
Abstract
Parents are an important source of sexual health information for adolescents, and quality parent–adolescent sexual communication has been linked to positive sexual health outcomes. We sought to enhance the limited information about parent–adolescent sexual communication in India. The participants were 78 mothers and 91 fathers of adolescents ages 12–19 years. Both mothers and fathers reported limited past sexual communication, on average having talked to their child in general terms only and only a few times, although communication was somewhat better when the sex of the parent and adolescent were congruent. Only half of the parents had strong intentions to engage in these conversations during the following year. Parents’ reports and multiple regression analyses identified parents’ attitudes, knowledge, comfort, and history of sexual communication with their own parents as key factors in limiting parent–adolescent sexual communication engagement and intentions. A number of strategies to enhance parent-adolescent sexual communication are discussed.
Keywords
India has a poor record with respect to the sexual health of adolescents. This record includes one of the highest rates of untreated sexually transmitted infections (STIs) (World Health Organization [WHO), 2012], and the highest rate of sexual abuse during childhood globally (Singh et al., 2014). Female adolescents bear a disproportionate burden of the poor sexual health outcomes as a consequence of extreme gender inequity and the socioeconomic and political disempowerment of women (Das, 2014; McDougall et al., 2011). For example, 47% of girls marry before the legal age of 18 years, four million girls between 15 years and 19 years give birth annually, and the most frequent causes of death for young women are pregnancy-related (Gupta et al., 2010; International Institute for Population Sciences [IIPS] & Macro International, 2007; United Nationals Childrens Fund [UNCF], 2014; United Nations Population Fund [UNPF], 2018). The sexual health of male adolescents also is at risk because hegemonic masculinity prescribes that men should be indifferent about health care, and it promotes early sexual contact, often with sex workers (Chakraborty, 2010).
An important means to improve sexual health outcomes for adolescents is to provide them with information (Ackerson et al., 2012; Davis, 2013). Parents are an important potential source of such information, particularly because school-based sexual health education is highly controversial and is not widely offered in India (Chakraborty, 2010; Das, 2014; Ismael et al., 2015; O’Sullivan et al., 2019). More quality parent-adolescent sexual communication has been linked consistently to a range of positive sexual health outcomes in other countries including delayed initiation of sexual activity and more frequent use of contraceptive and condom (De Looze et al., 2015; Hutchison & Montgomery, 2007; Jaccard et al., 2002; Kao & Manczak, 2012). The goal of the current study was to add to the limited information about parent–adolescent sexual communication in India, including identifying factors that facilitate or serve as barriers to such conversations.
Parent–Adolescent Sexual Communication
Talking about sexual topics is a complicated issue for parents (Byers & Sears, 2012; Chakraborty, 2010). On the one hand, most parents believe that they should provide their children with sexual health information (al Zaabi et al., 2018; Lambert & Wood, 2005; Nair et al., 2013; Weaver et al., 2002). On the other hand, sociocultural norms in countries such as India strongly prohibit open discussions about sexuality, particularly for girls and women (Abraham, 2001; Das, 2014; Ismail et al., 2015). Researchers in a number of countries have shown that parent–adolescent sexual communication is infrequent, lacks detail, and is of poor quality (e.g., is indirect, limited in scope, fear-based, unidirectional, and does not encourage questions), if it occurs at all (Boyas et al., 2012; Liu et al., 2017; Rodgers et al., 2018; ul Haque & Faizunnisa, 2003; Weaver et al., 2002). Together, prohibitive social norms and the results of research suggest that, regardless of what Indian parents believe they should do, parent–adolescent sexual communication may be very limited.
Research in India with adolescents has shown that few identify their parents as an important source of sexual information (Jaya & Hindin, 2009) and only a minority report that they have discussed sexual topics with their parents (Abraham, 2001; Sathe & Sathe, 2005). For example, Kumar and colleagues (2013) found that only 35% of the female adolescents and 23% of the male adolescents in their Indian sample (n = 586) reported having had any sexuality discussions with their parents. Researchers have not assessed Indian parents’ perceptions of the extent, quality, or frequency of their sexual communication with their adolescent. Compared to their adolescent, parents typically describe their sexual communication with their adolescent more positively (Feldman & Rosenthal, 2000; Guilamo-Ramos et al., 2008; Jaccard et al., 1998). Thus, it is possible that Indian parents are more likely to believe that they have communicated more with their adolescent about sexual issues than adolescents report.
Intentions are an important determinant of behavior (Fishbein et al., 2001). As such, parents who have not formed intentions to engage in sexual conversations with their adolescent are unlikely to do so (Byers et al., 2018). Byers and Sears (2012) showed in their sample of Canadian parents of young adolescents that most of the parents who were not active in communicating about sexuality with their adolescent did not intend to do so in the next six months. As a result, they recommended that to be successful at enhancing parent–adolescent sexual communication it is important to increase motivation (i.e., intentions). Therefore, we also examined Indian parents’ intentions with respect to engaging in sexual discussions with their adolescent in the future.
Researchers have shown that parents identify a range of concerns that inhibit them from discussing sexual topics with their adolescent. These include their own discomfort, embarrassment, and lack of knowledge; fears that their adolescent will be embarrassed or respond negatively; concerns that these conversations will encourage sexual activity before marriage; and perceptions that their adolescent has received the information from other sources such as school or the media (Byers & Sears, 2012; Chakraborty, 2010; Liu et al., 2017; Masilamani, 2003). However, researchers have not examined how commonly Indian parents identify each of these concerns as barriers to sexual discussions with their adolescents. Yet this information is crucial to efforts to enhance parent–adolescent sexual communication and to improve adolescent sexual health outcomes.
We also sought to determine differences in sexual communication, communication intentions, and perceptions of barriers by mothers and fathers of daughters and sons. Given the strong gender-based social norms in India (Abraham, 2001), we expected that compared to mothers of sons, mothers of daughters would report greater sexual communication and sexual communication intentions and perceive fewer barriers to sexual communication; we expected the opposite pattern for fathers.
Factors Associated with Sexual Communication Engagement and Sexual Communication Intentions
A number of researchers have presented frameworks proposing that parent characteristics, youth characteristics, and the sexual communication context are closely linked to parent–adolescent sexual communication (e.g., Flores & Barroso, 2017; Jaccard et al., 2002). Because we were studying parents, we concentrated on the associations between parent characteristics (parents’ education, attitudes toward providing adolescents with sexual information, number of perceived barriers to parent-adolescent sexual communication, sexual knowledge, comfort with sexual topics, and sexual communication with their own parents) and parent–adolescent sexual communication engagement. Specifically, researchers in a range of countries, but not India, have demonstrated that parents who engage in more extensive and/or more frequent sexual conversations with their adolescent tend to have more education, more positive attitudes toward providing youth with sexual information, perceive fewer barriers to communicating with their child, feel more knowledgeable and comfortable having these conversations, and had better sexual communication with their own parents (Byers et al., 2018; DiIorio et al., 2000; Guilama-Ramos et al., 2008; Jerman & Constantine, 2010; Liu et al., 2017). We also assessed two youth characteristic: age and congruence between the sex of the parent and adolescent. Parents are more likely to support providing sexual health information to and engage in sexual conversations with older than with younger adolescents (Byers et al., 2008; Jaccard et al., 2002). Researchers in the United States has shown that mothers engage in more sexual communication with their daughters and fathers engage in more sexual communication with their sons (Hutchison & Montgomery, 2007; Jerman & Constantine, 2010).
Byers et al. (2018) showed that some of the factors associated with the extent of parent–adolescent sexual communication also are associated with parents’ intentions to engage in these discussions. Therefore, it is likely that the predictors identified earlier are associated with Indian parents’ sexual communication intentions. Byers and her colleagues also showed that parents who have already engaged in more extensive sexual discussions have stronger intentions to do so in the future suggesting that parents’ history of sexual discussions with their adolescent would be associated with their intentions to engage in such discussions in the future over and above the contributions of other predictors.
The Current Study
The goal of the current study was to provide information important to informing efforts to enhance adolescent sexual health in India by conducting a systematic study of parent–adolescent sexual communication using a sample of parents from across the country. We posed the following research questions: RQ1: What is the extent, frequency, and quality of parent–adolescent sexual communication? RQ2: How strong are parents’ intentions to communicate about sexual with their adolescent in the coming year? RQ3: What are mothers’ and fathers’ perceptions of barriers to sexual communication with their son or daughter?
We also tested the following hypotheses: H1: Mothers will report greater sexual communication engagement with daughters than with sons; fathers will report greater sexual communication engagement with sons than with daughters. H2: Mothers of daughters will report stronger sexual communication intentions than mothers of sons; fathers of sons will report stronger sexual communication intentions than fathers of sons. H3 and H4: Parents with an adolescent who is older and is the same sex as themselves, and who have more education, more positive attitudes toward providing youth with sexual information, perceive fewer barriers to doing so, feel more knowledgeable and more comfortable having these conversations, and had better sexual communication with their own parents will report greater sexual communication engagement (H3) and stronger intentions to engage in sexual communication in the future (H4) with their adolescent. H5: Parents’ history of sexual communication engagement with their adolescent will add to the prediction of sexual communication intentions over and above the other predictors.
Method
Participants and Procedure
The sample consisted of 169 parents: 78 mothers (46%) and 91 fathers (54%), almost all of whom were currently married (96%). On average, they were 40.7 years (SD = 5.2) old. They resided in 18 different Indian states and territories, with the largest number residing in Tamil Nadu (38%) and Kerala (26%). The majority (78%) indicated being of the Hindu religion, although 6% were Muslim, 12% were Christian, and 4% identified with another religion; on average they reported that religion was moderately important to their everyday life (M = 2.9; SD = 1.00). This sample primarily represents the Indian middle-class as most parents had a university degree (93%), worked outside of the home (64%), and had a partner who worked outside the home (61%). In terms of characteristics of the target adolescent, about half were girls (52%) and half were boys (49%), and they were fairly evenly divided across classes (grade) 7 through 12.
A crowdsourcing website (Mechanical Turk®; MTurk) that is popular with residents of India was used to recruit participants for a larger survey study about reproductive health education in India. Adults (N = 1140), 18 years and older, with and without children, who could complete a questionnaire in English responded. Individuals who gave consent to participate were directed to an online survey. The current study is based only on those participants who indicated that they had a child between the ages of 12 years and 19 years. As such, 776 participants who completed the survey were excluded because they did not have a child within this age range. An additional 195 participants were excluded because they responded incorrectly to validity items (n = 102), submitted multiple responses (based on examinations of duplicate MTurk ID and IP addresses) (n = 90), or omitted key items (n = 3). Participants received a small monetary compensation for completing the survey. Inclusion of individuals with and without children in the data collection reduced the likelihood that they would lie about their child status (i.e., claim to have an adolescent when they did not have an adolescent) in order to receive compensation. Data from the larger survey on sexual education in schools have been published elsewhere and are distinct from the current study (O’Sullivan et al., 2019).
Measures
Parents responded to four questions related to their sexual communication with their target adolescent: the extent of their communication about sexual health topics on a four-point scale (not at all (1), in general terms only (2), in some detail (3), and in a lot of detail (4)); the frequency of these discussions and the frequency of encouraging the adolescent to ask questions, both on five-point scales ranging from not at all (1) to very often (5); and the quality of the sexual health education they had provided to their adolescent on a five-point scale ranging from very poor (1) to very good (5). Parents who indicated that they had not talked to their adolescent at all were given a score of 0 on the quality item. Responses to each of these items are reported separately. In addition, responses were summed to yield a total Sexual Communication Engagement score, with possible scores ranging from 3 to 19 and higher scores indicating more sexual communication engagement. To support our decision to sum responses on the four items, we conducted a principal component analysis that yielded a one factor solution with loadings ranging from .79 to .91, accounting for 70.52% of the variance. The internal consistency of the four-item measure was high (α = .84).
Parents also indicated their intentions to talk to this adolescent about sexual topics in the coming year (Sexual Communication Intentions). Response options were yes definitely, yes probably, yes possibly, no, and not sure. Responses were recoded to the following: strong intentions (yes definitely and yes probably), weak intentions (yes possibly and not sure), and no intentions (no).
Parents were asked whether they had talked to their adolescent about sexual health topics as much as they should have. Those who felt that they had not done so then identified which of 11 possible barriers had stopped them from doing so (no/yes; see Table 1 for the list of the potential reasons). We also used these responses to calculate the Number of Perceived Barriers (α = .80 in the current study).
Number and Percent of Parents Who Endorsed Each Reason for Not Engaging in More Sexual Communication with their Adolescent
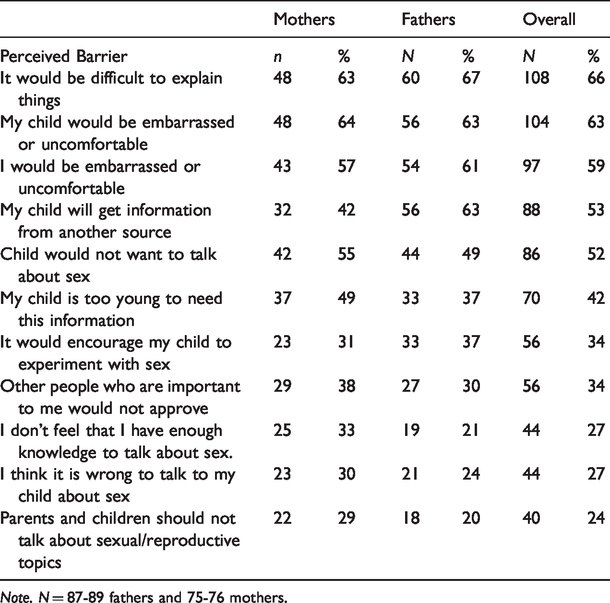
Note. N = 87-89 fathers and 75-76 mothers.
Results
Parent-Adolescent Sexual Communication and Communication Intentions
In terms of parent sexual communication with the target adolescent (RQ1), on average, parents indicated that they had discussed sexual health topics with their adolescent in general terms only (M = 2.25, SD = .77), had discussed sexual topics and had encouraged questions between once or twice and a few times (M = 2.56, SD = .96 and M = 2.44, SD = 1.14, respectively), and had rated the quality of the sexual education they had provided to their adolescent as neither poor nor good (M = 3.21, SD = 1.27). This resulted in an average Sexual Communication Engagement score of 10.57 (SD = 3.43) on a scale ranging from 3 to 19. To test H1, we conducted a 2 (sex of parent) x 2 (sex of adolescent) ANOVA, with Sexual Communication Engagement as the dependent variable. Neither the main effect for sex of parent or sex of adolescent were significant (F(1, 165) = 0.01, p = .932, η2 = .01 and F(1, 165) = 0.04, p = .874, η2 = .04, respectively). However, the two-way interaction was significant (F(1, 165) =18.90, p < .001, η2 = .10). Consistent with our hypothesis, fathers of a son reported significantly greater sexual communication engagement than did fathers of a daughter (Ms = 11.09 and 9.32, respectively); and mothers of a daughter reported significantly greater sexual communication engagement than did mothers of a son (Ms = 11.76 and 9.11, respectively).
In terms of parents’ sexual communication intentions (RQ2), more than half of the parents (56%) reported strong intentions to talk to their child about sexual topics in the following year, a third (33%) indicated weak intentions, and about a tenth (12%) indicated no intentions. We examined differences in the strength of mothers’ and fathers’ sexual communication intentions using a 2 (sex of parent) x 2 (sex of adolescent) ANOVA (H2). Neither the main effect for sex of parent nor for sex of adolescent was significant (F(1, 165) = 0.01, p = .949, η2 = .01 and F(1, 165) = 0.00, p = .963, η2 = .00, respectively). However, the interaction was significant (F(1, 165) = 8.16, p = .005, η2 = .05). Fathers of a son reported significantly stronger sexual communication intentions than did fathers of a daughter (Ms = 1.54 and 1.24, respectively); and mothers of a daughter reported significantly stronger sexual communication intentions than did mothers of a son (Ms = 1.58 and 1.25, respectively).
Parents’ Perceptions of Barriers to Sexual Communication
Almost all of the parents (165/169; 97.6%) indicated that they had not talked to their adolescent as much as they thought they should have, and so they responded to a question regarding 11 possible reasons for not doing so (RQ4). The percentage of mothers and fathers who endorsed each reason is reported in Table 1. Three reasons were endorsed by more than half of both mothers and fathers: they (the parent) would be embarrassed or uncomfortable; their child would be embarrassed or uncomfortable; and, it would be difficult to explain things. However, the other potential barriers were endorsed by substantial percentages of the mothers (29% to 55%) and fathers (20% to 63%). On average, parents endorsed 4.8 (SD = 3.0, range = 0 to 11) reasons as barriers to their communication about sexual health topics with their adolescent. A 2 (sex of parent) x 2 (sex of adolescent) ANOVA found no significant difference in the number of barriers reported by mothers and fathers of a son or a daughter (F(1, 161) = 0.05, p = .862, η2 = .05 for sex of parent, F(1, 161) = 0.27, p = .696, η2 = .21 for sex of adolescent, and F(1, 161) = 1.45, p = .231, η2 = .01 for the interaction).
Factors Associated with Sexual Communication Engagement and Communication Intentions
The means and standard deviations for the predictors included in this study are presented in Table 2. On average, parents had highly positive attitudes toward children learning about sexual health, identified between four and five barriers to communicating with their adolescent about sexual health topics, felt moderately knowledgeable about and moderately comfortable talking about sexual health topics, and reported poor sexual communication with their own parents. Correlations among the predictors are presented in Table 2. No problems with multicollinearity were detected. At the bivariate level, all of the predictors except adolescent age and parent education were significantly associated with sexual communication engagement and sexual communication intentions.
Means, Standard Deviations, and Correlations among Predictor Variables
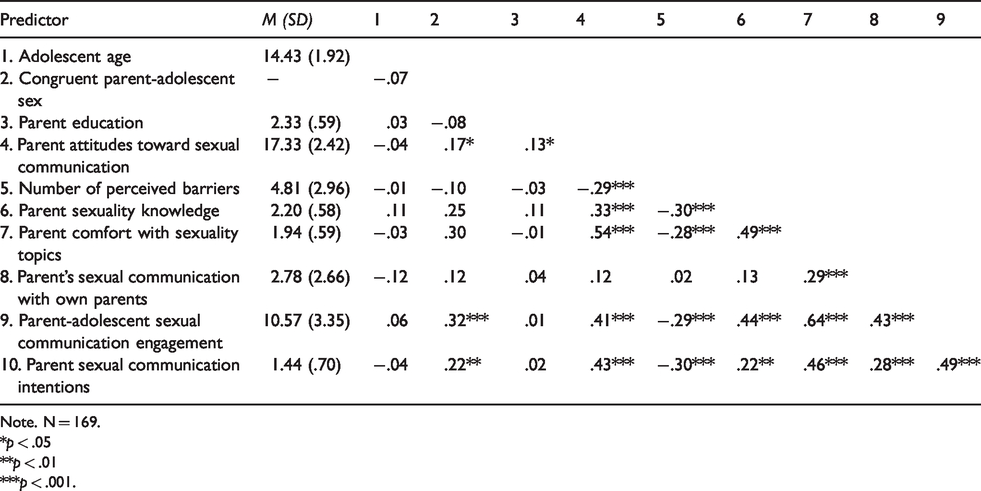
Note. N = 169.
*p < .05
**p < .01
***p < .001.
We used a multiple regression analysis to predict parent–adolescent sexual communication engagement from the eight predictor variables (H3). It was significant and accounted for 54% of the variance, F(8, 160) = 25.23, p < .001 (see Table 3). Parents reported greater sexual communication engagement if their adolescent was older and the same sex as them and if they reported fewer barriers to sexual communication, greater comfort discussing sexual health topics, and better sexual communication with their own parents.
Multiple Regression Analyses Predicting Sexual Communication Engagement and Sexual Communication Intentions
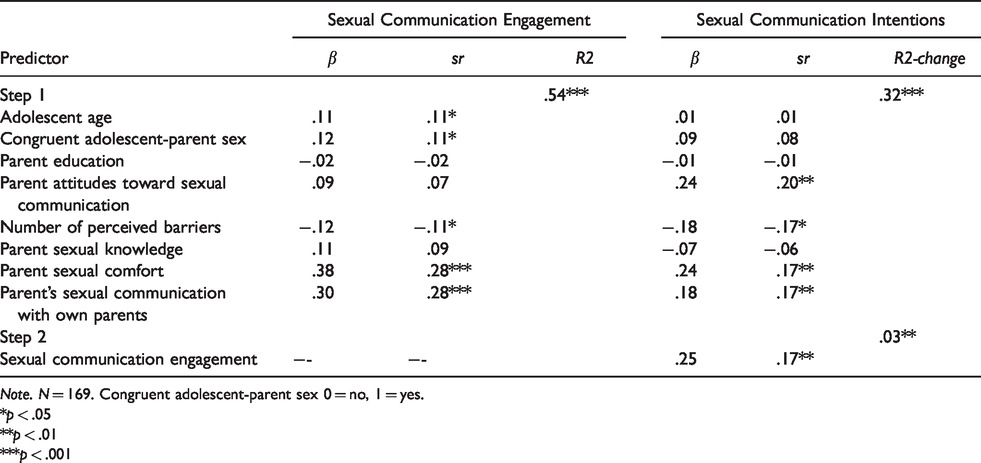
Note. N = 169. Congruent adolescent-parent sex 0 = no, 1 = yes.
*p < .05
**p < .01
***p < .001
We used a hierarchical multiple regression analysis to predict the strength of parents’ intentions to talk to their adolescent about sexual health topics in the coming year. At Step 1, we entered the eight predictor variables (H4). At Step 2, we entered past parent-adolescent sexual communication engagement (H5). The block of predictor variables was significantly associated with Sexual Communication Intentions, accounting for 32% of the variance (F(8, 160) = 9.29, p < .001; see Table 3). Parents with more positive attitudes toward providing adolescents with sexual health information, who perceived fewer barriers to discussing sexual health topics, felt more comfortable discussing sexual health topics, and had better sexual communication with their own parents reported stronger sexual communication intentions. Past parent-adolescent sexual communication engagement entered at Step 2 accounted for an additional 3% of the variance (Fchange (1, 159) = 6.80, p < .01). Parents who reported greater sexual communication engagement with their adolescent in the past reported stronger intentions of sexual communication.
Discussion
Parent–adolescent communication is an important potential means to enhance sexual health outcomes for adolescents. This study provides some empirical insights into Indian parents’ sexual communication with their adolescent as well as factors that might help or hinder the communication process. In line with our expectations, both mothers and fathers reported limited past sexual communication, on average having talked to their adolescent only in general terms and only a few times. Furthermore, only half of the parents had strong intentions to engage in sexual discussions with their adolescent in the coming year. In keeping with research conducted in the United States (Hutchison & Montgomery, 2007; Jerman & Constantine, 2010), we found that communication was greater when the sex of the parent and the adolescent were congruent. We extended these findings by showing that this also extends to sexual communication intentions. However, these differences were not large—that is, communication was limited even with an adolescent of the same sex as the parent, and parent–adolescent sex congruence was not associated with the number of perceived barriers. These findings attest to powerful gender and sexual norms in India that prohibit open discussions about sexuality (Abraham, 2001; Chakraborty, 2010; Das, 2014; Ismail et al., 2015) and suggest that these norms also guide sexual socialization in the family context including parent–adolescent communication about sexual topics. They also are consistent with research showing that only a minority of Indian adolescents report that they have discussed sexual health topics with their parents at all (Abraham, 2001; Jaya & Hindin, 2009; Kumar et al., 2013; Sathe & Sathe, 2005). In addition, they add to a body of research in a number of countries showing poor or limited parent–adolescent sexual communication (Boyas, et al., 2012; Liu et al., 2017; Rodgers et al., 2018; ul Haque & Faizunnisa, 2003; Weaver et al., 2002) and limited intentions to engage in these discussions (Byers & Sears, 2012).
These findings are particularly troubling because parent–adolescent sexual communication in India is likely more limited than indicated by our data. First, we did not assess the sexual health topics covered. It is likely that the parents who engage in these conversations discuss some, perhaps less controversial, topics in general terms but do not discuss other important topics at all (Byers et al., 2008; Chakraborty, 2010). Second, parents tend to report more extensive sexual communication with their adolescent than their adolescents report (Feldman & Rosenthal, 2000; Jaccard et al., 1998). Finally, our sample was highly educated. As such, our participants may be more aware, than are parents with limited education, of the negative sexual health outcomes that Indian adolescents experience as well as the importance of providing adolescents with sexual health information. Research is needed to determine parent–adolescent sexual communication engagement on each of a range of topics from both parents’ and adolescents’ perspectives among Indians from a range of socioeconomic backgrounds.
Parents’ Perceptions of Barriers to Parent-Adolescent Sexual Communication
On average, the parents in this study had highly positive attitudes toward their adolescent receiving sexual health information and thought that they should have talked to their adolescent about sexual health more than they had. The results shed light on their perceptions about why they had not done so. Indeed, on average parents identified just under five different barriers (out of a possible 11) to having these conversations. The finding that a majority of mothers and fathers identified their perception that sexual communication would be difficult and awkward for them and for their adolescent is not surprising, given sociocultural norms prohibiting conversations about sexuality and parents’ lack of preparation to have these discussions (Abraham, 2001; Chakraborty, 2010; Das, 2014; Ismail et al., 2015). We also found that a substantial minority of parents appeared to retain traditional attitudes opposing or limiting sexual communication (e.g., sexual conversations would encourage their adolescent to experiment with sex and parents and children should not talk about sexual-reproductive topics). Even more parents felt that their adolescent was too young for such conversations, even though the target adolescents were at least 12 years of age and so likely to have entered puberty. This finding is in keeping with previous work showing that, on average, Indians feel that parents should start talking to their children about sexuality when they are 14 years or 15 years old, and they endorse grade levels for sexual health education that are later than recommended internationally (O’Sullivan et al., 2019; United Nations Educational, Scientific, and Cultural Organization [UNESCO], 2013). Finally, more than half of the parents indicated that their adolescent would get the information from another sources. These findings parallel those found in a study of Chinese parents (Liu et al., 2017). It is unlikely, however, that Indian adolescents would get sexual health information from formal, authoritative sources because there is limited implementation of sexual health education in Indian schools and most health care professionals do not adequately address the sexual needs of adolescents (Chakraborty, 2010; Das, 2014; Ismail et al., 2015). This situation leaves many adolescents to get their information from informal sources such as peers, films, the internet, and pornography (Jaya & Hindin, 2009).
Factors Associated Sexual Communication Engagement and Communication Intentions
In keeping with research in other countries (Byers et al., 2018; DiIorio et al., 2000; Guilama-Ramos et al. 2008; Jaccard et al., 2000; Jerman & Constantine, 2010; Liu et al., 2017), our results provide support for conceptual frameworks that propose that parent source characteristics are closely linked to parent–adolescent sexual communication (e.g., Flores & Barroso, 2017; Jaccard et al., 2002.) An important extension of these frameworks is our finding that in India, these characteristics are also associated with the strength of parents’ intentions to engage in these discussions. This suggests that these factors may inhibit parent–adolescent sexual communication in India through their effects on both motivation (intentions) and behavior (Fishbein et al., 2001; Fisher & Fisher, 1998). In particular, parents’ perceptions of more barriers to such communication, lower comfort with sexual topics, and history of sexual communication with their own parents emerged as unique predictors of their engagement in sexual communication with their adolescent. Attitudes were also uniquely associated with sexual communication intentions. It appears that whereas perceptions of barriers, comfort and personal history likely affect both intentions and their enactment, beliefs about the appropriateness of providing sexual health information to adolescents (i.e., attitudes) play an important role in contributing to intentions specifically. Our finding that attitudes were associated with sexual communication on the bivariate level suggests that they may be indirectly linked to sexual communication behavior through intentions. Longitudinal research is needed to assess and test models (e.g., integrative model of behavioral prediction; Fishbein et al., 2001) that integrate attitudes, intentions (motivation), and skills (comfort, knowledge) to identify the mechanisms by which these factors influence parent–adolescent sexual communication engagement.
Implications
The results of this study strongly indicate that adolescents in India are not getting from their parents the information they need to protect their sexual health, even though almost all of the parents in our study felt that they should be talking to their adolescent about sexual topics more than they had. This situation suggests that parents need help to engage in these discussions in a way that meets the sexual information needs of their adolescent. Because many of the variables we assessed are amenable to change, our findings on barriers to such discussions as well as factors associated with more extensive sexual communication engagement point to ways to facilitate such conversations. First, the results suggest a need for an education campaign aimed at enhancing attitudes toward parent–adolescent sexual communication in general as a means to increase parents’ motivation and intentions to engage in these discussions. Such a campaign should aim to change attitudes and counter myths and misinformation by highlighting the importance and positive sexual health outcomes of quality parent–adolescent sexual communication (De Looze et al., 2015; Hutchison & Montgomery, 2007; Jaccard et al., 2002; Kao & Manczak, 2012). Second, the results point to the need for parent training. Based on our findings, such training needs to: counter myths and misinformation in order to enhance attitudes toward parent–adolescent sexual communication as well as increase motivation and intentions to engage in sexual discussions (Byers et al., 2018); increase sexual knowledge about sexual health topics as well as strategies for how best to approach these discussions (Geasler et al., 1995; Weaver et al., 2002); and enhance comfort and self-efficacy. Our finding that parents’ history of sexual communication with their own parents emerged as a unique predictor of both sexual communication engagement and intentions suggests that successful efforts to enhance parent-adolescent sexual communication will also increase the likelihood that these adolescents will, in turn, engage in these discussions with their own children.
Third, the results have implications for designing more informative sexual health policies that can be implemented at the state level. Given the limited parent–adolescent sexual communication engagement, it is important to provide adolescents with sexual information through other means and not assume that they will get this information from their parents. For example, it is important to make sexual information from formal, authoritative sources such as schools and health care professionals more readily accessible to adolescents. This includes adoption of a comprehensive school sexual health curriculum as well as of protocols in which health care professionals routinely communicate that they are open to discussing sexual concerns. It also involves providing training to teachers and health care providers in order to ensure that they have the skills and comfort to provide this information because research suggests that, even in North America, most teachers and health care professionals do not feel adequately trained to discuss sexual issues (Cohen et al., 2004; Dermer & Badenberg, 2015; Gott et al., 2004; Miller & Byers, 2012). Finally, given adolescents’ reliance on informal sources for sexual information (Chakraborty, 2010), it is important that adolescents have access to a made-in-India website that provides them with accurate and reliable information they need and want, as has been done in other countries (e.g., www.sexualityandu.ca in Canada). The Indian government would need to disseminate the availability of this website widely to ensure up-take by as many adolescents as possible.
Limitations and Conclusion
The results need to be considered in light of the study’s strengths and limitations. Strengths are that we used an anonymous survey and that we sampled fairly broadly across India. However, the sample was highly educated and appears to represent the Indian middle class. As such, even though we did not find that parent education was associated with either sexual communication engagement or communication intentions, the extent to which the results can be generalized to less educated or affluent Indians is not known. In addition, the results are based on correlational data, so it is impossible to draw causal conclusions about the direction of cause-effect relationships and the influence of any third variable (e.g., liberalism and conservativism) on the association between parent characteristics and sexual communication engagement and intentions. Finally, we assessed the perspective of parents only, and these self-report data may have been subject to biased responding. As such, future research should study parent-adolescent sexual communication from the perspectives of both the parents and the adolescent.
Nonetheless, the results strongly suggest that, despite real threats to their sexual health, parents in India are not providing their adolescents with the information they need to protect their sexual health. That is, parents are not engaging in in-depth discussions of sexual health topics with their adolescent even though almost all of the parents in our study felt that they should be talking to their child about these topics more than they had. This suggests that parents need help to be able to meet the sexual information needs of their adolescent. The results point to the importance of enhancing parent comfort in discussing sexual topics and providing information that counters the myths and misinformation that serve as barriers to these discussions as important foci of intervention.
Footnotes
Acknowledgements
The authors greatly appreciate the help of Mary Byers with data collection and feedback provided on the measures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.