency that most empirical studies in the Western context adopt the stress process model in explaining caregiving’s health implications may be rooted in the individualistic culture of emphasizing individuals’ independence and freedom of choice (Hofstede, 1980; Schimmack et al., 2002). Adult children who provide informal caregiving to older adults are found to experience increased depressive symptoms (Bookwala, 2009; Pinquart & Sörensen, 2003a), stress (White-Means & Chang, 1994), and reduced self-efficacy and general subjective wellbeing (Pinquart & Sörensen, 2003b). Moreover, conforming to the norm of noninterference in intergenerational relationships, most grandparents in the United States are not socially expected to care for their grandchildren (Cherlin & Furstenberg, 1986). Much of the United States grandparenting literature focuses on grandparents with sole parenting responsibilities for grandchildren as a response to adult children’s plight, such as marital dissolution, drug abuse, and incarceration (Swartz, 2009). Therefore, grandparental childcare is found to be associated with adverse self-reported health, ADL limitation, depressive symptoms (Minkler et al., 2000), and lower satisfaction with health (Minkler & Fuller-Thomson, 1999). A few recent studies indicate potential positive effects (Arpino & Bordone, 2014; Szinovacz & Davey, 2006), but excluding sample selection bias caused by the small and selective samples is challenging.
China has a different context that filial piety and reproductive obligation of Confucianism still prescribe strong intergenerational ties among grandparents, parents, and grandchildren throughout life (Chen et al., 2000). Family duties are often prioritized over individuals’ own needs, and intergenerational caregiving is highly universal and normative (Chen et al., 2000; Gu et al., 2007). Grandparents who care for grandchildren are often found to have enhanced life satisfaction and decreased depressive symptoms (Guo et al., 2008; Xu, 2019; Xu et al., 2012). However, empirical evidence is mixed regarding the health implications of caring for aging parents, with some suggesting adverse effects on females’ life satisfaction (Chen et al., 2019) while others observing enhanced life satisfaction among rural female caregivers and urban male caregivers (Xu, 2019). Thus, further exploration is needed to clarify the impact of parental caregiving.
Among parent caregivers and grandchild caregivers, a unique group is the “sandwich generation” (Miller, 1981). In Western literature, sandwich caregivers are often defined as those caught by childcare and parent care responsibilities (Grundy & Henretta, 2006). As indicated by the name, they are often assumed to be significantly disadvantaged by multiple-role conflicts and role strain (DeRigne & Ferrante, 2012). Empirical studies also associate sandwich caregiving with higher levels of depressive symptoms (Hammer & Neal, 2008), distress (Doress-Worters, 1994), and various unhealthy behaviors (Chassin et al., 2010). However, in the context of China, sandwich caregivers are often those caring for aging parents and young grandchildren (Falkingham et al., 2020), and they may benefit more than caregivers with sole caregiving responsibilities, given that familial caregiving is prevalent and socially expected. For example, Xu (2019) finds higher life satisfaction and fewer depressive symptoms among the Chinese sandwich caregivers. However, sandwich generation in four-generation families, especially their mental health and wellbeing, still received scant attention and needs further investigation in China’s context.
Intergenerational Living Arrangements as An Indicator of Caregiving Intensity
The level of caregiving varies across caregivers and also has implications for individuals’ wellbeing. Recent research points out the importance of highlighting the potential effects of caregiving intensity (Arpino et al., 2018). Although intensive caregiving for parents (Cheng et al., 2020) or grandchildren (Pan et al., 2020) usually leads to stress, a lighter level of care may cause health benefits for caregivers (Chen & Liu, 2012). To tease out unexplored heterogeneities, empirical studies often adopt intergenerational living arrangements to indicate the intensity of care provision, with multigenerational coresidence representing heavier involvement in caregiving responsibilities relative to non-coresidence (Chen et al., 2011; Chen et al., 2015; Cong & Silverstein, 2008). Living arrangements can comprehensively capture the nature of care provision as well as other potential sources of support. For example, recent decades of China witnessed many young people migrate to cities seeking employment and leave their dependent children to be cared for by grandparents (Song & Chen, 2020), constituting many “skipped-generation” households. This “skipped-generation” coresidence clearly indicates that middle-aged and older adults are likely to take custodial responsibilities in place of their adult children.
Multigenerational coresidence is much more prevalent in China than in many Western countries. Our analysis of 2011 China Health and Retirement Longitudinal Study dataset shows that around 59.6% adults aged 45 and above live with their children and around 68.2% live with grandchildren. Evidence about health implications related to living with aging parents is lacking, but much attention has been paid to grandparenting, especially in skipped-generation households. A large body of Western literature has found adverse situations of custodial grandparents in physical health (Musil et al., 2011), psychological wellbeing (Minkler et al., 2000), and financial conditions (Burnette et al., 2013; Minkler & Fuller-Thomson, 2005). In China’s context, divergent documentation exists regarding the health conditions of these grandparents, with some showing the decline of global cognitive function and episodic memory (Pan et al., 2020), while others indicating beneficial effects on self-reported health and psychological wellbeing (Chen & Liu, 2012; Silverstein et al., 2006). We need more investigation into the question of whether custodial grandparenting duties further enhance grandparents’ role fulfillment or exceed their physical and psychological capacity (and thus becoming a chronic stressor).
China’s Context: Gender and Rural/Urban Divide
The gendered nature of care provision shapes intergenerational caregiving patterns as well as caregivers’ wellbeing. In most societies, females are socialized to bear the responsibility of caring for family members and would feel guilty if they failed to conduct the commitment (Bauer & Sousa-Poza, 2015; Doress-Worters, 1994). With China’s transformation into a market-oriented economy since the late 1970s, gender essentialism has become more prevalent as a result of the market logic to naturalize women’s reproduction and household obligations at home and inferiority in the labor market (Ji et al., 2017). Therefore, the patrilineal and patriarchal family structure still endorses a highly gendered labor division ideal within households today, with males providing financial support and females caring for family members (Fan, 2003). The majority of existing literature often finds female caregivers more vulnerable (Penning & Wu, 2016) or disadvantaged (Xu, 2019) in physical and psychological health, given their more intense caregiving loads. However, from the normative perspective, it is also possible for female caregivers to acquire a higher sense of role fulfillment as it conforms to normative expectations, while male caregivers may be cast as failing to achieve masculinity ideals (Demantas & Myers, 2015; Legerski & Cornwall, 2010).
Another critical characteristic that may influence caregiving’s health implications is the prominent rural-urban divide identified by “Hukou,” a legal registration status of households. Since the establishment of the People’s Republic of China in 1949, cities have received most forms of policy inclination from the state, and therefore urban residents have been holding substantial socioeconomic advantages (McKay, 2000; Oi, 1993). According to the China Statistical Yearbook 2011, the per capita annual disposable income of urban households was more than three times that of rural ones, and around 70% of the urban adults aged 60 years and above relied on social insurances as their primary income source, while this proportion was only 10% among their rural counterparts (Cai & Cheng, 2014). Previous studies often find the rural grandparents have worse health conditions with an assumption of their vulnerability in response to the caregiving duties (Chen & Liu, 2012; Xu, 2019). Indeed, older adults who provide grandparental childcare for their migrant children are more likely to get financial support as a form of “time-for-money” reciprocity and thus have enhanced role fulfillment and decreased depressive symptoms (Cong & Silverstein, 2008).
To sum up, there remain several research gaps in the existing literature. First, more attention needs to be paid to the potential overlap of individuals’ multigenerational caregiving roles (sandwiched between childcare and old-age care for parents) and the level of care intensity, as the unexplored heterogeneities may have attributed to mixed empirical findings. Second, previous studies tend to regard female and rural caregivers as disadvantaged groups given their relative vulnerability in financial conditions and physical health, but it is possible for them to benefit more from role consistencies from the normative and cultural perspective. Third, causal inference from previous studies is limited due to selective samples or a lack of longitudinal data. To address these issues, our research comprehensively examines the caregiving patterns across generations by taking middle-aged and older adults as the pivotal generation and taking intergenerational living arrangements into account, with particular attention paid to gender and rural-urban divide. Finally, we make full use of longitudinal data by using random-effect models and, therefore, strengthen causal arguments.
Research Hypotheses
Despite the long-lasting debate surrounding the role stress hypothesis and role enhancement hypothesis and the mixed empirical evidence in Chinese and Western studies, we posit that the role enhancement hypothesis may suit China’s context better in assessing the caregivers’ wellbeing, given that the strong familism culture prioritizes family duties over one’s own needs. Intergenerational caregiving can enhance one’s sense of self-fulfillment, bring about higher social support from family members, and thus lead to higher life satisfaction. We come to the first hypothesis:
Hypothesis 1 From the normative perspective, we also reason that sandwich caregivers may benefit more from fulfilling the desired familial prospects. After all, the Chinese idiom “Si Shi Tong Tang” reflects a Confucian ideal that the four-generation family structure was once only within reach of the most privileged families. This argument leads to our Hypothesis 2:
Hypothesis 2: Life satisfaction of the sandwich caregivers caring for both parents and grandchildren is higher than that of non-caregivers and caregivers caring for either parents or grandchildren. We further decompose the caregiving patterns, using living arrangements as a proxy of care intensity. We predict that older adults caring for grandchildren in skipped-generation households have heavier involvement in caregiving activities because they are likely to take custody of the dependent grandchildren in place of the absent adult children generation. Thus, we come to Hypothesis 3, 3a, and 3b:
Hypothesis 3: Life satisfaction of caregivers varies across intergenerational living arrangements.
Hypothesis 3a
Hypothesis 3b We maintain that cultural components play an essential role in intergenerational caregiving, and, therefore, attention must be paid to gender ideologies. Given that gender essentialism still thrives in today’s China, females may acquire a higher sense of role fulfillment from caregiving duties, which leads to Hypothesis 4:
Hypothesis 4: The beneficial effect of intergenerational caregiving on life satisfaction is more pronounced among female caregivers than among their male counterparts. The rural-urban divide also contributes to disparities in caregiving’s health implications. Compared to their urban counterparts, rural residents are prominently disadvantaged in socioeconomic status and pension availability, while familial support may serve as the most critical source of later-life support. Hence, we infer that the rural residents may benefit more from the financial assistance and family support associated with care provision. This assumption leads to Hypothesis 5.
Hypothesis 5
Data and Measurement
Data is drawn from the 2011 and 2013 waves of China Health and Retirement Longitudinal Study (CHaRLS), one of the earliest longitudinal surveys in China, conducted by Peking University (China) and funded by the National Institute on Aging (the United States), World Bank, and National Natural Science Foundation of China (Zhao et al., 2013). CHaRLS is a nationally representative sample of the community-dwelling adults aged 45 and above and contains rich information about physical and mental health and work and retirement conditions. The national baseline survey was conducted across 28 provinces in 2011 and followed up every 2 years. CHaRLS adopted the four-stage stratified Probability Proportionate to Size sampling and has a baseline sample of 17,587 residents (including one “family respondent” and his/her spouse, if available, within each household) from 10,257 households.
We limit our sample to respondents aged 45–64 in 2011, a group at the highest risk of being sandwiched between the care of grandchildren and older parents across the life course, consistent with prior studies in China 1 (Falkingham et al., 2020; Xu, 2019). Besides, our sample only includes family respondents but not their spouses, given that family respondents answered all questions and acted as a proxy for their spouses to provide the caregiving and household-level information. Based on the criteria above, there were 6810 respondents in the 2011 wave and 7399 in 2013. Around 9.6 and 4.0% of these respondents were further excluded due to their adoption of proxy or assistance during interviews. We then deleted 342 observations with missing values. As a result, we included 6040 respondents of the 2011 wave and 6874 of the 2013 wave (N = 12,914 observations in total) into the final sample. Analysis of longitudinal changes in the sample size shows that 3495 respondents were repeatedly interviewed in both waves, 2545 were only interviewed in the 2011 baseline, and 3379 were newly interviewed respondents in the 2013 follow-up.
Key Independent Variable
The intergenerational caregiving patterns serve as our first set of independent variables. We define caregiving as spending at least 1 h caring for any parents (or parents-in-law) or young grandchildren under the age of 16 in the past 12 months. We divide the caregiving patterns into four categories: (1) non-caregiving, (2) parent care only, (3) grandchild care only, and (4) sandwich caregiving (caring for aging parents and young grandchildren). Figure 1 shows the proportions of each category in the 2011 baseline. Intergenerational caregivers comprise around 41.7% of all respondents, with 25.4% caring for grandchildren only, 11.5% caring for parents only, and 4.9% caring for both generations. Distribution of intergenerational caregiving patterns by living arrangements, CHaRLS 2011 baseline, N = 6040.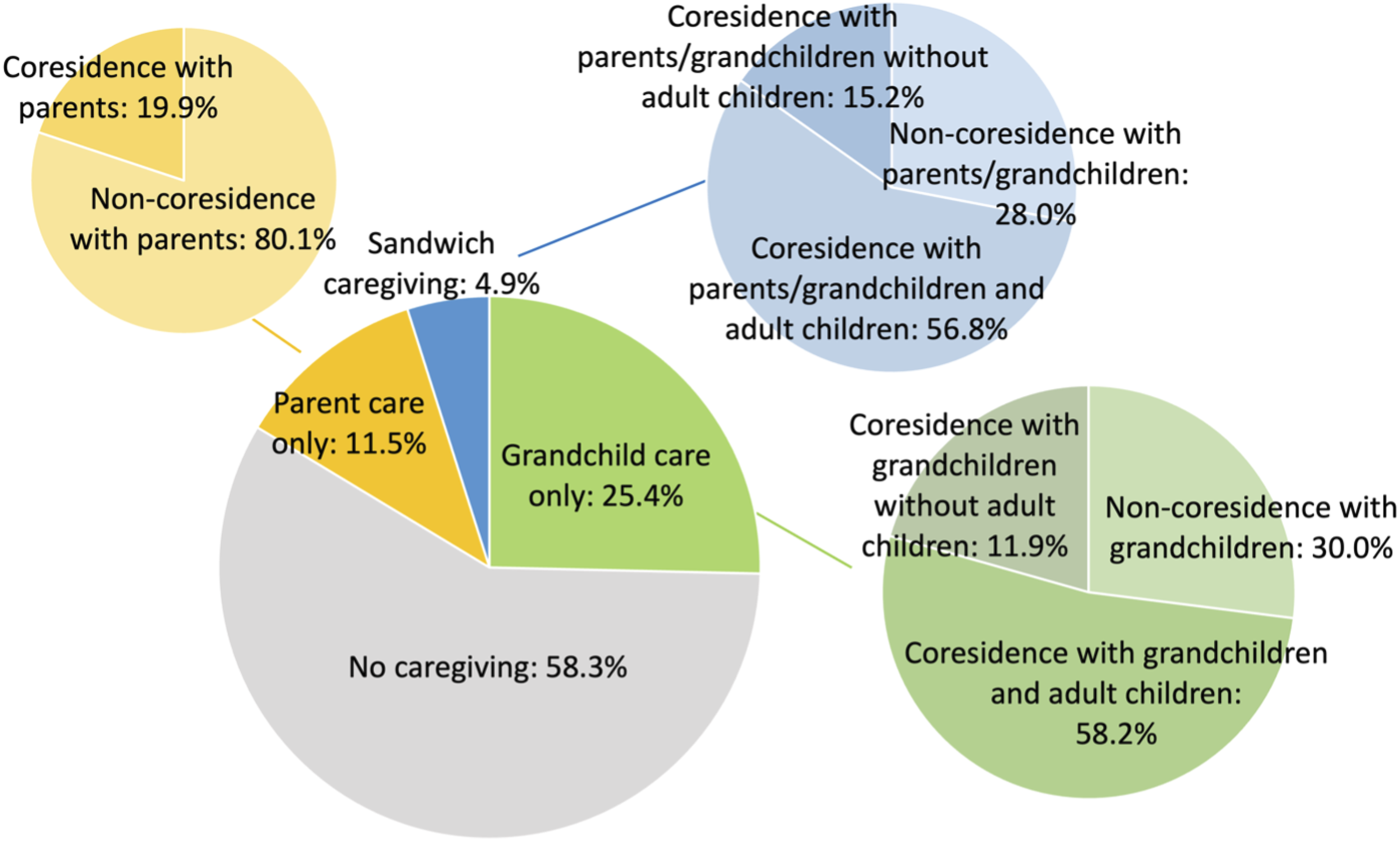
To investigate the heterogeneity in caregiving intensity, we further divide caregiving patterns by living arrangements according to whether respondents live with any parents, adult children, and grandchildren under the age of 16. Non-caregivers serve as a reference group. As shown in Figure 1, 80.1% of parent caregivers do not live with their parents. In comparison, only 30.0% of grandchild caregivers do not live with their grandchildren, 58.2% live in the same households with both grandchildren and adult children, and 11.9% in skipped-generation households. Sandwich caregivers have similar living arrangements to grandchild caregivers. More than one-half of them co-reside with their care recipients as well as the adult children generation, while 15.2% share the households with their care recipients without the adult children generation present.
Dependent Variable
Descriptive Statistics of Dependent Variable and Covariates (CHaRLS 2011 Baseline).
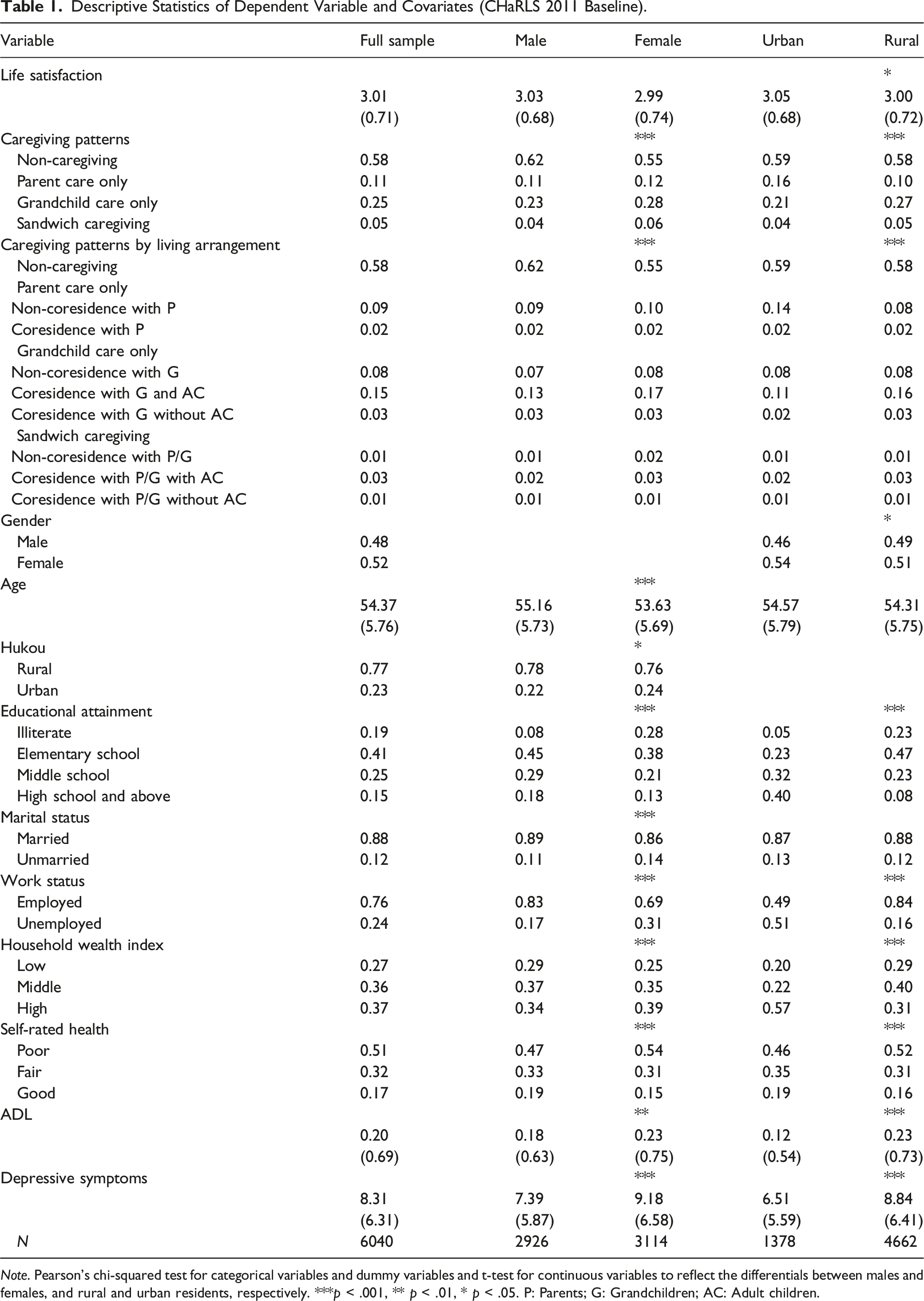
Note. Pearson’s chi-squared test for categorical variables and dummy variables and t-test for continuous variables to reflect the differentials between males and females, and rural and urban residents, respectively. ***p < .001, ** p < .01, * p < .05. P: Parents; G: Grandchildren; AC: Adult children.
Covariates
We also include covariates to control for the socio-demographic characteristics of respondents. Gender and educational attainment are time-constant, and all other covariates may have variations across waves. We adopted dummy variables to measure gender (male = 1, female = 0), Hukou (urban = 1, rural = 0), marital status (married = 1, unmarried = 0), and work status (engaged in any work = 1, no work = 0). Educational attainment includes four categories (illiterate = 0, elementary school = 1, middle school = 2, and high school and above = 3). Considering that many older adults are not in the labor market (e.g., retirees, homemakers.) or mainly rely on offspring’s financial support, we divide the household wealth index into low (= 0), middle (= 1), and high (= 2) levels to reflect financial conditions of our respondents (Elo, 2009). We also measured self-rated health, activities of daily living (ADL), and depressive symptoms to capture physical and mental health. Self-rated health is classified into poor (= 0), fair (= 1), and good (= 2) conditions. CHaRLS adopts the five-item scale to measure the difficulty performing activities of daily living, including dressing, bathing, eating, getting in/out of bed, and using the toilet. ADL in our sample reflects the number of activities with at least some difficulty, ranging from 0 to 5, with a higher score indicating higher physical disability.
CHaRLS also used the 10-item CES-D scale to capture respondents’ depressive symptoms during the week prior to interview. All respondents were asked the frequency of feeling (1) depressed, (2) everything was an effort, (3) sleeping was restless, (4) happy, (5) lonely, (6) bothered by things that do not usually bother them, (7) they could not get going, (8) having trouble keeping their mind on what they are doing, (9) hopeful about the future, and (10) fearful. Answers for each question include less than once a day (= 1), 1–2 days (= 2), 3–4 days (= 3), and 5–7 days (= 4). The depressive symptoms are indexed from the summary of these answers after adjusting the anchors to 0 to 3 and reverse coding feeling hopeful and happy. In our sample, the depressive symptoms vary from 0 to 30, with a higher value standing for a higher depressive level. Table 1 displays the descriptive statistics of life satisfaction and all covariates by gender and Hukou status in the 2011 baseline. We also conducted t-test for continuous variables and Pearson’s chi-squared test for categorical variables and dummy variables to compare the distribution of males and females, and rural and urban residents, respectively. As shown, males and urban residents both hold substantial advantages in educational attainment, work status, household wealth, self-reported health, ADL, and depressive symptoms relative to their female counterparts and rural counterparts. We did not display the distribution of the variables in 2013 wave, as they were very similar to the 2011 baseline.
Analytic Strategy
Random-effects regression is adopted to model life satisfaction. Although our dependent variable is an ordinal variable from a five-point Likert scale, we treat it as a continuous one to make the statistical analysis more interpretable while largely preserving information in the ordering. To examine the validity of this approach, we performed ordered logit models in preliminary analysis and found similar effects for the key variables, confirming the well-established argument that using ordinal data from Likert scales in parameter tests could yield unbiased results that are highly close to “the truth” (Norman, 2010; Sullivan & Artino, 2013). Moreover, given that our key predictors are not available from the 2015 wave of CHaRLS, we conducted lagged dependent models to examine how caregiving patterns in 2011 and 2013 related to respondents’ life satisfaction in 2013 and 2015. The results also turn out to be highly consistent with our current ones (results not shown). We illustrate the random-effects regression in the following equation (Wooldridge, 2016)
The dependent variable
We treat
Furthermore, we conduct separate analyses of the subsamples. We adopt the Z-test proposed by Cohen (1983) to compare the coefficients of
Discussion of Results
Random-Effects Models of Life Satisfaction, with Caregiving Patterns as Key Predictors.
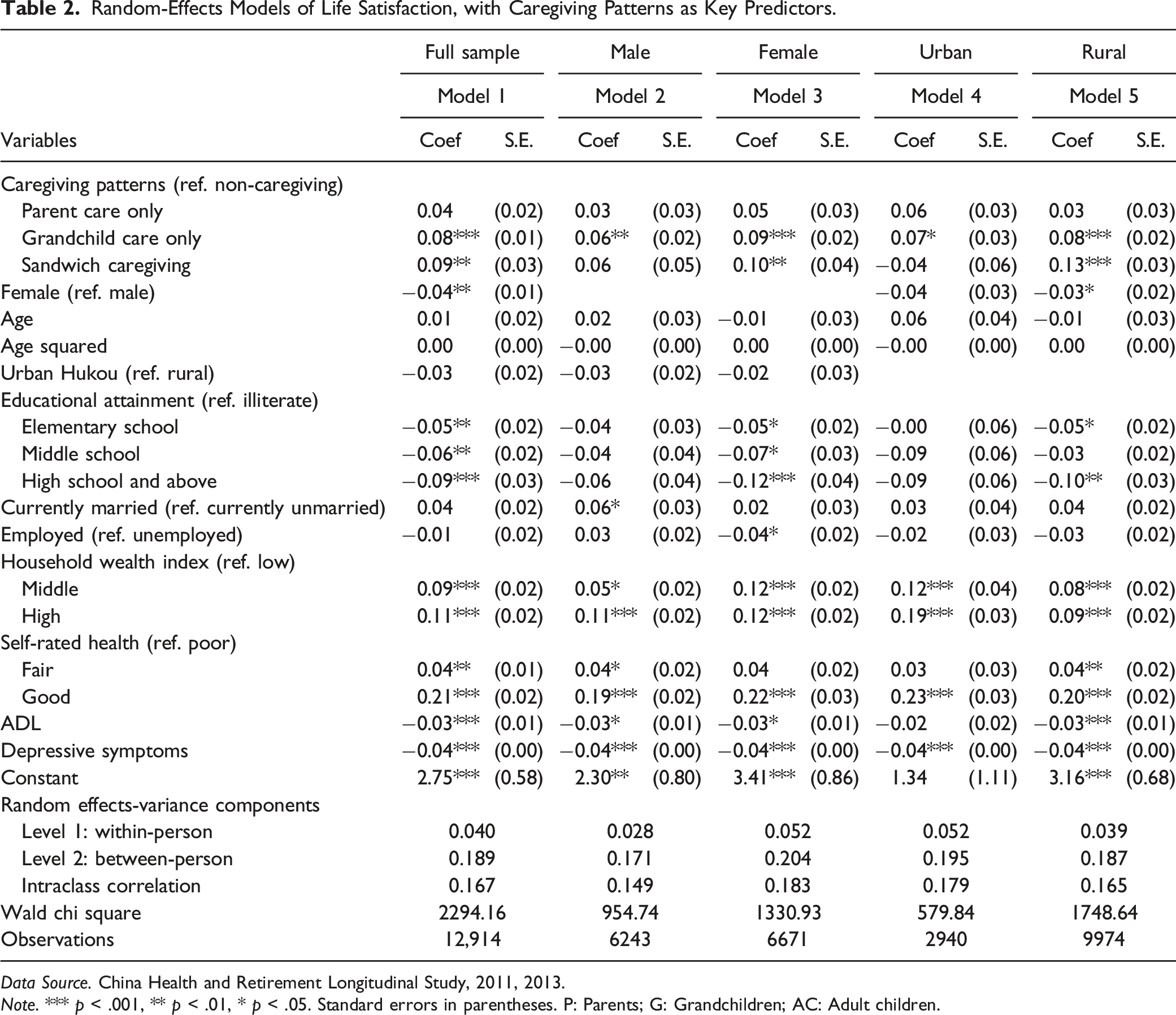
Data Source. China Health and Retirement Longitudinal Study, 2011, 2013.
Note. *** p < .001, ** p < .01, * p < .05. Standard errors in parentheses. P: Parents; G: Grandchildren; AC: Adult children.
Random-Effects Models of Life Satisfaction, With Caregiving Patterns by Living Arrangements as Key Predictors.
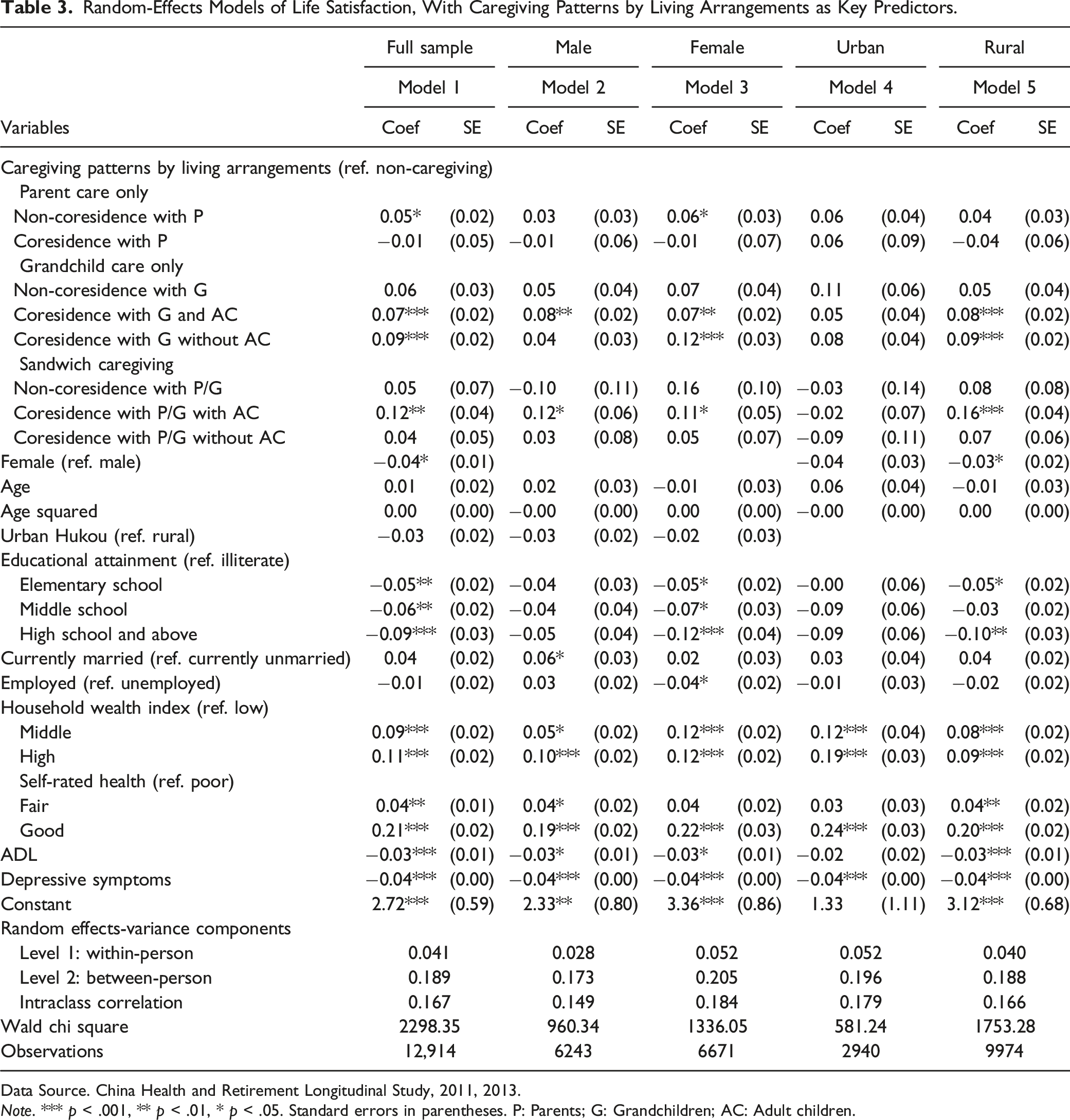
Data Source. China Health and Retirement Longitudinal Study, 2011, 2013.
Note. *** p < .001, ** p < .01, * p < .05. Standard errors in parentheses. P: Parents; G: Grandchildren; AC: Adult children.
The Effect of Caregiving Patterns on Life Satisfaction
The results for Model 1 of Table 2 partially support our Hypothesis 1. Individuals caring for grandchildren only have higher life satisfaction than the non-caregivers, but we did not find evidence showing similar advantages of caring for parents only, which is different from previous study showing the adverse impact of parent caregiving on life satisfaction among females aged 18 and 52 years (Chen et al., 2019). On the other hand, previous empirical studies lend support to our findings of the emotional rewards of caring for grandchildren only (Guo et al., 2008; L. Xu et al., 2012). As hypothesized from the normative perspective, grandparents are culturally expected to act as care providers for grandchildren, so they will experience better wellbeing and feel their lives are being meaningfully occupied when carrying out their duties.
Model 1 of Table 2 also supports Hypothesis 2. As shown, sandwich caregiving is associated with improved life satisfaction that is even higher than caring for grandchildren only. This is consistent with Xu (2019)’s finding that sandwich caregiving can translate into a higher life satisfaction for rural females. A few Western studies also suggest that sandwich caregivers may enjoy role satisfaction (Stephens et al., 1994) and receive more help with childcare and household tasks and financial and emotional support from their older parents as reciprocity (Ingersoll-Dayton et al., 2001). Although less is discussed about the underlying mechanisms in China’s context, we reason that the stronger intergenerational solidarity may yield higher role fulfillment for sandwich caregivers, and adult children may also provide more emotional and financial support given that they benefit the most from childcare assistance.
The Effect of Caregiving Patterns and Living Arrangements on Life Satisfaction
Model 1 in Table 3 partially supports Hypothesis 3 that caregivers’ life satisfaction varies across individuals’ living arrangements. When examining caregivers who care for their parents only, we find that those
By contrast, the benefits are most robust among those caring for grandchildren only. Regardless of whether living with adult children or not, grandparents who live with their grandchildren have enhanced life satisfaction. Our results also indicate that the skipped-generation arrangement does not cause deleterious effects but contributes positively to the wellbeing of grandparents. Although this finding is different from Western studies, empirical research in China’s context supports our finding and suggests that the psychological benefits of custodial grandparents could be attributed to the stronger emotional closeness and greater remittances from adult children (Cong & Silverstein, 2008; Silverstein et al., 2006). Given China’s top-ranking labor force participation rates for both young males and females, middle-aged, and older adults often retire earlier or adjust their work activities voluntarily to help the young family survive the work-family conflicts (Chen, 2004; Ji, 2017). For those with migrant children, grandchildren left to be cared for by the grandparents serve as a bridge that strongly bolsters emotional bonds between the grandparents and migrant children. Moreover, many older adults still rely on financial transfers from adult children for later-life support, and thus caring for grandchildren enables efficient time-for-money exchange, especially among rural residents who are more likely to get remittance for grandparental childcare from their migrant children (Cong & Silverstein, 2008).
The Gendered Nature and Rural-Urban Divide in Caregiving’s Effects
We find evidence supporting Hypotheses 4 and 5 from Models 2–5 of Tables 2 and 3. As shown in Models 2 and 3, females tend to benefit more from caring for grandchildren and sandwich caregiving, and the differences are statistically significant between females and males who care for grandchildren only when living with grandchildren in the skipped-generation households. It is not plausible that this female advantage may result from a lighter caregiving level, considering that Chinese grandmothers are found to spend three times as much time as grandfathers in childcare (Chen et al., 2011). Instead, we endorse a normative perspective and posit that they benefit from the consistency of their caregiver’s identities and gender roles. Indeed, males who provide grandparental childcare or sandwich caregiving also display higher life satisfaction, but it only holds when they co-reside with care recipients with the adult children present in households.
We also find prominent differentials between rural and urban residents from Models 4 and 5 of Table 2. Rural residents tend to benefit more from grandchild caregiving and sandwich caregiving, and the subgroup differentials are statistically significant in terms of sandwich caregiving. It is noteworthy that urban sandwich caregivers even have slightly lower life satisfaction than non-caregivers. With the inclusion of living arrangements in Table 3, we can see that urban residents do not show enhanced life satisfaction as their rural counterparts do, especially when it comes to sandwich caregiving. Urban residents hold less conventional social norms, so that it is understandable for them to achieve lower role fulfillment from caregiving activities. Moreover, time-for-money exchange is less meaningful for them, given their advantageous financial conditions. Besides, urban caregivers are more likely to suffer from work-family conflicts and multiple-role conflicts compared to rural residents who mostly have agricultural or informal work and much flexibility on schedule.
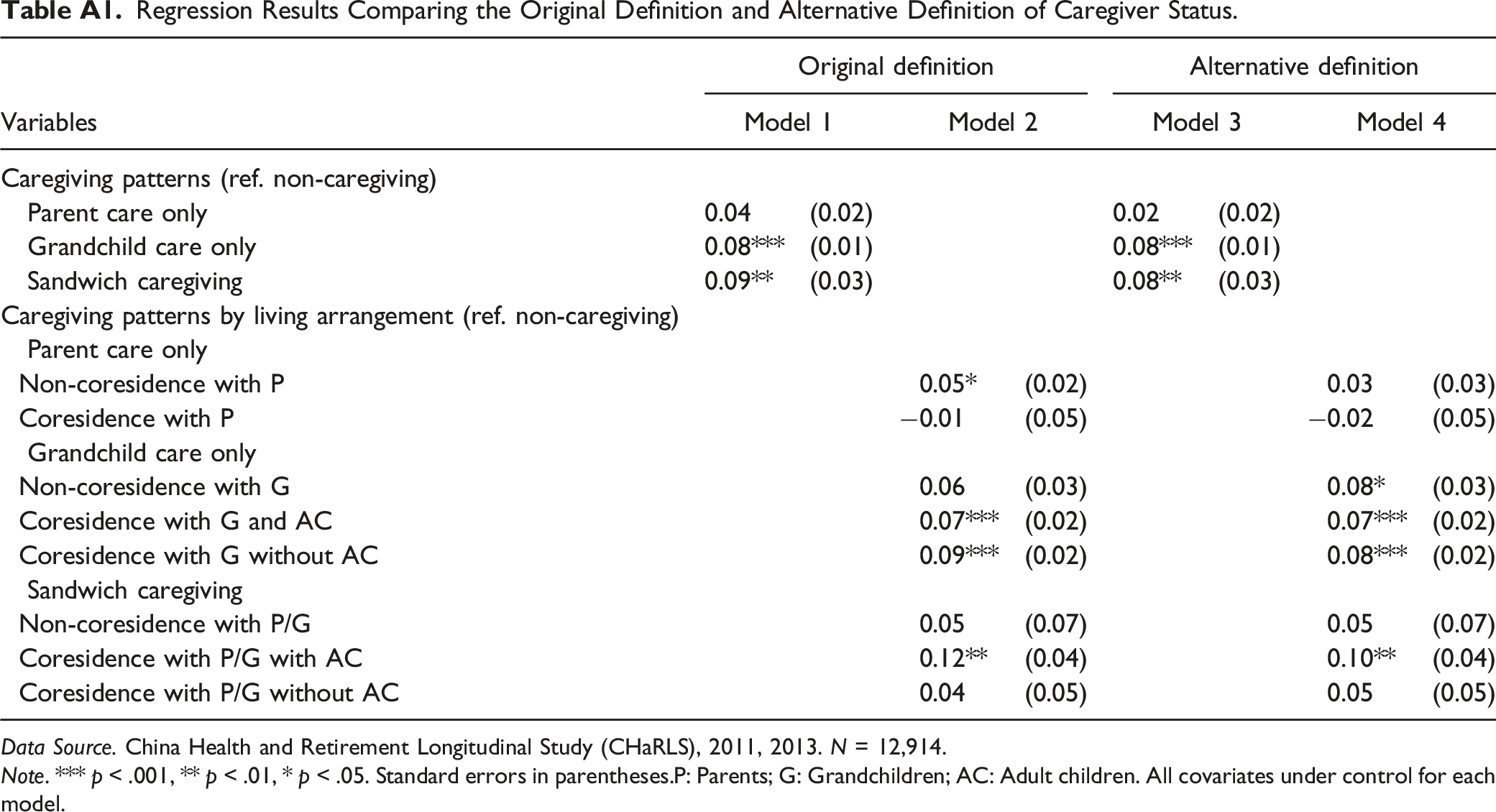
Sensitivity Analysis Using an Alternative Definition of Caregiver Status
Given that there has not been a clear consensus in the literature regarding how to define caregiver status (Bastawrous, 2013), we conducted sensitivity analysis by experimenting with a less liberal definition of family caregivers, which is providing informal care for at least 1 h per week (or 52 h per year). This alternative definition is widely adopted in Western studies. For example, Health and Retirement Study (HRS, in the same family as CHaRLS) asked respondents if they spent 100 h or more taking care of their grandchildren in the previous 2 years. This alternative definition did not change our definition of caregiver status much, as most caregivers spent more than 52 h per year on caregiving and only 4.0% of the whole sample provided 1–52 h of care. We compared two sets of regression models adopting: (1) the alternative definition (1 hour per week/52 h per year as cutoff) and (2) the original one (providing any care or not). The results turn out to be remarkably consistent (see Appendix Table A1). These sensitivity analyses give us additional confidence in the robustness of our findings.
Conclusion
Informal caregiving is an essential form of intergenerational exchange around the world. Care for aging parents or budding young grandchildren could be an expression of love, fulfill a type of culturally valued obligation, and consequently produce emotional rewards. At the same time, it could also be a stressor in mid and later life when it becomes too burdensome. Recent attention on the sandwich generation in the Western countries certainly reflects the concerns of scholars and the public alike on whether the generation caught in the middle could be overburdened as a result. Our findings clearly suggest that national contexts matter. Compared with the Western literature on caregiving, where the stress process model is often invoked, our analyses using the longitudinal CHaRLS data suggests that caregiving in general, regardless of whether it is caring for parents only, grandchildren only, or both generations, promotes the life satisfaction of middle-aged and older caregivers in China’s context. Instead of being a source of strain, caring both for grandchildren and parents turns out to be highly rewarding. The sandwich caregivers, just like the grandchild caregivers, have significantly higher life satisfaction than non-caregivers and those who care for parents only. Thus, a rising number of mid and older adults caught between the caregiving obligations of two generations does not necessarily translate into an increase in emotional and health risks.
However, it would be hugely amiss if we characterized caregiving as a uniformly positive life experience. This is far from the case. Our findings suggest that the life satisfaction benefits from caregiving vary across intergenerational living arrangements. Parent caregivers only benefit from not living with their parents, while sandwich caregivers only benefit from living with their care recipients when the adult children generation is present in households. In other words, the stress process still may very well apply when the sandwich caregivers do not receive much help from the adult children in a skipped-generation household. By contrast, grandchild caregivers who co-reside with grandchildren always show substantially higher life satisfaction, no matter the adult children generation is present or not in the households. Thus, our findings help to underscore the point that the understanding of caregiving has to be contextualized. Our findings that female caregivers and rural caregivers get a stronger boost in life satisfaction is further evidence that caregiving is not in and itself a stressor but can be seen as an expression of intergenerational support, particularly when bolstered up by a strong normative culture and family needs.
Although we did not explicitly investigate the underlying mechanisms linking caregiving and life satisfaction, our findings provide a glimpse into the family strategies individuals adopt in response to changing life circumstances. Our target population is the earliest cohort who experienced the official one-child policy since the 1980s, so the drastically decreased fertility rates elevated their perceived value of younger generations. However, the younger generations are faced with higher job uncertainty and work-family conflicts with China’s transformation into a market-oriented economy. Given that institutionalized care is still lacking and culturally stereotyped, middle-aged, and older adults choose to take over most intergenerational caregiving responsibilities on both ends. Caregivers are also more likely to receive financial assistance from younger generations, especially in the “skipped-generation households,” as a result of massive rural-to-urban migration in recent decades. This “time-for-money exchange” is especially beneficial for females and rural residents who are financially disadvantaged. Informal care provision also enhances emotional closeness across generations, and it may be an important reason why grandparents still show substantially higher life satisfaction when living in skipped-generation households. Future research should investigate further into these various mechanisms.
On another front, the cultural revolution in the late 1960s to early 1970s largely weakened filial piety that once dominated Chinese cultural norms for thousands of years. Rapid urbanization featured by the massive rural-to-urban migration of young adults further worsened the geographic separation between generations (Chen & Liu, 2009). As a result, we may expect the parent and sandwich caregivers to have worse wellbeing than non-caregivers. However, our findings suggest that the middle-aged and older Chinese do not abandon filial piety and continue to shoulder substantial familial obligations (Hermalin, 2010). They still enjoy psychological rewards caring for aging parents, although these rewards are largely dependent on intensities of care provision. Because of the varying degree of filial attitudes individuals have in a transitional society, we believe this is a fruitful area for future research, as the psychological impact of caregiving could differ significantly for those who are shouldering the responsibilities voluntarily or obligatorily.
This study is not without limitations. First, we use living arrangements as a proxy for caregiving intensity instead of the exact caregiving hours. We did so because caregiving hours are measured in a crude way in CHaRLS, and respondents often report the duration of coresidence with their care recipients as caregiving time. Second, we may not capture the full extent of caregiving responsibilities across individuals’ life course since we only have two waves of data given that the 2015 wave does not produce parent caregiving variables. Third, we only examine life satisfaction and do not include other dimensions of subjective wellbeing, such as happiness, due to data limitation. Fourth, we do not explore the underlying mechanisms between caregiving and psychological wellbeing directly. Future studies could fill this gap by investigating the buffering effects of financial support and cross-generation emotional closeness as well as caregiving-related changes in self-esteem and self-care time.
Footnotes
Acknowledgments
We thank Joan Kahn for her helpful comments in earlier drafts of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix
Regression Results Comparing the Original Definition and Alternative Definition of Caregiver Status.
| Variables | Original definition | Alternative definition | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
| Caregiving patterns (ref. non-caregiving) | ||||||||
| Parent care only | 0.04 | (0.02) | 0.02 | (0.02) | ||||
| Grandchild care only | 0.08*** | (0.01) | 0.08*** | (0.01) | ||||
| Sandwich caregiving | 0.09** | (0.03) | 0.08** | (0.03) | ||||
| Caregiving patterns by living arrangement (ref. non-caregiving) | ||||||||
| Parent care only | ||||||||
| Non-coresidence with P | 0.05* | (0.02) | 0.03 | (0.03) | ||||
| Coresidence with P | −0.01 | (0.05) | −0.02 | (0.05) | ||||
| Grandchild care only | ||||||||
| Non-coresidence with G | 0.06 | (0.03) | 0.08* | (0.03) | ||||
| Coresidence with G and AC | 0.07*** | (0.02) | 0.07*** | (0.02) | ||||
| Coresidence with G without AC | 0.09*** | (0.02) | 0.08*** | (0.02) | ||||
| Sandwich caregiving | ||||||||
| Non-coresidence with P/G | 0.05 | (0.07) | 0.05 | (0.07) | ||||
| Coresidence with P/G with AC | 0.12** | (0.04) | 0.10** | (0.04) | ||||
| Coresidence with P/G without AC | 0.04 | (0.05) | 0.05 | (0.05) | ||||
Data Source. China Health and Retirement Longitudinal Study (CHaRLS), 2011, 2013. N = 12,914.
Note. *** p < .001, ** p < .01, * p < .05. Standard errors in parentheses.P: Parents; G: Grandchildren; AC: Adult children. All covariates under control for each model.