
Abstract
People reflect on their own aging, and this subjective awareness has an influence on developmental outcomes. Scholars have recently operationalized subjective aging in terms of awareness of age-related change (AARC), which captures awareness of both gains and losses. We examined associations of AARC-gains and AARC-losses with physical functioning, subjective well-being, and engagement with life (enjoyable activities and sense of purpose). Importantly, we extended previous research by not only assessing main effects of gains and losses but also testing their interaction. We hypothesized that awareness of losses would be more weakly negatively associated with health and well-being among those who possessed higher awareness of gains. A total of 399 older participants aged 65 to 91 (235 women and 164 men) were recruited via Prime Panels crowd-sourcing platform to complete an online questionnaire. Greater AARC-losses was associated with poorer health, lower subjective well-being, and lower sense of purpose. AARC-gains was associated with better outcomes in general, and moderated associations of AARC-losses with physical functioning, subjective well-being, and sense of purpose (but not engagement in leisure activities). Consistent with predictions, moderation effects showed that negative associations of AARC-losses with the outcomes were weaker among those who reported higher AARC-gains. Results provided some support for a role of AARC-gains in buffering negative effects of AARC-losses on developmental outcomes.
The subjective experience of aging has important implications for health and well-being (Diehl et al., 2014). Diehl and Wahl (2010) refined perspectives on subjective aging by introducing the concept of awareness of age-related change (AARC), defined as “[…] all those experiences that make a person aware that his or her behavior, level of performance, or ways of experiencing his or her life have changed as a consequence of having grown older […]” (Diehl & Wahl, 2010, p. 340). This study reports findings of an examination of associations of AARC-gains and AARC-losses with physical functioning, well-being, and engagement with life. Our aim was to make a conceptual case for possible interaction effects of AARC-gains and AARC-losses in their associations with key developmental outcomes and to empirically test this proposition using a cross-sectional sample of older adults. We were particularly interested in the possibility that associations of AARC-losses with poorer outcomes for health and well-being would be less evident among older adults who reported higher levels of AARC-gains.
AARC and Major Developmental Outcomes
According to Diehl and Wahl (2010), subjective awareness of personal gains and losses occurring as a result of growing older are implicated in psychological processes that shape one’s sense of present competencies. Thus, positive views of one’s own aging are expected to broadly align with favorable evaluations of self-concept and well-being (e.g., Pinquart & Sörensen, 2001). AARC is also believed to influence development indirectly through the operation of self-regulatory processes (see Baltes, 1997; Brandtstädter, 2009; Heckhausen & Schulz, 1995). More specifically, people who evaluate their own aging in a more positive light might more readily adapt to changing life circumstances, whereas those with more negative perceptions of their own aging may be quicker to disengage from attainable goals, resulting in unfulfilled developmental potential (Wilton-Harding & Windsor, 2021). Through its influence on personal meaning making and self-regulation, AARC is hypothesized to influence key developmental outcomes including physical and mental health, psychological well-being, and engagement with life (Diehl & Wahl, 2010). In general, greater AARC-losses are expected to undermine—and greater AARC-gains enhance—developmental potential.
A growing number of studies have now reported associations of AARC with older adults’ health and well-being. For example, AARC-losses have been shown to predict higher depressive symptoms (Dutt et al., 2018a) and poorer psychological well-being (Brothers et al., 2016) in longitudinal studies and to covary with daily negative affect (Neupert & Bellingtier, 2017). A recent systematic review and meta-analysis (Sabatini et al., 2020) found that overall, AARC-gains was associated with more favorable and AARC-losses less favorable outcomes for emotional well-being, with AARC-losses also associated with poorer self-rated health.
The Present Study
Whereas previous studies have focused on independent associations of the AARC dimensions, our contention is that AARC-losses and AARC-gains are likely to interact in their associations with developmental outcomes. Aging is accompanied by an objective increase in the ratio of developmental losses to gains (e.g., Baltes, 1997), thus some awareness of losses may be normative with aging. Recognizing that AARC may indirectly influence health and well-being through its role in self-regulation (Diehl & Wahl, 2010), we postulate that a growing awareness of AARC-losses may be less detrimental for health and well-being when it is accompanied by AARC-gains. For example, AARC-losses might prompt disengagement from a valued activity that is becoming more difficult with aging (e.g., giving up a sport due to health problems), which in turn could undermine well-being. However, concurrent AARC-gains might facilitate reengagement with new alternative activities (e.g., an appreciation of how one’s experience and knowledge could make them a valued mentor to others). We examined possible interactions between AARC-gains and AARC-losses in their associations with physical health, well-being, and engagement with life. These three domains align with the primary developmental outcomes associated with AARC in Diehl and Wahl’s (2010) model. Previous research has shown that AARC-losses is negatively associated with these outcomes (Sabatini et al., 2020), and in light of the postulated mechanisms described above, we expected that for each domain, AARC-loss associations would be weaker in the context of higher AARC-gains. For example, a greater relative appreciation of AARC-gains could help preserve positive health behaviors and a sense of personal competency even in the context of recognizing objective aging-related losses.
Implicit in this predicted AARC-losses × AARC-gains interaction is the notion that a given individual’s AARC-losses is largely independent of their AARC-gains. This is consistent with Diehl and Wahl’s (2010) original conceptualization of the constructs as multidimensional, and empirical findings where small-to-moderate correlations between AARC-gains and AARC-losses have typically been reported (e.g., Brothers et al., 2016; Dutt et al., 2018b; Kaspar et al., 2019). We expected that AARC-losses would be associated with poorer health and well-being, and lower engagement, but that these associations would be moderated, or buffered by AARC-gains. Specifically, we expected that the negative associations between AARC-losses and the outcome variables would be weaker among those with higher AARC-gains.
Method
Participants
Cloud Research’s Prime Panels platform (Chandler et al., 2019) was used to recruit 429 participants from the U.S., who completed an online survey via Qualtrics software. A minimum age of 65 was chosen as this broadly represents the lower cutoff in the literature commonly used to designate older adulthood (e.g., Saz & Dewey, 2001). We excluded 30 participants from the current analysis: 17 with missing data on one or more key study variables, six who self-reported as having been diagnosed with mild cognitive impairment or dementia, three who were below the minimum age, and four who failed in their responses to two or more of three attention check items where participants were requested to respond with a prespecified answer. In the final sample of 399 people, ages ranged from 65 to 91 (M = 70.09, SD = 4.41), with 235 females and 164 males, most of whom identified as White (94%). Participants were compensated for their time according to their agreement with the platform through which they were recruited into the study (approximately US$1.50). The sample size was deemed adequate based on power analyses using the powerreg module in Stata 15 (StataCorp, 2017). Assuming a model with 8 predictors, alpha of .05, and total R 2 of 0.42, 310 participants would be required to detect a significant interaction accounting for 2% of the variance at power = 0.90. Participants provided informed consent and the study was approved by the Flinders University Social and Behavioral Sciences Research Ethics Committee (Project No. 8429).
Measures
Awareness of age-related change
We used the short-form Awareness of Age-Related Change Scale (AARC-10SF; Kaspar et al., 2019). The AARC-10SF consists of 5 items assessing awareness of gains and 5 items assessing awareness of losses. Participants respond using 5-point scales ranging from 1 (not at all) to 5 (very much). Scores for each subscale were summed, with higher scores representing greater awareness of gains (α = .77) and losses (α = .78), respectively.
Physical functioning
Physical functioning was measured using the Physical Functioning scale (PF-10), a subscale of the Medical Outcomes Study 36-item Health Survey (Ware & Sherbourne, 1992). Participants responded to 10 items assessing the extent to which physical health limits them in daily activities on scales ranging from 1 (limited a lot) to 3 (not limited at all). Total scores are calculated by recoding items (1 = 0, 2 = 50, 3 = 100) and taking the mean, with higher scores indicating better physical functioning.
Subjective well-being
The 12-item Scale of Positive and Negative Experience (Diener et al., 2009) was used to measure affective well-being. Participants rated how often they experienced six positive and six negative feeling states in the past 4 weeks using a scale from 1 (very rarely or never) to 5 (very often or always). Items were summed to create total scores for positive affect (α = .94) and negative affect (α = .89). Cognitive-evaluative well-being was assessed using the 5-item Satisfaction with Life Scale (SWLS; Diener et al., 1985). Participants were asked to rate their level of agreement with statements using responses from 1 (strongly disagree) to 7 (strongly agree). Scores were summed to produce a total score (α = .91). In our data, after reversing negative affect, the three well-being indicators were strongly intercorrelated (rs from .61 to .73). We therefore created a composite subjective well-being score by first standardizing, then taking the mean across the three standardized subscales (see Linley et al., 2009; Mackinnon & Sherry, 2012). We based the subjective well-being score on just the mean of the two affect variables for a single participant who had missing data on the SWLS. To facilitate interpretation, we converted the composite well-being score to a T-metric (M = 50, SD = 10).
Engagement with life
We assessed engagement with life using measures of (1) the extent to which participants engaged in activities and (2) the extent to which activities were regarded as meaningful (reflecting sense of purpose in life). Activity engagement was measured using the 10-item Pittsburgh Enjoyable Activities Test (PEAT; Pressman et al., 2009). Participants respond the frequency of engaging in activities using 5-point scales from 0 (never) to 4 (every day). Items were summed to form a total score (α = .75).
Purposeful engagement was assessed with the Life Engagement Test (LET; Scheier et al., 2006). The LET consists of 6 items, with participants responding on 5-point scales from 1 (strongly disagree) to 5 (strongly agree). Items were summed to form a total score with higher values representing greater purposeful engagement with life (α = .87).
Covariates
Consistent with previous investigations of AARC and well-being (e.g., Brothers et al., 2016; Dutt et al., 2018a), analyses were controlled for age, gender (coded male = 0, female = 1), education, and physical health (with the exception of the model where our physical functioning measure was the outcome). In keeping with Brothers et al., our education variable distinguished those with a high school degree or below (low education, 46%) with those with an Associate’s or Bachelor’s degree (medium education, 40%) and those with a postgraduate degree (high education, 14%). Education categories were dummy coded (with low education the reference) for regression analyses.
Results
An overview of the approach to analysis is provided in supplementary materials, and descriptive statistics and bivariate correlations are provided in Supplementary Table 1.
AARC-Gains as a Moderator of Associations Between AARC-Losses and Physical Functioning
Results of the moderated regression analysis that included physical functioning as the outcome variable are shown in Table 1. The main effects model (Step 1) revealed that higher levels of AARC-losses were associated with poorer physical functioning (sr 2 = .30), whereas higher AARC-gains were associated with better physical functioning (sr 2 = .01). Step 2 revealed a significant AARC-losses by AARC-gains interaction that accounted for an additional 1% of the variance, displayed in Figure 1. Figure 1 shows a strong main effect of AARC-losses; however, a subtle buffering effect of AARC-gains on the relationship was also evident, with the negative association of AARC-losses with physical functioning weaker among those with high AARC-gains. Simple slopes analyses revealed that both slopes displayed in Figure 1 were significantly different from zero at p < .001 (at AARC-gains = −1 SD, AARC-losses b = −4.14, SE = 0.29; at AARC-gains = +1 SD, AARC-losses b = −2.90, SE = 0.30).
Hierarchal Regression Analysis Results: Physical Functioning (n = 399).
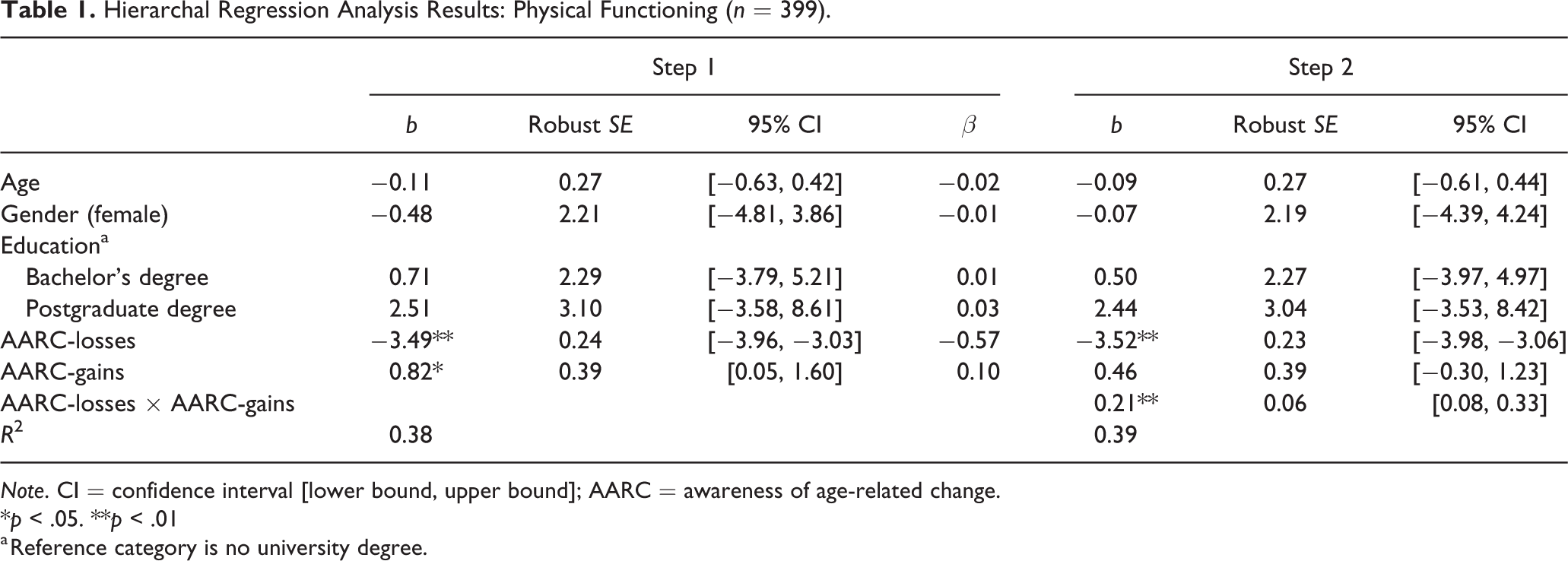
Note. CI = confidence interval [lower bound, upper bound]; AARC = awareness of age-related change.
*p < .05. **p < .01
a Reference category is no university degree.
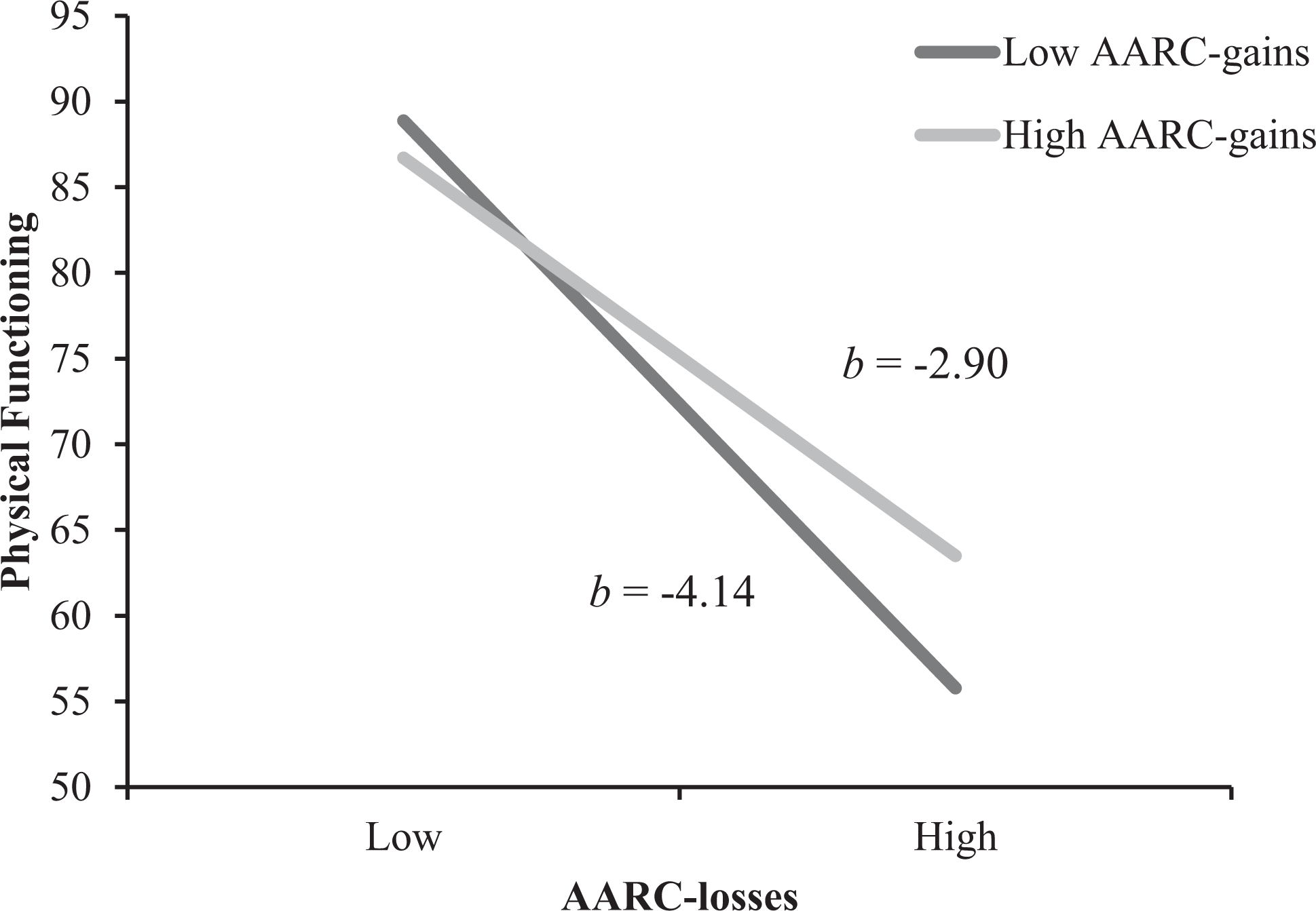
The Relationship Between AARC-Losses and AARC-Gains in Predicting Physical Functioning. Note. High and low values of AARC-losses and AARC-gains represent 1 SD above or below the mean. Both slopes are significantly different from zero (p < .001). bs represent slopes for AARC-losses at high and low values of AARC-gains. Predicted values shown here are based on regression parameter estimates reported in Table 1, Step 2 (n = 399). AARC = awareness of age-related change.
AARC-Gains as a Moderator of Associations Between AARC-Losses and Subjective Well-Being
Next, we examined associations of AARC-losses and AARC-gains with our subjective well-being composite. Results of the regression analyses are shown in Table 2. At Step 1, main effects emerged, with AARC-losses related to lower well-being (sr 2 = .10) and AARC-gains related to higher well-being (sr 2 = .18). The AARC-losses × AARC-gains interaction term entered in Step 2 contributed significantly to model fit, accounting for an additional 2% of the variance in subjective well-being. The results once again pointed to a subtle moderating effect of AARC-gains, whereby the negative association of AARC-losses with subjective well-being was weaker at higher levels of AARC-gains (Figure 2, both slopes significantly different from zero at p < .001. at AARC-gains = −1 SD, AARC-losses b = −1.28, SE = 0.13; at AARC-gains = +1 SD, AARC-losses b = −0.71, SE = 0.13). Follow-up analyses (see Supplementary materials) showed patterns consistent with those reported here when satisfaction with life and affect balance were analyzed as separate outcome variables.
Hierarchal Regression Analysis Results: Subjective Well-Being (n = 399).
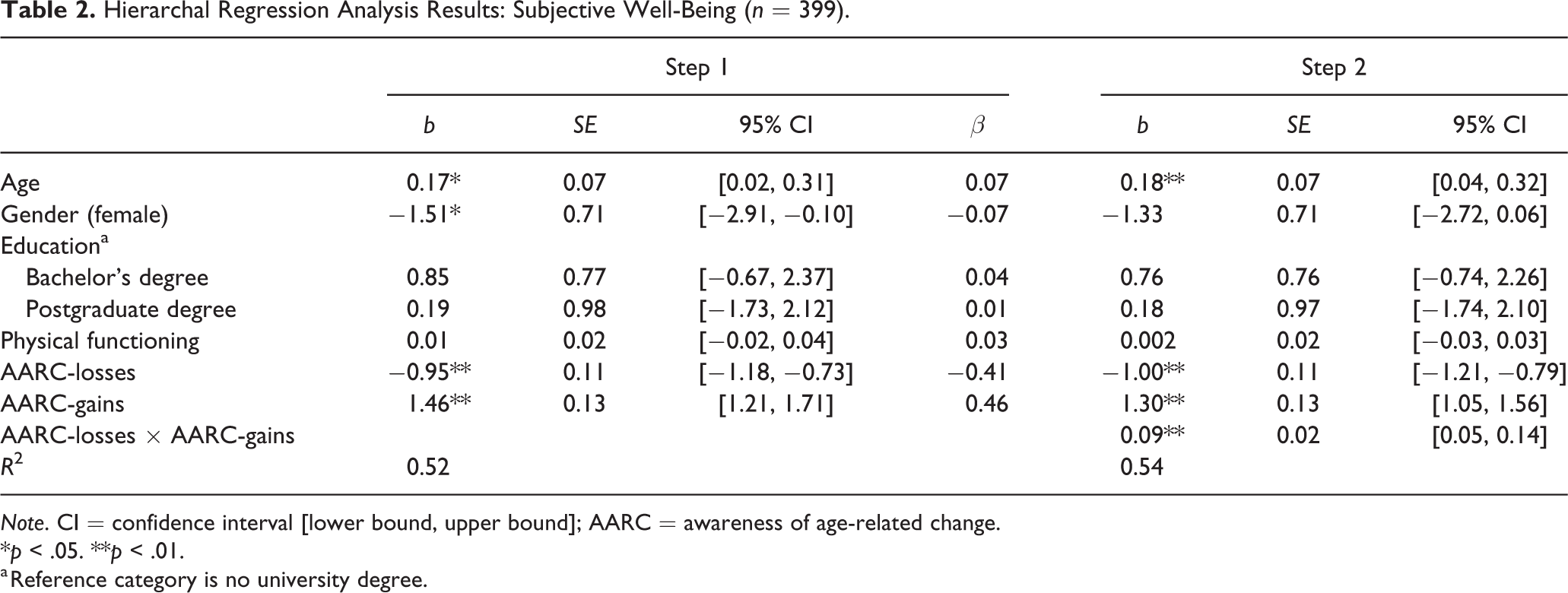
Note. CI = confidence interval [lower bound, upper bound]; AARC = awareness of age-related change.
*p < .05. **p < .01.
a Reference category is no university degree.
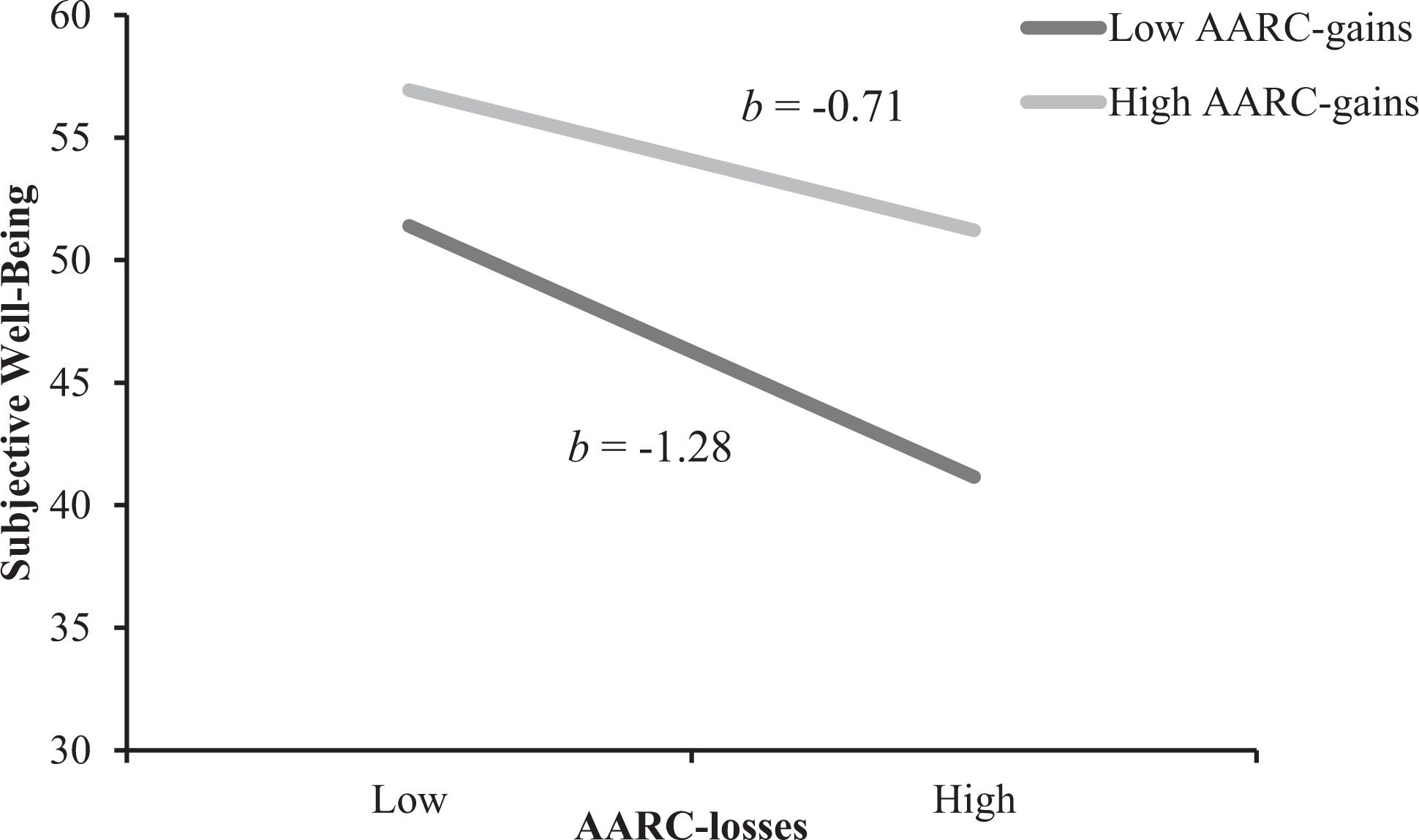
The Relationship Between AARC-Losses and AARC-Gains in Predicting Subjective Well-Being. Note. High and low values of AARC-losses and AARC-gains represent 1 SD above or below the mean. Both slopes are significantly different from zero (p < .001). bs represent slopes for AARC-losses at high and low values of AARC-gains. Predicted values shown here are based on regression parameter estimates reported in Table 2, Step 2 (n = 399). AARC = awareness of age-related change.
AARC-Gains as a Moderator of Associations Between AARC-Losses and Engagement With Life
Focusing first on participation in activities, the main effects model (Step 1) revealed a significant association for AARC-gains, which was associated with higher levels of activity participation (sr 2 = .15), whereas AARC-losses was not reliability associated with participation in activities. Addition of the AARC-losses × AARC-gains interaction term at Step 2 did not contribute significantly to model fit (See Supplementary Table 2).
Results of the regression analyses used to examine associations of AARC-losses and AARC-gains with life engagement are reported in Table 3. The analysis that included life engagement test scores as the dependent variable revealed main effects for AARC, with AARC-losses (sr 2 = .10) associated with lower levels of perceived engagement with life, and AARC-gains (sr 2 = .21) associated with higher engagement with life. At Step 2, the AARC-losses × AARC-gains interaction was statistically reliable, accounting for an additional 2% of the variance. Consistent with physical functioning and subjective well-being, the pattern of results pointed to the negative association of AARC-losses with engagement with life being weaker among those with higher AARC-gains (Figure 3, both slopes significantly different from zero at p < .001; at AARC-gains = −1 SD, AARC-losses b = −0.59, SE = 0.06; at AARC-gains = +1 SD, AARC-losses b = −0.32, SE = 0.05).
Hierarchal Regression Analysis Results: Engagement With Life (n = 399).
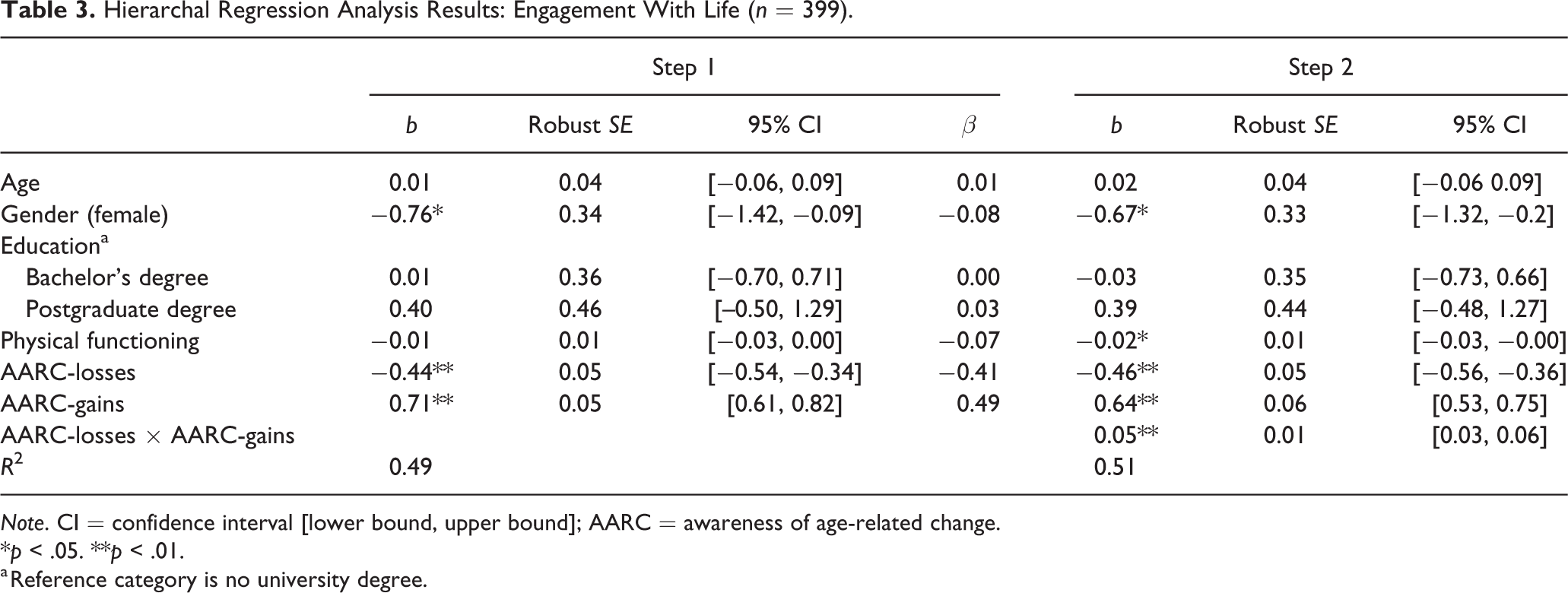
Note. CI = confidence interval [lower bound, upper bound]; AARC = awareness of age-related change.
*p < .05. **p < .01.
a Reference category is no university degree.
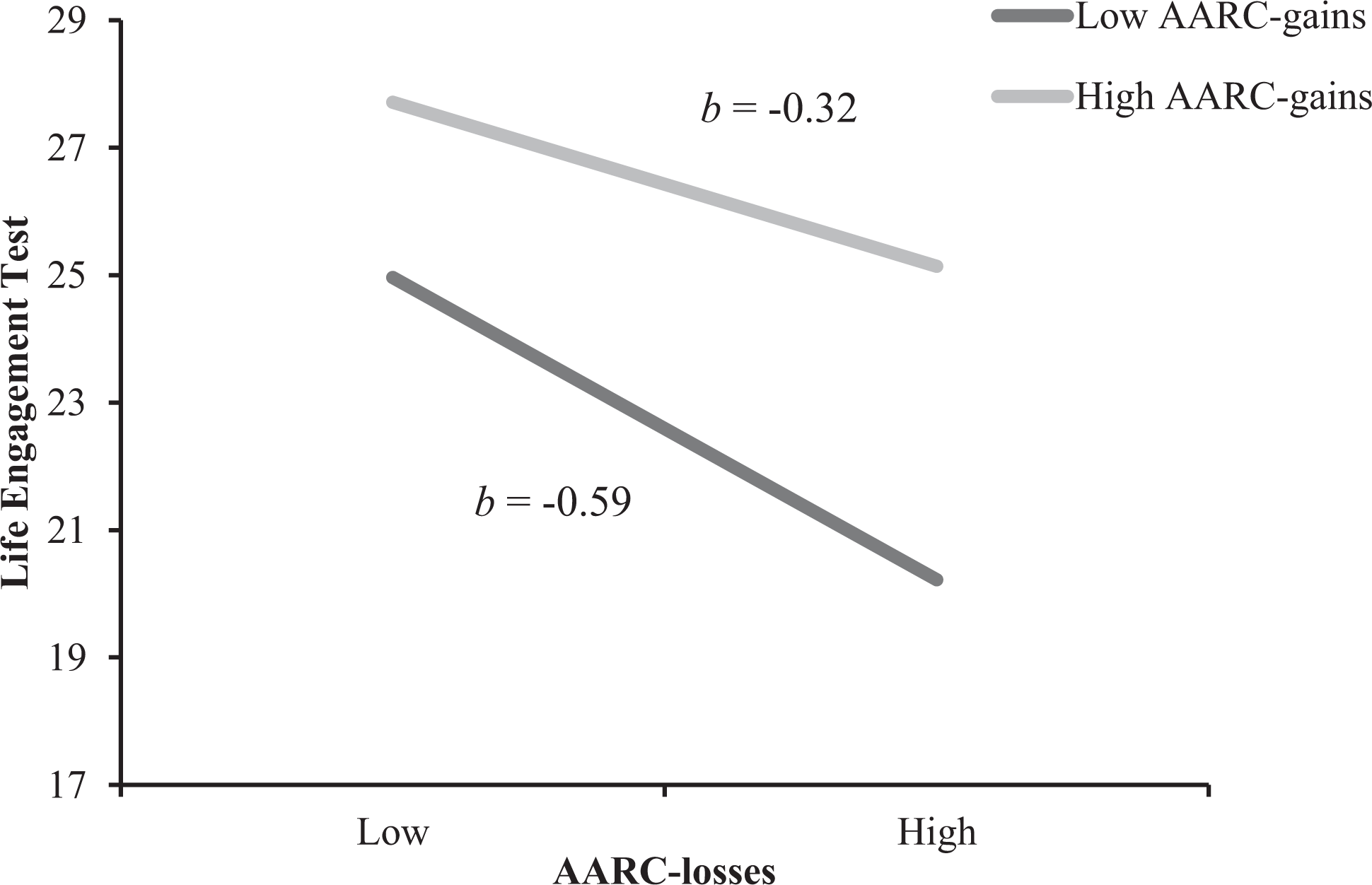
The Relationship Between AARC-Losses and AARC-Gains in Predicting Engagement With Life. Note. High and low values of AARC-losses and AARC-gains represent 1 SD above or below the mean. Both slopes are significantly different from zero (p < .001). bs represent slopes for AARC-losses at high and low values of AARC-gains. Predicted values shown here are based on regression parameter estimates reported in Table 3, Step 2 (n = 399). AARC = awareness of age-related change.
Discussion
Whereas previous research has focused on the independent main effects of AARC-gains and AARC-losses on aspects of health and well-being (e.g., Sabatini et al., 2020), we considered the extent to which negative associations of AARC-losses with health, well-being, and engagement with life would be weaker among those with reporting relatively higher AARC-gains. The findings generally supported our hypotheses, with moderating effects of AARC-gains evident in associations of AARC-losses with three out of four outcomes (physical functioning, subjective well-being, and engagement with life). The exception was activity participation, where only AARC-gains emerged as a significant correlate.
Taken together, our findings suggested that awareness of positive developmental changes associated with aging might to some degree offset deleterious effects on key developmental outcomes that arise from the awareness of age-related losses. As suggested by Diehl et al. (2014), a greater relative awareness of positive aspects of aging could help individuals to proactively engage with the environment via assimilative methods of coping (e.g., Brandstadter, 2009) in ways that facilitate adaptation in response to losses. With its focus on personal competencies and self-understanding, AARC-gains is also conceptually related to psychological coping resources such as self-esteem and self-efficacy which have also been shown to moderate associations of stressors with well-being (e.g., Hajek & Konig, 2019).
It was noteworthy that we did not find an interaction of AARC-losses with AARC-gains in the model that included participation in leisure activities as the outcome. Results from the relevant model showed that AARC-gains was associated with greater involvement in activity. Although the negative association of AARC-losses with activity engagement fell short of significance in the final adjusted model (p = .08), follow-up analyses (not shown) indicated that this was a result of shared variance between AARC-losses and physical functioning, suggesting that those in poorer health are both more aware of age-related losses and engage in less leisure activity. The divergent findings in relation to our two indices of engagement might reflect the fact that the PEAT captures self-reported volume of enjoyable activities (Pressman et al., 2009), whereas the life engagement test assesses the extent to which people find meaning and purpose in their activities (Scheier et al., 2006). While AARC-gains may not result in overall levels of leisure activity being better preserved in the presence of AARC-losses, AARC-gains may facilitate the selective re-prioritization of goals (e.g., Baltes, 1997; Brandstadter, 2009) in ways that help preserve a sense of meaning associated with activities. According to socio-emotional selectivity theory (Carstensen, 2006), as people grow older and view their time remaining as more limited, they place less importance on goals which expand their knowledge/experience, and invest more time and energy into goals from which they gain emotional meaning. It may be the case that an awareness of age-related loss that accompanies health restrictions commonly results in disengagement from overly challenging activities, and that this association does not vary as a function of AARC-gains. Based on our findings, we speculate that AARC-gains may, however, contribute to the construction of personal meaning around alternative activities that do not overly tax declining resources (see Hess, 2014). For example, attributes of AARC-gains captured by the AARC-10SF such as better appreciating personal relationships and better understanding what is important in life (Kaspar et al., 2019) might help older adults to assign value and meaning to comparatively less physically and cognitively demanding activities such as spending time with close others, even when overall levels of leisure activity may have been reduced.
Our results showed that across the outcome variables, the association of the AARC-losses × AARC-gains interaction with physical functioning was weaker than the associations of AARC-losses × AARC-gains with well-being and engagement with life. This could indicate that any protective effect of gains is less evident in the domain of health relative to well-being due to physical functioning being more age-vulnerable than socio-emotional functioning (Charles & Carstensen, 2010).
Limitations and Outlook
Our findings should be considered in the context of several limitations. First, our cross-sectional analysis did not allow for us to examine the stability of the identified relationships over time. While AARC-losses and AARC-gains have been demonstrated to independently impact well-being and developmental regulation over time (e.g., Dutt et al., 2018b), the potential for AARC-gains to buffer the negative effects of AARC-losses as aging and functional decline progress is not known. The study design also limits our ability to confirm the direction of the relationships identified here. While we have argued that AARC influences developmental regulation, and some emerging studies point to the effect of subjective ageing on health and well-being as being stronger than the reverse (Dutt et al., 2018a; Spuling et al., 2013), a degree of bidirectionality is likely. For example, declining health is likely to contribute to awareness of age-related losses, as well as being a developmental outcome influenced by awareness of aging (Diehl & Wahl, 2010). Indeed, in our data, the relatively large main effect of AARC-losses in the model with physical health as the outcome may well point to reverse causality (i.e., AARC-losses being more salient to those in poor health). Long-term longitudinal studies that include measures of AARC, significant developmental outcomes, as well as plausible intervening variables (e.g., measures of self-regulation) are needed to establish a better understanding of dynamic links between subjective perceptions of gains and losses and objective changes with aging that may take place over years and decades.
Second, participant self-selection into the study and completion of surveys online introduces a sampling bias in favor of those with relatively better health, cognition, and digital literacy. Participants in our sample reported higher mean scores for AARC-gains relative to AARC-losses; however, this pattern is consistent with those reported in previous studies (Brothers et al., 2016; Dutt et al., 2018a; Kaspar et al., 2019), indicating that the finding is not a unique reflection of our positively selected sample. Participants were relatively racially homogenous and reported high levels of education. The sample is therefore not broadly representative of older people, particularly marginalized groups. As research around the AARC concept continues to develop, it may be informative to contrast outcomes among those for whom an awareness of losses might be regarded as objectively accurate (e.g., those with age-related physical and/or cognitive impairments) with those for whom AARC-losses align with more enduring negative views of the self. Moreover, the moderating effects of AARC-gains on association of AARC-losses with the outcomes in our data showed small effect sizes and were relatively subtle. This was reinforced by results of simple slopes analyses which showed that negative associations of AARC-losses with well-being remained reliably different from zero even at high levels of AARC-gains. It may be that stronger (or indeed weaker) effects emerge in replication attempts with more diverse samples. However, based on the preliminary findings reported here, it seems likely that AARC-gains ameliorate rather than fully buffer negative associations of AARC-losses with health and well-being.
Notwithstanding these limitations, this study adds important new knowledge to the understanding of developmental regulation and well-being in older age. Our results replicate several previous studies demonstrating independent main effects of AARC-gains and AARC-losses on health, well-being, and engagement (see Sabatini et al., 2020). That AARC-gains were found to moderate the relationship between AARC-losses and poor outcomes suggests that the two constructs do not only operate independently. Rather, AARC-gains appears to have a protective function that can reduce negative effects of AARC-losses, at least for some important developmental outcomes. Research aiming to identify effective methods to strengthen AARC-gains could ultimately prove valuable for promoting the well-being of older people.
Supplemental Material
Supplemental Material, sj-docx-1-jbd-10.1177_01650254211039025 - Subjective perceptions of age-related gains buffer negative associations of perceived age-related losses with health, well-being, and engagement
Supplemental Material, sj-docx-1-jbd-10.1177_01650254211039025 for Subjective perceptions of age-related gains buffer negative associations of perceived age-related losses with health, well-being, and engagement by Tim D. Windsor, Mandy J. Abbott, Monica Cations, Alexis J. Howard and Bethany Wilton-Harding in International Journal of Behavioral Development
Footnotes
Acknowledgment
We thank Professor Hans-Werner Wahl for comments provided on an earlier version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.