
Abstract
This study aimed to examine whether changes in generalized trust (GT) and particularized trust (PT) predict changes in depressive symptoms (CES-D 8), and whether changes in self-rated health (SRH), family support (FS), and life satisfaction (LS) mediate the relationship between changes in the two types of trust and depressive symptoms in Chinese older adults. Structural equation modeling was employed to analyze two-wave data on 3770 participants aged 65 and over. Our results showed that in a context where GT was low and PT was high, an increase in GT was associated with more depressive symptoms, while an increase in PT was associated with fewer depressive symptoms. As such, GT cannot be viewed as protective against depression in older adults in a given context. LS partially mediated the relationship between changes in PT and depressive symptoms. The findings support psychosocial processes rather than health-problem and support pathways.
Introduction
Depressive symptoms are not only a common mental health problem in later life, but also reduce older adults’ functional capacity (Kvelde et al., 2015; Suanet et al., 2020). In China, at least 30% of adults suffer from depressive symptoms, measured by the Center for Epidemiological Studies Depression Scale (CES-D) in 2012; moreover, older people were more likely to be depressed (Qin et al., 2018). Based on social capital theory, social capital is a kind of social resource that is embedded in interpersonal networks, and can be accessed to cope with life stressed and reduce depressive symptoms (Cao et al., 2015; Nyqvist & Forsman, 2015). The role of social capital may become more important for older adults due to the loss of occupational attachment and close relationships (Nyqvist & Forsman, 2015). A longitudinal study showed that structural social capital (e.g., social participation) has no effect on the CES-D scale in Chinese middle-aged and older adults (Liu et al., 2016). In contrast to structural social capital, cognitive social capital (e.g., trust) exerts a stronger association with depression across countries (Silva et al., 2007). The cognitive component relates to individual perceptions including trust and reciprocity (Cao et al., 2015), but trust transcends the particularism of personal relationships and universalizing duties based on reciprocity (Torches & Valenzuela, 2011) and has a stronger influence on depression than reciprocity (Cao et al., 2015; Kim et al., 2012). Theoretically, trust can be divided further into two types (Sato et al., 2018): generalized trust (GT) and particularized trust (PT). The former measures trust in most people, including strangers, while the latter refers to trust in particular individuals, such as family members, neighbors, friends, and those one already knows. However, previous research into the association between the two types of trust and depression has so far remained inconclusive (Cao et al., 2015).
It is of note that despite the loss of work-based social networks and close connections, older people tend to report high levels of trust. Results from cross-country research have revealed that age is positively associated with GT (trust in others in general and strangers) and PT (trust in family members and friends) (Li & Fung, 2013). The fact that older adults are more likely to experience a more rapid decline in cognitive and physical function than younger people and thus rely more on others’ assistance may explain why they would consider others to be more trustworthy (Li & Fung, 2013). Given that the two types of trust increase according to age, but this increase is not accompanied by a reduction in symptoms of depression among older adults (Qin et al., 2018), it warrants gerontological research to explore whether all social capital has the same influence on depression in later life.
Research exploring the mechanism through which trust affects depression is not comprehensive. According to the extant literature, health problems, family support (FS), and life satisfaction (LS) may work as mediators in such a relationship (Cao et al., 2015; Jhang, 2020; Kawachi & Berkman, 2000; Sun et al., 2020), but, to our knowledge, these indirect paths have not been explored simultaneously. Identifying whether changes in generalized and particularized trust are associated with changes in the symptoms of depression, as well as how changes in two types of trust affect depression via three indirect pathways, may be useful in preventing depression in older groups. We employed data from two waves of China Family Panel Studies (CFPS) to examine the direct and indirect relationships of changes in GT and PT with changes in depression in adults aged 65 and over in China.
Trust and Depression
Results on the relationship between the two types of trust and depression remain mixed, especially in the gerontological literature. These inconsistencies regarding trust may be attributable to different research designs and social environments. On the one hand, most studies on the trust-mental health link are based on cross-sectional data. It is difficult to avoid the possibility of reverse causality in results from cross-sectional studies. For example, individual depression could reduce the possibility of interaction with family and neighbors, which might lead to a decrease in PT. A large body of cross-sectional studies conducted on samples of older adults has consistently revealed the protective effect of PT against depression (Bai et al., 2020; Lu & Peng, 2019). However, a study using three-wave data revealed that PT increased depressive symptoms in the general population in South Africa (Adjaye-Gbewonyo et al., 2018). Previous research has shown that PT is negatively related to depressive symptoms in a cross-sectional analysis, but this was not the case in the following waves (Adjaye-Gbewonyo et al., 2018). A prospective analysis revealed that low levels of GT significantly increased the odds of developing depression in the adult population (Kim et al., 2012). Nevertheless, the assumption of stability in GT is problematic due to GT changing over time (Jhang, 2020). Moreover, most studies rely on single item to measure GT or PT (Adjaye-Gbewonyo et al., 2018; Bassett & Moore, 2013; Cao et al., 2015; Pollack & Knesebeck, 2004), so they may not fully capture the nature of the two types of trust. As indicated by Berggren and Bjørnskov (2011), GT is, in essence, trust without specific information, while PT is formed by observing others’ trustworthy actions and their individual-specific data. The measurement of GT and PT should include, but is not limited to, trust toward most people and family members. Although two-item GT is not predictive of somatic symptoms and anxiety (Jhang, 2020; Yamaoka, 2008), PT, consisting of three questions, is associated with anxiety in older adults (Jhang, 2020). To deepen the understanding of the association between trust and depressive symptoms, the present study analyzed the direct and indirect effects of changes in trust by using several items.
On the other hand, the diverse relationship between trust and depression may manifest in different trust environments (Adjaye-Gbewonyo et al., 2018; Pollack & Knesebeck, 2004). Some studies have suggested that GT reduces depression in older populations in China (Cao et al., 2015), while this relationship was not observed in older people in Finland (Forsman et al., 2012). PT (trust in neighbors) is negatively related to depression in older adults in the United States (US), but this relationship was not observed in Germany (Pollack & Knesebeck, 2004). Pollack and Knesebeck (2004) argue that higher PT in the US than in Germany may explain the difference. A longitudinal study conducted in South Africa revealed an unexpected finding, namely that GT and PT increase depressive symptoms measured by short-form CES-D (Adjaye-Gbewonyo et al., 2018). The study suggested that individuals who trusted others blindly in a society where overall trust was low may find themselves being taken advantage of and thus feel depressed. However, as district-level PT increased, people with high PT reported improvements in their depressive symptoms. As such, the function of trust may be contingent on external environments to which individuals are exposed. China presents an interesting profile for examining the issue because Chinese score higher on GT than those in many countries, including South Africa (Bjørnskov, 2006), despite a declining trend in GT recently found in China (Hu, 2015). As a cross-country comparative study showed that Chinese are characterized as having relatively higher PT than GT (Li & Fung, 2013), we expect that an increase in GT and PT would be associated with a decrease in symptoms of depression among older adults in a context where both GT and PT are high (Hypothesis 1).
Three Pathways from Trust to Depression
Although there are three mechanisms through which neighborhood-level social capital affects health reported in the literature, i.e. health-related behaviors, access to support and services, and psychosocial processes (Kawachi & Berkman, 2000), these pathways cannot be fully applied to individual-level trust. Given the weak or non-significant associations between health behavior variables and depressive symptoms in older Chinese adults (Sun et al., 2020), the health behavior pathway is replaced with the health problem pathway. The first perspective on the health problem pathway argues that older adults do not have the capacity to deal with health problems, which increases their somatic symptoms of depression (Dao-Tran et al., 2017). High-trusters may trust in health information and use information to address these problems. Self-rated health (SRH) is usually considered as a proxy for health problems, because SRH not only reflects objective health conditions in China (Wu et al., 2013), but also predicts depressive symptoms among older adults (Jang et al., 2021). Compared to GT, PT shows a consistently positive relationship with SRH in older adults, regardless of research design (Glanville & Story, 2018; Jhang, 2020; Sato et al., 2018). This indicates that the health information a high-truster receives from those familiar people is more likely to meet their needs and thus benefit their health status. Good SRH has been linked to low levels of depression in longitudinal studies (Han & Jylha, 2006; Fernández et al., 2016). Changes in PT rather than GT are found to influence changes in anxiety through changes in SRH in older Chinese adults (Jhang, 2020), but the indirect effects on depression of the two types of trust via SRH are not yet available in the literature. According to the mechanisms discussed, the mediating effect of SRH on the relationship between PT and depressive symptoms could be more prominent in this study.
The second perspective on the social support pathway highlights that high-trusters are more likely to receive instrumental and emotional support when dealing with life stressors (Cao et al., 2015). A cross-sectional study found that high GT reduces depression among older people through social support (Cao et al., 2015), but the social support received, including emotional and instrumental support, is not related to the initial levels and growth rates of depressive symptoms of older adults in a latent growth curve model. Given that FS has a greater influence on depression in older adults in Asia than in their counterparts in Western countries (Tengku Mohd et al., 2019), this study tested the mediating role of FS. Older adults who lack FS are more likely to have depression than those with support (Bincy et al., 2021). Research conducted in rural China found that receiving monetary support from children exerts a comparable beneficial influence on depression in older parents, but downward monetary support to children is positively related to symptoms of depression among specific older groups. Similarly, FS has a direct association with older adults’ depression and exerts moderating effects in counteracting stress from the medical domain in urban China (Sun, 2004). As trust resides mainly in families and a narrower circle of social networks in Chinese societies (Fukuyama, 2001), individuals with high PT may be more likely to receive FS than those with high GT. Therefore, the relationship between PT and depression, and not between GT and depression, may be mediated by FS.
The final perspective on the psychosocial processes posits that trust increases positive psychological status, which in turn ameliorates depressive symptoms (Sun et al., 2020). This pathway from the development and maintenance of social relationships, positive psychological status, and mental health has been identified in a theoretically integrated model (Kawachi & Berkman, 2001). The positive psychological states that are affected by integration with social ties benefit mental health due to increased motivation for self-care and modulation of the neuroendocrine reaction to stress. High levels of trust reflect to some extent the high-quality social relationships that are crucial components of LS. PT is predictive of LS in older Chinese people (Pan, 2018). Trust in known others (PT) has been widely theorized to contribute to individual well-being (Glanville & Story, 2018), but empirical studies usually do not differentiate between PT and GT. One study constructed a trust index (GT plus PT) to assess the relationship between trust, LS and depression in Chinese older adults (Sun et al., 2020). Another study examined the link between trust in the community and LS by constructing this trust score to include PT (e.g., trust toward people in your neighborhood, known others) and GT (e.g., trust toward other citizens of your country, unknown others; Zhang, 2020). In terms of the relationship between LS and depression, low LS as a step toward depression has been well-documented in longitudinal studies (Fernández et al., 2016; Lue et al., 2010). Recent research has uncovered the reciprocal relationship between LS and depressive symptoms among Chinese older married couples (Guo, 2020). However, it remains unknown whether GT and PT are linked to depression through LS. Taken together, PT seems to be more closely related than GT to mediators based on the extant literature. We hypothesize that changes in SRH, FS, and LS mediate the relationship between changes in PT and depressive symptoms rather than the relationship between changes in GT and depressive symptoms among older people (Hypothesis 2).
Methods
Sample
This study used data from CFPS, a nationally representative sample of people aged 16 years and older. The CFPS adopted a stratified three-stage probability random sampling method to collect information (Xie & Hu, 2014). The survey was launched in 2010, but the present study focused primarily on data regarding the CES-D collected in two later waves: 2012 (T1) and 2016 (T2). The total number of adults aged 16 years and over in 2012 and 2016 were 35,720 and 36,892, respectively. At T1 (overall response rate 74.1%), data were selected from a sample of 4615 adults aged 65 years or above; at T2, data were available for 3770 of these 4615 respondents, yielding an acceptable attrition rate of 18.3%. The missing rates for key items measuring depressive symptoms, LS, and the two types of trust ranged from 3% to 15% in 2012. This study used an expectation-maximization algorithm to impute these missing values via SPSS 22.0 because of its more accurate estimates than those using conventional methods under the assumption that the data were missing at random (Allison, 2009). CFPS was approved by the research ethics committee of Institute of Social Science Survey (ISSS) in Peking University and managed by ISSS. Written informed consent was obtained from all participants.
Measures
Dependent variable
This study used the eight-item CES-D, a valid and reliable instrument (Karim et al., 2015) to assess depressive symptoms. The response options ranged from zero (“rarely or none of the time”) to three (“most or all of the time”). Items that described positive affect were reverse coded. The alpha coefficients for the short-form scale were 0.77 in 2012 and 0.82 in 2016. Higher scores on the CES-D 8 denoted more depressive symptoms. The changes in depressive symptoms were calculated by subtracting the T1 scale of depression from that of the T2 scale.
Independent variable
Trust scale consisted of a total of six items that assessed the extent to which individual trust in others, such as Americans, strangers, parents, neighbors, officials in local governments and doctors, based on the literature (Berggren & Bjørnskov, 2011; Zhang, 2020). Response options ranged from 0 (“very distrustful”) to 10 (“very trustful”). Confirmatory factor analysis revealed that the two-factor model of trust fitted the data better than did the one-factor model in 2012 (χ2 = 166.89, df = 7, goodness of fit index (GFI) = 0.98, root mean square error of the approximation (RMSEA) = 0.08, χ2 difference (df = 1) = 194.23, p < 0.01) and in 2016 (χ2 = 116.62, df = 7, GFI = 0.99, RMSEA = 0.06, χ2 difference (df = 1) = 791.87, p < 0.01). The value of GFI was above 0.90 and that of RMSEA below 0.08 for a model that fitted the data well. The former two items were labeled as GT, while the latter four items were viewed as PT. The reliability of the subscale ranged from 0.62 to 0.68. The changes in GT and PT were calculated by subtracting the T1 subscale of trust scores from those of the T2 subscale.
Mediators
SRH was assessed by asking respondents how they felt about their current health. Responses ranged from 1 (“excellent”) to 5 (“very poor”). Changes in SRH were measured in the same way as changes in trust. Higher scores on changes in SRH represented a deterioration in SRH. Treating the ordinal variable as continuous is defensible based on the investigation of validity, reliability, and measurement invariance (Robitzsch, 2020).
FS measured whether respondents received monetary support and household assistance from adult children (Lin & Yi, 2011). Response options ranged from 0 (“no”) to 1 (“yes”). The measurement of FS was limited to the first three children because the vast majority of respondents did not have four children due to the national policy involving specific birth quotas formulated in 1970s in China. Respondents received scores of 3 as they received help from three children. Changes in FS were measured in the same way as changes in trust. When changes in FS contained more than six categories, structural equation modeling (SEM) produced coefficients within the range of acceptable bias as robust categorical least squares method did (Rhemtulla et al., 2012). Higher scores on changes in FS denoted an increase in support from adult children.
LS was measured by asking respondents how satisfied they were with their present life. Response on a 5-point Likert scale ranging from 1 (“very dissatisfied”) to 5 (“very satisfied”). Changes in LS were measured in the same way as changes in trust. Higher scores on changes in LS represented an improvement in LS. Single-item LS represents a valid instrument for the estimation of the average change in LS as multi-item scales (Gnambs & Buntins, 2017).
Covariates
Covariates included gender, age, household monthly income, education, marital status, chronic disease and social participation. Age was measured as chronological years. A square root transformation was applied to household monthly income to reduce right skewness. Education was dichotomized as junior high school or less and senior high school and above. Marital status was divided into two types: unmarried and married. Chronic disease measured whether the respondents reported that they had been diagnosed with any chronic diseases in the past six months (0 for “none” and 1 for “at least one disease”). Social participation was divided into two types; 0 for not a member of any groups and 1 for group membership. Most covariates were dichotomized to simplify the models.
Data analysis
Path analysis based on SEM with AMOS 22.0 assessed the relationship between changes in trust, mediators and depressive symptoms. Correlated residuals between household monthly income and education, between age and marital status, and between LS and SRH were established, based on strong relationships found in the previous literature (Chen & Li, 2020; Fernández et al., 2016; Kim, 2013). In the structural model, there were four equations. Equation (1) was changes in GT (X1) and PT (X2), changes in mediators such as SRH (M1), FS (M2), and LS (M3) for changes in depressive symptoms (Y) of the regression equation, including control variables. The other three equations were changes in GT and PT for changes in three mediators of the regression equations. There were six indirect effects that were the products of the effects of two types of trust on mediators and the effects of three mediators on depressive symptoms via the bootstrap method in AMOS.
Results
Overview of the Characteristics of the Chinese Older Sample (N=3770).
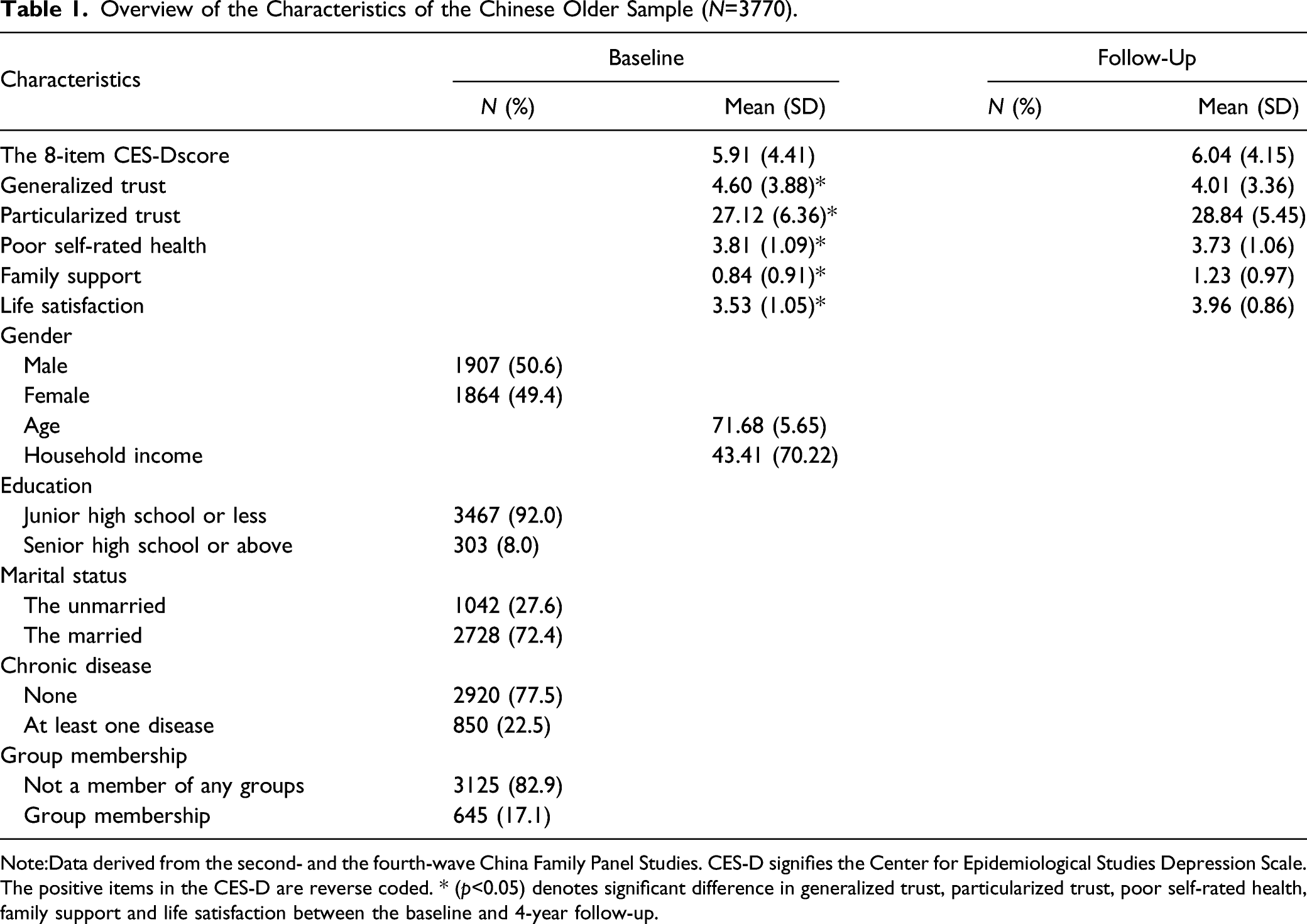
Note:Data derived from the second- and the fourth-wave China Family Panel Studies. CES-D signifies the Center for Epidemiological Studies Depression Scale. The positive items in the CES-D are reverse coded. * (p<0.05) denotes significant difference in generalized trust, particularized trust, poor self-rated health, family support and life satisfaction between the baseline and 4-year follow-up.
Bivariate Correlation Between Main Variables.
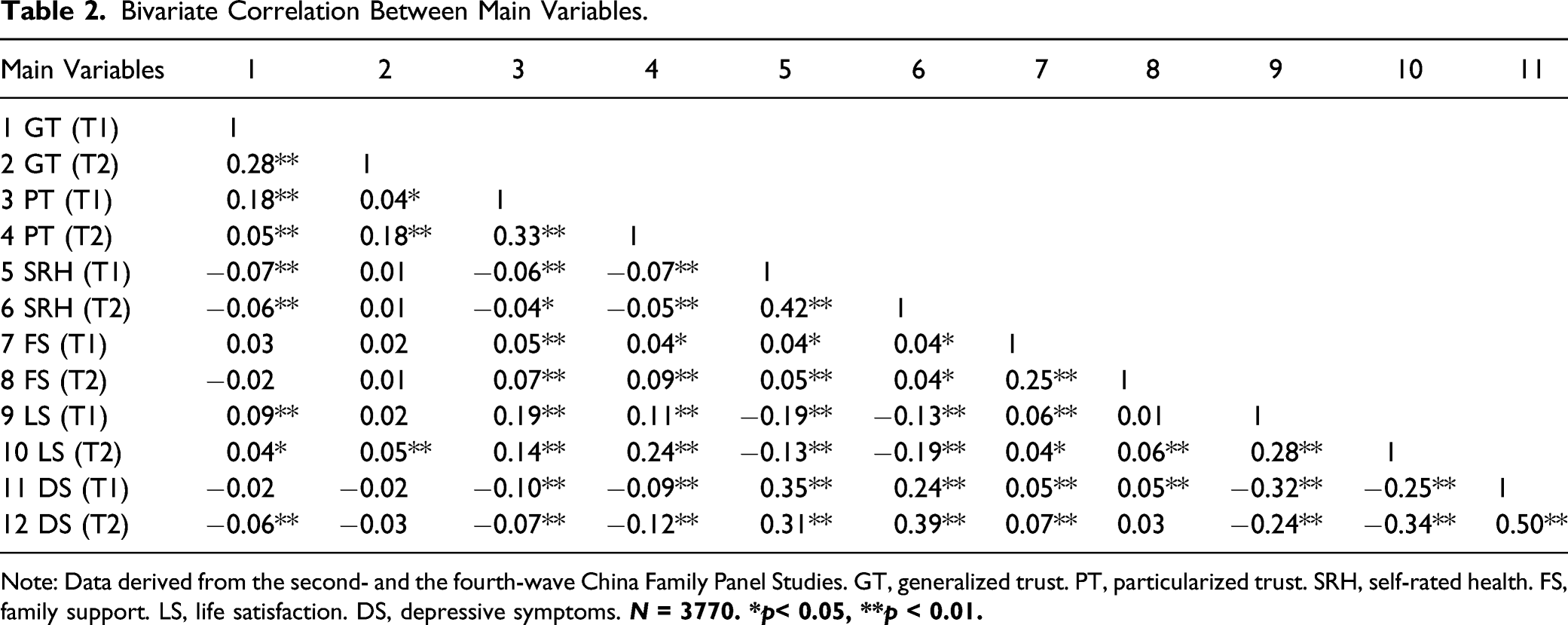
Note: Data derived from the second- and the fourth-wave China Family Panel Studies. GT, generalized trust. PT, particularized trust. SRH, self-rated health. FS, family support. LS, life satisfaction. DS, depressive symptoms.
Standardized Coefficients for Direct Relations in Structural Equation Model ofChanges inDepressive symptoms (CES-D 8).
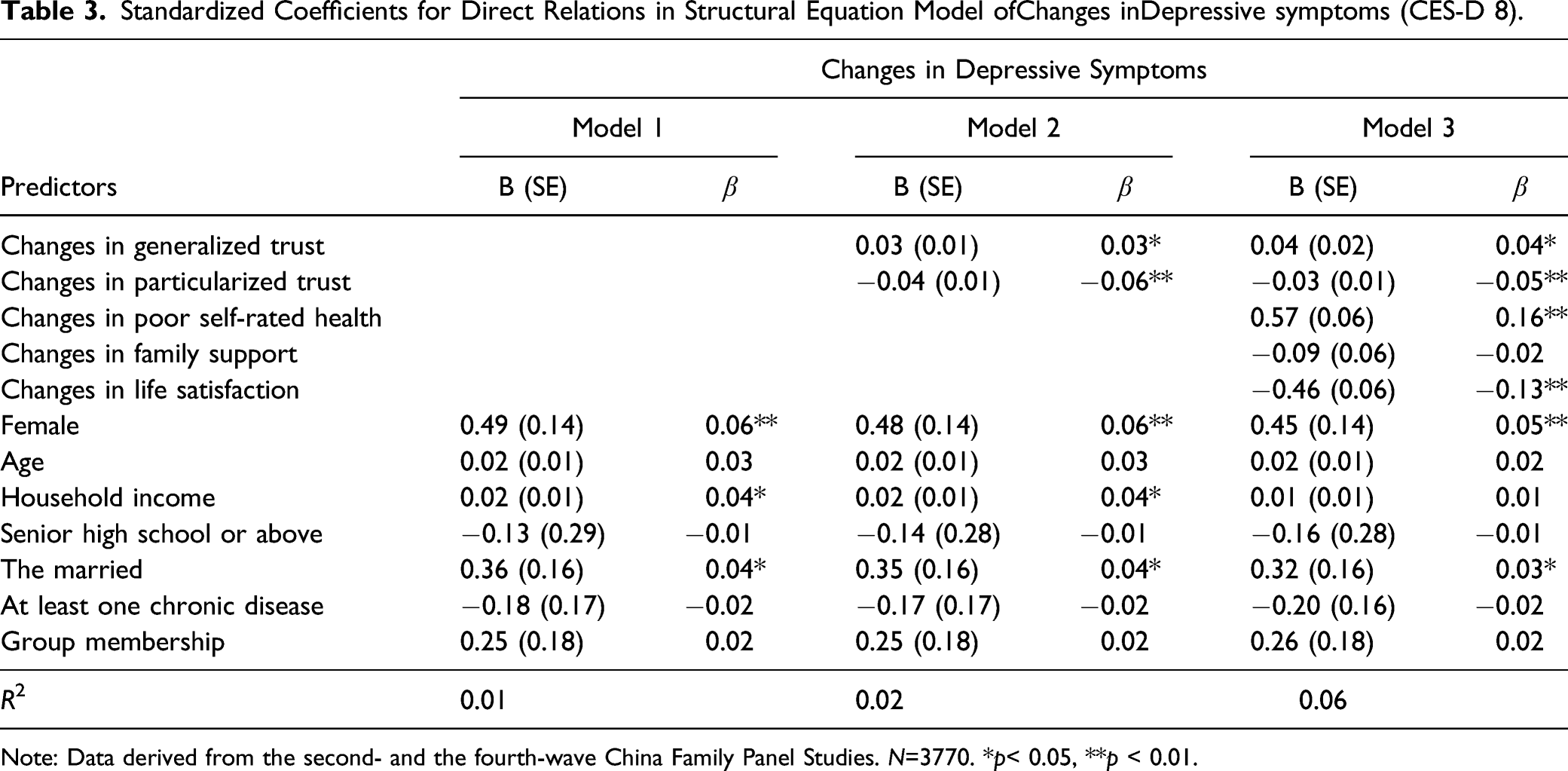
Note: Data derived from the second- and the fourth-wave China Family Panel Studies. N=3770. *p< 0.05, **p < 0.01.
Standardized Coefficients for Indirect Effects in Structural Equation Model ofChanges inDepressive Symptoms (CES-D 8).
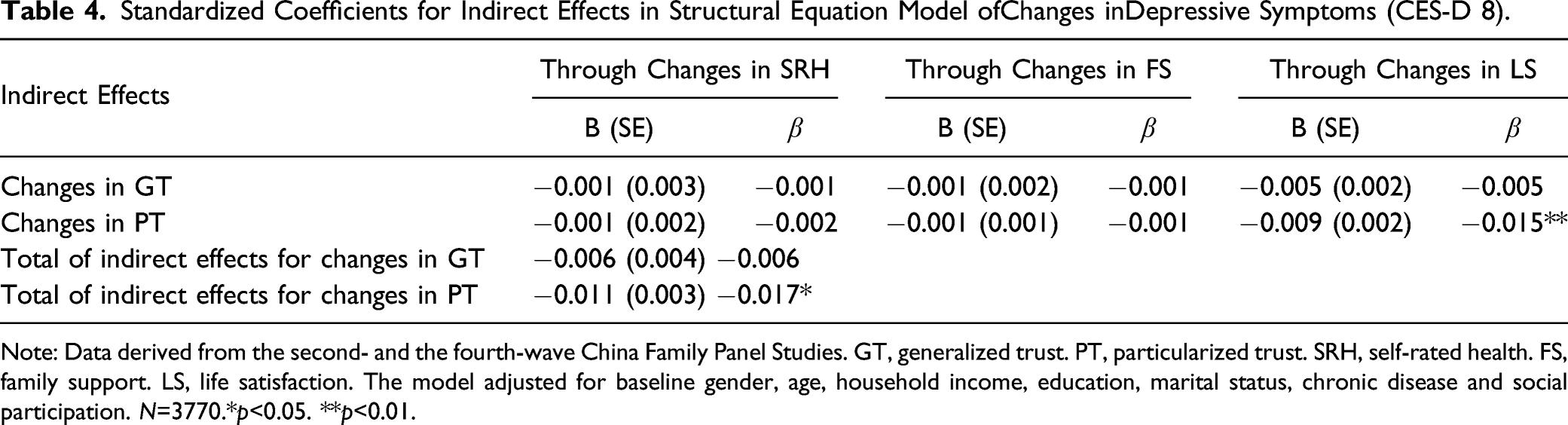
Note: Data derived from the second- and the fourth-wave China Family Panel Studies. GT, generalized trust. PT, particularized trust. SRH, self-rated health. FS, family support. LS, life satisfaction. The model adjusted for baseline gender, age, household income, education, marital status, chronic disease and social participation. N=3770.*p<0.05. **p<0.01.
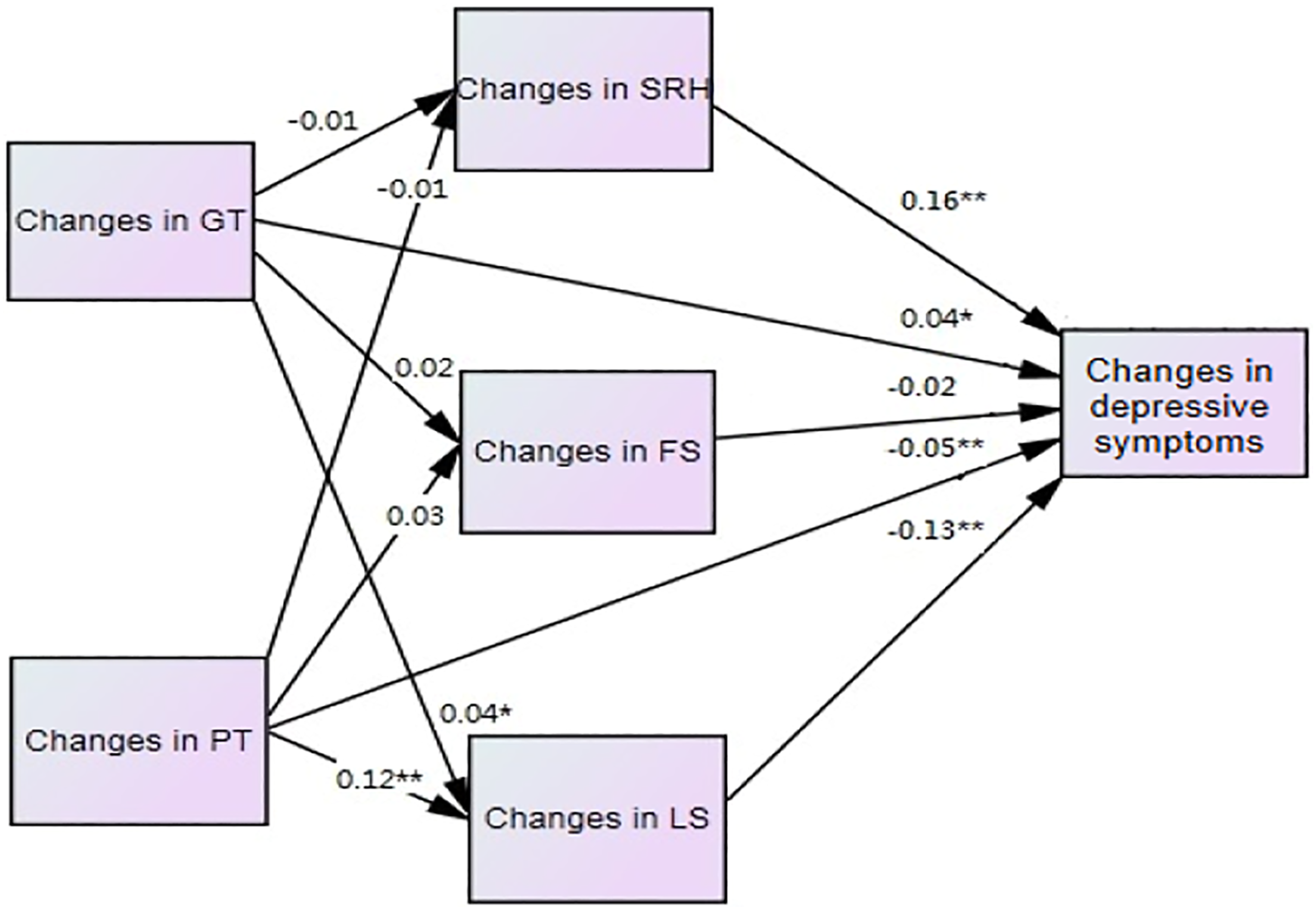
The standardized coefficients between changes in trust, SRH, FS, LS and depressive symptoms for the path model. Note: GT=generalized trust. PT=particularized trust. SRH=self-rated health. FS=family support. LS=life satisfaction. Seven control variables at baseline are included in the model. Model fit: GFI =0.95, RMSEA =0.07. *p< 0.05, **p < 0.01.
In addition, this study checked whether the results were robust. The dependent variable at T2 (CES-D-8 summed scores), rather than changes in depression, was examined in the alternative model after adjusting for a dependent outcome at T1. The effect on depression at T2 can be interpreted as the effect on change in mental health (Idstad et al., 2011). The results from the alternative model remained unchanged. The findings showed that increased levels of GT were associated with an increase in depression (β = 0.04, p < 0.05, results not shown), whereas an increase in PT was associated with a decrease in depression (β = −0.04, p < 0.05, results not shown). The mediation effects of changes in LS remained significant (β = −0.01, p < 0.01, results not shown).
Discussion
Using nationally representative panel data, this study aimed to analyze the direct effects of changes in GT and PT on depressive symptoms as well as their indirect effects through changes in SRH, FS and LS in old age in China. Contrary to our expectations, older Chinese people tend to distrust those they do not know, which aligns with previous research (Hu, 2015; Jhang, 2020). Low GT and high PT shown in China reflect a still-strong inheritance of differentiated order from traditional Chinese societies where socially related people are viewed as differentiated in terms of their closeness to the individual (Fei, 1992). The results coincide with the previous findings demonstrating that trust in foreigners and strangers is much lower than trust in family and neighbors in Chinese-centered societies like Taiwan and Hong Kong, while this is not the case in Australia (Ward et al., 2014). The principle of differentiation laid the groundwork for the development of different trusting relationships in Chinese societies.
We found an increase in GT to be associated with an increase in symptoms of depression in a context characterized as low-GT. The result of this study differs from that of previous research which emphasizes the protective role of GT for adults and older adults (Cao et al., 2015; Kim et al., 2012). Yet this study corroborates the longitudinal study that indicated the negative consequence of GT in a similar society with low GT (Adjaye-Gbewonyo et al., 2018). When exploring correlations between variables, this study reveals that correlation between GT at T1 and depression at T2 is negative, which seems to support these results from a prospective design. Taking the dynamic nature of GT into account, its benefits disappear. Older adults with improved GT in a society with low levels of GT may be taken advantage of by others and thus feel depressed (Adjaye-Gbewonyo et al., 2018).
The protective role of PT in reducing older people’s depression is in line with existing research (Bai et al., 2020; Lu & Peng, 2019), but is different from results of previous research that identified the negative influence of individual PT (Adjaye-Gbewonyo et al., 2018). As found by the previous study, individuals with high PT showed better mental health when district-level PT was high. This study extends the scope of previous findings from districts to the whole society where PT is high and where the protective role of PT is supported. We find partial support for Hypothesis 1. An increase in GT is related to more symptoms of depression, whereas an increase in PT is associated with fewer symptoms of depression. The distinct trust environments may result in inconsistent results related to individual-level trust.
Although, based on the literature, trust may affect older adults' depressive symptoms through three pathways, this study identified only an indirect pathway: an increase in PT affects depression through an increase in LS, which lends support to the psychosocial pathway. Hypothesis 2 is thus partially supported by the data. No direct association between changes in GT and SRH was observed in this study, which does not support the beneficial effect of GT on SRH found in other studies (Glanville & Story, 2018; Sato et al., 2018). We found negative correlations between GT at T1 and SRH at T1 and T2, which is similar to previous results (Glanville & Story, 2018; Sato et al., 2018). As stated above, previous research that assumes constant GT may bias results. Changes in PT also showed no relationship with changes in SRH, which is not in alignment with one previous study (Jhang, 2020). Different methods of measurement of changes in SRH may have contributed to the difference. The prior work that measured changes in SRH in a nonlinear way found only one type of change in PT that was linked to SRH in a stable and good condition. As such, when measuring changes in SRH in a linear way, changes in PT do not show significant associations with SRH. With regard to the association between SRH and depression, SRH′ s impact in this study was stronger than that in the previous study (Fernández et al., 2016) according to standardized coefficients. This study adds evidence to the health literature (Han & Jylha, 2006; Fernández et al., 2016) by showing that the deterioration in SRH is associated with the increased symptoms of depression in older groups in a non-Western country.
Contrary to our expectations, no relationship was found between changes in PT and FS. The limited range of PT and FS measured may account for this non-significant relationship. FS measurements that do not include spousal support may attenuate this relationship. PT that does not measure respondents’ trust toward their spouses and children may also weaken this relationship. Another possibility lies in the inclusion of changes in GT. Once changes in GT were excluded from the original model, the association between changes in PT and FS became significant, which suggests that it is essential to include the two types of trust in the model. Different from the cross-sectional literature (Guo & Buntins, 2017; Sun, 2004), FS does not play a crucial role in reducing depression among older adults in this study. Likewise, the results from cross-sectional research may overemphasize the importance of FS. The long-term effect of FS warrants further investigation in the future.
A previous study that measured trust without differentiating between GT and PT may have overestimated the mediation effect of LS (Sun et al., 2020). Our results show that changes in LS do not fully mediate the relationship between changes in PT and depression. Similar to other findings (Zhang, 2020), improvements in GT and PT are related to an increase in LS. The result that an increase in LS is associated with fewer depressive symptoms echoes the findings of other longitudinal studies (Fernández et al., 2016; Guo, 2020; Lue et al., 2010). The influence of changes in LS on depressive symptoms is similar to that on depressed mood in the prospective research (Fernández et al., 2016).
This study contributes to the development of social capital theory by advancing the understanding of different trust outcomes, contingent on different research designs and trust environments, and by examining three indirect paths that link trust to depression in older people. GT has been viewed as beneficial for older adults’ health. The results adds evidence to the field (Portes, 1998), suggesting an exploration of the negative effect of some social capital. Perhaps the negative effect of GT is reversed in an environment with high GT, as are the health benefits of PT in a context of high PT. The argument that the relationship between trust and depression depends on external trust environments warrants further investigation. Our findings suggest that the positive effect of GT on SRH and depressive symptoms should not be overstated, and that those of PT, SRH and LS on alleviating depression should not be ignored. Social isolation prevention programs (Saito et al., 2012), which facilitate the formation of interpersonal networks and promote social support from close friends, may be effective in increasing the levels of the two types of trust and mental health in older Chinese adults. Besides, policies aiming to reduce depressive symptoms in Chinese older people should consider the importance of SFH and LS in the face of rapid population aging in the near future.
This study has several limitations. First, the findings concerning trust cannot infer causality. However, these findings provide guidance for future researchers in the fields of social capital and health. Second, this study used an eight-item scale to assess depression. To obtain a more comprehensive assessment, future work that utilizes the full-scale CES-D is needed. Third, some of the drawbacks of SEM were that it obscured the sequential ignorability and conventional exogeneity assumption and could not be directly applied to nonlinear models (Imai et al., 2011). A sensitivity analysis to check the sequential ignorability assumption, the use of the instrumental variables method and the nonparametric identification results can be viewed as alternative methods to address these issues. Fourth, the benefit of PT may be underestimated because trust in important others such as children and spouses is not included in CFPS. However, in our assessment, no other data in China can better provide the needed information for this study. Furthermore, to confirm the influence of the social trust environment, future researchers should examine whether the same results are seen in countries that have low GT but high PT. Finally, spousal depressive symptoms are predictive of respondents’ depressive symptoms in a cross-lagged panel model (Guo, 2020). Failure to include spousal mental illness might affect the estimates of the effects of GT and PT in a longitudinal study.
In conclusion, the results reveal that PT is more beneficial than GT in reducing the depressive symptoms of older Chinese adults in the society where PT is high. The detrimental effect of GT manifests in a context of low GT. As such, GT cannot be viewed as a factor protecting against depression in older adults in a given context. We suggest that different research designs and trust environments may explain some inconsistencies regarding individual-level trust. Additional research to support the argument is needed. Changes in LS, rather than in SRH and FS, partially mediate the relationship between changes in PT and depression in old age. The indirect effect of PT on depression acts mainly through psychosocial processes rather than through the health-problem and support pathways.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
China Family Panel Studies was reviewed and approved by the Institute of Social Science Survey of Peking University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants in the study.