
Abstract
Adverse childhood experiences (ACEs) are linked to numerous poor mental health outcomes that affect vulnerable children and families. This study examined the prevalence of children’s ACEs and their association with emotional support-seeking among immigrant caregivers in low-resource communities in the United States. Using cross-sectional data from the 2023 National Survey of Children’s Health (N = 7,746), two complex logistic regression analyses were conducted to examine the association between children's ACEs and caregivers' emotional support-seeking. Approximately 57.2% of immigrant caregivers sought emotional support during the past 12 months, and 63.3% had children exposed to atleast two or more ACEs. Caregivers of children who experienced parental divorce and family mental illness had greater odds of seeking emotional support. However, immigrant caregivers of children exposed to atleast one ACE, and two or more ACEs had lower odds of seeking emotional support. These findings underscores the need for trauma-informed, culturally and linguistically responsive mental health and social support services for immigrant caregivers and their children experiencing adversities in low-resource communities in the U.S.
Keywords
Introduction
Adverse childhood experiences (ACEs) were first conceptualized during the late 1990s through a groundbreaking study conducted by the Centers for Disease Control and Prevention and Kaiser Permanente (Felitti, 1998). Initially, ACEs were defined as potentially traumatic events, including maltreatment (physical, emotional, and sexual abuse), neglect (emotional or physical), and household or familial dysfunctions (i.e., household alcohol or drug use, incarceration, or mental illness, and parental divorce or separation) that occur before age 18 (Felitti, 1998). Similar to the original definition, other scholars have expanded to define ACEs as potentially traumatic events that occur to a child between 0 to 17 years old that include experiencing violence, abuse, neglect, witnessing violence in the home or community, and having a family member die or attempt suicide (Merrick, 2019). These existing ACE frameworks serve as a foundation for modeling our understanding of how numerous early-life adversities negatively affect long-term well-being, and are used to inform numerous policy, clinical, and public health interventions in low-resource settings (Amos et al., 2023; Jackson et al., 2019). Although traditional ACEs frameworks have predominantly been used as frameworks (Felitti, 1998), recent studies have broadened the ACEs perspective beyond the traditional model to include discrimination, homelessness, and economic hardships in household and community contexts (Afifi, 2020; Census Bureau, 2023; Chipalo & Odii, 2025a; Karatekin et al., 2022; Karatekin & Hill, 2019). For instance, the National Survey of Children’s Health (NSCH) defines ACEs as potentially stressful or traumatic events that occur during childhood and may negatively affect a child’s physical, mental, and emotional health, behavioral development, and long-term life outcomes (Census Bureau, 2023). In the NSCH, ACEs commonly include experiences such as economic hardship, parental separation or divorce, parental incarceration, exposure to domestic or neighborhood violence, living with someone with substance use or mental illness, and experiences of discrimination (Census Bureau, 2023).
Regardless of the theoretical framework used to conceptualize ACEs, all ACEs share common risk characteristics that lead to a wide range of poor outcomes (Jaen et al., 2023). For instance, a multitude of studies have emerged linking ACEs to a wide range of poor outcomes affecting physical, mental, and behavioral well-being, and socioeconomic conditions of individuals in resource-constrained settings (Amos et al., 2023; Chipalo, 2023, 2024a, 2024b, Chipalo et al., 2025a, 2025b, 2026a, 2026b; Chipalo & Bloomer, 2026; Chipalo & Eya, 2026; Chipalo & Jeong, 2023; Chipalo & Odii, 2025a, 2025b, 2026, Hughes et al., 2023, 2025). These enduring ACEs can have long-lasting negative effects on health and well-being, including difficulty regulating emotions and behavioral problems, and other challenges such as limited education opportunities, disrupting academic performance and employment prospects later in adulthood (Anderson, 2022; Cronholm et al., 2015; Karatekin et al., 2022; Karatekin & Hill, 2019; Sacks & Murphey, 2018; Turney, 2014). ACEs can also increase the risk of sexually transmitted infections, injury, involvement in sex trafficking, and maternal and child health problems, including teen pregnancy, pregnancy complications, fetal death, and a range of chronic diseases and leading causes of death, such as cancer, diabetes, heart disease, and suicide (CDC, 2026; Chipalo, 2023a).
Although numerous studies primarily focus on assessing ACEs and their later consequences in adulthood (Crandall et al., 2019), scholars often overlook the role of emotional support-seeking among caregivers of children with multiple ACEs in low-resource settings (Hughes et al., 2023). Emotional support is defined as the process of providing comfort, validation, empathy, and encouragement to individuals experiencing emotional distress, thereby improving their emotional well-being (Liu et al., 2021). Emotional support can be obtained through informal networks, such as spouses, friends, neighbors, and extended family, or through formal avenues, including mental health professionals, social service providers, therapists, and structured peer support groups (Edwards & Gillies, 2004). However, how individuals access emotional support varies across sociocultural settings and may be influenced by perceived cultural norms, stigma, and the availability of social capital in their communities (Vogel et al., 2006). Studies have shown that emotional support plays an important role in mitigating the negative effects of caregiving stress and fostering family resilience, particularly in the context of exposure to various dimensions of adversities or challenging behaviors exhibited by children in under-resourced household settings (Bethell et al., 2017; Herbell et al., 2020; Hughes et al., 2023; Westphaln et al., 2022). Drawing from Lazarus and Folkman (1984) the transactional model of stress and coping, it is stated that individuals experiencing unenduring chronic stress often engage in support-seeking during difficult times as a way of regulating their emotionally charged stress. For caregivers in low-resource communities, this is a significant issue. For caregivers of children with behavioral or trauma-related challenges, access to emotional support may help reduce caregiver burden, enhance psychological well-being, and promote positive parenting practices in households with low resources (Brannan et al., 1997; Carmassi et al., 2021; Stewart et al., 2006).
By contrast, immigrant caregivers’ emotional well-being is frequently overlooked in most of the emerging research conducted in the U.S. and other low-income countries (Chipalo, 2023a, 2024a, 2024b, 2024c; Amos et al., 2023; Chipalo & Jeong, 2023; Chipalo, Nkwanzi, et al., 2025; Chipalo & Odii, 2025a, 2025b; Hughes et al., 2023, 2025; Vaughn et al., 2017). Despite this, Zayas et al. (2015) found that Latina immigrant mothers of traumatized children experience numerous emotional burdens and highlighted the need for culturally responsive interventions. Immigrant caregivers may encounter resettlement stressors, such as low-paying jobs, discrimination, limited education opportunities, and language and cultural barriers in their communities. These resettlement adversities inevitably make it more difficult for vulnerable caregivers to regulate their emotions due to insurmountable stressors that may result in child maltreatment practices (Alink et al., 2013). Other potential challenges that immigrant parents face in their communities may include the combined effects of structural inequality, discrimination, cultural dislocation, and systemic barriers, which can further exacerbate the cumulative negative developmental impact of ACEs on children and parental distress in low-resource communities (Perreira & Ornelas, 2011). Despite immigrant caregivers having resilience and adaptive coping skills to overcome seeking emotional support (Hughes et al., 2023), immigrant caregivers are also vulnerable to insurmountable barriers such as limited English skills, unfamiliarity with social service systems, limited social networks, and cultural stigmas surrounding mental health (Pumariega et al., 2005). In some communal or collectivist cultures, emotional concerns may be managed within large extended family systems, potentially reducing the need for formal help-seeking for emotional or mental health needs (Kagitcibasi, 2017). However, immigrant caregivers oftentimes exhibit remarkable resilience, drawing strength from religious institutions, ethnic communities, and family ties to cope with the stresses of caregiving in low-resource communities (Domènech Rodriguez et al., 2009).
Equally important, regardless of the immigration status of caregivers, caregivers of children with ACEs may be overwhelmed by emotional stress that can hinder their ability to provide responsive, nurturing care to their children (Vivrette et al., 2018). Consequently, continuous access to supportive caregiver-child interactions is very important for building strong resilience and adaptive coping skills and for mitigating the negative psychological impact of ACEs on caregivers living in resource-limited settings (Yoshikawa et al., 2012). In order to address emotional distress complications and maintain effective caregiving practices, parents often turn to emotional support from both formal and informal sources. Seeking emotional support is an important coping strategy that enables caregivers to navigate the challenges of parenting during difficult times (Herbell et al., 2020; Hughes et al., 2023; Taylor, 2011). While immigrant families may experience resettlement stressors and adversity, prior studies also highlight several strengths and protective factors that can foster resilience and promote positive health outcomes in immigrant communities with low resources. For example, the “immigrant health paradox” suggests that many immigrant populations exhibit better physical and mental health outcomes than expected, despite socioeconomic disadvantages and migration-related stressors (Coll & Marks, 2012). Additionally, ethnic enclaves and culturally connected communities may provide social cohesion, cultural continuity, and access to informal support systems that buffer against stress and psychological distress (Osypuk et al., 2009). Strong family relationships, kinship networks, and community support systems within immigrant communities have also been identified as important protective factors that promote coping, emotional support, and resilience among immigrant caregivers and their children (Suárez-Orozco et al., 2018).
Moreover, emerging studies have documented how exposure to adversities affects both children and their caregivers in low-resource settings (Bethell et al., 2017; Herbell et al., 2020; Hughes et al., 2023; Westphaln et al., 2022), significant gaps remain in existing studies linking children’s ACEs to their caregivers’ emotional distress. While existing studies have demonstrated that caregivers of children exposed to ACEs experience insurmountable psychosocial strain in their households (Felitti, 1998; Yoshikawa et al., 2012), few studies have systematically examined the association between distinct children’s ACE domains and caregivers’ emotional support-seeking behaviors in resource-constrained settings (Hughes et al., 2023). In addition, the current literature remains largely qualitative and lacks the scale and generalizability needed to inform broader policy or programmatic health interventions for caregivers low-resource settings. Emotional support is widely recognized as a key protective factor that can buffer the psychological effects of caregiving stress, especially in the face of adversity (Hughes et al., 2023). However, the pathways through which child-level ACEs influence caregiver-level support-seeking remain underexplored in quantitative research (Taylor, 2011). For instance, a recent study by Hughes et al. (2023) explored emotional support linking with ACEs among older adult populations, but did not extend its analysis to caregivers of minor children, particularly immigrant caregivers who may be navigating complex stressors related to cultural adaptation, systemic marginalization, and resettlement challenges in their communities.
Purpose of the Study
Given that numerous studies have shown that immigrant caregivers often experience structural barriers, including language difficulties, limited access to mental health resources, discrimination, and cultural stigmas surrounding emotional expression (Chipalo, 2024c; Guruge & Khanlou, 2004; Hughes et al., 2023; Pumariega et al., 2005), it is particularly important to examine how these vulnerable immigrant caregivers manage the emotional demands of caring for children with ACEs in households with limited resources (Hughes et al., 2023). Emotional support can serve as a non-medical health service, enhancing caregiver resilience and improving their overall quality of life and well-being in challenging circumstances (Hughes et al., 2017; Stewart et al., 2006).
The present study is guided by the Andersen Behavioral Model (ABM) (Andersen, 1968, 1995), which posits that service utilization is shaped by perceived predisposing factors (e.g., race, ethnicity), enabling factors (e.g., health insurance, social support), and need factors (e.g., stress or illness). The ABM framework posits that having a child exposed to ACEs constitutes a clear need that may motivate caregivers to seek emotional support as a coping strategy for stressful experiences (Hughes et al., 2023). The ABM suggests that as ACEs-related needs increase, parents are more likely to seek higher levels of emotional support care. Given the protective role of emotional support as a key component of well-being, sources of emotional support could be considered a non-medical health services (Hughes et al., 2023).
In order to address the significant gaps in existing knowledge, this study aims to: (1) Determine the prevalence of emotional support-seeking among immigrant caregivers with children who have experienced ACEs, and (2) Examine the association between children’s ACEs and immigrant caregivers’ emotional support-seeking in low-resource settings in the U.S. Therefore, this study hypothesizes that immigrant caregivers with children who experienced more ACEs will be more likely than those without ACEs to seek emotional support during the past 12 months. Therefore, this study seeks to contribute to a more nuanced understanding of how immigrant caregivers may respond to childhood trauma and to inform the development of culturally and contextually appropriate mental health interventions and policies for trauma-informed caregiving practices to strengthen resilience and emotional well-being of caregivers in households with limited resources in the U.S.
Methods
Data Source
This study used data from the 2023 National Survey of Children’s Health (NSCH), a cross-sectional survey conducted via web and paper for non-institutionalized U.S. children aged 0 to 17 years. The 2023 NSCH provides annual state-level and nationally representative estimates of child health and healthcare indicators (Census Bureau, 2023). The U.S. Census Bureau conducted this survey on behalf of the Health Resources and. The Maternal and Child Health Bureau of the Health Services Administration and the U.S. Department of Health and Human Services provided oversight and funding for this survey. The annual NSCH data are publicly available and provide detailed information on children’s social and environmental contexts, their health and mental health, and their families’ experiences with healthcare and support services. Parents or caregivers act as proxies to answer on behalf of their children (Census Bureau, 2023). Datasets are weighted to produce nationally representative estimates of non-institutionalized children under 18 years old living in U.S. households. The final unweighted analytic sample included 55,126 children. However, in the current study, we focused primarily on immigrant caregivers who reported being born outside the United States. Therefore, the sample size was reduced to 7,746 immigrant caregivers of children who responded to ACE-listed items. Detailed descriptions of the survey design are available at https://www.census.gov/programs-surveys/nsch/data/datasets.2023.html.
Ethical Considerations
The 2024 NSCH dataset used in the current study has been de-identified and is publicly available. Therefore, this study was exempted by the author’s Institutional Review Board at the University of Cincinnati.
Dependent Variable
Caregivers’ emotional support seeking was measured by asking caregivers the following question: “During the past 12 months, was there someone that you could turn to for day-to-day emotional support with parenting or raising children?” Responses were coded dichotomously as yes or no. Therefore, a “no” response indicated the absence of emotional support, and a “yes” response indicated the presence of emotional support-seeking during the past 12 months.
Independent Variables
Children’s adverse childhood experiences (ACEs), which were reported by caregivers are used as primary independent variables of interest in this study. This study used the ACEs measures derived from the NSCH (Census Bureau, 2023), a widely used measure that differs slightly from the original ACE measure (Felitti, 1998). Parents/caregivers were asked if the child had ever experienced the following: (1) Economic hardship (hard to cover basics like food or housing), Parental divorce/separation (parent or guardian divorced or separated), Parental death (parent or guardian died), (4) Parental incarceration (parent or guardian served time in jail or prison), (5) Exposure to violence (saw or heard parents ort adult slap, hit, punch one another in the home; and was a victim of violence or witnessed violence in their neighborhood), (6) Familial mental illness (lived with a family member who was mentally ill, suicidal, or severely depressed), (7) Familial substance use problem (lived with someone who has problems with alcohol or drug use), (8) Discrimination (treated or judged unfairly because of race, or health condition). All these items resulted in 8 binary measures indicating whether a child had experienced each adverse event and were dichotomously coded as “yes or no.” In addition, we created a cumulative ACE scores by summing each item, yielding a total score ranging from 0 to 8. A cumulative binary measure of ACEs was created by categorizing children into 0, 1, or 2 or more ACEs. The study is consistent with previous studies that have used the NSCH data to distribute ACEs in a similar manner (Baiden et al., 2024; Chipalo, 2024b; Chipalo, Nkwanzi, et al., 2025; Chipalo & Odii, 2025a; Hughes et al., 2023).
Control Variables
Control variables were selected based on the Anderson Behavioral Model (ABM), which includes predisposing, enabling, and need-of-care factors (Andersen, 1968; Andersen, 1995; Hughes et al., 2023). Predisposing factors included the child’s sex (0 = female, 1 = male), age group (0 = 0–5 years, 1 = 6–11 years, 2 = 12–17 years), and race/ethnicity (0 = White alone, 1 = Black/African American, 2 = Other), and caregiver’s sex (0 = male, 1 = female) and caregiver age, which was measured continuously. Enabling factors included marital status (0 = other, 1 = married), parental education level (0 = high school or lower, 1 = some college/associate degree, 2 = college degree or higher), parental employment status (0 = no, 1 = yes), household income based on the federal poverty level (0 = ≤100% FPL, 1 = 100%–199% FPL, 2 = 200%–399% FPL, 3 = ≥400% FPL), language spoken at home (0 = English, 1 = Spanish/other), child’s health insurance coverage during the past 12 months (0 = no, 1 = yes), and neighborhood support measured by whether people in the neighborhood help each other (0 = low neighborhood support, 1 = neighborhood support). Need factors included caregiver and child health status. The original health status categories (poor, fair, good, very good, and excellent) were recoded into a dichotomous variable comparing excellent health (1 = excellent) versus not excellent health (0 = poor, fair, good, or very good) for analytic purposes.
Statistical Data Analysis
This study used survey weights and clustering to account for the complex sampling design and to calculate national estimates. First, univariate analyses involving descriptive statistics were used to compute frequencies and weighted percentages for categorical variables. For continuous variables, means and standard deviations were reported, particularly for caregivers' age. Bivariate analyses, including chi-square tests (cross-tabulations), were used to estimate the prevalence and association of children’s ACEs and immigrant caregivers’ emotional support-seeking during the past 12 months. Two complex logistic regression models assessed the association between ACEs and emotional support-seeking among caregivers during the past 12 months, adjusting for selected descriptive predisposing, enabling, and need factors. In Model 1, this study included each individual ACE and the cumulative ACE count, along with the outcome (emotional support-seeking during the past 12 months), without adjusting for predisposing, enabling, and need factors. In Model 2, all individual ACEs and the outcome were included while controlling for predisposing, enabling, and need factors. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were reported to indicate the strength of associations between selected predictors and the outcome (emotional support-seeking during the past 12 months). The significance level was set at p < 0.05. All statistical data analyses were performed using SPSS version 31.0.
Results
Sample Characteristics of Immigrant Caregivers
Sample Characteristics of Children and Immigrant Caregivers (N = 7746)
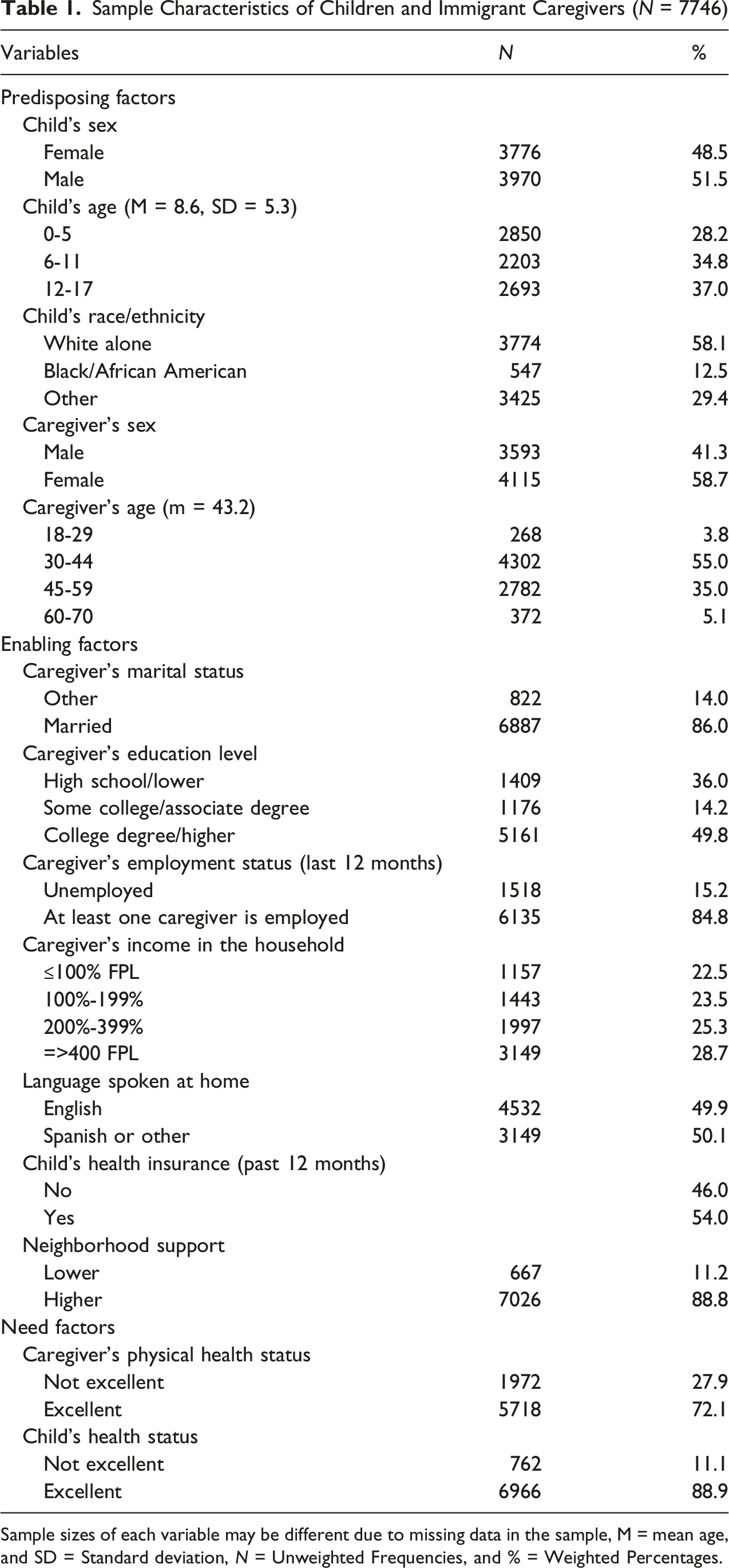
Sample sizes of each variable may be different due to missing data in the sample, M = mean age, and SD = Standard deviation, N = Unweighted Frequencies, and % = Weighted Percentages.
The Prevalence of Children’s ACEs and Immigrant Caregivers’ Emotional Support Seeking
The Prevalence of Children’s ACEs and Caregivers’ Emotional Support-Seeking Patterns (N = 7746)
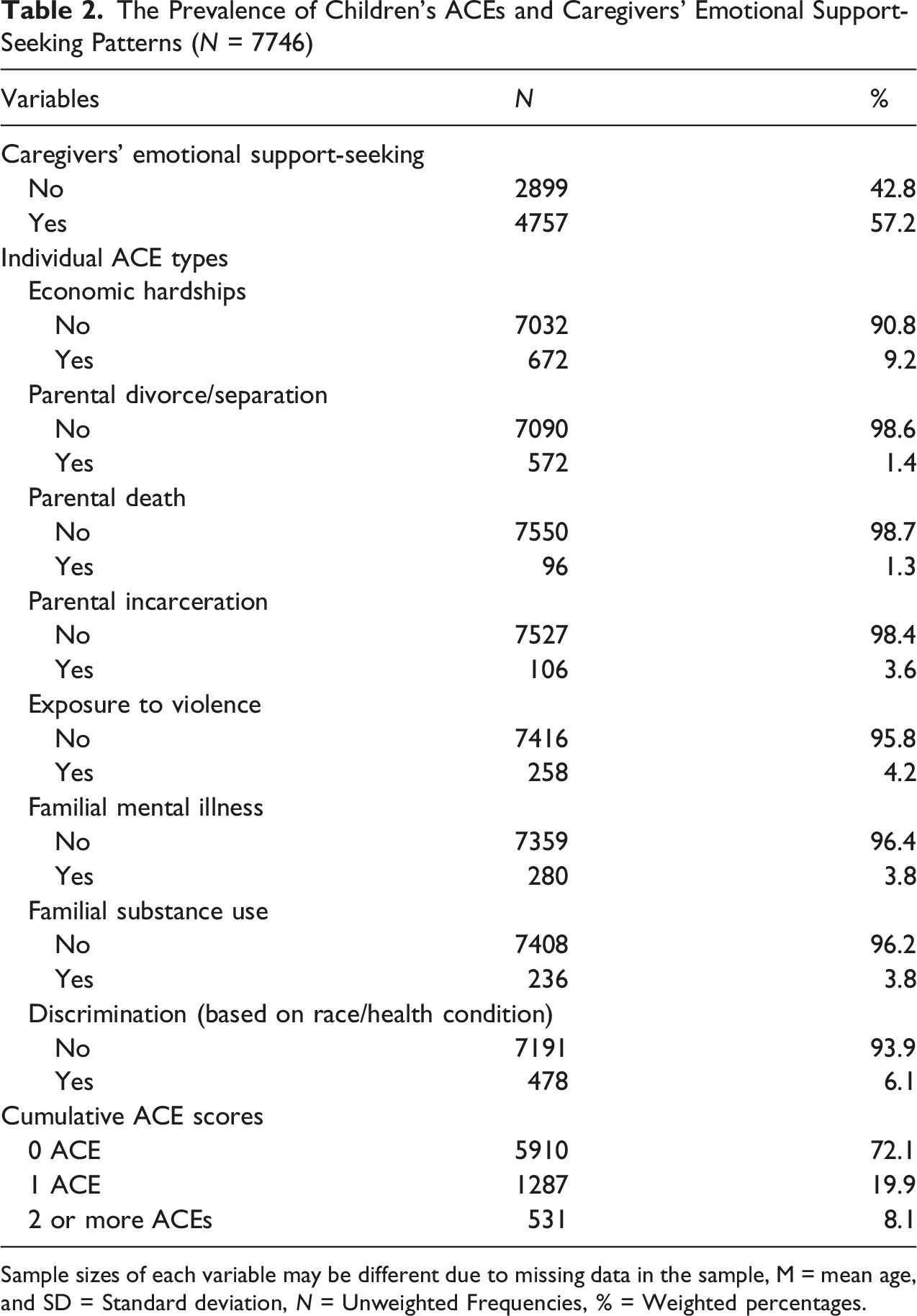
Sample sizes of each variable may be different due to missing data in the sample, M = mean age, and SD = Standard deviation, N = Unweighted Frequencies, % = Weighted percentages.
The Prevalence and Bivariate Association of Caregivers’ Emotional Support -Seeking with Children with ACEs
The Prevalence and Association of Children’s ACEs and Immigrant Caregivers’ Emotional Support-Seeking Patterns Among Immigrant Caregivers
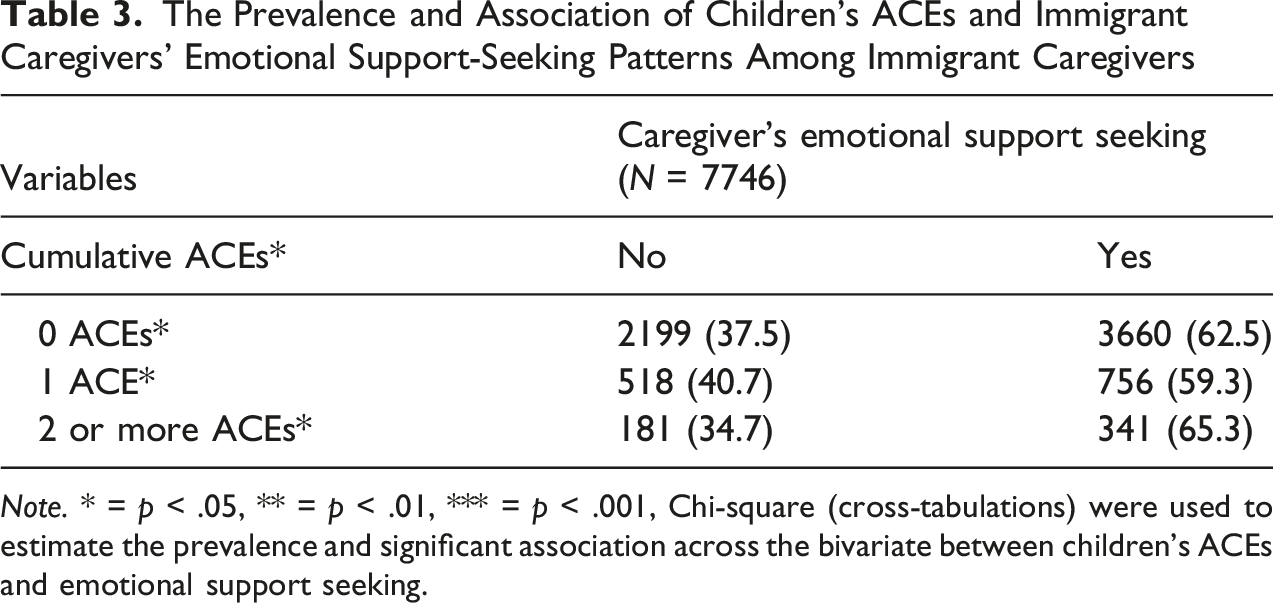
Note. * = p < .05, ** = p < .01, *** = p < .001, Chi-square (cross-tabulations) were used to estimate the prevalence and significant association across the bivariate between children’s ACEs and emotional support seeking.
Multivariate Association Between Children’s ACEs and Immigrant Caregivers’ Emotional Support-Seeking
Association Between Children’s ACEs and Immigrant Caregivers’ Emotional Support-Seeking Patterns
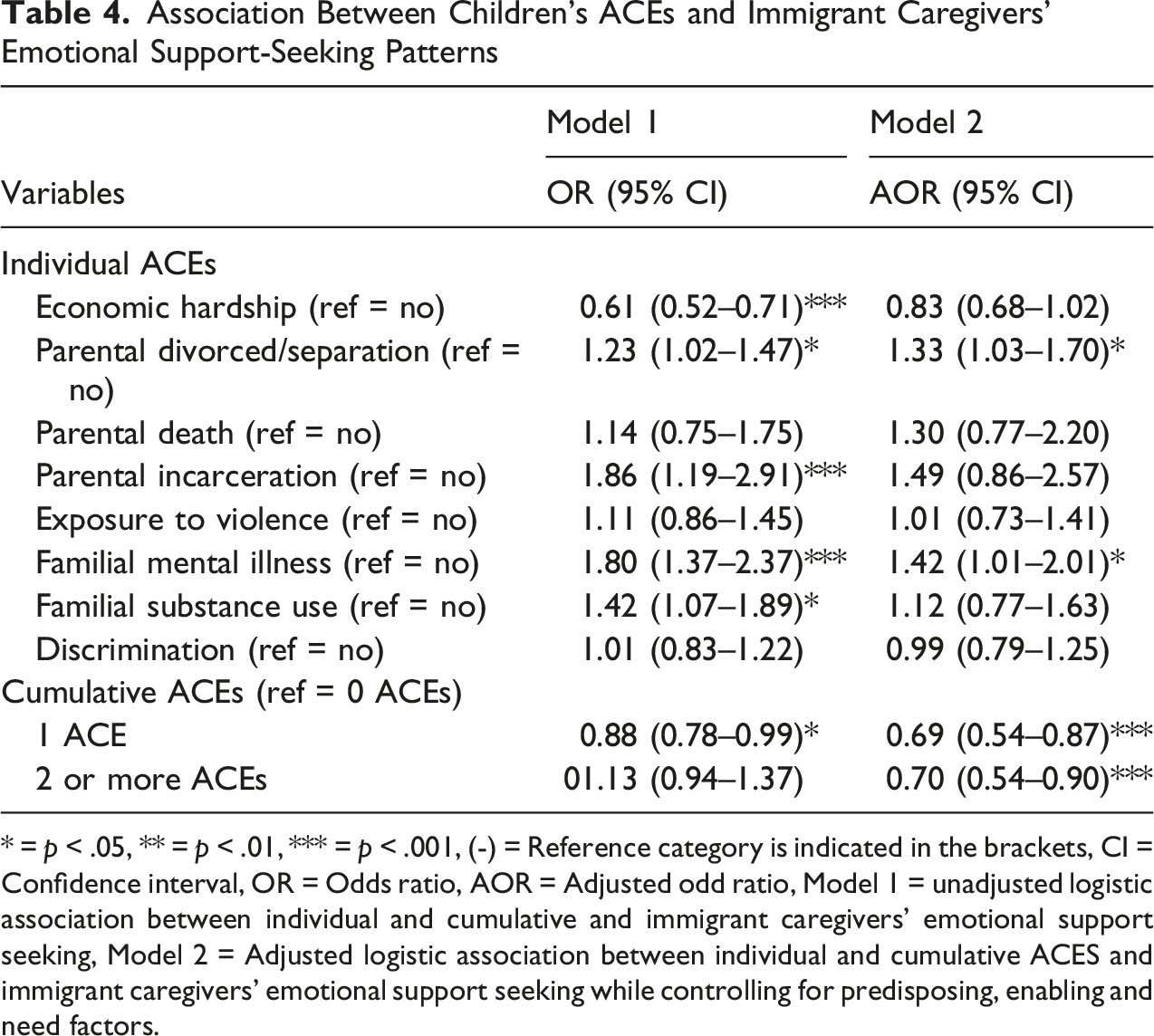
* = p < .05, ** = p < .01, *** = p < .001, (-) = Reference category is indicated in the brackets, CI = Confidence interval, OR = Odds ratio, AOR = Adjusted odd ratio, Model 1 = unadjusted logistic association between individual and cumulative and immigrant caregivers’ emotional support seeking, Model 2 = Adjusted logistic association between individual and cumulative ACES and immigrant caregivers’ emotional support seeking while controlling for predisposing, enabling and need factors.
On the other hand, immigrant caregivers of children who experienced economic hardship were significantly associated with lower odds of seeking emotional support during the past 12 months compared to those who did not experience economic hardship in the unadjusted model (OR = 0.61, 95% CI: 0.52–0.71, p < .001). In the adjusted model, immigrant caregivers with children who experienced any of these individual ACE types, including economic hardship, parental death, exposure to violence, and discrimination were not statistically significantly associated with emotional support-seeking during the past 12 months compared to those who did not.
Furthermore, regarding children’s cumulative ACEs, immigrant caregivers with children who experienced at least one of the ACE had lower odds of seeking emotional support during the past 12 months relative to those without ACEs, both before and after adjusting for other factors (OR = 0.88, 95% CI: 0.78–0.99, p < .05; AOR = 0.69, 95% CI: 0.54–0.87, p < .001). Similarly, immigrant caregivers of children who experienced two or more ACEs had lower odds of seeking emotional support during the past 12 months than those without ACEs in the adjusted model (AOR = 0.70, 95% CI: 0.54–0.90, p < .001), although this association was not statistically significant in the unadjusted model (OR = 1.13, 95% CI: 0.94–1.37, p > 0.05).
Discussion
The primary purpose of the current study was to determine the prevalence and examine the association between children’s ACEs and immigrant caregivers’ emotional support seeking in low-resource in the U.S. First, this study revealed that 57.2% of immigrant caregivers sought emotional support during the past 12 months, and approximately 65.3% of immigrant caregivers who sought emotional support cared for children who had experienced two or more ACEs in their households. As such, these prevalence estimates provide valuable insights into how early-life adversities experienced by children might be responsible for influencing help-seeking for immigrant caregivers who may face other insurmountable challenges related to caregiving responsibilities, such as structural and cultural barriers to accessing mental health and social support services in low-resource communities (Caballero et al., 2017; Hughes et al., 2023; Vaughn & Rojas-Flores, 2026).
Likewise, this study has demonstrated that immigrant caregivers of children who experienced parental divorce or separation were more likely to seek emotional support, echoing earlier studies emphasizing that family disruption may often increase psychological distress that may compel individuals in need to reach out for help in times of need (Amato, 2000; Mphaphuli, 2023; Ross & Mirowsky, 1999). Especially for immigrant families with children, family disruption can be exacerbated by limited extended family support systems, increased caregiving responsibilities, and unfamiliarity with local community resources (Neufeld et al., 2002; Stewart et al., 2006). At the same time, parental divorce or separation not only disrupts families but also divides financial resources, thereby increasing the need for support (Damota, 2019). This can be a major limitation, increasing caregiving responsibilities, and divorced or separated caregivers may have different parenting rules that can be challenging and ignite tensions and emotional struggles for caregivers in low-resource settings in the U.S.
Equally important, this study further emphasizes that immigrant caregivers with children who had lived in households with a family member with mental illness were more likely to seek emotional support. These findings align with prior studies suggesting that mental illness in the family often increases awareness of emotional strain, thereby reducing stigma around help-seeking and normalizing mental health service delivery and utilization (Chipalo, 2023b, 2024c; Hughes et al., 2023; Wilks, 2024). Similar to other forms of family disruptions, caring for someone with mental health challenges can be physically and emotionally exhausting and time-consuming for those involved in daily caregiving responsibilities (Chipalo, 2023b; van der Sanden et al., 2014). This may also require taking numerous precautions and exercising caution to provide the family member in need with the maximum available social support, thereby preventing emotional distress in communities with limited resources (Hughes et al., 2023). Henceforth, many immigrant caregivers may be more open to seeking emotional support services when mental health issues or adversities are already recognized within the family, especially in households with limited resources.
Moreover, while the association between children’s experiences of parental incarceration and emotional support seeking among immigrant caregivers was significant without controlling for other factors, the relational significant effects of emotional support seeking for caregivers diminished after accounting for potential predisposing, enabling, and need factors. This finding reflects that emotional challenges may be the consequence of structural and psychological barriers related to incarceration, including stigma, social exclusion, loss of institutional trust and other extenuating challenges that disproportionately affect minorities in the criminal justice system (Chipalo & Odii, 2024; Chipalo et al., 2026b; Turney, 2018; Turney & Goodsell, 2018; Wakefield & Wildeman, 2011; Wildeman et al., 2018). Therefore, children’s experiences of parental incarceration do not seem to have direct effects on one another because it’s the caregivers who may be incarcerated and who experience the emotional impact, rather than the children’s direct experience. In contrast, although other potential predictors, including economic hardship, were associated with a lower likelihood of seeking emotional support in the unadjusted model, this association was not significant after accounting for other factors. Financial strain in the family often limits access to care but can also reinforce cultural beliefs about self-reliance and stoicism, particularly among immigrant groups who may experience marginalization in their communities with limited resources (Caballero et al., 2017; Liu et al., 2021; Santiago et al., 2013; Vaughn & Rojas-Flores, 2026; Williams & Medlock, 2017).
A noteworthy finding emerged when cumulative ACE exposures (i.e., two or more ACEs) were associated with lower likelihood of emotional support-seeking among immigrant caregivers. This finding contrasts with prior studies in the general population, suggesting that families of children experiencing multiple adversities are more likely to engage with formal or informal emotional and social support systems (Hughes et al., 2023; Vaughn & Rojas-Flores, 2026). However, one important possible explanation is that immigrant caregivers may seek emotional support for a wide range of psychosocial, economic, migration-related, or family stressors beyond exposure to adversities of their children. Additionally, as adversity intensifies, caregivers may face greater structural, financial, emotional, and cultural barriers that may reduce their likelihood of seeking emotional support despite increased need in their households. Immigration-related stress, fear of discrimination, limited trust in institutions, and cultural stigma surrounding emotional vulnerability may further contribute to emotional withdrawal or avoidance among immigrant caregivers in low-resource settings (Kirmayer et al., 2011). Therefore, these findings highlight the importance of culturally responsive and trauma-informed interventions that reduce barriers to emotional support-seeking among immigrant families experiencing high levels of adversity in low-resource communities in the U.S.
Implications for Mental Health Clinicians
From the mental health clinical perspective, this study stresses the importance of adopting trauma-informed and culturally responsive practices within mental health and social service systems to address the emotional needs of immigrant caregivers of children who have experienced multiple adversities in resource-limited community settings. Clinical mental health providers should use traditional methods by providing maximum support services and involving cultural brokers or bilingual community health workers to connect formal services with immigrant caregivers, making it easier and less stigmatizing for them to seek emotional support in their communities. This may involve routine screening for ACEs in primary health and mental care, pediatric, and educational settings, which could be an important tool for early detection (Hughes et al., 2023). Identifying children with greater ACE exposures would allow for the timely provision of preventive services and referrals and reduce the risk of developing emotional challenges for caregivers in resource-constrained settings. However, early screening for ACEs must be accompanied by trauma-informed care practices and culturally competent referral networks to ensure that disclosure of additional adversities leads to meaningful social support rather than traumatizing them (Goddard, 2021). Additionally, community-oriented support strategies that do not depend exclusively on formal mental health systems should be adapted. For instance, peer-led support groups, parenting circles, and informal community dialogues may be more effective at engaging immigrant caregivers who may be hesitant to participate in conventional therapy to address their emotional concerns (Abo-Rass et al., 2025). These alternative mental health-related interventions can provide relational support, validation, and a sense of belonging, which are key for caregivers who might otherwise experience social isolation or cultural misunderstandings about their parenting and responses to their emotional needs in low-resource communities in the U.S.
Implications for Policy
On a larger scale, social policy reforms are essential for addressing the structural barriers that contribute to the underutilization of emotional support services for immigrant caregivers in limited-resource settings. Immigrant caregivers often encounter numerous challenges in accessing affordable, linguistically suitable mental health care due to factors such as lack of health insurance, immigration status, such as being undocumented, or geographic isolation (World Health Organization, 2023). Policymakers and advocates should focus primarily on investing in expanding access to trauma-informed care, especially within federally qualified health centers and community organizations that serve many immigrant families, in order to ensure that they have access to the essential services they need to cope with difficulties in their communities. Workforce development policies should aim to recruit and retain bilingual and bicultural providers, since representation in the mental health workforce has been shown to improve engagement and treatment results (Mc Donald, 2001). For instance, the inclusion of bilingual and bicultural providers is essential for effective mental health and trauma-informed practices, as these professionals are better positioned to build trust, reduce cultural and linguistic barriers, improve communication, and deliver culturally responsive care to caregivers and children affected by ACEs in resource-constrained settings in the U.S. Incorporating trauma-informed principles across child welfare, education, and public health systems can ensure immigrant caregivers receive comprehensive support, including support for mental and emotional concerns that come with parenting responsibilities in their households (Delgado et al., 2021).
Finally, social policies are needed to promote interagency cooperation, and data sharing can improve continuity of care and reduce duplication of efforts, especially for families navigating multiple service systems (Whicher et al., 2020). However, sharing such data would require proper data management systems to ensure maximum protection and confidentiality, achieved through data de-identification, especially when sensitive information is involved. Immigration policy must also be viewed as a major factor influencing emotional well-being for immigrant caregivers in low-resource communities. For instance, fear of deportation, family separation, and anti-immigrant rhetoric can significantly prevent caregivers from seeking emotional support, even when services are accessible (Lovato & Abrams, 2022). Therefore, policymakers should push for protective policies that can serve as shields for immigrant families against enforcement actions in health and education settings, fostering a safe environment where seeking help is encouraged in resource-constrained communities in the U.S.
Limitations of the Study
The current study has several limitations worth noting. First, the cross-sectional design precludes causal inference about the association between ACEs and caregiver emotional support-seeking behaviors. As such, future studies are needed to better disentangle the temporal and causal relationships between ACE exposure and help-seeking outcomes (Hughes et al., 2023). Second, several key variables available in the NSCH were relatively coarse and broadly categorized, which may limit the interpretation and nuance of the findings in this study. In this study, the ACEs examined were limited to those assessed in the NSCH. As such, important ACE categories, including sexual, emotional, and physical abuse, were not included in the dataset and may influence the interpretation of the findings, as some respondents may still be experiencing the long-term impacts of abuse despite not being specifically asked about these experiences. Even worse, because ACEs were parent-reported, child maltreatment could have been underreported out of fear of legal consequences due to mandated reporting law when abuse is involved. Simultaneously, ACEs assessed in the NSCH were not derived from a standardized, validated ACE scale, which may raise concerns regarding measurement consistency and the use of dichotomized indicators. However, it is recommended that future studies incorporate more comprehensive, validated ACE measures to improve the consistency and depth of assessment. It is also recommended that future studies involve age-eligible children, for example, those between 12 and 17 years old to answer the ACE questions directly without parental intervention, thereby avoiding reporting biases that may be exhibited by caregivers on behalf of children in resource-constrained settings in the U.S.
Furthermore, emotional support-seeking was reported by caregivers rather than directly by children, which may introduce reporting inaccuracies and potential social desirability bias, particularly for sensitive family and mental health-related experiences. Emotional support-seeking was also assessed using a dichotomous measure referring only to the previous 12 months, and may not fully capture support-seeking behaviors related to earlier childhood adversities. Thus, future studies should investigate these associations using longitudinal and mixed-methods approaches to better understand how children’s ACEs may influence emotional support-seeking over time for parents in limited-resource settings in the U.S. Finally, interaction or mediation effects among ACE indicators were not assessed in the regression models, as such analyses were beyond the primary scope and objectives of the current study. Despite these major limitations, this study contributes to the limited literature examining the relationship between children’s ACEs and caregiver emotional support-seeking behaviors among immigrant families living in resource-constrained settings in the U.S.
Conclusion
This study has demonstrated that 57.2% of immigrant caregivers sought emotional support during the past 12 months, and 65.3% of them had children who experienced two or more ACEs in their households. Although experiencing one or more ACEs were inversely associated with caregivers’ emotional support seeking, the study emphasizes the need for mental health interventions to focus on culturally sensitive, trauma-informed care practices and policies in limited-resource settings. Community-based mental health services, including peer support are important for emotional support for immigrant caregivers in resource-constrained settings. Robust policy implementation should aim to expand access to affordable, culturally appropriate, and linguistically appropriate mental health services in low-resource communities. Additionally, ACE assessment in pediatric care can help identify and better support families with the resources they need. Finally, future studies should explore how to effectively increase access to and use of formal emotional support among parents of children with ACEs in low-resource communities in the U.S.
Footnotes
Ethical Considerations
The Institutional Review Board at the University of Cincinnati exempted this study from human subjects, as all study procedures relied on de-identified, publicly available data from NSCH.
Author Contribution
This manuscript was solely written by E.C., starting from conceptualizing, analyzing the data, writing, and editing this manuscript.
Funding
The author received no financial support for conducting research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used for the study will be available upon request from the corresponding author. All datasets and syntax used during data preparation are readily available.
Public Relevance
This study emphasizes the negative impact of multiple exposures to ACEs on emotional support-seeking among immigrant caregivers. The findings highlight the urgent need for culturally appropriate and accessible mental health services for immigrant families.