
Abstract
Navigating healthcare infrastructures is particularly challenging for queer-identifying individuals, with significant barriers emerging around stigma and practitioner ignorance. Further intersecting, historically marginalised identities such as one’s race, age or ability exacerbate such engagement with healthcare, particularly the access to and use of reliable and appropriate health information. We explore the salience of one’s queer identity relative to other embodied identities when navigating health information and care for themselves and their communities. Thirty semi-structured interviews with queer community leaders from South Carolina inform our discussion of the role one’s queer visibility plays relational to the visibility of other identities. We find that leaders and their communities navigate these intersectional visibilities through unique and iterative approaches to health information seeking, sharing and use predicated upon anti-queer, racist, ableist and misogynistic sentiments. Findings can inform queer-inclusive, intersectionally informed interventions by health and information professionals such as non-profit advocacy organisations and medical librarians.
1. Introduction
This article starts with a reflective question: Should healthcare and information professionals make information and resources on HIV/AIDS preventive care most visible to Black, queer communities, who are disproportionately affected [1]? A ‘yes’ response evokes what is well-established in public health [2], communication [3] and information science [4] literature: HIV-related health disparities exist among Black, queer communities, and informational and advocacy-based interventions can combat these disparities. However, centering the experiences of the communities in question reframes these assumptions. Historically, social and healthcare institutions have framed queer bodies as deviant, in part, due to their becoming medialised objects. In turn, medicalisation reinforces the persistence of queer bodies as being infected or capable of infecting others, reifying this problematic deviancy [5,6]. The relationship between medicine and people of colour (specifically Black communities) is one of exploitation and systematic violence, which marks Blackness as abnormal and inhuman, thus legitimising it as a body on which to experiment [7]. From this perspective, the hypervisibility of information and resources on HIV/AIDS preventive care within Black, queer communities marks their bodies as sites of medical testing and advancement. Such informational resource allocation affirms queer visibility to be the embodiment of identity. This embodiment occurs within societal spaces, and how those embodiments are perceived and described become informed within and against normative discourses.
Informed by interviews with 30 queer community leaders in South Carolina, this article examines how queer visibility mediates communities’ engagements with health information. Within a health context, information can empower queer communities to define their own health needs, meanings and values, rather than having these needs imposed on them by others [8]. We also understand queer visibility as existent alongside other various intersecting identities. Queerness and other salient identities impact how queer communities engage with health information, and what information is made visible to them is not monolithic. Race, among other factors, might precede queerness in a community’s relationships to health information [9]. As will be explained, we use queer as an umbrella term that describes the complex and continually expanding understandings of gender and sexuality within and outside of binarised modes of thinking [10]. The rest of the article proceeds as follows. First, we review relevant literature exploring the relationship between queer visibility, intersectionality and embodied information. Next, we overview the qualitative methods used to explore our research questions informed by the literature review. Then, we frame our findings across three constructs describing how queerness operates as visible, invisible and hypervisible identities and explore how each construct shapes community health information practices. We conclude by identifying how this work contributes and advances prior research and share implications for information professionals working with queer communities.
2. Literature review
2.1. Queer visibilities
Before addressing the ethics of queer visibility, we first acknowledge the complexity around the term queer itself, especially given the use of the term within individual identificatory practices and larger LGBTQIA+ communal spaces. While both authors are queer-identifying individuals, this is not to say that it is a term with universal appeal or applicability. In particular, the term’s long history of use has been one marked by a negation of societal acceptance and most consistently rendered individuals as outsiders to normative society [11]. Our use, however, attends not to ignore this history nor to suggest that every identity under the expanding alphabet of LGBTQIA+ is a queer one. Instead, we utilise it as a sociopolitical stance against the exclusions mentioned above of genders and sexualities outside of cisnormative and heteronormative frameworks. We follow the arguments of other scholars and researchers engaging with and on behalf of LGBTQIA+ communities to note that understanding any of these identities in relationship to systems of exclusion requires particular contextualisation. So while we could say that an individual is a lesbian, this construct of lesbian is not universalised, just as transgender identities are far from essentialist. However, both lesbian and transgender individuals face the same systemic exclusions as not being imagined as part of normative society, thus rendering them queer. As such, we follow a line of thinking not to ascribe queerness as an identity necessarily, but as a way in which all identities within and beyond LGBTQIA+ face existence against ‘dominant ideologies’, which ‘influence the way they understand’ and ‘therefore live and practice’. [12]. Queerness for this research is not only an identity choice or non-choice, but something that becomes visible by navigating the world as an LGBTQIA+ individual, especially when choosing to be open and visible in doing so.
Visibility represents one’s ability to be recognised and exert control over how others perceive and represent them [13–15]. The notion of visibility within the queer politic suggests inherent positivity. Indeed, the ‘increas[ed] cultural representation of homosexual concerns as well as the recent queering of sex-gender identity undoubtedly has had important positive effects’ such as civil protection, the legitimisation of queer scholarship and general moments of queer empowerment [16]. However, Hennessy marks such discursive and cultural acknowledgement of queer identity as false liberation within late capitalism. Put differently, the welcoming of queer individuals into any system, whether it be businesses or healthcare, occurs because queer persons have become market consumers. They are visible as a ‘consumer subject but not social subject’ [16].
Such increased queer visibility occurs with perverse irony for various communities within the larger queer umbrella. For individuals living today with HIV/AIDS, their visibility in historical memory and current access to care fail to address the underlying stigma existing around the act of gay sex [17]. Similarly, the increased offering of transgender medicine and access to transition-related care ignores the realities that such provisions exist alongside a desire to mark these bodies as deviant, surveil them and bring them within normative notions of western gender binaries [18,19]. Both examples illustrate that the queer subject whose visibility seems new or part of a ‘phenomenon’, actually suggests increased subjugation and surveillance within normative discourse [5].
Who gets to be queer and visible depends on other lived experiences that precede and inform queerness. Lisa Duggan calls this phenomenon a ‘new homonormativity’ wherein select queer individuals find value and social acceptance despite their queer identities by attending to and often overtly embracing other privileged identities [20]. For instance, cisgender, gay, White men of relative means experience privilege because their gay identity is either secondary or overlooked. These homonormative queers engage in assimilationist queer politics to the detriment of pro-queer efforts for radical inclusion vis-à-vis groups like Log Cabin Republicans. Dean Spade argues that while many institutions have moved towards positive inclusion for transgender persons, these moves rarely attend to how such systems remain racist, classist and ableist [21].
Furthermore, these efforts often elide that transphobia is far more pervasive from legal and political standpoints than homophobia. Spade suggests that transgender individuals face ‘subjection’ rather than oppression, resulting in a person being a queer subject whose limited visibility does not protect discrimination in other ways, such as being transgender [21]. This type of queer visibility signifies queer identities as allowed, not embraced and supports the assimilation of certain White queers into neoliberal, pro-American spaces that reinstate racism, xenophobia, sexism, ableism and other non-inclusive ideologies [22].
Queer communities of colour have long explored how other identities of oppression and subjection exist alongside queerness. Audre Lorde (1984) spent her career making clear that her intersecting identities of woman and ‘Black, lesbian, warrior, poet’ influenced the visibility she possessed within society and informed how she did her ‘work’ advocating for others like her [23]. Lorde highlights the need for people to be constantly aware of how their identities become in/visible within social discourses and contends that pushes for radical inclusion must consider that marginalised identities experience visibility when other intersecting identities are not regulated or suppressed, for example, queerness as visible when it intersects with Whiteness, being cisgender and experiencing class privilege.
This condition of visibility may render queerness hypervisible. Hypervisibility, broadly defined as ‘the state of being extremely visible’ [24], has several dimensions. People with dominant intersectional identities, such as those identified in the above example, may experience hypervisibility, such as White queer academics experiencing enhanced citations to their works. Nevertheless, for those embodying forms of queerness not assimilationist in nature, hypervisibility brings negative consequences centred on marking their bodies as deviant. An example would be labelling a Black queer academic as ‘angry’ when they speak out against the disparity of citations and other forms of academic recognition between themselves and White queer academics (and White scholars more generally) at a conference. Another manifestation of hypervisibility is tokenisation, which results in queer individuals facing expectations to universalise their non-queer identities, such as race or ability to assimilate to the White or ableist logics of mainstream queerness [25,26]. An example would be a disabled queer person serving as the token minority on a diversity committee. This hypervisible tokenisation often produces adverse physical, psychological and emotional effects [27,28].
2.2. Embodied health information practices
It is well-established that queer communities experience health disparities compared with heterosexual and cisgender peers. Informational inequities partly produce these disparities. As an example, the site for this study, South Carolina, has what is called a ‘no promo homo’ law, which forbids public school health educators from discussing queer identities and issues ‘except in the context of instruction concerning sexually transmitted diseases’ [29]. This law results in a landscape where queer sexual health information constitutes either invisible or hypervisible sites of surveillance and pathologisation and can lead queer individuals like teens to make risky health decisions.
We envision information as a process, that is, the act of becoming informed or learning new information; as for knowledge, that is, one’s ability to recollect and show understanding of information; and as thing, that is, physical and digital resources such as data and documents [30]. As evidenced by their seeking, use and sharing, how one engages with information represents their information practices. Information practices provide a theoretical framework for envisioning, using and sharing as socioculturally shaped [31].
There is a particular everydayness to one’s information practices contingent on proximity to power, loosely coded as ‘culture’ within scholarship on information practices [32]. Power defines what information experts prescribe to be ‘good’, and whose information practices are ‘normal’ [33–36]. Information practices have been applied as a theoretical frame to critique deficit narratives framing those with oppressed identity intersections as lacking information that can only be provided to them by expert intermediaries like librarians. These intermediaries have training in assessing the ‘goodness’ of information, often using dominant cultural frames of value, such as information that has been peer-reviewed or undergone a formal publishing process [37].
Our deployment of information practices frames queer communities as already aware of how normative values of information exclude and marginalise their identities; these queer communities seek, use and share information despite this exclusion and marginalisation [38]. Furthermore, these practices become ‘embodied’ contingent on one’s work, lived experience and intersectional identities [39]. Elmore illustrates how Muslim women immigrants within the United Kingdom experience particular challenges in learning English. They find themselves having to alter their location, clothing and visibility relative to who else occupies the classroom with them. Their resultant information practices exemplify a uniquely embodied navigation of place, resulting in a focus on gaining and losing informational opportunities contingent on social capital tied to Islam’s cultural practices [40]. Cultural assimilation performance results in their access to information for these women, with their seemingly passive negation of Islamic culture proving quite agentic. Furthermore, when it comes to accessing information within queer communities, Floegel and Costello identify the act of world-building as a method to challenge normative presumptions of information poverty within queer populations [41].
Keilty’s work on embodied ‘pleasurable browsing’ when engaging with online pornography suggests that one’s desire for an authoritative or preferable piece of information can become complicated by their phenomenological orientation and attraction [42]. For Keilty, the failure to immediately choose a piece of pornography is not one of failure to use the content but instead a choice to engage with many options. Such embodied desires also inform one’s gender identity in that this identity and associated expressions can be embodied information. For instance, transgender and gender-nonconforming people may purposefully choose to express or hide these identities as a piece of information about themselves as a potentially protective action or as a means to obtain information in resolutely transphobic spaces [43]. Embodied information practices offer a new venue within queer theory to understand how one orients themselves to their world and their lived experience. These orientations produce understandings of bodies as valuable and authoritative sites of information. As a result, seeking, using and sharing health information becomes a queerly embodied undertaking. This article advances the connection between embodied information practices and queerness operating within a critical context – health. Furthermore, this article envisions intersectional identities as critical points of embodied information by positioning queer visibility as a critical mediator of health information practices among communities.
Informed by the literature review and theoretical framings, this article addresses the following research questions (RQs):
RQ1. How does visibility mediate the health information practices of queer communities?
RQ2. How does intersectionality complicate queer visibility?
3. Methods
This article reports on a larger research project consisting, in part, of semi-structured interviews with 30 queer community leaders in South Carolina about their own and their communities’ health information practices. South Carolina served as a critical geographical context due to the unique health disparities experienced by queer populations, including heightened economic instability, unemployment and lack of health insurance [44]. Community served as our observation unit due to the importance of community involvement in queer health information practices [45]. We assumed that leaders possess a snapshot of their communities’ more significant problems, practices and experiences while acknowledging that they are not community spokespeople [46]. We recruited adults and teens, aged 13–17 years, to acknowledge dynamic youth queer leaders [47,48]. Since some youth wished to participate without outing themselves to a parent or guardian, we obtained an Institutional Review Board (IRB) waiver of informed consent. Instead, we collected youth assent [49].
We used purposive sampling to identify visible queer organisations and affinity groups with an express interest in supporting queer persons. We asked these organisations and groups to self-nominate leaders and recruit additional participants through snowball and theoretical sampling. The latter strategy was to gather alternative perspectives and gaps in demographic representation guided by prior work, highlighting important intersectional identities for queer communities in the American South regarding health outcomes [50]. Participants existed across the spectrum of LGBTQIA+ identities. The majority of participants (60%) were White and the remaining 40% were Black and/or biracial. Participants also had various socio-economic and educational statuses, and many disclosed various disabilities – physical, intellectual, cognitive and sensory. The majority of participants were young adults (18–25 years, n = 11) and middle-aged (35–54 years, n = 7), although we interviewed participants spanning age ranges 13–17 years (n = 4) to 65+ (n = 1). We interviewed various leaders – from those one might traditionally think of, such as the head of a nationally recognised non-profit, to less traditional ones, such as a teen trying to establish the first gay–straight alliance (GSA) in his high school. We also took care to recognise various forms of leadership, from leaders, with a formal title such as the President of a queer community centre, to activists within hierarchical organisations that did not rely on titles. We asked participants to self-select pseudonyms.
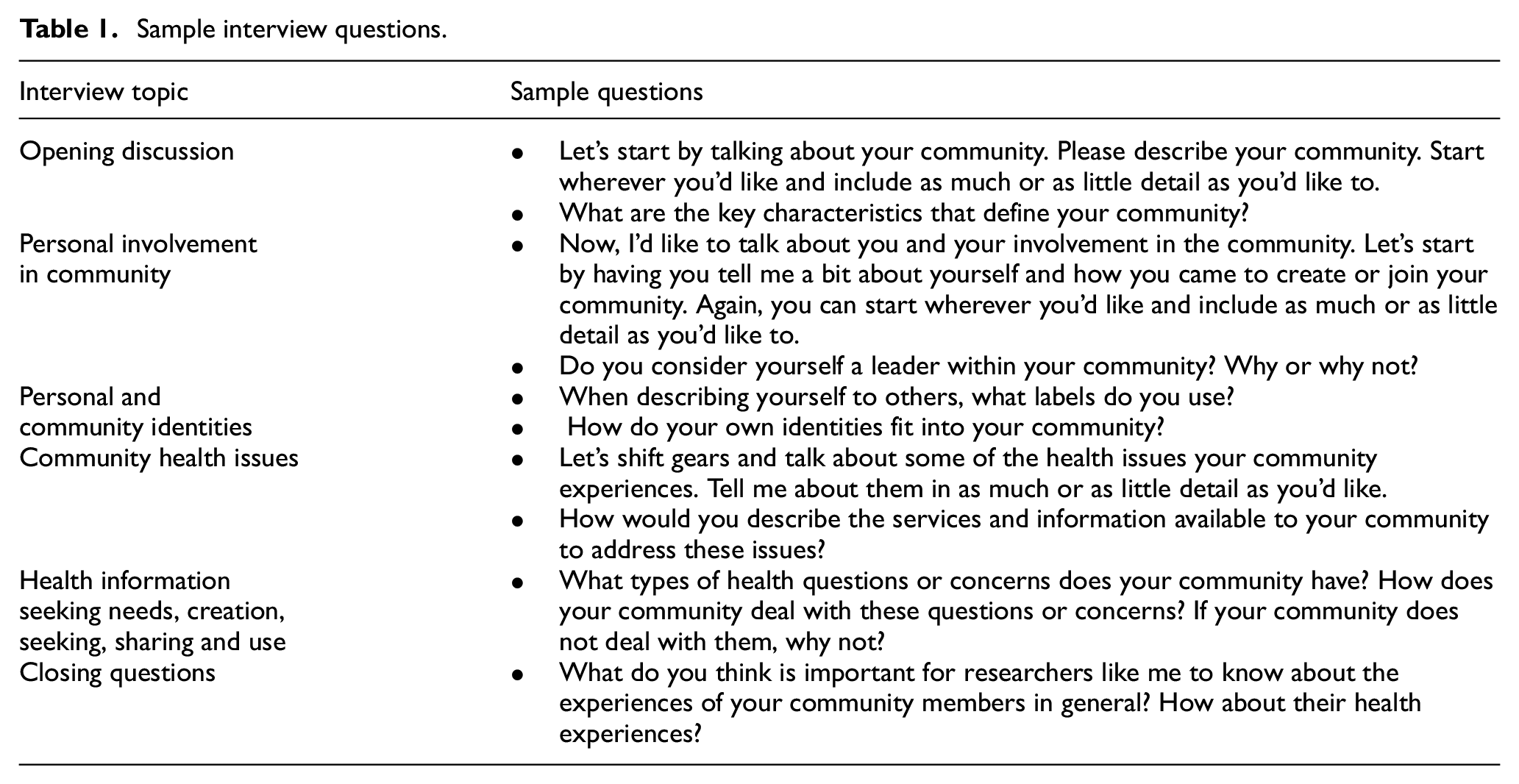
Interview topics focused on leaders’ health questions and concerns and how leaders and community members address them. Table 1 shows sample interview questions divided by key topics guiding the interview. Interviews ended with a drawing exercise, which asked participants to put their communities on a piece of paper and draw around them the people, places and things shaping how they engaged with health information. For this exercise, we gave participants a handout adapted from Greyson et al. [51] and verbally reviewed this handout, which offered participants specific prompts for what to include on their maps. The primary adaptations we made to the original handout prompts were to centre community as the unit of observation and add information creation as a suggested practice (e.g. People your community shares health advice, news and resources with, or creates health resources for, emphasis added). Critical focus on intersectional representation occurred through data collection. In practice, we achieved this focus by intentionally recruiting participants with intersecting experiences of social difference across locations such as race/ethnicity, spirituality and age [51]. Furthermore, during interviews, we incorporated interview questions that encouraged an intersectional perspective, for example, ‘What are the potential identities your community members have in common?’, and probes, for example, ‘What identities do you think were most important in shaping your community’s experience?’, guided by methodological literature on incorporating intersectionality into research design [52].
Sample interview questions.
This article focuses on interview transcript analysis, using the drawing exercise as an elicitation device. We analysed transcripts using a qualitative coding approach consisting of two stages. First, we used line-by-line open coding (specifically initial, process and in vivo codes) to develop a ‘microanalysis’ of the data followed by axial and focused coding to further reduce and recode, allowing core coding categories and their properties to emerge [53,54]. We paid particular attention to significant themes informed by the intersection of social identities, locations and experiences identified by participants. Throughout this process, we engaged in the constant comparative method, which involved comparing incidents (e.g. how different participants discussed their communities’ health information seeking), coding categories and other conceptual and theoretical frameworks in the same area of study [55]. We engaged in analytic memoing during this process to explore the deeper and more complex meanings behind emergent coding categories [54]. Keeping in mind that the analysis we are focusing on here is part of a broader codebook, the existing frameworks relevant to this work are the tripartite modalities of visibility, invisibility and hypervisibility [13–15,24]; queer assimilation [16,20,22]; and intersectionality [9,23].
We used member-checking and peer-debriefing to strengthen the finding’s trustworthiness [56]. For member-checking, we sent participants their interview transcript, a two-page executive summary, and a draft of a related, broader conceptual paper for their optional review and commentary of how well the findings reflected their lived experiences. Some participants did not follow up, others followed up but not substantively (e.g. saying ‘I have no objections to publication’), and a few shared more substantive comments and concerns. For example, Jake Hartwell emphasised that selecting aspects of his identity as shaping how he experiences visibility overly simplified these experiences. His critique highlights a vital clarification to make about the purpose of an intersectional framework: it does not purport to be a totalising theory of identity but instead seeks to understand how critical identity intersections determine one’s structural position [57]. For peer-debriefing, we relied on research mentors to provide feedback on our methodological choices and research study design, advisory board members to comment on how well our data collection instruments aligned with our research questions and colleagues to talk through emergent findings.
4. Findings and discussion
Three key constructs emerged from data analysis: visibility, invisibility and hypervisibility. We discuss each construct below, informed by participant narratives. Our reporting style deviates from what is typically the case for this type of qualitative analysis through its atomistic focus on certain participants. Through this choice, we hope to recognise the tension between wanting to both acknowledge a collective understanding of queer visibility vis-a-vis intersecting power dynamics informed by structural identities while also honouring participant feedback like Jake Hartwell’s, which remind us that such visibility is always an individualised experience. We also acknowledge the messiness and contested nature concerning the terms individual and community regarding queer populations. Our referencing of the use of community follows the deployed idea of a collective community as offered by participants. Furthermore, this interoperating use of individual and community echoes the complex relations latent within groupings constructed and contested at the site of both sexuality and gender [58]. We refer to participants using their chosen pseudonyms, pronouns and salient identities used to describe themselves.
4.1. Queerness as visible identity
One important observation to start this section is that our participants necessarily had a different relationship with visibility than queer people who were not considered leaders. Specifically, participants addressed the need to make themselves visible as leaders for three key reasons. First, so that other queer people could locate them and their communities, for instance, Princess Mocha (mixed race, genderfluid person) notes that queer people in her area could ‘be in the closet, hurting, and need us [her and her organization]’. Because she could ‘be the one person that they need’, she and her organisation ‘have to make ourselves visible’. Another reason for participants to be visible is to engender queer recognition in others. Charlie Burt (White, middle-aged, cisgender, lesbian) describes how the best part of her community is ‘the feeling that comes ... when we’re doing something visible and then there’s that queer kid in the audience that looks and you can kind of see the gears turning, that the world is changing for the good for that person’.
A final reason to be visible is to advocate for queer people. Johann (White, cisgender, older gay male) states that because they and their community ‘refuse to remain silent, that that is why things’, such as less visible protesting and vitriol at Pride events, ‘are changing’.
Moreover, in some instances, participants took their commitment to being visibly queer into their engagement with our research, deliberately choosing to retain their real name in place of our suggestions that they choose a fake name, with some suggesting that they had nothing to hide and others noting that being open about their identity as part of their job as leaders. Yet this visibility was not totalising as participants may not have their queerness rendered visible in contexts where they were not recognised as leaders. For instance, Pat (Black, Afro-Caribbean, transfeminine, gender nonconforming person, of college-age) notes that despite being a visible advocate within her community, ‘I don’t think that I’m necessarily looked at as a leader’ within the broader ‘leadership class’. This class is composed of ‘organisations who receive the bulk share of the financial and material resources that are available and also recognition by other established leaders in the community’. What is left unsaid in Pat’s account is that her invisibility is probably produced by the hypervisibility appended to the specific queer organisations that adopted assimilationist identities and principles. We now turn to such assimilation as we address how queerness can attain normative visibility via such assimilation.
As argued above, hetero-cisnormativity within late capitalism renders queerness, at best, only partially visible as a consumer identity [59]. For participants with other privileged identity intersections, queerness operated as a consumer identity that designated what health information and issues were essential to the community and what health practices were considered safe or responsible within this community context. In other instances, participants for whom queerness could be a ‘normal’ part of one’s lived experience exerted control over how their health was perceived and represented by marking their health questions and concerns as non-queer.
One way that leaders achieved such normative visibility was through the adoption of certain health narratives. For instance, the visibility of HIV/AIDS narratives informed narratives of participants who were White, cisgender, gay men. Such narratives echoed the increasingly consumerist politics of HIV/AIDS advocacy and prevention, marking it as an almost monolithic and uncontestable concern through reinforcing queer bodily value as biopolitical [60,61]. Tony Solano (White, cisgender gay male in college) describes how he and other community leaders orient their members towards HIV/AIDS and sexually transmitted diseases (STDs): ‘we would bring everybody together and would make a quick campfire about HIV and other STDs ... [to address] how to prevent them, stay healthy, how to recognize them, and most importantly, to be open with your sexual partner’. He expresses personal frustrations when younger members of his community resist this orientation: ‘young individuals ... are not doing that [getting tested] as much. It’s more a free for all’.
Because Tony Solano is a leader in his community, he plays a vital role in determining what health issues are important among community members and how they should approach them. Not centred in Tony Solano’s discussion of this role is his visibility as a normative queer person – a gay, cisgender, White man whose public perception is relatively accepted. While he can be open with his queer identity, expecting others to do the same overlooks crucial intersections of social difference that might not afford others the same visibility. The young people Tony Solano frames as incapable of controlling their health may instead prioritise and seek different health information.
Other participants sought mainstream visibility by subsuming their queer identities under other privileged ones to frame the health issues their communities faced as ‘normal’. Take Charles (White, cisgender, gay man in the age group of 50s–60s), who identifies as an ‘ordinary guy who does ordinary things’. He centres his community’s health questions and concerns around exercise and diet, expressing frustration with other community members that eat food full of ‘salt and sugar’ at potlucks.
Both Charles and Tony Solano engage in embodied information practices that render their queer identities visible and normalised. For Tony Solano, this means that he seeks out and prioritises HIV/AIDS research and presumes a potential universality to that need, one which he presumes to be a shared and equally embodied information need across all queer-identifying persons. Alternatively, Charles’ queerness is so normalised that it often exists as a reality of his identity, which is normal and arguably irrelevant to other queer-centric concerns. Crucially, for both of these participants, their queerness remains a visible identity because neither experiences an attempt to deliberately leverage it in relationship to other salient identities, making it visible, as opposed to invisible.
4.2. Queerness as invisible identity
Other participants belonged to communities where their queer and/or intersectional identities were at odds with normative discourses, rendering their queerness invisible. This invisibility operated in two interrelated ways – first, as invisible through oppressive erasure, and second, as agentic, allowing communities to prioritise healthcare needs pertinent to other intersecting identities.
Annalisa (a White, cisgender, queer woman in her 20s) addresses difficulties locating a community of queer persons who are survivors of intimate partner violence (IPV) due to these identities being erased. Noting the cishetoronormative presumption around IPV, Annalisa states: I’m a domestic violence survivor. And once that ended, I wanted to try to get a face to LGBT people who are facing this issue because most people don’t. And especially in the South it’s man-woman, man-woman. So, if you actually try to get any legal help, it really doesn’t work. So, I volunteered with – this more of a worldwide organization to break the silence against domestic violence, trying to get more of a face for the LGBT community there. With my own business, I donate to [ORGANIZATION] and any other domestic violence organization that I can find around. There’s not a lot of groups in [CITY] that I found for people. So still kind of searching for that.
Annalisa’s identities as queer and a survivor are rendered invisible by heteronormative and cisnormative rhetoric. Such invisibility echoes Kai Cheng Thom’s concern that for queer individuals, movements around justice for sexual harassment often ignore femme individuals who are not straight, White, cisgender women [62]. However, Annalisa recognises and embodies her invisible queerness to become an information resource for other queer people facing IPV. Specifically, she challenges the representational issues of IPV by informing others that queer, femme-presenting persons can be IPV survivors. Speaking on behalf of others like her, she notes that validating her queer identity at the intersection of IPV survivor requires extended queer labour that challenges recalcitrant heteronormative framings of IPV as occurring between specific types of queer persons.
One’s queerness could also be made invisible due to more dominant queer identities within a space. Tony (Black, transgender, heterosexual man in his 30s to 50s) illustrates this form of invisibility when recounting his engagement with queer spaces, specifically a lesbian bar; a space he used to engage in comfortably before coming out as a trans man: At least from my perspective, identifying as a trans male, it was more so the fact that I was no longer in a community, right? So, I would still frequent the same bars, the same places, and then it kind of became, ‘Why is that guy at a lesbian bar?’ It’s like, ‘Oh, you don’t know who that is?’ And then introduction to my new community of being trans. And then it was like, ‘Oh’. But I still wasn’t kind of – well, I got booted. I got the boot from that community.
Tony’s narrative illustrates how he became subject to particular animosity among bar patrons because others read him as a man entering into a space meant for women only. What is invisible here is Tony’s trans identity. While others rightly read him as a man, the presumption among bar patrons is that he possesses no inherent queerness. Since Tony’s masculinity is made visible, it occurs at the expense of his sexuality being made invisible. This invisibility complicates and contests clear lines of sexual orientation as one’s sex-assigned-at-birth has historically informed them. Specifically, Tony identifies with a sexuality attracted to the women he meets in lesbian bars. This identification runs into an iteratively new moment of queer phenomenological disorientation, as Tony is a body read by bar patrons as potentially unwelcome, or what Gayle Salamon calls a body that is both a ‘danger’ and in ‘danger’ as it unsettles cisnormative assumptions around gender and sexuality [63]. This paranoia among bar patrons does not suggest that they are trans-exclusionary or necessarily transphobic; instead, due to their historical relationship with violence enacted by cisgender men, Tony’s body is one warranting questioning.
Tony’s experiences with having his gender identity as a trans man attracted to women regulated how he provides information to others in his role as a queer community leader. Tony aims to include people with contested identities by asking questions about why and how they should be allowed into queer spaces to engage in health information work: If there’s something you – if there’s a reason a community doesn’t want you in, I want to know, one, why were you in the community to begin with? Do you still have that passion, that drives, that resource, that whatever? That everyone thought you were cool, and realized, wait, you’re not. Do you still have that part? Do you want to stay part of the community? Do you still want to help? Do you still want people to come to you to get whatever they need? If you’re as done with the community as community is with you, then cool. It’s a win-win. Bye. But if you still have that push, that drive, I’m not going to just dismiss you.
Like Annalisa, Tony’s once invisible queerness now impacts how his health information work, mainly how he determines whom he lets into his community. He avoids presumptions of universal negativity when making these assessments, as evidenced by his litany of questions around outsider involvement. Instead, Tony prioritises outsiders’ intention and passion for helping a queer community over their seeming threat based on perception alone. Although Tony does not outright say this, we can imagine that he, too, sought a willingness to dialogue and understand why he ‘got booted’ from a lesbian space after coming out as a trans man.
While participants like Annalisa and Tony agentically embraced their queer invisibility when others forcefully erased these identities, other participants actively lowered their queer identities’ salience to allow for other identities to emerge. Chloe (Black, cisgender, bisexual woman in her 20s–30s) describes how her community’s queerness takes a secondary role to their Blackness when it comes to using medical professionals as a health resource: In terms of being in the black community, what I have found is that there is, from my perception, a fear of doctors. And that’s a discussion that has – that’s a discussion that is constantly happening. It’s something that I even talk about with my colleagues who identify as Black. That naturally because of historical things, black people do not like going to the doctor. Which then presents another interesting aspect when I talk to Black or POC that identify as LGBT that don’t want to necessarily seek out resources from doctors just for fear of stigma or fear of how they’ll be treated.
Chloe and her community’s identity as Black inform their practice of health information avoidance. Such avoidance responds to ‘historical’ practices by medical practitioners that marked Black bodies as subject to exploitation [64]. This observation is not to say that Chloe’s queerness is outright invisible, but it makes more sense to prioritise needs based on racial identity for her and her community. While this move does not produce queer invisibility outright, it agentically aims to deprioritise it through increased visibility of a different shared identity. Chloe notes that she and her community members are not ignorant or indifferent to their queer identities, only that they have experienced healthcare discrimination primarily contingent on race, suggesting, if anything, that health systems produce queer invisibility for herself and others.
Participants may also assign other privileged identities more salience to bring visibility to their health questions and concerns tactically. For example, Allison (White, transgender, heterosexual White woman in her 50s–60s) notes how her transness subjects her to health care professionals who offer specific metrics for her transition process, such as how well she aligns with a male/female binary [65]. These professionals work to fit her transness into transnormative discourses, wherein Allison’s identity must match a visible and popular notion of how transitioning should look. Allison embodies her privileged identities at the intersection of age, specifically related to her trans experiences, to push back against these normative discourses when discussing her assessment of medical professionals as trustworthy: I know what I think makes me trustworthy. But when you go to judge somebody else, if they’re trustworthy, that’s an extremely individual basis. As I look at your face, do I see anything in your looks that are telling me you’re evil or that I’m evil to you? How do you sound? What’s your reflection? When you start quoting me stuff, do I think you’re giving me BS, or do I think you’re giving me knowledge? And there’s a lot of people that know the terms and the keywords, but they do not understand the underlying structure or information. And so when you ask questions, you need to dig beyond the surface to see what they’re saying ... Because a lot of people can’t answer those questions if they’re not really involved. Like I say, they’ve learned the keywords.
This quote from Allison speaks of how she navigates her visibility as a trans woman and clarifies that she has embodied her queer visibility as an information practice. She understands that others see her as a source of embodied information because she has identified as trans for a long time (openly or otherwise), but equally attends to avoiding sharing about this identity when it might prove detrimental to her community of potentially queer students. She uses a history of mistrust and potential threat around her visibility to question cautiously medical professionals tasked with advising her transition in an adjacent manner. Her Whiteness also affords her the ability to contest medical professionals. Unlike Chloe or Pat (whom we will discuss shortly), Allison can prioritise her concerns related to her queer identity while simultaneously avoiding concerns that her race might result in her being tokenised, exploited or ignored.
In some instances, participants choose to render their queer identities invisible as part of a risk/benefit analysis related to identity disclosure. Sarah (White, cisgender, pansexual woman in high school) notes that she ‘knows a lot of considerably popular people who tell the people they are straight because most of the popular people are very against any type of gay thing or anything like that. So, they have to keep it a secret’.
For Sarah and her community of other queer high schoolers, the potential social stigma of not aligning with heteronormativity outweighs any benefits of being out. This account complicates the seemingly universal understanding of queer visibility as honesty and safety as seen by other queer leaders with privileged identity intersections like Tony Solano. Keeping their queer identities a secret, Sarah and her community are not being dishonest or unsafe, but instead deciding on their terms that such visibility would bring about more harm than it would benefit.
4.3. Queerness as hypervisible identity
Like queer invisibility, hypervisibility operates simultaneously within both frames of oppression and as a point of agentic choice. Moreover, both frames reflect societal pressures that mark marginalised persons as different and in need of correction [24].
Participant narratives denote how queerness intersects with other historically exploitable identities to produce bodies that are hypervisible sites of exacerbated oppression. Pat illustrates such oppression when noting how her community must trade economic and embodied informational exploitation to access health resources: Our health information and data is profitable, point blank, period. But health information is profitable in a particular kind of way that I think it’s really important to be cognizant of, and people devise really interesting ways to get health information from you. I think one of the – a really subtle way that I don’t think people really realize that they’re providing health information is those DNA tests that people have been-that have gained popularity, especially among African-Americans who don’t really have access to genealogical information ... also I mentioned during our interview, I talked about pharmaceutical companies and how pharmaceutical companies are also really big into getting you to sign up for clinical trials or just trying to sell you drugs.
Like Chloe, Pat expresses a well-justified hesitation concerning established medical institutions, which she observes have a significant interest in gaining capital – monetary, medical, discursive and so on – from the bodies of persons of colour. She notes how queer bodies of colour become hypervisible sites of the communities’ collective paranoia around HIV/AIDS and STDs, suggesting that the aforementioned pharmaceutical companies prey upon her and her community as sites to profit upon for drug treatments. Specifically, Pat notes how the prevalence of health care professionals, often uninvited, in trans of colour spaces, illustrating the mainstream desire to see trans bodies of colour as sexually promiscuous.
Pat further explains how her community must play into this hypervisibility themselves as ‘carriers’ to gain access to health information and services: So, accessing proper healthcare – a lot of us also – some of us are able to access healthcare if we’re positive. So, if we are positive, we can go to places like the immunology center and we’re able to get on like treatment regimens, and other federally funded programs are able to get us dental care and healthcare. Things like that. There are some people who are referred to as bug chasers, who try to become positive in order to access those things as well.
Through this account, Pat demonstrates how some of her community members attempt to test positive through bug chasing to access health information and resources. Such bug chasing represents an agentic attempt among community members to be healthy, even if the practice exists outside traditional notions of efficacious health behaviours. While bug chasing may not be a desirable practice, Pat notes its legitimacy among community members who perceive it as one of the few outlets for access available to them.
Pat’s narrative echoes Chloe’s around how bodies of colour, particularly Black bodies, are sites of historical exploitation among the medical sciences. Pat’s narrative evokes ideas similar to Somerville’s argument that queer Black bodies often exist as sites of the sexually perverse, which works to ‘naturalize and legitimize a cultural myth’ that they are to blame for sexual transgression in this case, HIV/AIDS [7]. Her community’s desire to become hypervisible is a double-edged sword, one that gives them health care with the caveat that they play into a historical trope of being paraphilic. Pat’s narrative reminds us that the choice to avoid visibility can be a strategic act. For her and her community, marginality is not necessarily negative. Her choice and the choice of the individuals she works with to avoid visibility works to avoid tokenisation and exploitation within racist and anti-queer medical spaces whose research relies on models driven by profits instead of ethics.
Queer communities also wielded hypervisibility to engage in direct, embodied informational activism. Kim Williams (White, cisgender, pansexual woman, in her 30s–50s) exemplifies this activism when discussing how her organisation exists for queer people who have hit their breaking point: I’ll walk you to the hospital. I’ll sit with you until they take you back. I will do whatever it takes to get it done. But I think everybody’s trying to reach out more. I don’t really know. The people that I deal with, would [local LGBTQ+ organization] help them? No. Okay? They are in trouble. I always say, ‘Mocha [Kim’s organizational co-founder] and Kim get the broken’. Okay. And then we kind of tape them up and duct-tape them and get them back to where they can go.
Kim Williams exists on the periphery of queer activism within SC and stands out as visible in her willingness to help when others will not. Both Kim and her co-organiser Mocha mark this latter work as diverging from other queer activist organisations, which avoid hypervisibility to align with respectability politics. Consider the comparison of her organisation with another that she feels operates under the radar: We just have to educate more, and I need to make it more visual. I know the [ORGANIZATION], that we are not of the same blood. They like that stealth shit. I don’t like that stealth. I think that does us a disservice. We need to be out and proud. Maybe not as loud as we used to be. However, we do need to stand up and defend.
As Kim Williams notes, such hypervisibility has caused her organisation some trouble, including being kicked out of the library where we interviewed her and her co-founder for this project. During this interview, Kim Williams suggested that part of what makes her organisation have to be hypervisible relates to economic mobility. Speaking to us as researchers, she suggested that we were able to engage in queer-related research due to our grant funding; similarly, many of the queer organisations she was rightly critical of could afford to be patient and ‘stealthy’ due to their consistent funding streams. Kim Williams contests such stealth by asserting that if her organisation was to have such funding, and if they would invest their resources into becoming visibly inclusive: I want a big kitchen with a huge table like this for [crosstalk]. And we can put everybody and all the food on the table. That’s what we want. We want a home. We want a rainbow home. We want to get grants and funding, and we want to get something like [notable SC community leader] has, because it’s so beautiful.
Because her community lacks similar resources, Kim Williams envisions her activism via queer hypervisibility as fundamentally necessary. The queer people she is trying to reach are often at their most dire, whether facing economic hardship or thoughts of suicide; she notes that patience is not an option. Even if it comes with marked disdain directed at her and her organisation from others, her hypervisibility proves justifiable if it promises support to those whose needs are invisible in other communities engaging in queer assimilation.
Both Pat and Kim Willams’ navigations of queer hypervisibility are at odds with systemic rhetoric concerning queer exclusion and inclusion. Kim Williams becomes hypervisible to push back against homonormative assimilation ideas that exclude marginal intersectional identities such as class and mental health [20]. Pat questions hypervisible practices by community members. She views these practices as relevant in accessing healthcare and falling short of uprooting systemically racist practices producing these disparities in the first place [21].
5. Implications
Though each type of queer visibility produced within various intersectional identities proves iteratively different, some notable findings emerge that invite considerations worth further exploration in future research. While our implications are primarily for the health care profession and how they perceive queer communities monolithically, the extensions of these discussions certainly impact the work and identity salience of queer community leaders. Implications also add to an expanding scholarship around the role of access with relationship to queer information seeking and needs [66–68]. First, queer visibility informs embodied information practices and information access, focusing explicitly on health information. This particular concern for how access is negotiated within healthcare has precedence within information science research. For example, scholars like Senteio & Veinot explore how low-income communities of colour navigate resource barriers and adhere to health needs despite institutional failure [69]. However, theoretical linkages to queer visibility have been underexplored in the literature and are critical to understanding as it provides new ways to understand the unique, individual-level ways that queer visibility manifests in relation to information access.
Second, queer visibility is temporally contextual. How one embodies their queerness as an information practice changes over time and is relative to the saliences other identities afford a person. Therefore, queerness is not a fixed, stable identity frozen in time but instead constantly shifting based on these saliences. Such a consideration is hardly new, yet it does provide further affirmation of how temporality requires one to extend their utilisation of intersectionality as a theoretical framework. As Jasbir Puar rightly observes, ‘intersectionality demands the knowing, naming, and thus stabilizing of identity across space and time, generating narratives of progress that deny the fictive and performative of identification’ [22]. In other words, despite how generative intersectionality may be as a framework, it can be used to frame queerness as a fixed, demographic category instead of a messy, fluid positionality. Such neoliberalist framing leads to universalising identity as a constellation of similar experiences that follow a linear narrative. Such universalisation ultimately overlooks particular systems of oppression privileging some liberal queer members of LGBTQIA+ communities. Another related consequence is that simplifying an intersectional analysis may consist of naming identities and considering them separately to ultimately see how they influence each other, turning this analytical project into one that positions intersectionality as additive. Such positioning is antithetical to the aims of intersectionality, which are to view such identities as inextricable. The revaluation of one’s intersectional identity as a framework aligns with critical information studies of scholars whose work challenges the fixation on identity-specific categorisations of information practices void of nuanced discussions of how identity salience alters relative to a given set of spatiotemporal contexts. The scholarship includes meaningful discussions around race [70], ability [71] and nationality [72], among other identities.
Related findings denote that intersectional systemic oppressions mask politics of assimilation and essentialism. Perhaps unsurprisingly, the seductive nature of queer assimilation leads to troubling conflations among queer communities of a universalised queer experience. These conflations can lead to the negation of how other systemic inequalities like racism perpetuate in healthcare systems. Alternatively, queerness can also become a misguided move for embodied essentialism, such as assuming that younger members of a queer community do not take care of their health due to their age. These findings contribute to prior research by offering important links between theoretical issues within queer community making and the use of health-related infrastructures both individually and collectively. In particular, it echoes Chatman’s groundbreaking work on the importance of secrecy as an agentic information practice [73]. It also offers additional insight into Ruha Benjamin’s concerns of racialised hyper surveillance in a continually mediated information landscape, here with a heightened focus on the intersection of queerness [74].
Findings also have practice-based implications for health professionals and queer community leaders. The first is to recognise and leverage queer silence as informative to professional praxis. As findings and prior research demonstrate, visibility is not necessarily always desired by queer communities [75]. Furthermore, forms of invisibility and hypervisibility may prove agentic in advancing shared goals. Consider Allison, who directly confronts silences within her health information–seeking practices by embodying a critical lens of authority within medical professionals. Knowing that she faces severe repercussions on a personal level if she is to out herself to her students means she also questions the presumed neutrality and intent of medical professionals who might find themselves bound by similar institutional silences. Such connections between Allison’s health information needs and more prominent trans-antagonistic social ideologies suggest that there may be a desire to access information by queer communities. However, one’s choice not to obtain readily available information might occur out of retaining safeties possible through remaining invisible. In turn, information professionals, and health professionals, in particular, can take this increased inquisitive nature as an attempt to signal a desire for sharing in queer knowledge even if such sharing must happen discretely on their part. In response, information professionals can attend to what they perceive to be an increased inquisitive nature for queer populations they encounter and offer information, even if discreetly, about many potential queer information needs. Alternatively, the reality that a person may not share their queer identity does not mean that they might not benefit from receiving health information relevant to queer communities. As Allison, Sarah and, to a certain extent, Pat’s examples show us that there are queer youth who desire access to and need health-related information even if they are not openly discussing such desires, meaning that methods for making this available in abundance are worth consideration. Inquisitive visible queer youth might be seeking information, directly and indirectly, related to health needs not only for themselves but also for their friends and community. Thus, imagining ways to facilitate access becomes vital. When possible, health care professionals could provide queer-oriented healthcare resources within and in proximity to school settings to attend to such deliberate silence.
Furthermore, community leaders and healthcare professionals should recognise that silence does not necessarily reflect ignorance. For instance, we challenge presumptions like Tony Solano’s that younger queer folks do not care about their health because they do not speak about HIV/AIDS prevention issues. Presuming silence as an act of ignorance belittles the actualities of many queer youths. Instead, their silence is probably in response to social spaces in which their outness is detrimental or disallowed. Here, queer community leaders might explore policy changes in which schools shift practices to support queer students in verbally expressing concerns around their health information needs. Moreover, such a reorientation would afford space to consider why a group, such as the queer communities of colour, choose not to seek out explicitly queer health information. Here, such a choice is not one of being ignorantly silent but instead choosing to direct one’s voice to a more silent community-based need.
Finally, community leaders and healthcare professionals must recognise how queer hypervisibility often produces necessary and agentic embodied information practices. For Pat, the embodied information practices of simultaneously questioning healthcare’s hypersurveillance of her body as a queer body of colour and her engagement within bug chasing provide an intersecting and literalised use of the body to gain information. She notes that she and her community avoid many healthcare spaces because of costs associated with this work, thus producing information avoidance within a situation wherein health information presumes necessary medical, institutional authority. Despite its dangers and presumed negativity, bug chasing provides a way to access healthcare cheaply and for Pat’s community, effectively causing it to be a physically driven means of information access. In turn, healthcare professionals working within HIV/AIDS prevention could better serve communities of colour seeking basic healthcare and see preventive services as fulfilling those needs by allowing the use of preventive care with or without testing positive for a given sexually transmitted infection (STI)/STD. Such a reconsideration of resource access allows queer-focused healthcare to remain intersectional by noting that sexual activities and HIV/AIDS are hardly the only concern of queer communities and remain even less so when placed with other embodied identities.
6. Limitations
While our shared positions as queer researchers potentially aided in recruiting queer diversity or presences as White academics potentially hindered interest in participation across diverse identities. Similarly, while our recruitment efforts aimed to include non-academic spaces such as queer affinity groups and LGBTQIA+ community centres, our reliance on snowball sampling meant that many participants had previous ties to our academic institution or previous involvement with our institution. Beyond this, our questions and focus of research prioritised health information practices related to the participants’ potential queer identities. While we aimed to be as intersectional as possible in our focus, this particular identity emphasised that many of the points raised around race and class grew from participant concerns. In turn, future questioning can be more deliberate to allow participants to emphasise how other potentially salient identities factor into their health information practices. Finally, while our questions framed health practices broadly, many participants sought clarification about whether or not mental health issues fell under our lines of inquiry. Such moments of clarification on the part of our participants suggest that while we value the importance of including mental health issues in our analysis, we ought to be more deliberate in future research to evoke mental health concerns in our discussions directly.
7. Conclusion
Although it is a small geographically specific representation of queer community health practices, our research shows that one’s queer identity produces both barriers and unique points of access regarding how queer communities engage with information. However, when it comes to one’s relationship with medical institutions, queerness is often a relative identity that makes one’s use of and production of health information practices contextually embodied. When it comes to healthcare and the systems producing a thing called health information, discourses of health and those practicing those discourses often choose to see queerness as a priority of embodiment in some. On the contrary, it is a secondary and irrelevant point of identity in others. These embodiments produce unique orientations towards and against health information across one’s lived experience, wherein things like race, age and class produce tiered visibilities of one’s queerness. As we have shown, each version of one’s queerness and its visibility relative to other lived identities produced unique embodied information practices that marked one’s need to be seen or not seen as highly nuanced and anything but universal. Our article ultimately illuminates that when we discuss queer visibility and its relationship to healthcare, we must also discuss other identities and embodiments that always exist alongside queerness, whether it be race, ability or class. As such, our participants make it clear that no work done to increase the visibility of concern for queer health can exist without also attending to how healthcare has produced multiple points of marginality across other systems of oppression. Ultimately, our work shows that when it comes to prioritising the healthcare needs of queer persons across intersectional identities, focusing on the most visible and vocal or the most invisible and quiet is hardly enough. Within each instance of visibility, there exists a purposeful and potential silence. In the moments of invisibility, there also exists a voice full of agentic and focused amplification.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by grant funding from the Institute of Museums and Library Services as part of an Early Career Development Grant. The grant number is RE-07-18-0066-18.