
Abstract
Employing a multi-method approach, we investigated observed and parent-rated child behavioral inhibition (BI) and maternal reports of their own negative affectivity (NA) as predictors of young children’s internalizing problems. Participants were 201 children who were siblings between 2.5 and 5.5 years of age (mean = 3.86, standard deviation = 1.04) and their mothers. Due to the nested research design, multilevel model-fitting analyses were used to examine associations between predictors and internalizing problems, and to test a mediational process between maternal NA and internalizing problems. High levels of both observed and parent-rated child BI and greater maternal NA significantly predicted internalizing problems. Child age also moderated the association between parent-rated child BI and internalizing problems, with the association stronger for younger and mean age children, but not for older children. Additionally, parent-rated child BI was found to mediate the association between maternal NA and internalizing problems, and the mediational effect was stronger for younger children.
Keywords
Introduction
A considerable amount of research has focused on associations between the child temperament dimension behavioral inhibition (BI) and internalizing problems. Early internalizing problems put children at risk for mood and anxiety disorders, substance abuse, and even potentially suicide (Krueger, 1999; Roza, Hofstra, van der Ende, & Verhulst, 2003). Previous studies have established links between family factors and child behavior problems; however, they tend to focus on a very specific domain such as parental depression and parenting styles. Generally, maternal disposition to negative emotions is an under-explored factor in child behavioral research, and a limited number of studies have investigated direct/indirect associations between this maternal characteristic and child temperament and behavior problems (Crawford, Schrock, & Woodruff-Borden, 2011). Studying this construct from a broad, domain-level perspective can help clarify how maternal behavior influences BI and internalizing problems. The presence of maternal negative affect in early childhood may be a family-level risk factor for behavioral maladjustment, and in turn the development of internalizing psychopathology.
Behavioral inhibition or fearfulness is a temperament dimension that reflects individual differences in reactions to unfamiliar stimuli, and is often manifested as inhibited and withdrawn behavior in the presence of strangers or in novel situations (Kagan, Reznick, Clarke, Snidman, & Garcia-Coll, 1984). BI is also thought to be an involuntary process. Eisenberg et al. (2004) used the term reactive control to describe the automatic responses (as opposed to effortful control) in controlling certain impulses, and reactive overcontrol is linked with inhibited behaviors. The social and behavioral consequences of BI have been widely studied in the literature, and multiple studies have reported BI as a primary predictor of childhood internalizing problems and related psychological disorders (e.g., Degnan & Fox, 2007; Morris et al., 2002; Steinberg & Fox, 2009). Eisenberg et al. (2001, 2009) found that pure internalizing problems (not co-morbid with externalizing problems) were associated with reactive overcontrol (or BI). Relatedly, social anxiety disorder is more prevalent among inhibited children than uninhibited children (Biederman et al., 2001).
Typically, internalizing problems increase with child age longitudinally, particularly in middle to late childhood (Bongers, Koot, van der Ende, & Verhulst, 2003, Gilliom & Shaw, 2004). However, links between BI and internalizing problems are complex and may be more or less significant at different stages of childhood, and in the presence of certain environmental factors. For example, in a longitudinal study Williams et al. (2009) found an interesting interaction whereby high BI children showed increased levels of internalizing problems at age 4 but lower levels in later childhood and adolescence than low BI children, yet they did not provide a plausible explanation. Other findings suggest that high BI children are at higher risk for becoming targets of peer victimization and developing social anxiety (e.g., Coplan et al., 2013; Wichstrøm, Belsky, & Berg-Nielsen, 2013); however, decreases in withdrawal behaviors are also prevalent if high BI children experience less peer inclusion (Rubin, Coplan, & Bowker, 2009). Because exposure to peers tends to increase with age in early childhood, it would be interesting to see how BI influences internalizing problems across age during this period of development before children enter school. Surprisingly, little is known about the interaction pattern between BI and age in predicting internalizing for preschool-aged children, particularly from a multi-method perspective.
As previously suggested, maternal negative affectivity (NA) is a family-level variable that may have an impact on the development of child BI and internalizing problems. Watson and Clark (1984) defined NA as a high-order mood dispositional dimension that reflects pervasive individual differences in negative emotionality and self-concept. Individuals high in NA tend to experience more intense levels of negative mood states such as nervousness, tension, and worry. More specific sub-constructs of NA include trait anxiety, low self-esteem, and neuroticism (Watson & Clark, 1984).
Maternal NA may influence children in various ways. From a temperamental perspective, Vaughn, Bradley, Joffe, Seifer, and Barglow (1987) suggested that maternal characteristics could be viewed as a primary source of individual differences in child temperament. They found that maternal factors such as anxiety level and personality assessed in the prenatal stage predicted infant temperament (Vaughn et al., 1987). Multiple investigations have also revealed genetic links between parent characteristics and child temperament, including BI (DiLalla, Kagan, & Reznick, 1994; Sheese, Voelker, Rothbart, & Posner, 2007). On the other hand, maternal NA could influence child BI through environmental influences such as parenting. Multiple studies have indicated that parenting moderated the link between maternal personality and BI (Fox, Henderson, Marshall, Nichols, & Ghera, 2005; Prinzie, Stams, Dekovic, Reijntjes, & Belsky, 2009), and it is possible that NA (more specifically neuroticism) may amplify life stresses that undermine parenting (Bornstein, Hahn, & Haynes, 2011). From a psychopathological perspective, maternal NA and its sub-constructs could also influence the development of behavioral problems in children, either directly or indirectly. Degnan and Fox (2007) proposed a resilience model in which parent personality could be one of the contextual factors that interacts with BI in relation to child anxiety disorders. In an empirical study, Feng et al. (2008) found maternal depression moderated the link between preschooler’s BI and emotion regulation. There are fewer investigations that directly examined maternal NA or trait-like constructs. One recent study found an indirect relationship between maternal characteristics (including negative affect and neuroticism) and child internalizing problems, with effortful control as a mediator (Crawford et al., 2011); however, the study was limited by a relatively small sample size (N = 65) and questionnaire-only design. In a meta-analytic review, Lovejoy, Graczyk, O’Hare, and Neuman (2000) suggested that it is broadband NA rather than depressive symptoms alone that lead to maladaptive parenting observed among depressed mothers. Therefore, examining broadband NA and relations with child BI would be particularly useful for investigators conducting developmental research on child behavior problems and family factors.
Another important consideration in studies of BI is the typically limited measurement strategy. Parent-report questionnaires are the most commonly used assessments in temperament investigations. These ratings are easy to collect, provide rich information on child behaviors based on daily observations, and usually have high internal reliability (Rothbart & Goldsmith, 1985). However, parent reports can be biased due to possible projections of parent personality on item responses (Rothbart & Hwang, 2002). Parental reports of child temperament can also be influenced by parental mental health conditions, such as depressive or anxiety symptoms (Mebert, 1991; Vaughn, Taraldson, Crichton, & Egeland, 1981). Other types of response biases in questionnaire measures may also apply, such as social desirability and contrast effects, and the tendency to exaggerate differences between twins/siblings (Saudino, 2003). As a complement to parent ratings, researchers have been successfully incorporating structured laboratory assessments into temperament studies (e.g., Durbin, Hayden, Klein, & Olino, 2007; Kagan, Reznick, & Snidman, 1987). The behavioral approach allows researchers to capture detailed parameters of temperament as compared to the global perspective in parent reports. However, Goldsmith and Gagne (2012) suggested that there are difficulties differentiating state- and trait-like behaviors and ruling out environmental influences in the laboratory setting. Thus, using a multi-method approach by combining both types of assessment is thought to be more comprehensive and accurate in temperament investigations (Gagne, Van Hulle, Aksan, Essex, & Goldsmith, 2011; Hwang & Rothbart, 2003).
The Current Study and Hypotheses
The aim of the current study was to investigate the relationship between maternal NA, child age, BI, and internalizing problems. We focused on maternal NA as a broadband construct, which is a composite variable derived from maternal depression, neuroticism, trait anxiety, and current negative affect state. We used a multi-method approach with both laboratory and parent ratings. In addition, instead of assessing a single child, we examined sibling pairs within each family. This approach increases power to detect potential effects and also allows for the examination of how much of the variance in child traits was due to family environment (sibling interactions) (Krull, 2007). Because of the nested nature of the data, regression analyses were conducted with multilevel models.
We hypothesized that higher levels of maternal NA and child BI would predict internalizing problems (including both anxious-depressed and withdrawn problems). Based on the Williams et al. (2009) findings, we also hypothesized an interaction between BI and age in predicting internalizing problems. Specifically, the link between higher BI and internalizing problems would be stronger in younger than older children. Additionally, we proposed a multilevel moderated mediation model (Figure 1) to further explore the relationship between higher maternal NA and internalizing problems. Child BI would partially mediate the relationship between maternal NA and child internalizing problems, providing evidence of an indirect relationship between mother and child. Because of the hypothesized interaction between BI and age, we also expected the mediation effect to be stronger for younger than older children.
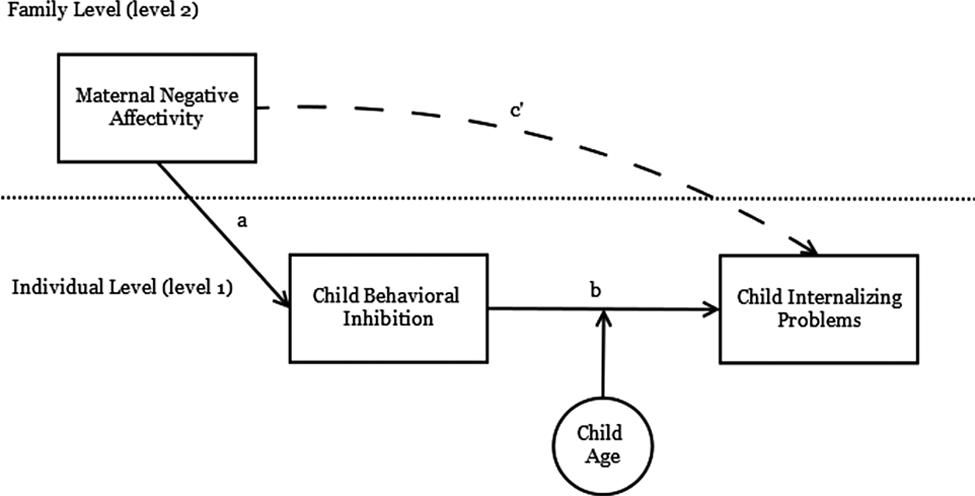
The conceptual presentation of the proposed multilevel moderated mediation model.
Method
Participants
Participants in this study included 100 English-speaking families with two or three siblings (N = 201) between 2.5 and 5.5 years of age (mean age = 3.86, standard deviation (SD) = 1.04). Participants included 104 boys (mean age = 3.77 years, SD = .99) and 97 girls (mean age = 3.96, SD = 1.08). The sample comprised 57 full sibling pairs, 10 monozygotic twin pairs, 32 dizygotic twin pairs, and 1 set of triplets. Regarding racial distribution, 13% of children, 7% of mothers, and 8% of fathers were reported as Hispanic or Latino. Participants in the sample were predominately white (84% children; 88% mothers; 87% fathers), followed by individuals identified with more than one race (11% children; 5% mothers; 4% fathers) and African American individuals (4% children; 4% mothers; 7% fathers). Less than 3% of the families reported themselves as Asian American, Pacific Islander, and other races. The average annual household income was approximately $70,000, ranging from $20,000 to over $200,000, and mean parental education (in years) was 15.82 for mothers and 15.12 for fathers, ranging from 8 to 22.
Procedure
Families from the Dallas–Fort Worth Metroplex (an area encompassing both cities as well as the surrounding suburban areas) were recruited using flyers on campus, pediatricians’ offices, day care centers, and Internet postings. Qualified participants with two children in the proper age range completed a series of online surveys using SurveyMonkey (https://www.surveymonkey.co.uk/). Of the 126 families who completed the online surveys, 100 families also agreed to participate in a subsequent 1–2 hour laboratory visit. The laboratory visit included a series of behavioral and cognitive assessments which were described to the children as “fun games.” Parents were asked to fill out additional questionnaires regarding child behavioral problems and parent anxiety during the visit. Participants received a $25 gift card for completing all online surveys, and they were compensated with another $50 gift card upon completion of their laboratory visit. All procedures were reviewed and approved by the University Institutional Review Board.
Measures
Laboratory assessment of behavioral inhibition
Child BI was measured observationally with the Laboratory Temperament Assessment Battery-Preschool Version (Lab-TAB, Goldsmith, Reilly, Lemery, Longley, & Prescott, 1995) Stranger Approach episode. In this episode, the experimenter instructs the child to stand by the wall waiting for him/her to return and then leaves the test room. Subsequently, a stranger wearing a dark blue sweatshirt and sunglasses enters and greets the child. The stranger gradually approaches the child while maintaining a neutral facial expression and tone. The stranger greets the child and asks the child a list of questions such as “Are you having fun today”, “What’s your favorite game?”, and, etc. If the child refuses to answer, the stranger pauses and proceeds to the subsequent question. Finally, the stranger makes an excuse to leave and the experimenter returns to the test room. The behavioral coding was carried out based on a modified version of the preschool Lab-TAB coding protocol (Goldsmith et al., 1995). The 2-minute episode was divided into 7 to 8 discrete 10-second trial epochs marked by each question across the timeline. Intensity levels of facial fear, distressed vocalizations, activity decrease, approach/escaping behaviors, and verbal hesitancy were coded on a 0 to 3 or 0 to 2 (verbal hesitancy) interval. Frequencies of nervous fidgeting and latencies to first fear response and vocalizations were also counted in percentages and number of seconds, respectively. Coders were trained to reach at least 80% absolute agreement with master coders before proceeding to code independently. A subsample of 40 cases was rated by a separate coder, and the median inter-rater reliability indexed by intra-class correlation coefficient (ICC) was 0.89.
Parent report measures of behavioral inhibition
The Toddler Behavior Assessment Questionnaire – Revised (TBAQ-R; Goldsmith, 1996) is a 120-item parent-rated questionnaire that assesses multiple dimensional traits of child temperament. The TBAQ-R social fear subscale was used to measure BI as it represents a parallel to the Lab-TAB Stranger Approach episode. The TBAQ-R contains items describing child behaviors in specific situations, and parents rate these behaviors based on the frequency of occurrence over the previous month. For example: “When one of the parents’ friends who did not have daily contact with your child visited the home, how often did your child talk much less than usual?” All items are formatted in a 7-point Likert scale that ranges from 1 (“never”) to 7 (“always”). The internal consistency for the 10-item social fear subscale was 0.86, and it typically ranges from 0.83 to 0.87 (Goldsmith, 1996).
Parents also reported on child temperament using the Emotionality Activity Sociability temperament scale (EAS; Buss & Plomin, 1984). This 20-item scale captures four major dimensions of temperament: emotionality; activity; shyness; and sociability. The items are general statements (e.g., “Child likes to be with people”) about the child, and parents respond on a scale of 1 (“strongly disagree) to 5 (“strongly agree”). The shyness and sociability subscales were used in the current study to assess BI. Cronbach’s alpha was 0.75 for the 5-item shyness subscale, and 0.89 for the 5-item sociability measure. Published internal consistencies for these sub-constructs range from 0.80 (emotionality) to 0.88 (shyness) (Rowe & Plomin, 1977).
Maternal negative affectivity
We measured maternal negative affectivity with four different scales on relevant specific constructs: depressive symptoms; trait anxiety; and neuroticism. Mothers reported their depressive symptoms on the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). Items include cognitive, emotional, behavioral and positive affect attributes rated on a 4-point Likert scale from 0 (“rarely or none of the time/less than 1 day”) to 3 (“most or all of the time/5–7 days”). Sample item includes “I felt that people disliked me.” The Cronbach alpha was 0.84, with published internal consistencies ranging from 0.84 to 0.90 (Radloff, 1977).
Mothers rated their trait anxiety with the State-Trait Anxiety Inventory (STAI; Spielberger et al., 1970). The current study used the A-Trait subscale on the STAI, which includes 20 statements describing general feelings (e.g., “I have disturbing thoughts”) with a 4-point Likert scale from 1 (“almost never”) to 4 (“almost always”). The Cronbach alpha was 0.90, and it typically ranges from 0.86 to 0.95 (Spielberger, 1989).
The Big Five Inventory (BFI; John & Srivastava, 1999) neuroticism subscale was used to assess neuroticism as a relevant NA measure. Participants were asked to rate statements describing the self (e.g., “worries a lot”) on a scale from 1 (“disagree strongly”) to 5 (“agree strongly”). The Cronbach alpha was 0.81 with a typical range of 0.75 to 0.90 (John & Srivastava, 1999). We also measured mothers’ current negative affect with the negative affect subscale in the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). Participants respond to a series of words (e.g., “upset”, “ashamed”) describing their current feelings and emotions on a 1 (“very slightly or not at all”) to 5 (“extremely”) Likert scale. The reliability of the 10-item negative affect scale was 0.86, and it was consistent with the typical range of 0.84 to 0.87 (Crawford & Henry, 2004).
Internalizing problems
Child internalizing problems were assessed with the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2000). The CBCL is a standard 100-item questionnaire that measures children’s socio-emotional functioning and behavioral problems. Parents were asked to rate their child’s behaviors in the past two months on a scale from 0 (“not true”) to 2 (“very true or often true”). The anxious–depressed problem and withdrawn problem subscales, as well as the broadband internalizing problem scale were used in the current study. Sample items include “Gets too upset when separated from parents”, and “Avoids looking others in the eye.” Cronbach’s alpha was 0.87 for the 36-item internalizing problems, 0.70 for the 8-item anxious–depressed problems, and 0.70 for the 8-item withdrawn problems scales. This was fairly consistent with the published internal consistencies for the CBCL, which average 0.76 for narrow constructs and 0.92 for broad constructs (Achenbach & Edelbrock, 1983).
Data Analysis
Due to the nested research design, multilevel models were used to examine the relationship between predictors and internalizing problems. As three data points are required to define a slope and estimate error, there are not enough level 1 units (2 children in a family) to model random slopes across each individual within families (Kenny, Kashy, & Cook, 2006; Krull, 2007). Thus, random intercepts models were used to address the non-independence across families. The regression analyses were performed using the lme4 package in R (Bates, Mächler, Bolker, & Walker, 2014). In the null model (without predictors), the cross-level ICCs for the outcome variables were 0.41 (internalizing), 0.31 (anxious–depressed), and 0.18 (withdrawn), indicating multilevel models were appropriate and necessary. The hypothesized mediational process was examined using 2-1-1 multilevel moderated mediation models. The level 2 variable, maternal NA was the initial predictor of level 1 outcome internalizing problems, and this process was mediated by the level 1 variable child BI. Age was included as a moderator of path b (BI to internalizing problems). A total of six models were run to accommodate the two different measures of BI and the three outcomes. All multilevel mediation procedures followed Krull and MacKinnon (2001) and Zhang, Zyphur, and Preacher (2009), and the moderated mediation procedures followed recommendations of Bauer, Preacher, and Gil (2006) and Preacher, Rucker, and Hayes (2007). The mediational analyses and the indirect effects were conducted and calculated in Mplus 7 (Muthén & Muthén, 1998–2012).
Results
Missing Data and Data Reduction
Data were screened for missing values before hypothesis testing. The variables that had missing values were internalizing problems (4.0%), anxious–depressed problems (0.5%), and withdrawn problems (0.5%). The Little’s Missing Completely at Random test suggested that the data were missing completely at random, χ2 (41) = 40.03, p = 0.51. The missing values were then imputed using the expectation-maximization algorithm. Imputed data were used in later analyses.
To obtain a composite score for the Lab-TAB rating of BI, means of raw coded responses across all trial epochs were taken as levels of the corresponding parameters. Then we conducted a factor analysis using principle axis factoring with oblique rotation to detect the latent structure of Lab-TAB BI. Three factors were extracted and explained 60.01% of the total variance (Kaiser–Meyer–Olkin test = 0.61, Bartlett’s test of sphericity: χ2 (28) = 245.14, p < 0.001). Based on the factor loadings, the factors represented “most prominent fearful responses”, “vocal fear”, and “less prominent fearful responses.” Because all factors were considered to be critical components of Lab-TAB BI, coded responses that loaded on any of the three factors (all but activity decrease) were standardized and averaged to construct the composite Lab-TAB BI score. In addition, composite scores for parent-rated BI were obtained by standardizing and averaging scores from TBAQ-social fear, EAS-shyness, and EAS-sociability (reverse-scored), inter-correlations ranged from 0.35 to 0.73 (ps < 0.01). Similarly, the maternal NA score was generated by standardizing and averaging BFI-neuroticism, STAI-trait anxiety, CES-D, and PANAS-negative affect scores, inter-correlations ranged from 0.43 to 0.65 (ps < 0.01). Lab-TAB BI, internalizing problems, anxious–depressed and withdrawn problems were moderately positively skewed and were square root transformed into normality. Maternal NA was substantially positively skewed and was transformed via logarithm.
Descriptive Statistics and Inter-correlations
Descriptive statistics and correlations are presented in Table 1. Lab-TAB BI was moderately correlated with parent-rated BI. Parent-rated BI was also positively correlated with internalizing, anxious–depressed, and withdrawn problems; however, Lab-TAB BI was only significantly associated with anxious–depressed problems. Because maternal NA was positively correlated with parent-rated BI, partial correlations were also tested to examine the associations between parent-rated BI and internalizing problems. All partial correlations remained significant after controlling for maternal NA (Table 1). It was also noteworthy that age was negatively associated with BI, regardless of measurement. Maternal NA was also correlated with child internalizing problems. Gender differences for BI and behavior problems were also examined. Parent ratings of BI were significantly higher for girls, t (199) = 3.28, p = 0.001, Cohen’s d = 0.47. No gender differences were found for Lab-TAB BI, or internalizing, anxious–depressed, and withdrawn problems.
Descriptive Statistics, Bivariate Correlations and Partial Correlations (with 95% Confidence Intervals).
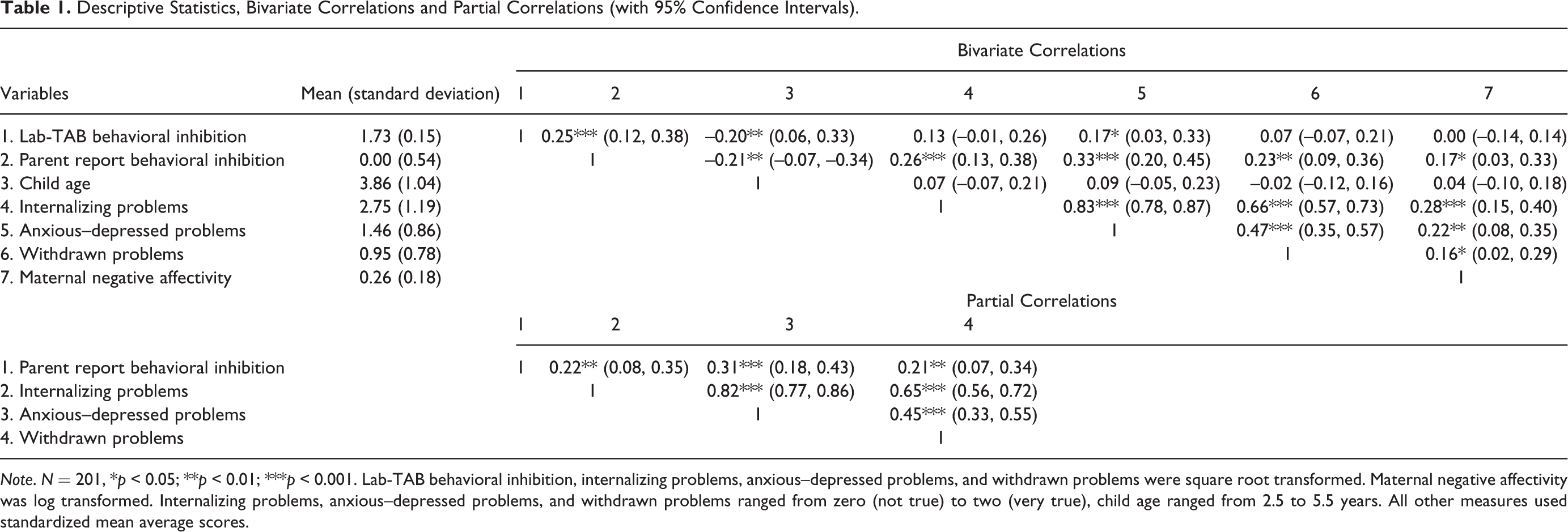
Note. N = 201, *p < 0.05; **p < 0.01; ***p < 0.001. Lab-TAB behavioral inhibition, internalizing problems, anxious–depressed problems, and withdrawn problems were square root transformed. Maternal negative affectivity was log transformed. Internalizing problems, anxious–depressed problems, and withdrawn problems ranged from zero (not true) to two (very true), child age ranged from 2.5 to 5.5 years. All other measures used standardized mean average scores.
Multilevel Models
Parent-rated behavioral inhibition as the predictor
Three multilevel regression models were tested (Table 2: models 1, 3, & 5) using parent-rated BI to predict internalizing, anxious–depressed, and withdrawn problems. As predicted, parent-rated BI, child age, and maternal NA positively predicted broadband internalizing problems and anxious–depressed problems; however, only BI was a significant predictor of withdrawn problems. Consistent with our hypothesis, child age moderated the association between BI and internalizing and anxious–depressed problems (BI × age interactions, see models 1 & 3 in Table 2). Because both models exhibited a similar interaction pattern, model 1 was used as an example to illustrate this moderation effect (Figure 2). As expected, the relationship between BI and internalizing problems differed across age. BI significantly predicted internalizing problems for younger children (-1 SD, 2.82 years, estimate = 0.92, standard error (SE) = 0.19, t (177.11) = 4.82, p < 0.001) and mean age children (3.86 years, estimate = 0.63, SE = 0.14, t (169.90) = 4.69, p < 0.001), but not for older children (+1 SD, 4.90 years, estimate = 0.35, SE = 0.20, t (166.85) = 1.77, p = 0.08). Surprisingly, maternal NA did not interact with BI to predict internalizing problems, so these interaction terms were excluded in the final models. No gender effects were found on any of the outcome variables.
Final Models of Predictors of Internalizing, Anxious–Depressed, and Withdrawn Problems (with 95% Confidence Intervals (CIs)).
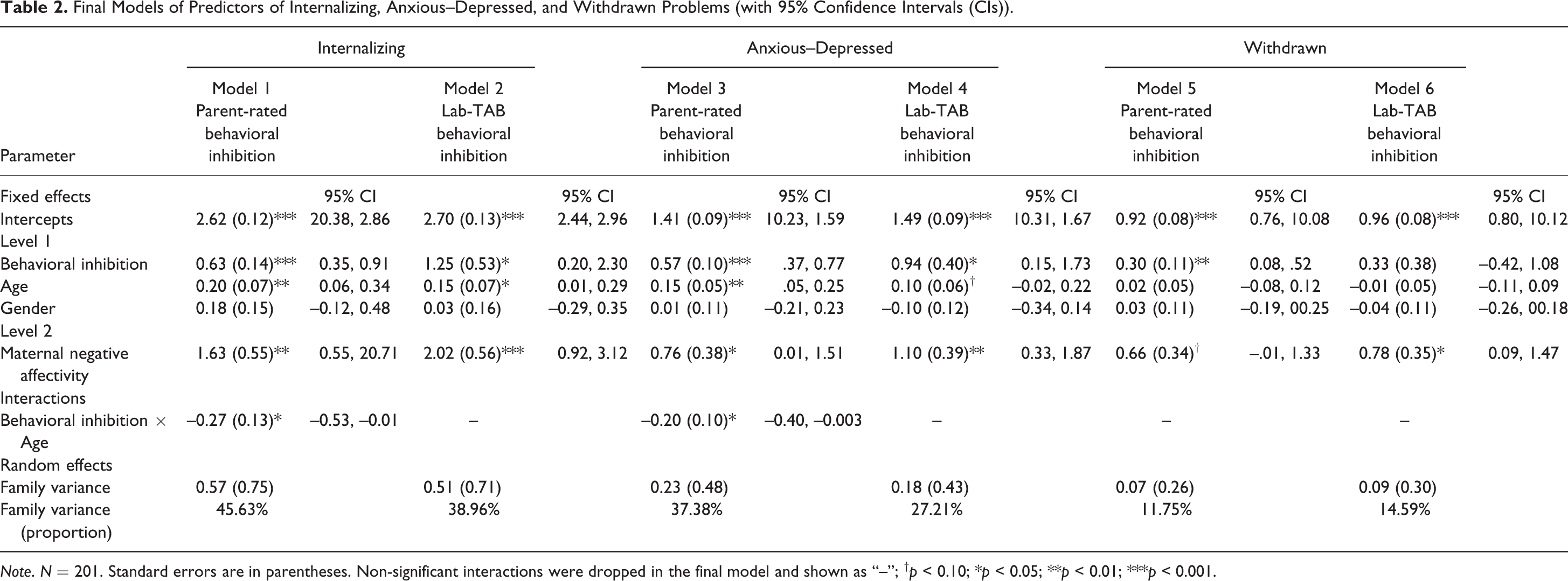
Note. N = 201. Standard errors are in parentheses. Non-significant interactions were dropped in the final model and shown as “--”; † p < 0.10; *p < 0.05; **p < 0.01; ***p < 0.001.
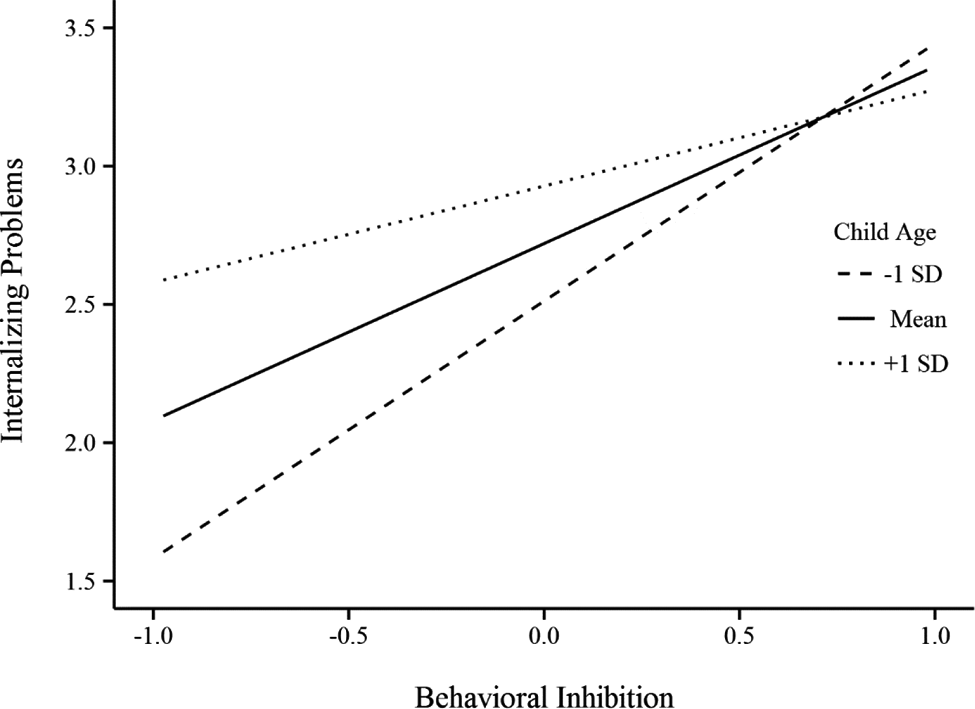
Child age moderated the relationship between behavioral inhibition and internalizing problems. Graphic shows that behavioral inhibition (BI) significantly predicted internalizing problems for younger children (-1 standard deviation (SD), 2.82 years of age, p < 0.001, N = 44) and mean age children (3.86 years of age, p < 0.001, N = 109), but not for older children (+1 SD, 4.90 years of age N = 48).
Lab-TAB-assessed behavioral inhibition as the predictor
Three models were tested (Table 2: models 2, 4, & 6) using Lab-TAB rated BI as the predictor to the same set of outcomes. As hypothesized, Lab-TAB BI, age, and maternal NA positively predicted internalizing, but age was not a significant predictor of anxious–depressed problems. Surprisingly, in contrast to the findings with parent-rated BI, only maternal NA had a main effect on withdrawn problems. No significant interactions (BI × age or NA × BI) were found, nor gender effects.
Multilevel mediation models
To establish the proposed mediational models in our hypothesis, the first step was to examine if the association between maternal NA and BI (path a) was significant. As expected, maternal NA significantly predicted parent-rated BI, estimate = 0.53, SE = 0.25, t (94.33) = 2.45, p = 0.016; however, maternal NA did not predict Lab-TAB BI (p > 0.05). Therefore, subsequent mediational analyses only included parent-rated BI in the models. In addition, because there was no significant main effect of maternal NA on withdrawn problems (see model 5 in Table 3), the mediational model did not test withdrawn problems as an outcome.
Direct and Indirect Effects in Moderated Mediation Models.
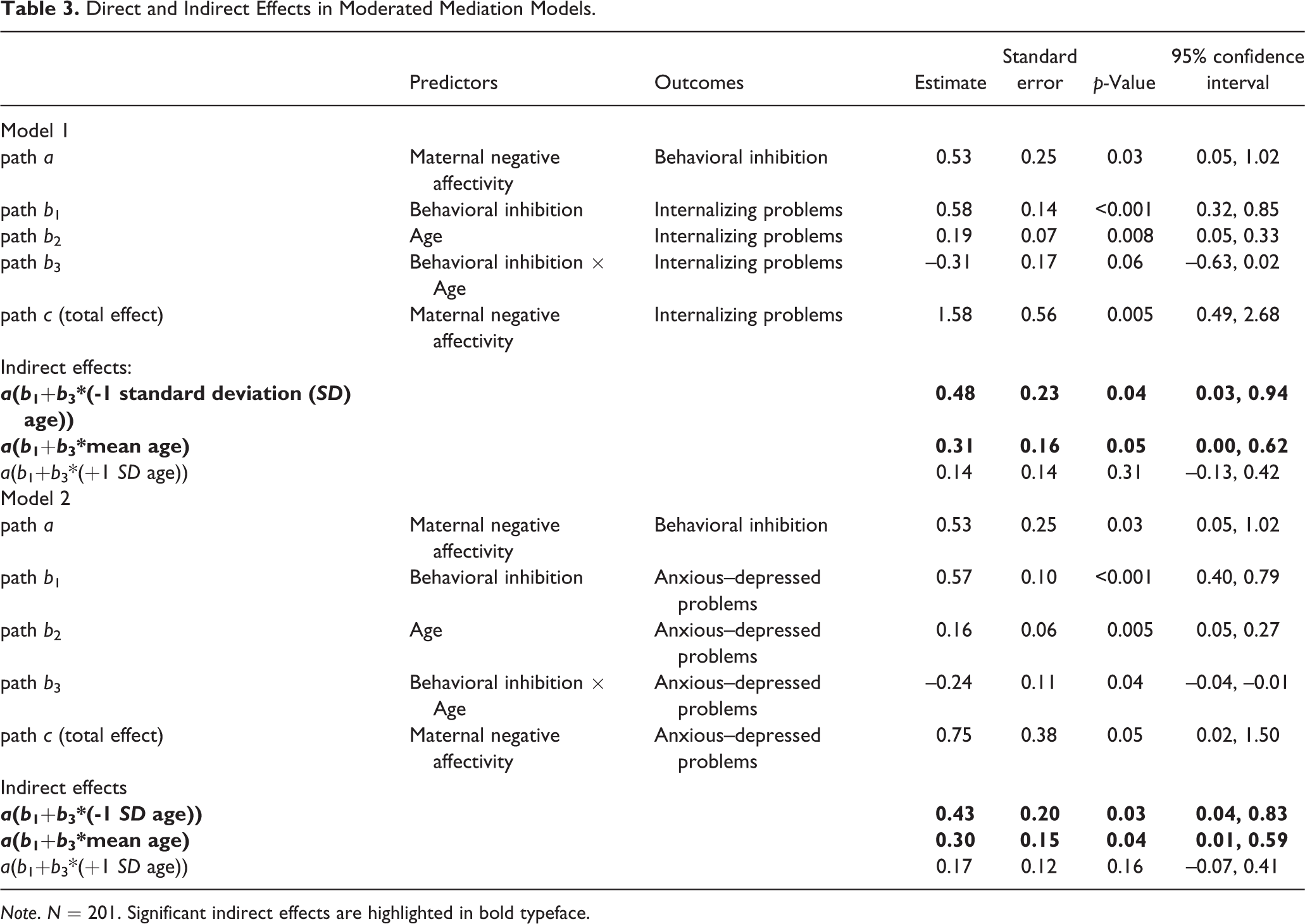
Note. N = 201. Significant indirect effects are highlighted in bold typeface.
Broadband internalizing problems as the outcome
First, the basic 2-1-1 mediational model without age was modeled. The indirect effect was approaching statistical significance, suggesting that parent-rated BI mediated the relationship between maternal NA and child internalizing problems (estimate = 0.26, SE = 0.14, p = 0.056, explained 16.46% variance in the total effect). Next, age was introduced into the model as a moderator of the path b. The results indicated that the mediational process was conditional in terms of child age (Table 3, model 1). Specifically, the indirect effects were significant for younger (-1 SD, 2.82 years) and mean-aged children (3.86 years), but not for older children (+1 SD, 4.90 years).
Anxious–depressed problems as the outcome
A significant indirect effect was found in the initial model without age (estimate = 0.26, SE = 0.13, p = 0.04, explaining 34.67% variance of the total effect). Similarly, when age was introduced as a moderator of path b, the indirect effects in the moderated mediational model remained significant for younger and mean-aged children, but not for older children (Table 3, model 2).
Discussion
The purpose of the current study was to investigate both maternal and child predictors of internalizing problems in preschool-aged children. As hypothesized, Lab-TAB ratings of child BI moderately correlated with parent ratings, and this finding was consistent with the literature (Dougherty, Klein, Durbin, Hayden, & Olino, 2010). Interestingly, parent-rated BI was associated with internalizing problems and all of its related subcategories, but observer-rated BI was only associated with anxious–depressed problems. This suggested that even though both measures captured the essential structure of BI, our assessment of observed BI was tailored more specifically to measure the expression of anxiety in social interactions. In addition, the significant partial correlations indicated that maternal NA did not influence the link between parent ratings of BI and child internalizing problems. As for gender differences, girls showed higher levels of parent-rated BI than boys, but this difference was not significant in observed BI. This finding was somewhat surprising, as previous studies have reported similar gender differences in BI with both observed measures and parent reports (Gagne, Miller, & Goldsmith, 2013). The null finding in the current study might be attributed to a relatively low power with our sample size, as compared to 714 children in the Gagne et al. (2013) study.
Firstly, regardless of measurement method, child BI positively predicted internalizing and anxious–depressed problems; however, Lab-TAB BI had noticeably lower predictive power than the parent ratings. This was particularly evident when BI was used to predict withdrawn problems, in which the observed measure did not yield a significant result. Other temperament studies with a multi-method approach have reported similar findings (e.g., Dougherty et al., 2010; Durbin et al., 2007). This difference could be attributed to the fact that mothers rated both BI and internalizing problems, and the observed assessment was limited to a one-time observation.
Secondly, age negatively predicted internalizing and anxious–depressed problems but not withdrawn problems. Our result extended the previous research (Williams et al., 2009) into a younger and narrower age range (2.5–5.5). As hypothesized, high BI is associated with greater internalizing problems for younger but not older children. One possible explanation of this effect is that during the preschool period, older children are more often exposed to stressful social situations, and they gradually learn to cope with the negative emotional experience. Individual resilience and positive affect may play an important role in these situations. Children with high levels of resilience may use positive emotions to recover from negative experiences, and this could be further enhanced by positive reinforcement, resulting in fewer internalizing problems (Tugade & Fredrickson, 2004). On the other hand, internalizing problems may also be decreased through negative reinforcement: Rubin et al. (2009) found that high BI children exhibit more withdrawal behaviors if they experience more peer exclusion. The tendency to withdraw from social situations could eventually reduce their exposure to negative relationship experiences, which in turn could lead to fewer withdrawal behaviors and fewer internalizing problems. Other factors such as parenting, school environment, early psychological intervention, and individual resilience may also influence the development of both BI and internalizing problems, and longitudinal data are needed for these investigations. These environmental experiences could also influence the assessment of BI in increasingly complicated ways as children age throughout the preschool period.
Lastly, maternal NA positively predicted internalizing and anxious–depressed problems. Similar to Crawford et al. (2011), this finding provides further evidence that maternal traits could affect behavioral problems in children. Because most previous research focused on more specific constructs such as maternal depressive symptoms and trait anxiety, this new finding provides a fresh insight for future research. It would be interesting for future studies to include maternal NA as a variable when investigating related child or family outcomes and processes. Unfortunately, we did not find a significant interaction between maternal NA and child BI on internalizing problems, only direct effects. Although previous studies have found or suggested an interaction effect between maternal mental health and child temperament, it is possible that trait level factors in both the mother and child have parallel effects on internalizing problems.
The relationship between maternal NA and child internalizing problems was further explored by modeling BI as a mediator and age as moderator. As expected, we found a significant moderated mediation that favored younger and mean-aged children. Mothers with high NA are more likely to have children with high BI, and these children tend to have more internalizing problems. Moreover, younger children with high BI were particularly at-risk for the development of internalizing problems, and this interaction strengthened the mediation effect of BI at earlier ages. Additionally, because the total effect was only partially mediated by child BI, one could argue that younger children were less exposed or have yet to respond to other environmental factors that could become potential mediators (e.g., maladaptive parenting, poor family functioning, and negative peer relationships). In early childhood, BI as a heritable trait might be one of the factors that mediate the association between maternal NA and internalizing problems. It is possible that the remaining direct effect could be fully explained by socialization experiences, and these processes would be more complicated with additive or interactive effects from various environmental factors at older ages. Child BI and maternal NA may also have a bi-directional relationship, whereby BI is both affected by and influenced by maternal NA (through both shared genes and elicitation of negativity from mothers) (Pardini, 2008). This calls for more comprehensive future investigations that focus on genes, social-environmental factors, and more comprehensive models of these relationships.
A major strength of the current study is the multi-method assessment approach to BI. It provided a basis for what to expect with different assessment methodologies in the future. The results suggested that parent-rated measures of BI are useful in exploring preliminary findings as they are inexpensive to implement and have relatively higher predictive power than the observed measures. However, these findings need to be interpreted with caution and further validated as they could be subject to potential rater biases associated with parent ratings, including potential contrast effects and overlapping rater variance (due to the fact that parents rate both BI and behavior problems) (Dougherty et al., 2010). In addition, there is some overlapping content between parent ratings of BI and internalizing problems which could further contribute to shared method variance and larger associations than observed between Lab-TAB BI and internalizing problems. This also leads to the first major limitation of the present study, whereby laboratory BI assessment was limited to a single episode. Future studies should consider employing multiple types of laboratory-based BI assessments.
The second major strength of this investigation is that the relatively wide age range allowed us to model age in the mediation process with cross-sectional data; however, these findings do not reflect actual developmental trajectories. For future research, it is important to collect longitudinal data to provide a clearer illustration of the developmental path for behavior problems. Therefore, the fairly wide age range could also be a limitation to the current study. The statistical power was relatively low to draw confident conclusions on any particular effects that were detected at a specific age.
In conclusion, emphasizing broad trait-like characteristics over specific mental health symptoms or neurotic personality traits may help clinical practitioners to intervene at earlier stages, because not all at-risk mothers with high levels of NA show symptoms of diagnosable mental disorders. Moreover, better understanding of the relationship between BI and internalizing problems would also provide a standpoint for developing future intervention protocols. As one would expect, more research is needed to further examine the impact of maternal NA and temperament traits on child development, including longitudinal studies. As suggested by the findings of the current study, the indirect relationship between maternal traits and child behavior should be more extensively studied in future investigations. More complex models with multiple mediators/moderators (e.g., parenting styles, family functioning, and peer relationship quality) and genetically-sensitive samples would provide a more complete presentation of this mother–child association and a better understanding of early behavior problems.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The TEXAS Family Study is supported by a Research Enhancement Program grant from the University of Texas at Arlington (P.I.: J. R. Gagne).