
Abstract
Spousal loss is a major life event with profound mental health implications. Despite abundant research on the psychological well-being of widows, most studies rely on post-bereavement data, risking recall bias. Therefore, this study analysed data from the National Survey of the Japanese Elderly to enhance our understanding of the bereavement process. We observed the levels and trajectories of depressive symptoms before, during, and after spousal loss using the first seven waves of the survey from 1987 to 2006. The results showed a modest increase in symptoms prior to loss and a significant spike at bereavement, with no subsequent decline. Participants’ age at loss moderated recovery, with later life bereavement being associated with quicker adjustment. These findings highlight the need to address mental health deterioration in later life and indicate age-related resilience with increasing age globally.
Introduction
Bereavement—the loss of a close other—is one of the most distressing events in life (Stroebe et al., 2007). The impact of bereavement has been explored since the 1940s (Lindemann, 1944). Its effects on longevity (see Shor et al., 2012; Stroebe et al., 2007 for reviews), physical and physiological health (see Ennis & Majid, 2021 for reviews), functional impairment (Song & Kim, 2023), daily routines and health behaviours (Stahl & Schulz, 2014), loneliness (Szabo et al., 2020), and psychological health (see Stroebe et al., 2007 for reviews) are well documented. In fact, major psychological disruptions following bereavement are so common that they are expected and normalised. The DIagnostic Statistical Manual of Mental Disorders explicitly states that the “response to a common stressor or loss, such as the death of a loved one, is not considered a mental disorder” (American Psychiatric Association, 2013).
This study aims to revisit the effects of spousal loss on the mental health of bereaved individuals and the potential buffers with a particular focus on demographic factors using data from Japanese older adults. The contributions of this study include the application of an econometric approach to control for unobserved time-invariant heterogeneity and the extension of existing findings to an East Asian context, as most prior evidence has been drawn from the Western populations. Although there has been a recent accumulation of evidence from Asia, particularly China (Chen et al., 2020; Jiao et al., 2024; Yang & Gu, 2021), evidence from non-Western contexts remains relatively scarce. In the following sections, we summarise previous findings, relevant theories, and mechanisms underlying the relationship between spousal bereavement and mental health.
Spousal Loss and Health: Potential Mechanisms
As attachment theory suggests, the loss of an attachment figure, such as one’s spouse, can trigger severe psychological reactions (Bowlby, 1980). In addition to negative effects of the loss itself, it also entails several complex practical changes for the bereaved. According to social production function theory, marriage is an important source of health and well-being, enabling spouses not only to gain emotional benefits and behavioural confirmation but also to access resources that foster stimulation, behavioural confirmation, affection, and comfort (Ormel et al., 1999). Consequently, spousal loss disrupts access to such resources. First, a spouse often represents one of the strongest social ties; losing one’s spouse can lead to diminished social relationships, resulting in loneliness and social isolation (Freak-Poli et al., 2022; Niino et al., 2025; Okabayashi et al., 2004; Schmitz, 2021). Conversely, it may increase interactions with children, friends, and neighbours in response to the loss (Freak-Poli et al., 2022), which can help moderate the negative impacts of bereavement. Second, the surviving partner is often expected to take on roles previously fulfilled by the deceased (e.g. household chores); this expectation may have gendered implications and is moderated by the extent of reliance on one’s children (Jiao et al., 2024; Utz et al., 2004). This shift can increase physical and psychological burdens, potentially worsening the surviving partner’s health. Third, surviving partners, especially women, may face economic insecurity due to reduced household income (HallerÖD, 2012; Streeter, 2020). Financial strain can restrict daily activities and negatively affect health-related behaviours (e.g. engaging in hobbies, maintaining social relationships, adhering to healthy behaviours, and accessing health and long-term care services). Despite these negative impacts, spousal loss may alleviate caregiving burdens (Keene & Prokos, 2008), particularly when the deceased had chronic conditions requiring intensive informal care. Such relief can positively influence caregivers’ mental health. Therefore, spousal loss can have differential health impacts shaped by the associated stressors and coping mechanisms, with important gendered implications.
Relevant Literature on Moderators of Bereavement Outcomes
The dual process model explains bereavement coping as an ongoing oscillation between loss-oriented coping, which focuses on grief and the loss itself, and restoration-oriented coping, which involves adjusting to life changes following the loss (Rackoff & Newman, 2022; Stroebe & Schut, 1999). Coping processes are shaped by factors such as age, gender, socioeconomic status, personality, social support, and cultural or religious context, leading to diverse mental health trajectories after bereavement.
Age and Widowhood Effects
Although studies of the transition to widowhood often focus on older adults, evidence on heterogeneity within this population and on how age moderates the health effects of bereavement remains inconclusive. Some theories and evidence suggest that older individuals are better able to cope with spousal loss than those who experience it at a younger age. For older married couples, spousal loss is considered an “on-time” event in the life course, as the likelihood of experiencing such a loss increases with age. For example, Thompson et al. (1989) found that older adults may draw on prior life experiences, such as earlier losses, to manage bereavement more effectively. Other studies indicate that older adults generally have better affective experiences (Lawton et al., 1992). Recent studies also suggest that loneliness following spousal loss decreases with age and that widowhood is associated with increased loneliness among the young-old but not among the old-old (Yang et al., 2018; Yang & Gu, 2021).
In contrast, some studies suggest greater vulnerability among older bereaved individuals. Evidence from a Danish sample aged 50 or older showed that the likelihood of suicides increases among men over 80 and is the highest among women aged 65 and 79 (Erlangsen et al., 2004). While suicide is an extreme reaction to spousal loss, depressive symptoms remain elevated among widows aged 65–74 years (Mendes de Leon et al., 1994). Another study from Switzerland indicates that younger age facilitated adaption following spousal bereavement (Bennett et al., 2020). However, a meta-analysis reported no significant differences in the mortality effects of widowhood between individuals aged 65 or younger and those aged 65 or older (Moon et al., 2011). Some other studies do not find differences by age at bereavement (Szabo et al., 2020). Taken together, these mixed findings underscore the need for a more nuanced understanding of depressive symptom trajectories following spousal loss in later life.
Gender Modification Effects
As noted above, widowhood has gendered implications, reflecting gender norms that shape the adjustment process following spousal loss. While spousal loss negatively affects mental health for both men and women (Streeter, 2020), some studies report that its impact is greater for men than for women and that different underlying mechanisms operate across genders (Umberson et al., 1992). Women are more likely to experience financial strain, whereas men may face greater difficulties adjusting to household tasks previously performed by their spouse. For instance, Streeter (2020) reports that women experience declines in income and wealth following spousal loss, whereas men’s financial circumstances remain relatively stable. Despite this, the study indicates that men tend to experience more severe mental health declines than women. Another study reports that this pattern reflects the protective effect of marriage against men’s depressive symptoms: married men are less depressed than married women, whereas widowed men and women exhibit comparable levels of depression (Lee et al., 2001). The study also indicates that compared to women, men tend to spend shorter widowhood duration, dislike household chores, and provide less assistance to their children. In contrast, some studies did not find gender differences in the mental health effects of bereavement in either the short or long term (Sasson & Umberson, 2014). As gender interacts with coping mechanisms following spousal bereavement in complex ways, a better understanding of gender as a moderating factor is needed.
Co-Residence With Children
As previously described, spousal death leads to loneliness and social isolation through the loss of one’s closest social relationship. Yet, increased alternative contact with others and post-bereavement living arrangements can moderate the negative consequences of spousal death by improving access to social and emotional support. A previous study reports that, following widowhood, informal support from friends and relatives increases, whereas widowed individuals without children exhibit low levels of social participation (Utz et al., 2002). Widowhood is also a major driver of co-residence with children (Hanum et al., 2024), and living with a child may help widowed older parents respond to bereavement-related shocks. Indeed, several studies indicate that co-residence with adult children is associated with better mental health and well-being among older adults (Grundy & Murphy, 2018; Jiao et al., 2024). In Western contexts, including Europe and North America—where much of the empirical evidence on widowhood has been produced—a larger proportion of older adults live alone compared with other regions, such as Asia (United Nations Department of Economic and Social Affairs, 2020). Cultural contexts, including normative expectations regarding filial care and intergenerational co-residence, therefore shape coping strategies following widowhood and highlight the need for evidence from diverse settings.
Widowhood Period
While the literature on spousal bereavement highlights key demographic moderating factors, longitudinal data indicate that the widowhood period is also an important factor. A recent meta-analysis showed a general negative association between time since loss and the prevalence of depression (Kristiansen et al., 2019). Using longitudinal data from the Health and Retirement Study from 1994 to 2008, Sasson and Umberson (2014) observed that bereaved late middle-aged participants (aged 52–63 years at baseline) experienced an initial elevation in depressive symptomatology; this was followed by a linear decline over time. Interestingly, participants who were bereaved at the beginning of the study showed a continual decline in depressive symptoms throughout the 14-year study period, but the slope was more gradual. Sasson and Umberson (2014) found that gender did not play an important role in influencing adjustment, underscoring the significance of examining bereavement trajectories using longitudinal data.
While Sasson and Umberson (2014) illustrated an interesting pattern in the adjustment process, their findings may not be generalisable to older adults, as the participants experienced spousal loss around the age of 60. The Current Population Reports showed that the median age at widowhood in the United States was 71.8 for men and 72.0 for women in 2008 (Kreider & Ellis, 2011). While the 2016 reports did not provide the same specific data, we inferred that the age at spousal loss is increasing in the United States. As most countries are experiencing growth in the number and proportion of older adults (United Nations, 2024), the age at which individuals experience spousal loss is likely to continue to increase globally.
Japanese Context
Japan is at the forefront of population ageing. According to the 2020 Census, approximately 29% and 15% of Japan’s total population is aged 65 years or older and 75 years or older, respectively (Statistics Bureau, Ministry of Internal Affairs and Communications, 2020). As older individuals are more likely to experience spousal bereavement, this phenomenon is particularly prevalent in ageing populations. At least 10 million people in Japan experience spousal bereavement, accounting for approximately 9% of the total population (Statistics Bureau, Ministry of Internal Affairs and Communications, 2020). Owing to gender disparities in mortality rates, women are more likely than men to experience bereavement and comprise over 80% of the bereaved population.
Widowed individuals may sustain their livelihoods partly through social security mechanisms contingent upon eligibility, including survivor’s pension benefits, lump-sum payments to offset funeral expenses, health insurance coverage, and other forms of social welfare benefits. Although policy responses may be similar among high-income countries, living arrangements in Japan may be distinct from those observed in Western contexts.
Within the context of traditional filial piety, adult children have historically borne the responsibility of caring for ageing parents, which is often manifested through multigenerational co-residence. Consequently, even after spousal bereavement, such normative expectations may function as a protective factor, mitigating psychological distress and instrumental disruptions (Nakagawa & Hulur, 2021; Tiedt, 2013). However, this normative expectation is gradually eroding in contemporary society (Ogawa & Retherford, 1993), and multigenerational co-residence has become less common than in previous generations (Statistics Bureau, Ministry of Internal Affairs and Communications, 2020). Nevertheless, living with children in old age is still observed because of social exchange and filial norms in response to the needs of older parents and adult children (Taniguchi & Kaufman, 2017). Hasegawa (1985) identified family structure as a factor contributing to the lower prevalence of depressive symptoms in Japan.
Extra-familial support networks in Japan are comparatively weaker than in Western countries such as the United States (Kikuzawa, 2006). Furthermore, men tend to have limited social ties beyond the workplace, particularly after retirement, and often rely on their spouses’ social networks and emotional support. Therefore, men may be disproportionately affected by spousal bereavement and the transition to widowhood in Japan (Tiedt et al., 2016; Yamauchi & Hirakawa, 2020). This is reflected in empirical findings indicating that marriage is positively associated with health and well-being among men but not women (Raymo et al., 2008).
Given the cultural variations in the experience, response to, and recovery from spousal loss, this phenomenon must be examined in non-Western contexts, where empirical evidence is limited and populations are ageing rapidly. Although the health implications of spousal bereavement and widowhood have received increasing attention in Japan and other East Asian countries, longitudinal evidence from nationally representative samples of older adults remains limited.
Current Study
This study examined the effects of spousal loss on the mental health of bereaved individuals and the potential buffering factors using data from the National Survey of the Japanese Elderly (NSJE). It aimed to enhance the understanding of the effects of bereavement on mental health and the potential coping mechanisms in the context of bereavement-related psychological distress in a non-Western context. With an adequate sample of respondents who experienced spousal bereavement over a 19-year period, the NSJE allowed us to study the trajectories of depressive symptomatology as the participants transitioned into widowhood. Using this dataset, we investigated changes in depressive symptoms at the time of spousal loss (i.e. reaction) and the post-bereavement trajectory (i.e. recovery). We hypothesised a significant increase in depressive symptoms at the time of loss (
Another advantage of using the NSJE is that its sample consists of older adults. Conversely, most other publicly available datasets focused on ageing populations (e.g. the Health and Retirement Study). As the global population is ageing, it is increasingly important to understand bereavement processes among older adults and identify potential moderators. Through the NSJE, we focused on three potential moderators of gender, age at loss, and co-residency status with children, which were expected to shape influencing factors and coping processes in later-life bereavement, grounded in the dual process model of bereavement, underlying mechanisms, and cultural context. Gender differences in social roles, social networks, financial resources, and caregiving responsibilities are particularly pronounced in Japan, suggesting that widows and widowers may experience distinct stressors, including loneliness and financial insecurity. Age at loss reflects whether bereavement occurs “on time” within the life course, which can influence coping expectations and preparedness. Finally, co-residence with children is a salient source of instrumental and emotional support in Japan, where intergenerational living has historically served as a primary safety net for widowed parents.
While Sasson & Umberson (2014) did not find gender differences in their data, we hypothesised that women would show greater adjustment to spousal loss than men (
Our study is also advantageous for its empirical strategy. By implementing an econometric method, we attempted to control for the observed and unobserved factors that influence depressive symptomatology and assessed the effects of spousal loss on depressive symptomatology by comparing bereaved and non-bereaved individuals and partially addressing potential endogeneity.
Methods
Data
The NSJE is a nationally representative longitudinal dataset that was initiated in 1987 using a two-stage stratified sampling method to collect data from Japanese adults aged 60 years or older (JAHEAD/NSJE Project Group, nd). We used data from the first seven of the nine publicly available waves collected between 1987 and 2006. Participants were surveyed every three to four years. Although Waves 8 (2012) and 9 (2017) are currently publicly available, data from these waves were excluded from the analysis because of the longer interval between these waves and the previous waves, which differed from the regular survey schedule. Ethical review was not required for this study as it involved a secondary analysis of publicly available data.
Several features of this dataset make it ideal for examining bereaved individuals’ adjustment processes. First, it is a large-scale dataset: 5,215 people completed at least one survey across the first seven waves, and approximately one-tenth of the respondents transitioned into widowhood over the course of the survey. Second, the participants are older than those in many other publicly available datasets of similar scale. The age at which the NSJE respondents experienced spousal loss was over 70 (Nakagawa & Hulur, 2021), which more closely reflects the age at which spousal loss has typically occurred in recent years. Third, the data come from East Asian cultures and a specific generation, allowing us to explore whether the findings from Western samples can be replicated. All participants in the first seven waves were born before World War II, indicating that they witnessed significant political, economic, and cultural transitions during Japan’s high growth period (1954–1972). Regarding family life, this period was marked by the solidification of traditional gender roles in marriage, with men assuming economic responsibilities and women taking charge of the household (Yamada, 1998). This suggests that gender differences in bereavement adjustment may be more pronounced in this sample than in Western populations.
As noted above, post-bereavement living arrangements may be an important modifier of the effects of widowhood on mental health in Japan. The NSJE is well suited for examining the role of living arrangements in spousal loss, as half of the bereaved participants lived with their children (Nakagawa & Hulur, 2021). The data analysed may appear outdated, but the findings from this study remain relevant today, given that similar normative expectations surrounding intrafamilial support and gender persist among later cohorts (Uchikoshi et al., 2023), even amid the declining importance of intergenerational co-residence and the increasing prevalence of nuclear families.
Measures
Depressive symptomatology: Depressive symptoms were assessed using the Japanese version of the Center for Epidemiologic Studies Depression Scale (CES-D), one of the most widely used measures of depressive symptomatology (Radloff, 1977). We used a 9-item version of the CES-D, consisting of three subscales: depressed affect, somatic complaints, and interpersonal problems. The low positive affect subscale was excluded because previous research using this dataset indicated the subscale’s low validity among the Japanese population (Yatomi et al., 1993). The response format varied across the seven waves, with the first four waves using a 3-point Likert-type scale and the remaining waves using a 4-point Likert-type scale. Upon reviewing the responses, most participants consistently endorsed “rarely” across items and waves. Therefore, each item was dichotomised (0 = rarely; 1 = sometimes, occasionally, or often), and the total score was calculated by summing the nine items. To deal with missing data, the mean of the dichotomised items was computed and multiplied by nine. For instance, if an individual reported symptoms for two items and one item was missing, the CES-D score was calculated as 2.25 (=2/8 × 9). Individuals who did not provide any valid responses to any of the nine items were excluded from the analysis. Although treating depressive symptomatology as a count variable prevented the use of the clinical CES-D cut-off, and the inconsistent scaling requires caution in interpretation, this approach allowed for consistent analyses across all seven waves. The mean score of depressive symptoms in this sample was 1.35, with a standard deviation of 1.91.
Time since spousal loss (TIME): Time was coded as the number of years since the spousal loss. Theoretically, it could range from −19 (bereavement occurred immediately after the first wave) to +19 (bereavement occurred just before the seventh wave), with 0 representing the time of spousal loss. In this dataset, the observed range of time since spousal loss was from −19 to 18.5 (Q1 = −6, Median = −1, Q3 = 3).
Widowhood phase (Pre-loss, Post-loss): We created two dummy-coded variables to distinguish between waves occurring before and after spousal loss. The first dummy variable represented the post-loss phase (hereafter referred to as “post-loss”), coded as 1 for waves following spousal loss and 0 for those preceding it. The second dummy variable represented the pre-loss phase (hereafter “pre-loss”), coded as 1 for waves prior to spousal loss and 0 for those following the loss. Using both dummy variables allowed us to estimate separate coefficients for the trajectories before and after spousal loss (see details in the Analytic plan section).
Age at spousal loss (Age): Age at the time of spousal loss was calculated in years. Participants’ average age at the time of spousal loss was 74.9 years, ranging from 63 to 91 years (Q1 = 70, Median = 75, Q3 = 79). For the analyses, this variable was centred around the average age.
Gender of participants (Men): Gender was coded as 0 for women and 1 for men. Similar to the findings from the United States (Sasson & Umberson, 2014), the majority of the bereaved sample comprised women (73.9%).
Cohabitation with children (Cohabitation): In each wave, the participants were asked about their cohabitation status, including the relationship, age, and gender of their cohabitants. If they reported living with children or children-in-law, they were categorised as cohabiting with children and coded as 1; all other responses were coded as 0, which included those from individuals without children. To examine the moderating effects of cohabitation with children, we derived two separate variables: pre- and post-loss cohabitation. Pre-loss cohabitation refers to the status reported in the last wave before the bereavement, whereas post-loss cohabitation refers to the status reported in the first wave after the bereavement. For most participants (82.57%), the cohabitation status remained unchanged before and after the loss. However, a sizable proportion (11.49%) transitioned to co-residency following bereavement. We used continuous co-residency as the reference group. Owing to the small number of participants who transitioned out of co-residency (n = 31), we grouped them with those who did not live with their children before or after the loss. Consequently, we defined three co-residency categories: continuous co-residency (n = 288; reference group), transitioned into co-residency (n = 60; Group 1), and post-loss without children (n = 234; Group 2).
We also included several covariates to control for the factors influencing depressive symptomatology, such as socioeconomic variables, physical health status, and social relationships (Zenebe et al., 2021). For these variables, participants were asked to report information on house ownership, co-residency status, activities of daily living (ADL), instrumental activities of daily living (IADL), and group participation in each wave.
House ownership: House ownership was coded as 1 if respondents resided in a house, apartment, or building they owned; otherwise, it was coded as 0. This variable served as an indicator of socioeconomic status. Individuals who own their homes may be more likely to stay in the same residence following the death of a spouse, whereas those without home ownership may encounter the need to relocate to more affordable and potentially smaller accommodations.
Co-residency status: This was measured by the number of people with whom the respondent lived at the time of the survey. A value of 1 indicated living alone, whereas values greater than 1 indicated cohabitation with others.
Activities of daily living: We assessed ADL based on the reported difficulties with six tasks similar to those on the Katz scale (Katz et al., 1963): bathing, dressing, eating, standing up, going out, and toileting.
Instrumental activities of daily living: We measured IADL based on the difficulties in tasks such as shopping, using a telephone, going out alone using public transportation, and performing light household chores (Lawton & Brody, 1969). The variables of ADL and IADL were combined to calculate the percentage of accumulated disabilities for all ADL and IADL items.
Group participation: This was assessed as an indicator of social relationships by asking participants to report the number of clubs, local organisations, or religious groups to which they belonged.
Analytic Plan
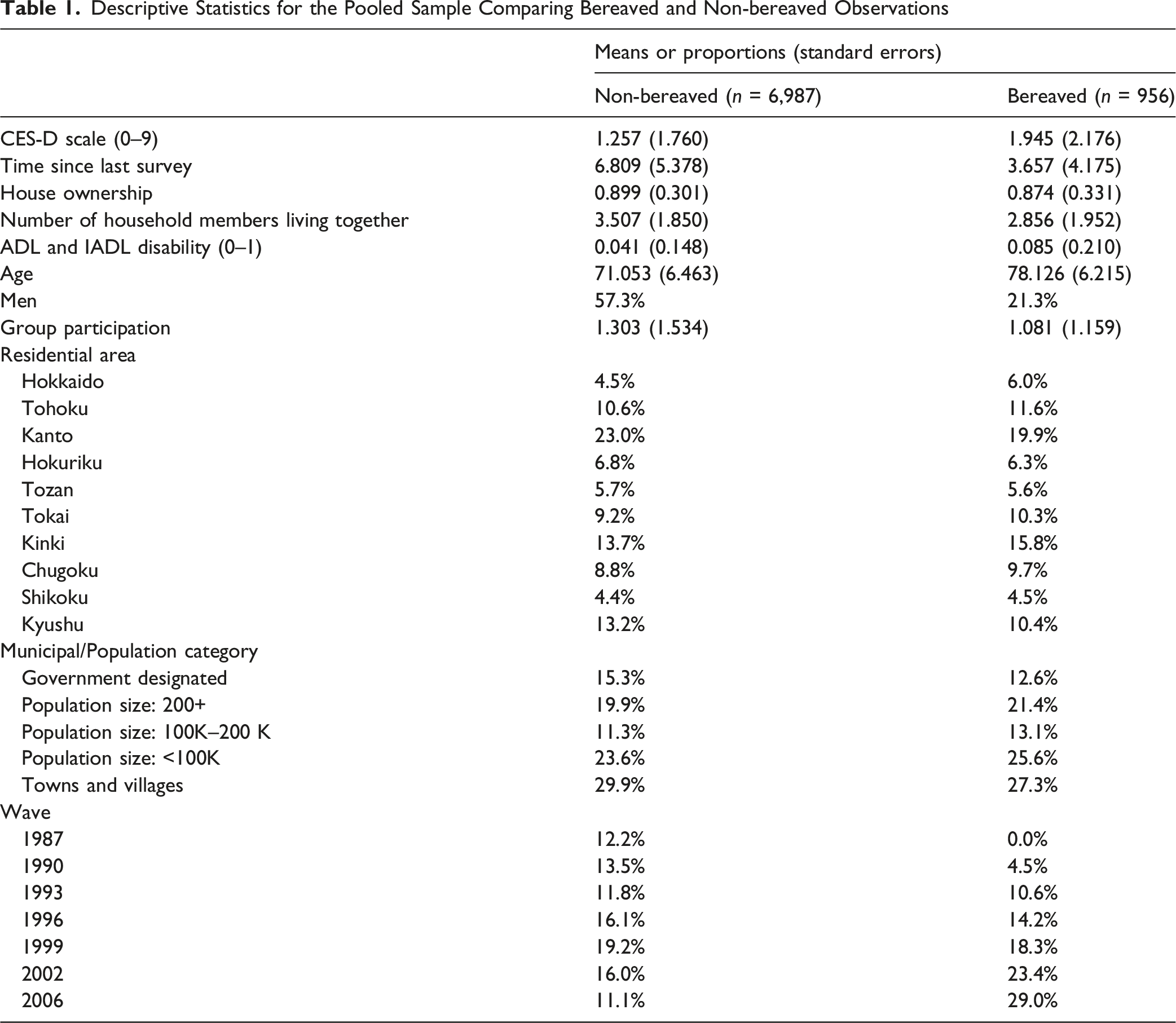
Descriptive Statistics for the Pooled Sample Comparing Bereaved and Non-bereaved Observations
Subsequently, to examine the first set of research questions (H1.1 and H1.2), we employed a discontinuous model (Singer & Willett, 2003). This model simultaneously estimated the pre-loss slope, instantaneous shift at the time of loss (reaction), and post-loss slope (recovery) among the bereaved participants. To estimate the main effects of the pre- and post-loss slope coefficients and their respective standard errors, we ran two separate models: Models H1a and H1b. Model H1a included TIME, a pre-loss dummy variable, and the interaction term TIME × pre-loss. The interaction term allowed us to interpret the TIME coefficient as the post-loss slope (recovery). Model H1b included TIME, a post-loss dummy variable, and the interaction term TIME × post-loss. In this model, TIME represented the pre-loss trajectory, whereas the post-loss coefficient captured the reaction or instantaneous shift in depressive symptoms at the time of spousal loss. In both models, the interaction terms were interpreted as the difference in the slopes of depressive symptoms before and after the loss.
To address the second set of research questions (H2.1, H2.2, and H2.3), which examined the moderating effects, we created three interaction terms between the post-loss dummy variable and each moderator. As the outcome variable—depressive symptomatology—was a count variable, all models were estimated using Poisson pseudo-maximum likelihood regressions with fixed effects (Correia et al., 2020), implemented in Stata MP version 19.0 (StataCorp LLC, College Station, TX, USA). All analyses controlled for house ownership, co-residency status, ADL, group participation, residential location-by-scale fixed effects, time fixed effects, and individual fixed effects. In the Results section, we report the coefficients (γ), standard errors (SE), and incidence rate ratios (IRRs).
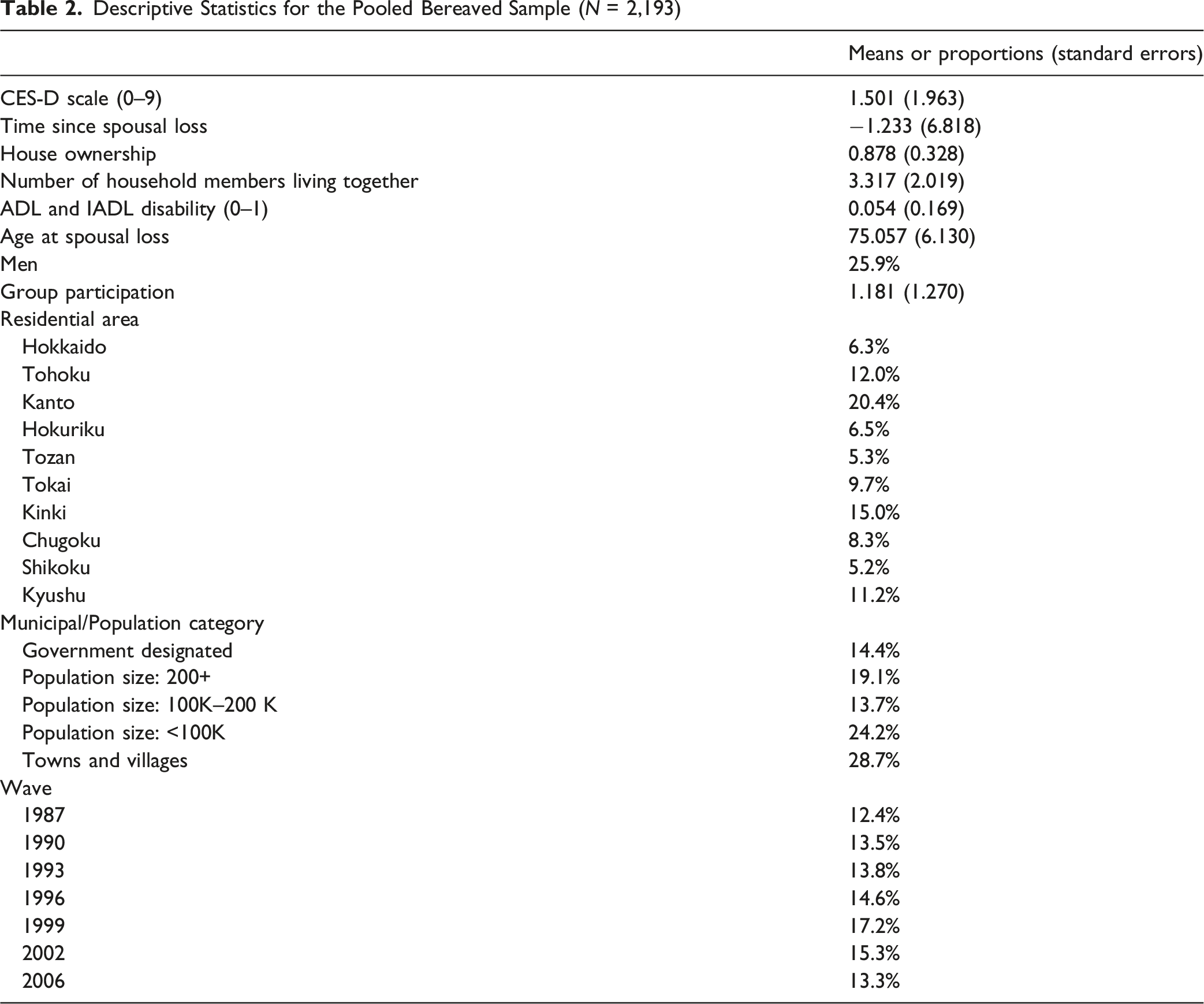
Descriptive Statistics for the Pooled Bereaved Sample (N = 2,193)
Results
Propensity Score Analysis
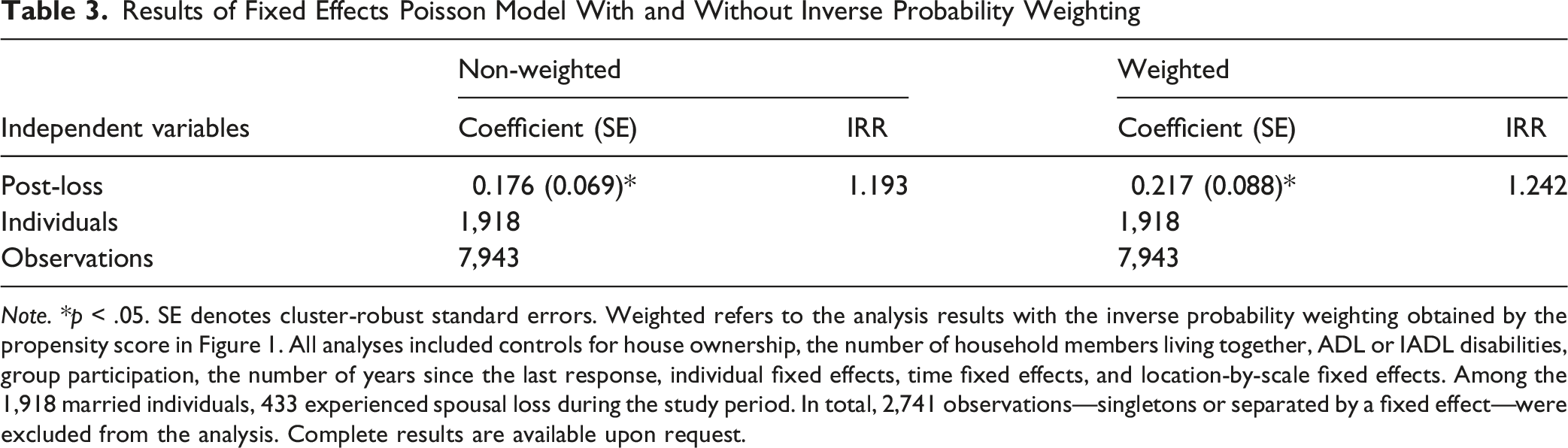
The propensity score analysis showed that Rubin’s B—the absolute standardised difference in the means of the linear index of the propensity score between the bereaved and (matched) continuously married groups—was 15.9. Rubin’s R—the ratio of the variances of the propensity score index between the bereaved and continuously married groups—was 0.99 (Figure 1). Both values fell within Rubin’s recommended thresholds (B < 25 and 0.5 < R < 2), indicating a sufficient covariate balance between the groups. Therefore, after adjusting for age, gender, years of education, self-rated health, CES-D score, house ownership, presence of children, and group participation at baseline, we found no significant differences in depressive symptomatology or other observed factors between the bereaved and continuously married samples. Using inverse probability weighting based on the estimated propensity scores, we evaluated the impact of bereavement on depressive symptoms. Bereavement had a detrimental effect on mental health (γ = 0.217, SE = 0.088, IRR = 1.242; Table 3). This result remains unchanged even when we adopt a linear model to account for the potential reduction in outcome variation due to dichotomisation (the result is not presented here but is available upon request). Kernel density plots of bereaved and non-bereaved individuals before and after inverse probability weighting. Results of Fixed Effects Poisson Model With and Without Inverse Probability Weighting Note. *p < .05. SE denotes cluster-robust standard errors. Weighted refers to the analysis results with the inverse probability weighting obtained by the propensity score in Figure 1. All analyses included controls for house ownership, the number of household members living together, ADL or IADL disabilities, group participation, the number of years since the last response, individual fixed effects, time fixed effects, and location-by-scale fixed effects. Among the 1,918 married individuals, 433 experienced spousal loss during the study period. In total, 2,741 observations—singletons or separated by a fixed effect—were excluded from the analysis. Complete results are available upon request.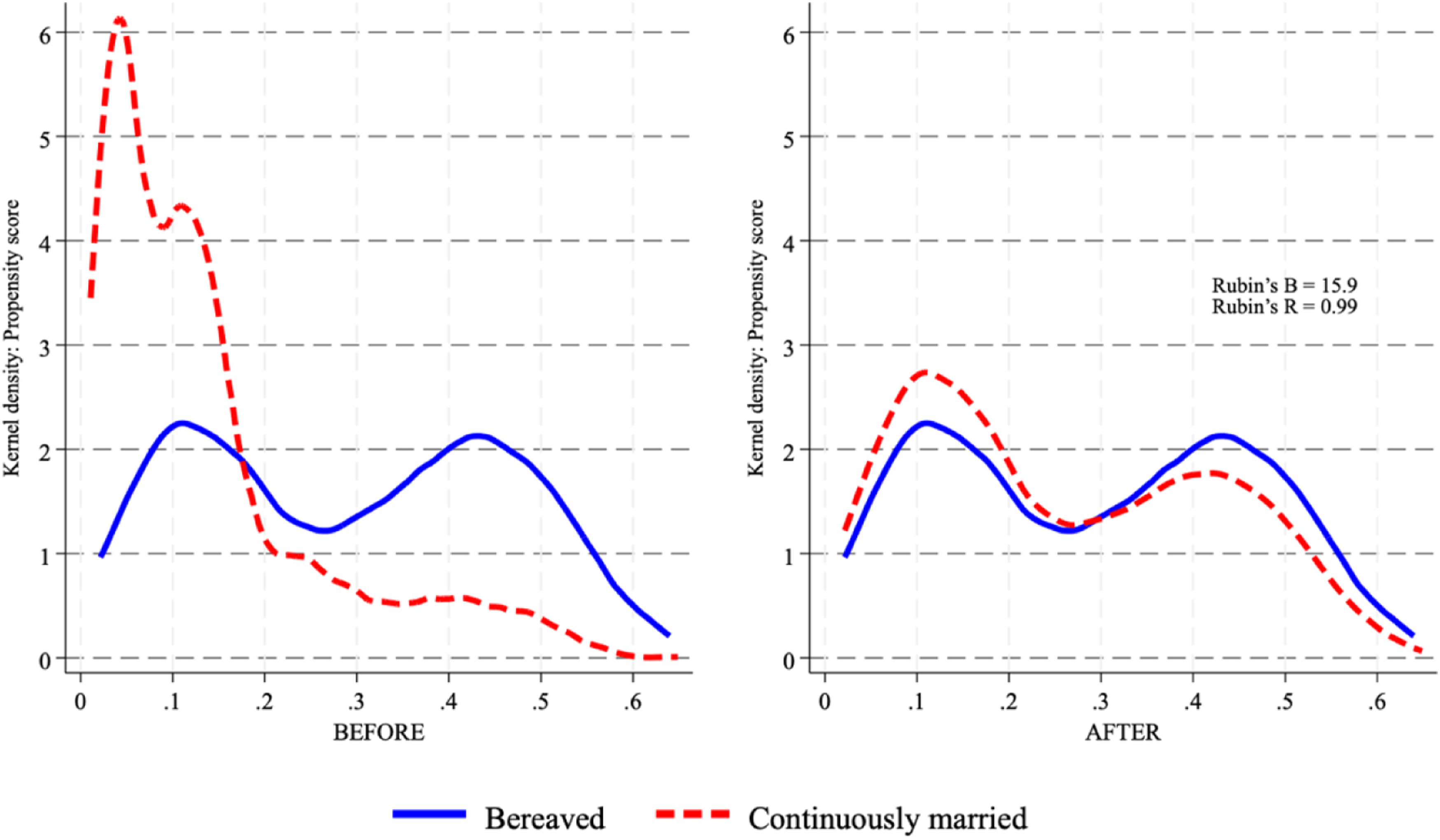
Trajectories of Depressive Symptoms
Results of Fixed Effects Poisson Models for Depressive Symptoms Following Spousal Loss
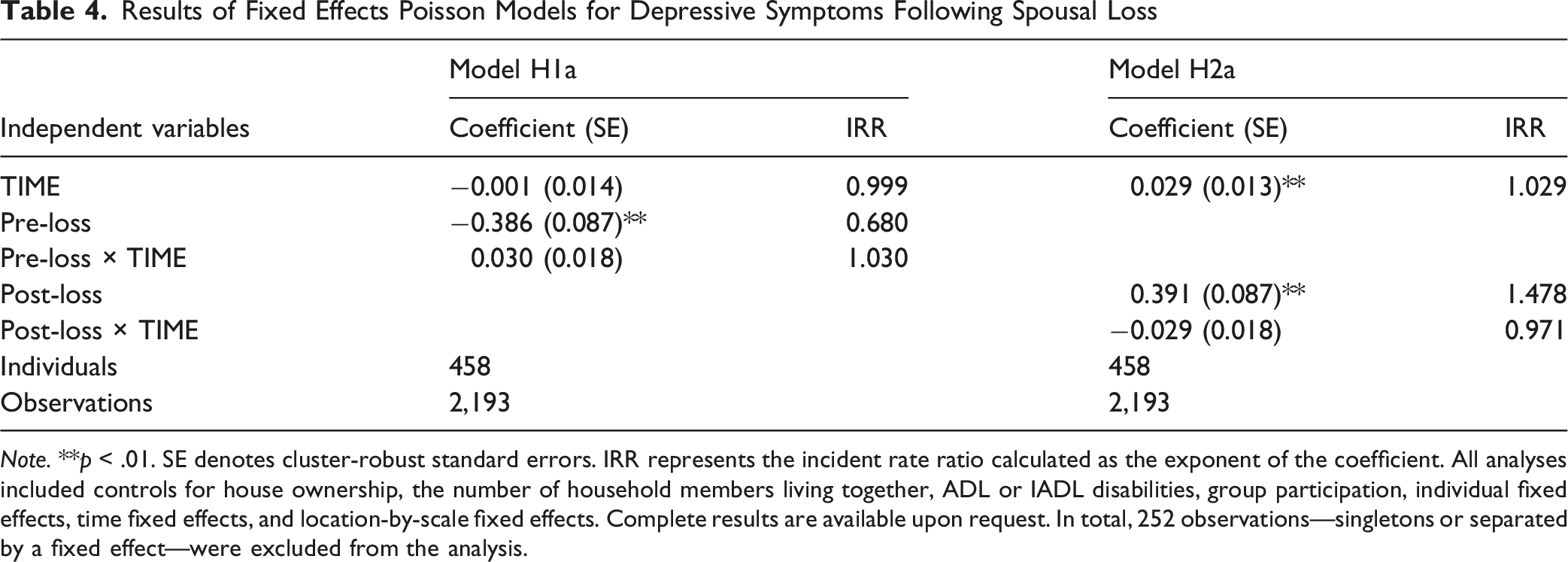
Note. **p < .01. SE denotes cluster-robust standard errors. IRR represents the incident rate ratio calculated as the exponent of the coefficient. All analyses included controls for house ownership, the number of household members living together, ADL or IADL disabilities, group participation, individual fixed effects, time fixed effects, and location-by-scale fixed effects. Complete results are available upon request. In total, 252 observations—singletons or separated by a fixed effect—were excluded from the analysis.
Moderating Effects
Results of Fixed Effects Poisson Models for Depressive Symptoms and Moderators
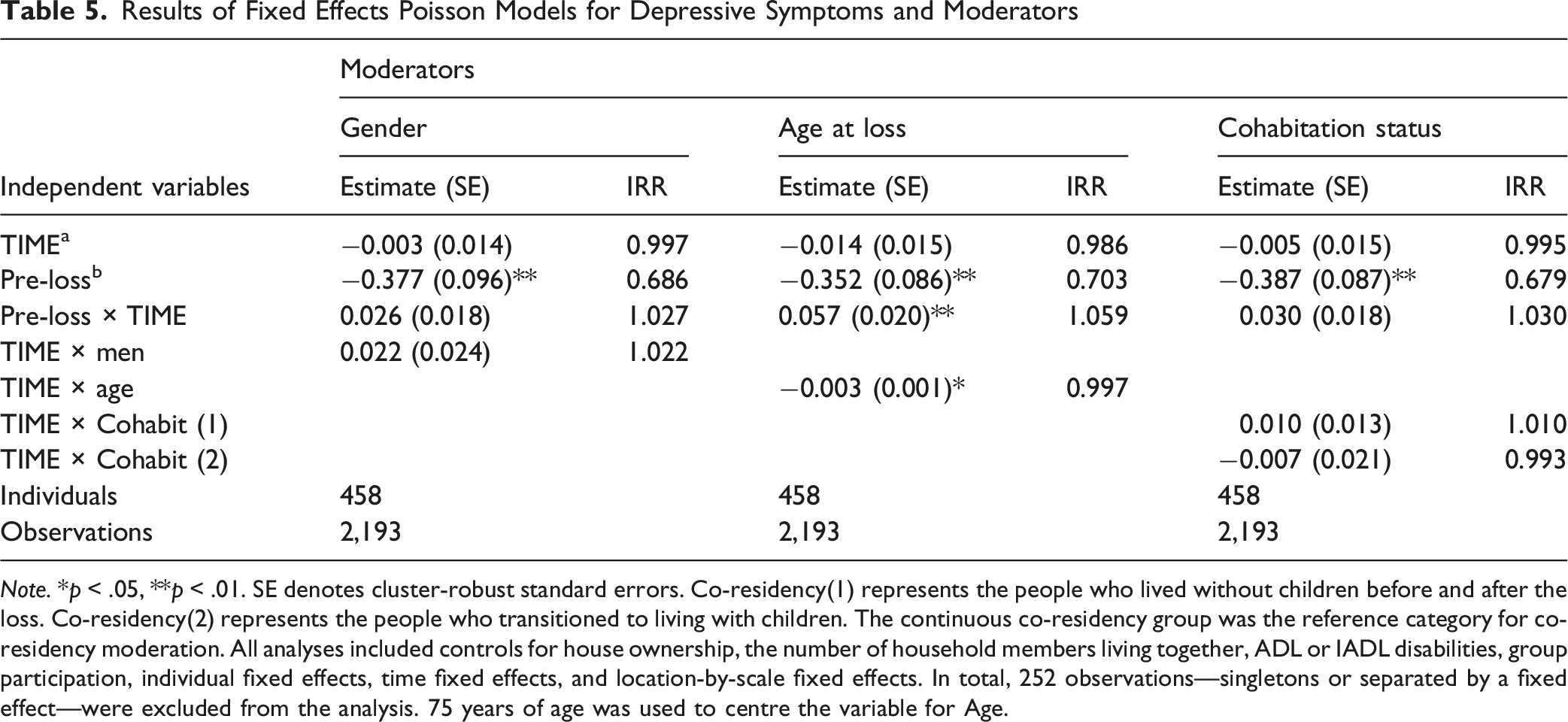
Note. *p < .05, **p < .01. SE denotes cluster-robust standard errors. Co-residency(1) represents the people who lived without children before and after the loss. Co-residency(2) represents the people who transitioned to living with children. The continuous co-residency group was the reference category for co-residency moderation. All analyses included controls for house ownership, the number of household members living together, ADL or IADL disabilities, group participation, individual fixed effects, time fixed effects, and location-by-scale fixed effects. In total, 252 observations—singletons or separated by a fixed effect—were excluded from the analysis. 75 years of age was used to centre the variable for Age.
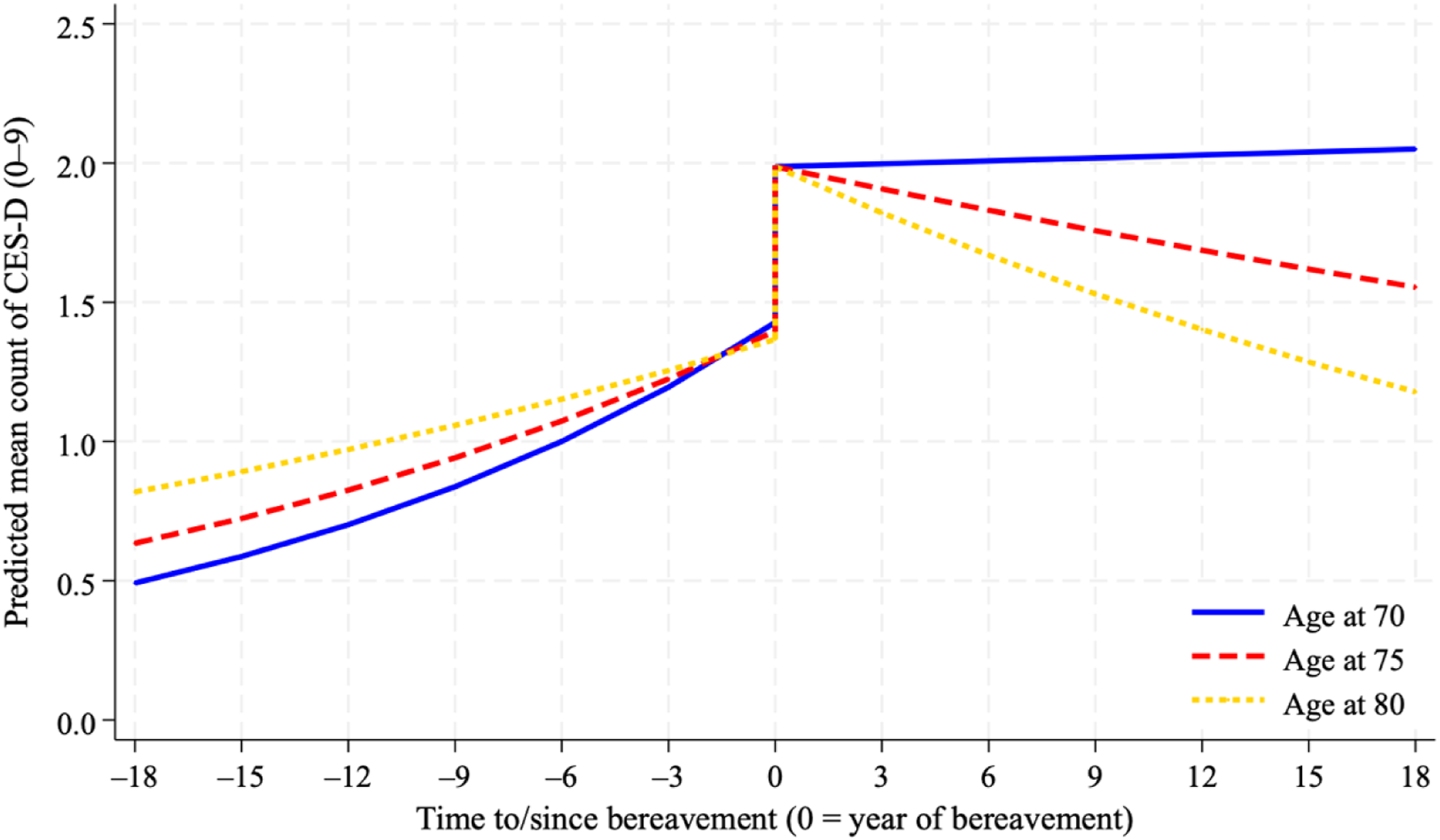
Trajectories of depressive symptoms moderated by age at spousal loss.
Discussion
This study examined the trajectories of depressive symptoms among Japanese older adults as they transitioned into widowhood. Our findings advance the literature and contribute theoretically to the understanding of bereavement adjustment by revealing potential cultural differences in the mental health effects of widowhood between Western and East Asian contexts. Our study suggests that context-specific evidence is essential by reflecting on pre- and post-bereavement circumstances as well as the coping strategies adopted by surviving partners, including demographic characteristics, the normative expectations, and grief practices.
First, our econometric approach contributes to the robustness of the evidence regarding the negative effects of bereavement on mental health. Spousal death can deteriorate the health of bereaved individuals through various channels, including diminished social ties (Freak-Poli et al., 2022; Niino et al., 2025; Okabayashi et al., 2004; Schmitz, 2021), increased physical and psychological burdens on surviving partners as they assume the roles previously fulfilled by the deceased (Umberson et al., 1992), and substantial financial strain (HallerÖD, 2012; Streeter, 2020). By employing fixed effects models and propensity score methods, we estimated the effects of spousal loss on depressive symptomatology while controlling for observed and unobserved heterogeneity. This enabled an accurate comparison between bereaved and non-bereaved individuals.
Second, our sample characteristics differ notably from those of previous studies that addressed similar questions (Chauhan et al., 2025; Sasson & Umberson, 2014). The data were collected in East Asia, specifically Japan, and participants experienced spousal loss at an older age than in most previous studies (Shor et al., 2012). While some patterns of adjustment were consistent with findings from Western cultures, our study revealed meaningful differences. Consistent with previous research, spousal loss was a significant life disruption for Japanese older adults, as evidenced by a marked increase in depressive symptoms at the time of loss. However, unlike the findings of studies conducted in Western contexts, we did not observe a significant decline in depressive symptoms during the years following bereavement. Notably, we found a moderating effect of age at loss, with individuals who experienced spousal loss at an older age demonstrating a more rapid decline in depressive symptoms after the loss.
Trajectories of Depressive Symptoms
Although spousal loss could be considered an “on-time” event for older adults (Lawton et al., 1992; Thompson et al., 1989; Yang et al., 2018; Yang & Gu, 2021), our results demonstrated that it is never emotionally easy, in alignment with attachment theory (Bowlby, 1980), as depressive symptoms spiked at the time of loss and showed no evidence of subsequent decline. These findings partially replicate those of Sasson and Umberson (2014), who reported an immediate increase and significant post-loss decline in depressive symptoms.
One of the reasons for the lack of a decline in depressive symptoms may lie in cross-cultural differences in bereavement practices and expectations. A previous review highlights that grief practices vary across cultural contexts, including funerary rites and mourning periods, which may shape post-bereavement coping strategies (Mohagheghpour & Songhori, 2026). In individualist cultures, such as Western Europe, grief is largely understood as an intrapersonal and psychological process oriented toward autonomous recovery, whereas in East Asian cultures it is often conceptualised as a shared, communal obligation. The presence of practices such as ancestor veneration, which is common in East Asia, institutionalises continuing bonds with the deceased.
Our findings align with those of Nakagawa and Hulur (2021), who also used the NSJE dataset. Their study focused on trajectories of life satisfaction among bereaved participants; however, the similarity in patterns suggests that the observed outcomes are not unique to depressive symptoms but reflect broader cultural processes of adjustment to spousal loss in East Asian contexts. For example, in Japan, several memorial services are offered after someone’s death. Although these services are more frequent within the first year, they continue periodically thereafter and may delay the bereaved spouse’s adjustment process. Rooted in Buddhist traditions, these rituals are intended to help manage grief and maintain psychological bonds with the deceased (Klass, 2001).
However, limited empirical evidence supports the long-term effectiveness of continuing bonds. For instance, Lalande and Bonanno (2006) found that continuing bonds reported at 4 months post-loss were associated with reduced distress at 18 months among Chinese participants but not among American participants. Conversely, continuing bonds reported at 18 months post-loss were linked to increased distress in both samples. This may help explain the pattern observed in our Japanese sample: ongoing memorial practices may sustain emotional bonds with the deceased, thereby maintaining elevated levels of depressive symptoms even years after the loss.
Another notable pattern was a significant upward trajectory of depressive symptoms prior to spousal loss, a finding consistent with previous studies (Rackoff & Newman, 2022; Szabo et al., 2020). Although the specific mechanisms underlying this pre-loss increase cannot be fully identified within the scope of the present study, pre-bereavement circumstances likely play an important role. Health and well-being within married couples are interdependent, a phenomenon often described as emotional contagion (Ruthig et al., 2012). When spouses experience chronic or terminal conditions prior to death, their partners may suffer physical and psychological distress resulting from anxiety, anticipation of loss, and caregiving burden. Certain pre-bereavement experiences, such as caregiving and anticipatory grief, may adversely affect mental health in the short term before bereavement, yet potentially buffer the negative impact of loss and facilitate post-bereavement adjustment (Keene & Prokos, 2008; Victor, 2026). Future research should therefore examine the mechanisms driving pre-bereavement mental health deterioration and identify factors that promote recovery following spousal loss.
Contrary to our expectations, we did not observe significant gender modification effects, even though the study sample experienced historical periods characterised by strongly gender-divided role ideologies, in which gender differences might be expected to be more pronounced. This absence of observed gender differences may reflect the fact that men and women face distinct post-bereavement challenges and adjustment processes, such as increased household labour responsibilities and financial strain (Streeter, 2020; Umberson et al., 1992). However, the current study is limited in its ability to examine the underlying mechanisms that may explain the lack of gender differences, due to insufficient data on pre- and post-bereavement roles and stressors.
Protective Factors of Recovery From Spousal Loss
To better understand the moderating mechanisms involved in recovery from spousal loss, we examined several potential protective factors of key demographics: gender, age at loss, and cohabitation status with children. Gender and cohabitation status did not emerge as significant moderators of adjustment to spousal loss. Given the cultural differences in gender roles and family structures (Hasegawa, 1985; Nakagawa & Hulur, 2021; Taniguchi & Kaufman, 2017; Tiedt, 2013) and implications from social production function theory (Ormel et al., 1999), we expected these factors to play a more prominent role. However, our findings are consistent with previous research from Western contexts, which found no gender differences after adjusting for time since bereavement (Sasson & Umberson, 2014; Schmitz, 2021).
Our results revealed the moderating effect of age at the time of spousal loss on the trajectory of depressive symptoms. The older the participants were at the time of loss, the steeper the trajectory of depressive symptoms, indicating faster recovery. Lawton et al. (1992); Yang and Gu (2021); Yang et al. (2018) suggests that older adults tend to exhibit better emotional control and stability, as well as lower levels of loneliness, than younger individuals. Our findings provide further evidence of older adults adjusting more effectively to extreme life stressors. These results are also consistent with those of a meta-analysis of 123 studies conducted by Shor et al. (2012), which found that the harmful effects of widowhood on mortality decreased with age. However, this age-related moderation should be interpreted with caution because it may be confounded by the expectation of spousal loss. The anticipation of spousal death can buffer its psychological impact (Carey, 1977), and older individuals may be more prepared to accept the loss owing to age-related expectations. Unfortunately, the dataset did not include information on the cause of death or whether the loss was anticipated, making it difficult to determine whether the observed effects were solely attributable to the age at loss. The sample may also represent a selectively surviving group, with better physical and mental health and resilience to the difficult experience of spousal death, which we could not explore in this study.
Limitations
Despite the NSJE’s strengths, the study had several notable limitations. First, it was not designed to focus on bereavement, and no data were collected on the spouses’ health or illness prior to their death. This restricted our ability to examine the potential mechanisms underlying the patterns observed in this study.
Second, the data were collected at three-to four-year intervals, indicating that the participants did not necessarily report their depressive symptoms immediately following spousal loss. The mean duration between the occurrence of bereavement and individual survey was 1.35 years. Consequently, the reaction coefficient (i.e. the instantaneous shift) reported in this study was projected from the pre- and post-loss trajectories and was likely to be underestimated. Therefore, the increase in depressive symptoms at the time of spousal loss might have been greater if the data were collected immediately after the event. This may also explain the absence of a significant post-loss decline in depressive symptoms; the symptoms might have already stabilised in most participants by the time of the next wave. Previous research has shown that bereaved individuals experience the greatest decline in symptoms within 6 months of the loss, with grief typically stabilising by 18 months post-loss (Bonanno et al., 2004). Furthermore, depressive shock subsides within one year following spousal death (Domingue et al., 2021). To better understand the mechanisms of spousal bereavement, an event-induced, intensive, longitudinal design that follows individuals shortly after spousal loss would be beneficial. However, it is also important to balance the participant burden, especially among older adults. The NSJE remains a valuable resource for understanding the lives of Japanese older adults.
Conclusion
This study extends the longitudinal literature on spousal bereavement and depressive symptoms in the East Asian culture and provides robust evidence in this context. Some patterns, such as the initial increase in depressive symptoms at the time of spousal loss, mirrored those found in Western contexts. However, unlike in the Western context, we did not observe a significant decline in depressive symptoms during the years following bereavement.
Our results also revealed an important moderating effect: the age at which Japanese older adults experienced spousal loss influenced their post-loss adjustment. This buffering effect of age at loss is noteworthy as the global population continues to age, highlighting the importance of age-sensitive approaches for bereavement support. Considering the adverse mental health consequences associated with bereavement, it is essential to strengthen support systems beyond the family, particularly within local communities. One potentially effective intervention is social prescribing, which facilitates links between bereaved individuals and community resources to mitigate post-bereavement loneliness, social isolation, and other social determinants of health (Lee et al., 2026). This can foster social integration among older adults, including those who are widowed or living alone, and help mitigate the psychological impact of spousal loss.
Footnotes
Acknowledgements
The data for this secondary analysis, “the National Survey of the Japanese Elderly <Wave1 (1987), Wave2 (1990), Wave3 (1993), Wave4 (1996), Wave5 (1999), Wave6 (2002), and Wave7 (2006)>, the University of Michigan, and the Tokyo Metropolitan Institute of Gerontology,” were provided by the Social Science Japan Data Archive, Centre for Social Research and Data Archives, Institute of Social Science, University of Tokyo.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a Grant-in-Aid for Scientific Research by the Japan Society for the Promotion of Science (23H00063). However, the founder was not involved in conceptualisation, design, data collection, analysis, the decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.