
Abstract
The ability of individuals to accommodate the emotional transition into roles requiring the construction of a leader identity is an under-researched phenomenon. To address this research gap we consider the experience of 32 nurse managers undergoing a leadership development programme, exploring how an emotional attachment to their professional group identity may cause identity conflict during the construction of a managerial leader identity. We consider how competing desired identities can result in negative emotional experiences, calling into question existing work, which assumes that desired group identities are congruent with leader identities. Our work suggests that identity work can mitigate identity conflict at the individual level, enabling nurse managers to function in their role, but emotional distress will continue due to a perceived loss of professional identity and group influence. We contend it is only by eschewing an emotional attachment to a professional group identity that nurse managers will be able to overcome this negative emotional experience.
Moving into roles that require the construction of a leader identity is an emotional transition for individuals, because it challenges their other social identities (Driver, 2012; Fineman, 1997; Petriglieri & Stein, 2012; Tee et al., 2013). The existing identity literature, however, is often criticized for neglecting the influence of emotion, particularly in relation to leadership (Cascón-Pereira & Hallier, 2012; Vince & Broussine, 1996). Identities are constructed in line with the emotional attachments developed with various social groups, generating a sense of meaning and belonging (Fotaki, 2010; Stavrakakis, 2008). As a result social groups frame identity work, as individuals strive to construct identities that support their continuing, emotionally important, group membership (Harding, 2007). Understanding emotional influences on identity work, therefore, may provide important insights into the complex nature of identity transitions (Driver, 2009; Roberts, 2005).
Extant literature suggests that individuals who feel able to construct desired identities experience increased self-esteem and a sense of legitimacy, in addition to high levels of group influence (DeRue & Ashford, 2010; Stavrakakis, 2008). The picture, however, may be more complex as multiple, competing identities reside within an individual’s self-concept (Brown & Toyoki, 2013; Wright et al., 2012), triggering identity conflict and negative emotions (Petriglieri, 2011; Stavrakakis, 2008; Sveningsson & Alvesson, 2003). In this paper we consider how social group members engage in identity work, the dynamic, narrative process through which individuals construct subjectively desired identities (Thornborrow & Brown, 2009; Watson, 2008), to deal with identity conflict associated with identity transition.
To date, scholars suggest identity work results in positive identity transitions, reducing identity conflict and protecting against negative emotions (Humphreys & Brown, 2002; Thornborrow & Brown, 2009; Wright et al., 2012). We interrogate this assumption by considering the identity work engaged in during the ongoing construction of leader identities. While influential leaders need to conform to socially determined ‘desirable’ leader constructions, they must also be perceived by others as representative of the social group they are attempting to lead (DeRue & Ashford, 2010; Petriglieri & Stein, 2012; Tee et al., 2013). In other words, leaders must be able to construct and communicate to other group members a desirable leader identity and a desirable social group identity. This raises two questions: What is the emotional experience of attempting to construct a leader identity alongside a social group identity; and How do individuals engage in identity work to deal with that experience?
To address these questions we consider the experiences of 32 subordinate professionals, in this case nurses, moving into professional hybrid roles (Marinetto, 2011; O’Reilly & Reed, 2010; Tummers, Steijn, & Bekkers, 2012), requiring the construction of a desired group identity alongside a desired leader identity (Tee et al., 2013). Considering the experiences of nurses moving into hybrid roles complicates matters, as the desired group identity is associated with subordination, rather than leadership (Abbott, 1988; Allen, 1997). Existing research suggests that nurses often struggle in managerial leadership positions (Burgess & Currie, 2013), bringing issues of identity conflict and emotional experiences to the fore. In exploring the experiences of nurse managers, our work responds to recent calls for research into the identity work engaged in by subordinate or marginalized individuals constructing leader identities (Srinivas, 2013).
The remainder of the paper unfolds as follows. We begin by exploring the socially constructed nature of desired identities, and how they drive identity work. In doing so, we consider how a discrepancy between an individual’s self-concept and their desired identity causes identity conflict, and explore the way identity work is employed to mitigate negative emotions, within the context of the construction of managerial leader identities. While existing research assumes that leader identities are congruent with the desired identities of social groups (Thornborrow & Brown, 2009; Wright et al., 2012), we use nurse identities to illuminate a circumstance in which that is not the case.
Exploring the experiences of nurses in hybrid roles, we adopt a narrative approach (Humphreys & Brown, 2002) to explore the identity work employed to mitigate negative emotions during ongoing identity transition. By analysing interview discourse about the way individuals discuss their experiences, and attempt to resolve potential identity discrepancies, we draw insight into their identity work and resulting emotional responses. Through our analysis we explore how nurse managers said they perceived a leader identity and a nurse identity to be incongruent, triggering identity conflict and a feeling that they had lost group influence. We suggest that, rather than a positive influence on identity work, encouraging identity transition and facilitating the construction of desired identities (as outlined by Srinivas, 2013, and Thornborrow & Brown, 2009), a continuing emotional connection to a social group identity can exacerbate negative emotional experiences for professionals constructing leader identities.
Identity and Leadership in Social Groups
All individuals develop emotional attachments with multiple social groups, providing a sense of meaning or belonging, and guiding behaviour, in line with group expectations (Fotaki, 2010; Stavrakakis, 2008). Group memberships influence identity construction, as individuals strive to communicate to others a desired group identity (Harding, 2007; Petriglieri & Stein, 2012; Sveningsson & Larsson, 2006). Desired identities are preferred versions of self or group identity (Thornborrow & Brown, 2009) and frame identity work, social interactions through which individuals attempt to influence how their identity is perceived by others (Alvesson & Willmott, 2002; Sveningsson & Alvesson, 2003; Watson, 2008).
Desired identity constructions rely on the acceptance of individual identity claims by others, affirming that they perceive that individual’s identity to be a legitimate one (Brown & Toyoki, 2013; Pritchard & Symon, 2011). Subsequently, constructing an identity reflecting the desired identity of other group members is crucial for influence within social groups (DeRue & Ashford, 2010; Stavrakakis, 2008). Due to multiple group memberships, however, individuals construct different desired identities depending on the social context (Alvesson, 1994; Ellis & Ybema, 2010; Sveningsson & Alvesson, 2003), resulting in multiple, contradictory narratives. These contradictions can undermine an individual’s ability to communicate to other group members a desired identity, triggering individual identity conflict (Alvesson & Willmott, 2002).
Identity conflict occurs when individuals feel that others perceive them as acting in a manner incongruent with a desired group identity, or when they themselves feel unable to sustain multiple identities (Petriglieri, 2011). In times of conflict, individuals engage in identity work to create a sense of coherence between competing identities, enabling them to move between multiple identity constructions (Clarke et al., 2009; Sveningsson & Alvesson, 2003). This is an ongoing process, as individuals move between old and new identities, allowing them to accommodate new identity demands without sustained identity conflict (Ibarra, 1999). In some cases, identity work results in positive, generative change for individuals, and increases their group influence, as they are seen as continuing to strive towards a desired group identity (Thornborrow & Brown, 2009; Wright et al., 2012).
Similar to the construction of social group desired identities, leadership influence relies on the communication of a desired leader identity to potential followers (DeRue & Ashford, 2010; Ibarra & Barbulescu, 2010; Sveningsson & Larsson, 2006). Leaders of social groups, however, also need to maintain their desired group identity to remain influential (Petriglieri & Stein, 2012; Tee et al., 2013), making the transition towards a leader identity emotionally challenging if it threatens their ability to communicate a desired group identity to others (Driver, 2012; Fineman, 1997; Vince & Broussine, 1996). Identity transition is further complicated, as the behaviour of group leaders is framed by the desired group identity (Tee et al., 2013). Social group identity demands generate the potential for identity conflict, as leaders may, at times, be required to act in ways incongruent with their desired social group identity, triggering negative emotional responses and undermining their group influence. While previous research acknowledges the potential emotional challenges of developing a leader identity alongside pre-existing social identities, it concludes that the experience can be positive, encouraging individuals to engage in identity work to accommodate multiple identity demands (Kippist & Fitzgerald, 2009; Noordegraaf & De Wit, 2012).
Based on the above, we suggest that extant research does not account for the experiences of groups who face ongoing struggles in leadership positions. Individuals occupying hybrid positions, roles in which they are required to construct desired professional and managerial leader identities (Kippist & Fitzgerald, 2009), are a group who regularly experience identity conflict arising from fragile identity constructions, and negative emotional experiences when transitioning towards managerially defined leader identities (Harding et al., 2014; Thomas & Linstead, 2002; Sveningsson & Alvesson, 2003).
In this paper, we explore how professional hybrids attempt to mitigate associated identity conflicts by addressing two questions: What is the emotional experience of attempting to construct a leader identity alongside a social group identity; and How do those in hybrid roles engage in identity work to deal with that experience? We do so by focusing on nurses, a group traditionally viewed as subordinate followers, rather than leaders (Abbott, 1988; Allen, 1997), thereby responding to calls for further research into the identity work engaged in by subordinate groups moving into managerially defined leadership roles (Srinivas, 2013).
Research Context
To date there has been relatively little exploration of leader identity constructions among subordinate groups. This is surprising, as collective subordinate group identities are influenced by subordination to more powerful groups (Abbott, 1988; Pratt & Rafaeli, 1997), rendering their potential identity conflict more explicit when constructing leader identities. Nurses provide an illuminating context from which to explore the emotional experiences of professional hybrids for two reasons. First, they attach emotional significance to their ability to construct a desired professional identity, bringing emotional elements of identity transition to the fore (Brown & Lewis, 2011; Brown & Toyoki, 2013; Kreiner et al., 2006). Second, existing research into nurse hybrids suggests that they often experience identity conflict, and are seen by other professionals to lack influence in their new roles (Burgess & Currie, 2013).
The assumption that nurses in hybrid roles struggle with identity conflict is perhaps unusual for a group who regularly engage in identity work. Nurses continually engage in identity work due to the emotionally demanding nature of their role, in which they are required to present an appropriate self-image to others depending on the context (Hayward & Tuckey, 2011). Previous research argues that nurses are a professional group who encounter little difficulty in embracing certain aspects of their identity, while distancing themselves from others (Bolton, 2001). Consequently, nurses should be adept at overcoming identity conflict and negative emotions. While nurses’ leadership struggle is often attributed to the dominance of physicians within healthcare settings (Diefenbach & Sillince, 2011; Finn et al., 2010), it is also acknowledged that nurses play an influential role in medical decisions and treatments, and cannot be perceived as merely passive team members (Hughes, 1988; Svensson, 1996). We argue, therefore, that one of the challenges for nurses constructing leader identities is their difficulty in accommodating the discrepancies between leader and desired professional identities, rather than the influence of medical hierarchies.
Nursing is a predominantly female profession, with 90 per cent of the workforce made up of women (NHS, 2010). This is, in part, due to the inherently ‘feminine’ identity of the profession (Porter, 1992, p. 512), framed by symbols of Florence Nightingale, encouraging ideals of obedient, altruistic and passive caring, despite the increasing technical skills, academic education or leadership roles required by modern nurses (Goodrick & Reay, 2010). The symbolic function of nursing complicates issues of identity construction for group members, influencing their desired professional identity, in spite of the demands of their modern role (Fotaki, 2010).
Although a minority group, male nurses occupy a disproportionate amount of nursing leadership positions (Cross & Bagilhole, 2002). One influence on the high proportion of male to female nurse leaders is the underlying societal assumption that men are more ‘desirable’ leaders than women (Fotaki, 2013; Pullen & Simpson, 2009). Desirable leader identities are associated with masculine, authoritative behaviours (Offermann, Kennedy, & Wirtz, 1994, p. 49), and with power, charisma, and influence over others (Alvesson & Sveningsson, 2003; Den Hartog et al., 1999). Nurses moving into hybrid roles must communicate leader identities to others, while remaining representative of the collective nursing identity (Petriglieri & Stein, 2012; Stavrakakis, 2008), such as in the case of Modern Matrons (Currie, Koteyko, & Nerlich, 2009) or Ward Managers (Bolton, 2003). 1 How nurses are able to align a distinctly feminized professional identity with a more masculine leader identity remains unexplored.
A further influence on the construction of leader identities is the institutional context, particularly in public sector organizations (Currie & White, 2012; Noordegraaf & De Wit, 2012). In these professionalized settings, despite a policy focus on the need for transformational leadership, more managerialist forms of leadership develop (Blomgren, 2003; Currie & Lockett, 2007). Managerial leadership is defined as transactional, concerned with day-to-day performance management. To conceptualize it another way, O’Reilly and Reed (2010) define managerial leadership as ‘leaderism’, a hybrid state between professionalism and managerialism, suggesting professionals may be more willing to take on hybrid roles when framed as leadership. Moreover, it is a type of leadership framed by concern with efficiency and meeting targets (Currie & Lockett, 2007). Consequently, subordinate professionals constructing leader identities in the context of hybrid positions may encounter difficulties, as they attempt to align the competing demands of two incongruent desired identities (Blomgren, 2003; Kippist & Fitzgerald, 2009; Noordegraaf & De Wit, 2012).
Research Design
Data collection
To explore the identity work used to deal with identity conflict, we adopt a narrative approach, which enables us to explore the way individuals negotiate, share and contest identities (Alvesson & Karreman, 2000; Boudens, 2005; Humphreys & Brown, 2002); and which has been used in other studies exploring identity work and identity constructions (Brown & Toyoki, 2013; Wright et al., 2012). Expression of emotion in narratives offers insights into the process of identity development, and gives an indication of how the individual would like to be perceived by others (Horrocks & Callahan, 2006). 2
Data collection focused on two leadership development programmes within the same mental healthcare provider in the English NHS, purposely chosen for the access offered to individuals moving into roles requiring the construction of both nurse and leader identities. We conceptualize leadership development programmes as formative areas of identity transition, which encourage ongoing identity work, making them an ideal setting to explore the construction of leader identities (Carroll & Levy, 2010; Petriglieri & Stein, 2012). We do not claim that attending these programmes classes these individuals as ‘leaders’, but they represent a group of individuals in hybrid positions who are required to construct a managerially framed leader identity alongside their pre-existing professional identity.
In order to become ‘immersed’ in the social context of the leadership development programmes, one researcher enrolled in both programmes running between September 2009 and October 2010, and attended all course events. A total of 120 hours of participant observation was recorded in field notes, used to contextualize subsequent semi-structured interviews and interactions with study participants, contributing to a more in-depth understanding of the research context (Fairhurst, 2009). 3 Additionally, the primary researcher came from a professional nursing background. During interviews, this enabled the mutual identity construction of both the researcher and the interviewee as members of the same social group, something found to be beneficial in other explorations of identity work (Thomas & Davies, 2005).
Semi-structured interviews offer insights into identity work, as individuals attempt to construct desired identities through narratives (Brown & Toyoki, 2013). An interview protocol was developed from themes and conclusions derived from the literature, and supplemented by participant observations from the programmes, but respondents were encouraged to speak freely when discussing perceptions of their identity. Interviews subsequently differed between respondents, as they engaged in their own narratives, but the main themes focused on: their perceptions of their own identity (how they talked about themselves as a nurse or managerial leader); the way they thought others perceived them, or their experiences of interactions with others due to their perceived identity; the emotional experience of constructing a managerially framed leader identity; and the ways in which they attempted to deal with competing identity demands. Example questions can be found in the Appendix.
At the close of the programmes, all nurses attending the course were invited to participate in the study. In total 32 nurse managers were recruited and were interviewed twice over two years. The first round of interviews was conducted immediately after the close of the programme, and the second round conducted 12 to 18 months later. Interviews took place at two time points, as identity transition is an ongoing process, developing and changing over time (Hirst et al., 2004). In total we conducted 64 interviews, all interviews lasting between 45 and 60 minutes.
Data analysis
All 64 interviews (totalling 60 hours total interview time) were recorded and transcribed. Following an inductive coding technique, as outlined by Strauss and Corbin (1990), interview data were reviewed line by line to generate first-order codes. Transcripts were first explored for the way nurse managers talked about their identities. We then coded for instances when interviewees talked about being a ‘nurse’ or ‘leader’ in discussion with the interviewer. Following this, we coded for the emotional experiences reported by nurse managers, and how they talked about their experience of trying to align desired nurse and leader identities. Finally, transcripts were examined for examples of identity work used to deal with identity conflict and emotional experiences.
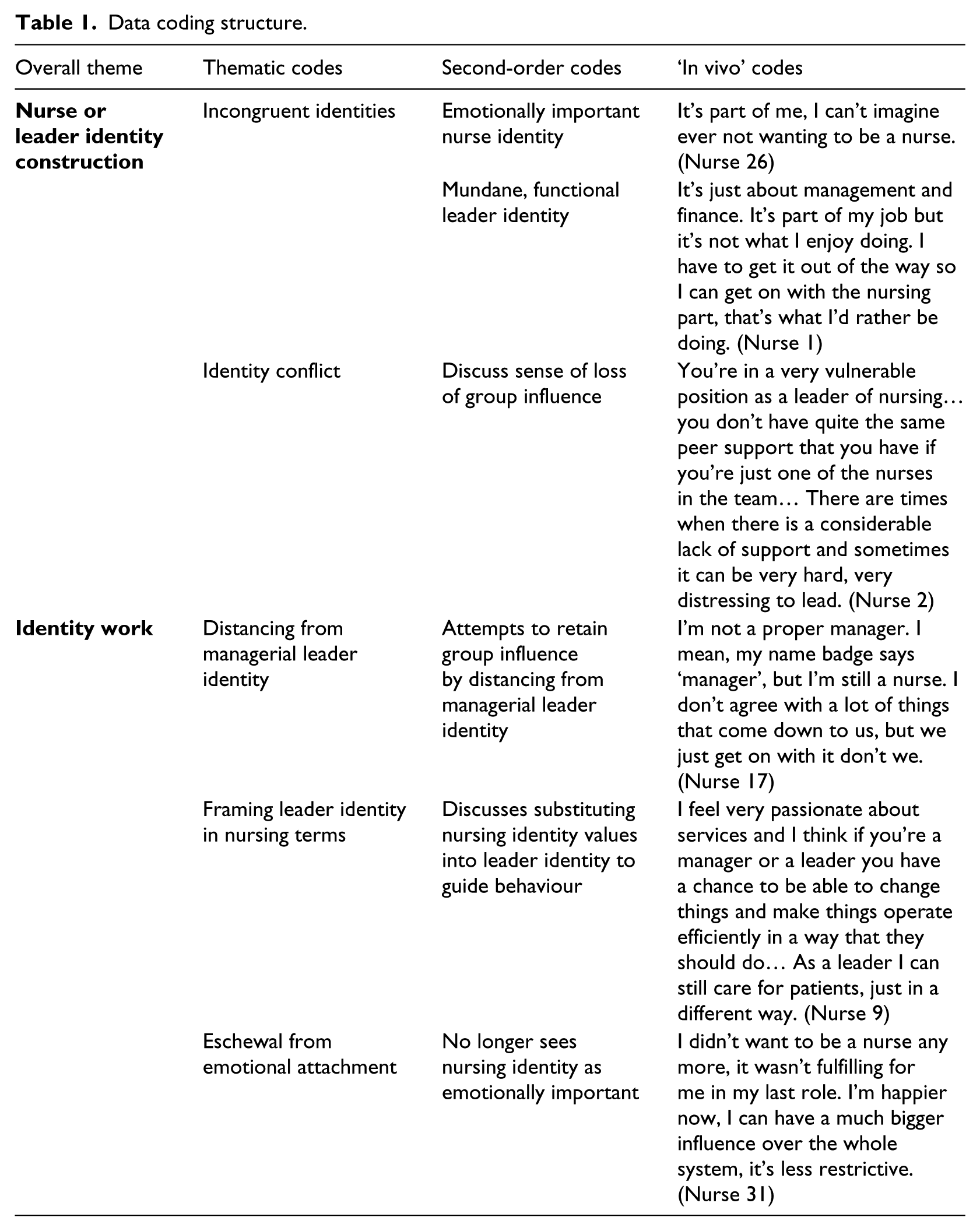
Following first-order coding, in second-order coding we identified two overarching categories: the way interviewees discussed nurse and leader identities in distinctly different ways, and the identity conflict which arose from this; and the use of identity work to deal with the emotional experiences associated with identity conflict. In the first category, nurse managers talked about nursing in a passionate way, associated with positive emotions, while their leader identity was discussed in a more mundane, functional manner. They also talked about concerns that they were losing their ability to construct a desired professional group identity, undermining their associated group influence, causing emotional distress. In the second category, we explored how nurse managers talked about three types of identity work in attempts to deal with their negative emotional experience: attempting to gain group influence by distancing from managerial leader identity demands; attempting to retain professional influence by framing discussions about their leader identity in nursing, not managerial terms; and finally, eschewing their emotional need to construct a desired nurse identity, moving towards a desired leader identity. Our coding structure, and examples of data, linked to first-order codes, is outlined in Table 1.
Data coding structure.
Findings
Identity conflict and emotional experiences
As outlined above, the nurse managers interviewed were not acting in traditional, ward-based roles, which are commonly associated with nurses, but occupied hybrid positions requiring them to construct a leader identity alongside their professional identity. While the nurse managers acknowledged that the functions of their role were primarily managerial, they were clear about their positive emotional connection to a professional nurse identity:
I do very much have that kind of emotional connection with nursing… it’s like having a child and then being able to connect… you feel something inside. I feel something inside about what I do; I feel something passionate about nursing. (Nurse 13)
In addition to the positive emotions associated with the nursing identity, being a nurse was often talked about as an integral part of their sense of self:
I love my work, I love the client group… I don’t just come to work for the money. I come to work because I really enjoy my job… It’s who I am. (Nurse 16)
Throughout interviews, discussions about nurse identities engendered passionate and animated responses. In contrast, when talking specifically about their identity as managerial leaders, discussions became less animated and more subdued. Interviewees were explicit that theirs was a ‘managerial leadership role’ (Nurse 31), and conversations about their leader identities were framed by managerially influenced discourse:
Now I’m managing staff, managing budgets, managing teams, managing services. I have to think about meeting performance targets and making sure everything runs efficiently. It’s different to nursing. (Nurse 12)
The way in which nurse managers talked about their managerial leader identity was distinct from the positive emotional language framing their nurse identity. The demands of their leader identity were reported as functional requirements of their hybrid role, while the demands of their nurse identity were described as more emotionally fulfilling:
I’d much rather be in the day room chatting to patients, being around the staff team rather than answering my phone in my room. I don’t enjoy the management stuff… I find a lot of solace in my clinical work. When things are getting on top of me I find the clinical work a welcome break. I’m still a nurse at the end of the day, that’s why I’m here. (Nurse 22)
Problematically, nurse managers reported that the demands of their leader identity could sometimes detract from behaviours they associated with their nurse identity, such as being able to prioritize caring for patients:
People expect me to prioritize things that I would rather not. I would rather be seeing the patients, but there are times when I can’t because my management responsibilities dictate that I do something, which is unfortunate… I’m not happy when that happens. (Nurse 2)
As a result, nurse managers had to accommodate the functional demands of their managerial leader identity with the demands of their emotionally significant nurse identity. Interviewees said this could often be problematic, and that they found the two identities difficult to align:
I do struggle to get my head out of being a clinician and into being a manager. Because I have to keep both heads at the moment and it’s difficult, because it is all about finance and being able to understand the processes and what targets need to be met… it doesn’t quite fit together for me as a clinician with that. It can be very difficult. (Nurse 11)
In addition to the identity conflict reported by the nurse managers, stemming from their struggle to align competing identities within their own self-concept, interviewees also said they felt concerned that they no longer enjoyed influence among others in the nursing group:
I still have close friends on the nursing side and they said people don’t tell me anything now. So I’m not as in the know as I was. (Nurse 18)
When asked to explain why they felt this was the case, nurse managers suggested that their managerial identity detracted from their ability to convince others of their identity as a desired group member, making them feel like outsiders and undermining their group leadership potential:
Your credibility isn’t quite the same with the staff group if you’re an outsider going in. The team in practice don’t allow outsiders in and when I’m out of the group it’s quite difficult to be a leader… I would say they see me as an outsider now because I’m the manager. (Nurse 13)
Nurse managers said they felt this loss of group influence could be difficult, as they attached emotional significance to their ability to construct a nurse identity. Nurse 13 (who above describes herself as an outsider) was explicit about her desire to continue to be seen by others as a ‘nurse’, and even kept a picture of herself in a nursing uniform on her office wall, seemingly to emphasize that identity to others. However, as outlined above, she said that constructing a leader identity detracted from her ability to remain an influential member of the nursing group, resulting in identity conflict and a sense of loss:
It’s been difficult for me to see the value of people like me… I question whether we can even call ourselves clinicians. I don’t know what I am any more. (Nurse 13)
The nurse managers reported a sense of identity conflict and a struggle to construct a desired group identity, triggering feelings of identity loss and confusion. Interviewees discussed their nurse identity in positive terms, while their leader identity was seen as more functional and mundane, an identity demanded by their role, rather than one which was emotionally important. In the next section we consider how the nurse managers talked about the different identity work they used in attempts to mitigate their identity conflict.
Identity work
Over the two-year data collection period, only five of the 32 nurses interviewed moved into different roles. The remaining 27 continued in their initial hybrid roles, requiring the ongoing construction of leader and nurse identities. There was little change in the identity conflict the 27 hybrid managers reported due to difficulties in accommodating two distinct identity constructions, and their concerns that they had lost some of their nurse identity. We now consider the identity work the nurse managers said they engaged in, in an attempt to deal with their identity conflict and overcome negative emotional experiences.
The first type of identity work reported by nurse managers was distancing themselves from behaviours associated with undesirable managerial leader identities. Nurse managers reported instances in which they attempted to retain nursing group legitimacy, by distancing themselves from a managerial identity, as the latter could be negatively perceived by other nurses:
How you sell something that’s going to be unpopular is a trick isn’t it. You know sometimes I play the ‘we’ve got to do this, we’ve got no choice, don’t blame me, it weren’t my idea’, you know, or we blame some manager who’s not in the room… My last line is ‘we’ve got no choice in this because these decisions are made above my head’. (Nurse 15)
This nurse manager was attempting to deflect negative reactions to managerial decisions onto other, higher-level managers, to protect his identity as a member of the nurse group, and to make clear that he did not agree with the incongruent behaviours of ‘managers’. This identity work was also reported by nurse managers who attempted to distance themselves from a manager identity by highlighting their own commitment to behaviours associated with a nurse identity, suggesting a typical ‘manager’ would not act in a similar way:
Those normal managers, they don’t want to get up at 6 in the morning and they don’t want to work Christmas Day or New Year’s Night… It’s not like that for me, it’s not about the spreadsheets and leaving by 5pm… I’m still part of the team, it’s important for them to see that. (Nurse 7)
By engaging in identity work of this type, interviewees suggested they were trying to protect their nurse identity by attempting to stop other group members ‘seeing you as management and treating you accordingly’ (Nurse 15). By distancing themselves from undesirable behaviours, which might undermine their ability to construct a desired nurse identity, nurse managers engaging in this identity work suggested they were reluctant to construct a leader identity, but keen to influence the group by virtue of their group membership.
The second type of identity work discussed by nurse managers was their attempts to construct a leader identity by framing it in language associated with their nurse identity. This was indicated by a return to the animated, positive emotional discussions, which characterized nursing identity constructions:
[The ward] is like my baby actually… I’m so passionate about this place and I think that what makes me a good leader is my passion for this place and for nursing… it’s more than leadership. (Nurse 10)
Rather than attempting to construct a managerially framed leader identity, nurse managers drew on dialogue reflective of the way they talked about their nurse identity. In another example of this identity work, a nurse manager described substituting behaviours associated with their nurse identity, such as caring for patients, into their leader identity:
I suppose I always thought I’d never be able to move out of clinical practice, that was why I came into nursing and the main reason for getting up every morning… but with the staff I manage it’s important for me to keep them well and motivated for the service they provide. I’ve swapped service users for staff. So that need that I have has been superseded by staff… I still care for people but they happen to be staff and not people who use the service. (Nurse 14)
Nurse managers engaging in this type of identity work suggested they did not try to distance themselves from a leader identity, but that their continued commitment to a nurse identity influenced their leader behaviour, arguably making them better leaders:
I would find it hard to make the decisions that I make now around moving money, around staffing, resources, without my clinical knowledge and background… because I’m a nurse, that has an influence on the way on the way I act as a leader. (Nurse 16)
By engaging in identity work to frame their leader identity in emotional language associated with nursing, nurse managers were attempting to overcome some of the identity conflict associated with the transition towards a leader identity. Rather than trying to accommodate managerial leader identity demands, they relied on their continuing emotional attachment to their nurse identity to guide the way they constructed, and viewed themselves, as professional nursing leaders.
Despite the potential success of the two types of identity work outlined above at overcoming identity conflict, the 27 nurses remaining in hybrid roles continued to report negative emotions. While they described how identity work enabled them, as individuals, to accommodate conflicting identities, they still reported feeling a loss of nursing group influence. The extent to which nurse managers said they felt they could persuade others of their continuing identity as a nurse was limited:
I think they probably view me as someone who used to be a nurse. I do struggle with that sometimes… I’ve always taken pride in being a nurse. I’ve always liked that that’s part of my identity. Now I’d hate to think I’m not a nurse… it upsets me that the others don’t see me like that. (Nurse 14)
Overall, nurse managers in hybrid positions suggested the identity work they engaged in enabled them to overcome some of the identity conflict they experienced as individuals, but said it did not help them overcome their feeling that they had lost an emotionally important group membership. They still desired to be part of the nursing group, and yet did not feel they were able to convince others of that identity due to the demands of their leader identity, even when they attempted to frame the leader identity as professionally, rather than managerially, defined.
Not all nurse managers, however, reported the same ongoing emotional distress in response to a perceived loss of group influence. As mentioned above, five of the 32 nurses had moved into different roles by the end of the study. These individuals had moved away from hybrid roles into senior levels of management. In these roles they no longer had any clinical responsibilities, and were positioned within the general management structure of the organization. When asked about why they had moved into these positions, and any conflict they felt when attempting to retain their nurse identity, these five nurse managers said they had moved away from a desire to construct a nurse identity:
I really didn’t want to let go of my nurse identity because it’s quite rewarding… After a year of trying to do that I realized I really couldn’t do that and run a team at the same time because it pulls you in too many directions… I’m not a nurse any more. I used to be a nurse but now I’m a manager and I enjoy that. (Nurse 29)
The five nurse managers said they no longer felt conflicted about their loss of group membership, and suggested they were now committed to a more managerially framed leader identity, rather than one framed by their nurse identity:
I was limited when I was a nurse manager… but now I step into a managerial leadership role and an organizational one, which puts me at a distinct advantage because I work in several layers of the organization…. I’m not trying to influence just nurses any more, it’s a more strategic thing. (Nurse 31)
By eschewing emotional attachments to the construction of a desired nurse identity, these five nurse managers reported that they felt less conflicted and experienced less emotional distress than when they attempted to construct a leader identity alongside a nurse identity:
Yes I’m definitely happy here, I wouldn’t want to go back to being a ward manager, it pulls you apart… I’m able to make a difference now, I can influence things. (Nurse 18)
The five nurse managers who had moved from hybrid roles into general management roles reported that they no longer experienced the negative emotions characterizing the narratives from other nurse managers. They attributed this to the sense that they no longer held emotional connections with their ability to construct a desired nurse identity, and have others perceive them as a member of the nurse group. While the identity work reported by the other 27 nurse managers was successful in overcoming individual identity conflict, but limited in overcoming negative emotions arising from a loss of professional identity, the five nurses who eschewed emotional attachments to their nurse identity reported less identity conflict or emotional distress.
Discussion
In this paper we have explored how nurses in hybrid positions discussed the identity work they employed to overcome the identity conflict, and potentially negative emotional experiences, associated with the construction of a managerial leader identity. In doing so, we highlighted how incongruence between a desired professional group identity and a managerially framed leader identity can influence the emotional experience of constructing a leader identity. We now consider our findings in the context of existing research, offering further development of our understanding of the identity challenges faced by hybrid professionals.
Consistent with extant literature, nurse managers in our study associated positive emotions with their professional group membership. In interviews, nurse managers used passionate and emotive language when discussing nursing, with most nurses saying that they were keen to continue to be seen by others as a member of the profession, highlighting their emotional identification with a desired nursing identity (Fotaki, 2010; Thornborrow & Brown, 2009). In contrast, nurse managers discussed their identity as managerial leaders in more mundane ways, with less positive emotional associations.
Nurse managers reported that the biggest source of their identity conflict was their perceived loss of group influence, and the feeling that they were no longer able to construct a desired nurse identity. To deal with this identity conflict, nurse managers discussed three types of identity work: attempting to reaffirm their professional identity and gain influence by distancing from managerial leader identity demands; attempting to retain professional influence by framing their leader identity in emotional language associated with a nurse identity; and finally, eschewing their emotional attachment to the construction of a desired nurse identity, moving towards a desired managerial leader identity. We now consider each of these types of identity work in turn.
All 32 of the nurse managers taking part in the study said they initially struggled to align an emotionally important nurse identity with a functionally demanded leader identity, triggering identity conflict. One way in which many of the nurse managers attempted to cope with this conflict was by distancing themselves from managerial leader behaviours, which were perceived as undermining their ability to construct a desired nurse identity. Distancing from negative identity elements, which Petriglieri and Stein (2012) conceptualize as distancing from ‘unwanted selves’, should develop the potential for individuals to move between different identity constructions, as they can reaffirm their group identity, and protect their group influence, by distancing themselves from a managerial identity. In this way, competing identities can remain in flux, enabling individuals to function adequately in a hybrid role, while remaining a member of the professional group (Clarke et al., 2009; Sveningsson & Alvesson, 2003). These initial findings resonate with the conclusions of Blomgren (2003), who suggested nurse managers respond to identity conflict by either embracing or rejecting managerial associations. The nurse managers in our paper who said they distanced themselves from managerial elements of their leader identity, which they perceived to be negative, could be seen as rejecting managerial associations in a similar way.
We suggest the second type of identity work we explored is an extension of Blomgren’s typology, as we found examples of nurse managers who did not reject their managerial associations, but framed their leader identity through emotive language associated with a nurse identity. These nurse managers were not embracing or rejecting a managerial leader identity, rather they were attempting to reframe the managerial identity in way that enabled them to accommodate competing identity demands. Ibarra (1999) suggests that individuals who attempt to transfer the behaviour associated with previous identities into the development of a new identity are better able to accommodate role demands and overcome emotional distress, as they feel they are more ‘authentic’ to themselves. Our initial findings also support the arguments of Bolton (2001) that nurses are adept at taking on different identities in multiple contexts, avoiding identity conflict. However, despite the potential for the identity work discussed in overcoming identity conflict, when we consider our findings further they call into question the conclusions of Ibarra (1999) and Bolton (2001).
While the two types of identity work described above were used to mitigate the individual identity conflict stemming from competing identity constructions, nurse managers continued to experience negative emotions as they reported a sense that they had lost some of their desired group identity and, consequentially, had lost group influence. As such, we develop the insights of Ibarra (1999) and Bolton (2001), by illustrating that nurse managers engaging in these types of identity work continue to talk about their experience of negative emotions, due to a perception that an association with a leader identity undermines their nurse identity. While nurse managers may be adept at overcoming individual identity conflict (in line with Bolton, 2001), we suggest they were less adept at overcoming the emotional distress associated with their perceived loss of an emotionally important, desired group identity.
The finding that emotional distress is linked to a continuing commitment to a desired professional group identity is illuminated further when we consider the insights offered from five nurse managers who moved away from hybrid positions over the course of the study. Although a small group, these nurse managers (now general managers) had moved into strategic management positions, and suggested they were able to resolve their identity conflict and overcome negative emotional experiences because they were no longer emotionally attached to the construction of a desired nurse identity. As a result, the nurse managers said they no longer experienced negative emotions when they felt others did not perceive them as nurses. In other words, not only are this group embracing their managerial leader identity (as suggested by Blomgren, 2003), they are distancing themselves from an emotional attachment to their nurse identity.
These findings build on the work of Srinivas (2013), who considered a subordinate individual confronted with similar emotional issues of identity conflict, moving into a managerial role requiring identity transition. Like us, he suggested negative emotions arose due to the incongruence between an emotionally important social identity (as an Indian man) and a managerial leadership identity (which required him to conform to a more colonial, British identity). Srinivas suggests that subordinate individuals are only able to overcome the identity conflict associated with the development of an incongruent leader identity when they are able ‘to analyze, to remain detached, to eschew idealism for practicality’ (Srinivas, 2013, p. 1665). In other words, it is only by disassociating from an emotional attachment to the group identity that nurse managers were able to overcome emotional distress. That is not to say that these five managers dissociated themselves from their past experience as a nurse, rather that they no longer associated their ‘true self’ (Ibarra 1999) with an ability to construct a desired nurse identity.
The finding that nurse managers said they were only able to resolve issues of identity conflict and emotional distress when they were emotionally detached from the professional group offers insight into the ongoing identity struggles faced by professional hybrids (Kippist & Fitzgerald, 2009; Noordegraaf & De Wit, 2012; Thomas & Linstead, 2002). Problematically, for most professional hybrids, emotional detachment from a social group will not be beneficial, as it will undermine the ability of professionals to influence others in the group, negatively influencing their ability to lead (Tee et al., 2013). Therefore, we extend the work of Srinivas (2013) by presenting a context in which individuals attempting to overcome identity conflict are not able to emotionally detach from their social identity. The individual discussed by Srinivas (2013) was able to emotionally distance himself from a social group identity, as he was no longer attempting to influence others in that social group. Similarly, the five nurse managers in this paper who had moved into the general management structure were no longer attempting to influence nurses, but were now leaders within the wider organization. Subsequently, one could argue that these individuals were only able to overcome the identity challenges associated with professional hybrids when they moved into more senior positions, as they were no longer required to accommodate two incongruent identities, and were able to emotionally detach from the professional group. We suggest that professional hybrids need to retain social group influence by demonstrating to other group members an ongoing emotional attachment to their group identity, and are unable to eschew this emotional attachment until they are no longer in a role requiring them to influence that social group.
While the fragility of hybrid identities is often noted (Harding et al., 2014; Thomas & Linstead, 2002), existing research suggests that hybrids are ultimately able to overcome identity conflict, relying on emotionally important group identities to legitimize their changing identity to both themselves and other group members (Kippist & Fitzgerald, 2009; Noordegraaf & De Wit, 2012; Sveningsson & Alvesson, 2003). In our paper, we have illustrated how relying on an emotionally important group identity does not mitigate negative emotions and identity conflict, but actually perpetuates a negative emotional experience. While the nurse managers suggested identity work could mitigate individual-level identity conflict, the negative emotions associated with a loss of group membership could only be resolved by eschewing emotional attachments to the professional group. Ibarra and Barbulescu (2010) argue that an individual can only firmly inhabit a role when they are able to resolve the conflicts and contradictions between their identity narratives. We suggest that nurse managers will struggle to resolve their identity conflicts, as they are required to remain emotionally attached to their group membership for leader influence (Tee et al., 2013), yet to be emotionally detached from their group membership to overcome the identity conflict associated with their role. Previous work suggests that ongoing desired group identities will facilitate the construction of leader identities by enhancing group influence (Thornborrow & Brown, 2009; Wright et al., 2012). In this paper, we have shown how desired group identities can undermine the construction of leader identities for professional hybrids.
Conclusions and Implications
In this paper we have explored the emotional challenges faced by professional hybrids attempting to construct a managerial leader identity incongruent with their professional group identity. While existing work has assumed that individuals accommodate desired leader and group identities, we considered the case of nurse managers, who have not traditionally been seen as leaders. In doing so, we have addressed calls for greater exploration of the identity work used by low-status groups when constructing leader identities (Srinivas, 2013).
Our findings question the assumptions of existing research into professional hybrids, which suggests that desired leader and group identities can always be aligned, or that incongruent identities can be accommodated without causing emotional distress (Clarke et al., 2009; Noordegraaf and De Wit, 2012). While previous work suggests that desired group identities will facilitate the construction of leader identities by enhancing group influence (Thornborrow and Brown, 2009), in this paper we have shown how desired group identities can undermine the construction of leader identities. In doing so, we offer insight into professional hybrids as a group occupying a structural position which exposes them to negative emotions, as they remain emotionally attached to their group membership to ensure leader influence (Tee et al., 2013), and are subsequently unable to achieve the emotional detachment required to overcome identity conflict (Srinivas, 2013). By drawing on the emotional influence of desired identity constructions, our findings build on existing work exploring the ‘fragile’ nature of hybrid identity constructions, and the identity conflicts widely reported by professional hybrids (Harding et al., 2014; Kippist and Fitzgerald, 2009; Thomas and Linstead, 2002).
We also extend our understanding of identity work processes by considering how identity work may actually exacerbate feelings of identity conflict among individuals, rather than facilitating individuals to overcome conflict. Existing work assumes that when identity work is guided by behaviour associated with previous identities, individuals will be better able to overcome emotional distress and move between competing identity constructions (Bolton, 2001; Ibarra, 1999; Sveningsson and Alvesson, 2003; Wright et al., 2012). We conclude from our work that this may be the case when overcoming individual identity conflict, but when identity work is guided by a group identity that does not support the construction of a leader identity, it may enhance, rather than overcome, emotional distress.
Our conclusion that those emotionally committed to a professional group identity will experience negative emotions, while those who are able to adapt their identity are able to overcome identity conflict, offers further avenues for research. In particular, more work is needed into the way individuals are able to emotionally detach themselves from their ability to construct a desired social group identity. Does the emotional detachment occur before, or after, they move into different roles? Is it the cause or the result of the transition? More work is needed to understand the process through which emotional detachment occurs, and to explore whether this would be beneficial, or detrimental, to the identity constructions of professional hybrids.
As with any study exploring issues of identity, we acknowledge the limitations of our findings. Interviews were conducted over a two-year period within one NHS organization, and can only offer a temporal snapshot of the issues faced by individuals in one setting. Further to this, despite considering the findings in a reflexive manner, our interpretation of the nurse manager narratives may be different to conclusions drawn by other researchers. We acknowledge that our conclusions only offer partial insight into the phenomenon at hand, and should be viewed as one part of the identity puzzle, rather than an ‘answer’ to issues of identity.
While our empirical work focused on individuals from a nurse background, we suggest that our findings can be applied to other professionalised contexts, particularly those where a professional group identity may conflict with a managerial leader identity. In addition to professional groups whose identity is associated with subordination, our work has implications for other cultural groups who may find identity alignment with managerial leadership identities difficult, based on gender (Fotaki, 2013) or cultural minorities (Srinivas, 2013). Furthermore, while nurses may represent an extreme case, we suggest hybrids in any context that are emotionally connected to the group identity may experience a similar conflict as they undergo identity transitions. As such, our work can offer insight into the emotional experience of any leader identity constructions (Tee et al., 2013), as well as extending our understanding of the experiences of more traditional professions, such as doctors (Llewellyn, 2001) or academics (Fotaki, 2013).
Footnotes
Appendix
Funding
This research was funded by an Economic and Social Research Council CASE award. The views expressed are those of the authors and not of the ESRC.