
Abstract
To provide a comprehensive view of the unique contexts shaping adolescent development in the U.S., we utilized latent class analysis (LCA) with indicators of risk and protection across multiple domains (family, peers, school, neighborhood) and examined how latent class membership predicted heavy episodic drinking, illicit substance use, and depression in adolescence and 6 years later when participants were young adults. Data came from Wave 1 (W1) and Wave 3 (W3) of the nationally representative U.S.-based Add Health study (N = 6,649; M age W1 = 14.06; M age W3 = 20.38; 53.8% female; 56.1% White/European American, 22.8% Black/African American, 9.5% Hispanic, 6.7% Biracial, Asian or Pacific Islander 4.2%, American Indian/Native American 0.7%). A six-class solution was selected with classes named: Two Parent: Low Risk, Two Parent: Relationship Risks, Two Parent: Neighborhood Risks, Single Parent: Low Risk, Single Parent: Relationship Risks, and Single Parent: Multidimensional Risk. Subsequent analyses suggested that adolescent social relationships are particularly important for prevention interventions as the classes marked by substance using peers and a lack of closeness to parents and teachers in adolescence (Two Parent: Relationship Risks and Single Parent: Relationship Risks) had consistently poorer outcomes in adolescence and young adulthood.
Keywords
Adolescence is often a time of transition, marked by shifting family relationships, decreased parental monitoring, the crystallization of peer relationships, and the emergence of new risk and protective factors (Catalano et al., 2012). Adolescent risk and protective factors occur across multiple domains of influence (e.g., family, neighborhood) and carry important implications for later alcohol and substance use and depression (Stone et al., 2012; Thapar et al., 2012). While risk factors often accumulate across domains resulting in a cascading effect on development (Catalano et al., 2012), it is important to recognize that risk in one domain does not guarantee risk in another and protective factors in one domain can offset risk in another (Leventhal & Brooks-Gunn, 2000). Exploring the influence of combinations of risk and protection on concurrent and later outcomes is a critical step in understanding adolescent development more comprehensively. In this study, we use a person-centered approach (latent class analysis [LCA]) to identify patterns of adolescent risk and protective factors across multiple domains and examine how these patterns predicted heavy episodic drinking, illicit substance use, and depression in adolescence and young adulthood.
Risk and Protective Framework
Masten’s (2001) risk and protective framework describes development as being influenced by both risk and protective factors. Risk factors increase the likelihood of undesirable outcomes and protective factors buffer against risks, promote resilience, and decrease the likelihood of undesirable outcomes (Cairns et al., 2014). In some instances, risk and protective factors can represent opposite ends of a spectrum. For example, low parental warmth and involvement are both seen as risk factors for multiple negative outcomes during adolescence (e.g., adolescent alcohol initiation; Ryan et al., 2010), but high parental warmth and involvement have been shown to offset some of the risks that accompany growing up in an economically disadvantaged neighborhood (Benzies & Mychasiuk, 2009).
Bioecological Model
The multidimensionality of risk and protective factors can be understood from a bioecological perspective (Bronfenbrenner & Morris, 2006), which presents a series of interrelated nested systems that influence human development. The microsystem consists of interpersonal relationships experienced in the immediate environment of the individual (e.g., family, school, peers); the exosystem represents influences through the broader environment (e.g., government policies); the macrosystem can be thought of as the cultural environment (e.g., norms and values); and the mesosystem consists of interactions within and across systems (e.g., interactions parents have with teachers; Bronfenbrenner & Morris, 2006). Development is shaped by the interactions between and within these different developmental domains. The following sections outline risk and protective factors that are theoretically relevant for understanding the context and systems shaping adolescent development and summarize past empirical research linking the specific risk and protective factors to drinking, illicit substance use, and depression in adolescence and young adulthood.
Family structure and parenting
Parents influence development in a variety of ways and both the number of parents and parenting style have been found to carry important implications for adolescent development. The influence of family structure (i.e., single-parent and two-parent families) can be understood from a Family Stress Model (Conger & Elder, 1994) theoretical perspective, which argues that the economic instability associated with single parenthood can negatively impact adolescent development through increased parent–adolescent conflict and harsh and uninvolved parenting (Conger et al., 2010). Family structure in adolescence has been shown to relate to both adolescent and young adult drinking, substance use, and mental health, with adolescents and young adults from single-parent families typically viewed as being at a higher risk for these negative outcomes (Barrett & Turner, 2005; Brown & Rinelli, 2010; Hemovich et al., 2011).
Baumrind (1991) classified parenting styles along the dimensions of warmth/responsiveness versus control/demandingness, which remains a popular theoretical explanation of the implications of parent–adolescent interactions. Parental warmth and involvement are central to healthy development for adolescents as both dimensions help adolescents appropriately manage increased autonomy, internalize rules and behaviors endorsed by their parents, form prosocial peer networks, and hold a positive self-concept (Wang et al., 2014). Warmth and involvement in adolescence are negatively associated with both concurrent and later substance use and poor mental health and the two factors in concert may be particularly protective, as parental involvement in adolescence has been shown to be more effective in preventing problem behaviors when paired with parental warmth (Wang et al., 2014).
Peers
Adolescence is often accompanied by increasing value placed on peer relationships (Viner et al., 2012). Peer influences can be explained by the social development model (Hawkins & Weis, 1985), which posits that adolescents’ behaviors are learned through observing the behaviors of those they bond with socially. When adolescents feel attached to an individual or group, they are likely to adopt similar behaviors to maintain the social bond. Bonds with prosocial peers have been shown to be protective, whereas affiliation with substance using or antisocial peers has been linked to substance use and poor mental health (Sussman et al., 2007).
School
Ainsworth (1969) and Bowlby (1988) initially outlined the importance of secure parent–child attachments, but new attachments formed in adolescence (i.e., attachments to teachers) have become an important area of study (Groh et al., 2014). When adolescents experience a secure attachment, they internalize feelings of self-worth and feel confident in managing the increased autonomy that accompanies the adolescent period (McElhaney et al., 2009). Empirically, a positive teacher–adolescent attachment has been shown to promote resilience (Pianta et al., 2003) and decrease the likelihood of emotional, behavioral, and alcohol and substance use problems (Yeung & Leadbeater, 2010).
Teachers can also foster a connection to the school and promote feelings of belonging (Anderman, 2003). Stage-environment fit (Eccles et al., 1997) stresses the importance of schools meeting students’ developmental needs to promote student engagement. When there is a good stage-environment fit, adolescents are likely to feel they belong at school (Shochet et al., 2006). When there is a misfit, adolescents often question whether they belong and disengage from school—first psychologically then physically (Eccles & Roeser, 2003). This disengagement can culminate in school dropout, which dramatically limits opportunities and has a strong impact on health and well-being (Freudenberg & Ruglis, 2007). Consistent with this rationale, school belonging during adolescence has been shown to longitudinally predict substance use (Rostosky et al., 2003) and mental health (Turner et al., 2014).
Neighborhood and poverty
As autonomy increases in adolescence, the neighborhood becomes more important (Viner et al., 2012). Neighborhood influences can be understood from a social disorganization theoretical perspective. Social disorganization theory (Shaw & McKay, 1969) was initially developed to explain how characteristics of an environment promote criminality but is now presented as a systems theory, where disorganized neighborhoods result from structural factors (e.g., poverty) and disorganization leads to diminished health of the neighborhood and its residents (Kubrin & Weitzer, 2003). Adolescents’ neighborhoods affect their development, resources, supervision received, and social connections and influence both their immediate and later health and well-being outcomes, including substance use and depression (Murry et al., 2011; Viner et al., 2012).
Patterns of Risk and Protection
Most research on adolescent risk and protective factors has used variable-centered approaches in which the effect of a risk or protective factor is studied in isolation. However, adolescents experience multiple influences simultaneously. Adolescents have families and peers, attend schools, and live in neighborhoods; all of which can shape their development directly and interact with other factors to increase or decrease the likelihood of a given outcome. While the literature on patterns of adolescent risk and protective factors is not as extensive as the research on individual factors, there is evidence that risk factors can accumulate to have a cascading effect on development and protective factors can offset risks. For example, adolescents growing up in poverty are more likely to experience high levels of family conflict, associate with delinquent peers, and receive a lower quality education, which combine to dramatically increase their risk for multiple negative mental, emotional, and behavioral outcomes (Murry et al., 2011). However, the increased risk that accompanies living in high-poverty neighborhoods can be offset by more proximal protective factors at the family, peer, and school domains (Leventhal & Brooks-Gunn, 2000). More specifically, while growing up in an economically disadvantaged neighborhood increases the risk for multiple negative outcomes later in life, economically disadvantaged parents may still be warm and highly involved in their adolescents’ lives, both of which have been shown to buffer against neighborhood risks (Pearce et al., 2003). Similarly, adolescents who are at an increased risk for substance use and depression due to parenting risk factors are significantly less likely to abuse substances or develop depression when they attend a high-quality school (Guibord et al., 2011).
One way to identify patterns of risk and protection is to use person-centered analyses (e.g., LCA), which enables the identification and examination of the effect of unique patterns of variables. LCA has previously been effective in identifying adolescents’ profiles of risk (e.g., Lanza et al., 2010; Syvertsen et al., 2010). For example, Syvertsen and colleagues (2010) uncovered latent classes of protective factors in adolescence and found classes with substance using peers and poor parent–adolescent relationships were associated with the greatest odds of alcohol and cigarette use; however, analyses were cross-sectional and risk factors at the neighborhood level were not included. Our study aims to build on extant studies by including risk and protective factors across multiple domains of influence and incorporating longitudinal data to investigate how membership in these subgroups during adolescence predicts outcomes during adolescence and into young adulthood.
Current Study
Given the multidimensional nature of risk and protective factors, it is important to identify patterns of factors to provide a more comprehensive view of adolescent development. Additionally, examining associations between these patterns of risk and protection and adolescent and young adult outcomes can inform prevention efforts by providing evidence for when and where best to direct effective interventions (e.g., family-based interventions). In the current study, we (1) utilized LCA to identify unique subgroups from a large sample of adolescents based on their combinations of risk and protective factors. We chose indicators from family, school, peer, and neighborhood domains based on their theoretical relevance and empirical evidence of their importance for later outcomes and (2) assessed how latent class membership predicted heavy episodic drinking, illicit substance use, and depression in adolescence and 6 years later when participants were young adults. Outcomes were selected based on their high prevalence during young adulthood and links to adolescent risk factors (Catalano et al., 2012; Stone et al., 2012).
Although our LCA was somewhat exploratory, we hypothesized we would find latent classes demonstrating an absence and accumulation of risk, as well as classes with domain specific risks (e.g., adolescents with only school risk factors; Hypothesis 1). We also formed tentative hypotheses based on our anticipated latent class model. We expected classes with multiple risk factors to have significantly worse drinking, substance use, and depressive outcomes than classes with an absence of risk (Hypothesis 2a). Additionally, we thought certain combinations of risk factors would be particularly problematic. For example, we anticipated adolescents from latent classes with substance using peers would struggle with substance use as adolescents and young adults (Hypothesis 2b). Similarly, we anticipated adolescents from latent classes without positive relationships would be at an increased risk for depression (Hypothesis 2c). Finally, consistent with previous literature, we expected latent classes with risk factors in distal domains (i.e., at the neighborhood level) and protective factors in proximal domains (i.e., parents and peers) to have relatively comparable outcomes to latent classes with an absence of risk (Hypothesis 2d).
Method
Participants
Data came from the National Longitudinal Study of Adolescent to Adult Health (Add Health Add Health; Harris et al., 2009), a large, nationally representative sample of adolescents in Grades 7–12 in the U.S., recruited in 1994–1995. Participants were followed into adulthood through four waves of data collection (Harris et al., 2009). We included data from participants and their parents (90% of adolescents had a parent participate) who were aged 12–16 at Wave 1 (W1) and provided data 6 years later at Wave 3 (W3; 25% attrition between the waves; adolescent N = 6,649; M age W1 = 14.06; M age W3 = 20.38; 53.8% female; 56.1% White, 22.8% Black/African American, 9.5% Hispanic, 6.7% Biracial, Asian or Pacific Islander 4.2%, American Indian/Native American 0.7%; parent N = 5,975; 93% mothers). To account for attrition and missing data, we conducted all analyses with the W3 longitudinal weight, which adjusted for bias related to nonresponse and the sampling design (Chen & Chantala, 2014).
Measures
W1 LCA indicators
Indicators of multidimensional risk and protective factors came from W1 adolescent and parent reports. U.S. census tract data were used to determine neighborhood poverty. Eight indicators came from single items on a continuous scale. In many cases, these variables were skewed, with six indicators having skewness values above 2.0, which is thought to be the acceptable value for large sample studies (West et al., 1995). Skewed continuous variables often result in spurious latent subgroups (Asparouhov & Muthén, 2015) and do not capture the full range of the scale (Vasilenko & Espinosa-Hernandez, 2019). Because categorical indicators can be used to represent the presence or absence of a given factor (e.g., peers use substances or they do not) and yield conceptually distinct classes with a more parsimonious solution, we recoded indicators into nominal variables.
Family structure
A family structure variable was created using adolescent reports. When responding to maternal and paternal relationship items (could be a biological parent, stepparent, or other caregiver), adolescents were given the option to indicate that they did not have a mother or father figure in their life. If an adolescent reported having both a mother and father figure in their life, they were coded as growing up in a two-parent family. If they reported not having a mother figure (3.8%) or father figure (28.2%), then they were coded as growing up in a single-parent family. Family structure was coded as 1 = single parent (31.3%) and 2 = two parent (68.7%).
Parental warmth
Adolescents reported how warm their mothers and fathers were on a 5-point scale with responses ranging from 1 (strongly agree) to 5 (strongly disagree; e.g. “Most of the time, your mother is warm and loving toward you”). We coded responses as 1 = not warm (not sure, disagree, strongly disagree; 7.6% of mothers, 10.1% of fathers), 2 = somewhat warm (agree; 34.6% of mothers, 29.2% of fathers), 3 = very warm (strongly agree; 54.0% of mothers, 32.6% of fathers), or 4 = no mother/no father (3.8% of mothers, 28.2% of fathers). We then recoded adolescents based on the number of highly warm parents they had in their life (0 = no very warm parents, 39.3%; 1 = one very warm parent, 34.9%; 2 = two very warm parents, 25.8%).
Parental involvement
Variables for parents’ involvement were created from adolescents’ reports of whether they had engaged in an activity with their mother/father in the past 4 weeks (e.g., “worked on a project for school”). We coded responses 0 (had not occurred in the past week) or 1 (had occurred), summed responses, and created a separate involvement variable for mothers and fathers: 1 = no involvement (zero yes responses; 9.4% of mothers, 18.3% of fathers), 2 = some involvement (one yes response; 30.5% of mothers, 22.1% of fathers), 3 = high involvement (two or more yes responses; 56.3% of mothers, 31.5% of fathers), and 4 = no mother/no father (3.8% of mothers, 28.2% of fathers). As with parental warmth, we then recoded adolescents based on the number of highly involved parents in their life (0 = no highly involved parents, 37.2%; 1 = one very involved parent, 37.8%; 2 = two very involved parents, 25.0%).
Peer substance use
Adolescents were prompted to think of their three best friends, then asked, “how many smoke at least 1 cigarette a day?” and “how many drink at least once a month?.” Responses were categorized 0 (no best friend who drank or smoked; 69.5%) or 1 (at least one best friend who drank or smoked 30.5%).
Teacher caring
Adolescents responded to the item, “How much do you feel that your teachers care about you?,” on a 5-point scale ranging from 1 (not at all) to 5 (very much). We dichotomized responses as 0 = teachers do not care much (not at all, very little, and somewhat; 45.2%) or 1 = teachers care (quite a bit and very much; 54.8%).
School belonging
Adolescents reported how strongly they agreed with the statement, “I feel like I am part of this school,” on a 5-point scale, with responses ranging from 1 (strongly agree) to 5 (strongly disagree). We dichotomized responses as 0 = does not feel they belong (strongly disagree, disagree, neither agree nor disagree; 22.9%) or 1 = feels they belong (agree, strongly agree; 77.1%).
Neighborhood safety and drugs
Adolescents responded to the statement, “I feel safe in my neighborhood.” Responses were given on a 5-point scale ranging from 1 (strongly agree) to 5 (strongly disagree). We dichotomized responses as 0 = not safe (strongly disagree, disagree, neither agree nor disagree; 9.0%) or 1 = safe (agree, strongly agree; 91.0%).
Parents were asked “in this neighborhood, how big a problem are drug dealers and drug users?” Responses were given on a 3-point scale (1 = no problem at all, 2 = a small problem, 3 = a big problem). We dichotomized responses as 0 = not a problem (60.5%) or 1 = a problem (a small problem or a big problem; 39.5%).
Poverty
Parents reported their combined household income (M = US$46,486). Incomes at or below US$16,000 were coded 1 (in poverty; 18.7%) and incomes over US$16,000 were coded 0 (not in poverty; 81.3%); US$16,000 was roughly the poverty threshold for a family of four in 1994 when the data were collected (Lee et al., 2009; U.S. Bureau of the Census, 1994).
Census tract data were used to determine poverty areas. Consistent with the census definition (U.S. Bureau of the Census, 1994), neighborhoods were classified as poverty areas if 20% or more of households were at or under the poverty line. Participants were coded as 0 if they were not in a poverty area (73.5%) or 1 if they were in a poverty area (26.5%).
Dependent variables
Outcome variables came from W1 and W3 data. W3 data were collected approximately 6 years after W1. As is common in the Add Health data set, some questions were not asked in an identical fashion at all waves. For example, at W1, there were 19 items from The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), but only 9 items at W3. In the interest of continuity, we scored the W1 and W3 dependent outcomes in the same manner (i.e., we used the same 9 items from the CES-D at both W1 and W3). All outcomes were determined using self-reports.
Heavy episodic drinking
At W1, participants were asked “over the past 12 months, on how many days did you drink 5 or more drinks in a row?.” Response options ranged from 1 (every day or almost every day) to 7 (never). To be consistent with the W3 measure, we estimated how likely participants were to engage in heavy episodic drinking in the past 2 weeks at W1. We recoded the variable into 0 = no heavy episodic drinking in past 2 weeks (once a month, 1 or 2 days in the past 12 months, never, or participant reported never drinking, 90.4% of participants) and 1 = any heavy episodic drinking in the past 2 weeks (every day or almost every day, 3–5 days a week, 1 or 2 days a week, 2 or 3 days a month, 9.6%). At W3, participants were asked to report the number of times they engaged in heavy episodic drinking in the past 2 weeks, with heavy episodic drinking defined as five or more drinks for men and four or more drinks for women in a single occasion (National Institute on Alcohol Abuse and Alcoholism, 2004). W3 responses were dichotomized as 0 = no heavy episodic drinking (66.6%) or 1 = any heavy episodic drinking (33.4%).
Illicit substance use
At W1 and W3, participants reported how many times in the past 30 days they used “cocaine,” “meth,” and “LSD, PCP, ecstasy, mushrooms, inhalants, ice, heroin, or prescription medicines not prescribed for you.” Participants who reported any use in the past 30 days were coded 1 (W1: 4.7%, W3: 7.3%); no use was coded 0 (W1: 95.3%, W3: 92.7%).
Depression
Depression was calculated using 9 items from The CES-D (Radloff, 1977), a valid and reliable measure of depressive symptoms (Beekman et al., 1997; Radloff, 1977; W1 α = .83; W3 α = .81). Participants were asked to rate on a 4-point scale (0 = never or rarely, 3 = most of the time or all of the time) how often a statement was true for them in the past 7 days (e.g., “You felt that people disliked you.”). The CES-D contains 20 items with a score of 16 (mean score of .80 per item) indicating potential depressive symptomology (Radloff, 1977). As Add Health only used a subset of items, we rescaled the cutoff level that corresponded to depressive symptomology as 7 (mean score of .78 per item). We dichotomized the variable as 0 = not depressed (W1: 68.1%, W3: 74.4%) and 1 = depressed (W1: 31.9%, W3: 25.6%).
Plan of Analysis
Our analyses consisted of (1) conducting LCA with dichotomous indicators to identify unique subgroups of adolescents based on the presence of risk and protective factors across domains at W1, (2) identifying any differences in demographics across classes as a mechanism to better conceptualize the latent classes, and (3) utilizing the three-step weighted analysis introduced by Bolck et al. (2004; Bolck, Croon, & Hagenaars [BCH]) to perform weighted logistic regression with adolescent latent classes predicting drinking, substance use, and depression outcomes at W1 when participants were adolescents and 6 years later when participants were young adults. Note that dichotomous indicators were used for our LCA. This was done both for the measurement issues discussed above in the measures section and because keeping indicators continuous and running latent profile analysis resulted in a large number of profiles (i.e., 11 profile solution) that were not statistically distinct on the indicators (e.g., multiple profiles did not differ significantly on parental warmth or involvement, no profiles differed from the sample mean by more than 1 SD on the friends using substances variable) making it difficult to interpret differences in profiles. Posterior probabilities were used to weight participants’ likelihood of membership in each latent class and dependent variables were regressed on class membership controlling for participants’ age, race/ethnicity, and gender, as well as the dependent variable at Time 1 (e.g., W1 heavy episodic drinking controlled when W3 heavy episodic drinking was the outcome). All analyses were run with Latent Gold 5.1 (Vermunt & Magidson, 2016) and models were run with 1,000 random start values.
Results
Model Selection
Table 1 includes Bayesian information criterion (BIC), Akaike information criterion (AIC), and consistent AIC (CAIC) fit information for 1–12 latent class models. AIC indicated a 10-class solution fit the data best, but BIC indicated an 8-class solution and CAIC indicated a 7-class solution. We also took into account the interpretability and distinctness of the different classes. For example, the six-class solution resulted in a distinct class characterized by single parents with no risk factors at any level. The seven-class solution broke up this class into two smaller single parent, lower risk classes, where one was slightly more likely to feel like their teachers cared and also had some higher neighborhood risk factors. Because these two classes were similar and the seven-class solution led to classes that seemed less differentiated (more posterior probabilities fell into the .40–.60 range), we opted to select the more parsimonious six-class solution which had similar fit indices to the eight-class solution (e.g., six-class BIC: 76,936.81; eight-class BIC: 76,874.08).
Fit Indices for Models 1 Through 12.
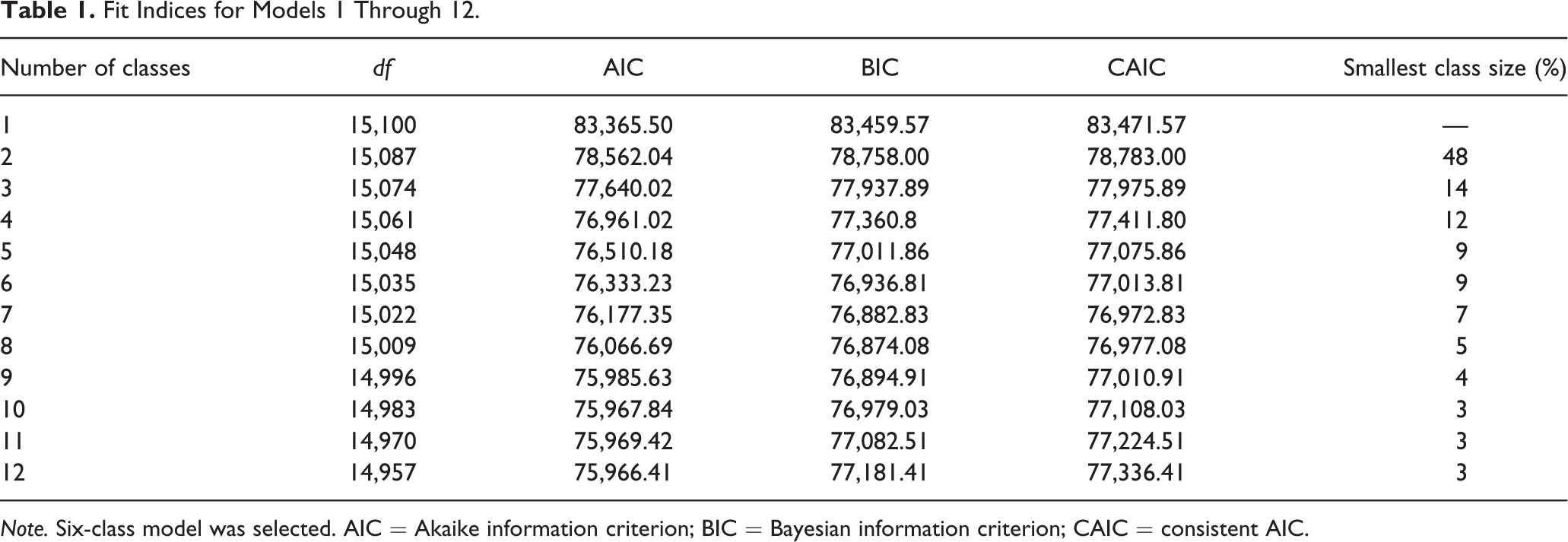
Note. Six-class model was selected. AIC = Akaike information criterion; BIC = Bayesian information criterion; CAIC = consistent AIC.
Latent Classes
Consistent with our first hypothesis, we identified latent classes with an absence of risk, an accumulation of risk, and domain-specific risks. We named classes based on their distinct patterns of risk and protective factors as determined by the item response probabilities. Three latent classes consisted of two-parent families and three were single-parent families (Table 2). We labeled the three 2-parent classes as Two Parent: Low Risk (34% of the sample), Two Parent: Relationship Risks (20%), and Two Parent: Neighborhood Risks (9%) and the three single-parent classes as Single Parent: Low Risk (18%), Single Parent: Relationship Risks (11%), and Single Parent: Multidimensional Risk (9%). The Two Parent: Low Risk class had multiple protective factors (e.g., two warm and involved parents, safe neighborhood) and no measured risk factors. Adolescents from the Two Parent: Relationship Risks class did not have a highly warm or involved parent, were likely to have a close friend using substances, felt that teachers did not care about them, but had protective factors at the neighborhood level. Parents from the Two Parent: Neighborhood Risks class were relatively evenly distributed across the different levels of warmth and involvement and had protective factors in the peer and school domains; however, these families were likely to be living in impoverished neighborhoods where drugs and safety were a concern. The Single Parent: Low Risk class was very similar to the Two Parent: Low Risk class except that it was likely to be a single-parent family. The Single Parent: Relationship Risks class was similar to the Two Parent: Relationship Risks class; adolescents from this class did not have a highly warm or involved parent, they were likely to have a close friend using substances, and they did not feel like their teachers cared about them. Finally, the Single Parent: Multidimensional Risk class had risk factors at multiple levels. Parents were unlikely to be highly warm or involved, adolescents did not feel like their teachers cared about them, and families were likely to be impoverished, living in impoverished neighborhoods, and experiencing concerns regarding drugs and safety in the neighborhoods. The only protective factors for this class were that adolescents’ close peers were not likely to be using substances and adolescents reported feeling like they belonged at school.
Item Response Probabilities for Six Latent Classes.
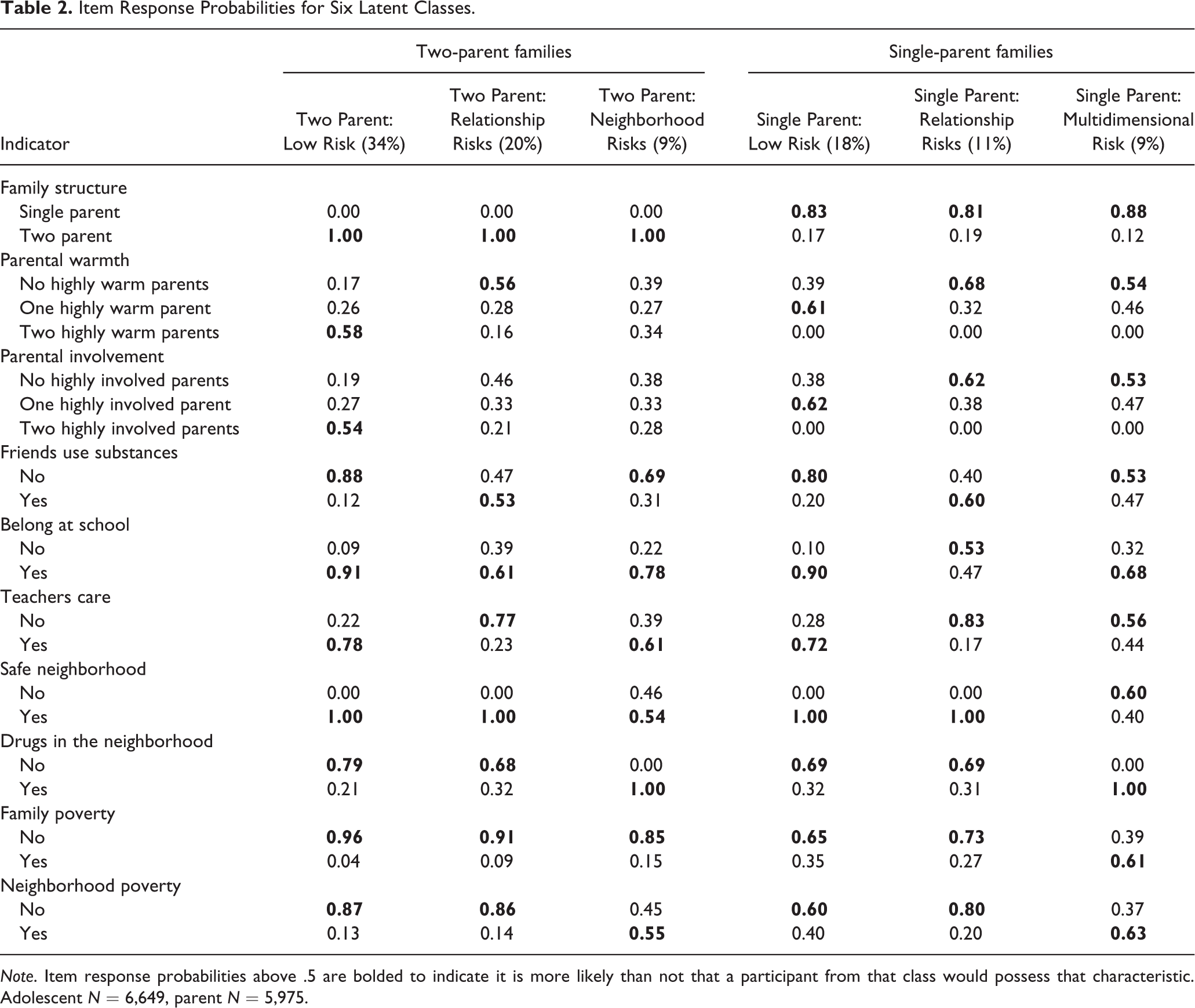
Note. Item response probabilities above .5 are bolded to indicate it is more likely than not that a participant from that class would possess that characteristic. Adolescent N = 6,649, parent N = 5,975.
Age, race and ethnicity, and gender across latent classes
Before examining how latent class membership predicted our outcomes of interest, we were interested in understanding any potential differences in demographics across classes as a mechanism to better conceptualize the latent classes. As such, we examined how class membership varied as a result of W1 participants’ age, race and ethnicity, and gender. Results indicated that class membership varied significantly across age and race and ethnicity (both p < .001) but not gender (p = .95). There were multiple significant differences between classes in terms of age. The youngest class was the Two Parent: Low Risk class (M = 13.80, SD = 1.00; significantly younger than Two Parent: Relationship Risks, Single Parent: Relationship Risks, and Single Parent: Multidimensional Risk), then the Single Parent: Low Risk (M = 13.96, SD = 1.04; significantly younger than Two Parent: Relationship Risks, Single Parent: Relationship Risks, and Single Parent: Multidimensional Risk), Two Parent: Neighborhood Risks (M = 14.10, SD = 1.07; significantly younger than Two Parent: Relationship Risks, Single Parent: Relationship Risks, and Single Parent: Multidimensional Risk), Single Parent: Multidimensional Risk (M = 14.16, SD = 1.02), Two Parent Relationship Risks (M = 14.36, SD = 0.99), and Single Parent: Relationship Risks (M = 14.42, SD = 1.00) classes. The largest age difference was between the Two Parent: Low Risk and Single Parent: Relationship Risks class (about 7 months) and all classes were within 1 SD of each other indicating that classes were relatively comparable in terms of age.
Significant differences in race and ethnicity seemed to be driven primarily by a high percentage of European American/White adolescents in the Two Parent: Low Risk (81%; 6% Hispanic; 5% African American), Two Parent: Relationship Risks (79%; 8% Hispanic; 4% African American), and Single Parent: Relationship Risks (66%; 11% Hispanic; 10% African American) classes. All other classes demonstrated more diversity in terms of race and ethnicity as there were at least two race/ethnicity groups comprising over 20% of the subgroup (Single Parent: Low Risk: 50% European American/White, 32% African American, 11% Hispanic, Two Parent: Neighborhood Risks: 52% European American/White, 22% African American, 12% Hispanic, and 10% Biracial; Single Parent: Multidimensional Risk: 44% African American, 32% European American/White; 10% Biracial; 9% Hispanic).
Predicting Young Adult Outcomes
Participants were weighted based on their probability of latent class membership and weighted logistic regressions using the BCH approach were conducted to examine associations between latent class membership and W1 and W3 heavy episodic drinking, illicit substance use, and depression controlling for participants’ age, race and ethnicity, and gender. Results revealed latent class was a significant predictor for all outcomes of interest at both W1 and W3 (heavy episodic drinking in the past 2 weeks W1: Wald = 112.28, p < .001; W3: Wald = 28.54, p < .001; illicit substance use W1: Wald = 12.57, p < .05; W3: Wald = 30.61, p < .001, depression W1: Wald = 200.22, p < .001; W3: Wald = 57.88, p < .001) indicating prevalence rates differed significantly across latent classes.
Heavy episodic drinking
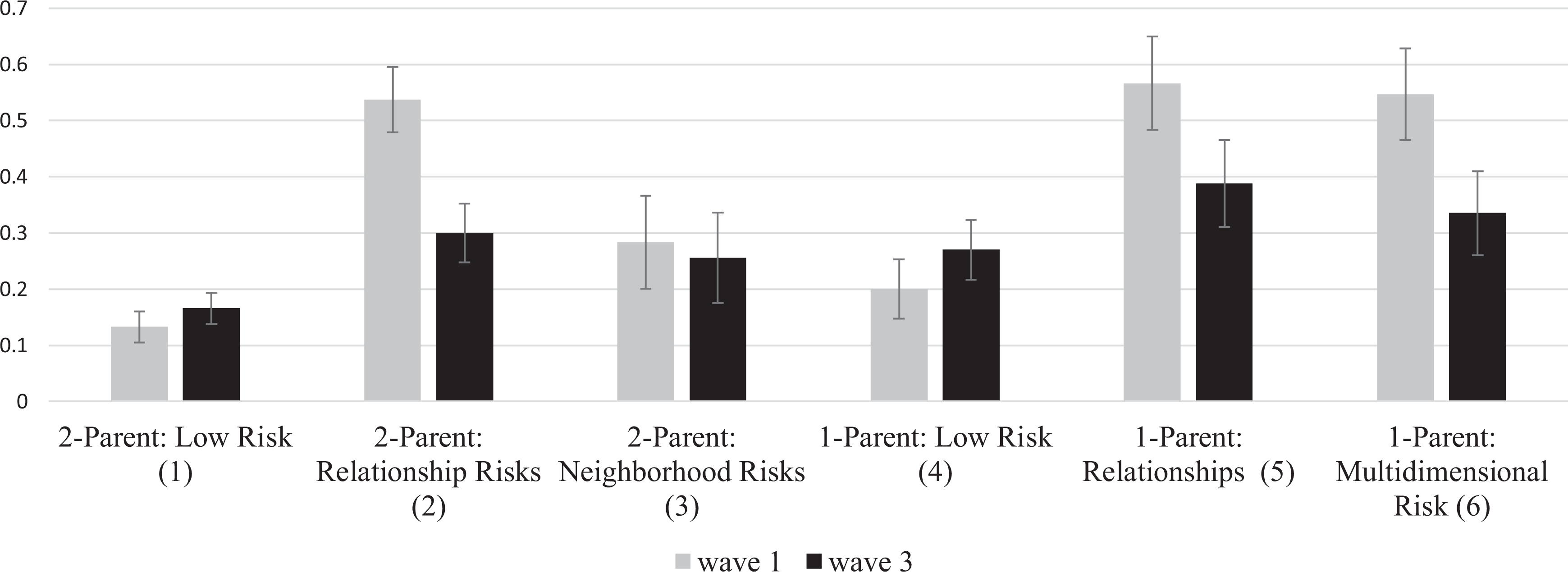
Consistent with our hypothesis, classes with the fewest risk factors (i.e., the Two Parent and Single Parent: Low Risk) had the lowest rates of heavy episodic drinking at W1 (both low-risk classes around 4%; significantly lower than all other classes; Hypothesis 2a). Conversely, adolescents from the classes that were characterized by substance using peers and an absence of protective factors in proximal domains were the most likely to report heavy episodic drinking at W1 (i.e., Two Parent: Relationship Risks: 27%; Single Parent: Relationship Risks: 36%; Single Parent: Multidimensional Risk: 26%; all significant differences reported in Figure 1; Hypothesis 2b).
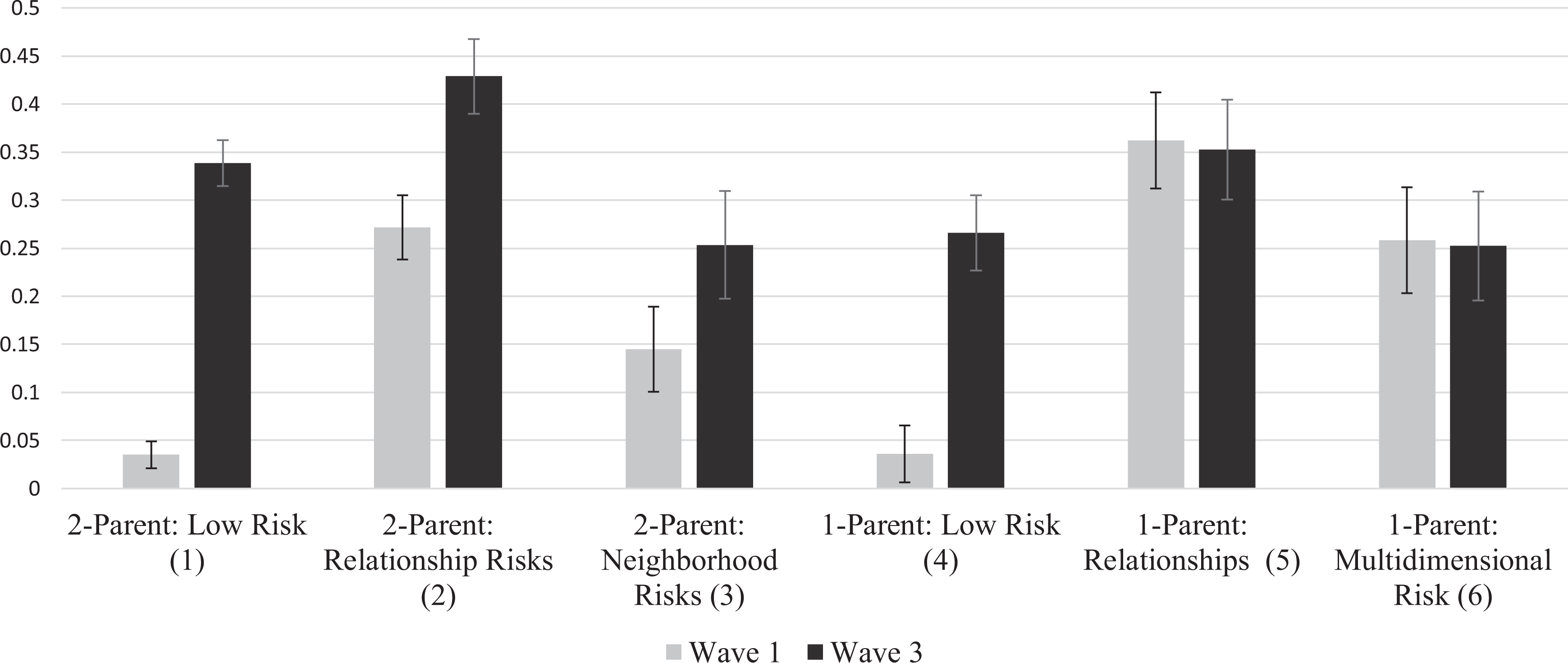
Proportion of Participants Reporting Heavy Episodic Drinking in the Past 2 Weeks.
At W3, our hypotheses for heavy episodic drinking were only partially supported. As expected, rates remained high among the Two Parent: Relationship Risks (43%; significantly higher than all other classes; Figure 1) and Single Parent: Relationship Risks (35%; significantly higher than the Single Parent: Low Risk, Two Parent: Neighborhood Risks, and Single Parent: Multidimensional Risk; Hypothesis 2b) classes. However, young adults from the seemingly lowest risk class, Two Parent: Low Risk, showed the greatest increase in heavy episodic drinking between W1 and W3, with 34% reporting drinking heavily in the past 2 weeks at W3 (significantly higher than the Single Parent: Low Risk and Two Parent: Neighborhood Risks classes and not statistically different from the Single Parent: Relationship Risks and Single Parent: Multidimensional Risk classes). Similarly, participants from the Single Parent: Low Risk class reported a marked increase in heavy episodic drinking between W1 and W3. At W3, 27% of young adults from the Single Parent: Low Risk class reported heavy episodic drinking in the past 2 weeks, a rate that did not differ significantly from the Two Parent: Neighborhood Risks (25%) or Single Parent: Multidimensional Risk (25%) classes.
Illicit substance use
The prevalence rates of illicit substance use were largely consistent with our hypotheses; classes with fewer risk factors and more protective factors in proximal domains had lower reported rates of illicit substance use (Hypotheses 2a and 2d). At W1, the lowest rates of illicit substance use were in the two low-risk classes (both slightly above 0% and significantly lower than the Two Parent: Relationship Risks, Single Parent: Relationship Risks, and Single Parent: Multidimensional Risk classes). The highest rates of illicit substance use occurred in the Two Parent: Relationship Risks (10%; significantly higher than all other classes except Single Parent: Relationship Risks) and Single Parent: Relationship Risks (14%; significantly higher than all other classes; Figure 2).
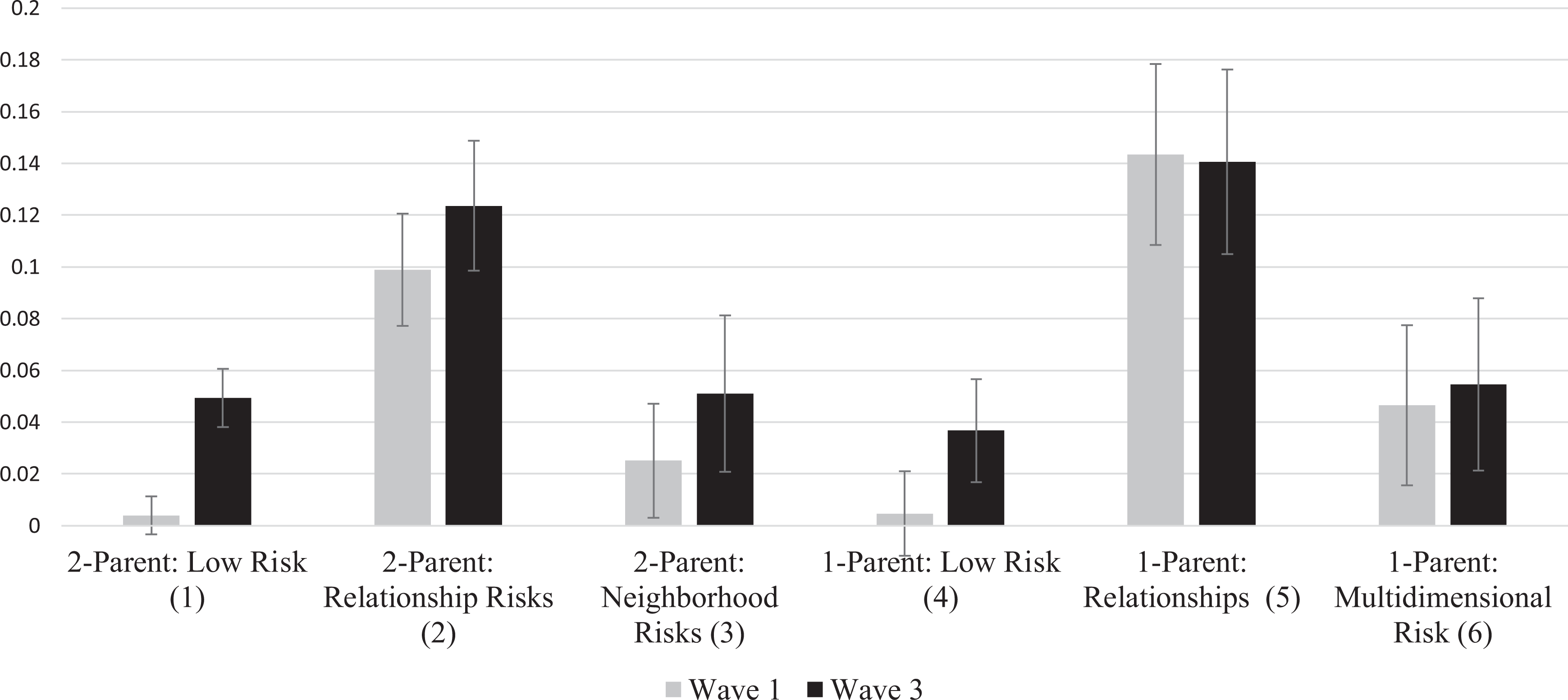
Proportion of Participants Reporting Illicit Substance Use in the Past Month.
The differences in rates of illicit substance use were largely extended to W3. The Two Parent: Low Risk, Single Parent: Low Risk, Two Parent: Neighborhood Risk, and Single Parent: Multidimensional Risk classes all had rates of illicit substance use around 4% or 5% and these classes did not differ significantly from one another. Young adults from the Two Parent: Relationship Risks (12%) and Single Parent: Relationship Risks (14%) had considerably higher rates of illicit substance use, which were significantly higher than all other classes (Figure 2).
Depression
Consistent with our Hypothesis 2c, the highest rates of depression at W1 fell in classes that were characterized by a lack of positive relationships (i.e., Two Parent: Relationship Risks, 54%; Single Parent: Relationship Risks, 57%; and Single Parent: Multidimensional Risk, 55%; significantly higher than all other classes). The Two Parent: Low Risk (13%) and Single Parent: Low Risk (20%) classes had the lowest rates of depression and adolescents from these classes were significantly less likely to meet the CES-D cutoff for depression than nearly every other latent class (all significant differences reported in Figure 3).
Proportion of Participants Demonstrating Depressive Symptomology on CES-D (a Score of 7 or Higher on the CES-D Was Conceptualized as Demonstrating Depressive Symptomology).
At W3, rates of depression declined across four of the six profiles, but the differences across classes remained relatively the same. Once again, rates of depression were highest in the Two Parent: Relationship Risks (30%), Single Parent: Relationship Risks (39%), and Single Parent: Multidimensional Risk (34%) classes (all significantly higher than other classes; Figure 3). Again, young adults from the Two Parent: Low Risk class had the lowest rates of depression (17%) which was significantly lower than all other classes.
Discussion
This study provides an overarching view of the patterns of risk and protective factors experienced by adolescents with the six unique latent classes demonstrating the diversity of contexts adolescents grow up in. As expected, some classes displayed multiple risk factors across domains (i.e., Two Parent: Relationship Risks, Single Parent: Relationship Risks, Single Parent: Multidimensional Risk), while some had little risk with protective factors in multiple domains (Two Parent: Low Risk and Single Parent: Low Risk). Additionally, one class (i.e., Two Parent: Neighborhood Risk) primarily experienced risk only at the neighborhood level.
Proximal Risk and Negative Outcomes
Utilizing LCA with the BCH approach allowed us to examine how unique patterns of risk and protection in adolescence predicted heavy episodic drinking, illicit substance use, and depression during adolescence and young adulthood. While there is evidence that risk factors at proximal levels (e.g., family and peer) and distal levels (e.g., neighborhood) are associated with adolescent and young adult heavy episodic drinking, illicit substance use, and depression, our latent classes provided the opportunity to explore if proximal or distal risks appear to be more relevant for adolescent development. Our results suggest that proximal, social factors are more impactful for heavy episodic drinking and substance use as the two classes demonstrating the highest rates of adolescent and young adult heavy episodic drinking and illicit substance use were the Two Parent: Relationship Risks and Single Parent: Relationship Risks classes. These classes where unique in that they were the only subgroups where adolescents were not likely to have a highly warm or involved parent, felt teachers did not care, and had close friends using substances. While the Single Parent: Multidimensional Risk class was similar in that these adolescents did not feel like their parents were warm and involved or their teachers cared, they did have better adolescent and young adult heavy episodic drinking and substance use outcomes. This is somewhat surprising especially given that adolescents from this class also likely experienced risk at the neighborhood level. However, most adolescents from the Single Parent: Multidimensional Risk class did not have a close friend using substances. This is meaningful as there is a bevy of research to suggest that associating with substance using peers in adolescence is a key risk factor for both adolescent and young adult alcohol, substance use, and depression (Cairns et al., 2014; Leung et al., 2014; Stone et al., 2012). Adolescents often adopt similar behaviors to their peers and vice versa (Hawkins & Weis, 1985). As such, it is likely that adolescents from both of the Relationship Risks classes and their peers were reinforcing each other’s drinking and substance use behaviors.
The Two Parent: Relationship Risks, Single Parent: Relationship Risks, and the Single Parent: Multidimensional Risk classes had the highest rates of adolescent depression, a trend that was largely carried into young adulthood. Again, the accumulation of proximal social risk factors appears to be having both immediate and downstream consequences. Warmth, involvement, and perceptions of caring all promote secure attachments (Scott et al., 2011), which in turn protects against depression (Lee & Hankin, 2009). Adolescence is often a time of transition, where adolescents experience changes in their relationships with parents and peers (Oberle et al., 2011), making it a key developmental period to understand attachment. Secure attachments can be formed within different systems through multiple mechanisms including within the family (Wang et al., 2014) and the school (Groh et al., 2014). Our findings suggest that adolescents from these classes may not have had strong positive relationships with the adults in their lives and this accumulation of risk at proximal, social levels played a role in their mental health as young adults. Additionally, because alcohol, substance use, and depression often co-occur, it is possible that this increased risk for heavy episodic drinking and substance use for the classes marked by poor relationships also increased the risk of depression in adolescence and young adulthood, or alternatively, this increased depression led participants to seek out unhealthy coping mechanisms (i.e., heavy episodic drinking and illicit substance use) and pushed them to find substance using peers (Cairns et al., 2014). However, it is also important to note that while participants from the Single Parent: Multidimensional Risk class did have higher rates of depression than the lower risk classes (i.e., Two Parent: Low Risk, Single Parent: Low Risk, Two Parent: Neighborhood Risks), their rates of illicit substance use were comparable. This would indicate that while depression may increase the risk for illicit substance use, it does not guarantee it and instead there are multiple pathways of risk to substance use and depression (Colder et al., 2013).
Our results also suggest that protective factors in one domain can offset risk in another. For example, adolescents from the Two Parent: Neighborhood Risk class were likely to be living in impoverished areas where drugs were a concern, presumably increasing their risk for multiple negative outcomes. However, these adolescents reported protective factors at the school level and were likely to have at least one highly warm and involved parent. Young adults from this class had outcomes relatively comparable to both the Two Parent: Low Risk and Single Parent: Low Risk classes. This indicates that it might be possible to offset neighborhood risk by bolstering protective factors in other domains (e.g., within families or within school settings) and further suggests the utility of both family (e.g., Strengthening Families Program; Kumpfer et al., 1996) and school-based intervention efforts (Greenberg et al., 2003).
Implications of Family Structure
The three single-parent latent classes were very similar to the three 2-parent latent classes in terms of risk and protective factors (i.e., there were single and two-parent classes characterized by no risk factors, relationships risks, and neighborhood risks). The fact that the single-parent classes had comparable outcomes to their corresponding two-parent classes suggests that it is not having a single parent that increases the risk of poor outcomes but is instead the factors that are more likely to accompany single parenthood (e.g., more adolescent–parent conflict, more socioeconomic stress, and less parental monitoring). This is consistent with the Family Stress Model and empirical work that has found factors like socioeconomic status (SES), social support and stress, peer approval of substance use, attachment, and parent–adolescent communication patterns to underlie associations between family structure and adolescent heavy episodic drinking, substance use, and depression (Barrett & Turner, 2005, 2006; Crawford & Novak, 2008; Levin & Currie, 2010). This is further reinforced by the Single Parent: Low Risk class generally having lower incidences of heavy episodic drinking, illicit substance use, and depression. Additionally, while the social development model (Catalano & Hawkins, 1996; Hawkins & Weis, 1985) and theories of social exclusion (e.g., Leary, 1990) might suggest that adolescents from single-parent families experience more risk factors in other proximal domains (e.g., affiliation with substance using peers) as a result of strained family relationships and less parental modeling, our results did not bear this out. Roughly 54% of participants in the Two Parent classes fell into the Low Risk class with protective factors across domains. This percentage was similar within the Single Parent classes, as about 47% of participants from Single Parent classes were in the Low Risk class. While it is possible that this could be in part due to a small degree of misclassification to the probabilistic nature or LCA, our results do further suggest that living in a single parent family is not an insurmountable challenge, not only in terms of drinking, substance use, and depression outcomes, but in terms of the accumulation of additional proximal risk factors too.
Ultimately, our results indicate that parenting is more about quality than quantity. Single parenthood can present challenges for both the parent and adolescent, but positive results in the Single Parent: Low Risk class indicate adolescents and their parents can overcome these challenges. As such, it is important to ensure that single parents receive the support they need to ensure they are able to remain involved and parent their adolescents with warmth.
Appropriately Timed Prevention
Examining heavy episodic drinking, illicit substance use, and depression in adolescence and young adulthood provided us with a better idea of when differences across profiles emerged. For illicit substance use and depression, these patterns were largely consistent across time points. However, while rates of illicit substance use in the Two-Parent Relationship Risks and Single-Parent Relationship Risks remained relatively stable, adolescents from other classes (i.e., Two Parent: Low Risk and Single Parent: Low Risk) reported higher rates of illicit substance use in young adulthood. These increases for the low-risk classes were even more dramatic in terms of heavy episodic drinking (Two Parent: Low Risk W1: 4%, W3: 34%; Single Parent: Low Risk W1: 4%, W3: 27%). In fact, young adults from the Two Parent: Low Risk had the third highest rates of heavy episodic drinking and did not differ significantly from young adults from the Single Parent: Relationship Risks class. These increases in heavy episodic drinking and illicit substance use in the two lowest risk classes may stem from these classes having significantly higher percentages of young adults attending college (64% of Two Parent: Low Risk; 46% of Single Parent: Low Risk) as college students engage in heavy episodic drinking more frequently than their noncollege-enrolled peers (White & Jackson, 2005) and the transition to college is seen as a risky period for experimentation with illicit substances (Skidmore et al., 2016). When college attendance was included as a covariate in the regression models, latent class membership remained a significant predictor of heavy episodic drinking and illicit substance use (p < .001), but there were fewer significant differences between classes. This suggests a portion of the variance between classes was attributable to college attendance, but latent class was a significant predictor of heavy episodic drinking and illicit substance use above and beyond college attendance. For the young adults from the Two Parent: Low Risk and Single Parent: Low risk latent classes, it is possible that an accumulation of protective factors and an absence of risk factors in adolescence led to an increased likelihood of college attendance, which led to more dramatic increases in rates of heavy episodic drinking and illicit substance use.
Another explanation for the higher rates of heavy episodic drinking in the Two Parent: Low Risk class specifically comes from the higher SES of these families as this class had the lowest probability of experiencing poverty. Previous research has found young adults from more affluent families are at a greater risk for heavy episodic drinking due to greater parental acceptance of alcohol and infrequently enforced consequences (Patrick et al., 2012). Additionally, it is possible that individuals from these low-risk classes may have encountered unique, unmeasured risks (e.g., inconsistent consequences) that resulted in higher heavy episodic drinking rates in young adulthood. Ultimately, these results articulate the importance of appropriately timed interventions. While interventions in early-to-mid adolescence may be crucial for preventing heavy episodic drinking, illicit substance use, and depression in some classes (e.g., classes marked by poor relationships and a lack of attachment), it is important to recognize that prevention efforts still may be needed for those in lower risk classes, particularly around key transition points (e.g., college attendance).
Limitations and Future Directions
Although the longitudinal nature of our study is a strength, we do not know factors that preceded the LCA indicators. For example, membership in the Two Parent: Relationship Risks and Single Parent: Relationship Risks subgroups were associated with multiple negative outcomes, but we do not know why these individuals felt a lack of connection to teachers and school and associated with substance using peers. It is possible these adolescents were demonstrating behaviors that strained their family and school relationships (e.g., using substances) before data were collected at W1. Similarly, it is important to note that while all indicators in the study have been linked to adolescent and young adult heavy episodic drinking, substance use, and depression, we cannot assume the directionality of the associations. For example, a lack of parental involvement increases the risk for adolescent substance use, but adolescents who use substances have also been shown to withdraw from their families and disclose less about their activities, limiting their parents’ opportunities for involvement (Coley et al., 2008). Adding additional time points in future studies to model patterns of risk and protection along with the emergence of heavy episodic drinking, substance use, and depression across adolescence may provide a better picture of the directionality of these associations.
While we attempted to capture the contexts influencing adolescent development by including risk and protective factors from multiple domains of influence, we did not include potentially meaningful factors at the individual level. Future research could build on our findings by including individual-level factors into an LCA model along with variables at proximal and distal levels. This could be valuable as individual traits that promote resilience (e.g., self-efficacy; Fergus & Zimmerman, 2005) in the face of other risks could be identified. Additionally, we only examined how patterns of risk and protection were associated with three outcomes. Future research could expand on our findings to include additional outcomes relevant for adolescent and young adult wellbeing (e.g., academic achievement, marijuana use). Finally, it is important to remember data came from one cohort of participants. Caution should be taken when considering the generalizability of the study to additional groups of adolescents.
Conclusion
Some adolescents experience an accumulation or absence of risk, while others experience risk factors in specific domains and protective factors in others. For adolescent and young adult heavy episodic drinking, substance use, and depression, it appears that an accumulation of risk in social relationships carries more weight than risk in more distal areas (i.e., in the neighborhood). Ultimately, our results further indicate that adolescent development is complex and is shaped by multiple events and relationships that carry implications for well-being. Examining these multiple factors together is an important step to better understand and facilitate healthy development as well as inform effective prevention efforts.