
Abstract
Caregivers of children/youth with emotional and behavioral disorders often can experience significant strain associated with the day-to-day care of their children, and reducing strain can bring tremendous advantages to children, caregivers, and families. This study examines several predictors of caregiver strain hypothesized to be related to caring for children with emotional and behavioral disorders. Specifically, children’s symptoms, child and caregiver demographics, caregiver mental health, and caregiver relationship to child were examined to better understand both objective and subjective strain among a sample of families participating in a system of care in southeast Indiana. Regression analyses demonstrated that children’s externalizing symptoms are the strongest predictor for both objective strain and subjective strain. Moreover, caregivers who had experienced mental health issues reported higher levels of subjective externalized strain; biological parents tend to experience higher subjective internalized strain than other relative caregivers do. Implications for practitioners, caregivers, and future research are also discussed.
As concerns about quality of life for children and youth with disabilities have drawn increased attention over the past several decades, focus has extended to better supporting their families. Starting with the deinstitutionalization movement in the 1970s, many people with disabilities moved back to their communities, and family members took additional responsibility of caring for their children with significant needs. Subsequently, the provision of services and supports for family members has become an important component of community-based services for children/youth with disabilities, and its success appears also to depend, at least in part, on our ability to reduce associated caregiver strain (Bernheim, 1990; Brannan, Heflinger, & Bickman, 1997). In the social services field, systems of care—an organizational framework guiding community-based service delivery for persons with emotional and behavioral disorders (EBDs)—have emphasized the “family-driven” principle—that services and supports should be determined by caregivers and tailored for the “whole” family rather than just the individual (Hunter & Friesen, 1996; Stroul & Friedman, 1986). Caregiver strain is often an important component used in evaluations of programs for persons with EBDs (Abidin, 1992; Bernheim, 1990; Webster-Stratton, 1990).
Researchers have documented that the caregivers of children/youth with EBDs often experience significant strain associated with caring for young people with these challenges (Angold et al., 1998; Brannan & Heflinger, 2001; Farmer, Burns, Angold, & Costello, 1997; Huang et al., 2005; Meltzer, Ford, Goodman, & Vostanis, 2011; Taylor-Richardson, Heflinger, & Brown, 2006). This strain has been defined as the “demands, responsibilities, difficulties, and negative psychic consequences of caring for relatives with special needs” (Brannan et al., 1997, p. 212). This includes the perceptions of strain that is directly related to caring for their children/youth with EBDs and does not include other stressful life events that the family experiences, such as scarce resources. In systems of care, caregivers are expected to shape and drive the care their children and family receives and to meaningfully involve themselves in system/service development and even policy making in the community (Stroul & Friedman, 1986). However, increased strain can create difficulties for caregivers to participate in treatment and services with their children, communicate/coordinate effectively with service agencies, or make appropriate choices with and for their children, any of which might affect children’s use of mental health services and subsequent clinical outcomes (Brannan et al., 1997; Brannan, Heflinger, & Foster, 2003; Brannan & Heflinger, 2006; Friesen & Koroloff, 1990; Kazdin, 1989; Kazdin & Whitley, 2003).
Caregiver strain has been found to influence children’s services utilization, with some researchers indicating that when caregivers realize the strain associated with their children’s symptomology, they are more likely to access mental health services. Moreover, children’s severity and symptom type appeared to have relatively little effect on service utilization when parental perceptions of strain are taken into account (Angold et al., 1998; Farmer et al., 1997; Garland, Aarons, & Brown, 2003). In other words, caregiver strain levels, regardless of the type or amount of challenges exhibited by youth, accounted for decisions to seek services. Furthermore, some researchers have suggested that caregivers who report lower levels of strain are more likely to keep their children at home/in the community rather than use psychiatric hospitals, medications, and residential placements (Bickman, Foster, & Lambert, 1996; Brannan & Heflinger, 2006; Brannan et al., 2003; Cook, Heflinger, & Hoven, 2004; Foster, Saunders, & Summerfelt, 1996). This finding provides a compelling rationale for reducing caregiver strain as a component of service provisions for children/youth with EBDs.
Much of the existing research on caregiver strain has focused on the relationship between caregiver’s strain and children’s symptomology. It is well documented that the overall severity of a child’s emotional and behavioral symptoms increases caregiver strain and, further, that externalizing and internalizing behaviors predict caregiver strain to different degrees (Accurso, Garland, Haine-Schlagel, Brookman-Frazee, & Baker-Ericzen, 2015; Angold et al., 1998; Bussing, Gary, et al., 2003; McDonald, Gregoire, Poertner, & Early, 1997; Sales, Greeno, Shear, & Anderson, 2004). While these studies used a global measure of strain, other researchers have noted that caregiver strain can be divided into different dimensions, each having its own unique correlates. Brannan et al. (1997) conceptualized caregiver strain in two broad dimensions, objective strain and subjective strain, which can be divided into both subjective internalized strain and subjective externalized strain. Objective strain refers to the observable disruptions related to taking care of a child/youth with disabilities, such as workplace interruptions, challenging family relationships, disruptions of social activities, and financial pressure. Subjective internalized strain measures how caregivers feel about themselves, relative to their child’s problems, including emotions such as sadness, worry, guilt, and exhaustion. Subjective externalized strain examines caregiver feelings toward their child, such as embarrassment, anger, and resentment (Brannan et al., 1997).
Bussing, Gary, et al. (2003) and Bussing, Zima, et al. (2003) reported that having a child with externalizing symptoms such as oppositional defiant disorder predicted higher levels of caregiver strain in all three dimensions (objective, subjective internalizing, subjective externalizing). Brannan & Heflinger (2006) also found that externalizing symptoms were the strongest predictor for all three dimensions of caregiver strain, while internalizing symptoms significantly predicted subjective internalized and externalized strain. More recently, Vaughan, Feinn, Bernard, Brereton, and Kaufman (2012) examined the impact of a child’s co-occurring symptoms on caregiver strain, with results indicating that caregivers of children with symptoms in both externalizing and internalizing domains experienced more caregiver strain when compared to caregivers of children with symptoms in only one domain (Vaughan et al., 2012). Overall, these results suggest that different configurations of symptomology may predict different levels and dimensions of caregiver strain.
Children’s demographic information, such as gender and age, and caregivers’ demographic information, including gender, age, race, education, employment status, and income, have been examined as potentially contributing to caregiver strain (Accurso et al., 2015; Brannan & Heflinger 2006; Bussing, Gary, et al., 2003, Bussing, Zima, et al., 2003; Heflinger & Taylor-Richardson, 2004; Kang, Brannan, & Heflinger, 2005; McDonald et al., 1997; McCabe, Yeh, Lau, Garland, &Hough, 2003; Sales et al., 2004). However, findings about the relationships between at least some demographic factors and caregiver strain have not been conclusive. For instance, while some researchers have reported a positive relationship between caregiver subjective externalized strain and children’s age (Brannan & Heflinger, 2006; Heflinger & Taylor-Richardson, 2004), others reported no relationships between age and any strain dimension (Bussing, Gary, et al., 2003, Bussing, Zima, et al., 2003). Bussing, Gary, et al. (2003) and Bussing, Zima, et al. (2003) found that caregiver strain ratings were higher for boys than for girls across three dimensions; however, this was not indicated in other studies (e.g., Brannan & Heflinger, 2006; Heflinger & Taylor-Richardson, 2004). Researchers have also found that African American caregivers report less strain than their White counterparts (Brannan & Heflinger, 2006; Pruchno, 1999). Caregivers’ educational level, employment status, and household income also have been found in some studies to be associated with caregiver strain (McDonald et al., 1997, Kang et al., 2005), whereas others reported finding no association between income and caregiver strain (Brannan & Heflinger, 2006; Sales et al., 2004).
It is possible that different measurement tools contribute to some of the observed variance across studies, and it is also likely that the different samples and contexts used across studies account for the mixed findings reported in the literature. For instance, the children included in Bussing, Gary, et al. (2003) and Bussing, Zima, et al. (2003) were younger than the participants in some of the other studies (e.g., Brannan & Heflinger, 2006) and researchers have indicated that caregiver strain increases during the teen years. This might explain why relationships between children’s age and caregiver strain were not uncovered in Bussing’s study. Additionally, Bussing, Zima, et al.’s study focused on children with or at risk for attention deficit/hyperactivity disorder. Since this group tends to have higher percentages of males and more externalizing than internalizing behaviors, this might explain why the caregivers of boys report more strain than caregivers of girls.
Researchers have also attempted to clarify the relationship between caregiver strain and psychological distress (Brannan et al., 1997; Brannan & Heflinger, 2001; Sales et al., 2004), suggesting that these two constructs are positively correlated with a healthier mental health status associated with less strain. In Heflinger and Taylor-Richardson’s (2004) study, results indicated that poorer mental health status predicted increased caregiver strain in all dimensions. In addition, caregivers’ relationship to the children has been studied, with evidence suggesting that relative caregivers such as grandparents, aunts, and siblings experience similar levels of strain as do biological parents. One noted exception was that parent caregivers reported more subjective internalized strain than did other relative caregivers (Heflinger & Taylor-Richardson, 2004).
Because caregivers can experience different levels of strain across three known dimensions, understanding factors that are specifically associated with each dimension could assist practitioners to more quickly and effectively support caregivers experiencing high levels of strain. Indeed, providing such supports to caregivers might also reduce the use of more restrictive placements and help children/youth remain in their communities. Thus, the purpose of this study was to examine predictors of caregiver strain hypothesized to be related to caring for children with EBDs, and investigate the extent to which these factors contribute to measured caregiver strain. Specifically, children’s symptom levels in both internalizing and externalizing behavior, children’s gender and age, as well as caregiver gender, age, education, annual household income, mental health status, and their relationship to the children were all examined to understand both objective and subjective strain among a sample of families participating in a system of care in southeast Indiana.
Based on previous research, it was hypothesized that internalizing and externalizing behavior problems among youth who were participating in the systems of care would predict divergent patterns in each domain of caregiver strain, and that externalizing behaviors would more greatly affect caregiver strain. Given the inconsistencies in the existing research base, no prior assumptions were made about the relationships between caregiver strain and other demographic factors. Since few studies have included both caregivers’ mental health state and their relationship to children, these variables were included in our study. This study adds to the current body of knowledge by exploring a specific sample of young people served in a system of care to understand how the following variables predicted each dimension of strain: (a) caregivers’ mental health status and their relationship to their children and (b) demographics of child and caregiver.
Method
Data for these analyses were collected from 2010 through 2014 as part of the federally required Child and Family Longitudinal Outcome Study of the One Community One Family (OCOF) system of care partnership in southeastern Indiana. Partially funded from 2008 to 2014 by the Substance Abuse and Mental Health Services Administration and serving eight counties in southeastern Indiana, the OCOF partnership works to address the challenges of implementing community-level collaboration designed to prevent and improve outcomes for children and youth with or at risk for EBDs and their families. Approximately one-third of the youth served by OCOF had been diagnosed with a conduct disorder (30%); this was followed by youth with mood disorders (20%), attention deficit/hyperactivity disorder (19%), and anxiety disorders (14%). By bringing together a spectrum of mental health, social supports, and other necessary services to participants once they enroll in wraparound services (Community Mental Health Services, n.d.), families become part of a process that includes a strengths-based, family-driven collaboration among youth, mental health, child welfare, juvenile justice, schools, residential providers, foster parents, community coalitions, social service agencies, and other child-serving entities (J. A. Anderson, Ergulec, Cornell, Ruschman, & Min, 2016).
The outcome study was designed to longitudinally investigate the extent to which clinical changes of participating youth and their caregivers were observed over time in the wraparound program. Young people and their families who receive wrap services from OCOF were informed about and invited to participate in this study. Outcome data on child clinical and functional status (e.g., symptomology, diagnosis, and social functioning) and family life (e.g., family functioning, caregiver strain, and material resources) were collected by the OCOF evaluation team, within 30 days of the child’s entry into OCOF and at 6-month intervals up to 24 months postenrollment. Only families who completed the interview at intake were considered to be participants in the longitudinal study. The data used for this current study came from the first wave. The participant recruitment and data collection procedures complied with established ethical standards, and were approved by the university’s institutional review board.
Sample
Data presented in this study were selected from 161 families who participated in the longitudinal study of OCOF (n.d.). Of 161 total participants, 52 youths—30 younger than 6 years and 22 older than 18—were excluded from these analyses, since two primary instruments (Caregiver Strain Questionnaire [CGSQ] and Child Behavior Checklist [CBCL]) used in this study focused only on school-aged children, ages 6 to 18. Of the remaining 109 participants, several families were excluded from the analyses because of missing values on one or more of the primary variables: caregiver strain (n = 7), child symptomology (n = 6), caregiver age (n = 11), caregiver education (n = 11), household income (n = 13), and caregiver mental health status (n = 2). After removing cases with missing values in the study variables (15.6%), 92 families with complete data were included in the study. Independent sample t tests were conducted to check the degree of difference between cases with and without missing values. Results suggested few differences between families with and without missing information, with only one statistically significant difference in household income observed at .001 levels. Families who were missing in household income variable (M = 1.75, SD = 0.30) reported lower caregiver subjective externalized strain than families who were not (M = 2.22, SD = 0.82).
Table 1 presents the study variables for the 92 families who had complete data available for analyses. Almost all the participants were Caucasian. Approximately 60% (n = 55) of the youth were boys, and ages ranged from 6 to 18 (M = 11.79, SD = 3.19). Caregivers ranged in age from 26 to 71 years (M = 41.67, SD = 10.88), and 91% of the caregivers were female. With regard to education background, 25% (n = 23) of caregivers had not completed high school, 34% (n = 31) had a high school diploma or GED, and 41% (n = 38) had a postsecondary degree. The average household annual income was calculated as 4.39, indicating the income range was between $15,000 and $24,999. Twenty-eight percent (n = 26) of caregivers reported having mental health issues. Caregiver relationships to the focal child included biological parent (71%), grandparent (13%), foster parent (7%), aunt or uncle (5%), and other (4%).
Sample Descriptive Statistics (N = 92).
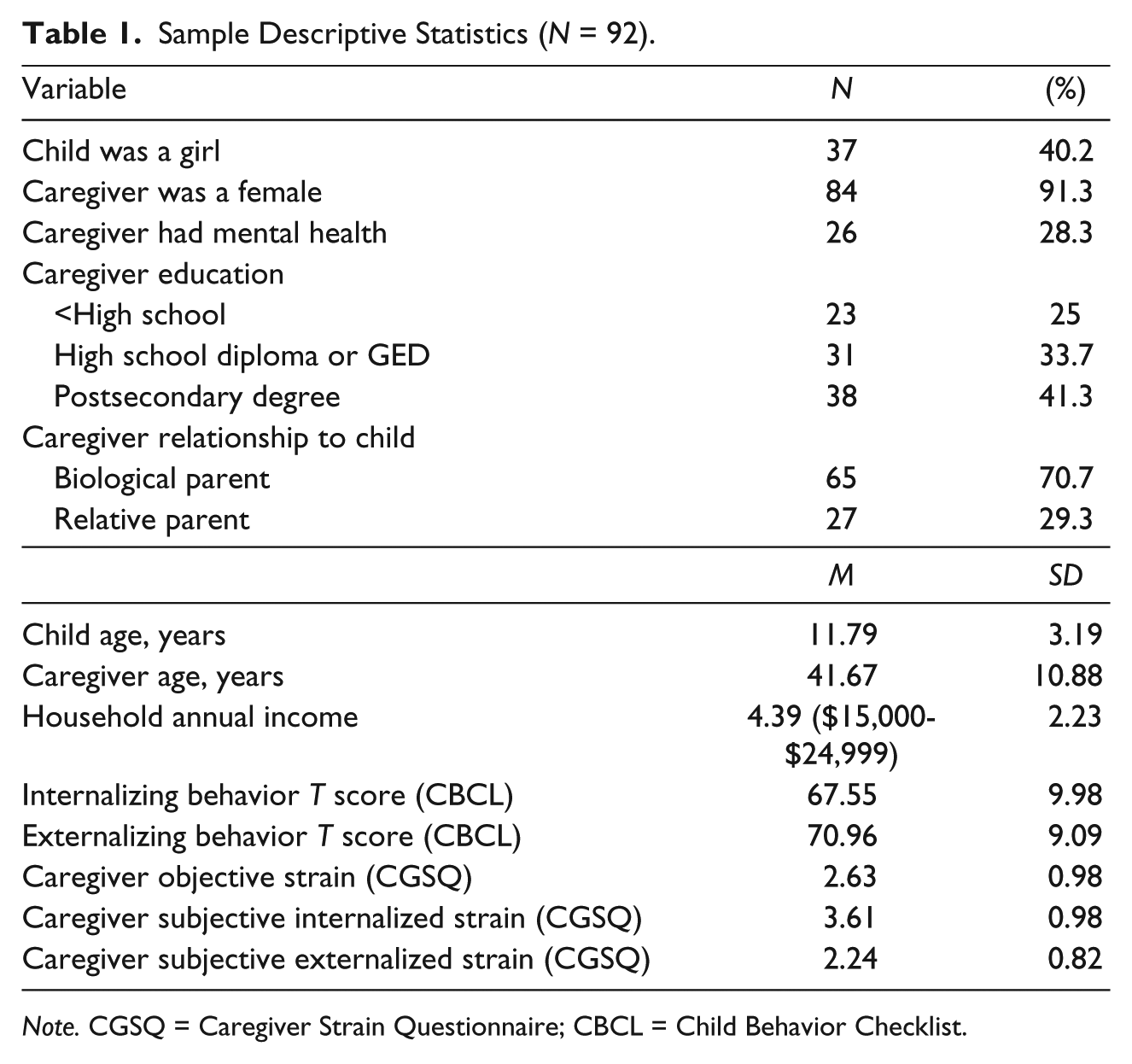
Note. CGSQ = Caregiver Strain Questionnaire; CBCL = Child Behavior Checklist.
Instruments
Caregiver Strain
Caregiver strain was measured by the CGSQ (Brannan et al., 1997), a self-report instrument that was used to access strains related to caring for a child/youth with EBDs. The questionnaire consists of three subscales: Objective Strain (e.g., interruption of personal life, financial strain, discordant family relationship), Subjective Internalized Strain (e.g., worry, guilt), and Subjective Externalized Strain (e.g., anger, embarrassment). The CGSQ contains 21 items and asks caregivers, “In the past 6 months, how much of a problem was the following?” Caregivers responded to each item on a 5-point scale: not at all (1), a little (2), somewhat (3), quite a bit (4), and very much (5). Subscale scores are the mean score of the items corresponding to a given subscale, with higher scores indicating greater caregiver strain. Scores ranged from 1 to 5. Adequate internal consistency (Cronbach’s α coefficient ranging from .74 to .93), reliability (total score Cronbach α coefficient = .93), and construct validity have been documented for the CGSQ in multiple studies (Brannan et al., 1997; Brannan & Heflinger, 2001; Kang et al., 2005; Taylor-Richardson et al., 2006). For the participants enrolled in OCOF, average caregiver objective strain, subjective internalized strain, and subjective externalized strain were 2.63 (SD = 0.98), 3.61 (SD = 0.98), and 2.24 (SD = 0.82), respectively.
Child Symptomology
Child internalizing and externalizing symptoms were assessed by the CBCL 6-18 (Achenbach & Rescorla, 2001). The CBCL provided a caregiver report of behavior and emotional problems among youths, ages 6 to 18. The CBCL describes 113 problem behaviors, and caregiver responded to each item on a 3-point scale: not true (0), somewhat or sometimes true (1), and very true or often true (2). Two broad syndrome subscales: internalizing (e.g., anxious/depressed, withdrawn/depressed, somatic complaints), externalizing (e.g., rule-breaking behavior, aggressive behavior) were used in the analysis. The syndrome scores were calculated by summing the items within each subscale and then converting the raw scores into standard T scores by using scouring programs developed by the authors. Higher scores indicate more severe problem behaviors. The CBCL has been widely used in children’s mental health services, and adequate internal consistency and reliability have been demonstrated. The internal consistency α coefficient is .90 for the internalizing scale and .94 for the externalizing scale, and the reliability is .91 for the internalizing scale and .92 for the externalizing scale (Achenbach & Rescorla, 2001). For the participants in this current study, average internalizing and externalizing behavior T scores were 67.55 (SD = 9.98) and 70.96 (SD = 9.09), respectively, which were both above the clinical cutoff of 64 (Achenbach & Rescorla, 2001).
Child and Caregiver Demographics
The Enrollment and Demographic Information Form was used to collect information related to demographics, diagnosis, and enrollment at baseline on all children and youth receiving services from the OCOF. Child/youth’s gender and age were collected in this form, with gender as a categorical variable and age (in years) as a continuous variable. The Caregiver Information Questionnaire–Revised was used to collect information about primary caregivers (i.e., demographics, family composition, and child’s/youth’s service use history) to whom the evaluation instruments were administered at baseline and every 6 months thereafter. A primary caregiver refers to the person who lives with the child and provides a majority of the child’s day-to-day care-giving. Caregivers’ gender, age, highest level of education, annual household income, and relationship to the children were collected. Caregiver gender was coded as a categorical variable, and age as a continuous variable. Caregivers’ education was entered as a continuous variable, with 0 for kindergarten and 18 for doctoral degree. The annual household income was coded as a continuous variable, with 1 indicating less than $5,000, and 10 indicating $100,000 and more. Based on the participants’ response about their caregiver role, all primary caregivers were relatives in the family household environment; there were no staff as caregivers in this study. Their relationship to the child included biological parent, adoptive parent, foster parent, grandparent, sibling, aunt, or uncle. Caregiver relationship to the child was coded as a categorical variable, with 1 for biological parents and 2 for other relative caregiver.
Caregiver Mental Health Status
Caregiver mental health status was collected in the Enrollment and Demographic Information Form. The question, “What were the problems leading to (child’s name) being referred for services?” is a multiple-choice question. The response options include maternal/paternal/ caregiver mental health and maternal/paternal/caregiver substance abuse/use. If the caregiver did not choose any of the mental health status response options, 0 was assigned to indicate that their mental health was not a reason for the child’s referral for services. On the other hand, if the respondent chose any of the above options, additional information, including caregiver gender and relationship to the child, was examined to better understand whether the primary caregivers’ mental health issues were associated with their child’s referral to the system of care.
Specific coding procedures were used to ascertain whether each of the respondents in this study had reported to be experiencing mental health problems or using drugs. Under this condition, two different scenarios were possible: (1) Biological parent: If the caregiver was a biological mother and she chose maternal mental health or maternal substance abuse or both, she was coded as 1; otherwise, she was coded as 0. If the caregiver was a biological father and he chose paternal mental health-related options, he was coded as 1 regardless of the mother’s mental health status; otherwise, he was coded as 0. (2) Other caregivers (i.e., foster parent, grandparent, aunt, or uncle): If the caregiver was a relative caregiver rather than a biological parent, the participant was coded as 1 only if caregiver mental health or caregiver substance option was selected; otherwise, the caregiver was coded as 0. In the second scenario, since the biological parent was not the primary caregiver, maternal or paternal mental health status was not relevant in this case. This process ensured that the researchers understood whether or not the primary caregiver for each young person in the study reported having mental health challenges.
Data Analysis
Prior to conducting regression analyses, preliminary data analyses were performed to check appropriate assumptions. All the continuous variables roughly met the normality assumption, and no evidence of nonlinear relationships among variables was observed. Although some low to medium correlations were found between some independent variables at .01 level, such as child age and caregiver age (r = .356) and internalizing and externalizing behavior T scores (r = .457), the authors chose to keep these variables in the model because these correlations were reasonable and such that magnitudes would not significantly influence the model. In addition, no evidence of multicollinearity among these variables was observed. Next, three separate multiple linear regression analyses were conducted to examine to what extent this set of predictors (i.e., children’s internalizing and externalizing behavior, child age, child gender, caregiver gender, caregiver age, caregiver education, annual household income, caregiver mental health status, and caregiver relationship to the child) accounted for objective and both types of subjective strain. Child gender, caregiver gender, caregiver mental health status, and caregiver relationship to the child were included in the models as categorical variables; child externalizing and internalizing levels, child age, caregiver age, caregiver education, and annual household income were entered as continuous variables.
Results
Caregiver Objective Strain
The model in predicting caregiver objective strain was statistically significant, F(10, 81) = 9.075, p < .001, with approximately 47% of the variance of objective strain was accounted for by this set of predictors (R2 = .528, adjusted R2 = .470). The regression coefficient for externalizing symptom was statistically significant, t(81) = 6.704, p < .001, indicating that more problems with child externalizing behaviors associated with increases in objective caregiver strain, even after controlling for other variables in the analysis. The regression coefficients for other predictors in this model were not significant at .05 level (see Table 2).
Summary of Multiple Regression Analysis for Variables Predicting Caregiver Strain (N = 92).
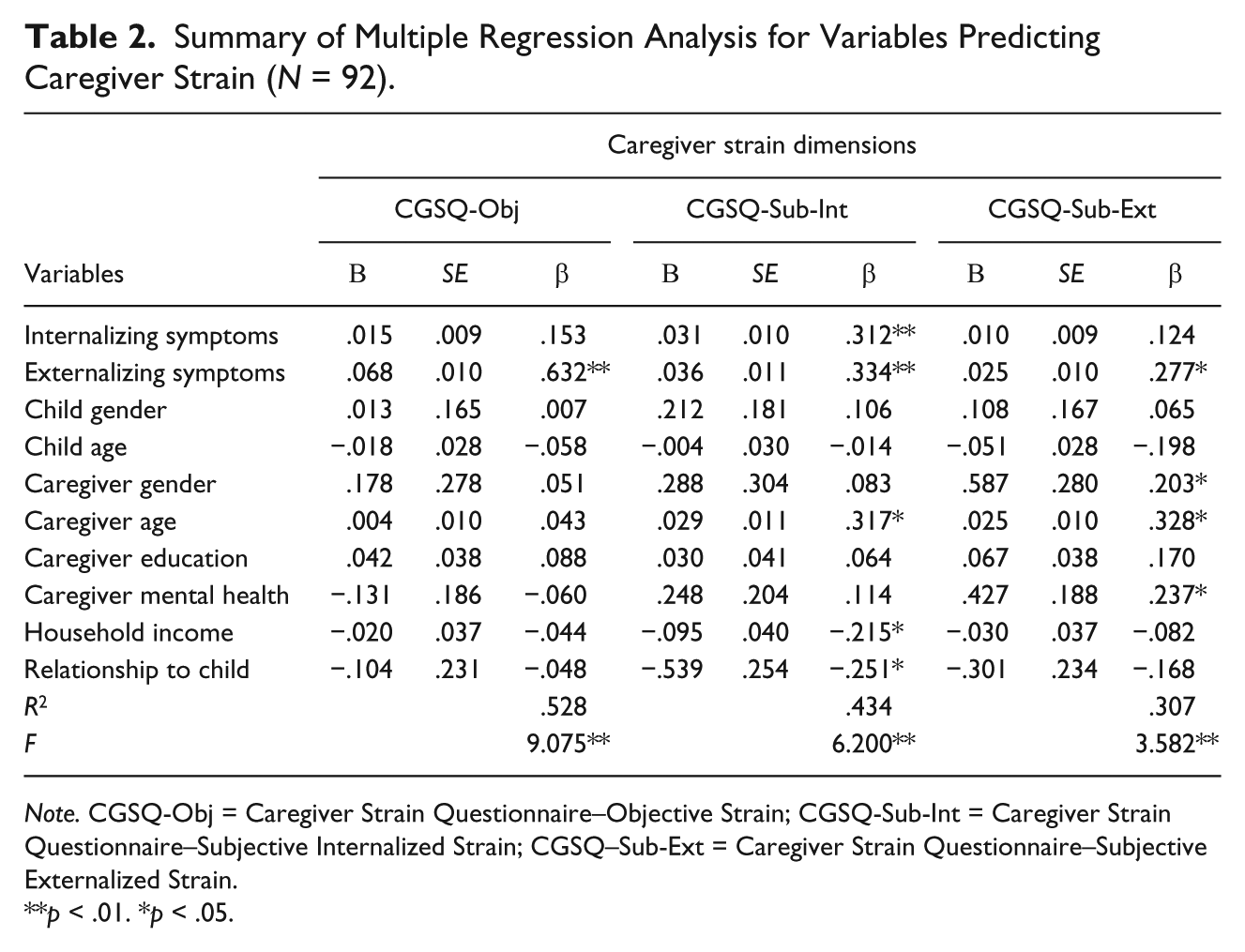
Note. CGSQ-Obj = Caregiver Strain Questionnaire–Objective Strain; CGSQ-Sub-Int = Caregiver Strain Questionnaire–Subjective Internalized Strain; CGSQ–Sub-Ext = Caregiver Strain Questionnaire–Subjective Externalized Strain.
p < .01. *p < .05.
Caregiver Subjective Internalized Strain
The prediction model was statistically significant, F(10, 81) = 6.200, p < .001, with an R2 = .434 and an adjusted R2 = .364, indicating that approximately 36% of the variance in caregiver subjective internalized strain was accounted for by the model. Internalizing symptom, externalizing symptom, caregiver age, household income, and relationship to the child were significant predictors of caregivers’ subjective internalized strain. Child internalizing problems, externalizing problems, and caregiver age were positively related to subjective internalized strain. Higher household income was associated with lower strain on the subjective internalized dimension. Relative caregivers reported less subjective internalized strain than caregivers did biological parent caregivers (see Table 2).
Caregiver Subjective Externalized Strain
The prediction model was statistically significant, F(10, 81) = 3.582, p < .001. Approximately 22% (R2 = .307 Adjusted R2 =.221) of the variance in caregiver subjective externalized strain was accounted for by the model. Internalizing symptom, externalizing symptom, caregiver age, and caregiver mental health were significant predictors of caregiver subjective externalized strain (see Table 2). Child internalizing problems, externalizing problems, and caregiver age were positively related to subjective externalized strain. Caregivers’ mental health status was a significant predictor of subjective externalized strain; caregivers whose mental health problems were leading to the children’s referral for services reported greater strain compared to their counterparts (see Table 2).
Discussion
Researchers and practitioners increasingly understand the importance of not only recognizing the potential for toxic strain associated with raising children with EBDs but also assisting caregivers to copy with these pressures. Overall, a larger proportion of the variance in caregivers’ objective strain was explained by these models than in either of the two subjective strain dimensions; the poorest fit was for subjective externalized strain. These results are consistent with findings from other studies in terms of the portion of variance explained by the model (e.g., Brannan & Heflinger, 2006; Heflinger & Taylor-Richardson, 2004). Indeed, it appears that other factors should be considered when caregivers report higher levels of subjective strain, especially subjective externalized strain. For example, when caregivers express negative feelings, such as embarrassment, anger, or resentment toward their children or report difficulties in relating to their children, finding ways to support these caregivers might be helpful in addition to more thoroughly considering the factors that might be contributing to these feelings.
Overall, the findings from our study generally supported the study’s hypotheses. Each dimension of caregiver strain had different correlates, and children’s externalizing symptoms strongly predicted higher strain across all three measurement dimensions. In other words, caregivers of children with higher levels of acting out behaviors found it more difficult to handle their children’s behavioral demands and experienced higher degrees of negative feelings toward themselves and their children. This appears to be consistent with Brannan and Heflinger’s (2006) interpretation that “externalizing behavior is disruptive and difficult to manage, makes the care-giving role more challenging, and clearly places considerable stress on the caregiver and family” (p. 418). Again we suggest that dealing with the children’s externalizing problem behaviors might be effective in relieving their caregiver’s strain.
While internalizing symptomologies such as anxiety or depression among children/youth significantly predicted subjective internalized strain, they did not predict other strain dimensions. Since internalizing behaviors are internal and arguably less obviously persistent than observable acting out behavioral disorders, they tend to create fewer noticeable challenges for others and to cause less disruptions for caregivers’ work and family social activities, such as not leading to a child being sent home from school. In other words, caregivers do not have to respond to the consequences of their child’s internalizing behaviors the same way or to the same extent as caregivers of children who manifest high levels of externalizing behaviors. And it follows that this group of caregivers experience less anger, resentment, or embarrassment about their children’s behaviors. Furthermore, because internalizing behaviors are less visible, they actually may engender empathy toward children (Meltzer et al., 2011). Researchers have noted that it is more likely the caregivers of children with emotional challenges attract sympathy and support from others, while parents of children with acting out behaviors are blamed, blame themselves, or both for their children’s challenges (Meltzer et al., 2011). Thus, the presence of higher externalizing problems may engender more caregiver anger and resentment, while higher internalizing problems do not. This also appears to be supported by other studies that found that higher child internalizing problems were associated with lower levels of subjective-externalized strain (Heflinger & Taylor-Richardson, 2004), and levels of internalizing behaviors were not related to caregiver externalized strain (Bussing, Gary, et al., 2003, Bussing, Zima, et al., 2003b; Brannan & Heflinger, 2006). Nevertheless, it is natural and understandable for caregivers to experience worry, guilt, and sadness about their children’s challenges, irrespective of whether they are internalized, externalized, or a combination of both.
Caregiver’s mental health status was associated only with subjective externalized strain. Caregivers with mental health issues associated with their children’s referral for services reported higher levels of resentment or anger toward their children; yet they did not report higher levels of objective strain or subjective internalized strain. This appears to be inconsistent with Heflinger and Taylor-Richardson’s (2004) study, which found that caregiver mental health predicted all dimensions of caregiver strain. This is understandable, since compared to Heflinger and Taylor-Richardson’s study, most of the caregivers in this current study generally had a healthier mental health status, with approximately 28% reporting having mental health issues. Also, in the current study, mental health was a categorical variable and measured by whether or not caregiver mental health problems led to the child’s referral for services, while in Heflinger and Taylor-Richardson’s (2004) study, caregiver mental health was a continuous variable measured by the 12-item Short Form (SF-12) Health Survey. The different instruments used in these two studies, and the consequential difference in measurement sensitivity might have contributed to this difference. According to Brannan and Heflinger (2001), caregivers can distinguish their own psychological distresses from strain related to caring for their children; however, caregiver strain was treated as an unabridged structure in this study rather than individual dimensions. We speculate that perhaps caregivers can recognize the objective behavior demands and their own internal feelings that are related to caring for their children but may not fully distinguish their own psychological distress from externalized types of subjective strain (e.g., resentfulness, anger) related to caring for the children. We further wonder whether having mental health problems interferes with caregivers’ abilities to moderate their own moods and feelings toward their children. One possible suggestion is that for caregivers with mental health issues, more attention should be given to their subjective externalized strain and we recommend that future researchers explore this possible connection.
Caregiver relationship to children only significantly predicted subjective internalized strain. Specifically, biological parents tended to report higher levels of sadness, worry and guilt about their children’s problems than did other caregivers, such as foster parents, grandparents, uncles or aunts. The results also are consistent with Heflinger and Taylor-Richardson’s (2004) study, which suggested that relative caregivers reported lower levels of strain on internalized feelings than did parents. Thus, it might be helpful to tailor approaches to assisting different groups of caregivers in coping with their strain; for biological parents, closer attention should be given to their internalized feelings. However, this does not suggest that relative caregivers do not experience strain of caring for the children. Indeed, Heflinger and Taylor-Richardson’s study indicated that relative caregivers experience similar levels of stain as parents, and these strains are predicted by similar variable sets.
Caregiver’s gender and age were related to some dimensions of caregiver strain. For example, caregiver age was positively related to the two subjective types of strain; specifically, with increases in caregiver age, more negative feelings toward themselves and their children were reported. Caregiver gender only significantly predicted subjective externalized strain, with female caregivers reporting more anger, resentment, and embarrassment related to their child’s problems. Perhaps, these types of strain are more pronounced for older mothers, especially for children who are preteens (Sales et al., 2004). Children’s gender did not relate to any dimension of caregiver strain, which is consistent with previous studies (Brannan & Heflinger, 2006; Heflinger & Taylor-Richardson, 2004). Thus, patterns of the strain experienced by caregivers are similar whether they are raising girls or boys. Finally, child’s age also had no statistical effect on the dimensions of caregiver strain. Although some other studies found a positive relationship between children’s age and subjective externalized strain dimension (Brannan & Heflinger, 2006; Heflinger & Taylor-Richardson, 2004), we noted that the youth in those studies were older than the participants in this current study.
Annual household income was associated only with subjective internalized strain and had no significant impact on other dimensions of caregiver strain. Caregivers with higher annual incomes appeared to experience lower levels of sadness, worry, or guilt than caregivers with lower incomes. This appears to be consistent with the conceptual model of stress and coping, which supports that greater income is a resource that may help protect families from strain. It is also possible that a higher income is associated with greater stability, which in turn offers better opportunities to work. Some researchers also have reported that working outside the home might provide respite, allowing time away from the caregiving role (Bussing, Gary, et al., 2003; Sales et al., 2004). Such opportunities may also increase caregivers’ feelings of broader social support from friends and the community, which also may alleviate perceptions of strain (McDonald et al., 1997). Interestingly, educational background was not shown to be associated with any dimension of caregiver strain. Thus, we encourage future researchers to explore the associations among work, education, and preparation for work, with short- and longer terms perceptions of caregiver strain.
Limitations
Several limitations should be acknowledged when considering the findings of this research study. First, because the samples were drawn from systems of care enrollees in one region of one state, Indiana, the generalizability of these findings may be limited to children/youth who enrolled in the OCOF system of care. The extent to which these findings may be generalized to other clinical populations (i.e., presenting problems other than EBDs) and/or other geographic areas is unknown. Still, this research does provide some implications for service delivery systems (e.g., systems of care) in similar communities, such as reaching out to caregivers proactively. Second, the omission of race/ethnicity as a predictor variable was a shortcoming, since race has consistently been found to predict reports of caregiver strain (Brannan & Heflinger, 2006; Kang et al., 2005; McCabe et al., 2003). However, since the large majority of the participants in the OCOF system of care were Caucasian, there is no variance in race/ethnicity. Third, rather than using a direct measure, such as SF-12 Health Survey, caregiver mental health status was drawn from a question about problems and risk factors leading to child’s referral to the system of care. We suggest that a reliable mental health instrument should be used in future research to obtain more accurate information about the relationship between caregiver mental health and caregiver strain. Still, the superficial inquiry about caregiver mental health status at enrollment used in this study provided some intriguing and potentially important information for practice and also points to a possible area for intervention. In addition, not all factors related to caregiver strain were measured in this study. Numerous other factors have been shown to influence or mediate a caregiver’s strain, such as social support, family coping skills, child competencies, access and barriers to care, system characteristics, and mental health service use (Abidin, 1992; Accurso et al., 2015; Brannan & Heflinger, 2006; McDonald et al., 1997). The authors have considered more complex models involving additional constructs that they plan to test; however these were beyond the scope of this study. We encourage researchers to continue the development and study more complex models to improve our understanding of how to best prevent caregiver strain, intervene in caregiver mental health, and support caregivers of young people with mental health challenges.
Implication for Practice
Despite these limitations, the results of this study provide relevant information about the contribution of child symptomology and other factors on caregiver’s strain. We argue that it may be useful for practitioners and family members to learn more about the different kinds of caregiver strain, the factors related to these types of strain, and ideas for avoiding, confronting, or overcoming different kinds of strain. Although it is well known to researchers in the children’s mental health field, this kind of information will also be beneficial for practitioners and caregivers for several reasons. First, understanding these relationships can assist practitioners to more quickly and effectively engage and support caregivers by providing more nuanced understandings about the types of symptoms and factors that can be associated with specific types of strain. Since different symptom patterns and characteristics may make caregivers more or less vulnerable to various types of strain, practitioners could use clinical intake information from caregivers and children to identify potentially needed services and supports. This may be particularly pertinent for families with children who are experiencing high levels of externalizing behaviors.
We likewise recommend proactively anticipating possible higher strains and supporting caregivers accordingly, particularly when their child’s externalizing problem behaviors are clinically significant. Furthermore, caregivers of children with severe externalizing behaviors should receive additional support immediately on diagnosis. Although children’s internalizing behaviors (anxiety/depression) predicted only one dimension of caregiver strain (subjective internalized strain), these challenges cannot be ignored. Even though this kind of strain may appear less problematic overall, there can be no doubt that caregivers worry when their children appear depressed or anxious. Perhaps providing targeted supports for children with internalizing behaviors will be sufficient to reduce caregivers’ strain levels. We note that increased awareness among practitioners, including primary care providers, also could lead to increased simple but crucial responses such as directing a caregiver to a parent support group. These efforts might fend off later challenges associated with internalizing issues such as substance abuse and suicide ideation among children/youth. On the other hand, practitioners might also take into account possible variations among caregivers whose children have high levels of externalizing or internalizing behaviors, or a possible need for different support/coping strategies tailored to parents’ needs and preferences.
It might also be potentially useful for caregivers to have the same information. We talk about “family driven” and “empowering the parents” frequently in systems of care; thus, parents and caregivers who have this knowledge and information will assist with informed decision making for themselves and their children. Parents might generally know that their strain is coming from their children’s challenges, but they might not understand the nuances, including different dimensions of strain and their respective correlates. Caregivers might combine their responses to general parenting stress with strains specifically related to the children’s problems and then link aggregated strain with their children. We again recommend that parents be provided with informed knowledge so they can proactively reflect on their strain experiences, better understand their situation, and make informed decisions about how to proceed. Although each family is unique, understanding or at least having awareness about strain, when it is toxic, and how to combat it can assist caregivers to better reflect on their day-to-day experiences, make corresponding adjustments, and seek services and supports proactively instead of waiting for strain to take its toll.
Implications for Research
This study examined several predictors of caregiver strain hypothesized to be related to caring for children with EBDs. Future research could explore some areas in more depth, such as caregiver strains predicted by income and/or education, which is unclear and findings across disciplines are contradictory. For instance, some studies found that caregiver resources such as education, employment, and income were significantly associated with days of youth service use (Burnett-Zeigler & Lyons, 2010). Is it possible that “days of services utilization” mediate between caregiver resources and caregiver strain? Future research could examine more complex models to investigate the mechanisms behind these relationships. In addition, this current study is cross-sectional and does not imply causality. Therefore, results do not conclusively demonstrate that child symptoms and other factors contribute to caregiver strain. It is possible that caregivers who perceived themselves to have greater strain tend to rate their children as more severe (Accurso et al., 2015) or that the added strain placed on caregivers influenced their mental health in ways that were not uncovered or examined in this study (Brannan & Heflinger, 2001; Sales et al., 2004). Longitudinal studies are recommended to help clarify these complex relationships. Finally, the researchers found specific relationships between types of caregiver strain and different types of “predictors.” A next step may be to develop and test interventions that build on what has been learned.
Footnotes
Authors’ Note
The opinions expressed are those of the authors and do not necessarily represent views of funders or partners.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from SAMHSA (Grant No. 6 11S5 SM05851802) to the Indiana Families and Social Services Administration and CMHC, Inc., to Indiana University for evaluation of the One Family One Community project.