
Abstract
Loneliness occurs in people of all ages but can be particularly debilitating in older adults. In this population, there are many factors that enter into the loneliness–loss pathway. The purpose of this study was to examine the interrelations of situational factors, coping, and pet attachment that affect loneliness in 191 older adults who experienced loss over time. Data showed that loneliness was lower among study participants who lived in 55 and over residences than private residences, those who experienced loneliness due to loss, those who reported lower coping, and those who reported higher pet attachment. The results of this study suggest that nurses working with this population need to evaluate loneliness by means of situational factors such as living arrangements. Nurses should also examine the effects of loss over time and discuss coping mechanisms, including the benefit of pet relationships in this vulnerable population. Implications for nursing are addressed.
Loneliness has no boundaries and can be experienced by people of all ages; however, it may be heightened in older adulthood due to loss. Loneliness is often associated with forms of emotional and social isolation, particularly for older adults (Perlman & Peplau, 1982). In adulthood, individuals may experience loss of social networks due to the death of a spouse, parent, friend, colleague, neighbor, and/or pet (Krause-Parello, 2007). These losses experienced by older adults may increase the risk for social isolation (Coyle & Dugan, 2012). There are situational factors that may increase an older adult’s risk for loneliness, including being single/divorced/widowed, living alone, housing type, and poor health. According to the Administration on Aging (2011), 29% or 11.3 million noninstitutionalized older adults live alone, and it is posited that as this population increases, so will the number of individuals living alone. Alterations in situational factors may also increase the likelihood for ineffective coping mechanisms and networks that increase feelings of loneliness in older adults.
In the seminal literature, two factors and two forms of isolation have been identified in the loneliness discussion: (a) situational factors, (b) characterological factors, (c) emotional isolation, and (d) social isolation, respectively (Weiss, 1973). Situational factors that may influence loneliness include loss, divorce/separation, acute/chronic illness, and moving (Weiss, 1982). Characterological factors that can influence loneliness include personality characteristics such as introversion, shyness, and low self-esteem (Weiss, 1982). Over the past three decades, researchers have examined the characterological factors related to loneliness across the life span in great length (Anderson & Harvey, 1988; Kaiser & Berndt, 1985; Kalliopuska & Laitinen, 1991; Mahon, Yarcheski, Yarcheski, Cannella, & Hanks, 2006; Zimbardo, 1977). However, limited work has been published on the interrelation of situational factors and loss that impact loneliness. Therefore, this research will address a gap in the literature by providing valuable subjective insight on loss, based on situational factors that are known to influence loneliness in older adults.
Because emotional and social isolation play dual parts in the loneliness experience, it is important to understand the potential antecedents. Emotional isolation can result from a loss of close attachment such as a spouse, parent, friend, colleague, or pet, in contrast to social isolation that can occur from a lack of involvement with others limiting one’s social network. Regardless of the cause, loneliness related to loss in older adults is likely to increase over time (Coyle & Dugan, 2012).
Loss of a significant person or object can lead to loneliness. Research supported that there are temporal and sequential components that must be considered when examining the relationship between loneliness and loss in older adults (Krause-Parello, 2007). In addition, there are different types of loss that enter into the loneliness–loss equation such as loss of family members as well as health-related losses (Ward, Mathias, & Hitchings, 2007).
The loss of a spouse is the most common loss among older adults and has been suggested as the most stressful life event for older adults (Arbuckle & de Vries, 1995; Ward et al., 2007). There are many transitions that can occur due to loss of a spouse. Transitions may include changes in living arrangements (Adams, Sanders, & Auth, 2004), social support networks (Leen, 2010), and cognitive functioning (Ward et al., 2007).
Moreover, the loss of a child regardless of age or the amount of time that has passed is difficult for many parents to cope with (Smith, Nunley, Kerr, & Galligan, 2011). According to Smith and colleagues (2011), regardless of the length of time that has passed since the loss of a child, there are emotional and psychosocial outcomes for the parent. Moreover, recent research revealed that some older adults reported missing the emotional support derived from the parent–child relationship (Moore, 2007).
Coping mechanism and social support networks are important during the aftermath of a loss to help alleviate the feeling of loneliness (Weiss, 1974). In particular, for older adults as time passes, social networks and family support dwindle due to mortality (Parkes, 1988). According to Weiss (1969), relational losses, inevitable with age, should result in older adults seeking new coping resources and relationships to replace the lost provision of social support. However, many who have lost someone or something may find it difficult to move forward and spend a lot of energy and time thinking about the past (Moon, 2011). Due to life transitions, older adults may turn to friends, neighbors, and colleagues to become a significant part of their social network (Liebler & Sandefur, 1998).
Pets are often cited in the literature as a coping mechanism and a form of social support (Collis & McNicholas, 1998) for older adults (Krause-Parello, 2012) and help ease the pain of loneliness due to a loss. Research supported that a personal pet may serve as a companion and that this relationship may act as a coping resource for older females (Krause-Parello, 2008). Therefore, the purpose of this study was to examine the interrelations of situational factors, coping, and pet attachment that impact loneliness in older adults who experienced loss over time. The findings of this study will help in the understanding of how pets affect the loneliness–loss–time trajectory based on the knowledge uncovered from older adults who experienced loss.
Conceptual Framework
The theoretical framework guiding this study is based on the concepts and propositions regarding loneliness as loss in older adults, as posited by Lopata (1969) and Weiss (1969, 1973). According to Lopata, loneliness is defined as an emotion experienced by an individual who wishes for a level of contact unlike from the one currently encountered. Loneliness is also often accompanied by a sense of dissatisfaction with social interactions, as a consequence of emotional or social isolation due to a loss of significant others (Lopata, 1969; Weiss, 1973).
Weiss (1969, 1973) further proposed that older adults are vulnerable to relational losses and therefore are at risk for some degree of loneliness. The losses faced by older adults can be considered a natural part of life course transitions, and age-related losses and the loss of social contacts increase the risk of loneliness (Leen, 2010). Furthermore, Kübler-Ross (1969) and Parkes and Weiss (1983) in a further examination posited a theoretical link between time of loss and networks utilized as coping mechanisms in the grieving process. Therefore, based on the fact that loss is foreseeable with age and the understanding that there are situational factors and coping networks that affect the loneliness–loss pathway for older adults, this inquiry is an important area of study.
Purpose
This research sought to examine the following research questions:
Research Question 1: Do loss and loneliness differ according to situational factors for older adults? Research Question 2: What are the differences between type of loss and time period (≤11 months vs. ≥1 year) when loss was experienced for older adults? Research Question 3: What are the relationships between loneliness and situational factors in older adults? Research Question 4: What situational factors explain the most variance in loneliness and do coping and pet attachment together explain additional variance in loneliness for older adults?
Method
Design and Sample
This cross-sectional study was based on a secondary analysis of data from 191 participants who participated in doctoral dissertation research that examined subjective well-being of older adults (Krause-Parello, 2007). The inclusion criteria for participation in this analysis were men and women (a) aged 55 to 84, (b) owned a dog or a cat, (c) resided in a housing community specifically for older adults or attended a senior citizen community center, and (d) were able to communicate in English.
Instruments
Demographics
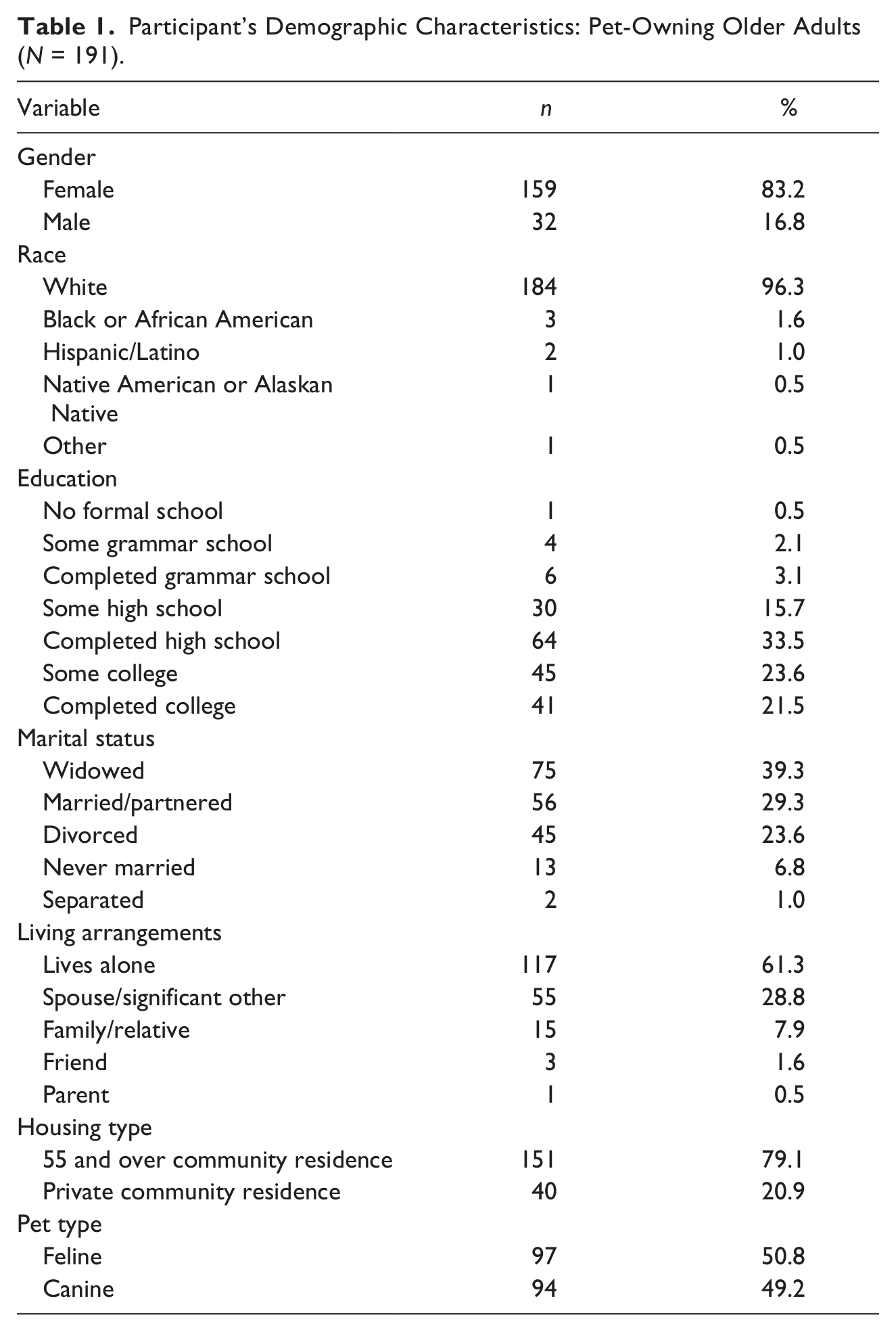
A demographic questionnaire was developed and used to collect situational factors. The demographic information collected included gender, race, education, marital status, living arrangements, health status, and type of pet (see Table 1). Additional questions were asked on the participants’ experience of loneliness due to loss, type of loss, and time period of loss.
Participant’s Demographic Characteristics: Pet-Owning Older Adults (N = 191).
The Revised UCLA Loneliness Scale
Loneliness was measured using The Revised UCLA Loneliness Scale (Russell, Peplau, & Cutrona, 1980). The 20-item summative 4-point Likert-type rating scale measures the subjective experience of loneliness by degrees of agreement and disagreement: 1 (never), 2 (rarely), 3 (sometimes), and 4 (often). Total scale scores can range from 20 to 80, with higher scores indicating higher levels of loneliness. Psychometric evidence for the Revised UCLA Loneliness Scale has been reported in college students (Russell et al., 1980) and older adults (Krause-Parello, 2007). The Cronbach’s alpha in this sample was .85.
Coping Strategy Indicator (CSI)
Coping was measured using the CSI: Seeking Support subscale (Amirkhan, 1990). The 11-item summative 3-point Likert-type scale measures seeking support as a coping mechanism by degrees of agreement and disagreement: 1 (not at all), 2 (sometimes), and 3 (a lot). Total scores can range from 11 to 33, with higher scores indicating a greater use of that coping strategy. Psychometric evidence for the CSI: Seeking Support subscale has been reported by the instrument developer (α = .93) and in older adults (Krause-Parello, 2007). The Cronbach’s alpha in this sample was .90.
Pet Attachment Scale
Pet attachment support (PAS) was measured by the Pet Attachment Scale (Albert & Bulcroft, 1988). The nine-item summative 5-point Likert-type rating scale measures PAS by degrees of agreement and disagreement: 1 (strongly disagree), 2 (disagree), 3 (neutral), 4 (agree), and 5 (strongly agree).The scale scores can range from 9 to 45, with higher scores indicating a higher level of pet attachment. The scale developer has given permission to substitute the word sad for lonely in Question Number 6, to avoid overlapping content with the Revised UCLA Loneliness Scale (K. Bulcroft, personal communication, March, 13, 2006). Psychometric evidence for PAS has been reported in a sample of community-residing pet owners representing various stages of family development from young married couples to older, widowed individuals (Albert & Bulcroft, 1988). The Cronbach’s alpha in this sample was .90.
Analysis
Data analysis consisted of descriptive statistics, independent t tests, Pearson correlation, and incremental multiple regression using SPSS for Windows®, Version 20. Two-tailed tests were used to determine the level of significance at the .05 level. Two groups for time period in which loss occurred (≤11 months vs. ≥1 year) were formed for analysis of period of loss. Time periods were coded as follows: 0 (none), 1 (≥10 year), 2 (6-9 years), 3 (3-5 years), 4 (1-2 years), 5 (7-11 months), and 6 (0-6 months). Losses for each participant were summed whereby the higher the total loss score, the greater was the perceived loss.
Results
The sample included participants (N = 191) whose age ranged from 55 to 84 years (M = 71; SD = 8.39), and the majority were White (n = 184, 96.3%), with a small percentage of Blacks (n = 3, 1.6%), 2 Hispanic/Latino, 1 Native American or Alaskan Native, and 1 undeclared individual. A majority of the participants completed high school (n = 64, 33.5%), some college (n = 45, 23.6%), or completed college (n = 41, 21.5%). The majority were widowed (n = 75, 39.3%), followed by married/partnered (n = 56, 29.3%), divorced (n = 45, 23.6%), or never married (n = 13, 6.8%), with a small percentage separated (n = 2, 1.0%). A majority of the participants lived alone (n = 117, 61.3%), followed by living with a spouse or significant other (n = 55, 28.8%), family/relative (n = 15, 7.9%), or a parent (n = 1, 0.5%). Most of the participants lived in a community for individuals aged 55 years and older (n = 151, 79.1%), while the remainder lived in a private community residence (n = 40, 20.9%). Participants had either a pet feline (n = 97, 50.8%) or a pet canine (n = 94, 49.2%; see Table 1).
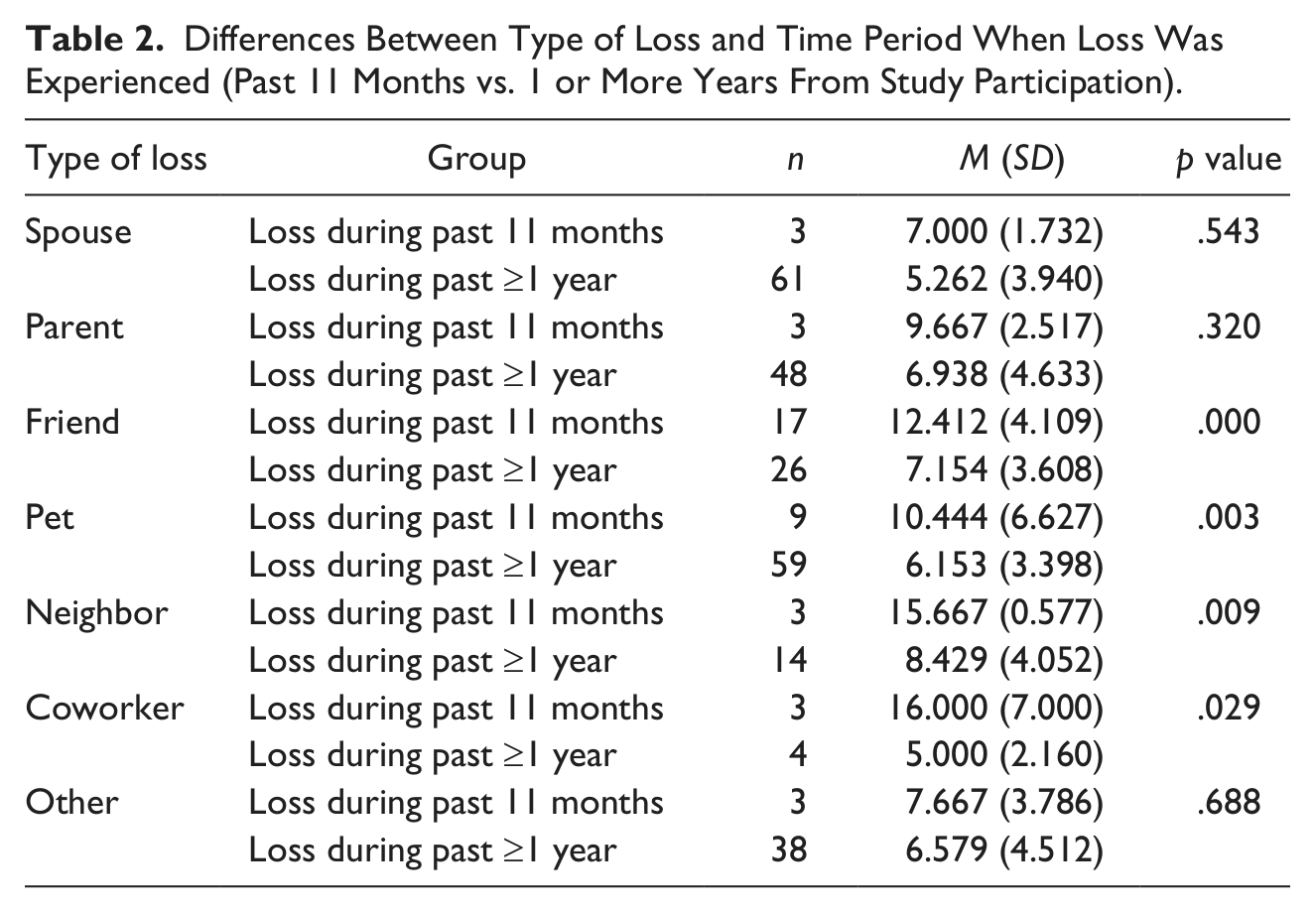
Independent t tests were conducted to evaluate whether differences occurred between the type of loss and time period when loss was experienced (≤11 months vs. ≥1 year) in the study participants. The test was statistically significant for participants who lost friends, t(41) = 4.42, p = .000; pets, t(66) = 3.11, p = .003; neighbors, t(15) = 3.00, p = .009; and coworkers, t(5) = 3.04, p = .029. No statistically significant differences (all ps > .05) were found between loss of a spouse, parent, or other, or according to gender as shown in Table 2. A follow-up analysis was conducted with alpha adjusted for seven loss groups (p ≤ .007); the test was statistically significant for participants who lost friends, t(41) = 4.42, p < .007, and for those who lost pets, t(66) = 3.11, p < .007.
Differences Between Type of Loss and Time Period When Loss Was Experienced (Past 11 Months vs. 1 or More Years From Study Participation).
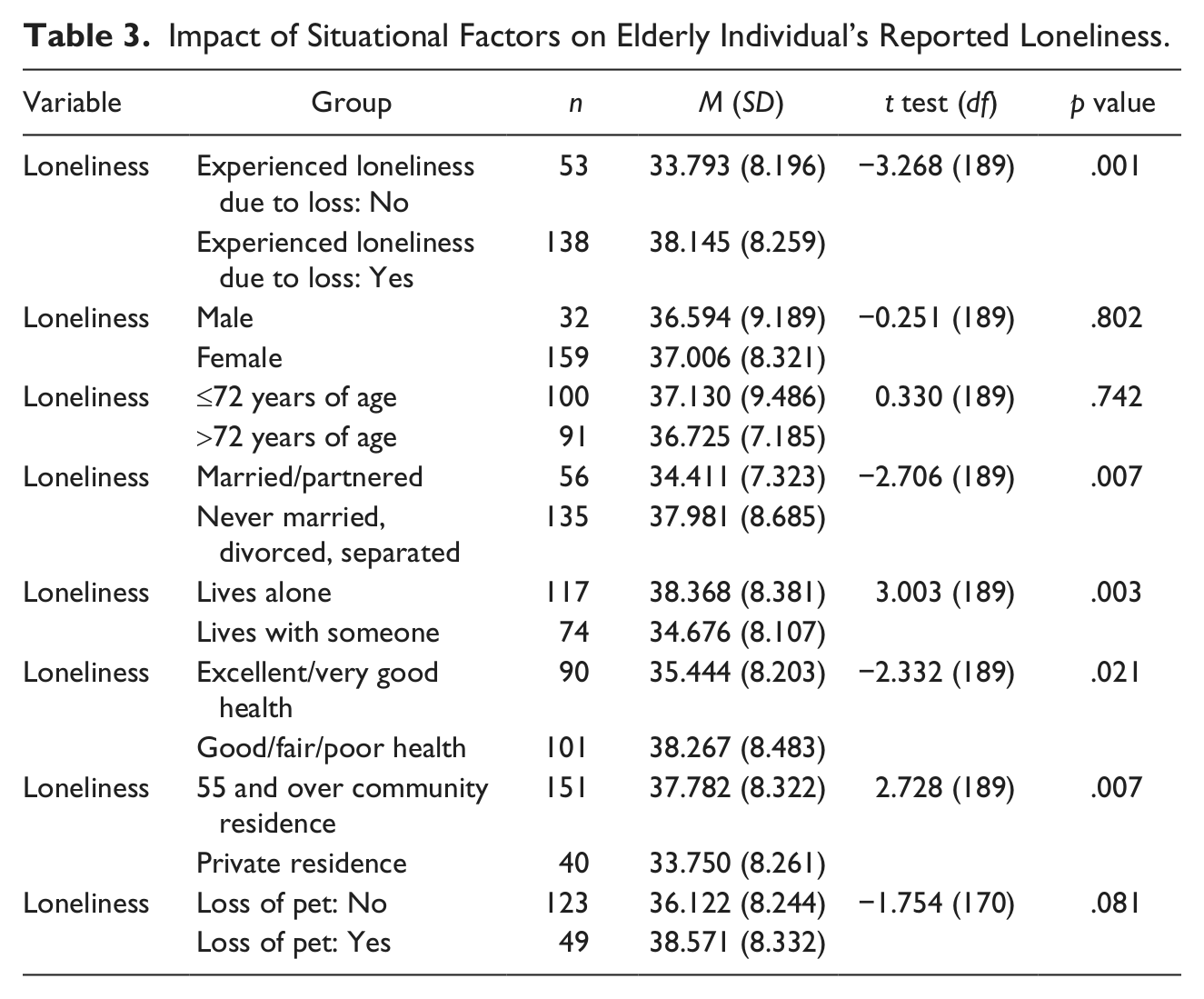
Independent t tests were also conducted to evaluate whether a difference occurred between situational factors and loneliness. The test was statistically significant for experience of loneliness due to loss, t(189) = −3.27, p = .001; marital status, t(189) = −2.71, p = .021; living arrangements, t(189) = 2.73, p = .007; health status, t(189) = −2.33, p = .003; and housing type, t(189) = 2.73, p = .007. No statistically significant differences (all ps > .05) were found for gender, age, or loss of a pet as shown in Table 3. A follow-up analysis was conducted with alpha adjusted for eight loss groups (p ≤ .006); the test was statistically significant for experience of loneliness due to experiencing loss, t(189) = −3.268, p < .006, and due to living alone, t(189), p < .006.
Impact of Situational Factors on Elderly Individual’s Reported Loneliness.
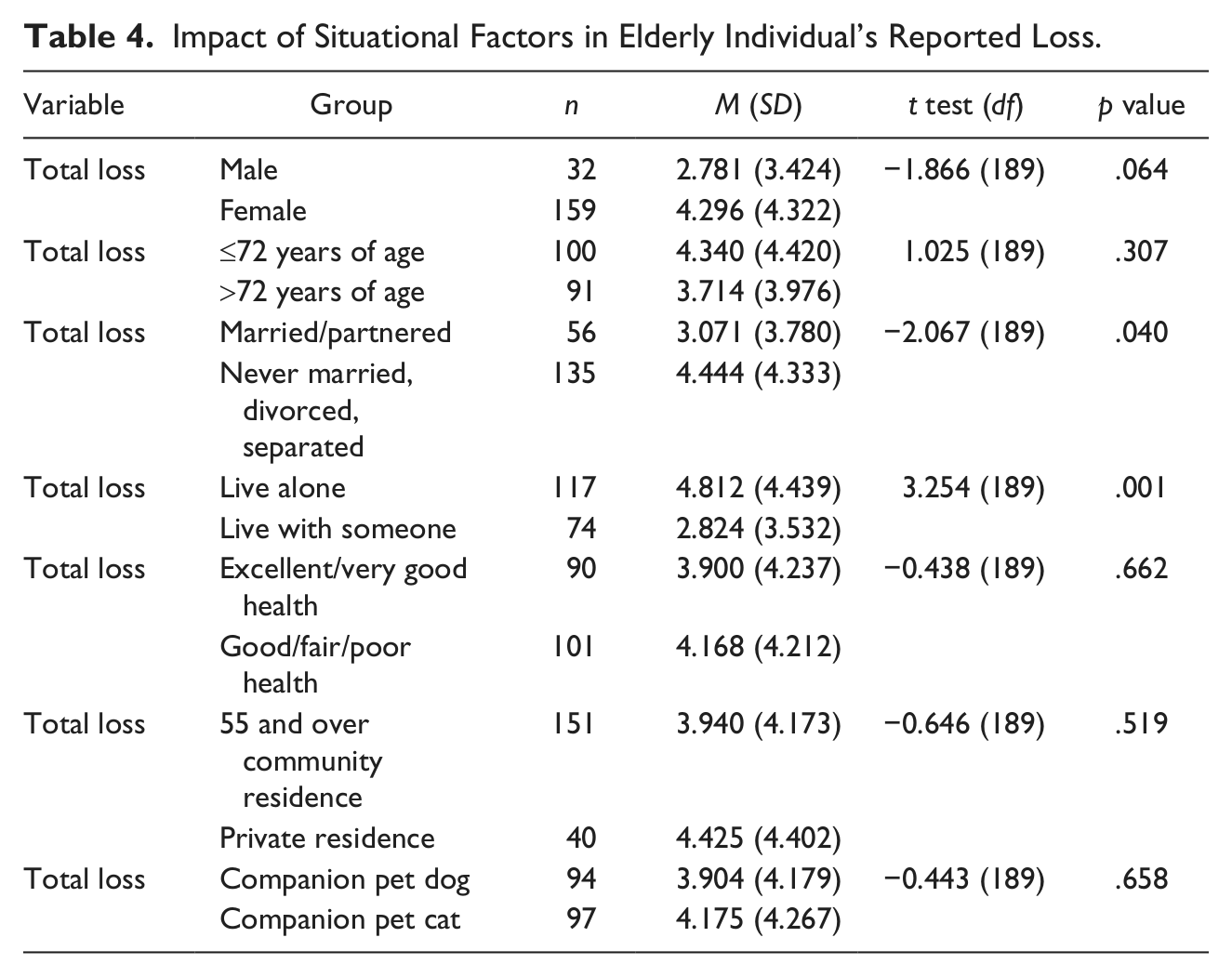
Independent t tests were also conducted to evaluate whether differences occurred between situational factors and loss. The test was statistically significant for greater loss related to marital status, t(189) = − 2.07, p = .040, and living arrangements, t(189) = 3.25, p = .001. No statistically significant differences (all ps > .05) were found for gender, age, health status, housing type, and whether the pet was a dog or a cat as shown in Table 4. A follow-up analysis was conducted with alpha adjusted for six situational factors (p ≤ .008); the test was statistically significant for living alone, t(189) = 3.254, p < .008.
Impact of Situational Factors in Elderly Individual’s Reported Loss.
Correlation coefficients were computed between total loneliness and the situational factors under investigation (see Table 5). The results supported statistically significant relationships among total loneliness and (a) loneliness due to loss (r = .231, p ≤ .01), (b) marital status (r = .193, p ≤ .01), (c) living arrangements (r = −.213, p ≤ .01), (d) health status (r = .167, p ≤ .05), (e) housing type (r = −.195, p ≤ .01), (f) coping (r = −.316, p ≤ .01), and (g) pet attachment (r = .182, p ≤ .05). A follow-up post hoc test using a Bonferroni approach was calculated to minimize Type I error. This was calculated by dividing .05 by the 16 computed correlations, which resulted in a corrected coefficient p value of .003 to declare significance. The post hoc test supported significant correlations between total loneliness and loneliness due to loss (p = .001), living arrangements (p = .003), and coping (p = .000).
Pearson Correlations Between Loneliness and Situational Factors (N = 191).
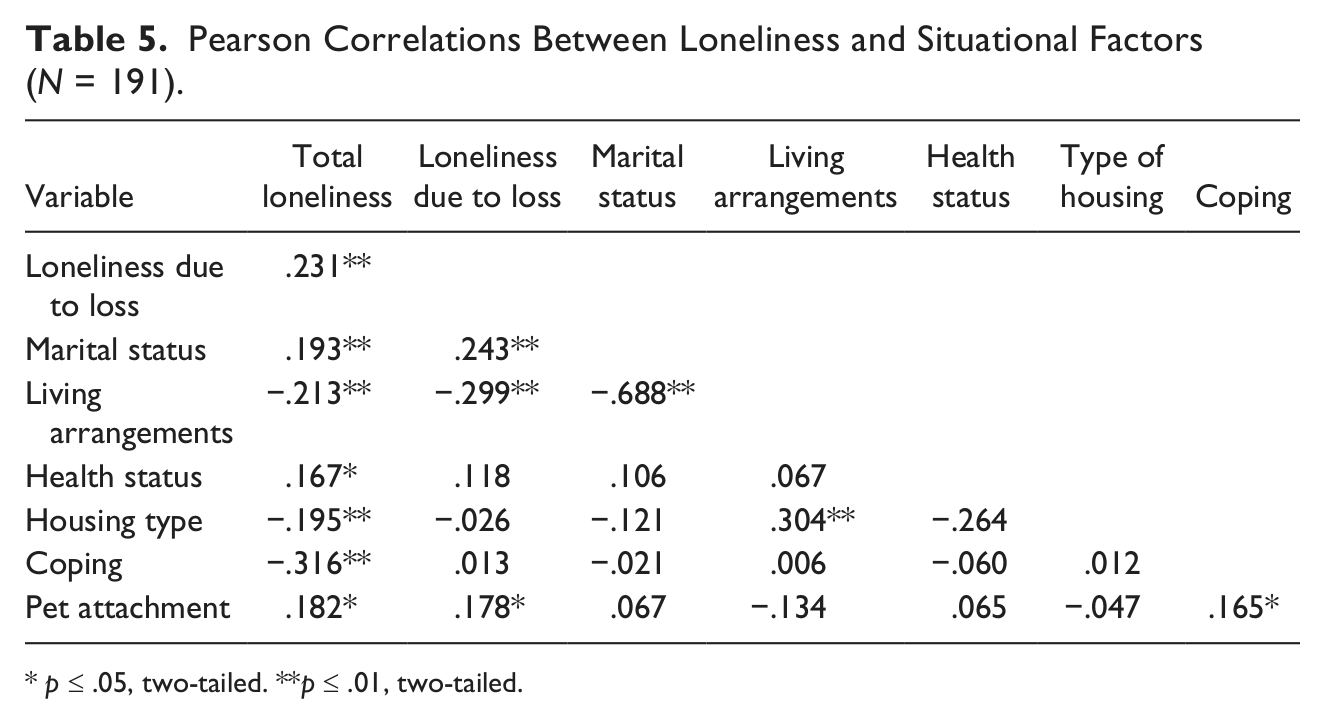
p ≤ .05, two-tailed. **p ≤ .01, two-tailed.
Incremental multiple regression analysis (Tabachnick & Fidell, 2007) was undertaken to determine which specific situational factors explained the most variance in the dependent variable “loneliness,” and whether coping and pet attachment explained additional variance in loneliness. The situational factors that were entered at Step 1 included the variables that demonstrated significant correlations with loneliness as shown in Table 5, with the exception of marital status due to its high correlation with the variable “living arrangement” (r = −.688, p ≤ .01). Coping and pet attachment were entered at Step 2.
The adjusted R2 for the situational variables entered at Step 1 was .095, and at Step 2 with the inclusion of coping and pet attachment, the R2 value increased to .242. Similarly, the F statistic at Step 1 was 6.004 (p = .000), and at Step 2, it increased to 15.496 (p = .000). Situational variables entered at Step 1 that were statistically significant included experienced loneliness due to loss (B = .161, p = .014) and type of housing (B = −.147, p = .044). Situational variables that were not significant included living arrangement and health status. Variables included at Step 2 included experienced loneliness due to loss (B = .161, p = .020), type of housing (B = −.143, p = .036), coping (B = −.341, p = .000), and pet attachment (B = .185, p = .006). Variables not significant at Step 2 included living arrangement and health status.
Discussion
Study findings provide further evidence to support the theoretical framework used in this study whereby feelings of loneliness were greater in participants who experienced a loss compared with those who reported no loss. The findings have implications for nurses working with older adults. Nurses in clinical practice can use the results of this study when developing individual plans of care for their older patients. The plans of care should incorporate and reflect any changes in marital status, living arrangements, and health status. Pet ownership or possibly pet therapy visits should also be explored. Nurses working with older adults should discuss coping mechanism networks used by older adults in the loneliness–loss trajectory.
The role of marital status was found to be a factor in that those who were never married, divorced, or separated had significantly greater loneliness compared with those who were married or partnered. This finding is consistent with prior research on marital status and the effect on social relationships in relation to loneliness in older adults (Leen, 2010). Marriage or partnerships can increase older adults’ social network due to a broader network of friends and family or in contrast may lead to a narrower network (Kalmijn & Broese van Groenou, 2005).
Living arrangements and housing type also played a role whereby considerably greater loneliness was reported for those who lived alone compared with those who lived with someone and those residing in 55 and older community residences. These finding are consistent with work conducted by Yeh and Lo (2004) in that older adults who live alone due in part to smaller social support networks have greater risk for higher loneliness.
Living arrangements also emerged as a significant predictor in loneliness for study participants. Many times, as people age, there are alterations in their living arrangements, whether or not by their own choice. Therefore, it is important for nurses working with the older adult population to include a discussion on current living arrangements and choices or alternative arrangements, if warranted.
Study participants reporting good/fair/poor health compared with those reporting excellent/very good health reported significantly greater loneliness. Research has supported that loneliness has a negative impact on health outcomes in older adults (Cacioppo et al., 2002) and negative health can be an antecedent to loneliness. In addition, age-related increases in blood pressure and poorer sleep quality were found in those who reported greater loneliness. Older individuals may be seen by nurses in a health care facility reporting somatic complaints that may be contributed to loneliness and loss (Ward et al., 2007). As evidenced by this study, there is a relationship between impaired health and loneliness. Consequently, health care practitioners need to be cognizant when older adults are presenting with somatic complaints, as this may be a cue that feelings of loneliness or social isolation may be present.
Study participants who lost friends, pets, neighbors, and coworkers reported significantly greater loss when the loss occurred within 11 months compared with when the loss occurred at 1 or more years from the subject’s participation in the study. No statistically significant differences were found between time period of loss and loss of Spouse, Parent, or Other. These findings may suggest that due to the nature and length of the relationships older adults have with spouses and parents, one can posit that regardless of the length of time that has passed for the loss of significant family members, the feeling of loneliness remains compared with other types of loss where less time, energy, and commitment may have been invested.
The significant predictors of the demographic variables that explained the most variance in loneliness included type of housing and experienced loneliness due to loss. Significant predictors when coping and pet attachment were added with the demographic variables included type of housing, experienced loneliness due to loss, coping, and pet attachment. The results supported that loneliness was lower among study participants who lived in 55 and over residences than private residences, those who experienced loneliness due to loss, those who reported lower coping, and those who reported higher pet attachment.
Moreover, after a corrected significant level was computed, there was a significant relation between coping and loneliness. Coping mechanisms and social support networks are important for older adults in relation to loneliness and can be revealed in many forms.
In this sample of pet-owning older adults, the attachment to their personal pet was significantly related to a decreased feeling of loneliness. This finding supported theory in that an attachment to a personal pet can serve a coping mechanism, source of social support, and a companion (Collis & McNicholas, 1998; Rook, 1990). As recommended in other studies, the benefits of pet relationships should be examined and discussed with the older adult population (Gulick & Krause-Parello, 2012; Krause-Parello 2008, 2012).
In this study, there are potential sources of bias that should be discussed. In regard to the sample, a nonprobability sampling technique was used, namely, a convenience sample.
Data were collected cross-sectionally, and all participants were pet owners. The samples consisting of three participants for a particular group need to be interpreted with caution. The findings of this study need to be reproduced in a larger sample of older adults so that the loneliness–loss pathway can be further assessed.
In conclusion, older adults have a greater risk for loneliness due to situational factors related to loss. Therefore, it is important for nurses to be mindful of these factors when obtaining health histories and information on current health conditions, and it is suggested that questions related to pets and pet ownership should also be included in the conversation. Loneliness can be caused by many factors, and by knowing what factors influence loneliness in older adults, nurses can advocate for appropriate referrals and evidence-based interventions to impede the loneliness–loss pathway such as pet therapy visits if an individual does not own a pet. Nurses need to take an active role in developing a plan of care to assist older adults with their loneliness by including pet therapy visits if they are open to this intervention.
Footnotes
Acknowledgements
Dr. Krause-Parello recognizes co-author and doctoral dissertation committee member Dr. Gulick for her collaboration and support during the development of this manuscript and dissertation process. Dr. Krause-Parello also acknowledges dissertation committee members Drs. Flynn (Chair), Eller, and Guarnaccio and the study participants and their pets.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary study was funded in part by Sigma Theta Tau International, The Honor Society of Nursing, Kean University’s Chapter, Lambda Iota.