
Abstract
Behavioral inhibition (BI) is an early-emerging temperamental trait characterized by a consistent tendency to respond with fear or withdrawal in unfamiliar situations. While BI is widely recognized as a strong early-life predictor of anxiety disorders, relatively little is known about whether the expression of BI varies across sociodemographic groups or whether it is sensitive to large societal stressors, such as the COVID-19 pandemic. The present study addressed these gaps by leveraging a large population-based sample (N = 8,631) of 4- to 7-year-old children. The data were drawn from a public health survey administered between 2018 and 2021 in the Netherlands. Linear regression analyses revealed that girls and children with a migration background showed higher levels of BI, while children’s age and parental educational level were only associated with specific BI subdomains, such as inhibited behavior when interacting with unfamiliar peers. However, all effect sizes were very small. No other significant associations were found, suggesting that BI is relatively stable across different population groups and unaffected by major societal stressors such as the COVID-19 pandemic. These findings provide new insights into the population-level stability of BI and underline the importance of further longitudinal research into environmental and contextual influences on BI.
Introduction
From the first cautious steps of a toddler to the hesitant approach of a child meeting new peers, the nuances of early behavior reveal much about their inherent personality. Some children explore their world without any fear, while others tend to exhibit noticeable caution and restraint. These early behaviors are expressions of a child’s temperament, which can be defined as foundational individual differences in activity, affectivity, attention, and self-regulation (Shiner et al., 2012). Temperamental traits emerge early in life and are formed by interactions between genetic, biological, and environmental factors (Shiner et al., 2012). Although individual differences in temperament are typically not problematic, certain patterns can predispose children to mental health challenges later in life.
One temperamental style that can significantly affect a child’s development is behavioral inhibition (BI). A behaviorally inhibited temperament is characterized by fearfulness, restraint, shyness, and withdrawal in response to unfamiliar people, objects, or situations (Clauss & Blackford, 2012; Fox et al., 2005; Henderson et al., 2015). BI is already noticeable in early childhood; 15% to 20% of healthy children are born with high levels of BI (e.g., Kagan & Snidman, 1999). These children have the consistent tendency to respond to unfamiliar situations as if they are threats, resulting in increased physiological reactions such as elevated heart rates and cortisol levels and heightened vigilance and cautiousness (Clauss & Blackford, 2012; Fox et al., 2005; Henderson et al., 2015). Studies consistently reported that children with high BI levels are at a greater risk of developing anxiety problems in later life, particularly social anxiety disorder (Clauss & Blackford, 2012; Sandstrom et al., 2020). In addition, BI is linked to negative affect and disengaged emotion regulation; children with high levels of BI experience more negative emotions, which they tend to suppress instead rather than manage them through healthy coping strategies including problem-solving and seeking social support (Leen-Feldner et al., 2004; Penela et al., 2015). Hence, high levels of BI in early childhood are associated with an increased risk of later mental health problems, thereby creating opportunities for prevention (Mian, 2014; Rapee et al., 2005). Gaining insight into this temperamental pattern is therefore of key importance.
Research has already provided valuable insights into developmental patterns of BI. Much of this knowledge has been derived from studies using extensive laboratory-based observations, capturing both behavioral and physiological features of BI (e.g., Pérez-Edgar & Fox, 2018; Sandstrom et al., 2020). These intensive methods have clarified how BI develops within individuals, showing that while this trait is moderately stable over time, it is not always a fixed characteristic (Chronis-Tuscano et al., 2009; Degnan & Fox, 2007). In fact, although high levels of BI often persist, there is also a significant proportion of children that display a meaningful decrease in inhibited behavior over time and do not develop subsequent mental health problems (Degnan & Fox, 2007). Factors related to this variability in developmental trajectories are varied and complex and consist of both internal factors including cognitive processes (White et al., 2011), external factors such as parenting (Ryan & Ollendick, 2018), and broader environmental circumstances (Liu et al., 2023).
Nevertheless, while these observational studies have been fundamental for understanding individual temperamental trajectories, these designs are less suited for large-scale population research, as these procedures are costly and highly time consuming (Bishop et al., 2003). As a result, current knowledge about BI has largely been derived from relatively small or selective samples, limiting insight into how BI is distributed across the population. Insight into demographic and contextual variation in BI is needed to understand whether elevated levels of inhibition occur uniformly across children or are more common in particular subgroups. This knowledge is essential to be able to predict which children are potentially at greater risk for later mental health problems, enabling a more targeted approach for early intervention. Parent-reported questionnaires offer a more efficient alternative for assessing BI in larger samples and have demonstrated moderate convergence with observational measures (Bishop et al., 2003; Van Brakel et al., 2004; Vreeke et al., 2012). Although this has enabled initial investigations into demographic differences in BI, for example across gender (Fernandes et al., 2022; Paulus et al., 2015) and migration background (Vreeke et al., 2013), evidence on the variation BI within larger, representative samples of young children remains limited, restricting the ability to draw broader conclusions. In addition, less attention has been given to other contextual factors, such as family composition and the broader ecological context in which a child grows up, including the impact of significant societal events. Widespread societal disruptions, such as the coronavirus disease of 2019 (COVID-19) pandemic, may exacerbate temperamental vulnerabilities in young children, for example through increased stress, disrupted routines, and limited opportunities for social interaction. These shifts may alter early social experiences during a critical developmental period, potentially increasing inhibitory tendencies (Alcon et al., 2024).
To address these knowledge gaps, the current descriptive epidemiologic study, which included a very large and representative sample of children aged 4 to 7 years in the Netherlands, aimed to investigate the associations between BI and a wide range of sociodemographic characteristics (i.e., age, gender, migration background, parental educational level, family composition, region of residence, urbanization of the home environment). Furthermore, recognizing that BI is susceptible to environmental influences, our study also explored the impact of the COVID-19 crisis on BI levels over the years around the crisis. Given the limited and sometimes conflicting evidence regarding these potential associations, this study was primarily exploratory in nature. However, to provide a clear direction for our data analyses, we formulated the following hypotheses based on the available broader literature. First, although two previous studies in preschoolers reported no gender differences in BI levels (Fernandes et al., 2022; Paulus et al., 2015), we hypothesized that girls in our sample would demonstrate higher levels of BI than boys. This expectation is based on broader developmental research showing that girls exhibit higher levels of anxiety, withdrawal, and other internalizing behaviors compared with boys (Chaplin & Aldao, 2013; Gagne et al., 2013; Keyes & Platt, 2024). In addition, our large sample size enables the detection of potential subtle gender differences that might not have been captured in previous, smaller studies (Fernandes et al., 2022; Paulus et al., 2015). Regarding age, we hypothesized that the expression of BI would not differ between younger and older children, reflecting the moderate stability of BI during childhood (Chronis-Tuscano et al., 2009). Furthermore, we expected that potentially unfavorable social circumstances would be associated with higher BI levels, as socioeconomic disadvantages are commonly linked to mental health disparities (Kirkbride et al., 2024). Specifically, these factors included lower parental educational levels, single-parent or divorced households, migration backgrounds, and lower urbanized regions (Dinisman et al., 2017; Kirkbride et al., 2024). Finally, we anticipated that children’s average BI levels would be higher during the COVID-19 crisis compared with before the crisis, in line with meta-analytic evidence that showed that pandemic-related stressors led to small increases in emotional reactivity, anxiety, and withdrawal symptoms in preschool-aged children (Alcon et al., 2024). By identifying potential protective and risk factors related to BI, this research will provide valuable insights that can inform more effective intervention strategies, ultimately supporting better outcomes for behaviorally inhibited children.
Methods
Study Design and Setting
This descriptive cross-sectional epidemiologic study utilized anonymized data from a digital parental questionnaire known as ‘Jij en Je Gezondheid’ (translation: ‘You and Your Health’; JEJG), developed by the Public Health Service Amsterdam in 2017 (Public Health Service Amsterdam, 2026). This parental questionnaire is used to assess the health and development of children prior to the routine appointment with a youth health care professional during their first elementary school years. The questionnaire is implemented by youth health care services in various regions of the Netherlands, including the Amsterdam region – a large urban center surrounded by smaller towns and villages in the west of the country – and the provinces of Groningen, Drenthe, and Flevoland – located in the north and center of the Netherlands and characterized by rural landscapes, agricultural areas, and smaller cities. The collected data were suitable for analyzing associations between BI and population characteristics such as gender, migration background, and parental educational level. Data were collected per school year and were available from school year 2018–2019. As the measure of BI in the JEJG questionnaire was adjusted in school year 2021–2022, we used the data from school years 2018–2019, 2019–2020, and 2020–2021. Anonymous reuse of public health data did not require formal ethical approval under Dutch law (Article 1, Paragraph 2 of the Medical Research Involving Human Subjects Act). For the current research purposes, institutional ethical approval was obtained from the Psychology Research Ethics Committee of Leiden University in January 2023 (V1-4155). The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines and adhered to recommendations for reporting descriptive studies (Lesko et al., 2022; Von Elm et al., 2007).
Participants and Procedures
Parents with a child around the age of 5 were invited by the Public Health Service to fill in the questionnaire. After completing the questionnaire, parents received immediate feedback based on their answers and were invited to schedule an appointment with a youth health care professional, who also reviewed the child’s scores. During the appointment, the youth health care professional could provide additional guidance and recommendations if necessary. After each school year, the Public Health Service Amsterdam combined all the questionnaire data into a dataset, removed all personal identifiable information, and cleaned the data, thereby making it available for research purposes.
The questionnaire was completed by parents from a total of 8,643 children around the age of 5 years (range, 4–7 years). We excluded cases with missing values on the questionnaire measuring BI (n = 12), resulting in a sample of parents of 8,631 children. All parents completing the questionnaire gave written informed consent that their anonymized answers could be used for public health research.
Measures
The JEJG questionnaire consisted of several sub-questionnaires, of which the following factors were considered for the current study.
Population Characteristics
The child’s age was recorded in whole years, as decimal values were not available. Gender was categorized as either ‘boy’ or ‘girl’. Migration background was classified as ‘Dutch’ (i.e., both parents and the child were born in the Netherlands), ‘Western migration background’ (i.e., the child and/or a parent were born in another European country, North America or another Western oriented country such as Australia and New Zealand), or ‘non-Western migration background’ (i.e., the child and/or a parent were born in a country in Africa, Asia, or South America). Parental education was classified as ‘low’ (i.e., primary, lower secondary, or lower vocational education), ‘medium’ (i.e., upper secondary or intermediate vocational education), or ‘high’ (i.e., higher professional or university education). Family composition was classified as ‘original two-parent household’ (i.e., child lives together with both (biological) parents), ‘one-parent household’ (i.e., child lives with one parent only), or ‘reconfigured or other family structure’ (i.e., co-parenting, child lives together with one of their biological parent and his or her (new) partner, or another family structure). The family’s region of residence was recorded as Amsterdam, Groningen, Flevoland, or Drenthe. Due to the limited regional variability in the available data, with the JEJG predominantly administered in Amsterdam, the variable was dichotomized into ‘Amsterdam region’ and ‘other Dutch region’. Finally, the urbanization level of the home environment was determined based on postal codes and was categorized into three levels: ‘strongly urbanized’ (i.e., >1,500 addresses per square kilometer), ‘moderately urbanized’ (i.e., 1,000–1,500 addresses per square kilometer), or ‘hardly urbanized’ (i.e., <1,000 addresses per square kilometer; Statistics Netherlands, 2026).
Behavioral Inhibition
BI was measured with the Dutch version of the Behavioral Inhibition Questionnaire – Short Form (BIQ-SF), a 14-item parental questionnaire with strong psychometric properties (Edwards, 2007; Vreeke et al., 2012). Parents rated the frequency of their child’s inhibited behaviors on a 6-point Likert-type scale ranging from hardly ever (1) to almost always (6). The questionnaires measure BI across six subscales, reflecting situations wherein behaviorally inhibited children typically exhibit this behavior: interactions with unfamiliar peers (three items), unfamiliar adults (two items), and in unfamiliar situations (three items); adjusting to new settings (referred to as ‘preschool/separation’ by Vreeke et al. (2012); two items); performance in front of others (two items); and facing physical challenges (two items). Total BIQ-SF scores were derived by summing the ratings on all items, resulting in a possible score range from 14 to 84. Higher scores indicated a higher level of inhibited behavior. In addition, subscale scores were calculated by summing the ratings of relevant items for each context. In the current sample, the total BIQ-SF score showed good internal consistency (α = .90; ω = .90). At the subscale level, sufficient internal consistency was observed for unfamiliar peers (α = .86; ω = .86), unfamiliar adults (α = .88; ω = .89), unfamiliar situations (α = .78; ω = .80), new settings (α = .78; ω = .78), and performance (α = .75; ω = .76). Only the physical challenges subscale showed lower internal consistency (α = .51; ω = .53).
Moment of Questionnaire Completion – COVID-19 Pandemic
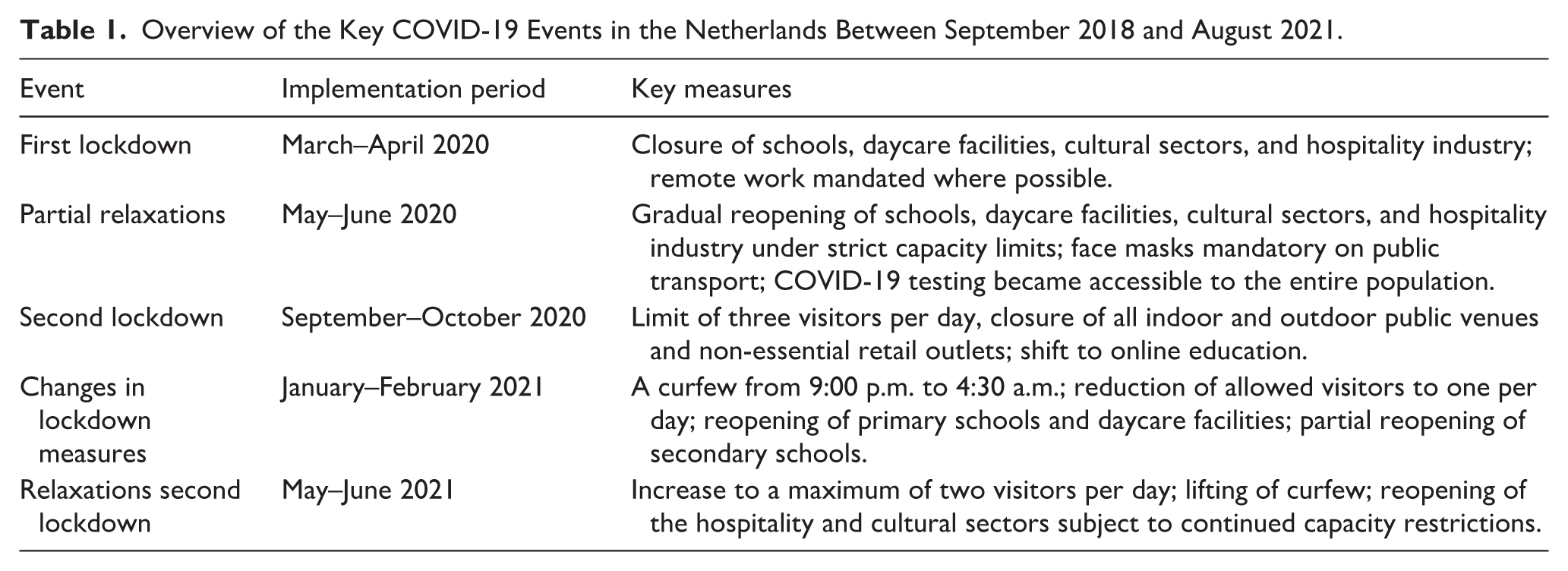
The month and year of questionnaire completion were recorded. To reduce large variations in the number of respondents per time period and create more balanced group sizes, the months of questionnaire completion were grouped into 2-month periods, resulting in 18 2-month periods spanning from September–October 2018 to July–August 2021. These 2-month periods were subsequently analyzed in relation to the most important events related to the COVID-19 pandemic in the Netherlands that may have affected children’s mental health (Panchal et al., 2023). We distinguished five key events, as outlined in Table 1. These events included the first lockdown (March–April 2020), the following partial relaxations (May–June 2020), the second lockdown (September–October 2020), changes in these lockdown measures (January–February 2021), and relaxations of the second lockdown (May–June 2021; Hoekman et al., 2020; National Institute for Public Health and the Environment, 2026a, 2026b).
Overview of the Key COVID-19 Events in the Netherlands Between September 2018 and August 2021.
Statistical Analysis
The data were obtained as Statistical Package for the Social Sciences (SPSS) files and subsequently cleaned using IBM SPSS Statistics version 29. Further data analyses were conducted using R (version 4.3.3; R Core Team, 2024). Descriptive statistics were calculated to describe the study population. To assess the potential associations between the population characteristics and BI, seven linear multivariable regression analyses were performed. The dependent variables included the continuous total BIQ-SF score and the scores of its six subscales, while the population characteristics were included as the independent variables. To account for multiple testing across the seven regression models, a Bonferroni correction was applied, adjusting the significance threshold by multiplying each p-value by 7. To assess the influence of the COVID-19 crisis on the average BI levels, another linear regression analysis was performed with the categorical variable indicating the 2-month period as the independent variable and the continuous total BIQ-SF score as the dependent variable. When statistically significant findings emerged from this analysis, a post hoc analysis was performed to examine whether the observed association could be explained by differences in population characteristics. In this analysis, the population characteristics were added to the model to examine whether the identified association remained statistically significant.
All relevant assumptions for the regression analyses were checked and met. Across all analyses, the lowest category of each categorical independent variable was used as the reference category, as listed in Table 2, and was omitted from the regression tables. Only age was analyzed continuously. Given the large sample size, which increases the likelihood of detecting statistically significant effects, standardized regression coefficients (β) were reported, as well as partial eta squared values (ηp2) as a measure of effect size. Partial eta squared values were interpreted according to Ferguson (2009) with .040 indicating a small effect, .250 a medium effect, and .640 a large effect. For the seven models assessing population characteristics, Bonferroni-adjusted p-values (padj) were reported, while for the COVID-19 analysis, unadjusted p-values (p) were used. Statistical significance was evaluated at α = .05. Unstandardized regression coefficients (B), associated 95% confidence intervals (CI), standard errors (SE), and unadjusted p-values for all the analyses can be found in Supplemental Appendix 1.
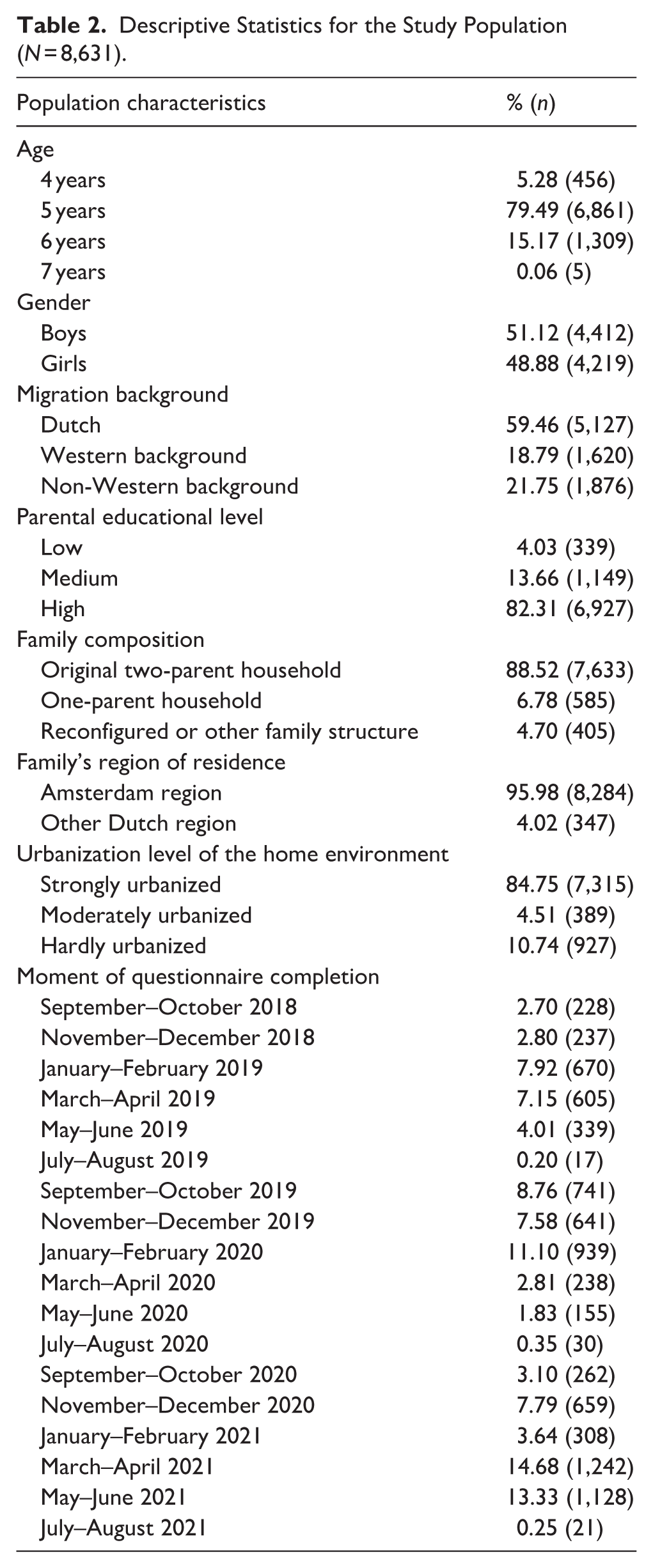
Descriptive Statistics for the Study Population (N = 8,631).
Results
Table 2 presents the descriptive statistics for the study population. Data were analyzed for parents of 8,631 children with a mean age of 5.10 years (SD = 0.44) and a mean total BIQ-SF score of 34.44 (SD = 10.43). Data regarding parental educational level was missing for 216 children (2.50%) and migration background and family composition for eight children (<.10%), with all other characteristics complete.
Associations Between Population Characteristics and BI
Table 3 shows the results of the linear regression analyses examining the associations between population characteristics and BI, as measured by the total BIQ-SF score. Table 4 presents the associations between population characteristics and the BIQ-SF subscales, which captured the different situations wherein behaviorally inhibited children typically exhibit this behavior. Since all population characteristics were simultaneously included in the regression models, the reported associations represent mutually adjusted effects. Girls and children with a migration background had significantly higher total BIQ-SF scores compared with boys and children with a Dutch background. However, partial eta squared values indicated that these effects were very small (ηp2 < .040). No other significant associations with the total BIQ-SF score were observed. Analyses of the BIQ-SF subscales showed that both girls and children with a migration background scored higher on the subscales unfamiliar peers, unfamiliar adults, unfamiliar situations, and physical challenges but lower on the performance subscale. Partial eta squared values remained below .040, indicating very small effect sizes.
Associations Between Population Characteristics and Behavioral Inhibition as Measured With the Total Behavioral Inhibition Questionnaire – Short Form (BIQ-SF) Scores (N = 8,631).
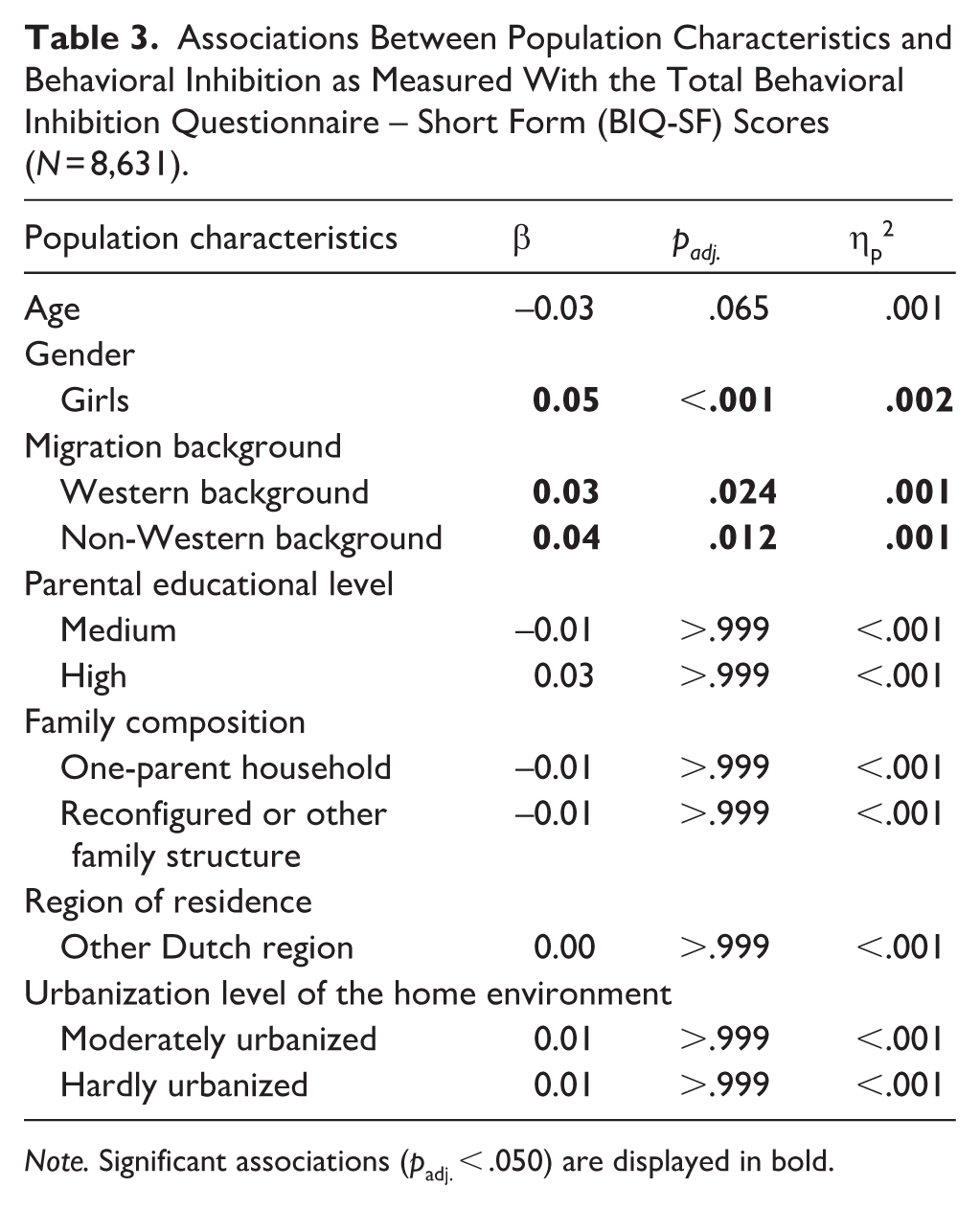
Note. Significant associations (padj. < .050) are displayed in bold.
Associations Between Population Characteristics Behavioral Inhibition as Measured With the Behavioral Inhibition Questionnaire – Short Form (BIQ-SF) Subscale Scores (N = 8,631).
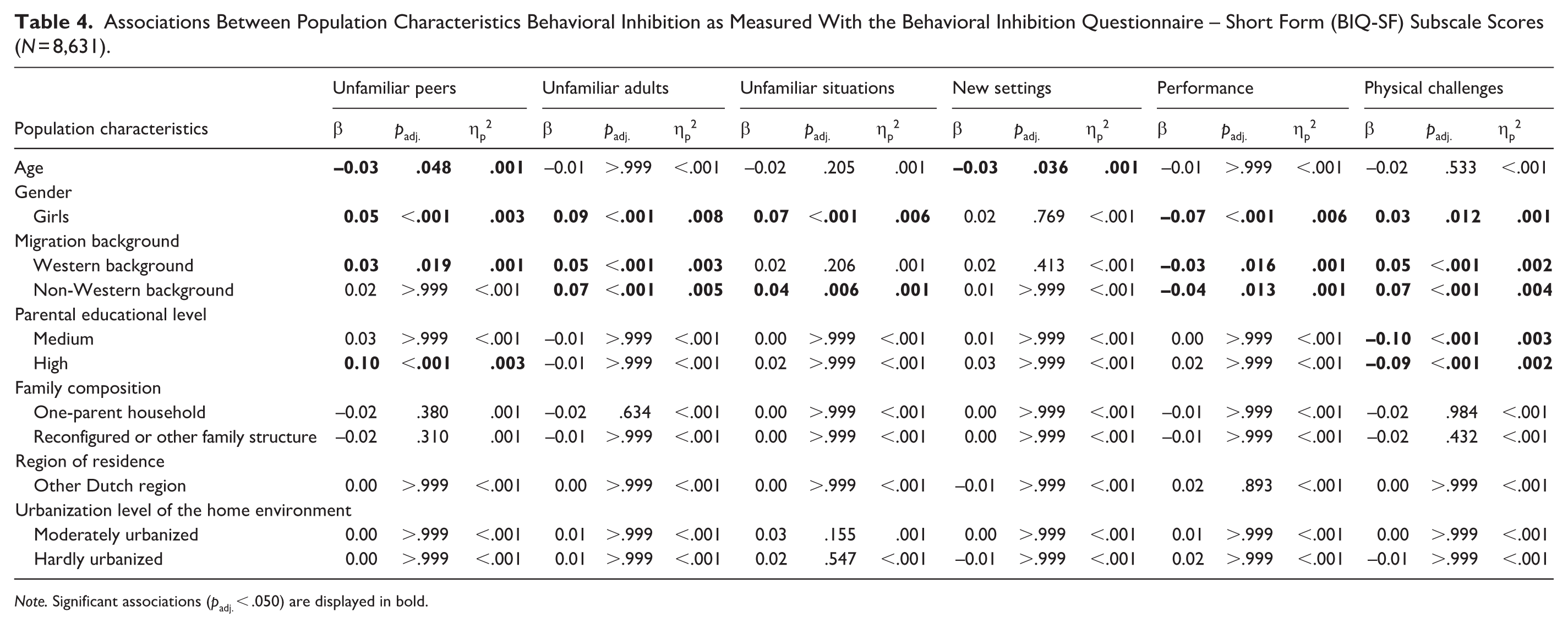
Note. Significant associations (padj. < .050) are displayed in bold.
In contrast to the findings for the total BIQ-SF scores, significant associations with age and parental educational level were observed for specific BIQ-SF subscales. Age was significantly associated with unfamiliar peers and new settings scores, with older children scoring lower than younger children. Furthermore, children of parents with a low educational level scored lower on unfamiliar peers than those of parents with a high educational level and higher on physical challenges than those of parents with a medium or high educational level. For these associations, partial eta squared values also indicated very small effect sizes (ηp2 < .040). No statistically significant associations were found between BI and family composition, region of residence, or the urbanization level of the home environment.
Association Between the Month and Year of Questionnaire Completion and BI
For parents of 8,460 out of the total of 8,631 children, the month and year of completing the questionnaire were recorded (<2% missing data). The mean number of respondents per 2-month period was 470, with a range from 17 to 1,242 respondents per period, as the questionnaire was typically completed between September and June, outside of the summer holidays (see also Table 2). In Figure 1, the development of the average total BIQ-SF scores over time is presented. The linear regression analysis showed that average BIQ-SF scores of parents completing the questionnaire in July–August 2019 (n = 17) were significantly lower compared with parents completing the questionnaire in September–October 2018 (n = 228; β = −0.03, p = .002, ηp2 = .001). No other statistically significant associations were identified.
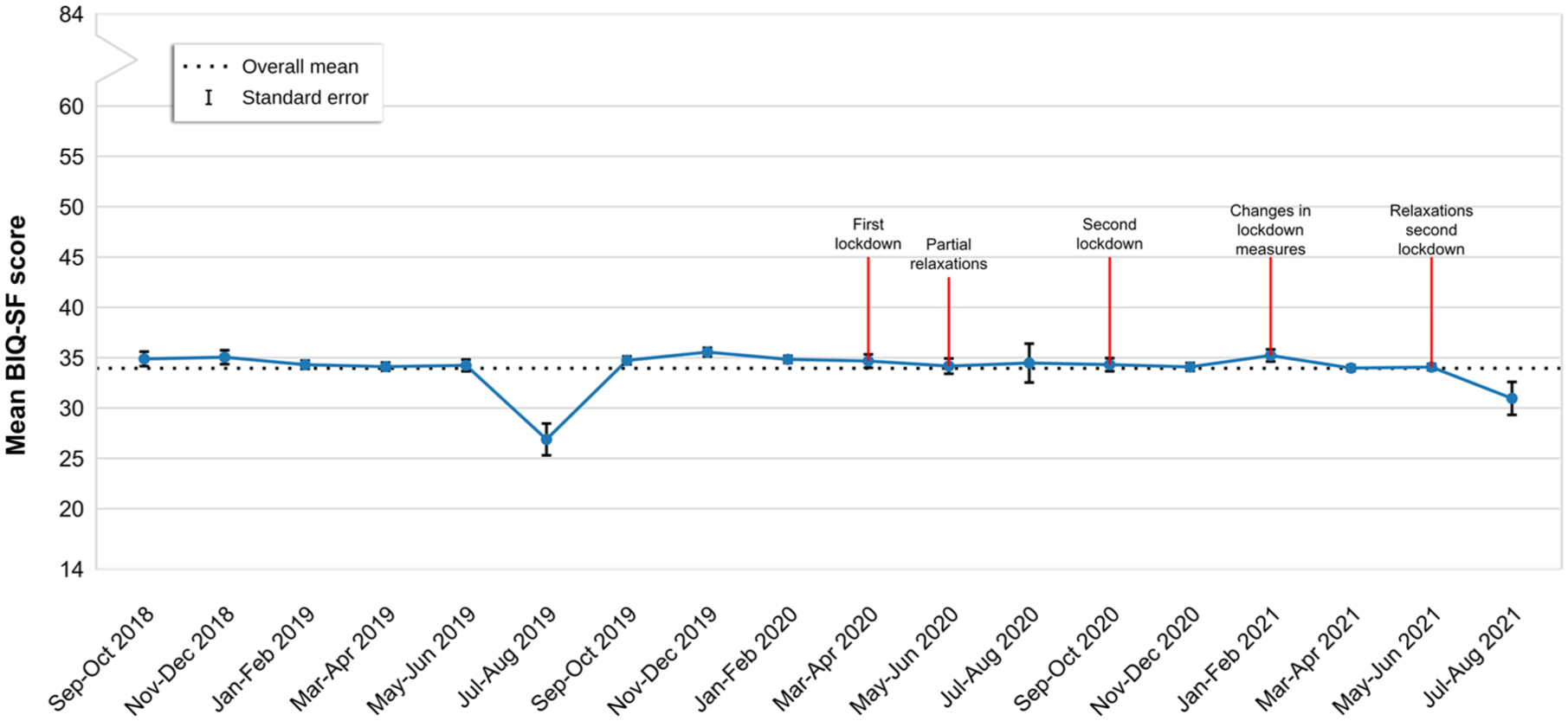
The development of the average levels of behavioral inhibition over time and its relation with the COVID-19 measures (n = 8,460).
A post hoc analysis was conducted to examine whether the association between parents completing the questionnaire in July–August 2019 and total BIQ-SF scores could be explained by the other population characteristics, by adding these variables to the model. The observed association remained statistically significant in the adjusted model (β = −0.03, p = .003), indicating that this association could not be attributed to these characteristics. However, as this period is before the first COVID-19 lockdown, this was unrelated to the COVID-19 measures.
Discussion
This study explored the distribution of BI and its associations with various population characteristics, including age, gender, migration background, parental educational level, family composition, region of residence, and urbanization level of the home environment, as well as the potential impact of COVID-19 measures in a large, representative, non-clinical sample of 4- to 7-year-old children. While small differences in BI were observed based on gender and migration background, associations with age and parental educational level were limited to specific BI domains. No associations were found between BI and other population characteristics or COVID-19 measures, suggesting that BI was largely evenly distributed across the population and that average levels of BI remained stable over time across the population. Understanding these distributions and associations is essential, as early BI has been linked to later anxiety disorders. Therefore, identifying potential patterns within the population may inform early detection strategies.
The current findings regarding the observed differences in BI based on gender and migration background align with previous research reporting gender and cultural differences in children’s temperament (e.g., Chen, 2018; Else-Quest et al., 2006), which may extend to specific traits such as BI. Earlier studies similarly reported higher levels of shyness and withdrawn behavior in girls compared with boys (Charbonneau et al., 2009; Gagne et al., 2013) and higher levels of BI in children from non-Western backgrounds compared with those from Western backgrounds (Rubin et al., 2006). However, evidence for these differences remains inconclusive, as previous studies did not report similar findings (Fernandes et al., 2022; Paulus et al., 2015; Vreeke et al., 2013), and we found reversed associations for the performance subscale. The inconsistent findings may be partially attributed to variability in the methods used to assess BI, differences in sample composition, and how studies accounted for potential confounding variables such as socioeconomic position (SEP). Another possible explanation is the influence of cultural norms and values on how BI is perceived and socially reinforced (Sanson et al., 2004). In many cultures, inhibited behavior is more socially accepted in girls than in boys, as it aligns with traditional expectations that girls should be more reserved and well-behaved, whereas boys are expected to be more outgoing and active (Doey et al., 2013). In addition, while BI is often associated with social competence in non-Western cultures, it tends to be perceived more negatively and linked to peer rejection in Western contexts (Lane & Song, 2015; Rubin et al., 2009). These gender norms and cultural differences may shape how BI is expressed, interpreted, and reported by parents, contributing to variability across populations, contexts, studies, or even between individual families. Furthermore, it is important to note that all observed effect sizes were very small, which suggests that their practical significance may be limited and should be interpreted with caution.
Our study also found that younger children exhibited higher BI levels in peer interactions and in new settings compared with older children. These observed age differences might reflect a natural developmental trend, where older children gradually become more confident in social activities. In addition, children with lower-educated parents displayed lower BI levels in peer interactions but higher BI levels when facing physical challenges. These findings align with research suggesting that socioeconomic conditions shape temperament expression. Lower SEP has been associated with greater emotional reactivity and lower persistence, which may contribute to higher BI levels in physically demanding situations (Jansen et al., 2009; Strickhouser & Sutin, 2020). However, the lower BI levels in peer interactions and the absence of associations with other BIQ-SF subscales suggest that SEP-related associations are context-dependent rather than uniform across domains. Moreover, BI is not a direct health outcome but a temperamental trait that is influenced by a combination of environmental exposure and parental perception. Since these factors were not measured in the current study and the BIQ-SF subscales consist of only a few items, it remains uncertain whether these identified patterns reflect meaningful associations and truly indicate differences in anxiety vulnerability. Further research is needed to better understand these relationships between SEP and BI.
Another notable finding was that the average BI levels remained consistent over time across the population, with no associations related to the COVID-19 pandemic. This finding is in line with a recent cohort study investigating shyness levels during and before the pandemic (Schmidt et al., 2025). While previous studies have documented increased anxiety symptoms in children during the COVID-19 pandemic (Madigan et al., 2023; Panchal et al., 2023) and linked BI in toddlerhood to higher anxiety in young adults during the pandemic (Zeytinoglu et al., 2021), our findings suggest that BI itself was unaffected, supporting the notion that it represents a trait-like characteristic rather than a transient emotional response (e.g., Pérez-Edgar, & Fox, 2018). An exception to this overall stability was observed in July–August 2019. In this period, average BI levels were significantly lower which could not be explained by differences in other population characteristics. However, this is likely attributable to the very small number of respondents in this period (n = 17), suggesting that this finding may reflect a statistical anomaly rather than a meaningful pattern. Nevertheless, due to the cross-sectional design of the study and the absence of anxiety-related questions in the JEJG questionnaire, we cannot infer causality or determine the impact of the pandemic on anxiety levels in our sample. Therefore, it remains possible that the within-person developmental trajectory of BI and its association with anxiety were affected by the COVID-19 crisis, highlighting the need for longitudinal research to examine the long-term impact on young children.
The findings should be interpreted in light of several strengths and limitations. A major strength of this study is its large and representative sample with minimal missing data, which enhances the generalizability of the findings. In addition, as the data were originally collected for health monitoring, rather than specifically for research purposes, and all parents of children around the age of 5 within the participating regions were invited to fill in the questionnaire, the risk of selection and response bias was substantially lower compared with other studies. Furthermore, BI was assessed using a validated parent-reported questionnaire. Although parent-reported measures are inherently sensitive to informant bias, they allow for the assessment of children’s behavior across a broader range of everyday contexts that are difficult to capture in laboratory-based observations (Bishop et al., 2003). Moreover, the use of parent-reported measures enabled the inclusion of a very large sample, which would not have been feasible using observational methods. Limitations include the lack of blind assessments, as the youth health care professional had access to the parents’ responses for the routine appointment. This may have led to socially desirable answering, potentially influencing the results. Another limitation is that age could only be analyzed in whole years, resulting in limited variance within this variable. As a result, our findings might not have captured the developmental nuances that occur within this age period. Furthermore, as the internal consistency of the physical challenges subscale was low, these results should be interpreted with caution as they might not accurately reflect the true underlying construct of BI in these situations. Finally, due to the cross-sectional design, no causal inferences can be drawn.
In conclusion, this study contributes to the growing body of research on BI by demonstrating that, although very small differences were observed based on gender, migration background, age, and parental educational level, BI appeared to be largely evenly distributed across the population. No evidence was found for an association between COVID-19 measures and BI, suggesting that the average BI levels of 4- to 7-year-old children remained stable during this period. Using a large and representative sample, this study addresses previous limitations in BI research, which often relied on selective or non-representative samples. These findings highlight the complex interplay between sociodemographic and environmental factors in shaping the expression of BI. Although the observed effects were small, identifying these factors is an essential step toward understanding which children may be more vulnerable to persistent BI and later anxiety. Future research should explore how these influences evolve over time and whether they contribute to differential mental health trajectories, ultimately informing the development of early interventions to support behaviorally inhibited children.
Supplemental Material
sj-xlsx-1-jbd-10.1177_01650254261461445 – Supplemental material for Behavioral Inhibition in Young Children: A Descriptive Study in a Very Large Non-Clinical Population
Supplemental material, sj-xlsx-1-jbd-10.1177_01650254261461445 for Behavioral Inhibition in Young Children: A Descriptive Study in a Very Large Non-Clinical Population by Nina L. Komrij, Mia P. Kösters and Leonie J. Vreeke in International Journal of Behavioral Development
Footnotes
Acknowledgements
The authors thank Anouk Wisse from the Public Health Service Amsterdam for the collaboration in providing and processing the ‘Jij en Je Gezondheid’ data and Dr. Frank de Vos for the statistical advice and guidance.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. Anonymous reuse of public health data did not require formal ethical approval under Dutch law (Article 1, Paragraph 2 of the Medical Research Involving Human Subjects Act). For the current research purposes, institutional ethical approval was obtained from the Psychology Research Ethics Committee of Leiden University in January 2023 (V1-4155).
Consent to Participate
All participants gave written informed consent that their anonymized answers could be used for public health research.
Author Contributions
Conceptualization: NLK, MPK, LJV; Methodology: NLK, MPK, LJV; Data curation: NLK; Formal analysis and investigation: NLK; Visualization: NLK; Writing – original draft preparation: NLK; Writing – review and editing: NLK, MPK, LJV; Funding acquisition: MPK, LJV.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw, the Netherlands Organization for Health Research and Development (grant number 555002021).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon request from the Public Health Service of Amsterdam and can be obtained by contacting
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.