
Abstract
Patient needs and practice conditions demand that clinical nurses in acute care hospitals engage in a unique professional practice role—care and management of clinical situations for multiple patients, simultaneously. Nurse Residency Programs (NRPs) facilitate the integration of Newly Licensed Registered Nurses (NLRNs) into this professional practice role through competency development in seven management areas. Purpose of this study was to identify effective components and strategies of NRPs in each area. A sample of 907 nurses in 20 Magnet hospitals with NRPs operative for at least 3 years participated in individual or small group interviews and 82 participant observations. All interviews were digitally recorded, transcribed, and analyzed thematically. Effective strategies were identified for all but one of the seven management areas. Suggestions for improvement in NRPs to better meet NLRN professional socialization needs, patient outcomes, and challenges of the health care system today are offered.
Keywords
Clinical nurses in hospital practice today are charged with caring for acutely ill patients with complex, diagnostic, and treatment regimes. As knowledge workers, nurses must synthesize an array of multisourced data and bring that synthesis to bear on patient care (Porter-O’Grady, 2003). In addition to providing the bulk of daily patient care, they are the major interdisciplinary coordinators of care and must adopt comprehensive perspectives covering the continuum of patient care (Reinsvold, 2008). Clinical nurses practice in challenging, often chaotic, work environments characterized by personnel shortages, shrinking resources, advanced technologies, and seemingly unending documentation (Buerhaus, 2004; Cornell et al., 2010; Needleman et al., 2011; Porter-O’Grady, Clark, & Wiggins, 2010). In addition, they must work with the largest number of coworkers of any occupation or profession (Kalisch & Begeny, 2005). In contrast to other health care professionals who provide service to clients sequentially, nurses are professionally accountable for provision of care and management of diverse clinical situations for multiple patients, simultaneously (Ebright, Patterson, Chalko, & Render, 2003; Kramer, Schmalenberg, & Maguire, 2010; Lindberg & Lindberg, 2008). These professional role demands and practice conditions place heavy demands on all nurses, but particularly on Newly Licensed Registered Nurses (NLRNs) as they must develop competence and become integrated into the professional nurse practice role of the clinical nurse during a time of great stress.
NLRNs consistently identify seven management skills as areas of very high concern during their transition and integration into professional practice—delegation, collaborative nurse–physician (RNMD) relationships, feedback to promote self-confidence, autonomous decision making, prioritization, constructive conflict resolution, and getting my work done/utilizing the nursing care delivery system (Kramer, Brewer, & Maguire, 2011; Kramer & Schmalenberg, 1977; Schmalenberg & Kramer, 1979). In a nationwide preparation-practice gap survey (Berkow, Virkstis, Stewart, & Conway, 2009), more than 5,000 frontline nurse leaders ranked NLRN lack of proficiency in these seven areas the very lowest of 36 competencies essential to safe and effective nursing practice. Nurse Residency Programs (NRPs) have been established to assist NLRNs in transitioning from academia to practice and becoming integrated into the professional practice role of the nurse (Kramer, Maguire, Halfer, Brewer, & Schmalenberg, 2011). Outcome effectiveness of NRPs (Kramer, Halfer, Maguire, & Schmalenberg, 2012) is augmented when NRPs are operational on clinical units with nurse-confirmed Healthy Work Environments (HWE; Kramer, Brewer, et al., 2011). In this study, the seven issues of concern and corresponding competencies are used to assess the process effectiveness of NRPs. The research question is as follows:
Research Question 1: What NRP components and strategies do NLRNs and clinical nurses practicing on clinical units with Very Healthy Work Environments (VHWE) identify as effective in NLRN transitioning and integrating into professional practice?
Background information on NRP and HWEs will be provided in this section. An overview of the 7-study research program will also be presented because elements of that program impacted decision making in the Effective NRP Components study reported here.
NRPs
In the late 1970s, NRPs, based on grounded theory derivations of the professional-bureaucratic role conflict theory, were established to decrease Reality Shock (Kramer, 1974). In the 1980s, the emphasis shifted to change theory and constructive abatement for handling of Transition Shock resulting in increased retention and improved performance (Duchscher, 2009). Since the 1990s and the increasing recognition of nurses as full-fledged professionals, many NRPs are now based on Merton’s three-stage theory of professional socialization—knowing = Academic stage, becoming = Transition stage (initial 3 months post-hire), and affirming/integrating = Integration stage (4 months to 1 year); (Kramer, Maguire, Halfer, et al., 2011). Many NRPs are now the full-year in length needed for inclusion of Transition and Integration stages of professional socialization (Bratt, 2009; Duchscher, 2012; Halfer, Graf, & Sullivan, 2008; Krugman et al., 2006; Shanahan & Warren, 2010).
Goals of the Transition stage of professional socialization in nursing, similar to medical internship or clerkships, include clinical skill development and practice (Benner & Wrubel, 1982), and practice in planning, organizing, and providing safe care to selected patients under the guidance, support, and protection of a preceptor. Some experience in management of a clinical situation may be obtained—contacting physicians and answering their questions, contacting or handling inquiries from families, other health care professionals, other departments and services, ordering tests, and arranging for follow-up care. However, provision of care and management of a clinical situation is usually for one patient, or provided sequentially if NLRN is assigned to more than one patient. During the precepted apprenticeship, NLRNs care for patients assigned to the preceptor and are not included in the staffing roster. Time-off unit to attend stress-reduction seminars, observations on other units, skill practice, and didactic classes is available as backup and responsibility for patients is provided by preceptor. Expected NLRN performance in this dependent role is competence in technical skills and safe, quality care of patients assigned to the NLRN by his or her preceptor. Some NRPs begin Mentoring—that is, career planning and development, integration in professional communities—in this stage.
Major goals and expected NLRN role performance during the independent Integration stage is competent performance of the professional practice role of nurses, that is, provision of care and management of clinical situations for multiple patients, simultaneously (Ebright et al., 2003; Kramer et al., 2010; Lindberg & Lindberg, 2008). A full analysis of goals, activities, and expectations for each stage of NRPs in 34 Magnet hospitals can be found in Kramer, Maguire, Halfer, et al. (2011).
Healthy Unit Work Environments (HWE)
HWEs, defined as unit environments that enable nurses to engage in the eight professional practice processes and relationships identified as essential to quality patient care (Kramer & Schmalenberg, 2002), facilitate NLRNs meeting professional role demands that emanate from increased patient acu NLRNs who engage in initial professional practice on HWE units experience less environmental reality shock (Kramer, Brewer, et al., 2011) and have higher retention rates than NLRNs on other units (Kramer et al., 2012). HWEs are also related to increased patient safety and improved patient outcomes (Institute of Medicine [IOM], 2004).
Steps and components of the eight professional practice processes that constitute HWEs were measured with the Essentials of Magnetism II© (EOMII) process instrument. National Magnet Hospital Profiles (NMHP) based on EOMII data from more than three fourths of the 341 Magnet hospitals have been established (Kramer & Schmalenberg, 2002, 2012; Schmalenberg & Kramer, 2008). VHWE are EOMII scores ≥1 standard deviation (SD) above the NMHP mean, HWE are EOMII scores between 1 SD above and 1 SD below the NMHP mean, Work Environments Needing Improvement (WENI) are EOMII scores ≤1 SD below the NMHP mean. Most Magnet hospitals reflect a 54% VHWE, 28% HWE, and 18% WENI distribution of clinical units, but NLRNs are placed on all three types of units during the transition and integration processes of professional socialization (Kramer, Maguire, Brewer, & Schmalenberg, 2011).
Overview of Research Program
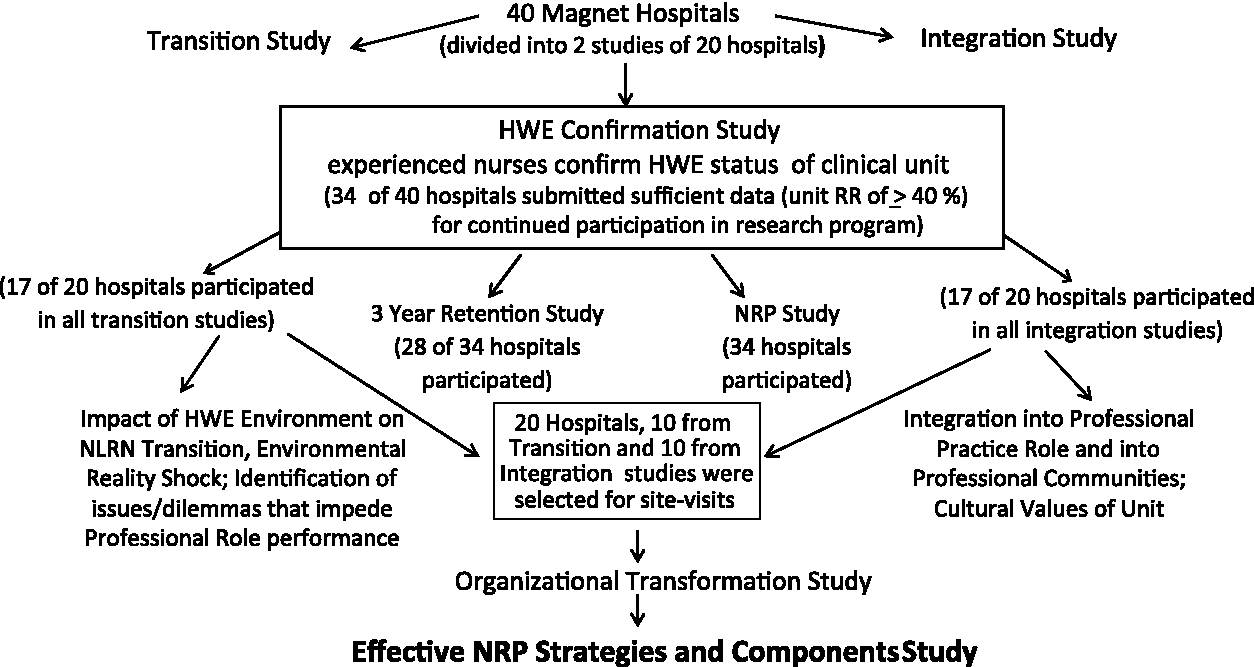
This 5-year program, designed to assess the impact of HWEs and NRPs on NLRN transition and integration into professional practice, consisted of seven studies. The study reported here is bolded in Figure 1. National representation (Kramer, Maguire, Brewer, et al., 2011) by geographical location, type of hospital, and size of community guided sample selection for the original 40 Magnet hospitals, for the split of the 40 hospitals into 20 Transition and 20 Integration-stage hospitals, and for selection of the 20 hospitals for the qualitative study reported here. To be selected for the 40-hospital sample, hospitals had to have NRPs operative for at least 3 years. For all studies, half of the hospitals were selected because they had published NRPs—Versant, United Health Consortium, Milwaukee, Practical Application of Clinical Experience (PACE), Transitioning Across the Continuum (TRAC), Dedicated Transition units, Building Excellence Together through Mentorship. The other half of the hospitals had “hospital-developed” programs. Six of the original 40 hospitals were dropped from the research program because of EOMII unit response rates ≤40% (Kramer, Schmalenberg, Brewer, Verran, & Keller-Unger, 2009). This decreased the pool for sample selection in the remaining studies from 40 to 34 hospitals.
Impact of healthy work environment and nurse residency programs on NLRN expectations, retention, transition, and integration into clinical nurse professional practice role
The HWE/NRP research program utilized environmental role theory (Kramer, Brewer, et al., 2011), Brewer, Verran, and Stichler’s (2008) Systems Research Organizing Model, and Donabedian’s (1988) Structure-Process-Outcome framework to guide selection and decision making related to design, sample, measurement, and analysis. The program was also guided by the “Best of the Best” principle—that is, to find out “what works” ask people who are working/practicing on units or in departments where it is most likely that “what works” will be operational and consequently identifiable. To obtain a sample of the Best of the Best hospitals, the 40-hospital sample was selected on the basis of excellent designations (Balridge, Thomson Reuters Top 10, Top 100 Hospitals, Health Grades Awards, Best Places to Work, Leapfrog Group Top Hospitals, JD Power and Associates Distinguished Award) in addition to Magnet.
Purpose
The goal of this study was to elicit from NLRNs and experienced nurses practicing on clinical units with confirmed VHWE, the components and strategies of NRPs effective in NLRN integration into the professional practice nurse role. NRPs and HWEs are structures that enable or promote the transition and integration processes of professional socialization that lead to desired outcomes—decreased environmental reality shock, increased retention and higher “nurse-assessed” quality of patient care. Transition and integration processes were assessed through identification of effective NRP strategies/components related to each of the seven issues of concern.
Method
Design and sample
In this qualitative study, site visits of 1.5 to 4 days (average = 2.5 days) were made by one of three Health Science Research Associates (HSRA) investigators to each of the 20 hospitals selected from the 34-hospital sample. Purpose of the visit was to conduct interviews and make participant observations. Data were collected in three, 1.5-month segments from October to mid-December (2009), February to March (2010), and from April to mid-June of 2010 to allow for periodic transcription and analyses.
Units for interviews were selected based on two criteria: (a) They regularly employed NLRNs and (b) they had “experienced nurse-confirmed” VHWE (Kramer et al., 2009). To be selected, hospital had to have at least five clinical units meeting the two criteria above.
The method developed by Haas and Shaffir (1987) to understand the relationship between dilemmas faced by physicians in their initial practice role was adopted for use in this study of NLRNs. Identification of dilemmas (MDs) or issues of concern (NLRNs) and corresponding competencies that need to be developed provide the basis for planning and selection of content and activities for Intern-Residency program. The seven issues of concern discussed earlier—delegation, prioritization, conflict resolution, and so on—were used to construct the interview schedule and as the basis for selection of participant observations. The lead-in interview question was, “What does this hospital do, what components, people, or strategies have or are helping you (or NLRNs) master the professional practice role of the nurse?” This was followed by “What has helped you learn how to delegate? Prioritize? How to work within the nursing care delivery system to get your work done?” (Interviewers used the words dilemmas or issue of concern, rather than problem, as NLRNs often associate the latter with individual deficiencies). Interview schedule was pretested on eight nurses in a local Magnet hospital; changes were made as indicated.
Data collection instruments and procedures
Individual and small group (two to three RNs) interviews were conducted with two to four NLRNs and experienced nurses on each of the selected VHWE units. Experienced nurses on units where NLRNs are practicing not only participate in NRPs but are also in a position to observe how well NLRNs are transitioning and integrating. Nurse managers on all selected VHWE units were group interviewed. Group or individual interviews were conducted with hospital/unit educators. Purpose, interview questions, and seven issues of concern or challenges were explained in writing and verbally prior to the interview. To accommodate 12-hr schedules, interviews and participant observations were conducted as early as 6:00 a.m. and as late as 9:00 p.m. On-site investigators appointed by each hospital obtained Institutional Review Board approval. Permission to digitally record interviews was obtained before commencement of interview.
An interview schedule was developed and pretested on nurses in a local Magnet hospital. In addition to validating the interpretation/meaning of questions, pretesting enabled investigation of differences in responses from individuals and small groups. Mayan (2001) recommends focal-group interviews if difficulty in accessing information from participants is anticipated. No differences in spontaneity, content of responses, or in willingness to share were noted between individual and group interviewees. Preferences for group or individual interviews were made by interviewees and on-site investigators.
Participant Observations (Strauss, 1987) of NLRNs engaged in activities such as giving or receiving change-of-shift report, team huddles, and interdisciplinary patient rounds were made in each of the 20 hospitals. In 12 hospitals, interviewers also observed NLRNs giving individual or group presentations, often during Clinical Coaching sessions. Observations of NLRNs’ evidence-based practice or evidence-based management presentations, participation in shared governance councils, and participation in Conflict Resolution or Crucial Conversations sessions were conducted in eight hospitals.
An audit trail was established to substantiate trustworthiness of the large volume of data. These data included notes about the context of the study, methodological decisions, and self-awareness of the researcher (Rodgers & Cowles, 1993; Strauss, 1987). An analyses and syntheses of literature related to the seven issues of concern identified by NLRNs were completed by the last seven coauthors and withheld from the interviewers until all digital transcriptions had been analyzed.
Many interviewees offered contextual documentation of effective components and strategies that they had cited during their interviews. Some mailed documentation to the investigators after the site visit. These contextual data were combined with the digital recordings for analysis as they supplemented descriptions or observations of effective strategies and components.
Data analysis
Paterson, Thorne, Canam, and Jillings’ (2001) meta-analysis/meta-synthesis procedures were used to analyze the content of participant observation notes and interview transcriptions. Utilizing constant comparative analyses (Strauss, 1987), data were compared and analyzed, and tentative categories, that is, abstractions of phenomena observed (component/strategies) were formulated for each of the seven issues.
To be classified as effective, a strategy or component had to be cited by at least half of the interviewees on half of the units in a hospital. Interviewers were careful not to suggest or lead interviewees into confirming strategies already identified by other interviewees. Two self-awareness, data-analytic decisions warrant explication. To avoid intellectual contamination and premature categorization of interview recordings and participant observation notes, the last seven coauthors who performed the literature analyses were not informed of the potential analytical categories until after the constant comparative analyses were completed. Nor did the interviewers know the results of their literature searches prior to analysis of the transcripts.
As in most qualitative reports, quotes will be used to illustrate ideas and experiences, evoke emotion, and support researcher conclusions. Principles and cautions cited by Sandelowski (1994) were used to achieve a proper balance between the obligations of scientific reporting and the taking of artistic license. Excerpts from multiple interviewees will be separated by ellipses points.
Results
Whereas core clinical competencies change over time (American Organization of Nurse Executives [AONE], 2010), the same seven management issues identified as problematic for NLRNs as early as 1966 continue to be of high concern today. None of the interviewees suggested additional or different issues. Virtually all agreed that these were the major problem areas encountered by NLRNs. Interviewees had little difficulty describing the parameters or dimensions of the concern—How, in what way does delegation cause you difficulty?
A few NLRNs with accelerated degrees who had worked as physician’s clerks or research assistants reported less difficulty developing collaborative RNMD relationships than did younger NLRNs who had not had such work experiences. Some concerns were described as having both a management and a clinical component. In Clinical autonomy, for example, critical thinking and corresponding decision making requires clinical knowledge, judgment, and competency. However, deciding whether to make an independent or an interdependent decision (Fagin, 1992) and how to effect this decision was perceived primarily as a management skill.
There was no question that NRPs were highly valued by virtually all interviewees. The Transition stage and role/activities of preceptor were well developed and implemented; the Integration stage, less so. The role and career development relationships and activities of Clinical Coaches were present in only about a third of the hospitals but, in those hospitals, it was clearly developed and well appreciated. The role, relationship, and activities of Mentors were seldom mentioned by interviewees in this study, although frequently the term mentor was used in lieu of preceptor. The seldom mention of mentor may well have been because the primary focus of this study was the issues impeding and the competencies needed to enact the professional practice role of clinical nurse, whereas the goal of the mentoring relationship, as defined online and in the literature, is related to another aspect of professional integration, that is, career planning and development and integration of newcomers into the various professional communities (practice group, shared governance councils, state and national organizations).
Characteristics of clinical units
The 20 hospital site visits resulted in 82 participant observations and 907 interviews with 330 NLRNs, 401 experienced nurses, 138 nurse managers practicing on 174 VHWE units, and 38 hospital/unit nurse educators. The number of interviewees in each hospital ranged from 25 to 76 with a mean of 45. Number of units per hospital ranged from 5 to 14 with a mean of 9. Largest number were Intensive Care Units (n = 40; 23%) followed by Telemetry (n = 28; 16%), Surgical Specialties (n = 26; 15%), Medical/Surgical (n = 21; 12%), Medical Specialties (n = 19; 11%), Oncology (n = 12; 7%), Obstetrics (n = 9; 5%), Emergency (n = 7; 4%), Orthopedic (n = 5; 3%), and Psychiatric, Rehabilitation, and Post Anesthesia Care Unit (PACU/Operating Room (n = 7; ≤2% each).
Characteristics of interviewees
At the time of interviewing, 71% (n = 236) of the 330 NLRNs were between 9 and 12 months post hire, well into the Integration stage of professional socialization. The other 29% were evenly divided between those who had 6 to 8 months of experience and those who had between 13 and 15 months. Almost 80% of the NLRNs participating in the program were prepared at the baccalaureate level; 4% had earned a master’s degree as initial nursing preparation. This is reflective of the total sample of NLRNs in the 34-hospital sample (Kramer, Maguire, Halfer, et al., 2011). Over half of the experienced nurse interviewees had between 5 and 15 years of experience; the others were evenly divided between those who had <5 or >15 years. Almost 90% of the experienced nurses were preceptors, >80% for several cohorts. More than 20% had served as clinical coaches.
Effective NRP Strategies and Components
The effective strategies and components of NRPs resulting from analysis of interview and participant observations recordings, and of the contextual data provided for the seven management issues of concern will be presented in two parts. The first will be the dimensions of the issue—How, in what way is delegation difficult for you? This presentation will be followed by the NRP strategies identified as effective in NLRN transition and integration into the dominant professional practice role of the nurse. Reference citations provided by interviewees will be included.
Some strategies were identified as effective in developing competency in more than one of the seven management issues. For example, similar strategies were mentioned for delegation, prioritization, and for getting work done areas. Other strategies were identified as effective for collaboration and clinical autonomy. Components and strategies will be cited in the area of most frequent citation.
Effective strategies for delegation, prioritization, and collaborative RNMD relationships were frequently begun in Transition and continued through Integration stage. Strategies in some of the seven areas, such as restoration of self-confidence through feedback, had a different focus in Transition than in the Integration stage. In Transition, feedback was related to NLRNs skill performance or specific patient care activities. In Integration, feedback was more often focused on how well NLRNs provided care and managed clinical situations for multiple patients, simultaneously.
Many interviewees, particularly experienced nurses and nurse managers, described projects and activities that positively impacted nursing practice but were unrelated to or not directly related to NRPs. These have been analyzed and presented in a separate report (Kramer & Schmalenberg, 2012).
Delegation
Dimensions of the issue
Three categories emerged from the analyses: (a) Why delegate? (b) Do I delegate accountability, responsibility or both? (c) What constitutes delegation?
I know I should delegate, but PCAs (Patient Care Assistants) can do it faster than I can. I want to do them myself, so I learn and pick up speed . . . I was an aide here; we were equals, but now I have to tell PCAs what to do and hold them responsible for doing it . . . Aides are old enough to be my mother—asking them to do something is like telling my mother what to do . . . It takes more time to supervise PCAs, check to see that they did the task and did it right . . . I want to do it myself so I can show people that I can do it and earn their respect . . . delegation is a sign that I’m disorganized.
The second category was the accountability issue. When you delegate, do you delegate responsibility and accountability as well as the task? Or, the task only? Or, task and responsibility?
A third category cited by a majority of NLRNs and a third of the experienced nurses was:
Delegating a task to a PCA is not “delegating” if the delegated task is listed in the PCAs job description. And, if it is not delegating, then I am not responsible or accountable and I don’t have to spend my time supervising the PCA and seeing to it that the task was done correctly.
This perception of delegation is also reported by Anthony, Standing, and Hertz (2001) in a national survey evaluating nurses’ beliefs about their abilities to delegate and supervise direct nursing activities. The time conservation issue was very important to NLRNs. “If I delegate and have to spend time supervising and checking to see that the task was done, I might as well do the task myself; it takes less time.”
Effective strategies
The most helpful component cited by large numbers of interviewees in 11 hospitals was Evidence-Based Management Practice (EBMP) projects presented and discussed at monthly coaching/focus group/debriefing sessions. Often done jointly with other NLRNs or with clinical coaches, the EBMP process is similar to evidence-based practice with the addition of an internal organizational data step such as conduct of interviews or observation of peers (Titler et al., 2001). EBMP projects addressed questions such as, “What is the difference between delegation and assignment?” “Can responsibility and accountability for outcomes of a task be delegated?” and “Do you delegate to other RNs or only to Patient Care Assistant (PCAs)?”
In one hospital, a copy of a PowerPoint presentation titled, “What is Safe Delegation?” A New Grad Perspective was given to the interviewer. This presentation included the “Dead on” game strategy (Alfaro-LeFevre, 2009), which the NLRN interviewee and her peers found very helpful.
Prioritization
Dimensions
All three groups of interviewees but particularly experienced nurses reported that NLRNs have difficulty in “prioritizing patients in an assignment,” “prioritizing care, tasks and activities for all patients in an assignment,” and “understanding the unit priority system.”
What are you going to do first, Why? Which is more important? Why? What could happen if you don’t do this for this patient now? What is most important to the patient? For some patients: what adverse events have the highest probability of occurring? What will you look for to see if this is happening? How will you handle this?
NLRNs also reported difficulty in meeting the demands and obtaining the benefits of multitasking.
My preceptor walked in, greeted the patient by name, put her hand on the patient’s arm, smiled, and said: “do you remember me? I was your nurse yesterday.” Patient said, I remember you, we talked about (_______), but I don’t remember your name.” I’m Nurse Julie and this is Nurse Beverly. She and I will be taking care of you today. Did you sleep well last night? While the patient was answering, Julie’s hand moved to the patient’s wrist; she checked her pulse and watched her respirations. Then she asked the patient, how is the movement in that arm (with the IV)? Can you give my hand a squeeze? Then she asked: What did you eat for breakfast? I see that you still have a little of it on your lips. She took a Kleenex and wiped the side of the patient’s mouth where she was drooling a bit. Within a few minutes, and with the same activities, Julie had checked the patient’s vital signs, mentation, memory, color and skin temp, and degree of movement. I completely missed that she had checked her for dysphasia, which I have since learned is top priority on our unit because it may indicate an impending repeat stroke.
Effective strategies
Interviewees cited Coaching sessions in which EBMP projects were presented as the most effective strategies in learning how to prioritize care for a group of patients. In one of these sessions, a mock change-of-shift report on five to six patients was presented. NLRNs then listed care activities/observations/needs for each patient indicating what they would do first, second, and so on. Then the lists from each nurse were compared and discussed, looking for similarities, rationale, reasoning and judgments that lay behind the decisions made. These sessions were short (20-30 min in length) and were often attended by seasoned nurses/managers who would insert “unexpected happenings” so that NLRNs would need to demonstrate awareness of last minute prioritization changes that would be needed.
Another effective strategy was a class/activity on identification of prioritization patterns or systems for different patient populations. Several coaches explained it this way:
First, we present Nelson et al’s (2006) prioritization system based on patient problems. Airway, breathing, circulation (ABC) is top priority, followed by pain, elimination, change in mental status, risk of infection, safety. Medical problems is second, and third is the need for patient teaching, changes in activities of daily living, and other concerns of the patient . . . After they have that down pat, we explain that recognizing the dominant priority system for the patients on their unit will help them immensely . . . After ABC, you look for the dominant pattern for the patients on your unit. For oncology patients—pain control is top priority . . . In the ER, after ABC, the next priority is often doing what you need to do to get patients home or transferred out of the ER to the units so there’s room for other patients. I know that sounds very bureaucratic or money hungry, but we are here to provide a service and you are not doing that if patients are struggling to breathe or are in severe pain in the waiting room, while others who have been seen or are lying there waiting to be transferred . . . I never thought about it before but, in a way, that’s also true on rehab. Who’s scheduled first for therapy? You pass meds, do assessments, and get them ready so they can make their therapy appointment on time. That’s why those patients are here.
Getting Work Done: Managing Patient Care Delivery
NLRNs, experienced nurses, and managers in all hospitals had no problem expressing the difficulties that NLRNs had with this issue of concern. NLRNs expressed it as follows.
Getting my work done on time . . . dealing with constant interruptions . . . it’s CHAOTIC! Some days, I just feel like screaming! . . . I feel like I’m drowning from trying to do everything I need to do for 6 patients . . . What delivery system? There is no system. It’s the number of patients divided by the number of nurses and you race around trying to get everything done. That’s it. Did you know that studies show that patient mortality doubles when nurses have 10-patients versus a 5-patient assignment? . . . I’m scared to death that I will harm or kill a patient!
A few strategies were described by interviewees as helpful but none met the effective criterion identified for this study—half of the interviewees on half of the units in the hospital. Additional data are being collected. Results of analysis of new and old data will be reported in a subsequent article.
Clinical Autonomy—Making the “Right Decisions”—Doing No Harm
Dimensions
Two dimensional categories were cited most frequently by NLRNs. “What exactly is clinical autonomy and how does it differ from shared governance or participating in decisions about time off, vacation, and running of the unit during staff meetings? What exactly is the difference between independent decision making and interdependent decision making?”
A second dimension concerned timing, competence, and readiness. “I’m not ready yet; I have to develop competence and confidence before I can make decisions on my own.” Another dimension, identified only by experienced nurses, managers, and educators was related to the advice: “If you don’t know, ask” and “The only stupid question is the one you don’t ask.” NLRNs ask too many questions for which they already know the answer (Kramer & Schmalenberg, 2012).
Effective strategies
Preceptors, coaches, and managers reported that they may have learned as much participating in NRPs activities related to autonomy as did NLRNs. This was because NRPs often stimulated formation of Preceptor and Clinical Coach Councils as part of Shared Governance.
Autonomy was frequently the focus of these Council meetings. “I learned the difference between types of autonomy, independent and interdependent decision making, and relationship of autonomy to standing orders from participation in Coaching Council activities.”
Formal classes, computer simulations, and clinical coach presentations were cited as effective in reinforcing the critical thinking and decision-making components of clinical autonomy, and the relationship between autonomy and competence. “Did you know that physicians judge nurses’ competence primarily on the basis of their autonomous decision making?”
EBMP projects were frequently cited as an effective component. These projects often involved NLRNs interviewing experienced nurses on their unit to ascertain how they made decisions, when they called the physician instead of making an independent decision, and what they thought about before making either an independent or an interdependent decision (Fagin, 1992).
RNMD Collaboration
Dimensions
In general, NLRNs experience more collaboration difficulty with physicians than with representatives of any other discipline. Two dimensions needed for collaboration were cited by preceptors, coaches, and managers: (a) the nurse must portray competence and self-confidence and (b) structure and opportunity to collaborate must be available. NLRNs added a third dimension. “The words were used but we never did it in school or saw it happening with faculty . . . I’m not clear on exactly what collaboration means . . . MDs don’t see new grads as competent.”
Effective strategies
Three effective strategies were cited for advancing RNMD collaboration—interdisciplinary patient care rounds, SBAR—situation, background, assessment, and recommendations—communication technique and the rehearsed phone call. Only the latter is a common component of NRPs. All three need to begin in the Transition stage. Another strategy enthusiastically and universally endorsed in one hospital was a PowerPoint presentation made by coaches to new graduate nurse cohorts. Medical students and residents were also invited to attend; many did, as did the interviewer. A summary of some of the slides follows.
RNMD collaboration is a synergistic alliance that maximizes the contributions of each participant resulting in an action that is greater than the sum of what each professional contributes. The R in SBAR provides as opportunity for collaboration. Collaboration is based on MDs perceiving RNs as knowledgeable, competent professionals with a unique body of knowledge of benefit to the patient. Three prerequisites for collaboration are: 1) competence in the profession’s unique domain; 2) self-confidence and high self-esteem and; 3) effective communication. Physicians often insist upon reports in bullets. Nurses tend to report in narrative, and must learn how to bulletize their reports.
Texting messages to physicians to relay supporting data and a decision made was a common, effective communication technique in four hospitals. This practice, an outcome from a hospital-wide RNMD Collaboration committee, was well received and universally applauded.
Constructive Conflict Resolution
Dimensions of the challenge
A primary source of NLRN conflict occurs while delegating tasks to aides, but disagreements and conflict also occur between/among nurses and other disciplines.
If I ask an aide to do something, she will think I’m trying to push my work off on her. That causes conflict and bad feelings. Or she will just look at me, grunt and walk away. I don’t know whether she’s going to do it or not . . . Some RNs leave the patient’s room or even worse, the patient himself is a mess with important things left undone. Or she will say, “Oh, let’s see, did I do that, I meant to but I got distracted.” I begin to doubt if I can believe anything that RN is telling me. It gives me a very unsafe feeling and then I wonder how “safe” the patient is feeling. And it’s not just one time—it’s over and over.
Effective strategies
Two structural components not associated with NRPs—sessions on the principles of constructive conflict resolution, and conflict resolution workshops such as Crucial Conversations (Maxfield, Grenny, McMillan, Patterson, & Switzier, 2005)—were cited as effective in assisting NLRNs in developing competency in constructively resolving conflicts.
Feedback to Restore Self-Confidence
Dimensions of the challenge
Expectation-reality generated stress, known to occur in nursing as well as in other health care professions (Duchscher, 2012; Kahn, Wolfe, Quinn, Snoek, & Rosenthal, 1964; Kramer, 1974; Kramer, Maguire, Brewer, et al., 2011), causes a marked diminution of self-confidence and self-esteem. This interferes with NLRNs’ development of competence particularly in the areas of Clinical Autonomy, and RNMD Collaboration. Meaningful feedback can restore and augment self-confidence.
Ill-timed rites of passage such as graduation exercises held at the end of Transition stage (3-4 months post-hire) prematurely signal to NLRNs and others that the NLRN is competent and ready to enact the full professional practice role of nurse—care of and management of clinical situations for multiple patients, simultaneously. “They think I’m ready, but I know I’m not . . . Others expect more than I can deliver.” This conflict leads to additional loss in self-confidence and self-esteem.
Effective strategies
Feedback, a cornerstone of the Transition stage, takes different forms when NLRNs are “on their own” and when they are becoming integrated into the professional role. Forms identified include (a) assignment to a “difficult” patient, or a patient whose condition is volatile, prioritizing comments such as “You had a tough assignment today—good job,” “that was the right call,” or “well organized report”; (b) sending a consulting physician to the NLRN for report on his patient; or (c) NLRN being asked technical questions by experienced nurses, such as appropriate drug dosages or reactions.
Frequently cited as effective strategies were Feedback Workshops and the Generation Pact. Workshop content and activities included a discussion of concepts, forms, and sources of feedback, feedback principles and an opportunity practice principles in mock sessions—after a staged event, attendees use feedback principles to provide constructive feedback (La Monica & Karshmer, 1978; Schmalenberg & Kramer, 1979). The Generation Pact feedback system is an agreement between the NLRN (now 1 year post-hire), her Preceptor, and her Clinical Coach to provide daily or at least very frequent feedback to each other on performance of various aspects of the professional nursing practice role. This strategy demonstrates that, in addition to receiving feedback initiated by others, NLRNs need to seek out ways to elicit the feedback needed to evolve, sustain, or restore their self-confidence.
Discussion
Results of this study support the recommendation that development of two-stage, Transition plus Integration, NRPs are no longer an option but a necessity. These NRPs need to have clearly differentiated goals, components, expected role performance, and rites of passage. The career development relationships of preceptor, clinical coach, and mentor need to be articulated, defined, and introduced during the proper stage. The IOM (2010) advocates development of NRPs and recommends financial public and professional support for their development and implementation. The AONE (2010) advocates a two-stage program, a structured, precepted transition program to guide and support NLRNs, as well as a posttransition support program for acquisition of the professional role. Performance and cost-effectiveness due to stress reduction and increased retention have been demonstrated in the HWE/NRP program studies as well as in other studies detailed in Kramer, Brewer, et al. (2011) and Kramer et al. (2012).
The stability of the seven issues of high concern to NLRNs over time suggests that discussion of these seven management areas needs to be incorporated into professional nursing curricula during the Academic stage of professional socialization. Didactic content such as the American Nurses Association (ANA) definition of delegation and the delegation model, and the five Rights and Principles and Decision Tree for Delegation to PCAs would be of some help, but even more beneficial would be discussions centered on NLRNs perceptions and descriptions of the dimensions of the seven management areas. As with many health care professions, but particularly with nursing, it is not possible to provide nursing students experiences in the dominant professional practice role—care of and management of clinical situations for multiple patients simultaneously. Students could be assigned to care for two or three patients but professional responsibility and accountability is not the same in a dependent, supportive relationship as it is in an independent relationship. Providing students with discussion and activities to help them deal with issues such as how to prioritize multiple care, tasks, and activities for multiple patients; what is the difference between delegating a task or activity to a nonprofessional worker and transfer of responsibility for a patient to a professional practitioner; and what is the difference between transfer of professional responsibility for a patient and sharing professional practice or engaging in professional teamwork with a colleague?
NRPs are not synonymous with orientation programs, extended or otherwise (Bleich, 2012). The purpose of orientation programs is to help all new employees, professional and nonprofessional, to “determine their bearings or sense of direction” (Gove, 1971, p. 1591). An orientation is focused on the physical environment and hospital organizational policies and procedures—location of dining room, parking, fire, and evacuation drills, regulations regarding illness and absence. Professional socialization programs such as NRPs, fellowships, internships, and clerkships assist newly licensed aspirants through skill acquisition, guided evolutionary stages of professional judgment, and eventually effective performance of the professional role. They also continue the internalization and operationalization of professional values begun in academia, and they guide career development and integration of new practitioners into professional communities. Classifying NRPs as orientation programs is a disservice to the hospital and to the profession. NRPs are cost-effective investments (Ulrich et al., 2010) as well as attractors. NLRNs in this study frequently commented that not only did they highly value the NRP, but they were also attracted to “this specific hospital because of its NRP.” Some added that they drove more than 100 miles a day to and from this hospital so that they could begin their introduction into professional practice in this “Best of the Best” hospital.
Healthy Unit Work Environments augment the positive effects of NRPs (Kramer, Brewer, et al., 2011). It is suggested that everything possible be done to provide the structures (Kramer et al., 2010) needed for development of HWEs. Some HWE structures are the same as the strategies/components of NRP effective in NLRN development of competency in one or more of the seven management areas. For example, Interdisciplinary Patient Care Rounds or hospital-wide RNMD committees with representation from clinical nurses, not only promotes a HWE but also helps NLRNs development RNMD collaborative relationships. Clarification of the relationships between independent decision making in discipline-specific spheres of practice and interdependent decision making in overlapping spheres of practice (Fagin, 1992) has the potential for positively impacting nurses’ autonomous decision making. Clinical autonomy is not only an essential practice process in a HWE but also one of the seven areas of concern for NLRNs.
Because of their enthusiastic and frequent mention, we strongly recommend implementation of the following two components/strategies. The first is the creation of Preceptor and/or Clinical Coach Councils in the Shared Governance or hospital committee structure. Such Councils foster development of training and education programs for Preceptors and Clinical Coaches as well as promotion of formal and informal discussion of role enactment and suggestions for improvement. Of particular help were discussions on differences between the preceptor role (a supportive, dependent, cognitive apprenticeship relationship) and the Clinical Coach role (a peer career development relationship that fosters independence).
Implementation of EBMP projects have a high payoff as this strategy was identified as effective in the mastery of several competencies—prioritization, delegation, and clinical autonomy. EBMP projects were helpful not only to NLRNs but also to experienced nurses who explained: “EBMP projects stimulated me to improve my practice. When I helped my resident with her EBMP project, I learned the steps of evidence-based practice that I had not learned in school.” Another nurse explained, “These projects and presentations changed the culture, the soul of our unit—our way of looking at and evaluating what we are doing” (Kramer & Schmalenberg, 2012).
Footnotes
Acknowledgements
Participation in this interview/participant observation study required considerable time, effort and commitment on the part of the on-site investigators, chief nursing officers, nurse managers and clinical nurses in the 20 participating Magnet hospitals. In addition to obtaining IRB approval, on-site investigators and nurse managers were responsible for explaining the research to potential participants, planning of interview and work schedules, and arranging for the participant observations. The authors acknowledge the generous participation and thank: Donna J. King, RN, NE-BC, FACHE, Vice President Clinical Operations and Chief Nurse Executive, Advocate Illinois Masonic Medical Center, Chicago, IL; Shirley Wiesman, MSN, RN, ACNS-BC, Clinical Nurse Specialist and on-site investigator, Aspirus Wausau Hospital, Wausau, WI; Karen Profitt Newman, Ed D, MSN, RN, NEA-BC, VP, Chief Nursing Officer, Baptist Hospital East, Louisville, KY; Casey O’Brien, MSN, RN, CPN, Clinical Education Coordinator, Children’s Memorial Hospital, Chicago, IL; Cheri Hunt, RN, MHA, NEA-BC, Vice President/Chief Nursing Officer, Children’s Mercy Hospitals and Clinics and Children’s Mercy South Hospital, Overland Park, KS; Linda Everett, PhD, RN, FAAN, NEA-BC, CNO, and Mary Sitterding, RN, MSN, Director of Research and On-site Investigator, Indiana University Medical Kramer et al. 21 Center, Methodist Hospital, Riley Children’s Hospital, Clarian Health System, Indianapolis, IN; Janice Kishner, RN MSN MBA FACHE, Chief Nursing Officer, East Jefferson General Hospital, New Orleans, LA; Victoria Rich, RN, PhD, FAAN, Chief Nurse Executive PENN Medicine and Associate Professor of Nursing, PENN School of Nursing, Hospital of the University of PA, Philadelphia, PA; Susan Kelley, RN, MSN, VP and CNO, John C Lincoln Hospital, Phoenix, AZ; Carole Parisien RN, MSN, Nursing Analyst, Center for Nursing Research and On-site Investigator, Maine Medical Center, Portland, ME; Cynthia Padula, RN, PhD, Director of Research and On-site Investigator, The Miriam Hospital, Providence RI; Sheri Matter, MBA, MS, BSN, RN, NEA-BC, VP, Nursing Operations and CNO, and Sarah Harne-Britner, MSN, RN, CCRN, CNS-BC, Magnet Project Coordinator and On-site Investigator, Harrisburg Hospital and Community General Osteopathic Hospital, Pinnacle Health Systems, Harrisburg, PA; Donna D. Poduska, MS, RN, NEA-BC, Director, Resource Services and Onsite Investigator, Poudre Valley Hospital, Fort Collins, CO; Nancy J Lee, RN, MSN, VP Patient Care Services/CNO, Stanford Hospital & Clinics, Palo Alto, CA; Linda Birk, PD, RN, On-site Study Coordinator, University of Kentucky, Chandler Medical Center, Lexington, KY; Mary Jo Assi, MS, RN, APRN, BC-Director of Advanced Practice Nursing, The Valley Hospital, Ridgewood NJ; Deborah Fisher PhD(c), RN, PNP-BC, CPON, Nursing Research Facilitator and Onsite Investigator, Virginia Commonwealth University Medical Center, Richmond, VA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article