
Abstract
This report presents the findings of a spontaneous case of acute myeloid leukemia (AML) in a 6-year-old male cynomolgus macaque enrolled in a 9-month repeat dose-toxicity and toxicokinetic study. Abnormal hematology findings occurred approximately 6 months into daily oral dosing that included markedly decreased red blood cell mass and reticulocyte count, moderately decreased platelet counts, and the identification of abnormal cells in blood that were interpreted as neoplastic. Cytologic characteristics of the neoplastic cells included a moderate to high nucleus to cytoplasm ratio, medium to deep blue cytoplasm, and a round to oval nucleus with fine chromatin, often with multiple, irregularly shaped nucleoli. Following humane euthanasia, evaluation of bone marrow smears and formalin fixed paraffin embedded tissues revealed neoplastic cells of similar morphology. A panel of immunohistochemistry and cytochemical stains demonstrated expression of CD68 and myeloperoxidase, with weaker and less consistent expression of CD11c and CD45. No staining was detected for CD34, CD14, and T (CD3) and B (CD20) lymphoid markers. The neoplastic cells did not stain for any of the cytochemical stains applied (Periodic Acid Schiff, α-naphthyl acetate esterase, Sudan Black B, α-naphthyl butyrate esterase, and chloroacetate esterase). An interpretation of AML was made suggestive of a myelomonocytic lineage.
Introduction
Repeat-dose safety toxicity studies incorporate clinical pathology endpoints to evaluate the health of laboratory animals treated with test articles during the drug development process. Hematology, hemostasis, clinical chemistry, and urinalysis results comprise the minimal clinical pathology data base used in these studies. Results of clinical pathology testing are correlated with live phase observations, gross lesions, and microscopic examination of tissues from rodents, dogs, and nonhuman primates (NHPs) to assess the safety of new medicines intended for animals and people.4,5,24
The complete blood count (CBC) is the primary test used by most biopharmaceutical companies for the hematologic assessment of health and disease in laboratory animals. The CBC incorporates ~17–20 individual parameters/tests (depending upon the specific clinical pathology laboratory) to evaluate erythrocytes, leukocytes, and platelets. The leukogram consists of the total and differential leukocyte counts (relative and absolute counts) combined with the blood smear review. It is used to assess changes in the counts of individual leukocyte types that result from imbalances in leukocyte production vs tissue migration and leukocyte death. Alterations in total leukocyte counts and/or individual leukocyte morphologies due to physiologic leukocytosis, corticosteroid-induced leukocytosis, and inflammation (acute and chronic) occur often in safety assessment studies in laboratory animals. However, leukemia is a rare cause of these changes in safety assessment studies, particularly in NHPs.4,5,24
Leukemia is defined as a condition characterized by the neoplastic proliferation of leukocytes originating from blood, bone marrow, or lymphoid tissues. These cancerous conditions may be acute or chronic in onset and vary widely in specific leukocyte type and leukocyte cell numbers within the blood. The American Cancer Society estimates that ~62,770 people in the United States will be diagnosed with leukemia (all types) in 2024 18 and the National Cancer Institute estimates ~20,800 new cases of the acute myeloid leukemia (AML) form in 2024 and a 5-year survival rate from AML of 31.9% from 2014 to 2020. 9 There are myriad resources available that discuss genetic, infectious, and environmental agents associated with development of leukemia; cellular classification schemes; diagnostic techniques; and treatment options for people who develop leukemia.11,13,18
In contrast, there are few published reports of leukemia in rhesus and cynomolgus macaques. Exposure of rhesus macaques (Macaca mulatta) to whole body radiation has been reported to cause AML.14,21,23,28,33 Exposure to the antitumor alkylating agent procarbazine also caused development of AML in rhesus macaques that was detectable at an average of 77 months.1,27 In addition, AML occurred in one of seven rhesus macaques that underwent retroviral gene transfer to hematopoietic cells and cytotoxic chemotherapy. 26 Krugner-Higby et al 20 described a case of chronic myeloid leukemia in a female juvenile rhesus macaque that had experimental lead exposure as a neonate. A case of spontaneous chronic T-cell leukemia in a male rhesus macaque was reported by Cazzini et al. 10 B-cell leukemia in a rhesus macaque infected with simian immunodeficiency virus was described by Fortgang et al. 15 A T-cell lymphoproliferative disease of uncertain cause occurred spontaneously in a rhesus macaque. 16 There are even fewer published reports of leukemia in cynomolgus macaques (Macaca fascicularis). A male cynomolgus macaque housed in a primate research center in Japan developed acute megakaryocytic leukemia. Infection with simian retrovirus type D was the hypothesized cause of the leukemia in this animal. 22
The objectives of this article are to describe a case of AML that occurred as a spontaneous finding in a routine toxicity testing study in cynomolgus macaques; review reports of leukemia (spontaneous and iatrogenic) in rhesus and cynomolgus macaques; examine methods to identify the cell type of origin in poorly differentiated neoplastic hematopoietic cells; and discuss the decision process for determining whether the hematologic alteration was incidental or caused by test article administration.
Case Presentation
This nonhuman primate (NHP) was a 6-year-old male cynomolgus macaque from a routine 9-month, repeat-dose safety toxicity and toxicokinetic study for a small molecule given by oral gavage. The treatment groups were as follows: control vehicle, low dose, and high dose. The macaque described in this report was assigned to the low dose group. The animal was purpose bred for laboratory use. The study was conducted at Charles River Laboratories (CRL), Reno, Nevada, a facility fully accredited by the Association for Assessment and Accreditation of Laboratory Animal Care and registered with the United States Department of Agriculture (USDA). This facility has an Institutional Animal Care and Use Committee (IACUC) responsible for CRL compliance with applicable laws and regulations concerning the humane care and use of laboratory animals. The CRL IACUC reviewed and approved the animal use in this study. The NHP was socially housed in modified quad-rack, stainless steel caging. Modified quad-rack caging allows double USDA compliant floor space and vertical access within the cage. Primary enclosures were as specified in the USDA Animal Welfare Act (9 CFR, Parts 1, 2, and 3) and as described in the Guide for the Care and Use of Laboratory Animals. 12 Temperature and humidity were automatically controlled at 64°F to 84°F (approximately 18°–29°C) and 30% to 70%, respectively, with four or more air changes per hour with 100% fresh air (no recirculation). A twelve-hour light/twelve-hour dark cycle was maintained. Fresh drinking water was provided ad libitum, and animals were fed PMI Nutrition International Certified Primate Chow, No. 5048, daily. Analysis of the diet was performed by the manufacturer; no contaminants were known to be present in the diet or water at levels that would interfere with the study results. This diet was supplemented with fruit and/or vegetables two or three times weekly.
The macaque underwent repeated physical exams and was serologically tested. While in quarantine, it was confirmed to be clinically healthy and serologically negative for the following viral infections: simian immunodeficiency virus (SIV), Cercopithecine herpesvirus 1 (B virus), simian retrovirus (SRV), and simian T-cell leukemia virus (STLV). Tuberculin tests, polymerase chain reaction test for NHP plasmodium (malaria), and parasitological screening were conducted upon arrival at the testing facility, and all results were negative. The animal was prophylactically treated for parasites and vaccinated for measles and hepatitis A viruses.
Among the endpoints evaluated during the study were clinical and physical examinations, body and organ weight assessments, and anatomic and clinical pathology parameters. Blood collections were scheduled (2 prior to initiation of dosing and at approximately 1- to 4-month intervals during the dosing period) for the evaluation of hematology parameters using the ADVIA 2120i hematology analyzer (Siemens Medical Solutions Inc., Malvern, PA), coagulation parameters on the STA Compact (Diagnostic Stago Inc., Mount Olive, NJ), and serum chemistry parameters on the Cobas 6000 (Roche Diagnostics, Indianapolis, IN).
There were no noteworthy findings on the clinical pathology evaluations at the first 2 scheduled collections (Study Days 22 and 85); however, there was a marked decrease in the NHP’s red blood cell (RBC) mass (RBC count, hemoglobin, and hematocrit) at the next scheduled collection on Study Day 176 that triggered a more detailed clinical evaluation. The macaque was observed to have hunched posture, decreased activity and food consumption, and pale mucous membranes. Clinical observations in this animal up to this point were limited to fecal changes that were also observed in other animals. The animal was euthanized on Day 176 for humane reasons by intravenous administration of ketamine and Beuthanasia-D solution.
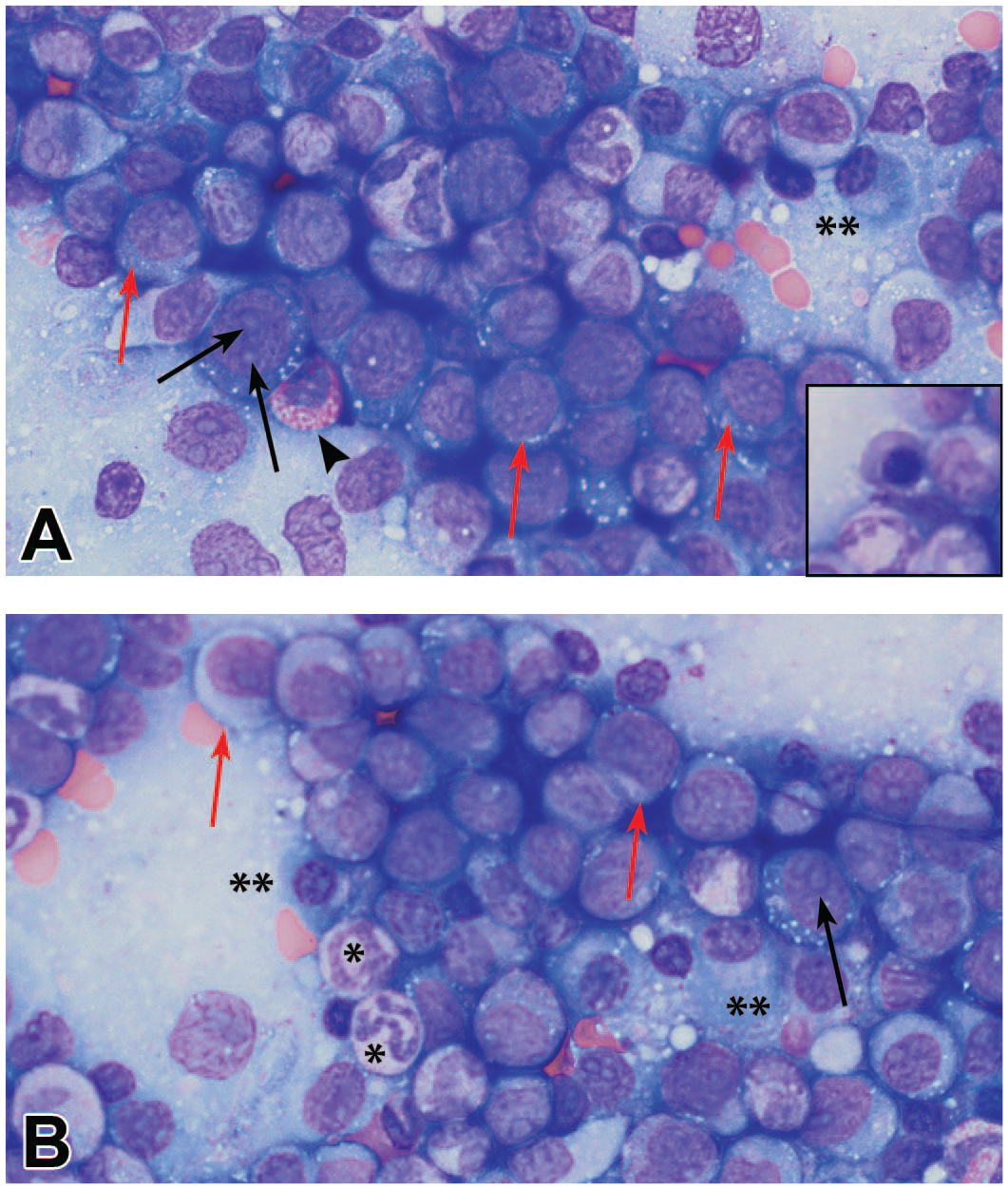
Hematology findings on the day of euthanasia were compared to those measured 2 weeks prior to initiation of dosing and changes included marked decreases in the RBC mass and reticulocyte count and moderately decreased platelet count (see Table 1). The magnitude of these changes triggered the evaluation of a routinely prepared blood smear stained with a modified Wright-Giemsa stain. Despite an absence of noteworthy changes in the total white blood cell (WBC) count or WBC subsets (counts of neutrophils, lymphocytes, monocytes, eosinophils, or basophils), there was a population of abnormal leukocytes in the peripheral blood that were interpreted as neoplastic. These cells were characterized by a moderate to high nucleus to cytoplasm (N:C) ratio, medium to occasionally deep blue cytoplasm that often contained few to several punctate colorless vacuoles, and a round to oval nucleus with fine chromatin often containing one to multiple prominent irregularly shaped nucleoli (characteristic of blast cells), or less commonly an irregularly shaped nucleus without prominent nucleoli (Figure 1A and B). Blood smears from the previous scheduled collections were re-evaluated and a low number of similar cells was observed on Day 85 but not at the earlier timepoints.
Select ADVIA 2120i hematology results from pretreatment to the day of euthanasia.
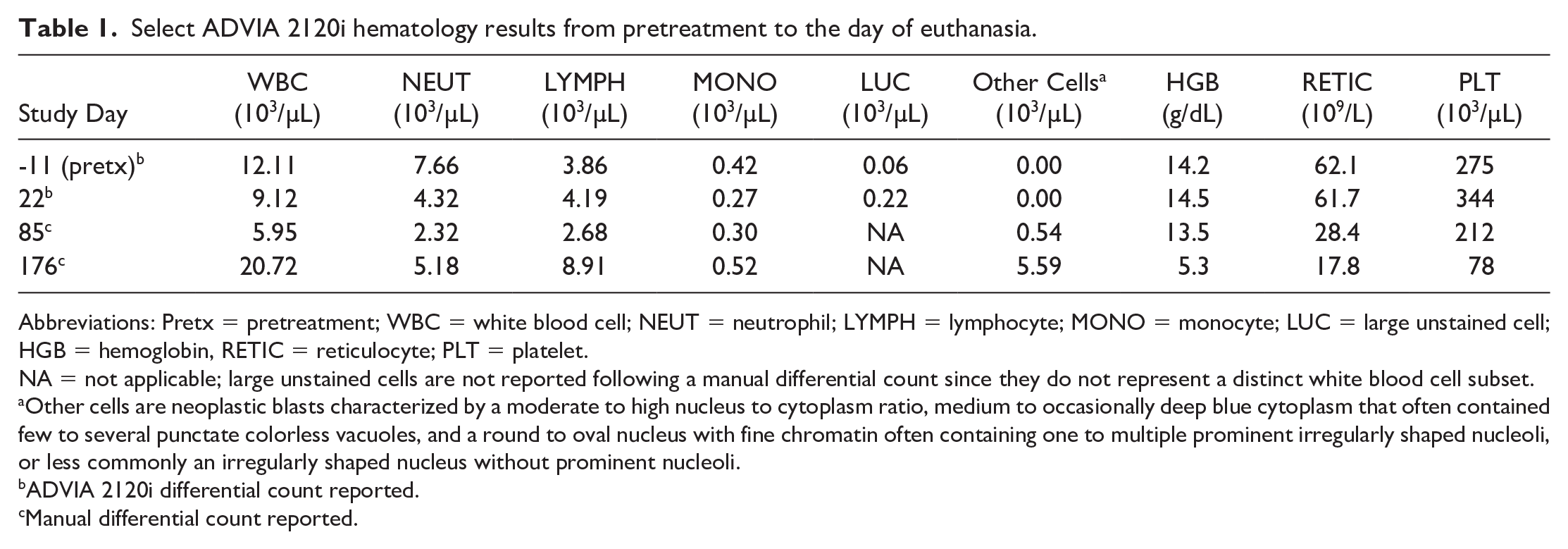
Abbreviations: Pretx = pretreatment; WBC = white blood cell; NEUT = neutrophil; LYMPH = lymphocyte; MONO = monocyte; LUC = large unstained cell; HGB = hemoglobin, RETIC = reticulocyte; PLT = platelet.
NA = not applicable; large unstained cells are not reported following a manual differential count since they do not represent a distinct white blood cell subset.
Other cells are neoplastic blasts characterized by a moderate to high nucleus to cytoplasm ratio, medium to occasionally deep blue cytoplasm that often contained few to several punctate colorless vacuoles, and a round to oval nucleus with fine chromatin often containing one to multiple prominent irregularly shaped nucleoli, or less commonly an irregularly shaped nucleus without prominent nucleoli.
ADVIA 2120i differential count reported.
Manual differential count reported.

Blood smears from a 6-year-old male cynomolgus macaque with AML (Study Day 176): (A) Neoplastic blasts characterized by a moderate to high nucleus to cytoplasm ratio, deep blue cytoplasm and a round nucleus with fine chromatin, containing 2 prominent nucleoli (black arrows); or with medium blue cytoplasm, oval nuclei without prominent nucleoli and containing several punctate colorless vacuoles (inset), a neutrophil (*) and lymphocyte (**) of normal morphology are also seen. (B) Neoplastic blasts having similar morphology with medium to deep blue cytoplasm and round, oval or irregular nuclei, with or without nucleoli (black arrows). Wright-Giemsa stain, 100X objective.
Bone marrow smears, obtained at necropsy, stained with modified Wright-Giemsa, were also evaluated and consisted of 43.4% blast cells having a similar morphology as those observed on the peripheral blood smear (Figure 2A and B). There were similar leukocytes with a moderate nuclear to cytoplasm ratio, light blue cytoplasm with or without fine pink granules, round to oval or indented nuclei with fine chromatin and indistinct or absent nucleoli, these cells were interpreted as promyelocytes (3.4%). Other leukocytes present in lower numbers included neutrophils at various stages of maturation ranging from myelocytes (3.1%), metamyelocytes (4.5%), band (11.5%), and segmented neutrophils (13.5%). No definitive monocytes or promonocytes were identified. Erythroid cells occurred in very low numbers consisting of mostly polychromatophilic rubricytes (0.6%) and metarubricytes (1.1%) and there were few small lymphocytes (13.5%), plasma cells (3.1%), and eosinophils (1.7%). The myeloid to erythroid ratio was increased at approximately 48:1. Megakaryocytes were seen infrequently.
Bone marrow smears from a 6-year-old male cynomolgus macaque with AML (Study Day 176): (A) and (B). Numerous neoplastic blasts (some examples identified with red arrows) characterized by a moderate to high nucleus to cytoplasm ratio, medium to deep blue cytoplasm and a round to oval nucleus with fine chromatin, most containing 1 to multiple prominent nucleoli (black arrows) and some containing several punctate colorless vacuoles, neutrophils (*), an eosinophil (arrowhead), plasma cells (**), and erythroid precursors (inset, metarubricyte) are also seen. Wright-Giemsa stain, 100X objective.
The hematology and bone marrow findings were consistent with an acute leukemia and additional peripheral blood and bone marrow smears were prepared and stained with five cytochemical stains utilizing commercially available kits. Cytochemistry stains detect cellular components to help determine cell lineage. Time between smear preparation and staining procedures ranged from 2 to 5 months, in part due to availability of staining kits. Periodic Acid Schiff (PAS; StatLab, McKinney, TX) and α-naphthyl acetate esterase (ANAE; Sigma Aldrich, St. Louis, MO) staining was performed at CRL, Reno, Nevada per manufacturer’s instructions and Sudan Black B (SBB), α-naphthyl butyrate esterase (ANBE), and chloroacetate esterase (CAE) staining was performed at Stokol laboratory at Cornell University as described previously. 29 The blast cells were negative for all stains but mature cells were stained as expected in control tissues as well as in the affected animal.
A detailed necropsy was performed under the supervision of a veterinary pathologist. A comprehensive set of tissues was collected, fixed in 10% neutral buffered formalin, embedded in paraffin wax, sectioned to 4–5 mm thickness, and processed to hematoxylin and eosin (HE)–stained slides. Additional immunohistochemical stains were applied to serial sections of affected spleen, bone marrow (sternum), liver, kidney, mandibular and mesenteric lymph nodes. These tissues were stained with the following anti-human monoclonal antibodies: anti–CD3 (polyclonal, Dako, Carpinteria, CA), anti-CD20 (clone L26, Dako, Carpinteria, CA), anti-CD45 (clones 2B11 and PD7/26 Agilent Technologies, Santa Clara, CA), anti-CD11c (clone 5D11, Sigma Aldrich), anti-CD34 (cloneEP3Y3Y, Abcam), anti-CD68 (clone KP1, Dako Carpinteria, CA), anti-CD14 (clone SP192, Abcam), and anti-myeloperoxidase (MPO; Polyclonal, Abcam). These antibodies had been previously validated with cynomolgus macaque tissues. In affected tissues, a qualitative assessment of immunohistochemical labeling of the neoplastic cell infiltrates was performed and the character of the staining and the percent positive cells were reported.
Microscopically, disruption of the normal tissue architecture was noted in the hematopoietic and lymphoid organs, most notably in the bone marrow and spleen, as well as in nonhematopoietic tissues. The splenic red pulp and bone marrow were expanded by a dense infiltrate of immature hematopoietic cells (interpreted as blasts) which displaced the normal hematopoietic progenitor cells in the marrow cavity (Figure 3A); erythrocytes and lymphocytes in the splenic red and white pulp, respectively, and extended beyond the splenic capsule into the surrounding adipose tissue. Greater than 20% of the hematopoietic cells in the bone marrow were considered blasts. Neoplastic cells were also present in circulation and infiltrating nonhematopoietic tissues such as the hepatic and renal parenchyma (Figure 4A) as well as in the lymph nodes (mandibular and mesenteric; medullary cords and sinuses). In the liver, the neoplastic cells were present within blood vessels, sinusoids, and expanded the centrilobular and portal areas. Additional findings in the liver included mild erythrophagocytosis and moderate pigment (hemosiderin) laden Kupffer cells in the hepatic sinusoids as well as diffuse mild hepatocellular vacuolization and minimal multifocal hepatocellular necrosis with inflammation. In the kidney, dense perivascular neoplastic infiltrates were noted bilaterally, extending into the interstitium, surrounding glomeruli and tubules (Figure 4A), and were often associated with mild tubular degeneration and protein casts.

AML, blast morphology (hematoxylin and eosin, HE) and immunohistochemistry (IHC) labeling in the bone marrow. (A) A high predominance of immature myeloid progenitor cells (blasts) with only very rare clusters of erythroid progenitors remaining can be appreciated at high magnification in the HE stained bone marrow section. The neoplastic blasts have a high nuclear to cytoplasmic ratio, round to oval and rarely indented nuclei with finely stippled vesicular chromatin, often a single prominent nucleolus, variable amounts of amphophilic cytoplasm and a high mitotic rate. Low magnification (inset) showing the hypercellularity of bone marrow. HE. (B) Neoplastic cells have diffuse mild to strong cytoplasmic expression of CD68 (greater than 75% of blasts), (C) slightly less myeloperoxidase (MPO) labeling (50%–75% of blasts), (D) and are equivocal for CD11c. (E) Small numbers of normal mature CD14+ monocytes/macrophage are scattered throughout the bone marrow and (F) rare CD3+ T lymphocytes are intermittently dispersed amongst the neoplastic cells. Neoplastic blast cells are negative for CD14, CD3 and CD20 markers (not pictured).

AML, extramedullary infiltration in the kidney, (hematoxylin and eosin, HE) and immunohistochemistry (IHC) labeling. (A) The neoplastic infiltrates in the kidney accumulated around blood vessels and interstitially. Dense sheets of neoplastic cells are surrounding renal tubules and glomeruli. With high magnification, myeloblast morphologic features similar to that described in the bone marrow can be appreciated. (B) Immunohistochemistry confirms that the neoplastic blasts have diffuse, mild to moderate cytoplasmic expression of CD68 (greater than 75% of blasts). (C) MPO expression is similar in character and intensity yet decreased in frequency (50%–75% of blasts). (D) CD11c expression is less prevalent and positive cells had cytoplasmic and subtle membrane labeling. (E) Very rare mature CD14+ monocytes/macrophages are admixed and (F) occasional CD3+ T lymphocytes are intermittently dispersed with infiltrating neoplastic cells. Neoplastic blast cells are negative for CD14, CD3, and CD20 markers (not pictured).
The neoplastic cells were pleomorphic, medium to large cells with a moderate nuclear to cytoplasmic ratio, had round to oval nuclei with finely stippled vesicular chromatin, often a single prominent nucleolus and variable amounts of amphophilic cytoplasm. A relative increase in mitoses was noted in the bone marrow as compared to concurrent study controls. Most of the neoplastic blasts lacked cytoplasmic differentiation. Rare immature band neutrophils were admixed. The histologic and clinicopathologic morphologic features were consistent with a poorly differentiated myeloid origin. Due to the lack of further neoplastic cell differentiation, a panel of immunohistochemical stains defining the myeloid lineage (anti-MPO), degree of myeloid/monocyte differentiation (CD68, CD14, and CD11c), cell immaturity/non-lineage restricted (CD34 and CD45), and lymphoid markers (CD3 and CD20) were applied. Immunohistochemistry (IHC) results revealed that the infiltrating immature hematopoietic cells (blast cells) in spleen, bone marrow, liver, kidney, mandibular, and mesenteric lymph nodes frequently expressed CD68, a glycoprotein of lysosomes and phagosomes expressed in the cytoplasm of most monocyte/macrophages, and MPO, an enzyme in granulocytes, monocytes and some tissue macrophages. CD68 was the most frequently expressed marker (greater than 75% of blasts; Figures 3B and 4B) followed by MPO (expressed in 50%–75% of blasts; Figures 3C and 4C). Some infiltrating neoplastic cells were also weakly positive for CD11c (a monocyte/macrophage/dendritic cell marker; Figures 3D and 4D); however, CD11c expression was less frequent and variable between tissues (noted in the spleen, liver, kidney, and lymph nodes and equivocal in the bone marrow). CD45 positive infiltrating neoplastic blasts were observed occasionally in the kidney and liver only. Mature monocytes and macrophage that were intermittently dispersed in the affected tissue expressed CD14 (Figures 3E and 4E); however, the infiltrating neoplastic blast cells were generally CD14 negative. The infiltrating neoplastic blast cells were negative for CD3 T lymphocyte (Figures 3F and 4F) and CD20 B lymphocyte markers.
After assessment of all the diagnostic testing, an interpretation of an AML was made based on the immature morphology of the cells (fine chromatin, nucleoli, moderate to high N:C ratio), the percentage of these cells in peripheral blood and bone marrow that exceeded 20%, 2 and on the positive staining for myeloid antigens (most consistently MPO and CD68) and negative staining for T and B lymphocyte antigens.
Discussion
Nonclinical safety assessment in drug development includes repeat-dose safety toxicity testing that has two main goals: identify test-article-related alterations and determine the adversity of those effects should they occur.7,9,21,25 In this study of a small molecule administered by oral gavage daily for 9 months, a single NHP developed leukemia. A weight of evidence approach, considering the factors listed below, determined the single case of leukemia was most likely a spontaneous finding and was not a test article-related effect. Only one of sixteen NHPs administered the test article daily by oral gavage in the 9-month study developed leukemia. This animal was given a low dose of test article and animals that were dosed with 10-fold higher doses (4–5X exposure) did not develop leukemia or any hematology effects, including findings on blood smear evaluation. The test article is a small molecule known not to be genotoxic and has no known effect or relationship to hematopoiesis, immune surveillance, or hormone concentrations. It is possible that the low dose NHP that developed leukemia in this case report was in a prodromal state (aleukemic leukemia) when selected for inclusion in the study, and neoplastic leukocytes were not seen in detectable numbers in the whole blood analysis until Study Day 85, although spontaneous AML was also considered. Prodromal periods in people who later developed clinical leukemia have ranged from weeks to months for some cases.24-26 In addition, the test article had been administered orally to over 100 male and female rats at doses equal to the low dose in this study or 10-fold higher for 2 weeks to 6 months and no rat developed any test article-related changes in hematology data.
While AML is the most common form of acute leukemia in adult humans and accounts for approximately 80% of all cases, it is rare in NHPs.6,28,33 Several classification schemes have been published using various laboratory tools to assess the direction and level of cellular differentiation, including light microscopy for morphology evaluation, cytochemistry staining to determine intracellular enzyme profiles, 7 and immunohistochemistry and/or flow cytometry for surface and intracellular antigen identification. The World Health Organization divided AML into two categories: AML with defining genetic abnormalities (AML-DGA), representing the majority of cases, and AML defined by differentiation (AML-DBD)13,17 with cytogenetic techniques more recently employed in identification and differentiation of AML-DGA. In the present case, genetic testing was not performed, as it is not readily available in NHPs. In one case of AML associated with retroviral gene transfer in a rhesus macaque, an animal that received transplantation of CD34+ cells transduced with a retroviral vector developed leukemia 5 years following the transfer. In this case report, linear amplification mediated (LAM)—PCR, inverse PCR, topoisomerase I—thymidine-adenine (TOPO TA) cloning, TaqMan RT-PCR, and Southern blot analysis were used to identify increased expression of BCL2-A1, a gene that is known to have antiapoptotic properties and was hypothesized to play a role in the development of AML. 26 These techniques were beyond the scope of the current case and were considered a limitation.
An interpretation of an acute leukemia was made in this case based on the immature morphology of the neoplastic cells and the percentage of these cells in peripheral blood or bone marrow (43.4% by cytologic evaluation in bone marrow) that exceeded 20%; 2 and the positive staining for myeloid antigens and negative staining for T and B lymphocyte antigens were consistent with a myeloid origin.
One study that evaluated 234 cases of human AML-DBD found that nine antigens were most commonly identified: MPO, CD34, CD11b, CD14, CD36, CD45, CD15, CD64, and CD65. 27 The neoplastic blast cells in the current case did not stain for CD34, a common marker of hematopoietic stem/progenitor cells. This lack of staining was similar to the lack of expression described in a case of irradiation induced AML in a rhesus macaque 23 and it has been reported that approximately 30% of human AML cases lack CD34 expression. 3 In addition, CD68 expression is highest in cells of monocyte lineage, weaker expression can be observed in granulocytes 30 and CD68 was detected in 33% of AML with minimal myeloid differentiation. 31 In this NHP, neoplastic cells in the spleen, bone marrow, liver, kidney, and mandibular and mesenteric lymph nodes most consistently expressed CD68 (pan monocyte/macrophage marker) followed by MPO (a granulocyte/monocyte/macrophage marker) and maturing granulocytic cells exceeded 20% of the hematopoietic cells in bone marrow on cytologic evaluation of the bone marrow, findings suggestive of a myelomonocytic lineage. 19 However, there was a lack of evidence of further macrophage differentiation, negative CD14 staining and infrequent positivity for CD11c.
The panel of cytochemistry stains (NSE [ANAE and ANBE], SBB, CAE, and PAS) stained mature cells in the control tissues as well as in the affected animal; however, because neoplastic blast cells did not stain, further differentiation could not be determined by this method. This lack of cytochemistry staining offers support for a poorly differentiated AML, though false negative results due to loss of stability (eg, decreased enzyme activity) is also possible due to the time lapse between smear preparation and staining.8,32 Stability of these staining procedures have not been established by the laboratories that performed the testing.
Spontaneous cases of AML in NHPs are rare.6,11,28,33 Most cases have involved prior exposure to irradiation, lead, retroviral gene transfer, or viral recrudescence. The animal in this case had no previous exposure to any of these potentially toxic or infectious agents. The NHP tested negative for tuberculosis, simian retrovirus, simian immunodeficiency virus, and herpes B virus and was vaccinated for measles and hepatitis A prior to the start of the study. Additional viral testing for lymphocryptovirus (LCV) such as Epstein–Barr virus (EBV) was not performed, however, no histologic evidence of active or latent LCV infection such as lymphoproliferative changes and/or the presence of Reed-Sternberg cells were noted in lymphoid tissues.
In conclusion, this case describes a spontaneous occurrence of AML in a cynomolgus macaque assigned to a routine toxicity study. The bone marrow contained a large number of neoplastic blast cells (>40% on cytology) of the myeloid cell lineage, which were also observed in peripheral blood, in multiple organs with histopathology, and supported a myeloproliferative disorder. Immunohistochemistry stains on tissues were suggestive of a myelomonocytic lineage but cytochemistry on blood and bone marrow smears did not provide support for this categorization of the type of AML. Classification of the AML was hindered by the lack of genetic testing, immunophenotyping by flow cytometry, and delay between smear preparation and cytochemical staining.
Although rare in NHPs, when the initial examination of blood smears is suggestive of a neoplastic hematopoietic process, the following, some of which were performed, are recommended either in-life or within several days of collection following identification and subsequent death of the animal:
Preparation of routinely stained (eg, Wright-Giemsa) blood and bone marrow smears and evaluation by a board-certified clinical pathologist.
Preparation of multiple unstained blood and bone marrow smears for future staining/analysis (at least 20 peripheral blood and 20 bone marrow smears).
Collection of peripheral blood and bone marrow samples for evaluation by flow cytometry.
Perform a gross necropsy overseen by a board-certified anatomic pathologist.
Collection and microscopic evaluation (HE) of the following tissues (at a minimum), regardless of gross pathology findings: ● Bone marrow ● Liver ● Spleen ● Lymph nodes ● Kidney ● Lung
Perform ancillary stains including immunohistochemistry and/or cytochemistry with panel of antibodies/reagents deemed appropriate from the above listed evaluations.
Footnotes
Acknowledgements
The authors recognize the Dr Tracy Stokol at Cornell University for performing cytochemical staining in her laboratory, and Cherrie Kolbe, Ashely Guzman and the histopathology and clinical pathology laboratory staff at Charles River Laboratories (Reno NV site) for their assistance with data analysis and sample and tissue preparation and staining.
Author Contributions
The analyses, conclusions, and opinions expressed in this article are those of the authors. All authors participated in the discussion involved in organization and crafting of this article and response to reviewers’ comments.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs AW, HP, and JS declared no real, perceived, or potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr AES owns stock in Eli Lilly and Company.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.