
Abstract
After having earned international accolades for its pro-people policies in the 1980s, especially in the provision of health and education services, the Zimbabwean government then presided over the progressive decay and near collapse of the very same sectors, despite continuously presenting itself as a people’s government. This article investigates the factors accounting for this decline and its impact on the Zimbabwean society.
Introduction
A number of studies have commented on the contradiction arising from the fact that some postcolonial governments established by former liberation movements in Southern Africa have proved to be undemocratic in their policies and practices and have emulated the very repressive colonial governments that they had fought so hard to overthrow. It is as if in the process of fighting colonial rule, liberation movements internalized some of the negative characteristics of the very same system that they opposed. Thus, with regard to governance, it appears these liberation movements brought about political independence without democracy (Melber, 2003a, pp. 9–24; 2003b; 2008, pp. 378–381; Gumede, 2009). Neither have the governments they established fulfilled the promises these movements made during the struggle for liberation, which continue to be repeated in the current rhetoric about empowerment of the people. 1 Indeed, most of the people remain mired in poverty, live in sub-standard accommodations, are unable to access basic social services and continue to eke out a living as they have always done despite the fact that these liberation struggles were waged in their name and it was their sacrifices that sustained the struggle against colonialism. In fact in all these societies the gap between the rich and poor has widened rather than narrowed, as is evidenced by the stark contrast between the imposing expensive mansions of the old and new elites in the suburbs with their manicured lawns and swimming pools, and the squalid squatter camps and miserable matchbox-style housing in the townships, some of which were actually built after independence in the various Southern African capitals.
Yet, for a brief moment, Zimbabwe seemed to be on the right course that was likely to set an example for the rest of Africa of how to devise and implement effective people-friendly policies that would improve the quality of life for the majority and justify the people’s suffering during the many years of anti-colonial struggle. Indeed, the 1980s in Zimbabwe seemed to signify the birth of an era of general prosperity and a more equitable socio-economic dispensation as the new leaders systematically dismantled the racist social and political structures inherited from colonialism, proclaimed the Growth with Equity development strategy, and publicly promised “education and housing for all by year 2000.” They spoke a language of socialist transformation that resonated very well with the majority of the Zimbabwean people. Indeed, for most of the 1980s, Zimbabwe made impressive achievements in the provision of essential social services such as health care and education and the country served as an example of how to balance development with a commitment to advancing the well-being of the majority.
Remarkable progress was recorded in the first 10 years after independence in the provision of schools, hospitals and clinics, the training of teachers and other professionals, the expansion of university education, the development of an innovative education-with-production program, the reduction of child and maternal mortality rates, an increase in life expectancy, and the development of a highly effective primary health care system. Hence, in recognition of Zimbabwe’s achievements in education, UNICEF commented in 1987 how: “Zimbabwe has demonstrated that, with strong political commitment and the involvement of the community, it is possible for a developing country to make basic education available to the great majority of its children” (UNICEF, 1994, p. 58). And for its part, UNESCO highly praised Zimbabwe’s educational system in the following terms:
The progress of the [recent] past… demonstrates that Zimbabwe’s system of education, which has been described as revolutionary and ambitious, is not just a short lived and predictable result of the independence euphoria, but truly a system built on modern and enlightened principles of education that take into account the country’s particular circumstances, opportunities and constraints. (UNESCO, 1987, p. 4)
In 1992, the World Health Organization (WHO) praised the country’s achievements in primary healthcare provision, declining child and maternal mortality and other health services, as follows:
Zimbabwe’s achievements in health during the 1980s have been truly impressive. The percentage of children fully immunized has nearly tripled from 25% in 1980 to 67% (in 1992) and the proportion of married women of childbearing age using modern contraceptive methods has risen from 14% to 36% during the same period. Life expectancy has increased from 55 to 59 years, while infant mortality has declined from 82 to 72 per 1000 births and maternal mortality has fallen to 90 per 100 000 deliveries. All of these current indicators are significantly better than the averages for Sub-Saharan Africa. (World Bank, 1992, p. x)
Undoubtedly, during the first decade after independence, Zimbabwe made notable strides towards creating a better life for its people and seemed to have laid a solid foundation for the country’s future prosperity and the people’s welfare.
Yet, less than two decades later, the picture had totally changed, as the country’s social services deteriorated rapidly and the government quickly lost both its capacity and its political will to promote the interests of the Zimbabwean people. In fact, the reversals in the earlier achievements were so far reaching that the quality of life of the majority of the population became worse than at any time in the colonial period as the country’s economy experienced a virtual meltdown and national politics mimicked and often surpassed the oppressive colonial system that the liberation struggle fought so hard to eliminate.
By 2009, the Zimbabwean education system was being described as a “national disaster” (Physicians for Human Rights, 2009, p. 5), and a December 2008 report by UNICEF revealed that
[s]chools and hospitals are closing, patients cannot access health care, teachers, nurses and doctors are not able to come to work. Urban water supplies are erratic, or not available at all due to weakened infrastructure, power outages and shortage of chemicals. The net effect on Zimbabwean children has been no schooling, lack of health care, no safe drinking water, reduced number of meals and increased morbidity and mortality (UNICEF, 2008a, p. 2).
Other reports on the country’s once-impressive social services were equally alarming (Medicins san Frontieres, 2009). Clearly, the promised better life for all had failed to materialize. Meanwhile, the political intolerance of the ruling ZANU-PF party had reached monumental heights characterized by the torture, assault, detention and/or general harassment of members of the political opposition.
Why did it all go so wrong for Zimbabwe? How did the prospect of attaining education and health for all by 2000 turn into a nightmare of hospitals without doctors or medicines and schools without books or teachers? How did the sparkling promise of Zimbabwe’s independence in 1980 turn into the nightmare of 2000 and beyond? This article seeks to address these questions by focusing on the history of education and health services delivery in Zimbabwe between 1980 and 2009, with the focus on determining how the hopes of 1980s turned into bitter despair by 2008 and how the early achievements of Zimbabwe’s educational and health policies eventually were followed by a devastating brain drain and a health crisis characterized by a cholera epidemic of startling proportions that killed thousands of people. It will be argued that the tragic collapse of Zimbabwe’s social services, following the steady crumbling of the economy after 2000, was the result of various factors. Among these factors, the most important were the unwise economic and political decisions of the ruling elite, which resulted in Zimbabwe being ostracized by the major world powers for its blatant violations of human rights, and the veritable meltdown of the country’s economy. In fact, the intolerant authoritarian nationalism that informed government policies and actions in this period contradicted the earlier promises of the liberation struggle to provide them with greater freedom to choose their government. This study maintains that the Zimbabwean case illustrates how a liberation movement in Southern Africa “won” the fight for independence but then proceeded to lose the post-liberation struggle for the betterment of the peoples’ lives and the promotion of their human rights.
The People-centered Policies of the 1980s
Zimbabwe’s impressive achievements in providing health and educational services for the majority of the population in the first decade after independence has to be seen within the context of the situation it inherited from colonial rule at independence – a situation that was unquestionably unfair to the Zimbabwean majority and highly skewed in favor of the dominant ruling white elite. It is well documented that under colonial rule the African majority was severely handicapped in law and in practice and greatly disadvantaged by their lack of access to economic and other opportunities. This was nowhere more evident than in the field of education.
Under the colonial education system, the vast majority of the population were systematically disadvantaged by a system that made certain that only as few of them as possible entered the school system and that those who did had to survive numerous hurdles in the form of periodic elimination examinations which meant that only a handful of those who began at Grade 1 reached the university level. According to Riddell, during the late colonial period, out of every 1000 African children, only 337 completed primary school, only 60 attended secondary school and less than 3 entered Form Six or Upper Sixth (Riddell, 1980, p. 15). In addition, education for the African population was grossly under-funded in comparison with education for the white population. Government educational expenditures per pupil in 1977–1978, for instance, were a mere $45 per black student as opposed to $491 per white student (Nhundu, 1992, pp. 78–98).
The type of education that was made available was not intended to produce well-rounded individuals who could take their rightful place as citizens. It was argued that Africans should not be “over educated” to the point of competing with white workers in the marketplace but should be given only practical education which would make them better laborers in agriculture and industry (Dorsey, 1975, p. 41). The colonial approach to African education was summarized aptly by a Member of the colonial Legislative Assembly in 1927, as follows:
We do not intend to hand over this country to the native population or to admit them to the same society or political position as we occupy ourselves… We should make no pretence of educating them in exactly the same way as we do the Europeans.
Not surprisingly, therefore, the frustrations “experienced by Blacks because of severely limited access to education” partly fueled the armed struggle against colonial rule (Nhundu, 1992, pp. 78–98).
Keenly aware of the need to address this injustice, the Zimbabwe African Union-Patriotic Front (ZANU-PF) announced in its 1980 election manifesto its determination to redress the past inequities in education and to establish free and compulsory primary and secondary education for all Zimbabweans. Following its victory at the polls, the new government introduced a wide range of reforms that completely transformed the country’s education system by, among other things, removing the racial divisions that existed and making education accessible to large numbers of Zimbabweans for the first time. Under Education Act No. 5/1987, the government abolished all forms of discrimination in education and made primary education free and compulsory. State support was provided for non-formal adult education, literacy programs and the expansion of teacher education.
The government then undertook a program of vast expansion in infrastructure through the construction of new schools and the rehabilitation of the thousands of schools that had been destroyed in the years of the anti-colonial armed struggle, increasing the number of primary schools by 87.6 percent from 2401 to 4504 between 1979 and 1989 and secondary schools by 748.6 percent from 177 to 1502 in the same period. As a result, primary school enrollment rose by 177.5 percent from 819,586 to 2,274,178, while secondary school enrollment increased by 950.9 percent from 66,215 to 695,882 (Kanyongo, 2005, pp. 65–74). Indeed, Zimbabwe educated more primary school children in the first decade of independence than during all the 90 years of white colonial rule. The government also accelerated the training of teachers, provided teaching and learning materials to schools, and introduced “hot-seating” in schools where two separate streams were taught using the same classrooms with one group attending school in the morning and another in the afternoon. It also introduced the Zimbabwe Integrated Teacher Education (ZINTEC) program which emphasized practical experience in the classroom rather than theoretical training. Finally, it involved communities more in the running of their schools.
The government’s commitment to developing the education sector was evident in the increase in public expenditure from 4.4 to 22.6 percent of recurrent public expenditure between 1979 and 1980 (Kanyongo, 2005, pp. 65–74). Remarkable advances were also made in promoting gender parity in access to education with the proportion of female students at both primary and secondary school level increasing noticeably after 1980 although absolute parity was not completely achieved. Meanwhile the school system was unified so that the inequalities between the socalled Group A (White) and Group B (Black) schools were abolished. Not surprisingly, under such aggressive reforms, the country’s literacy rate shot up considerably, reaching an impressive 94.2 percent among males and 87.2 percent among females and a total literacy rate of 90.7 percent by the end of the first independence decade; the highest rate in Southern Africa at the time (Kanyongo, 2005, pp. 65–74).
Such a rapid expansion of the education sector was bound to create some challenges, among which, according to Nhundu, were the following: “the crisis of unmet expectations, rising ‘educated unemployment’, declining educational quality and wastage, teacher shortages, an unmanageable educational budget and increased social differentiation” (Nhundu, 1992, pp. 78–98). Educated unemployment refers to the fact that the economy was not growing fast enough to absorb all the high school graduates being churned out by the country’s expanded education system. Related to this was the fact that the existing tertiary education institutions were simply not enough to absorb qualified high school graduates who wished to pursue further education, with the result that these institutions were introducing unrealistically stringent entry qualifications that marginalized a large number of otherwise qualified applicants. Until 1989, there was only one university in Zimbabwe with a total enrollment of only 2,000 students. The result was that, out of the 6,000 students who had entered “A” Level schools in 1988, only 1,937 could be absorbed by the one university in the country (Nhundu, 1992, pp. 78–98).
The government responded by increasing the number of public universities from one in 1990 to eight by 2006, and a number of private universities also emerged so that there were no less than 12 universities by 2008. The Zimbabwe Open University (ZOU) was also created to provide access to those who could not go to the regular universities. Its enrollment reached 24,000 by 2007. The rapid increase in enrollment created its own special problems such as under-funding, lack of qualified teaching staff and inadequate library and teaching resources. The result was that many of the so-called universities turned out to be little more than glorified high schools.
The impressive expansion of educational facilities notwithstanding, there was an in-built flaw in the government’s policies, which was that the education reforms were not financially sustainable. Pointing out this potential problem at the time, Nhundu observed:
A dilemma exists for the Zimbabwean government. Whereas it has committed itself to improving the quality of education, it will not be able to sustain current levels of funding for long, much less increase funding for education above current levels. (Nhundu, 1992, pp. 78–98)
Nevertheless, what had been achieved by the government since 1980 was remarkable, hence the glowing endorsements international organizations such as UNICEF and UNESCO made on Zimbabwe.
As in education, in the health sector the government made several remarkable achievements in transforming the unequal inherited colonial system, as the following passage reveals:
As early as 1983, the results were already evident. Infant mortality fell from 120 per 1000 live births in 1980 to 83 in 1983 and 61 in 1989. Maternal mortality rates fell by 28% over the same years. The national average of underweight children dropped from 21% to 17.7% in 1984 and to 11% in 1988. Life expectancy rose from 56 in 1980 to 61 in 1990. These achievements were startling; bringing Zimbabwe very quickly to preside over one of the best health delivery systems in Africa…The promise of health for all became a realizable dream. (Sokwanele, 2005)
These results become all the more impressive when seen against a background of gross inequality in the provision of health services under colonial rule where the emphasis was more on curative rather than preventive medicine, and the majority of the population suffered from high child and maternal mortality rates. Commenting on the colonial disparities in the provision of health services, Herbert Ushewokunze, the Zimbabwean Minister of Health in the early 1980s, pointed out how the incoming independence government,
inherited from the colonial and illegal periods of Southern Rhodesia, a health care system which is profoundly discriminatory in character, [and] discriminatory in geographical, financial and social terms. The Salisbury Group of hospitals alone, serving effectively less than 10 per cent of the population, has been receiving a third of the Health ministry’s budget of curative services and a very high proportion of that allocation has gone to one institution, the new Andrew Fleming Hospital. (cited in Mlambo, 1997, p. 74)
Under the slogan “health for all by 2000,” the new government introduced various measures that vastly improved the quality of life of the majority. Among these were placing a greater emphasis on preventive medicine through the construction of toilets and safe water supplies, immunization against childhood diseases, establishing family planning clinics, providing health education to the villages, training health workers, child nutrition programs in the schools countrywide, and providing free health care for all people earning less than $150 a month. Funding for the health sector was increased from 4.6 percent of the total budget in 1979–1980 to 5.9 percent in 1985–1986 (Sokwanele, 2005). By 1987 the healthcare budget amounted to 2.3 percent of GDP which was approximately “3 times higher than the sub-Saharan African average of 0.8% of GDP” (Munyuki & Jasi, 2009, p. 7; Trane & Bate, 2005).
Under the Government’s Planning for Equity in Health Policy initiative, the 1980s witnessed a very rapid growth of the public health sector. New hospitals and clinics were established across the country, while others were upgraded so that by 2000, the Government had established or upgraded no less than “456 health centres, 612 rural hospitals, 25 district hospitals and a provincial hospital in each of the country’s provinces,” and ensured that 85 percent of the population lived “within 8km of a health facility” (WHO, 2009). As noted above, such advances in the provision of health services to the majority of the Zimbabwean population earned the country accolades from international bodies. However, the Economic Structural Adjustment Programme (ESAP) in combination with other factors marked the start of the decline in the provision of both health and education services among other government programs.
Education and Health under the ESAP
For a variety of reasons, the Zimbabwean government adopted the International Monetary Fund (IMF) and World Bank promoted Economic Structural Adjustment Programme (ESAP) from 1991 to 1995 in a bid to revamp the economy. This economic austerity program insisted on, inter alia, public sector reforms, including the removal of subsidies for social service provision and the implementation of cost-recovery policies in education, health and other sectors. These programs referred to as SAPs became the subject of much controversy among scholars in the Global South, who maintained that the programs were deleterious to the interests and welfare of the poor. In the Zimbabwean case, the ESAP package coincided with the worst drought in Zimbabwe’s history, which ravaged the country in 1992. The combination proved disastrous for the welfare of the poor majority. In particular, the ESAP made access to both education and health services difficult, apart from the other socio-economic ills that it brought into existence (Mlambo, 1997, pp. 40–54).
With respect to education, cost-recovery meant that parents now had to pay the full cost for their children’s education. With the Education Act 1991 (N0. 26/1991), the government introduced fees at primary school level, reversing the policy of free compulsory primary education introduced in 1987. The result was that some parents withdrew their children from school since they could not afford to pay, while others withdrew only their female children when a choice had to be made between educating either boys or girls. Traditional prejudices against educating girl children were revived so that all the advances that had been made in promoting gender equality in education access were eroded. This was despite the fact that the government established a National Plan of Action (NPA) for the 1994–1996 period that included the objectives of narrowing gender disparities in education, with particular reference to basic education and the provision of universal quality primary education by the year 2000. According to Dhliwayo (2001, p. 11): “although parents prefer to send both a male child and a female child to school, if parents are forced to withdraw children, the girl child may lose out,” and he concluded that the “large increases in school fees necessitated by cost recovery in education have impacted negatively on females.”
The school drop-out rate increased when, as a result of the negative economic impact of ESAP, many parents lost their jobs and were forced to resort to the informal employment sector known in Zimbabweas “Siyaso” for survival. In response to the growing ESAP-induced hardships, the country experienced its first IMF riots in reaction to a 30 percent increase in bread prices in 1993, resulting in running street battles between the police and the people in the so-called High Density Areas (former colonial era Townships).
To cushion the very poor, the government introduced the Social Dimensions Fund (SDF), which included a scholarship fund to pay school fees for those who could not afford them, but this was largely inadequate and ineffective. The SDF’s weaknesses included poor targeting of beneficiaries, an urban bias, under-funding, and poor staffing and implementation strategies. By requiring potential beneficiaries to apply through a rather complicated process, it effectively excluded those who needed support the most, the poor and uneducated (Gibbon, 1995, p. 31; Saunders, 1996, pp. 4–6). From 1996 to 2000, the successor to ESAP, the Zimbabwe Programme for Economic and Social Transformation (ZIMPREST) supposedly sought to create the conditions for sustainable economic growth and social development. Like its predecessor, ZIMPREST did very little in this respect.
With regard to the health sector, the austerity years were very damaging, as expenditure on public health declined by 39 percent in 1994–1995 and per capital annual spending declined from $58 in 1990–1991 to $36 in 1995–1996 (Saunders, 1996, pp. 4–6). Even more significant was the fact that the country’s rural clinics, which serviced approximately 80 percent of the country’s population, received a dwindling portion of the country’s public health budget, amounting to only 49 percent in 1996 (Thompson, 2003, p. 6). Not surprisingly, the public health sector stagnated and even declined in some aspects, while there was a marked expansion of the private health sector which provided services that were largely unaffordable to the poor majority. The rapid liberalization of the health sector in the 1990s opened the door so private capital could increase its share of the domestic market at a time of government cuts in public expenditure and the imposition of fee payments for medical services, both of which initiated a process of decline in the public health sector that was eventually to result in the reversal of the earlier gains of the 1980s, as “the cost of both public and private health care soared, undermining access” (Munyuki & Jasi, 2009, p. 4).
User fees, particularly, had a serious negative impact on the utilization of health services. There was a sharp drop in health service usage following the introduction of user fees (Zigora, Chihanga, Makahamadze, & Hongoro Ropi, 1996). A 1993 UNICEF study reported that Zimbabwe’s health services declined by a whopping 30 percent and “fewer people were visiting clinics and hospitals because they could not afford hospital fees” (Dhliwayo, 2001, p. 9). According to Dhliwayo, the liberalization and privatization of health services “limited access to care to those who [could] afford the fees and… exposed the poor to potentially large unexpected costs.” Consequently, the 1990s saw a widening of the gap in access to health services between the well-to-do and the poor majority, with “the high salaried urban based consumers… serviced by the conventional medical private doctors with ultramodern services,” while the poor majority in both the rural areas and urban spaces increasingly resorted to traditional healers whose charges were affordable (Mudyarabikwa & Madhina, 2000, p. 12). By effectively transferring the burden of funding health services from the government to individuals and households, the government’s policies made it difficult for poor people to access the health services they previously enjoyed (Nyazema, 2010, pp. 233–262).
Under the ESAP regime, Government priorities in health provision shifted from the earlier people-oriented and egalitarian approach enunciated in 1984 to a more market-driven and privatization based strategy. Thus, while the earlier policy approach emphasized the need to redirect resources to the most needy members of the population and thereby put an end to the inherited colonial rural–urban racial bias by giving the poor majority greater accessibility and placing greater emphasis on preventive rather than curative medicine, the policy shift of the 1990s spoke an entirely different language. This policy approach was now based on the language of decentralizing the provision of health services, fees for services, outsourcing and the need to increase the role of the private sector in the provision of health services. Unsurprisingly, under this favorable dispensation, private medical institutions, including private clinics and nursing and maternity homes, increased as revealed in Table 1.
Changes in the Number of Medical Institutions, 1991–1996
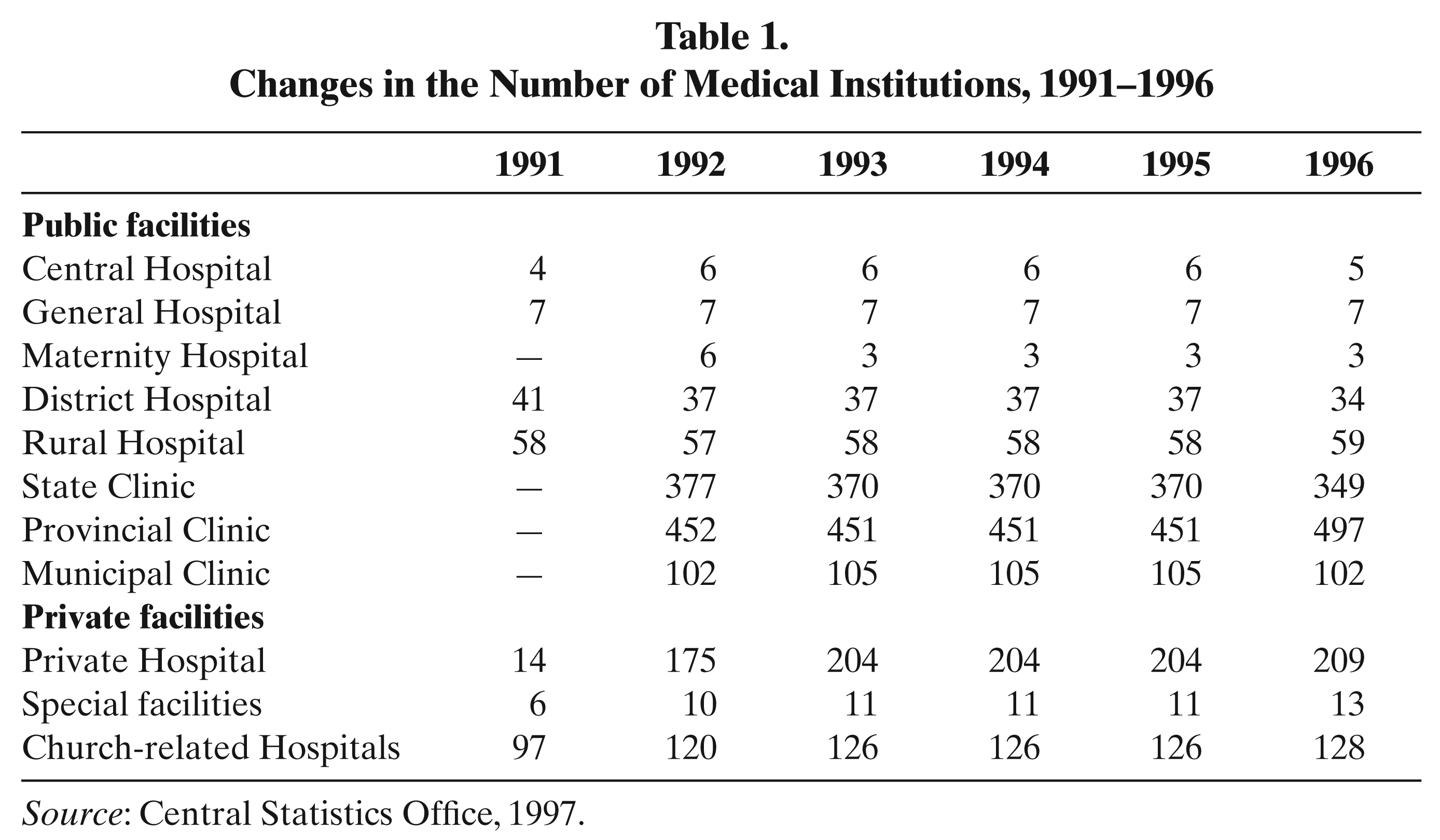
Source: Central Statistics Office, 1997.
Into the Abyss: Health and Education in the Crisis Years, 2000–2008
The slow decline of the country’s social services in the late 1990s escalated into a crisis of major proportions in the first decade of the new millennium as Zimbabwe’s economy went into a virtual meltdown. The decline of the Zimbabwean economy that followed in the wake of the chaotic land reform program that saw hordes of ZANU-PF supporters and sympathizers invading white-owned commercial farms and evicting thousands of Black farm workers from their homes became more severe as the decade unfolded, reaching its nadir in 2008. Much has already been written on Zimbabwe’s economic crisis and thus this subject need not detain us here, except to highlight some of the indicators of that crisis. These included a hyperinflation rate of 165,000 percent, a 99.9 percent decline in the value of the Zimbabwean currency as measured against the US dollar and 90 percent rate of unemployment by 2008. Meanwhile, it was reported that “living standards fell by 38 percent” between 1997 and 2007 (Hanke, 2008, p. 1).
The evidence of the disastrous impact of the economic crisis on the country’s public health sector is overwhelming. For instance, average life expectancy declined from 62 to 44 years between 1990 and 2008, while maternal mortality increased from 168 per 100,000 live births in 1990 to 880 per 100,000 live births in 2005 (USAID, 2010, p. 8). Infants and children under five mortality rose from 77 per 1000 live births in 1994 to 86 per 1,000 live births in 2009 while the percentage of under-weight children under the age of five increased from 13 percent in 1999 to 15 percent in 2010 (UNDP, 2010, p. 22; UNESCO, 2010, p. 22). The situation was arguably even worse than this, as the very poor no longer attended public health institutions where they were now required to pay fees and so deaths in the rural areas may have gone unreported.
Meanwhile, the HIV-AIDS epidemic was taking its toll on the Zimbabwean population. By 2006, AIDS was reportedly killing 2,500 individuals every week (Elhoweris & Parameswaran, 2006, p. 109). It was estimated that HIV prevalence among adults 15–49 years was as high as 15 percent in 2007 (WHO, 2008, p. 5), while approximately 1,320,739 adults and children were living with HIV and AIDS (Parreño, 2008, p. 2).
The clearest evidence of the collapse of the country’s public health system was the cholera outbreak of 2008. In August of that year, the first cases were reported in Chitungwiza, a dormitory town outside the capital Harare. Thereafter, the pandemic spread quickly across the country, while the numbers of those infected equally escalated so that by December 9 there were 16,141 suspected cases of cholera and 775 deaths in the country’s 62 districts. By December 26, the number of cases had risen to 26,497, while the numbers of deaths since the outbreak were reported by the Ministry of Health of Zimbabwe to have risen to 1,518, with outbreaks having spread to all the country’s 10 districts. The WHO reported that the “mortality outside of healthcare facilities remains very high” and, by implication, unrecorded. Cholera reportedly spread to Musina in South Africa, Palm Tree in Botswana and the Guro District in Mozambique (WHO, 2008).
Between August and December, the government downplayed the extent of the pandemic until it became impossible to pretend that there was no crisis, especially since the country’s health care services were clearly unable to contain it. Rather than take full responsibility for the collapse of its health services, the Government resorted to a childish blame game in which Dr Sikanyiso Ndlovu, then Minister of Higher Education, shamefacedly claimed that “the cholera epidemic in Zimbabwe is a serious biological chemical warfare, a genocidal onslaught on the people of Zimbabwe by the British” and their “American and Western allies so that they invade the country” (The Telegraph, December 12, 2008).
The truth, of course, was that the cholera outbreak had been caused by poor sanitation and contaminated drinking water due to the inability of the Zimbabwe National Water Authority (ZINWA) to provide purified water and to maintain water sanitation facilities. This parastatal had been established by the ruling party in 1999 in an attempt to wrest control of the country’s urban centers following the sweeping victory by the opposition Movement for Democratic Change (MDC) in the country’s municipal elections which placed over 80 percent of local governments under opposition control. ZINWA took over control of Harare’s water supply in 2005 and failed to provide adequate water supplies from the very beginning due to a combination of incompetence, a severe shortage of purification chemicals such as chlorine, and because of inadequate financial resources in the collapsed economy. Commenting on the country’s collapsing water supply system just before the cholera outbreak, UNICEF reported:
The proportion of people with access to safe drinking water has been declining since early 2000 and the situation is expected to worsen further during 2008 due to the current economic challenges and the crumbling infrastructure. Financial constraints, fuel shortages, lack of foreign currency for spare parts and treatment chemicals have resulted in decreased maintenance of the current water systems. The situation is exacerbated by frequent electricity power cuts, which reduce the pumping time into the reticulation water systems (UNICEF, 2008b, p. 2).
The country’s sewage system was also reportedly breaking down “due to age, excessive load, pump breakdowns and poor maintenance” resulting in sewage discharges contaminating major drinking water sources and supplies. As a result, Zimbabwe suffered minor cholera and diarrhea outbreaks in 2007, resulting in over 90 deaths (UNICEF 2008b, p. 3).
Meanwhile, on December 1, 2008, because of mounting economic and logistical challenges, ZINWA completely stopped pumping water to Harare. The city’s poor population, without access to boreholes, resorted to using unprotected well water for household needs. Commenting on the breakdown of the country’s water supply and sanitation systems, UNICEF noted in 2008:
Sewage systems in most urban areas have broken down due to age, excessive load, pump breakdowns and poor maintenance. The breakdown of sewage systems has led to large volumes of raw sewage being discharged into natural watercourses, which ultimately feed into major urban water supply sources, thus carrying a significant risk to public health (UNICEF, 2008b, p. 3).
The cholera outbreak in the country that year demonstrated just how far the collapse of the social services sector had placed Zimbabwean public health at risk.
The severity of the outbreak was expected given the collapse of the health delivery system in which four major hospitals had closed their doors for lack of staff and medicines, since the prevailing hyperinflation made it almost impossible for health institutions to purchase drugs and medicines. Thus, although the treatment of cholera basically focuses on “replacing fluids and electrolytes at the same rate as their loss” (Fisher, 2009) and cholera deaths are entirely preventable, the ailing health delivery system simply could not cope with the spread of the disease. As a result, the Government was forced to declare a national emergency on December 3, 2008, thus opening the doors to international assistance.
By 2008, the country’s public health system was in shambles. As one report at the time indicated:
The main referral hospitals in the country, including Harare Central, Parirenyatwa and United Bulawayo hospitals, are barely functioning and some wards have even been closed. Two government maternity hospitals in greater Harare have been closed. Many district hospitals and municipal clinics are either closed or operating at minimum capacity. The University of Zimbabwe Medical School closed indefinitely on 17 November. The system is paralysed by shortages of drugs and medical supplies, a dilapidated infrastructure, equipment failures and a brain drain. As a result, ordinary Zimbabweans are unable to access basic health care. (Amnesty International, 2008)
In a similar manner, following an impressive period of growth and expansion, the education sector went through a precipitous decline in the first decade of the new millennium. Hailed as a leader in Africa for a literacy rate of 93 percent for males and 87 percent for females by the end of the twentieth century, Zimbabwe came very close to achieving its goals of “education for all by 2000” (Tonini, 2005, p. 95). These notable achievements were reversed in the new millennium as the country’s declining economic situation, falling living standards and the chaotic land reform program displaced over 150,000 farm workers and forced children out of school to work in order to support their families or to seek refuge in the cities where they became street kids, engaging in prostitution, begging and crime. Meanwhile, the children of those who “invaded” former commercial farms could no longer attend school or had to contend with schools without adequate infrastructure or staff.
Commenting on the deteriorating state of Zimbabwe’s education system, a UNICEF (2008b, p. 3) report noted that the country’s poor economic situation had negatively affected school attendance and the education system was characterized by “low enrollment rates, declining attendance and completion rates, a low transition rate to secondary schools and insufficient learning spaces, teachers and learning materials.” In 2009, the Zimbabwe Teachers’ Association (ZIMTA) warned that the education system was on the verge of collapse because of a “critical shortage of teachers, teaching and learning materials, poor remuneration and low morale” and reported that teachers were either leaving the country or “simply stay away from their schools” as they “are some of the lowest paid professionals in the country” (Sokwanele, 2008).
Problems also bedeviled the higher education sector: a serious brain drain caused by senior and experienced academics who voted with their feet to go in search of greener pastures abroad to escape the low salaries and growing political intolerance, government interference in university matters, and the curtailment of academic freedom, which reduced the once acclaimed higher education system to a sorry state. The deterioration of standards at the flagship of the country’s higher education sector, the University of Zimbabwe, was a clear example of how the country’s system of higher education was undergoing a crisis by the first decade of the new millennium (Mlambo, 2005, pp. 107–130). Both the education and health sectors were, thus, in dire straits by the end of the first decade of the twenty first century.
Accounting for the Collapse of the Health and Education Sectors
Any explanation of the near collapse of the country’s social services sector and the rapid decline of health and education services in particular must take into account the economic meltdown that the country suffered in the wake of the government’s chaotic land reform program, the growing political intolerance of the ZANU-PF ruling party and the persecution of those perceived to be supporters of the political opposition. Zimbabwe’s economic meltdown followed the 2000 referendum in which the government suffered a humiliating rejection of its proposed constitutional reform and the ruling party unleashed its supporters in a campaign of terror and intimidation that saw hundreds of white farmers and thousands of farm workers, suspected of being opposition supporters, evicted from the land. The downward economic spiral that followed thereafter, as the Western world either boycotted Zimbabwe or imposed sanctions on its leadership and select businesses saw the country’s GDP plummet drastically between 2000 and 2008, while the inflation rate rose to unprecedented heights in modern history. These conditions had a severe impact on the country’s public funding for health and education, among others, and on salaries and the standard of living, triggering a stream of out migration by professionals that crippled both the public health and education sectors. Commenting on the deleterious effect of the economic meltdown on the health sector during his Statement on the 2009 Budget, the Zimbabwean Minister of Finance Tendai Biti stated:
The economic decline has contributed to the deterioration of health delivery, including the shortage of health professionals, inadequate supply of essential drugs, equipment, and other medical supplies, inadequate provision and maintenance of equipment, infrastructure, ambulances, and service vehicles… The above have contributed to an increase in the incidence of preventable diseases. (Biti, 2009)
A similar statement could also have been made with regard to the education sector where declining levels of government funding resulted in classrooms without chalk, paper, textbooks and other teaching aids, which contributed to growing frustrations among the country’s teachers, especially in the already poorly funded rural schools. Unsatisfactory working and living conditions, poor remuneration and an increasingly toxic political climate in which anyone suspected of opposing the ruling party was subjected to harassment fueled out migration to South Africa, Europe, the United States, Australia and other parts of the world where the country’s education, health and other professionals could make a reasonable living.
Out migration among medical professionals was fueled by a mixture of political and economic factors. A recent study of the causes of Zimbabwe’s medical diaspora found that the three major factors given by doctors who left the country were, in order of importance, “the bad political environment (74% in agreement), lack of opportunities for career advancement (73% agreed) and poor economic conditions in Zimbabwe (71% agreed)” (Chikanda, 2011, p. 2). Secondary factors included “unsatisfactory working conditions, inadequate remuneration and benefits, the collapse of the health care system” and concerns about their children’s future.
The extent of the manpower crisis in the public health sector by 2009 is documented in Table 2 and shows that, as of January that year, the health system was operating with only 57 percent of its staff capacity as nurses, doctors, pathologists, and other key professionals were leaving at a faster rate than the training institutions could replace them. And some of the training institutions were either functioning at highly reduced levels or not functioning at all due to budgetary constraints. For instance, the College of Health Sciences at the University of Zimbabwe was closed from November 2008 to May 2009. It was also reported in 2009 that academic posts at medical schools and nurse tutor posts were 60 percent vacant and, because of this, there were “significant failure rates for medical students and nurses in the past five years” (USAID, 2010, p. 75). The same report indicated the causes of the widespread shortage of skilled personnel in the public health sector included “out-migration due to lack of incentives, low salaries, and poor working conditions; HIV/AIDS, and a shortage of senior and experienced providers and managers.”
National Shortage of Staff per Cadre in January 2009
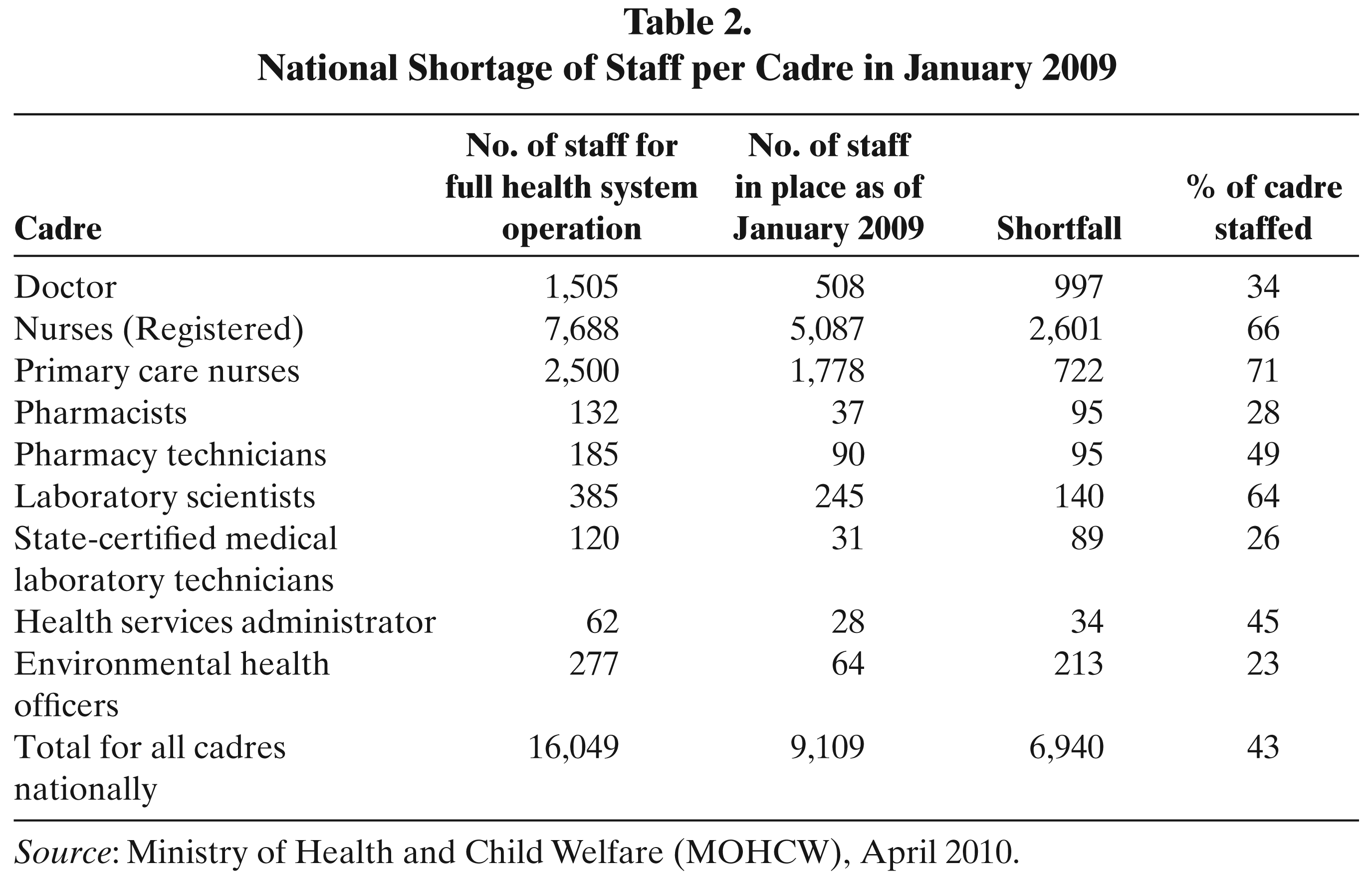
Source: Ministry of Health and Child Welfare (MOHCW), April 2010.
In the education sector, poor salaries and the political persecution of teachers by supporters of the ruling party, as they were suspected as being generally sympathetic to the opposition MDC, forced many of them to abandon the classroom, either to pursue alternative survival strategies within the country or to migrate to South Africa and other neighboring countries in search of greener pastures. The Progressive Teachers Union of Zimbabwe (PTUZ) estimated in 2007 that 25,000 teachers, approximately a quarter of the teacher population in the country, had emigrated since the beginning of the year to South Africa, Botswana or Namibia. Approximately 20,000 of them were said to be in South Africa working in “unskilled security or construction industry jobs” (Bevan, 2007). Another report noted that, of those teachers who still remained in the country in 2008, “morale is rock bottom and a significant proportion are inexperienced or untrained.” In addition, school attendance decreased considerably, with only 20 percent of children attending school at the end of 2008, as compared to 85 percent in late 2007.
Meanwhile, the country’s record hyper-inflation meant that the teachers’ already meager salaries could not pay even for basic necessities (Save the Children Alliance, 2009). Not surprisingly, therefore, in July 2011, the Principal Director for Finance and Human Resources in the Zimbabwean Ministry of Education, Sports and Culture reported that only 96,000 qualified teachers were in the government schools throughout the country as against the 111,000 teaching posts available. Even unqualified teachers were reported to be shunning the profession because of the poor working conditions (Mafu, 2011).
Conclusion
As this article has demonstrated, Zimbabwe made impressive strides in improving access to education and health services for the majority of its people in the immediate period following independence as a result of a successful campaign to redress the inequalities of the past. During this period, Zimbabwe received international accolades for its people-oriented policies and was regarded as an example to be emulated by developing countries elsewhere.
The adoption of the neoliberal Economic Structural Adjustment Programme (ESAP) in 1990 led to the gradual reversal of the country’s earlier gains and achievements, leading to both a large number of school dropouts and a substantial decrease in the use of public health services as a result of the new requirement that the users of these services pay fees to cover the costs of the services. The deterioration of both the country’s health and education services worsened with the onset of Zimbabwe’s economic crisis at the start of the new millennium when the economy’s downward spiral, the mounting political instability and the government’s repression of political dissent led to a massive brain drain of teachers, doctors, nurses and other specialists.
Due to the dwindling financial resources for the purchase of medicines for the hospitals and clinics and to pay the teachers, the country’s health sector all but collapsed in 2008, leading to a major cholera outbreak, while the school system was reduced to operating at minimal capacity. Clearly, the ruling elite’s promises at independence in 1980 of education and health care for all by 2000 were not met. If anything, the majority of the Zimbabwean people were in a more precarious position than at independence.