
Abstract
This study examined the extent to which community-level welfare spending and community trust moderated the association between social isolation and suicidal ideation among older adults in South Korea. Using data from the 2017 Korean Community Health Survey (N = 64,853, aged ≥65), we analyzed three social isolation indicators (living alone, lack of contact, and limited social participation) with multilevel logistic regression with cross-level interactions. All three types of isolation were associated with increased suicidal ideation, with lack of participation showing the strongest effect. While community trust had a direct protective effect, only welfare spending buffered the adverse impact of limited social participation on suicidal ideation. These findings highlight that system-level protections like welfare spending are crucial for mitigating mental health risks in socially isolated older adults. Strengthening welfare-based community infrastructures may be essential for suicide prevention among older adults.
Reducing late-life suicide among socially isolated older adults is a pressing public health issue in rapidly aging societies. Although prevention efforts have primarily focused on individual-level risk factors (e.g., depression and economic hardship) (Lee, 2020; Yoon & Cummings, 2019), growing evidence suggests that the broader social environment is an important contributor to mental health outcomes (Kim & Park, 2021). Reflecting this global shift, South Korea has increasingly adopted community-based approaches in its national strategies, emphasizing the roles of local government and community resources. Notably, the Second Five-Year National Suicide Prevention Plan (2009–2013) prioritized locally tailored interventions over centralized models (Lee, 2020). This has prompted increased attention to multilevel strategies that examine how community-level characteristics, such as welfare spending and community trust, buffer mental health risks among socially isolated older adults. Accordingly, the question is not only who is at risk but also under what community conditions risk intensifies or diminishes.
Social Isolation and Suicidal Ideation in Older Adults
Social isolation, typically characterized by living alone, lack of contact with close others, and limited social participation, is a well-established risk factor for suicidal ideation among older adults (Fässberg et al., 2012; Pantell et al., 2013). Although living alone captures the absence of cohabiting family members, it does not fully reflect older adults’ social vulnerability. Relational characteristics therefore warrant joint consideration: frequency of contact reflects the quality of close ties and available support, whereas social participation captures broader network connections and engagement in social roles (Harasemiw et al., 2018; Stavrova & Ren, 2020; Ward et al., 2024). Several mechanisms have been proposed that link social isolation to poor psychological well-being in older adults. First, socially isolated older adults often lack emotional, instrumental, and financial support, as smaller networks and less frequent contact reduce support availability (Harasemiw et al., 2018). Second, reduced contact decreases opportunities for routine monitoring and timely assistance with health management (Tucker, 2002). Third, isolation constrains social engagement, potentially fostering existential insecurity and a weakened sense of oneself as a ‘social being’, which are closely associated with suicidal ideation (Eades et al., 2019). Together, social isolation heightens suicide risk by intensifying psychological distress and undermining protective factors (e.g., social support and a sense of belonging) (Fässberg et al., 2012). Accordingly, identifying community-level resources that buffer these pathways is crucial for reducing the impact of social isolation on suicidal ideation.
Community Welfare Spending and Community Trust as Buffering Factors
Guided by an integrated ecological-sociological framework, we conceptualize suicide risk as shaped by interactions between individual vulnerabilities and broader community contexts. Ecological systems theory underscores that individual mental health is embedded within multiple environmental layers (Bronfenbrenner, 1979), while Durkheim’s theory highlights the roles of social regulation and social integration in conditioning suicidal risks (Durkheim, 1951). Within this framework, we operationalize social regulation as community welfare spending—reflecting macrosystem capacity to provide public goods (Esping-Andersen, 1990)—and social integration as community trust, representing cohesive bonds at the mesosystem level (Kawachi, 2006).
Welfare spending captures institutional investments that stabilize individuals’ lives through formal support (Esping-Andersen, 1990). By alleviating financial strain and improving access to services, it can buffer the mental health consequences of isolation. This may be especially salient in East Asian contexts such as Korea, where suicide risk is closely tied to socioeconomic inequality; community-based services (e.g., home-visit programs) can partially substitute for limited informal support (Chen et al., 2009). Empirical evidence also shows that institutional support reduces health disparities and mitigates the negative impact of low socioeconomic status (Bergqvist et al., 2013). Specifically, higher community-level welfare spending in Seoul has been associated with reduced mental health disparities among older adults (Ha & Nam, 2022). Relatedly, in a nationwide multilevel study, the protective association between community-level welfare expenditure and depressive symptoms was more pronounced among Korean older adults living alone than among those living with others (Lee et al., 2025).
Community trust functions as an informal contextual buffer by increasing perceived availability of support and community safety, reinforcing a broader sense that others are reliable and help is available (Kawachi, 2006; Kim & Park, 2021). High-trust communities may therefore mitigate the existential insecurity associated with isolation (Abrutyn & Mueller, 2016). Furthermore, such communities often benefit from stronger collective efficacy and informal social control, which can effectively monitor and support vulnerable residents (Kawachi, 2006). Evidence further indicates that higher community trust alleviates the emotional toll of isolation and attenuates its negative effects on depression among older adults (Takagi & Shimada, 2019). Consistent with these findings, Noguchi et al. (2017) demonstrated that community-level mistrust was associated with increased suicidal ideation, particularly among individuals experiencing psychological distress.
Although Durkheim’s theory underscores social regulation and integration as pivotal to suicide risk, identifying contemporary indicators for these constructs is essential. To date, research on community welfare spending and community trust has largely proceeded in isolation, overlooking the potential interplay between formal and informal resources. As Korea’s welfare regime expands, the formal sector may redefine the utility of informal assets. Specifically, the ‘crowding-out’ hypothesis suggests that expansive welfare provision might inadvertently weaken informal ties, whereas a ‘crowding-in’ effect posits that formal services could bolster social trust (Stadelmann-Steffen, 2011). This study addresses these dynamics by examining how institutionalized regulation (community welfare spending) and mesosystem integration (community trust) uniquely buffer the isolation–suicide link. By doing so, we extend Durkheim’s framework to test whether tangible institutional commitments can compensate for the diminishing protective power of traditional social bonds in a rapidly changing society.
Korea offers a particularly relevant context given the high levels of social isolation and suicide among older adults. In 2017 (our study year), 54.4% of older Koreans reported no participation in social clubs over the past year and participation in hobby clubs and civic organizations was below 5% (Ministry of Health and Welfare, 2017). Furthermore, the suicide rate among older adults reached 58.6 per 100,000 in 2017—the highest among OECD countries (Korea Foundation for Suicide Prevention, 2017). Examining whether community welfare spending and community trust buffer the psychological consequences of social isolation is, therefore, policy-salient and theoretically motivated. Although previous Korean studies consistently link social isolation to suicidal ideation (Kim & Min, 2020), multilevel analyses of cross-level buffering effects remain rare. Existing research has predominantly relied on individual-level indicators (e.g., living alone) (Kim & Min, 2020) or municipal-level aggregates that cannot capture individual-context interactions (Lee & Kang, 2020). While recent multilevel designs suggest protective effects of community welfare spending and cohesion on mental health (Ha & Nam, 2022; Kim & Park, 2021), their risk-modifying (buffering) effects have not been systematically examined.
The Present Study
Building on the evidence suggesting the advantages of community welfare spending and community trust in reducing health inequalities (Ha & Nam, 2022; Noguchi et al., 2017), this study examines their buffering roles in the relationship between social isolation and suicidal ideation among older Koreans. Welfare spending is defined as municipal-level expenditures on social welfare programs (e.g., public assistance, older-adult services), consistent with Korea’s local budget classification system and reflecting local capacity for social regulation. Community trust is defined as a local-level social capital indicator, measured as the proportion of residents reporting trust in their neighbors within each administrative area (si/gun/gu).
Analyses are conducted at the municipal (si/gun/gu) level, the primary local governance unit for implementing health and welfare policies in South Korea (Kang et al., 2015). We utilize multilevel modelling with cross-level interaction terms to assess whether community-level factors significantly attenuate the negative effects of individual-level social isolation on suicidal ideation (Aguinis et al., 2013; see Figure 1). This cross-level approach helps identify community conditions that mitigate individual suicide risk, providing a more nuanced framework for prevention. By providing empirical evidence on the buffering roles of community resources, this study offers practical insights for healthy aging policy. Conceptual model of the study (adapted from Aguinis & Edwards, 2014)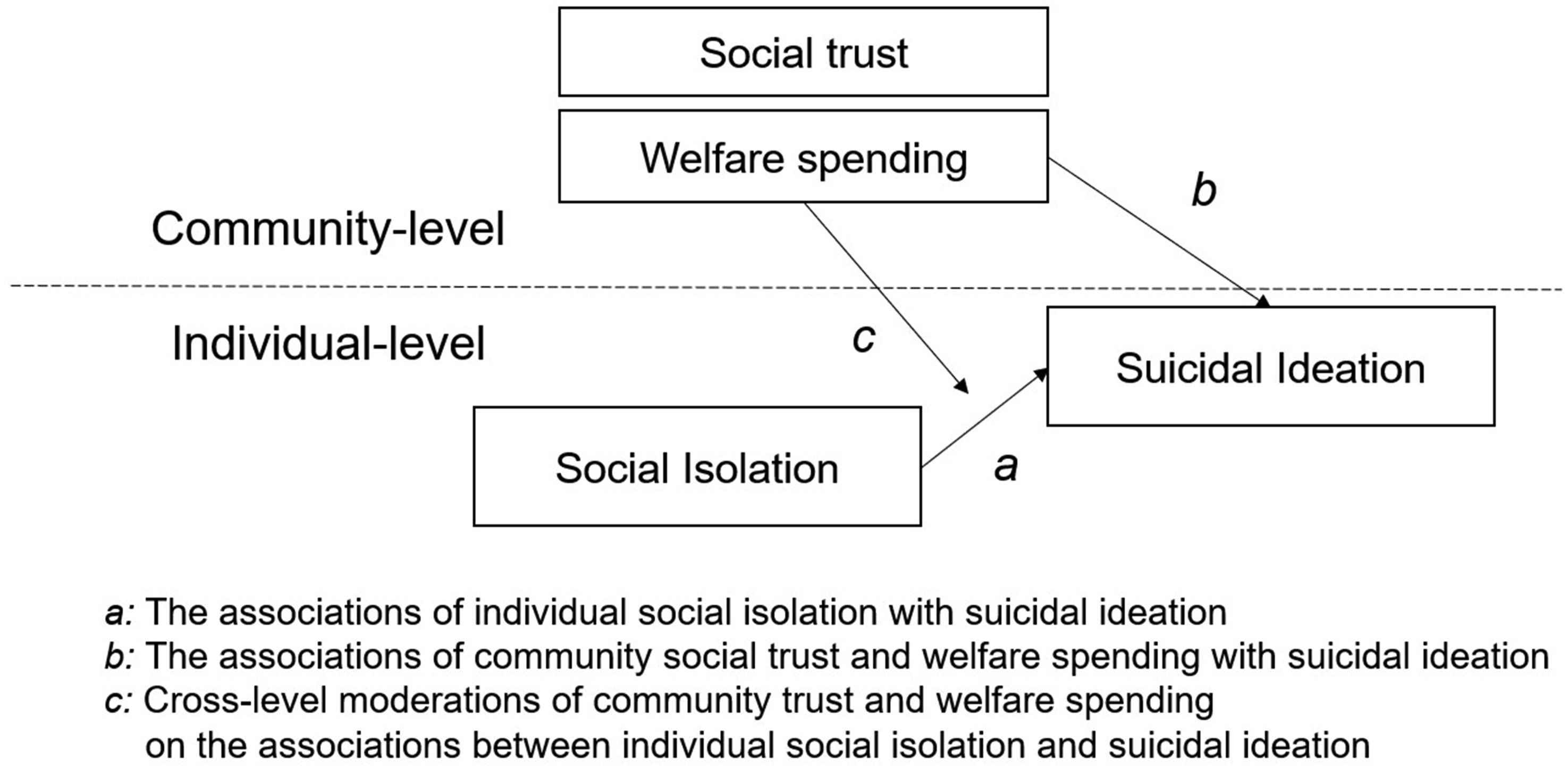
Methods
Data and Sample
Descriptive Statistics of the Individual-Level Variables
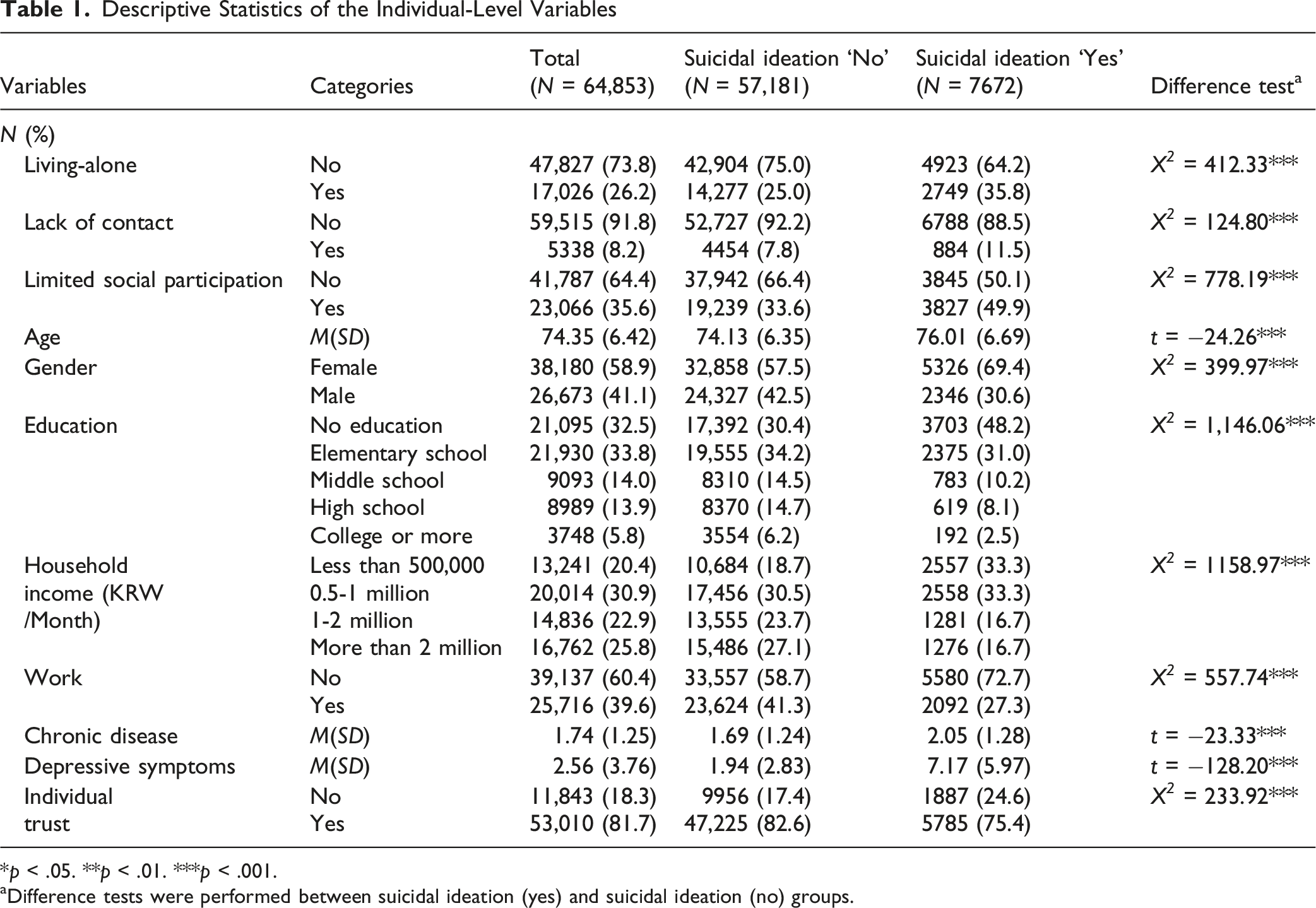
*p < .05. **p < .01. ***p < .001.
aDifference tests were performed between suicidal ideation (yes) and suicidal ideation (no) groups.
Community-level variables were drawn primarily from 2015 sources: community trust from the KCHS, and welfare spending and other control variables from regional statistics provided by the Korean Statistical Information Service (Statistics Korea, 2015). Using community-level measures from two years prior ensures temporal precedence of community context over individual-level variables, reducing simultaneity bias. Such lagged design is consistent with conceptualizing community resources as stock variables that influence later individual outcomes, thus representing a conservative modelling approach (Nauenberg et al., 2011).
Although more recent KCHS waves exist, the 2017 wave was utilized as it is the most recent year containing concurrent measures of social isolation and suicidal ideation. Furthermore, using pre-pandemic data avoids the potential confounding impact of COVID-19 on social trust and mental health. As individualism, social conflict, and distrust have intensified since the pandemic (World Health Organization, 2021), focusing on pre-COVID conditions helps clarify enduring community-level resources relevant for future interventions. Ethical approval for this research, which utilized public data, was obtained from the Institutional Review Board at Yonsei University.
Measures
Suicidal Ideation
Suicidal ideation was measured using a binary item, ‘Have you ever thought of wanting to die in the past year?’ (1 = yes, 0 = no). Although this binary item does not capture the severity of suicidal thoughts, it is a standard approach in large-scale population studies for identifying psychosocial risk and facilitating comparability across research (Pantell et al., 2013). In our data, this item showed convergent validity, as it was significantly correlated with depressive symptoms (measured by the PHQ-9; r = .451, p < .001) and perceived stress, the latter of which was measured by a single item asking participants to rate their overall level of stress in daily life on a 4-point scale (r = .298, p < .001).
Social Isolation
Social isolation was measured using three indicators: living alone, lack of social contact with family or friends, and limited participation in social activities. First, living alone (1 = yes, 0 = no) served as a proxy for the absence of a co-resident family member (Berkman & Syme, 1979). Second, lack of social contact was assessed by the frequency of in-person and non-physical interactions (e.g., calls or texts) with relatives, neighbors, and friends. Participants reporting no interaction in the past week were coded 1; all others were coded as 0. This one-week threshold aligns with the “low contact” criteria of the Berkman-Syme Social Network Index (Berkman & Syme, 1979), which has been used to identify individuals at high risk of social isolation (Stavrova & Ren, 2020). Third, limited social participation was assessed via the frequency of participation in religious activities, leisure activities, volunteering, and social gatherings (e.g., alumni associations, senior centers, and family meetings) in the past year. Participants reporting no participation in any activity were coded as 1, indicating social disengagement—detachment from normative social roles and essential community resources (Stavrova & Ren, 2020); otherwise, 0. Each indicator was dichotomized to identify individuals with significantly limited social connections, consistent with Korean geriatric studies (Park, 2010). This approach is well suited to population-based research, as the most substantial gains in well-being occur when moving from “no contact” to “any contact”, rather than from moderate to high levels of interaction (Stavrova & Ren, 2020). To ensure the stability of our findings, we re-estimated the models using alternative measures of social isolation: a continuous score for contact frequency and an ordinal variable for participation (higher values indicating greater engagement). This confirmed whether defining social isolation as a binary deficit remains robust compared to continuous scales.
Welfare Spending
Community welfare spending was calculated as the proportion of social welfare expenditure to the total local government budget using 2015 regional statistics. This measure, commonly used in studies on social expenditure and health disparities, accounts for differences in regional size and fiscal capacity (Kim & Park, 2021) and captures the extent to which local governments prioritize welfare in their policy agendas (Lee, 2020; Park, 2023). The social welfare budget in Korea encompasses general welfare—such as programs for basic livelihoods, older adults—and public health expenditures (Ministry of the Interior and Safety, 2023).
Community Trust
Community trust was operationalized as a community-level social capital indicator by aggregating residents’ responses to the 2015 KCHS item, “People in my neighborhood can be trusted” (1 = yes, 0 = no). Responses from participants (aged ≥19) within each administrative unit (si/gun/gu) were aggregated to calculate the proportion reporting neighborhood trust. Although trust is reported at the individual level, community aggregation is a well-established method for estimating community-level social capital (Kawachi, 2006). The intraclass correlation coefficient (ICC = .069) and group-mean reliability (λ2 = .986) demonstrate a stable and reliable representation of regional contexts.
Control Variables
Individual-level control variables from the 2017 KCHS included age (M = 74.35, SD = 6.42), gender (0 = male, 1 = female), education (1 = no education to 5 = college or more), household income (8 monthly gross income categories; 1 = ≤ 500,000 Korean Won (KRW) to 8 = ≥ 6,000,000 KRW), work status (1 = working, 0 = not working), chronic diseases count (0-5; e.g., hypertension, diabetes, dyslipidemia, arthritis), depressive symptoms (Patient Health Questionnaire-9 (Kroenke et al., 2001) summed scores, range: 0-27, α = .84), and neighbor trust (1 = trusting neighbors, 0 = not trusting neighbors). Because trust can operate at both individual and community levels, we controlled for individual-level trust to assess contextual effects of aggregated community trust beyond individual perceptions (Kawachi, 2006).
Community-level control variables included urban-rural status (1 = urban, 0 = rural), local population size, and the proportion of older adults (≥65 years). We also adjusted for local socioeconomic and fiscal conditions using the proportion of public assistance recipients (poverty proxy), per capita gross regional domestic product (GRDP), and the financial independence rate (FIR) of local governments. Data for all community-level control variables were retrieved from the Korean Statistical Information Service (Statistics Korea, 2015) and the Local Finance Integrated Open System (Ministry of the Interior and Safety, 2015). These variables account for socioeconomic characteristics of communities that may independently influence individuals’ mental health and suicide risk (Denney et al., 2015; Park, 2023), ensuring more conservative estimates of the buffering effects of welfare spending and community trust.
Data Analysis
We performed a series of multilevel logistic regressions with cross-level moderation analyses. Following Enders and Tofighi (2007), individual-level explanatory variables were group-mean centered, and community-level variables were grand-mean centered. Prior to model building, we evaluated multicollinearity among all core variables using variance inflation factors (VIFs) computed from auxiliary regressions conducted separately at the individual and community level. All VIFs fell below the conventional threshold of 10 (Kutner et al., 2004) at both the individual level (range = 1.03–1.44; mean = 1.20) and the community level (range = 1.22–6.18; mean = 3.54), indicating no evidence of severe multicollinearity. The relatively higher community-level VIFs—for the proportion of older adults aged 65 years and older (6.18) and community trust (5.08)—likely reflect the expected intercorrelation among area-level indicators. We then estimated a null (intercept-only) model to assess the appropriateness of the multilevel structure. To allow a focused interpretation of each cross-level interaction while preserving statistical power, the three social isolation indicators—living alone, lack of social contact, and limited social participation—were modeled separately (Aguinis et al., 2013). Consequently, six models (models 2–7) were tested, each including a cross-level interaction term between one isolation indicator and one community-level moderator (either community welfare spending or community trust).
Random slopes for each isolation indicator were estimated to assess variance across communities. Given the significance of random slopes, cross-level interaction terms were included to test the buffering effects of community welfare spending and community trust. Odds ratios (ORs) were estimated for every 10% increase in the proportion of community welfare spending and community trust (Noguchi et al., 2017). The final model is as follows:

Results
Descriptive Statistics of the Community-Level Variables
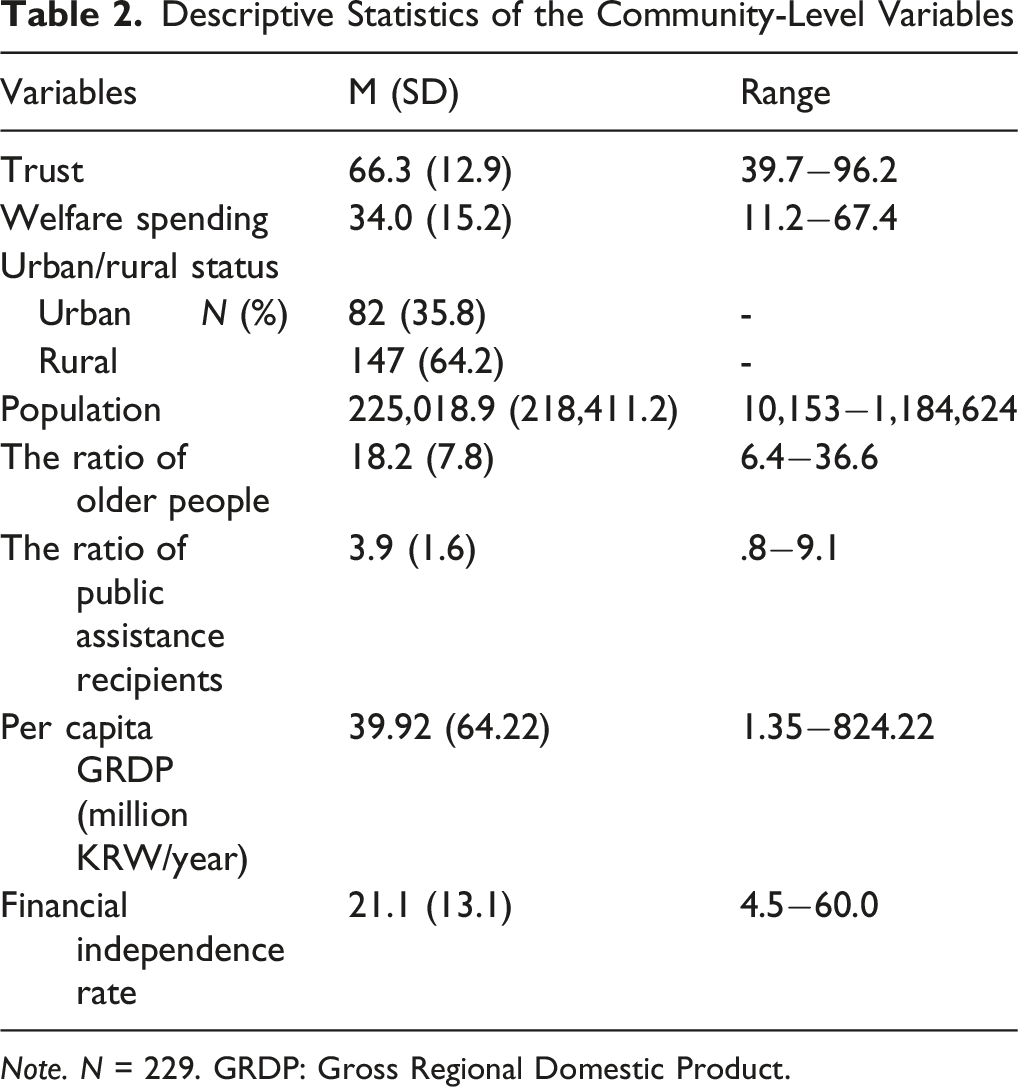
Note. N = 229. GRDP: Gross Regional Domestic Product.
Results of Multilevel Logistic Regression Analyses (Odds Ratios)
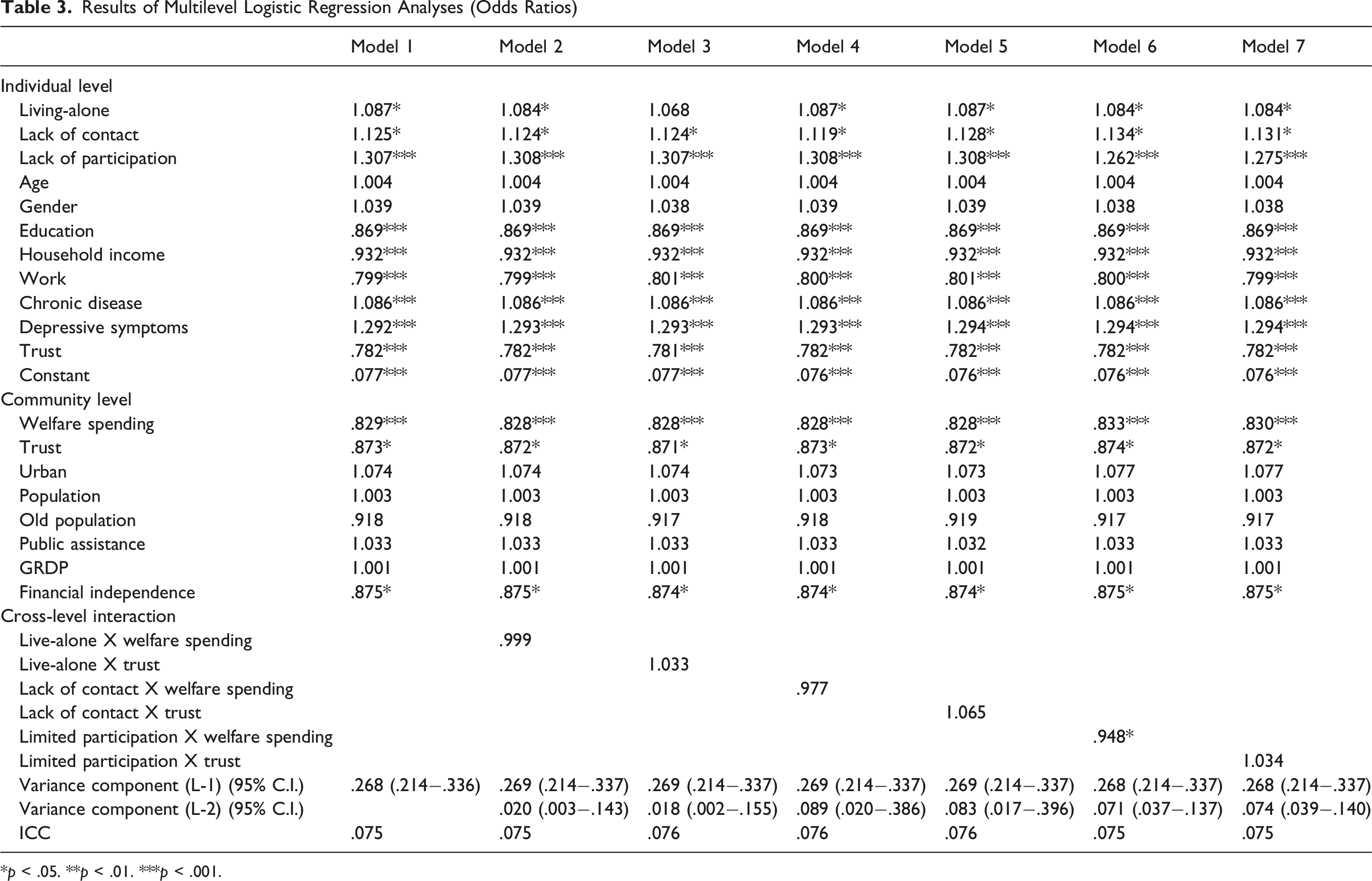
*p < .05. **p < .01. ***p < .001.
Random slope tests for all three social isolation indicators were significant, justifying the inclusion of cross-level interaction terms. Moderation analyses revealed that community welfare spending significantly attenuated the relationship between limited social participation and suicidal ideation (Model 6: OR = .948, p = .036). However, welfare spending did not significantly moderate the effects of living alone and lack of contact (Models 2 and 4). Furthermore, community trust showed no significant moderating effect in any model (Models 3, 5, and 7).
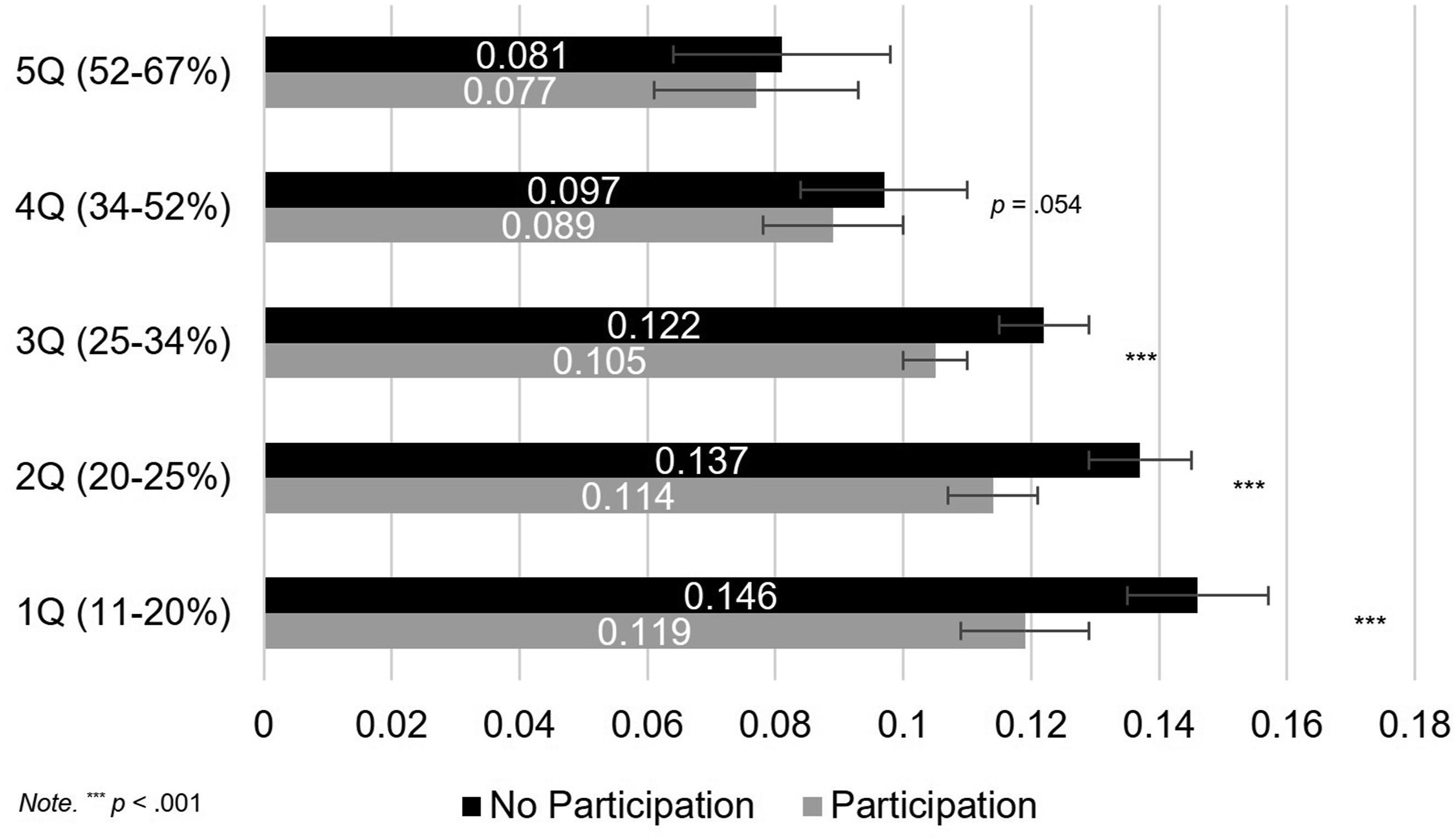
To further examine the significant cross-level moderations, we estimated ORs and marginal probabilities across quintiles of community welfare spending. As shown in Figure 2, the OR for suicidal ideation linked to limited social participation gradually decreased as the community welfare spending ratio increased. Notably, the detrimental effect of limited social participation was highly significant in lower-spending areas (1Q-3Q, p < .001), became only marginally significant in 4Q (p < .10), and was non-significant in the highest-spending districts (5Q, p > .05). Figure 3 presents the marginal probabilities of suicidal ideation. In communities with the lowest welfare spending (1Q), predicted probability was highest, showing a significant disparity (p < .001) between individuals with and without social participation. However, as the welfare spending increased, this gap diminished and was non-significant in 5Q (p > .05). Estimated odds ratios (ORs) for lack of participation by quintile of community welfare spending Marginal probabilities of suicidal ideation by quintile of community welfare spending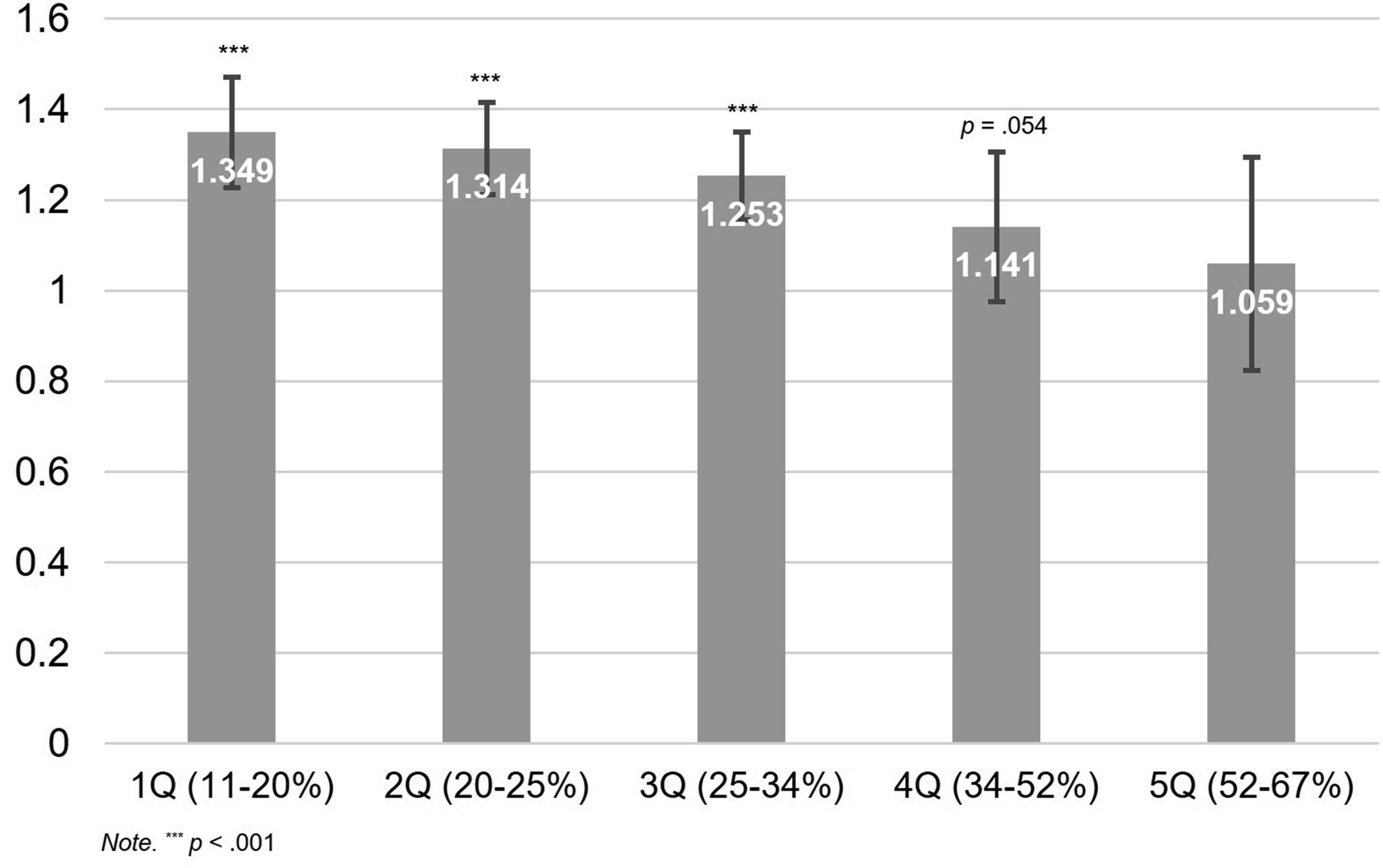
We estimated the predicted probability differences and standardized effect sizes to further evaluate the interaction (Table S1). In the lowest welfare spending quintile (1Q), socially isolated older adults had a 2.6 percentage point higher predicted probability of suicidal ideation (p < .001). This gap narrowed to a non-significant 0.3 percentage points in the highest quintile (5Q). Furthermore, a one-standard-deviation increase in welfare spending (SD = 15.2) was associated with a 0.74 percentage point reduction in the suicidal risk gap between isolated and non-isolated older adults (p = .015). Figure 4 illustrates the marginal effects of social disengagement on suicidal ideation significantly decrease as the community welfare spending increases from −1 SD to +1 SD (dy/dx = .027 and .010, respectively). The substantial decline in the marginal effect slope indicates that higher local welfare spending functions as a critical buffer, effectively mitigating the heightened suicide risk associated with social isolation in later life. Marginal effect of limited social participation on suicidal ideation across welfare spending level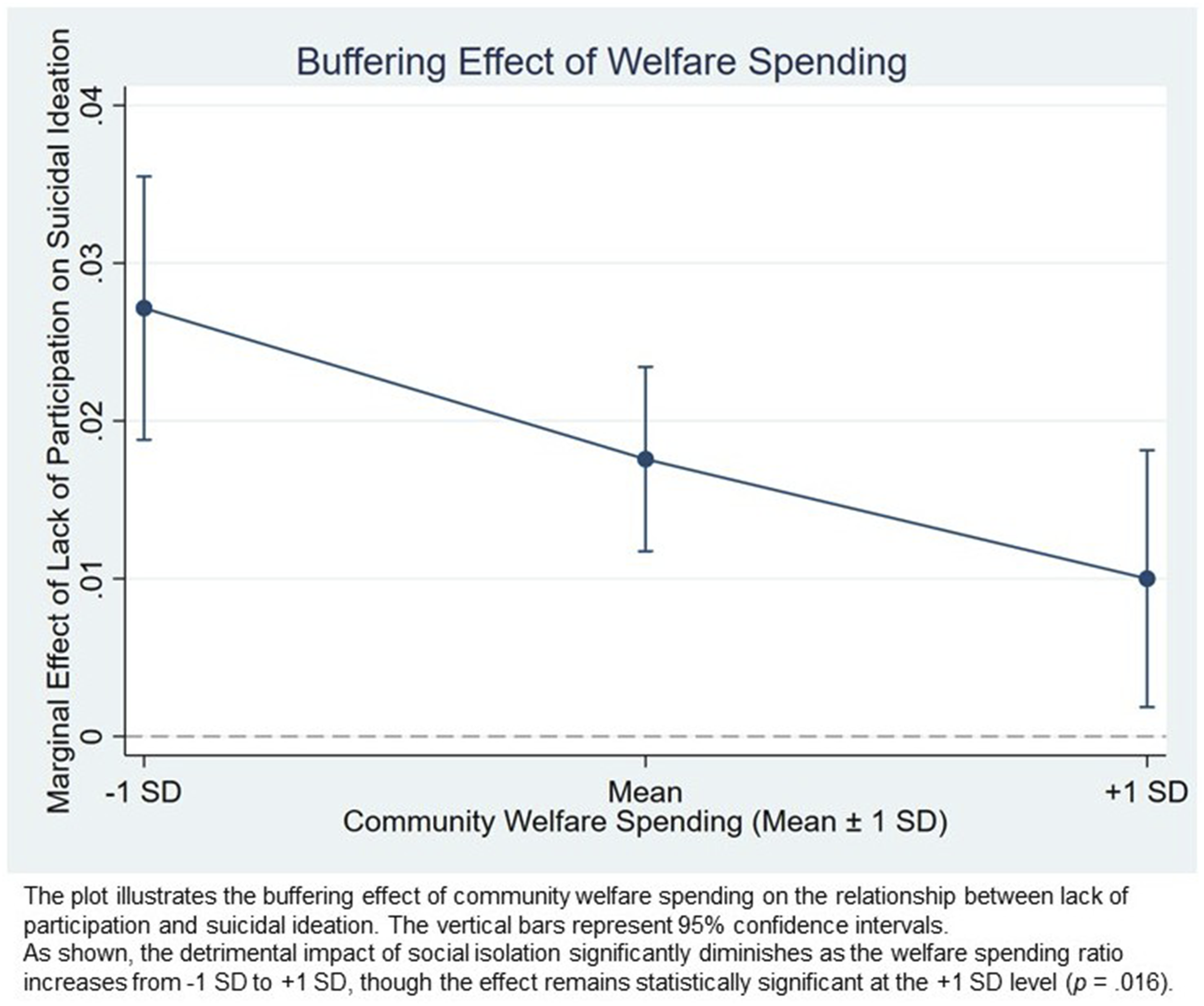
We also examined heterogeneity of the moderating effects by conducting stratified multilevel analyses by gender, age group (65-74 vs. 75+ years), education, and region (urban vs. rural). The buffering effect of community welfare spending was particularly strong among the old-old (75+; OR = .934, p < .05) and the higher-education group (middle school or above; OR = .915, p < .05). Furthermore, the results were marginally significant among females (OR = .954, p = .080) and older adults in rural areas (OR = .873, p = .073). The point estimate was largest (furthest from 1) among rural residents, although it did not reach conventional levels of statistical significance. We found no evidence of buffering among those aged 65–74, males, or urban residents. Full estimates are reported in Table S2 in the online supplementary materials.
Discussion
This study investigated the extent to which community-level resources, specifically community welfare spending and community trust, moderated the association between individual-level social isolation and suicidal ideation among older Korean adults. Using a nationally representative sample and multilevel models, we found that social isolation—measured by living alone, lack of social contact, and limited social participation—was significantly associated with elevated risk of suicidal ideation. We also found that community welfare spending significantly attenuated this risk, whereas community trust showed no comparable buffering effect. These findings suggest that prioritizing community welfare spending can be a key strategic target for preventive interventions aimed at reducing suicide risk among socially isolated older adults.
Our results indicate a robust association between social isolation and suicidal ideation among older Korean adults. Specifically, living alone, lack of social contact, and limited social participation each independently heightened risk, underscoring that regular social relationships and active social engagement are crucial for safeguarding older adults’ mental health (Franklin et al., 2017; Pantell et al., 2013). Older adults experiencing multiple forms of social isolation are particularly vulnerable, likely due to greater stress exposure, diminished access to emotional and instrumental support, and a weakened sense of social identity (Fässberg et al., 2012). In the Korean context, where both social isolation and suicidal ideation are prevalent, these findings point to integrated strategies that combine person-level outreach with ongoing community investment in welfare programs that facilitate social connectedness, civic participation, and timely service access.
Notably, among the social isolation indicators, limited participation in social activities showed the strongest association with suicidal ideation, highlighting the critical role of active social engagement in promoting older adults’ mental health. This finding supports the view that social engagement involves more than the mere presence of relationships; it requires sustained involvement in meaningful roles, such as volunteering, small-group programs, and ongoing community participation, both of which provide access to psychosocial resources buffering against depression and loneliness (Fässberg et al., 2012). Studies have consistently shown that social engagement helps individuals feel valued, fosters a sense of belonging and life purpose, and can significantly reduce the risk of suicidal thoughts (Eades et al., 2019; Franklin et al., 2017). Accordingly, prevention efforts should prioritize infrastructure that makes social participation accessible and rewarding, especially for marginalized individuals who are least likely to self-enroll.
Cross-level moderation analyses revealed that the adverse effects of limited social participation were significantly buffered in communities with higher welfare spending. These findings suggest that low social participation does not inherently translate into psychological risk in communities with stronger welfare support. The standardized estimates also indicate meaningful public health gains: higher welfare spending narrowed the suicide risk gap between isolated and non-isolated older adults. Greater welfare investments can improve the availability and affordability of social infrastructure—such as extended community center hours, staffed outreach and home-visiting, transportation subsidies—thereby lowering barriers to engagement. It may also help address the structural inequalities underlying mental health disparities among older adults (Bergqvist et al., 2013; Lee & Kang, 2020). Specifically, such investments improve access to essential resources, such as basic living necessities, housing improvements, and caring services, thereby fostering a more equitable distribution of well-being across the population (Bergqvist et al., 2013; Ha & Nam, 2022). Together, this more inclusive environment enables isolated older adults to re-integrate into community life and strengthens their resilience to psychological distress and suicidality (Yoon & Cummings, 2019).
Our findings remained robust across several sensitivity analyses. Specifically, the protective effect of welfare spending was consistently observed regardless of whether social isolation was measured as ordinal or continuous variables, or when additional confounders (e.g., perceived neighborhood reciprocity, prior suicide attempts, and senior center density) were controlled. Notably, while the buffering effect held for the welfare spending ratio, it was not significant for absolute per capita spending or GRDP-based indicators. This suggests that the protective mechanism is driven by relative local budget priorities—reflecting a community’s strategic commitment—rather than the absolute spending level.
It is also important to note that the buffering effect of welfare spending varies across demographic groups, supporting both the ‘vulnerability-sensitivity’ and ‘resource-utilization’ perspectives. This heterogeneity may be understood through two complementary perspectives. The significant effect observed among the old-old, together with marginal effects observed among females and rural residents, is broadly consistent with a vulnerability-sensitivity perspective, whereby socially vulnerable groups may benefit most from local welfare efforts. At the same time, the significant effect observed among older adults with higher educational attainment also points to a resource-utilization perspective, highlighting the role of policy literacy in navigating and using available services. Community welfare spending may also confer broader community benefits beyond direct service use. Residing in a community with a high welfare spending may strengthen perceived security and community satisfaction, providing an additional layer of protection.
Based on these findings, we propose three targeted policy actions. First, the community-based outreach programs should be expanded. As isolation-prevention efforts grow, local governments can mobilize residents as “gatekeepers” to maximize the reach of welfare resources. For example, Jongno-gu’s ‘Crisis Household Re-monitoring Team,’ leverages local residents and public-private partnerships to identify households at risk for solitary death and provide care services (e.g., hospital accompaniment) (Seoul Senior Welfare Center, 2025). Second, the welfare spending ratio should be institutionalized as a core Age-Friendly Community Indicator to guide municipal budgets, especially among older adults, for whom welfare spending appears most protective (World Health Organization, 2015). Third, the nationwide implementation of “Community Integrated Care” in 2026 provides a critical platform to institutionalize locally accountable welfare delivery. To make this actionable, local governments must adopt geographically differentiated resource allocation strategies. Our findings show that welfare spending’s buffering effect is particularly pronounced in rural areas. Therefore, policy-makers should prioritize outreach resources and community-care budgets for rural municipalities, where private social services are scarce. In urban settings, welfare spending should focus on diversifying social participation channels for the old-old and female seniors, who showed higher vulnerability. By using local welfare spending ratios as an evidence-based benchmark, the 2026 framework can move beyond a universal mandate to targeted interventions that address specific disparities between urban and rural communities.
Our findings also showed that although higher community trust was directly associated with lower suicide ideation, it did not significantly buffer the association between social isolation and suicidal ideation. This result diverges from previous studies suggesting that social capital can mitigate vulnerabilities in later life (Choi & Jun, 2022; Noguchi et al., 2017). A plausible explanation is that although community trust may foster a general sense of psychological safety, it cannot substitute for tangible, service-based supports needed to alleviate distress arising from limited social participation (Semmer et al., 2008). In an increasingly individualized society, community trust alone may be insufficient to buffer the risks of isolation. This lack of a moderating effect may suggest a weakening of traditional bonds in South Korea, where informal networks are no longer sufficient to perform their conventional protective roles. While the ‘crowding-out’ hypothesis often suggests that formal welfare may displace informal support, our findings rather imply that in the context of eroding social capital, institutionalized welfare acts as a necessary ‘functional substitute’ rather than a deterrent. Specifically, South Korea scored the lowest in the social support domain of the OECD Better Life Index, suggesting gaps in community-based support (OECD, 2017, p. 381). Consequently, tangible institutional commitments may be more effective in promoting social integration than a sole reliance on intangible community-building efforts.
A few limitations should be acknowledged. First, suicidal ideation was measured using a single binary item, limiting our ability to capture severity or distinguish ideation from active suicidal planning or attempts. Although this is common in large-scale surveys, future studies involving high-risk populations should utilize multi-item scales, such as the Geriatric Suicidal Ideation Scale (GSIS), to better characterize severity and reduce ceiling/floor effects. Second, social isolation was also measured using binary indicators, which may oversimplify the multifaceted nature of social connectedness. Future research incorporating multidimensional measures—such as perceived loneliness or the quality of relationship—could provide additional insights that complement the structural dimensions examined in this study (Ward et al., 2024). Third, although this study attempted to establish temporal ordering by incorporating earlier community-level data, its cross-sectional design limits causal interpretation. Longitudinal research is needed to more rigorously examine the proposed pathways. Fourth, while this study examined overall community welfare spending, future research would benefit from disaggregated data, such as budgets specifically targeting social isolation in older adults to capture more targeted welfare dynamics. Finally, findings based on older Korean adults may not be generalizable across cultures, underscoring the need for further cross-cultural research.
Despite these limitations, this study advances understanding of how community environments can shape individual mental health risks. By demonstrating that community welfare spending buffers the adverse effects of limited social participation on suicidal ideation, this study highlights the vital role of community-level fiscal investment in promoting older adults’ mental health. For policymakers and practitioners, these findings underscore the importance of multilevel interventions that simultaneously address individual and community-level resources to reduce suicidality among older adults. Ultimately, our findings suggest that a community’s commitment to social welfare can transform a potentially high-risk context into a more protective one. Future research should examine how informal social capital and institutional resources jointly influence mental health trajectories over time in older adults.
Supplemental Material
Supplemental material - Social Isolation and Suicidal Ideation Among Older Adults in Korea: The Role of Community Welfare Spending and Community Trust
Supplemental material for Social Isolation and Suicidal Ideation Among Older Adults in Korea: The Role of Community Welfare Spending and Community Trust by Bomi Choi, Susanna Joo, and Hyoun K. Kim in Research on Aging
Footnotes
Author Note
This research is based on the author’s doctoral dissertation under the supervision of Professor Hey Jun Jung.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available in the Korean Community Health Survey (https://chs.kdca.go.kr/chs/main.do). Community-level data are available in the regional statistics of the Korean Statistical Information Service (https://kosis.kr/) and the Local Finance Integrated Open System (![]() ).
).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.