
Abstract
The marital status of young medical workers deserves attention due to their working situation, occupational, and personal characteristics. This study investigated the marital decisions and the influencing factors of marital decisions (i.e., marital beliefs, marital policy, work stress, social support, and demographic variables) among 500 young medical workers in China. The results found that the majority of young medical workers decide to marry and have children, and most of them choose to marry or have children before the age of 30, have only one child, and have no preference for the sex of their child. Young medical workers placed the highest importance on marital relationships among the four dimensions of marital beliefs (i.e., marital salience, marital context, traditional norms, and marital relationships). The results further showed that marital salience, marital context, gender, age, educational level, job type, census register, and satisfaction with marital policy had influences on marital decisions. In the future, attention should be paid to different groups' marital beliefs and decisions, help young medical workers improve intimate relationships, enhance awareness of the importance of marriage and childbearing, and strengthen marital welfare policies and services.
Introduction
Significant changes in marriage and fertility have occurred across countries in recent decades. The emerging marital phenomena, such as delayed marriage, remaining unmarried, childless, high divorce rate, nonmarital cohabitation, and illegitimate birth, are prevalent in the United States, European countries, Japan, South Korea, and other developed countries (Matsuda, 2019; Raymo et al., 2015; Smock & Schwartz, 2020; Sobotka & Toulemon, 2008; Yu & Hara, 2023; Zaidi & Morgan, 2017). Similarly, the marital status of Chinese people is showing new trends. According to official statistics, the average age of first marriage and first childbearing for women in 1990 was 21.6 and 23.8 years, respectively, which rose to 26.3 and 27.5 years in 2018, with a delay of 4.7 and 3.7 years, respectively (Guangming Daily, 2021). The total number of registered marriages in 2021 is 7.643 million, the lowest since 1985, and the birth rate is also gradually decreasing (National Bureau of Statistics, 2022). To promote the harmonious development of the population and society, the government adjusted its marriage and childbearing policy in 2021, emphasizing the social value of marriage and childbearing, advocating marriage and childbirth at an appropriate age, and allowing a couple to have three children. Implementing the new policy shows that the Chinese government has shifted from restricting marriage and fertility to encouraging it.
As the leading group in marriage and childbearing, researches have been conducted to analyze and interpret the marital decisions of young people in the context of low marriage and childbearing rates. For example, studies conducted in both developing and developed countries have shown that developmental idealism beliefs about modern society, marriage, and family can be used to explain young people’s marital decisions and behavior, such as late marriage, low fertility, and self-choice (Allendorf et al., 2019; Allendorf & Thornton, 2015; Kavas & Thornton, 2020). Another study analyzed the decisions to marry late and not marry among young adults aged 20–35 years in Korea, and the results found that the decrease in positive marital beliefs was the main contributor (An et al., 2022). In China, traditional Confucianism emphasizes familyism, which is a male-centered differential ethical marital culture (Hao, 2022). Marriage and childbearing are also seen as everyone’s responsibilities, and the purpose of marriage is to have children and carry on the family line (Xu et al., 2014). For a long time after the founding of the People’s Republic of China, the implementation of the family planning policy restricted people’s marital behavior. With the reform and opening up and the development of the economy and society, more and more women participate in the work, the idea of individualism gradually spreads, and traditional marriage and family beliefs are abandoned, which leads to the shock of conventional marital behavior and the emergence of modern marital behavior (Xu et al., 2014; Xu & Xia, 2014).
Although numerous studies have analyzed the marital decisions of young groups, several research gaps should be noticed. First, studies have explored the marital decisions of young people such as university students (Peterson et al., 2012; Virtala et al., 2011), women (Edwards et al., 2019; Keskiner, 2020; Shen et al., 2022) and other young adults (Burgess et al., 2003; Rabenda-Nowak & Wylegly, 2022), whereas medical workers were neglected. Due to the particularity of the working situation and the occupational and personal characteristics, the marital decisions of young medical workers deserve attention. Regarding the working situation, the frequent occurrence of global public health events has increased the workload and posed potential risks to medical workers’ physical health, mental health, and ordinary life, especially under the strict prevention and control of the COVID-19 epidemic in China for nearly three years (Hou et al., 2022; Ning et al., 2022; Pan et al., 2020). In addition, the medical disputes and the tense relationship between medical workers and patients in recent years have also increased the uncertainty of Chinese young medical workers' working situations (Ye et al., 2022; Zeng et al., 2018; Zhou & Grady, 2016). The above working conditions could bring worries about marriage and childbirth for medical workers. Regarding occupational characteristics, medical workers' high workload, work stress, and occupational tension make them more involved at work and face work–family conflicts (Lv et al., 2021; Tan et al., 2023). Work–family conflict is an important factor hindering marital behavior (Cheung & Kim, 2022). Regarding personal characteristics, medical workers usually have a higher level of education, ranging from a journal college to a doctoral degree in China. Previous studies have shown that the improvement of education level is a significant factor leading to decreased marriage and childbearing (Chen & Guo, 2022; Ji & Yeung, 2014; Tian, 2013). It is crucial to pay attention to the marital status of this group. Therefore, under the low marriage and childbearing rate background and China’s latest marriage and childbearing policy, focusing on young medical workers and analyzing their marital decisions and influencing factors is conducive to providing adequate marital support for this group.
Second, in exploring the influencing factors of marital decisions, marital beliefs were proved to be important factors. For example, people with modern beliefs about marriage were likely to live together without marriage, remain single, and choose not to have children (Allendorf & Thornton, 2015). However, marital beliefs (e.g., gender roles, marital relationships, and marital context) and marital decisions (e.g., the decisions of cohabitation, whether and when to get married and have children) are multi-dimensional concepts, it is unclear the specific influence of the dimensions of marital beliefs on various types of marital decisions, and it is necessary to clarify the impact of marital beliefs on decisions.
In summary, this study attempts to analyze young medical workers’ marital decisions and the influence of marital beliefs on decisions in detail. Given the working situation of medical workers and the new marital policy in China, this study would also explore the policy and work-related factors on marital decisions.
Literature Review
Marital Beliefs and Marital Decisions
Marital beliefs refer to the description of the meaning or thought about marriage (Willoughby et al., 2013). Researchers usually use the terms of attitudes, expectations, and perceptions to interpret marital beliefs. For example, Braaten and Rosén (1998) believed marital attitudes were people’s beliefs about their current or future marriage and how they feel about the institution of marriage. Gubernskaya (2010) considered marital attitudes as public opinion about marriage and children. Vaterlaus et al. (2016) thought that marital expectations can be conceptualized as beliefs about how a marriage should be. However, marital beliefs represent a more descriptive construct and have multiple dimensions. For example, Gui (2022) proposed that elements of marital beliefs contain perceptions of marriage, romantic relationships, gender roles, and autonomy. Park and Rosén (2013) conceptualized marital beliefs regarding the intention to marry, marital attitudes, and marital relationships. In order to provide an overarching model of marital beliefs, Willoughby et al. (2013) proposed a marriage paradigm theory, which provides a six-dimension framework for marital beliefs. Specifically, three are beliefs about getting married, such as marital timing, marital salience, and marital context, and three are beliefs about being married, such as marital processes, marital permanence, and marital centrality. This theory provides a comprehensive conceptual framework for marital beliefs. Thus, the current study adopted the framework and defined the dimensions of marital beliefs were marital timing, marital salience, marital context, marital processes, marital permanence, and marital centrality.
Previous studies tend to analyze marital intention, the ideal or expected age of marriage and fertility, and the ideal or expected number of children from the cognition perspective (Karabchuk et al., 2022; Park & Rosén, 2013). It should be noted that these concepts refer to subjective views, which are different from marital decisions. In this study, marital decisions refer to the behavioral decision of a series of events related to marriage and childbearing, including whether to marry, when to marry, whether to have children, when to have children, whether to cohabitate before marriage, and the number of children. It is necessary to explore the relationships between marital decisions and marital beliefs.
Marital beliefs were proved to be the significant predictor of marital decisions. Theories can be applied to explain the influence of marital beliefs on marital decisions. The second demographic transition explains the emergence of the modern marriage phenomenon due to individualism, feminism, materialism, gender equality, and the change of marriage and family beliefs (Lesthaeghe & van de Kaa, 1986). Marriage culture theory describes marital decisions in transitioning from marriage culture to divorce culture (Hackstaff, 2010). Marriage culture comprises three beliefs: marriage is given, marriage is forever, and divorce is a last resort. In contrast, divorce culture encompasses marriage as an option, marriage as contingent, and divorce as a gateway. Hackstaff (2010) pointed out that the meaning of marriage is experiencing the decline of marriage culture and the emergence of divorce culture. Developmental idealism theory comes from the modernization theory, which holds that certain behaviors are labels of modernity and contribute to society’s development (Allendorf & Thornton, 2015). When applied to marriage and family, developmental idealism theory indicates that the delay in marriage, childlessness, increased education, and autonomy are inherent characteristics of modern society, and people who endorse this theory are expected to have behaviors consistent with the beliefs of developmental idealism (Allendorf et al., 2019; Allendorf & Thornton, 2015; Kavas & Thornton, 2020). Additionally, other researchers interpreted marital beliefs from both traditional and modern perspectives. Traditional marital beliefs are characterized by authority, familism, dependency, and patriarchy; modern marriage beliefs emphasize love, intimacy, autonomy, and equality (Keera Allendorf, 2013; Harkness & Khaled, 2014). The above theories explain the influence of marital beliefs on marital decisions and behavior from a macro perspective, which provides a theoretical perspective for people to understand the changes in marriage behavior. However, at the micro level, the impacts of the dimensions of marital beliefs on marital decisions remain to be verified.
The Governmental, Work Environmental, and Personal Factors
In addition to marital beliefs, young medical workers' marital decisions are closely related to governmental policy, work environment, and personal factors. People’s marital decisions are influenced by marital policies. Frimmel et al. (2012) explored the influence of the marriage promotion policy on marital decisions, explicitly investigating the effect of Austria’s marriage subsidy policy on marital decisions, and found that marriage subsidies help promote marriage and increase the number of marriages but have a limited effect on the number of births. In China, Early marriage policies advocated late marriage and childbearing and required couples to have one child. Under the strict policy, people’s marital decisions were exceptionally constrained (Cai & Feng, 2021). Since 2010, the marriage policy has been relaxed. The marital policies in 2021 have advocated marriage and childbearing at appropriate ages, allowed children to be born from one to three, and introduced related policies such as subsidies, marriage leave, childcare leave, and child care. Whether the policies encouraging marriage and childbearing can significantly increase young adults' marital decisions needs to be examined.
Due to the particularity of working situation and occupation characteristics, medical workers’ marital decisions might be influenced by work stress, especially during the COVID-19 pandemic. For example, Zhang et al. (2021) surveyed 615 primary healthcare workers and found that their work stress was high during the pandemic. The workload and intensity of work undertaken by medical workers have skyrocketed, and workload has become the most significant source of stress (Hou et al., 2022). Meanwhile, medical workers' high workload, work stress, and occupational tension make them more involved at work and need to balance work and family life (Lv et al., 2021). Under such circumstances, personal social support is crucial for medical workers (Fu et al., 2022; Woon et al., 2021) and adequate social support is helpful for medical workers. Therefore, this study hypothesizes that work stress and social support may influence the marital decisions of young medical workers.
Based on the above literature review, this study aims to (a) grasp the current status of marital decisions and beliefs of young medical workers, (b) analyze the influences of multi-dimensional marital beliefs on marital decisions of young medical workers, and (c) explore the impact of marital policy, work stress, and social support on the marital decisions of young medical workers.
Method
Participants and Procedures
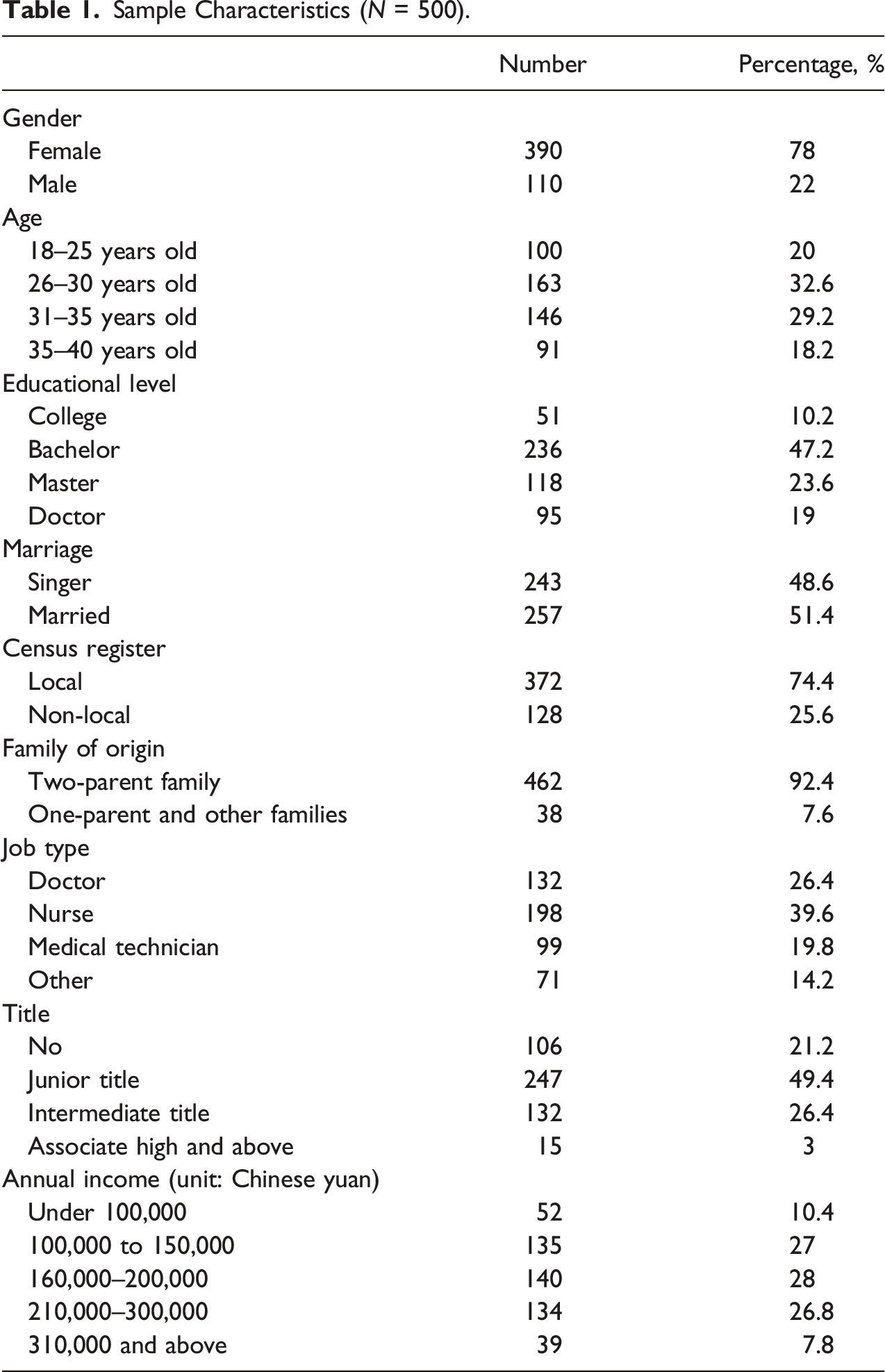
This study was conducted from October to November 2022. Since the prevention and control of the COVID-19 epidemic in China were still strict at that time, we collected data via the online platform. The online survey made it convenient to get data and was generally equivalent to the paper-and-pencil approach (Weigold et al., 2013). Snowball sampling recruited participants from the Class A tertiary hospitals in Shanghai. Since medical workers were in our research team, the snowball approach helped expand samples and access new participants (Biernacki & Waldorf, 1981). The inclusion criteria of participants were medical workers who: a) worked in the Class A tertiary hospitals in Shanghai and b) were aged 18–40. Participants were also informed of the anonymity of their responses, and no identifiable personal information was included. Ethics approval was granted by the Ethics Committee of Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. Finally, a total of 582 medical workers were collected, and 500 valid samples were included in the analysis of this study, excluding ineffective samples such as short answering time and conflicting information.
Sample Characteristics (N = 500).
Dependent Variable
Marital Decisions
Marital decisions include marital choice, marital time, premarital cohabitation, and the number of children. First, the marital choice was measured using the questions “Will you get married?” and “Will you have children,” the answer was yes or no. Married respondents who had children chose according to their current situation. Based on respondents’ answers, marital choice can be divided into two types: traditional choice (choose to marry and childbearing) and modern choice (marriage only, childbearing only, and no marriage). Second, marital time decisions were the age of marriage and childbearing. Excluding the sample that did not intend to marry and have children, respondents' marital time decisions could be divided into two types: marriage before age 30 and after age 30, and childbearing time decisions could also be divided into two types: having children before age 30 and after age 30. Third, the premarital cohabitation decision was measured by the item “Would you choose to live together before marriage,” and the response options were yes or no. Fourth, the number of child decisions is the number of children people intend to have, with response options of 0, 1, 2, and above.
Independent Variables
Martial Beliefs
The development of the measurement for assessing marital beliefs has three phases. Firstly, according to the marital paradigm framework, six dimensions of marital beliefs were initially identified, including marital timing, marital salience, marital context, marital process, marital permanence, and marital centrality (Willoughby et al., 2013, 2021; Willoughby & Hall, 2015). After the discussion of our research group, the marital process was divided into two specific dimensions, namely, marital relationships and gender roles. Secondly, ten young medical workers (5 males and 5 females; mean age = 31.30) were interviewed to identify the critical dimensions for them. Five dimensions are determined: marital salience, marital context, gender roles, marital permanence, and marital relationship. According to the above five dimensions of marital beliefs, we further searched relevant developed measurement tools, such as marital paradigms (Willoughby et al., 2013, 2021; Willoughby & Hall, 2015), trends in attitudes toward family issues (Thornton & Young-DeMarco, 2001), attitudes toward fertility and childbearing scale (Söderberg et al., 2013), marital context (Leonhardt et al., 2020), traditional view of marriage (Taylor & Vogel-Ferguson, 2015), attitudes toward marriage and child rearing scales (Adams et al., 2007), dynamic marriage (Kwong & Yin, 2000), marital meaning (Hall, 2006), and formed a 51-item pool. Thirdly, we established a triangular group to translate the English items into Chinese and make them more easily understandable. Through the discussion of the research group, 18 items were finally selected, including 3–4 items for each dimension. Specifically, four items for marital salience (i.e., marriage is more important than career success; being married has more benefits than being single and unmarried; having a happy and fulfilling marriage is an important achievement in life; I can’t accept not having children in my future life), four items for marital context (e.g., I got married because I do not want to be alone anymore; sexual needs are an important factor in getting married; I married for better financial conditions; children are an important consideration for me when I get married), three items for gender roles (e.g., men should earn money to support the family and women are responsible for taking care of the family; Men should be the ones making the really important decisions; Women have the freedom not to have children), three items for marital permanence (e.g., even if the marriage is unhappy, I will not divorce for the sake of the children; I will choose divorce if the marriage is unhappy; marriage is a lifetime choice, divorce is bad), and four items for marital relationships (e.g., love is the foundation of marriage and childbearing; couples should learn to adjust and improve when they encounter problems in their marriage; in marriage, increasing commitment to the spouse is necessary; a good relationship between husband and wife is more important than a parent–child relationship). A five-point Likert scale ranged from “completely disagree = 1” to “completely agree = 5.” The higher the average score, the higher the agreement with the corresponding dimension. The measurement occupied a good internal consistency coefficient (Cronbach’s alpha = .83) in this study.
Satisfaction with Marital Policies
One item, “How satisfied are you with the current marriage and child welfare policy,” was measured on a scale ranging from “very dissatisfied = 1” to “very satisfied = 5”. The higher the score, the higher the overall satisfaction with marital policies and services.
Work Stress
Work stress refers to the stress medical workers face during the prevention and control of the COVID-19 pandemic. Ten items were developed according to the interviews of medical workers. The items include heavy workload, physical and mental exhaustion, fear of infection, pressure from public opinion, worried about infecting family members, and five reverse scoring items, such as well organized, adequate medical supplies, positive co-operation from patients, meaningful, and rewarding. A five-point Likert scale ranged from “completely disagree = 1” to “completely agree = 5.” The higher the mean score, the higher the work stress. The Cronbach’s alpha of measurement was .70 in the current study.
Social Support
The social support instrument was the Perceived Social Support Scale (Blumenthal et al., 1987), which has been used by Chinese people (Jiang, 2001). A total of six items were used in this study (e.g., I can get emotional help and support from my family). A five-point Likert scale ranged from “strongly disagree = 1” to “strongly agree = 5.” The higher the average score, the higher the level of social support. The Cronbach’s alpha of measurement was 0. 91 in this study.
Analytical Strategy
The analysis process of this study is as follows: First, the dimensions and structures of marital beliefs are examined through factor analysis. Secondly, descriptive statistical analysis was carried out to understand the current situation of young medical workers’ marital beliefs and decisions. Finally, binary and multiple logistic regression analyses were conducted to explore the effects of demographic variables, marital beliefs, work stress, social support, and satisfaction with marital policies on young medical workers' marital decisions.
Results
Factor Analysis of Marital Beliefs
Factor Loadings of the Marital Beliefs (N = 500).
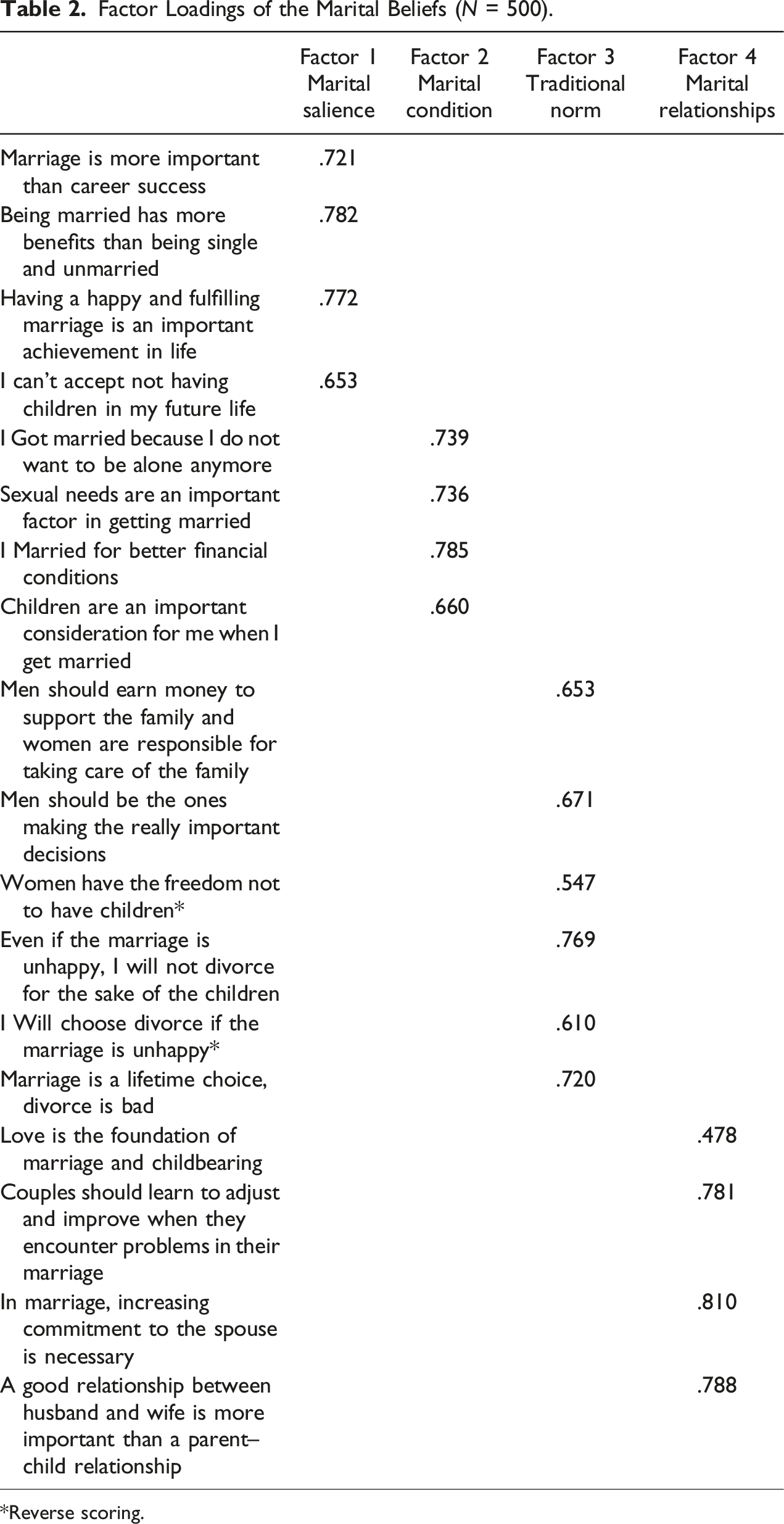
*Reverse scoring.
Descriptive Statistical Analysis of Marital Beliefs and Decisions
In the total sample, the mean scores for marital relationships, marital salience, marital context, and traditional norms were 3.89, 3.12, 2.64, and 2.11, respectively. It can be seen that young medical workers value marital relationships the most, followed by marital salience and marital condition, while the score of traditional norms was the lowest.
For marital decisions, 82.6% of participants said they would marry, and 77% said they would have children. 75.6% of respondents said they would marry and have children, while 24.4% would make modern marital choices. Among those who decide to marry, most participants decide to marry before the age of 30, and more of them would live together before marriage. The decision to have children before 30 was also predominant among respondents who decided to have children. The decision to have only one child was predominant, with the majority having no preference for the sex of the child.
Regression Analysis of Factors Influencing Marital Decisions
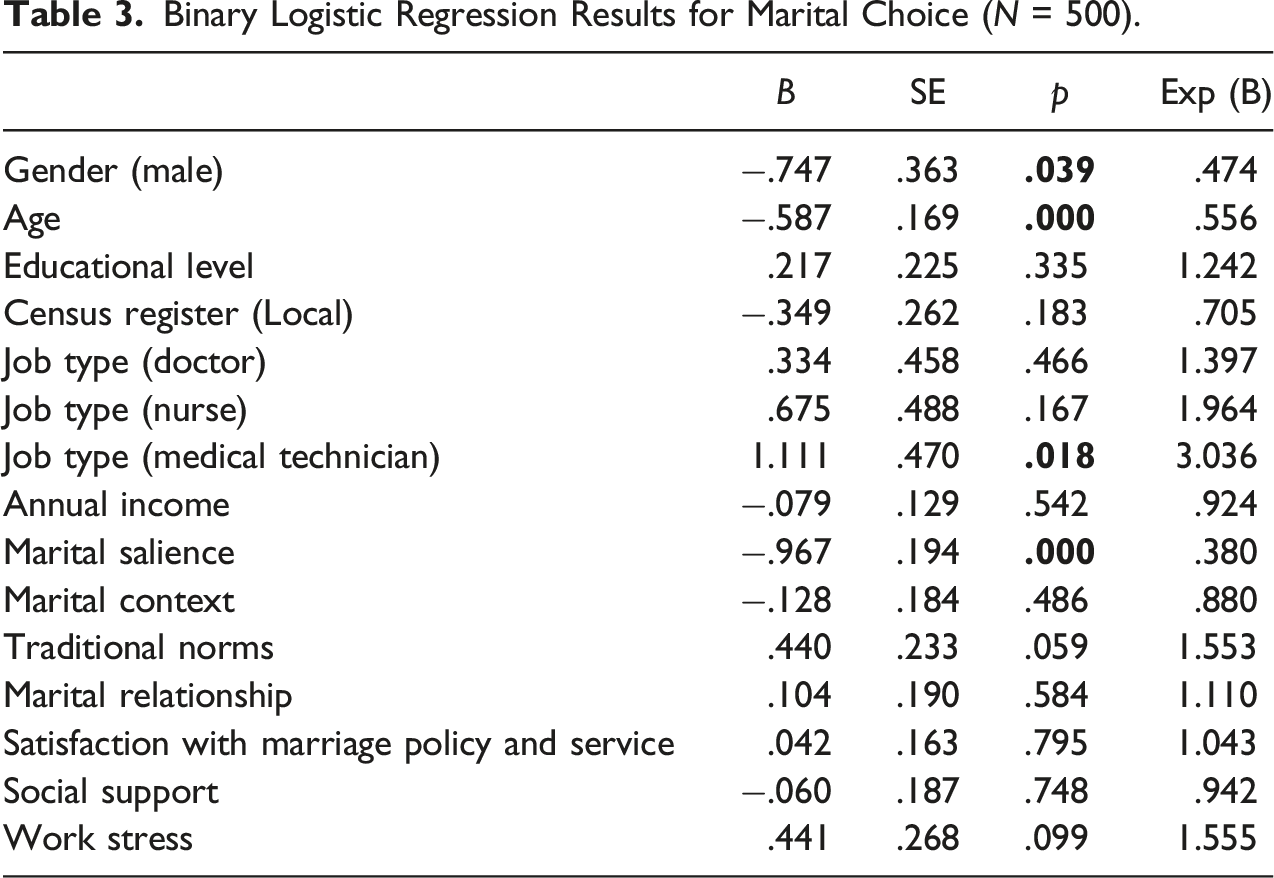
Factors Influencing Marital Choices
Binary Logistic Regression Results for Marital Choice (N = 500).
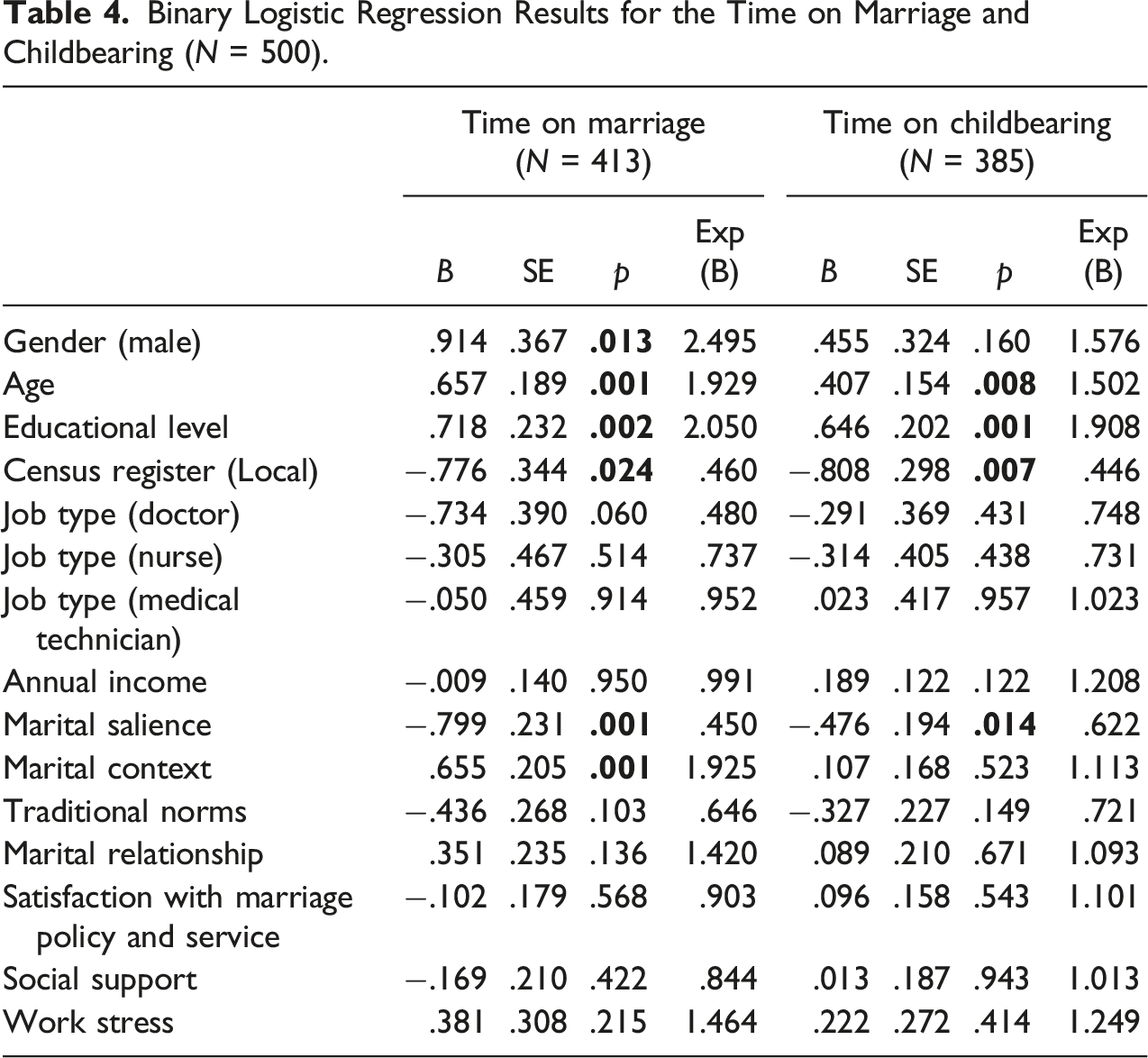
Factors Influencing the Time of Marriage and Childbearing
Binary Logistic Regression Results for the Time on Marriage and Childbearing (N = 500).
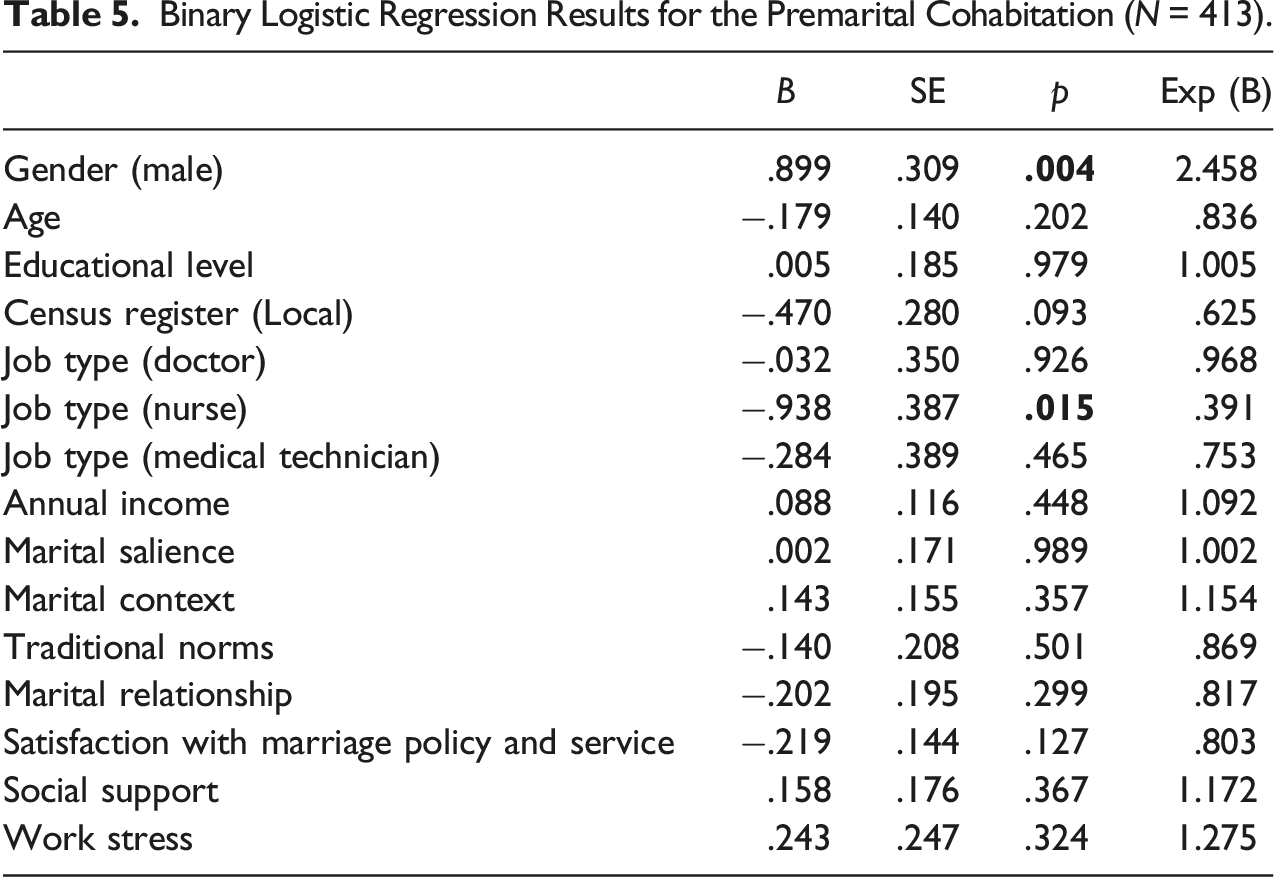
Factors Influencing the Cohabitation Before Marriage
Binary Logistic Regression Results for the Premarital Cohabitation (N = 413).
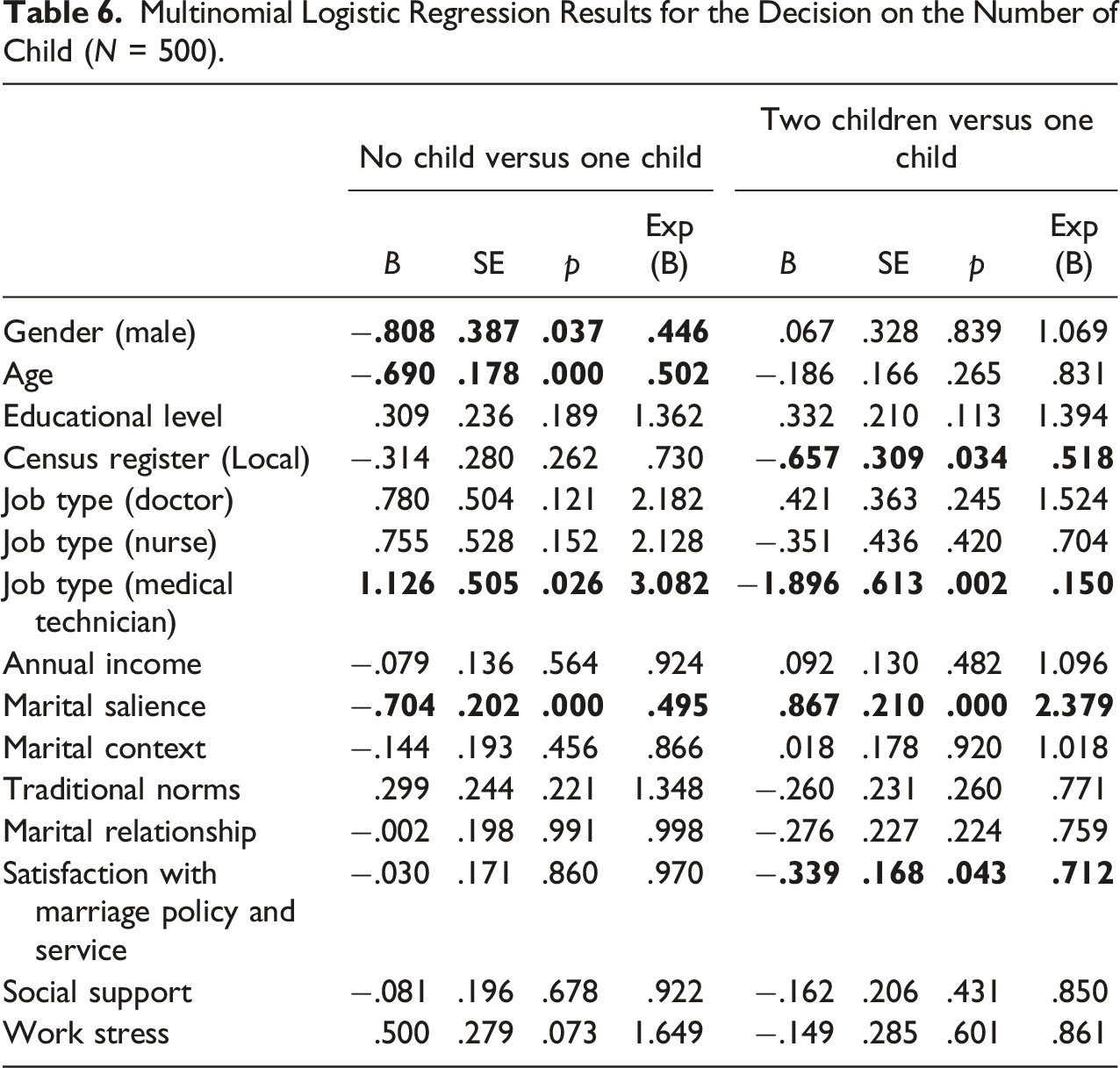
Factors Influencing the Decision on the Number of Children
Multinomial Logistic Regression Results for the Decision on the Number of Child (N = 500).
Discussion
This study aims to analyze the marital decisions and their influencing factors of young medical workers in China. The investigation of 500 young medical workers showed that about 75.6% of young medical workers said they would marry and have children, and 63.2% and 43.4% of young medical workers chose to marry and have children before 30, respectively. About 45% of participants decided to cohabitate before marriage, and 54% chose to have one child. Among the four dimensions of marital beliefs, young medical workers attach the most importance to marital relationships, followed by marital salience, marital context, and traditional norms. For the influencing factors of marital decisions, marital salience has a significant influence on different types of marital decisions; marital context have an impact on the time of marriage; higher satisfaction with marital policies does not make young medical workers more willing to have two children; work stress and social support have no influence on marital decisions; demographic variables could impact the marital decisions of young medical workers.
This study analyzed the marital decisions and beliefs of young medical workers, and the results are consistent with the existing studies, but there were new findings. For the similarities, the marital decisions of young medical workers reflect the characteristics of modern marital behaviors. A proportion of young people choose not to marry, not to have children, to marry later, to have children later, to have fewer children, and the marital beliefs reflect individualism and the importance attached to personal feelings. For example, Li et al. (2022) indicated that the marital beliefs of young adults are changing from traditional to modern; they pay more attention to their emotional needs and enjoyment of life, and their beliefs in traditional marital norms and functions have significantly decreased. Coontz (2007) concludes that the modern beliefs of marriage elevate the marital relationship above all other personal and family commitments, with increased conjugal emotions, passion, and personal identity, and the constant decay of other emotions and obligations. The findings of this study were consistent with existing research on young adults’ marital beliefs. However, shifts in marital decisions have lagged behind shifts in beliefs. In other words, the traditional beliefs of gender roles and the permanence of marriage have been abandoned, and the beliefs in pursuit of personal enjoyment, intimate relationship, and emotional satisfaction have been widely recognized. While for the marital decisions, most young medical workers still choose to marry and have children (75.6%), and modern marital behavior is not widely accepted by young people. Therefore, the degree of modernization of marital beliefs exceeds the degree of modernization of marital behavior.
The current study identified the influences of the four dimensions of marital beliefs on marital decisions. Interestingly, among the four dimensions of marital beliefs, only marital salience significantly impacts decisions. The more people consider marriage and childbearing unimportant, the more likely they choose modern marital decisions (i.e., remain unmarried, no children, late marriage, and childbearing). Marital context only affects the decision to marry, possibly because more considerations are taken before marriage (Leonhardt et al., 2020). The effects of traditional norms and marital relationships on marital decisions were not significant. Although young people generally attach importance to marital relationships, which are not the determining factor in marital decisions. The further analysis showed that there were no significant differences in the scores on marital relationships of various marital decisions groups. Participants all value marital relationships, but have different views on marital salience. Therefore, improving young medical workers’ awareness of marital salience is conducive to promoting marital behaviors, and strengthening marital counseling is conducive to improving the satisfaction of marriage and the well-being of individuals.
For other factors, satisfaction with the welfare policy only affects the decision about the number of children. The increased satisfaction with the welfare policy does not make individuals more willing to have two children. As Yang and Wu (2021) conclude, people are shifting from being influenced by fertility cost constraints to pursuing intrinsic happiness in their fertility decisions. Policies can impact people’s marriage decisions in the short term but have limited impact in the long term. Moreover, work stress and social support do not significantly affect young medical workers’ decisions of marriage and childbearing. Nevertheless, results from the impact of job type on marital decisions of young medical workers showed that medical technicians were more likely to decide not to marry, infertility, and fewer children, which was associated with their lower scores on the importance of marriage and children; nurses were less likely to choose premarital cohabitation, which may be related to the fact that the group of nurse is predominantly female and women are less likely to choose premarital cohabitation than men (Williams et al., 2007). The marital services should be targeted for different job type of medical workers.
This study identifies demographic variables influencing young medical workers’ marital decisions. Women were more likely than men to make new marriage choices, and the younger the age, the more likely they would make modern marital choices. A study using data from the National Household Survey shows that both men and women believe that men need marriage more than women; women are more likely to agree that they can have a satisfying life without it, and younger people are less likely to emphasize the need for marriage (Kaufman & Goldscheider, 2007). The more educated, the more medical workers will likely postpone marriage and childbearing. The correlation between increased educational attainment and delayed marriage may lie in the time conflict between schooling and marriage, with higher educational attainment implying an increase in age and a corresponding delay in marriage and childbearing. Men were more likely to cohabit before marriage and postpone marriage age. In a study of cohabitation, although young people are still more conservative in their attitudes towards cohabitation, men are more likely to cohabitate than women (Williams et al., 2007). Among the effects of household registration on young medical workers' marital decisions, those with non-local household registration were more likely to choose to marry and have children later. Peng et al. (2022) found that the risks of cohabitation and late marriage among the mobile population are on the rise. The risks of late marriage, cohabitation, and non-marriage increase as the range of mobility expands. Moreover, the migratory population is under pressure from various sources when making marriage decisions, such as housing, parenting, and health care (Yang & Xu, 2018).
There are several limitations. Firstly, this study measured satisfaction with marital policies and services through one item, which resulted in no specific analysis of the impact of different policies and services on the marital decisions of young medical workers. Secondly, the marital paradigms theory provides a comprehensive framework for us to understand the dimensions of marital beliefs. However, the framework was moderately adapted during the process of the study, and ultimately several of the original dimensions were not used in the analysis. Future research could comprehensively analyze the impact of the six dimensions of marriage paradigm theory on marital decisions. Thirdly, the cross-sectional study design could have been more conducive to capturing changes in young medical workers' marital beliefs and decisions, and future research could verify changes in marital beliefs and decisions through a longitudinal design. Finally, while this study mainly examined the effects of demographic variables, marital beliefs, social support, and work stress on marital decisions, the influence of other factors on marital decisions, such as family background, deserves further exploration.
Conclusion
Marital beliefs and decisions of young medical workers are changing, especially marital beliefs. Traditional marital norms and gender roles are abandoned, and personal emotions and marital relationships are seen as essential and primary. Although there were new phenomena of marital decisions, most young medical workers still choose to marry and have children. The influence of marital beliefs on the decision is mainly due to different views on marital salience. The analysis of factors influencing marital decisions reveals that significant factors were mainly at the individual level, such as gender, age, education, and marital beliefs. Neither social support nor work stress was a significant factor in deciding marriage and childbearing, nor was a high level of satisfaction with marital policy an incentive to have more children. The findings suggest individualized factors significantly impact young medical workers' marital decisions. Therefore, in the future practice of marriage and family services, on the one hand, attention should be paid to the marital beliefs and decisions of different groups, taking complete account of individual differences. On the other hand, improving young medical workers' awareness of marital salience is conducive to promoting marital behaviors, and helping them improve their intimate relationships is conducive to the longevity of intimate relationships and the well-being of individuals.
Footnotes
Acknowledgments
The authors thank their participants for their generous contributions to this research.
Author Contributions
Kaixuan Ma contributed to conception, design, and analysis; drafted the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Qiujie Guan contributed to conception, design, and analysis; drafted the manuscript; revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Weiwei Cheng contributed to conception, design, and analysis. Yang Niu contributed to design and analysis. Yijun Zhou contributed to analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 2022 Shanghai Youth Work Research Project (2022QYKTLX8-8)
Transparency and Openness Statement
The raw data, analysis code, and materials used in this study are not openly available but are available upon request to the corresponding author. The design, data collection and analysis were not pre-registered.