
Abstract
Community resources are essential for supporting older adults with disabilities and chronic conditions, yet how these resources are conceptualized and evaluated across the empirical literature remains unclear. This scoping review synthesizes U.S.-based research on community resources for older adults with age-related disabilities and chronic conditions, guided by the PAGER framework. Following PRISMA-ScR guidelines, we searched MEDLINE, PsycINFO, CINAHL, and Web of Science, ultimately including 21 peer-reviewed studies. Findings reveal four primary resource domains: healthcare-based services, home- and community-based services (HCBS), behavioral health supports, and environmental or structural resources. Accessibility and utilization emerged as the most consistently examined dimensions, while quality and effectiveness received limited attention. Structural barriers—including geographic inequities, workforce shortages, financial constraints, and insurance gaps—persistently limit equitable access. Existing research remains fragmented, often treating health, social, and environmental domains in isolation. This review identifies critical gaps in integrated, participation-centered approaches and calls for theory-informed frameworks that account for the intersecting needs of older adults aging with disability.
Keywords
In the United States, most older adults live with age-related disabilities and multiple chronic conditions, often accompanied by cognitive impairment or mental health challenges such as depression and anxiety (e.g., Watson et al., 2025; Jaul & Barron, 2017; Choi et al., 2020). These co-occurring conditions illustrate the growing complexity of aging, as physical, cognitive, and psychological factors intersect to shape daily functioning and care needs. National trends indicate rising population-level demands, including a projected doubling of dementia prevalence by 2060 and persistently high rates of late-life mental health conditions (Alzheimer’s Association, 2023). Simultaneously, the U.S. long-term services and supports (LTSS) system faces mounting pressure from increased demand for home- and community-based services, workforce shortages, and persistent geographic inequities. Together, these developments highlight the urgency of assessing whether community resources can meet the needs of older adults aging with increasingly complex and intersecting health conditions.
Community resources—here defined as the formal and informal supports within neighborhoods that enable older adults to manage disability, maintain autonomy, and participate in everyday life—have become central to this inquiry. Across the aging-and-place literature, communities are conceptualized as multidimensional environments that integrate physical infrastructure, social relationships, and locally available services (e.g., Bigonnesse & Chaudhury, 2022; Cutchin & Rowles, 2024). Recent theories of place and aging emphasize that well-being depends not on isolated services but on the broader constellation of physical, social, and organizational contexts in which daily life unfolds. Disability scholarship further highlights that disability arises not only from impairments but from environmental and social conditions that restrict participation (Putnam et al., 2021). In this study, participation is defined as involvement in life situations, including engagement in social, community, and daily activities, consistent with the International Classification of Functioning, Disability and Health (World Health Organization, 2001). Taken together, these perspectives illuminate why the availability, accessibility, and coordination of community resources are especially consequential for older adults with disabilities.
Importantly, access to community resources in the United States is shaped not only by need but also by financial and insurance-related factors. Because Medicare does not cover most long-term care, many older adults rely on Medicaid or out-of-pocket payments (Centers for Medicare & Medicaid Services Centers for Medicare & Medicaid Services, 2024. Although Medicaid is the primary payer for long-term services and supports, HCBS coverage is optional and varies across states, resulting in access that is stratified by wealth, insurance status, and policy context (Miller & Thunell, 2024). These structural constraints are particularly consequential for older adults with chronic conditions or dementia and influence not only whether services are available but also whether they can be obtained in practice. For example, greater HCBS investment has been linked to lower unmet need, while out-of-pocket spending remains common and burdensome (Shen et al., 2025; Waymouth et al., 2023; Yang et al., 2024).
Conceptualized ecologically, community resources function not as static service inventories but as dynamic, place-based arrangements shaped by spatial, organizational, and social conditions. Yet despite growing recognition of their importance, scholarship has rarely examined how these resources are defined, measured, or evaluated for older adults with disabilities. Much of the evidence remains fragmented, with most studies focused on single program areas or clinical conditions, offering limited insight into how supports operate collectively in everyday contexts. Although community resource systems span a wide range of services—including Home and Community-Based Services (HCBS), transportation, adult day programs, caregiver support, and neighborhood amenities—older adults, particularly those with disabilities, continue to experience substantial unmet needs. The absence of a universal HCBS infrastructure further shifts the burden of navigating fragmented supports onto individuals and families. Mental health care exemplifies these challenges, as significant barriers persist despite strong evidence for the effectiveness of late-life interventions (van der Auwera et al., 2017; Vasudev et al., 2019). Together, these limitations underscore the need for a more integrated understanding of community resources as components of a broader ecology of support.
A preliminary review of the literature across MEDLINE, PsycINFO, CINAHL, and Web of Science highlighted several recurring patterns. First, many studies on home- and community-based services focus on caregiver burden—emotional, financial, and logistical—rather than examining how older adults themselves access or use these supports. Second, community resources are frequently described in terms of isolated programs, with limited attention to coordination or integration across service domains. Third, much of the literature does not distinguish between older adults with and without disabilities, making disability-specific needs difficult to discern. Lastly, research in areas such as behavioral health often centers on particular clinical populations while paying less attention to systemic barriers such as transportation, insurance coverage, or geographic disparities. Together, these tendencies obscure how disability, chronic illness, and structural disadvantage intersect to shape resource access and use.
Despite increasing interest in aging in place, it remains unclear how community resources for older adults with disabilities and chronic conditions have been conceptually defined and empirically studied; which thematic dimensions (e.g., access, availability, utilization) have received the most attention; and whether existing research adequately captures the overlapping and intersecting needs of this population. Accordingly, this scoping review adopts a resource-centered perspective, synthesizing how community resources have been examined across diverse study designs and contexts, with particular attention to accessibility, utilization, quality, and effectiveness. This approach reflects the multifaceted and often co-occurring nature of aging-related impairments and assesses whether current research captures the complexity of needs in later life. By mapping which types of community resources have received empirical attention and how they have been studied, the review identifies the current scope of knowledge and key gaps for future work. The review is guided by the following research questions: RQ1: How does the literature conceptualize and categorize community resources for older adults with disabilities and chronic conditions? RQ2: How does empirical research examine these resources across dimensions such as accessibility, utilization, and quality—and what gaps remain?
Together, these questions allow us to synthesize how diverse strands of research define community resources, how these resources are measured and assessed, and where critical evidence gaps persist for older adults aging with functional limitations and chronic health needs.
Methodology
We followed the Patterns, Advances, Gaps, Evidence for Practice, Research recommendations (PAGER) framework (Patterns, Advances, Gaps, Evidence for practice, and Research recommendations) as outlined by Bradbury-Jones et al. (2022) to structure and synthesize key findings from this scoping review. The PAGER model facilitates a comprehensive interpretation of the literature by organizing insights in a way that highlights both conceptual contributions and areas for future inquiry.
Establishing the Parameters of the Scoping Review
Our review of access to community resources for older adults with late-life disabilities and chronic diseases was guided by key frameworks, including Person–Environment (P–E) Fit framework (Lawton & Nahemow, 1973). The review aimed to examine how community resources are conceptualized across the empirical studies included. Initially, our search terms focused on areas such as HCBS, chronic diseases, disability, and mental health conditions. After refining our inclusion criteria, we narrowed the search scope to studies providing empirical evidence on access to or quality of community resources. The review protocol was registered, and adherence to the PRISMA Extension for Scoping Reviews checklist (Tricco et al., 2018) is documented in Supplemental material 1. In this review, disability was operationalized using an inclusive approach encompassing functional impairments, mental health conditions, and chronic diseases that may limit daily activities and participation. This approach is informed by a multidimensional understanding of disability as arising from the interaction between individuals and their physical, social, and institutional environments (World Health Organization, 2001, p. 2023). Consistent with this interactional framework, disability is not a fixed attribute of the individual but arises from environmental, social, and structural barriers that shape opportunities for participation and therefore varies across settings depending on available opportunities and environmental constraints (Oliver, 1996). Accordingly, chronic disease is included insofar as it constrains functioning and participation within specific environmental contexts.
Search Strategy
A computerized literature search was conducted using a search strategy developed through an iterative process of selecting key search terms and identifying relevant databases. Keywords and subject headings related to age-related disabilities and chronic conditions as well as access to quality community resources were identified through preliminary searches. We searched four major databases, including MEDLINE, PsycINFO, CINAHL, and Web of Science, using combinations of keywords and controlled vocabulary related to “older adults,” “community resources,” “disability,” “chronic disease,” “accessibility,” and “aging in place.” (Supplemental material 2). In addition to database searches, we manually screened reference lists of included studies and consulted subject-matter experts with established research and practice expertise in aging, disability, and community-based services to identify potentially relevant studies not captured in database searches. These sources are included in the “other sources” category reported in Figure 1.
Study Selection
Studies were included if they met all of the following criteria: (a) published in English (b) published from 2010 onward. The 2010 threshold reflects a U.S. LTSS policy inflection point: the Affordable Care Act introduced new HCBS authorities (e.g., Community First Choice Option, Balancing Incentive Program) and accelerated state-level rebalancing toward community-based care (Kaye, 2012; Oyeka & Arora, 2023), (c) focused on adults aged 65 years and older (d) examined community resources (e.g., HCBS, social services, mental health services), (e) addressed disability or chronic disease in an aging population (f) were empirical and peer-reviewed, and (g) conducted in the U.S. Studies were excluded if they focused exclusively on institutional settings (e.g., nursing homes), or described interventions with no community component. Some studies were excluded despite addressing aging populations or community-level health disparities because they did not directly examine access to, availability, or utilization of community resources for older adults with disabilities or chronic diseases. These exclusions were necessary to maintain alignment with the review’s defined scope and population focus. Although older adults may experience diverse types of chronic illnesses and disabilities, this review does not aim to classify findings by condition-specific categories. Instead, it focuses on identifying the domains of community resource research that have received empirical attention in relation to aging with health-related vulnerabilities.
Screening was conducted in pairs by the seven co-authors, with any disagreements resolved through discussion or adjudication by a third reviewer. All authors participated in the screening process, with roles distributed across pairs to ensure consistency and reliability. The results of the search and study selection process will be reported in full and presented using a PRISMA-style flow diagram in the final scoping review (Tricco et al., 2018). Ultimately, 21 peer-reviewed articles were included, ensuring diverse representation across U.S. geographic contexts, types of community resources, and disability conditions within the evidence base. Figure 1 presents the full article selection process. PRISMA (Preferred Reporting and Identification for Systematic reviews and Meta-Analyses) flow diagram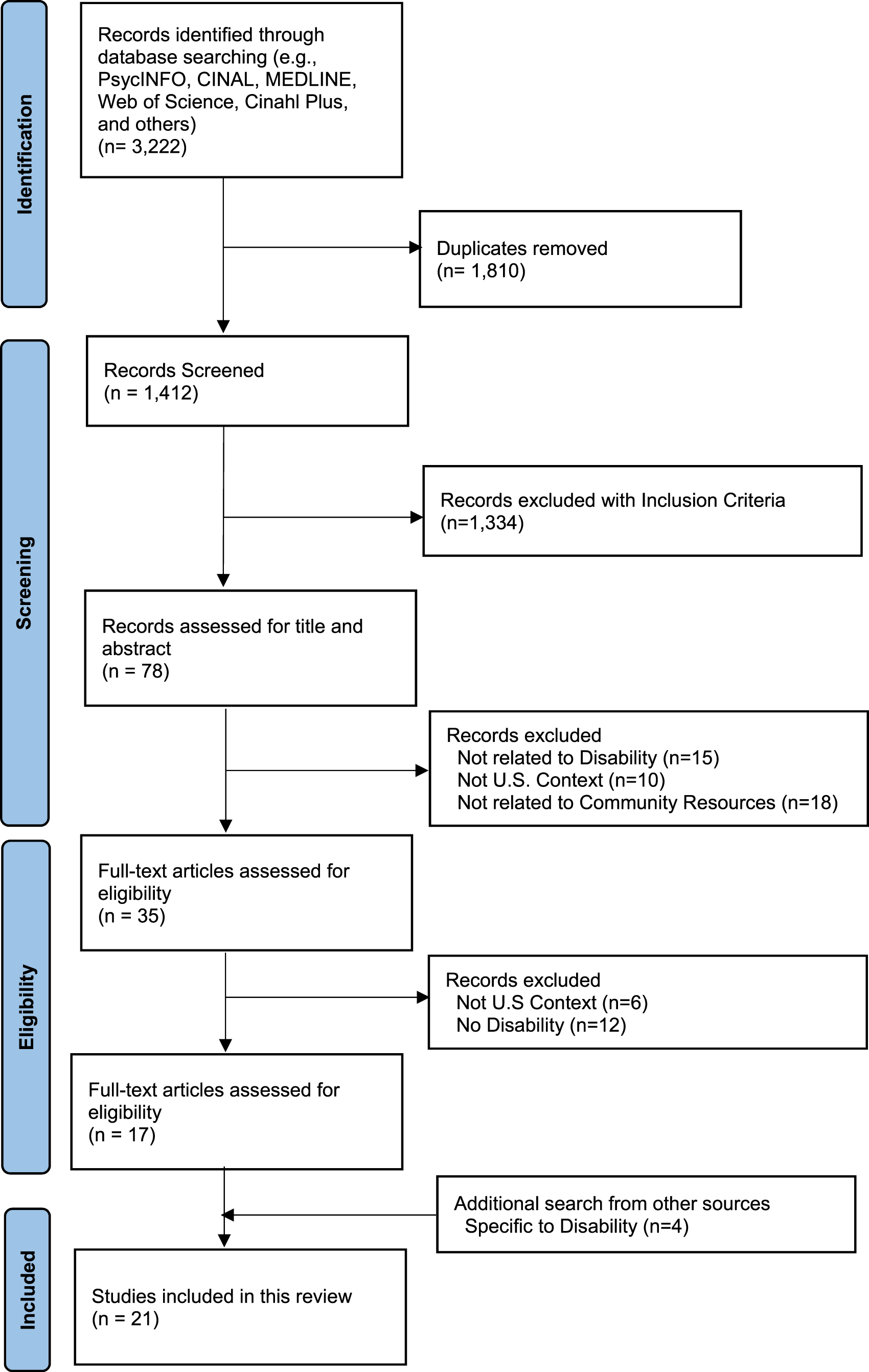
Charting the Data
Data extraction was conducted using a custom charting form, iteratively developed to capture the key elements of each study. This included author(s), year of publication, type of community resource(s) examined, place of residence, health condition, geographic scope of the study, study design, conceptual categories of community resources, and thematic focus of studies on community resources. The charting process was iterative and conducted collaboratively by the research team, with multiple rounds of refinement to ensure consistency and accuracy across these categories.
Collating, Summarizing, and Reporting Results
We used the PAGER framework to guide the interpretation of synthesized findings, enabling us to identify key patterns in the literature, advances in knowledge, evidence gaps, practical implications, and recommendations for future research. To support this process, we systematically collated and summarized data across the included studies, mapping conceptual, methodological, and thematic patterns. A descriptive analytical approach was employed to synthesize the evidence. Findings were then organized according to the two research questions, with specific focus on the conceptualization of community resources, dominant thematic dimensions, and cross-cutting barriers and disparities among different types of community-based supports.
Result
Before presenting findings related to RQ1 and RQ2, we first summarize the characteristics of the included studies to provide contextual background for interpreting patterns in how community resources are conceptualized and evaluated across the literature.
Sample Characteristics
A total of 21 studies met the inclusion criteria. A recurring pattern across the literature was the focus on community-dwelling older adults, including rural residents (Battista et al., 2015; Hay-McCutcheon et al., 2018), urban populations (Mathis et al., 2016; Rosso et al., 2013), and individuals living alone or in subsidized housing for low-income older adults (Lau et al., 2012; Park et al., 2019). Several studies also focused on Medicare beneficiaries, particularly those with chronic diseases or complex care needs (Andrilla et al., 2021; Chen et al., 2016; Gell et al., 2015; Sharma, 2014; Smith et al., 2019).
Across the included studies, there was a noticeable broadening in the range of health conditions examined. These included mental health disorders such as depression and anxiety (Andrilla et al., 2021; Gerlach et al., 2018), multiple chronic conditions (Chen et al., 2016; Li et al., 2023; Mathis et al., 2016; Smith et al., 2019), mobility limitations (Rosso et al., 2013; Satariano et al., 2016), and disability (Frochen et al., 2019; Gell et al., 2015; Li, 2016; Park et al., 2019). Sample sizes varied widely, ranging from small qualitative interviews with approximately 20 participants to large administrative datasets including over 1.9 million Medicare beneficiaries. The studies also differed in geographic scope, with some using national samples (Andrilla et al., 2021; Chen et al., 2016; Gell et al., 2015), others conducting statewide analyses (Battista et al., 2015; Gerlach et al., 2018; Li, 2016; Rahman et al., 2021), and several focusing on county-level analyses, including the spatial distribution of residential care facilities in Los Angeles County, California (Frochen et al., 2019) and the accessibility of subsidized senior housing and neighborhood resources in Chicago, Illinois (Park et al., 2019).
Study Characteristics
Most studies employed quantitative, cross-sectional designs using secondary data sources such as Medicare claims for older adults (Andrilla et al., 2021; Chen et al., 2016), the National Health and Aging Trends Study (Gell et al., 2015; Smith et al., 2019), and U.S. Census or American Community Survey data for ecological or Geographic Information System (GIS) analyses (Frochen et al., 2019; Hames et al., 2017; Park et al., 2019; Rahman et al., 2021; Smith et al., 2021; Thornton et al., 2016). GIS and spatial analysis methods were common, including hot spot analyses, GIS modelling, and regression examining associations between neighborhood factors and health outcomes in older populations (Battista et al., 2015; Frochen et al., 2019; Hames et al., 2017; Li, 2016; Li et al., 2023; Mathis et al., 2016; Park et al., 2019). Qualitative and mixed-methods designs were less common. For example, Lau et al. (2012) used in-depth interviews with Japanese American older adults living alone, and Battista et al. (2015) combined GIS analysis with interviews to study transportation barriers among rural residents. The majority of studies were cross-sectional, while a smaller number used cohort or longitudinal designs (Gauvin et al., 2012; Gerlach et al., 2018). This reflects a wide range of approaches for examining access to and quality of community resources for older adults in the United States.
Conceptual Categories of Community Resources
Across 21 studies, community resources were not defined through a single unified framework; instead, they were conceptualized in diverse ways—ranging from narrowly defined service infrastructures (e.g., provider density or facility proximity) to broader ecological systems that encompass social relationships, built environments, and organizational supports. These conceptual distinctions gave rise to notable operational differences across studies. Studies that defined community resources primarily in terms of service availability tended to rely on spatial or administrative indicators, such as provider proximity or the number of local programs. In contrast, studies informed by ecological or social frameworks emphasized factors such as community engagement, participation, and contextual relevance, often employing qualitative or mixed-method approaches. These differing conceptualizations influenced the selection of outcome measures, the assessment of program effectiveness, and the identification of resource types deemed essential for supporting aging in place.
Conceptual Categories of Community Resources
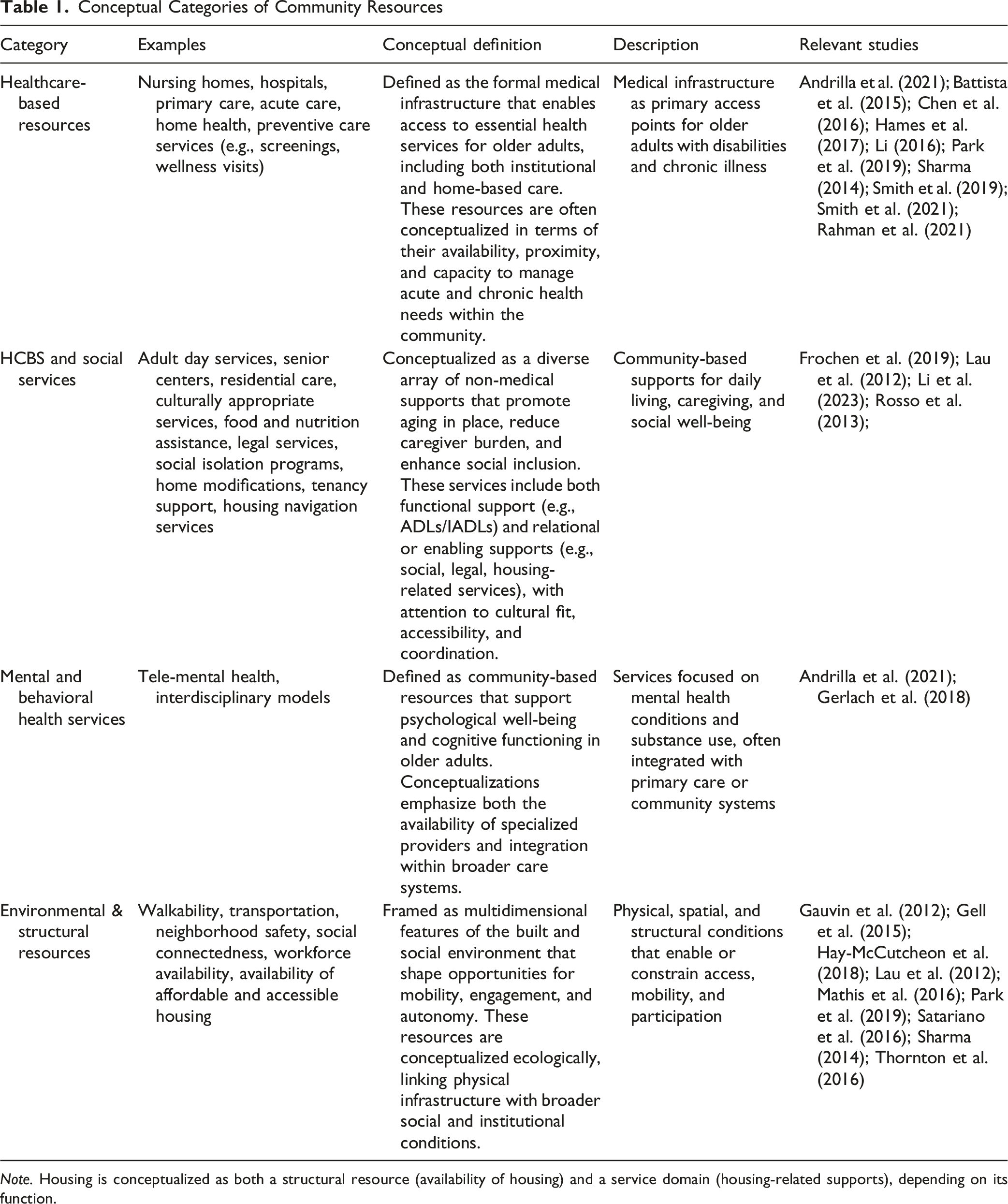
Note. Housing is conceptualized as both a structural resource (availability of housing) and a service domain (housing-related supports), depending on its function.
Healthcare-based resources were the most frequently emphasized domain, reflecting a medicalized orientation to “community” supports. Ten studies (Battista et al., 2015; Chen et al., 2016; Sharma, 2014; Smith et al., 2021) identified structural and spatial inequities in the distribution of providers and facilities, often mediated by geography, race, or income. These studies commonly relied on provider density, service proximity, or facility availability as proxies for community resource adequacy, positioning medical infrastructure as a core dimension of community capacity
A second major cluster of research conceptualizes HCBS and formal social services, which were conceptualized as integral to aging in place and a broader ecosystem of nonmedical care. Studies by Lau et al. (2012), Rosso et al. (2013), Frochen et al. (2019), and Li et al. (2023) illustrated how day programs, in-home services, and supportive housing not only supplement medical care but also provide social engagement, cultural continuity, and daily functioning. These studies underscore recurrent mismatches between service availability and the spatial distribution of vulnerable older adults with complex needs, highlighting persistent geographic inequities in supportive care.
Mental and behavioral health resources constituted a smaller, yet expanding, area of focus within the literature. Research such as Gerlach et al. (2018) and Andrilla et al.(2021) identified critical shortages of geriatric mental health providers, limited access to psychiatric care, and barriers to counseling and crisis services in rural and low-income communities. By treating psychological well-being as a core dimension of community support, this body of work expands the conceptualization of resources beyond physical health and social care. These studies highlight the need for more integrated mental health capacity in community settings to meet the needs of older adults with disabilities and chronic conditions.
Finally, environmental and structural resources such as walkability, neighborhood safety, transit access, and proximity to amenities were also conceptualized as enabling contexts for independence and participation. Built environment research (Gauvin et al., 2012; Mathis et al., 2016; Satariano et al., 2016) demonstrated how spatial features facilitate mobility and engagement which are critical for healthy aging. This stream broadens the concept of resources beyond services to include spatial justice and infrastructure equity. The literature advances an ecological understanding of community resources by integrating service-based and spatial determinants of health. GIS-based analyses (Frochen et al., 2019; Li et al., 2023) and neighborhood-level studies (Park et al., 2019; Sharma, 2014) demonstrate useful methodological approaches for mapping access and identifying systemic inequities.
Thematic Emphases in the Study of Community Resources
Thematic Focus of Studies on Community Resources
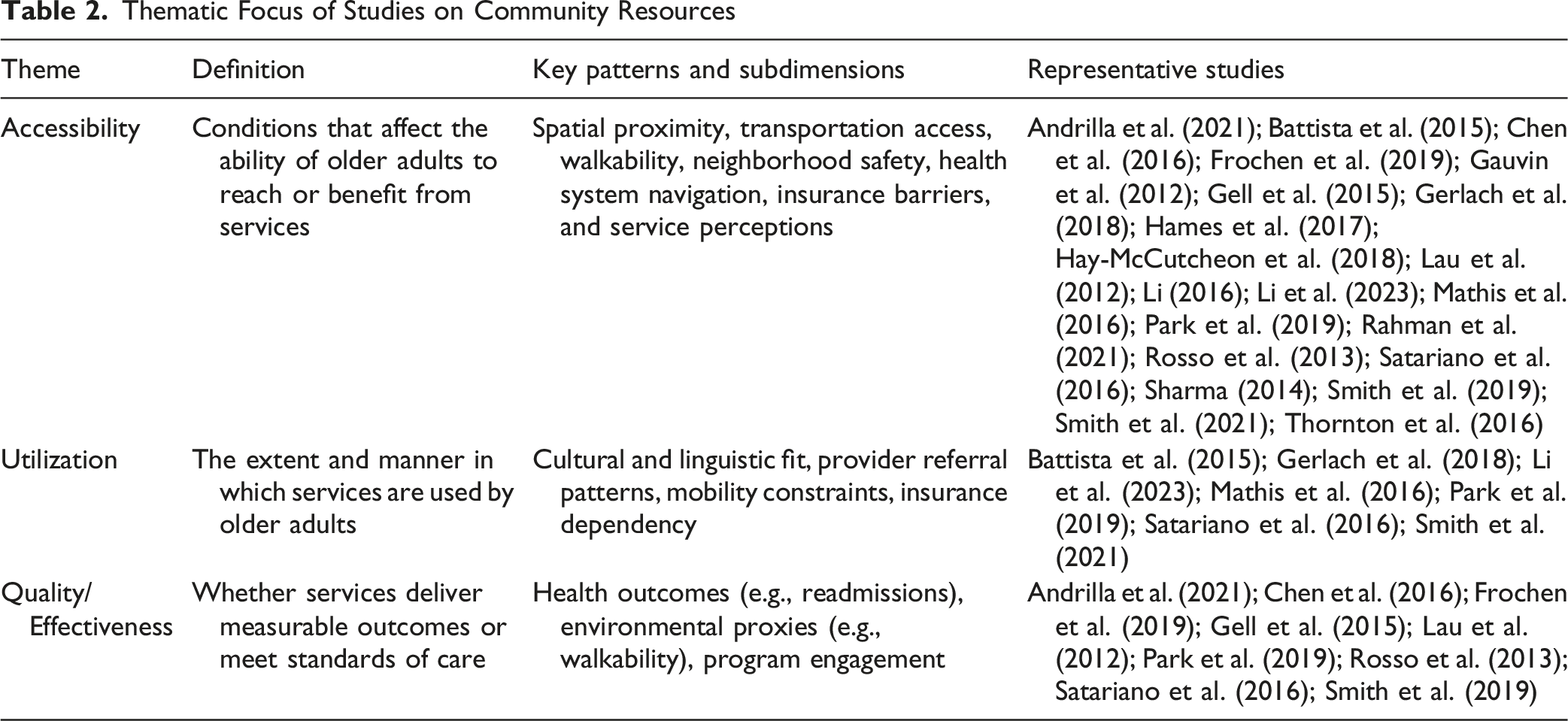
Accessibility and utilization together emerged as the most prominent focus across the studies, underscoring the central role of equitable access in shaping how older adults with disabilities and chronic conditions engage with community resources. Across contexts, barriers such as geographic distance, inadequate transportation, workforce shortages, and cultural or linguistic mismatches limited the meaningful use of available services (Battista et al., 2015; Lau et al., 2012; Li, 2016; Smith et al., 2019; World Health Organization, 2023). Environmental conditions, including neighborhood safety, walkability, and infrastructure, further influenced whether older adults could reach and consistently participate in community-based programs (Gell et al., 2015; Mathis et al., 2016; Satariano et al., 2016).
Patterns of service use reflected these same inequities. Older adults living in rural or socioeconomically disadvantaged areas consistently demonstrated lower participation in preventive and supportive services, even when facilities existed nearby (Chen et al., 2016; Sharma, 2014). Structural constraints such as limited insurance coverage, inflexible organizational practices, and high out-of-pocket costs often transformed nominal availability into functional inaccessibility. These findings highlight that accessibility and utilization are not separate dimensions but mutually reinforcing indicators of structural inequity within community care systems.
Quality and effectiveness received limited attention in the literature, yet studies that did examine these dimensions reported persistent disparities. Key issues included workforce shortages, uneven resource distribution, and culturally inappropriate care, especially in rural and underserved areas (Andrilla et al., 2021; Lau et al., 2012; Smith et al., 2019). These findings suggest that expanding access alone may not be sufficient to ensure equitable care for older adults. The absence of quality-focused research prompts critical reflection. It raises questions about how access is defined and whether the presence of services is assumed to equate to adequate care. If services are not effective, or not aligned with the needs and contexts of older populations, then access alone may offer limited benefit. These results point to the need for a more integrated understanding of accessibility, utilization, and quality as interconnected determinants of equity in aging services.
Discussion
This scoping review synthesizes U.S. research on how community resources for older adults with disabilities and chronic conditions are conceptualized and evaluated. Using the PAGER framework, we identify cross-cutting insights spanning theory and practice. Prior work shows that proximity to high-quality services supports mobility, independence, and aging in place (Gauvin et al., 2012; Rosso et al., 2013), yet structural and geographic inequities undermine equitable access. These patterns align with environmental gerontology perspectives that view aging outcomes as shaped by the interplay of social, material, and organizational dimensions of place (Oswald & Wahl, 2019; Rowles & Chaudhury, 2005).
Patterns
Two primary patterns emerged. First, community resources are typically examined within siloed domains—healthcare, HCBS, behavioral health, or environmental infrastructure—rather than as components of an integrated ecosystem (Andrilla et al., 2021; Frochen et al., 2019; Smith et al., 2021). Only a limited number of studies consider how health, social supports, and environmental conditions jointly influence outcomes (Sharma, 2014). Paired challenges such as mobility limitations and neighborhood walkability (Satariano et al., 2016) or heart failure and depression (Chen et al., 2016) are explored, but few studies address multiple interacting contextual factors. This pattern mirrors a broader tendency in aging research to treat physical, social, and service environments as discrete domains (Rowles & Chaudhury, 2005; Wahl & Oswald, 2010), despite evidence that neighborhoods are experienced as interwoven constellations of relationships, settings, and occupations (Cresswell, 2004; Dickie et al., 2006). From a disability perspective, this fragmentation obscures how participation restrictions—not impairments alone—shape everyday experience (Putnam et al., 2021).
Second, accessibility and utilization remain the most fully developed themes. Accessibility is influenced by spatial barriers, transportation shortages, workforce limitations, neighborhood safety, cultural and linguistic mismatches, and walkability (Battista et al., 2015; Hay-McCutcheon et al., 2018; Lau et al., 2012; Smith et al., 2019). Research on place reinforces that accessibility is also enacted through embodied routines and social interactions (Johansson et al., 2013; Prodinger et al., 2016). Utilization patterns mirror these inequalities: older adults in disadvantaged communities report lower engagement with health promotion, behavioral health, and social support services (Gerlach et al., 2018; Rahman et al., 2021), often due to financial constraints, administrative burdens, or stigma. These dynamics suggest that accessibility and utilization operate as interconnected mechanisms of structural inequality. Importantly, many studies measure impairment or functional decline but overlook participation (i.e., involvement in everyday life situations), a central construct in both the ICF framework and disability studies (Putnam et al., 2021; World Health Organization, 2001).
Financial and insurance structures are not peripheral but foundational determinants of access to community resources in the United States. The current evidence base largely treats barriers such as transportation, workforce shortages, and geographic availability as primary drivers of inequity, yet these operate within a deeper layer of financial stratification. In a system where long-term care coverage is fragmented and heavily means-tested, the ability to access community-based services is fundamentally conditioned by wealth and insurance status (Kaye et al., 2010; Miller & Thunell, 2024). Consequently, what appears as underutilization or service gaps may in fact reflect structural exclusion embedded within financing systems rather than failures of service supply alone. This underscores a critical gap in the literature: without incorporating financial access and policy context, assessments of community resource equity remain incomplete.
Advances
This review contributes by synthesizing fragmented evidence into a coherent account of how community resources are distributed, accessed, and experienced. Mapping geographic, demographic, and environmental data reveals consistent patterns of underutilization among rural, low-income, and racially marginalized communities (Frochen et al., 2019; Li et al., 2023; Smith et al., 2019). These findings parallel theoretical calls to examine aging within broader contextual ecologies (Wahl et al., 2012) and echo neighborhood-based insights that mobility, identity, and social participation emerge within lived contexts (Andrews et al., 2007; Rowles, 1983). Disability research similarly emphasizes participation—as opposed to clinical status—as a primary indicator of well-being in later life (Putnam et al., 2021).
A second advance is the gradual shift from documenting resource availability to assessing service effectiveness. Although most studies still prioritize presence or use (Gerlach et al., 2018; Smith et al., 2021), outcome-oriented approaches (Gerlach et al., 2018; Sharma, 2014) offer promising, if limited, evidence. Methodological innovations such as GIS-based mapping and spatial accessibility models improve the field’s capacity to quantify inequities and identify resource deserts. These approaches align with conceptualizations of place as layered across multiple scales—homes, neighborhoods, and service systems (Oswald & Wahl, 2019). For disability research, they create opportunities to analyze how resource environments interact with lifelong trajectories of impairment and adaptation.
Beyond thematic patterns, the literature has also evolved conceptually and methodologically in how community resources are examined. Methodologically, recent studies demonstrate greater sophistication, with spatial analytics such as GIS-based accessibility measures (Frochen et al., 2019; Li et al., 2023) enabling researchers to map resource deserts and identify geographic mismatches between need and supply. Telehealth and remote care models, including the SUpporting Seniors Receiving Treatment And INtervention (SUSTAIN) program (Gerlach et al., 2018), likewise represent innovations designed to mitigate geographic barriers and extend the reach of community-based supports.
Conceptually, the field has shifted from describing the mere presence of services to interrogating how structural and social contexts enable or constrain equitable use—marking an important move from availability-based to accessibility-centered frameworks.
A second methodological advance concerns how community resources have been examined across studies. Earlier research tended to employ single-dimensional indicators of resource availability, whereas more recent work incorporates spatial metrics, administrative data, and self-reported perceptions to capture multiple facets of resource environments. These heterogeneous operational approaches have meaningful implications for interpretation: studies relying on spatial indicators emphasize structural accessibility, whereas those using self-report measures capture perceived support, engagement, and environmental fit. Consequently, empirical findings reflect not only differences in resource conditions but also differences in how resources themselves were defined and measured.
Gaps
Major conceptual and empirical gaps remain. Most studies treat healthcare, social services, and the built environment separately rather than examining their interconnections. Few explore how overlapping constraints—particularly in behavioral health—shape access and outcomes, despite theoretical work describing place as an integrated constellation of material, social, and institutional forces (Wahl & Oswald, 2016). Research rarely assesses whether services lead to improvements in health, independence, or participation. Neighborhood scholarship demonstrates that mobility, social participation, and belonging emerge from multiple converging environmental features (Cresswell, 2004; Rowles, 2008), yet empirical studies seldom apply this insight.
From a disability standpoint, several gaps stand out: participation is infrequently measured; disability trajectories (aging with vs. aging into disability) are rarely distinguished; and older adults are often treated as a uniform group, masking disparities shaped by race, income, or disability (Putnam et al., 2021; World Health Organization, 2001). Intersectionality is seldom used to understand compounding disadvantage. Studies also overlook embodied and situated experiences—how disruptions to routines, social ties, and familiar environments shape engagement with community resources (Dickie et al., 2006; Johansson et al., 2013). Moving beyond ‘aging in place’to understand migration and aging: Place making and the centrality of occupation. Journal of occupational science, 20 (2), 108-119.). Theoretical models are underused, including ecological and neighborhood-based perspectives that conceptualize person–environment transactions as mutually constitutive (Dickie et al., 2006; Prodinger et al., 2016). The field lacks conceptual tools that account for the relational, contextual, and temporal dynamics of place, limiting understanding of how community resources function as components of dynamic support ecologies.
Evidence for Practice
These findings underscore the need to strengthen the broader support systems that sustain older adults’ health and independence. Viewing community resources as interconnected—rather than isolated—supports helps identify where systems can be made more inclusive and responsive. Workforce shortages and insurance gaps pose persistent challenges, but service-specific barriers reveal opportunities for targeted improvements that can meaningfully enhance daily functioning. A clearer understanding of how different resources operate and connect can improve coordination, reduce unintentional exclusion, and advance more equitable aging in place.
Improving accessibility requires more than expanding the number of services; it necessitates structural investments that ensure supports are usable, affordable, culturally appropriate, and aligned with older adults’ lived routines. Neighborhood and aging scholarship highlights that mobility, social participation, and engagement unfold through everyday occupations embedded within local environments (Cresswell, 2004; Dickie et al., 2006). This suggests that resources must not only exist but integrate into the rhythms of daily life. Studies provide instructive examples: churches offering emotional and practical support (Fields et al., 2016), senior centers fostering purposeful aging (Liao & DeLiema, 2021), and neighborhood planning connecting housing with services to enhance awareness and use (Bolkan et al., 2022; Choi, 2022). Collectively, these models highlight the importance of collaboration across public systems and community organizations to promote belonging, purpose, and dignity in later life. Emerging models such as Food as Medicine initiatives further illustrate how healthcare and social service domains can be integrated through nutrition supports. These programs link clinical care with services such as medically tailored meals and food assistance, with growing evidence of effectiveness and increasing coverage through Medicare and Medicaid. As such, they represent a promising example of how community-based resource systems can move toward more coordinated and person-centered models of care.
Limitations and Conclusion
Several limitations of this review should be acknowledged. First, the analysis was confined to studies conducted within the United States and published in English, which may limit the applicability of findings across diverse policy environments and cultural contexts. Search parameters and database scope may have also excluded relevant grey literature or studies not indexed in major repositories. Methodologically, the predominance of cross-sectional and observational study designs, including those using administrative claims data, limits the capacity for causal inference and constrains insights into how community resources evolve over time. Substantial heterogeneity in study designs, target populations, and outcome measures further complicates synthesis and reduces the potential for meta-inference.
This review shows that research on community resources for older adults with disabilities remains conceptually fragmented, often mirroring the structural silos of the care systems it examines. Synthesizing evidence across healthcare, HCBS, behavioral health, and environmental gerontology demonstrates that community resources function as interconnected ecologies of support that shape daily life, mobility, and social participation.
Availability alone is insufficient; the value of community resources depends on how accessibility, utilization, and quality interact to enable meaningful community living. This underscores the need to redefine community resources not as program inventories but as relational, place-based supports embedded in lived environments. Advancing the field will require theory-informed approaches that illuminate how functional capacities and environmental contexts jointly shape aging with disability. Incorporating ecological, intersectional, ICF, and neighborhood- and occupation-based perspectives can provide a fuller understanding of how older adults navigate community systems and where those systems must be strengthened to support equitable aging in place.
Supplemental Material
Supplemental material - Community Resources for Older Adults with Age-Related Disabilities and Chronic Conditions: A Scoping Review
Supplemental material for Community Resources for Older Adults with Age-Related Disabilities and Chronic Conditions: A Scoping Review by Oejin Shin, Ph. D, Sojung Park, Ph. D, Soobin Park, MSW, Sarah Sunghye Kang, MSc, Sunghei Han, MSW, MBA, Eunsun Kwon, Ph. D, Seoyeon Ahn, Ph D, BoRin Kim, PhD in Systematic Review or Meta Analysis.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.