
Abstract
Effective handoff communication is critical for patient safety. Research is needed to understand how information processes occurring intra-shift impact handoff effectiveness. The purpose of this qualitative study was to examine medical-surgical nurses’ (n = 21) perspectives about processes that promote and hinder patient safety intra-shift and during handoff. Results indicated that offgoing nurses’ ability to grasp the story intra-shift was essential to convey the full picture during handoff. When oncoming nurses understood the picture being conveyed at the handoff, nurses jointly painted a full picture. Arriving and leaving the handoff with this level of information promoted patient safety. However, intra-shift disruptions often impeded nurses in their processes to grasp the story thus posing risks to patient safety. Improvement efforts need to target the different processes involved in grasping the story and painting a full picture. Future research needs to examine handoff practices and outcomes on units with good and poor practice environments.
Inter-shift handoff is defined as the exchange of information, responsibility, and accountability between nurses about patients at shift change (Australian Commission on Safety and Quality in Health Care, 2010; Cohen & Hilligoss, 2010). Nurses’ handoffs are situated within a 24-hr cycle of clinical care in which the nursing, medical, and technical knowledge relevant to each patient needs to be transferred seamlessly between offgoing and oncoming nurses as they work to maintain safety. Quality handoff information enables nurses to recognize quickly changes in patient status and to anticipate risks (Patterson, Roth, Woods, Chow, & Gomes, 2004), thereby promoting safe care. By safety, we mean preventing errors and reducing risks by coordinating multiple aspects of patient care, identifying and intercepting hazards, monitoring, surveillance, and detecting when patient status deteriorates (Mitchell, 2008). Thus, handoff information must be accurate, complete, relevant, and timely (Australian Commission on Safety and Quality in Health Care, 2010; Staggers, Clark, Blaz, & Kapsandoy, 2011).
Handoff Communication and Patient Safety
Handoff methods vary and include written, tape-recorded, and oral face-to-face at or away from the patient’s bedside (Carroll, Williams, & Gallivan, 2012; Kerr, Lu, McKinlay, & Fuller, 2011; O’Connell & Penney, 2001; Randell, Wilson, & Woodward, 2011; Staggers & Blaz, 2013; Street et al., 2011; Strople & Ottani, 2006). Although nurses perceived improvements in patient safety after changing to bedside handoff (Chaboyer, McMurray, & Wallis, 2010; Sherman, Sand-Jecklin, & Johnson, 2013), overall data are inconsistent regarding the comparative strengths and limitations of different handoff methods in maintaining patient safety (O’Connell, Macdonald, & Kelly, 2008; Sherman et al., 2013; Staggers & Blaz, 2013).
Handoffs pose risks to patient safety because handoff communication is challenged by time constraints, interruptions, noise, and interpersonal tensions (Carroll et al., 2012; Kerr et al., 2011; Meissner et al., 2007; O’Connell et al., 2008; Randell et al., 2011; Staggers & Jennings, 2009; Welsh, Flanagan, & Ebright, 2010). Furthermore, handoff information is frequently inaccurate, incomplete, biased, or misunderstood (Dowding, 2001; Flemming & Hubner, 2013; Holly & Poletick, 2014; O’Connell et al., 2008; Pezzolesi et al., 2010; Rabol et al., 2011; Riesenberg, Leisch, & Cunningham, 2010; Sexton et al., 2004; Staggers & Blaz, 2013; Strople & Ottani, 2006; Welsh et al., 2010). To address information deficiencies, researchers have focused on standardizing the content of handoff information with support from written or computerized tools (Collins, Stein, Vawdrey, Stetson, & Bakken, 2011; Flemming & Hubner, 2013; Holly & Poletick, 2014; Patterson & Wears, 2010; Staggers et al., 2011; Strople & Ottani, 2006). Although research findings suggest improvement in handoff information after implementing standardization (Johnson, Jefferies, & Nicholls, 2012; Pothier, Monteiro, Mooktiar, & Shaw, 2005), the overall evidence linking improvement strategies with patient safety remains weak (Abraham, Kannampallil, & Patel, 2014; Cohen & Hilligoss, 2010; Patterson & Wears, 2010; Riesenberg et al., 2010; Riesenberg, Leitzsch, & Little, 2009; Staggers & Blaz, 2013).
To date, nursing research has focused on the handoff itself with little attention to the larger context of the practice environment (Abraham, Kannampallil, & Patel, 2012; Flemming & Hubner, 2013). Yet nurses work in challenging practice environments that can tax their ability to think critically and evaluate patient care (Ebright, Patterson, Chalko, & Render, 2003). Understanding the work of nursing in relation to handoff communication is essential for sustained process improvement. The aim of this study was to identify the processes that promote and hinder patient safety intra-shift and during the handoff by examining the perspectives of nurses who routinely participate in handoffs.
Methods
We used constructivist grounded theory methodology to explore nurses’ perspectives about handoff processes (Charmaz, 2006; Clarke, 2005; Glaser & Strauss, 1967). This method allows for the examination of actions and interactions intra-shift and during the handoff; nurses’ perspectives about what works well; and identification of situations that create risks to patient safety.
Data Collection and Procedures
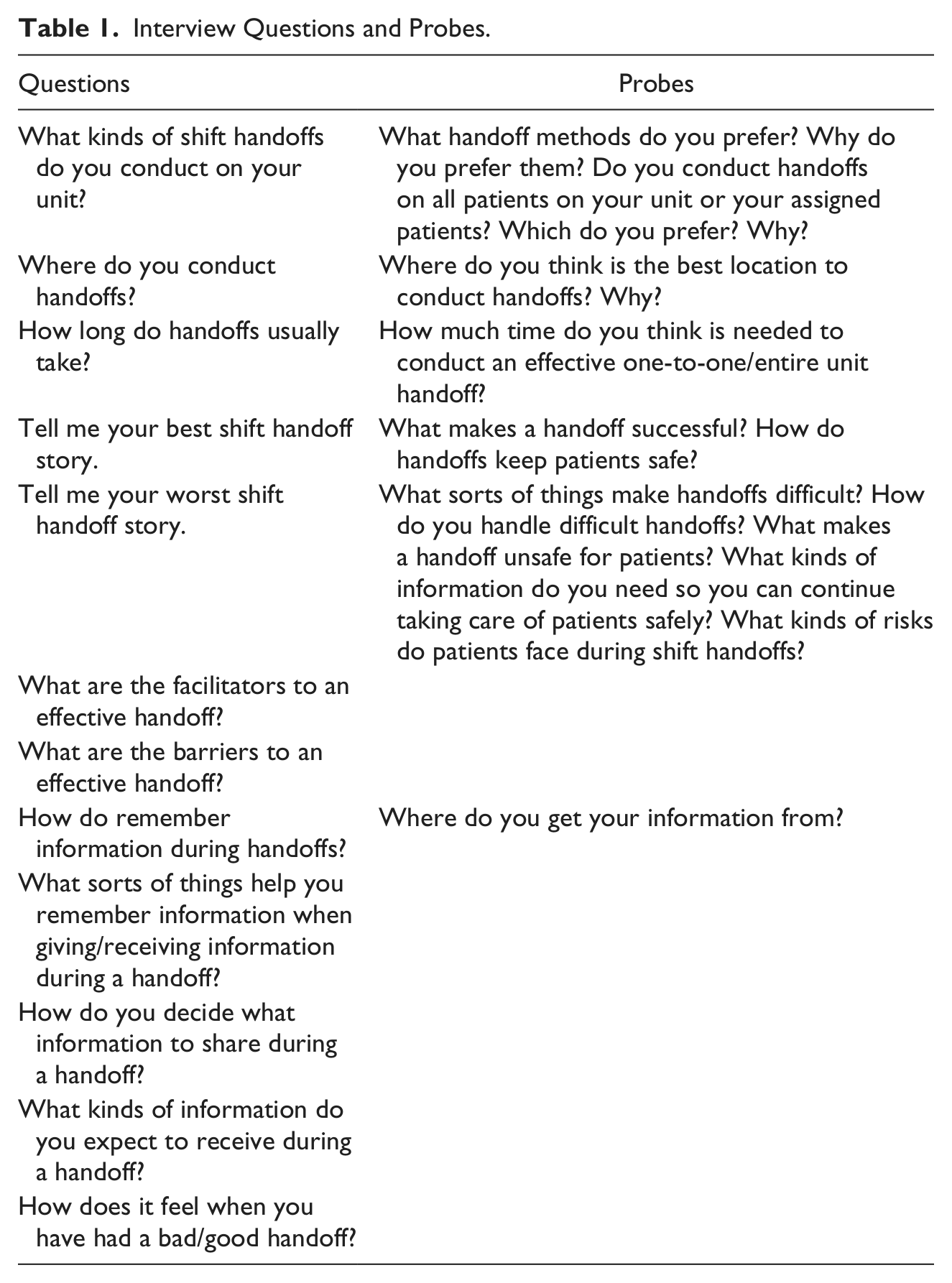
Ethical approval was obtained from the sponsoring university and the participating institution. Individual semi-structured interviews and ethnographic observations of handoffs were collected between November 2010 and December 2011. A purposive sample of 21 nurses participated in interviews. Registered nurses (RNs) and licensed vocation nurses (LVNs) who conducted handoffs were eligible to participate in interviews. Nurses who did not conduct handoffs on either unit were excluded from the study. Eighteen nurses were interviewed once; 3 nurses were interviewed twice as part of grounded theory methods; and the total was 24 interviews. Interviews lasting 45 to 60 min were recorded using a flexible investigator-created guide that was adaptable to responses and emerging themes (Table 1). Basic demographic information was collected at the end of the interview.
Interview Questions and Probes.
Using a researcher-developed checklist, the primary investigator observed 87 unique patient handoffs during 20 inter-shift reports. The primary investigator’s data collection included handoff time, methods, location, noise, interruptions, and interpersonal interactions. Field notes were taken and transcribed as soon as possible thereafter (Hammersley & Atkinson, 2007). Handoff observations captured how nurses actually interact during handoffs. Observations were conducted across all shifts on two medical surgical units. Verbal consent was obtained before observing handoffs. According to grounded theory methodology, rigor was maintained through reflexivity, peer review, analytic triangulation, and respondent validation (Angen, 2000; Charmaz, 2006; Clarke, 2005).
Setting and Participants
The setting was a 124-bed, university-affiliated urban government hospital in the Western United States. The hospital had a well-established computerized patient record system including bar coding medication administration technology. Nurses used computers on wheels to access patient records and scan medications. Staff on the 36-bed surgical unit comprised 37 RNs, 3 LVNs, 14 nursing assistants (NAs), and 5 unit clerks. Staff on the 20-bed medical unit comprised 22 RNs, 3 LVNs, 8 NAs, and 3 clerks. Staff cared for 3 or 4 patients according to hospital acuity policy; no handoff method was mandated, and staff had union representation. The average age of study participants was 39 (range = 24 years to 66 years). The average number of years of nursing experience was 12 (range = 9 months to 43 years). Interviewee characteristics are summarized in Table 2.
Characteristics of Study Participants.
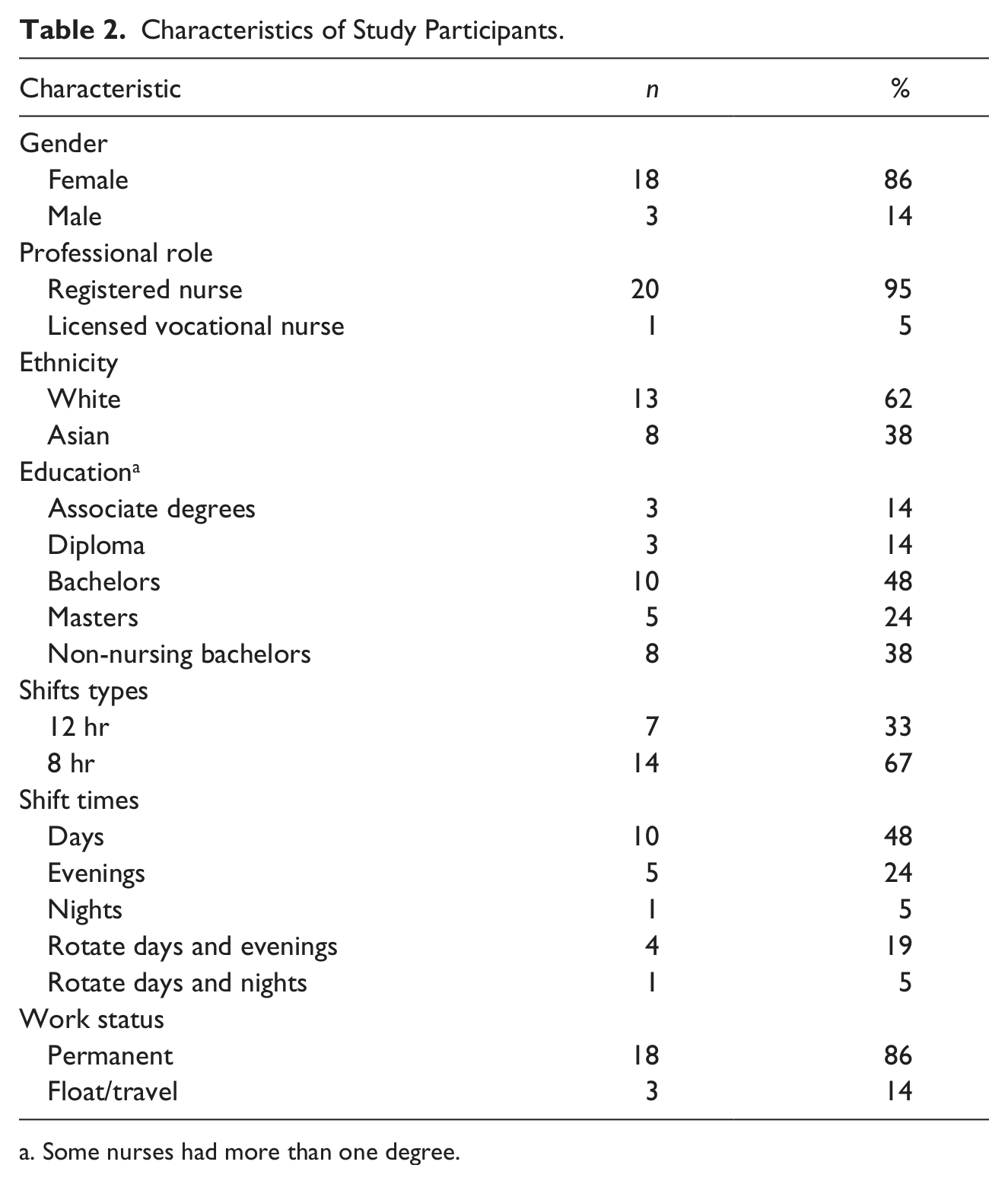
Some nurses had more than one degree.
Analysis
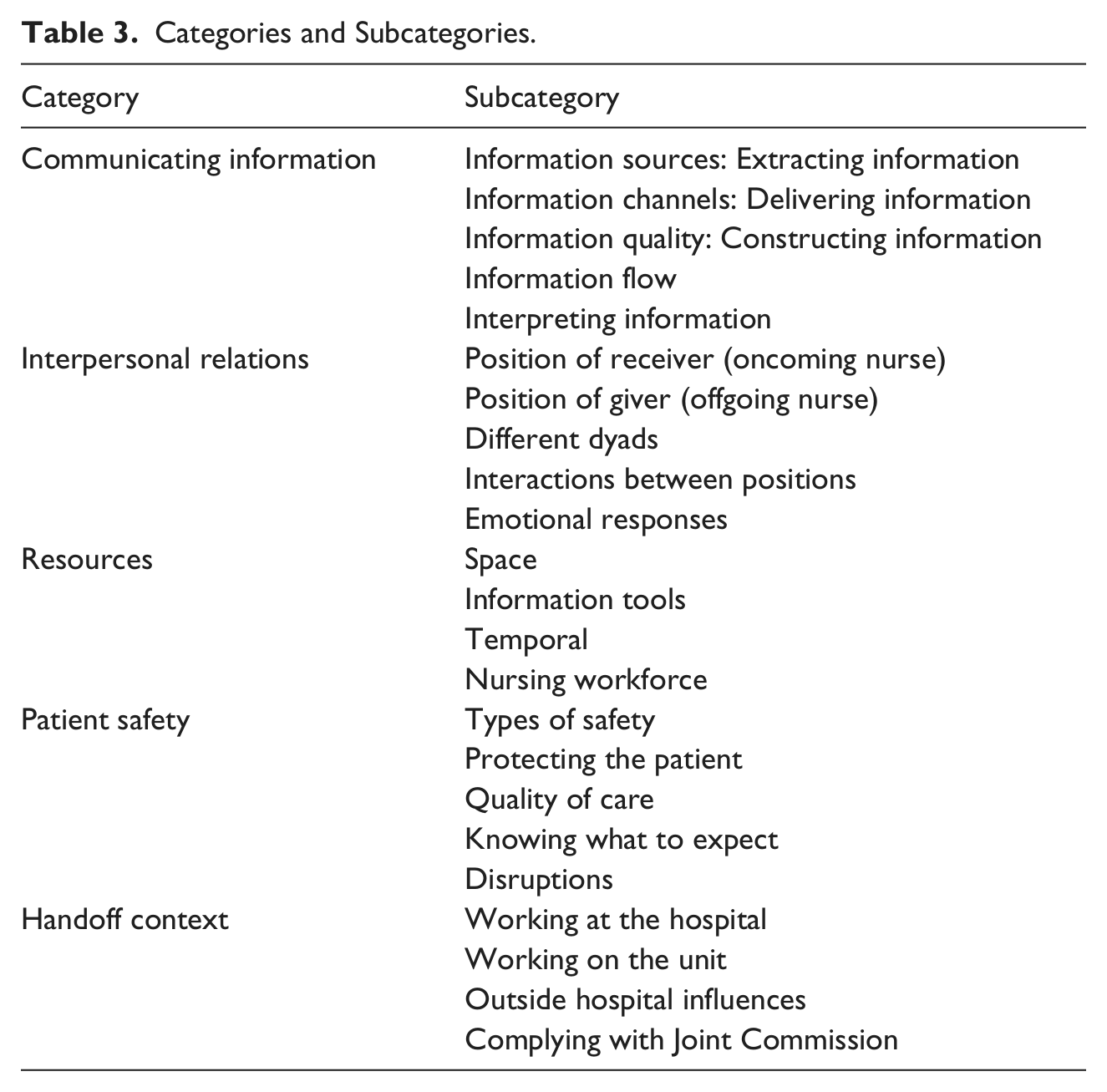
Data collection and analysis were conducted simultaneously using constant comparison (Clarke, 2005; Glaser & Strauss, 1967) and open, focused, and theoretical coding (Charmaz, 2006; Strauss, 1987). Open coding facilitated category development, focused coding specified the salient codes for categorizing the data, and theoretical coding determined the relationships between categories (Charmaz, 2006; Strauss, 1987). The categories and sub-categories are summarized in Table 3.
Categories and Subcategories.
Memo writing and diagramming aided a conceptual framework and analysis of relationships between categories (Charmaz, 2006). The numbers of observations and interviews were guided by theoretical sampling; this means that the ongoing analysis directed data collection to develop concepts, categories, and conceptual relationships (Charmaz, 2006; Clarke, 2005). Theoretical saturation was reached when relationships between categories were sufficiently developed and differentiated (Charmaz, 2006).
Results
Nurses on both units described two important patient safety promoting processes: grasping the story in the practice environment (intra-shift) and painting a full picture during the handoff exchange (Figure 1). However, nurses reported that disruptions in the practice environment and during the handoff often hindered them in grasping the story and jointly painting a full picture thus posing risks to safe continuity of care.
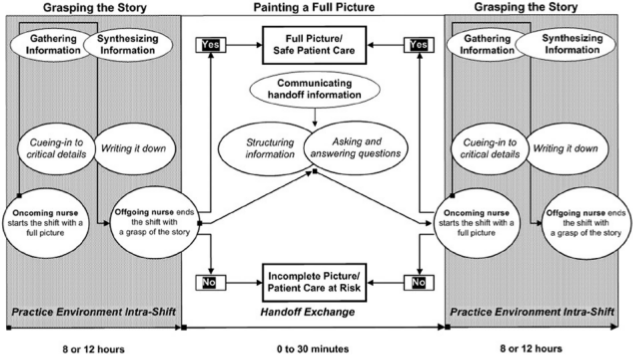
Conceptual model of handoff processes promoting patient safety.
Grasping the Story in the Practice Environment (Intra-Shift)
Context: The practice environment
Nurses worked 12- or 8-hr shifts and typically cared for four or more complex patients per shift. However, nurses (particularly those who worked day and evening shifts) might discharge two patients and receive two new admissions during the shift potentially caring for six or seven patients. Computers on wheels were located in hallways, nurses’ stations, and patient rooms. Nurses reported that the computers were heavy to push and often ceased functioning. Logging into computers was time-consuming because separate passwords were required to log into the computer and then access the patient record.
Throughout the shift, nurses were responsible for checking and acting upon physicians’ orders, administering medications, wound care, orchestrating admissions, discharges and transfers, and documentation. Administering medication (including scanning up to as many as 20 medications per patient) and orchestrating patient flow were two time-consuming workflow processes requiring nursing, medical, and technical knowledge. “It’s always prioritizing and a lot of juggling in your mind, trying to figure out what is important for your time to do right now.” (MA03#2) In this pressured practice environment, nurses had to manage large amounts of complex information.
Grasping the story: A safety-promoting process
Grasping the story involved multiple time lines and levels of information depth. First, after receiving handoff report, the oncoming nurse began the shift. Second, during the shift, the nurse cared for patients over the course of 8 to 12 hr. During the shift, the nurse gathered and synthesized information from the previous handoff, consolidated that information with their ongoing assessments and patient records, cued-in to critical details, and recorded information. Third, at the end of the shift and before the next handoff, the nurse moved into the offgoing position ready to give handoff report to the next nurse. Being prepared at the end of the shift with a good grasp promoted patient safety because the offgoing nurse had sufficient knowledge of the patient to transmit to the next nurse. This knowledge included information that helped the next nurse reduce risks to patients as the nurse was better prepared to coordinate patient care, prevent errors, and detect and intervene if a patient’s status deteriorated.
Facilitating processes in grasping the story
To grasp the story intra-shift, nurses gathered and synthesized information, continuously updating their knowledge of the patient. To facilitate nurses’ grasp of the story, nurses emphasized how important it was to receive complete information from the previous handoff and then: see a patient and make that connection with the patient and [handoff] information . . . it’s all kind of vague till I get out there . . . and . . . do quick assessments . . . then . . . [I can] start plugging [information] in and having it make sense . . . then it becomes a person’s condition. (MA02)
Cueing-in to critical details
The patient-specific details that nurses received from the prior handoff and during their assessments enabled them to cue-in more effectively to signs and symptoms of deterioration. For example, an out-of-range vital sign. I will jot that down and make a mental note to myself to make sure that this is under control . . . and depending on the patient diagnosis if they have pneumonia and they were having crackles . . . I will jot down crackles, mental note to . . . assess this area once again. (MA12)
Another nurse described being cued-in by a detail in handoff that a particular patient was at risk of falling when he became agitated. Receiving this detail helped an oncoming nurse monitor the patient more closely. As nurses cued-in to critical details, they were also synthesizing information. After hearing a pertinent detail in the handoff report, an experienced oncology nurse was cued-in to assess a patient’s abdomen. This patient had not had a bowel movement in three days. This detail alerted the nurse to a potential problem because she knew this was a change for this particular patient requiring prompt assessment: I went in and his abdomen was . . . distended and this guy had a prostate cancer history . . . red flags went off in my head . . . I immediately notified the doctor. . . . And sure enough he [had] a mass . . . he’s got metastatic disease . . . he could have perforated. (MA02)
Writing it down
As nurses gathered and synthesized information about a patient’s history, current status, pertinent details, interventions, and plan of care, they needed mechanisms for tracking and organizing information gleaned from the handoff and their assessments of each patient. Because nurses had multiple patients, they reiterated that “writing it down” was essential to grasp the story during the shift; written notes to themselves to their own structured method helped them remember large amounts of information, stay organized, and prepare them for the end-of-shift handoff: So if anything significant comes up [in an] assessment, I immediately put it down, it’s ingrained that anything happens I write it down . . . I systematically write . . . for each patient so I’m creating my own . . . written standard report. (SB06)
Hindering processes in grasping the story
Intra-shift disruptions could impede nurses’ collection, management, and synthesis of information. For example, when new patients arrived on the unit minutes before the next shift change, nurses were challenged to complete their grasp of the story with full assessments before the handoff. Under these circumstances, “the offgoing nurse doesn’t have an idea of what’s going on. They haven’t assessed the patient.” (SB17) Staff shortages and nurses temporarily floating off the unit often hindered nurses’ ability to complete assessments and cue-in to critical changes.
Furthermore, nurses often experienced delays in accessing information due to computer malfunctions: “One day, I went through five computers. They’ll shut down on you . . . you’re waiting 15-20 minutes. And . . . then it crashes.” (SB20) Accessing physicians’ orders was cumbersome and required nurses to check for new or changed orders every 2 hr. Moreover, evaluating order accuracy was difficult: You can see all these orders from different units and different dates . . . many years ago . . . everything is mixed up . . . bits of information that you have to evaluate . . . to even see if they are supposed to get aspirin today . . . it’s a huge deal. (SB13)
Without the needed time, focus, and attention to assess and identify critical changes in patient status, a nurse described arriving at the inter-shift handoff: not really have a good grasp on what was going on with my patients, and so I know that my report has been vague, not thorough, because I wasn’t sure of all the things that I was reporting about . . . maybe [I was] swamped that shift . . . I wasn’t . . . able to find out the answers to the questions that I wanted. (SB08)
Painting a Full Picture During the Handoff
Context: Handoff exchange
Handoffs occurred fours times in 24 hr (7:30 a.m., 3:30 p.m., 7:30 p.m., and midnight). Thirty minutes were allocated for handoff, but the midnight shift had no allocated handoff time. Charge nurses from the previous shift were responsible for completing nurse−patient assignments for oncoming nurses. Offgoing nurses each reported to as many as three or four oncoming nurses who would be assuming responsibility for their patients.
Generally, nurses conducted oral handoffs away from the bedside. Handoffs were usually conducted at the nurses’ station on the surgical unit and in the nurses’ lounge on the medical unit. Taped recorded handoff occurred during staff meetings, midnight handoffs, and when nurses were late to the handoff. Bedside handoff seldom occurred. From observations of handoffs, the nurses’ lounge was the noisiest location with as many as 15 nurses crowded into one room for report. Of all locations, the nurses’ station had the most interruptions.
Painting a full picture: A safety-promoting process
The processes involved in painting a full picture during the handoff differed from the processes of grasping the story in the practice environment (intra-shift). Painting a full picture involved the offgoing and the oncoming nurses interacting together during a brief handoff. This interaction usually occurred without patient involvement. When offgoing nurses acquired a good grasp of the story before the handoff, they were in a stronger position to paint a full picture during the handoff because they had comprehensive knowledge about a patient that included history, current status, critical details, interventions, follow-up, and plan of care. Consequently, the oncoming nurse had a better chance of beginning to see the full picture. Jointly painting a full picture promoted patient safety because nurses began the next shift with sufficient information to detect changes in a patient’s status and intervene to reduce possible risks such as: This patient is getting a lot of IV fluids, but I’m concerned because he’s got a really bad history of CHF so . . . watch out for this . . . anticipate . . . he may start sounding wet. (SB17)
Facilitating processes in painting a full picture
To successfully paint a full picture together, many nurses needed oral face-to face communication away from the bedside in a quiet interruption-free location; these conditions facilitated focusing attention and asking and answering questions. Some nurses preferred communicating at the bedside feeling improved patient trust and nurse-to-nurse accountability; others were concerned about privacy and frankness about pertinent details in patients’ presence.
When nurses cared for the same patients and shared care with the same nurse over several days, they identified patient and nurse continuity as contextual facilitators of handoff quality and patient safety. Cueing-in to critical information in the practice environment was easier when nurses already knew the patients they were receiving. When nurses shared care with the same nurse, handoff information was more focused on the key patient priorities because pertinent medical history was already known to both nurses.
To support painting a full picture, some nurses used the computerized patient record at handoff to verify information. On one unit, a nurse stated that the computerized record was now required because of a past serious medication error that had occurred when an offgoing nurse missed a new physician order right before shift change. However, few nurses were observed using computers during handoffs. Some resisted using the computer feeling this was a way of “checking up” on nurses, others said that the computer was too bulky or time-consuming to use.
Structuring handoff information
To facilitate communication during handoff, most nurses used some type of written format. Offgoing nurses read from their written format. As oncoming nurses listened to report, they wrote pertinent information on their written formats. Some nurses individualized their forms for writing their notes and others created more elaborate checklists. Nurses described these written formats as “SBAR” (situation, background, assessment, recommendation) or a “systems” checklist that included seven to nine systems such as neurological, respiratory, and cardiovascular.
Some nurses independently worked together to design a checklist to improve the handoff. When they were in a handoff together, they found that the use of the same checklist helped them better paint the full picture. Information was thorough, accurate, organized, and less biased. The checklist prompted the offgoing nurse to include the patient’s history, current status, and safety details such as fall risk, code status, and plan of care. The oncoming nurse could quickly identify information gaps and the offgoing nurse felt triggered to remember key information.
When nurses were asked what kinds of information they needed to paint the full picture, many responded, “it depends.” Some nurses wanted complete details that covered all the “systems” including the history and plan of care, others needed just the pertinent details or important changes, and others said that it depended on how well they knew the patient. Asking and answering questions were essential information gathering practices that supported nurses in painting a full picture.
Skillfully asking and answering questions
For oncoming nurses, clarifying information by asking questions was important. Offgoing nurses often appreciated being asked questions that prompted them to remember details. However, asking and answering questions required skill about when to interject without disrupting the offgoing nurse’s mental flow or making the reporting nurse defensive: I find a little break in their report where I can jump in . . . I just feel it out . . . if they’re relaxed or stressed and then I either jump or I wait even though I really want to know that information before the end. But it requires a lot more sensitivity at change of shift . . . because they’re stressed; they’ve been here for 8 hours or 12 hours. (SB13)
Likewise, answering questions required the skill of being open to the meaning of questions. Being asked questions often prompted the offgoing nurse to recognize their unclear information. Many offgoing nurses closed their report with, “Do you have any questions?”
Central to the success of asking and answering questions was mutual respect and trust. Nurses stated that when nurses respected and trusted each other, they were more likely to engage in interactive dialogues about patients and share their unique knowledge about patients and thus support each other in solving complex patient problems.
Furthermore, nurses stated that it was the process of asking and answering questions that helped them the most in learning how to conduct a good handoff. Nurses could reveal critical details not found in formal patient records or taped reports. Consequently, nurses “painted a full picture of the patient” together, resulting in the oncoming nurse’s optimal preparation: [When we] can actually talk about the [patient] and even though [we are] not in the patient’s room [we can] visualize . . . this person . . . because I really know this person . . . it helps the next nurse know [the patient] . . . that definitely improves care. (SB13)
Hindering processes in painting a full picture
Nurses considered handoff time “sacred” but time was frequently compromised. Handoffs could be delayed when oncoming nurses arrived late to work and/or offgoing nurses were detained in patient care responsibilities. Handoffs could end late because of meetings and educational trainings. Nurses felt pressured because either offgoing nurses wanted to leave or complete their charting or oncoming nurses were anxious about starting their shift at a time when they needed to synthesize the meaning of complex patient information: So you’ve got to be quick about it . . . thorough . . . hit the high points. It’s all about speed . . . hurry, hurry, hurry . . . give a quick, efficient report and allow time for questions . . . hurry, hurry, fast, fast, run, run. (SB20)
Meetings were frequently scheduled during handoff time. Also no time was allocated for midnight handoff. Reports for these situations were tape-recorded thereby hindering nurses jointly painting a full picture together. Taped report precluded asking and answering questions and weakened accountability. Furthermore, entire reports about patients could be missing. Although discussions were underway to allocate time to the midnight handoff, no changes had occurred.
Nurses reported that there was no mandated written or computerized format. Many nurses used the hospital’s pre-printed computerized “end of shift report” to write their notes, but this format was limited to basic demographic information, chief complaint, and vital signs. Without an agreed-upon standardized format, information was often incomplete.
Although nurses inhabited both the offgoing and oncoming positions, a nurse’s perspective about the nurse in the opposite position often depended upon their individual experiences (e.g., past interactions, personal perceptions) with the particular nurse. When nurses distrusted the other nurse, lacked communication skills, or failed to recognize the challenges faced by the nurse in the other position, tensions could arise. Nurses felt that their ability to ask and answer questions was blocked.
Nurses could interpret asking and answering questions negatively. Questions could be delivered in a manner that was disrespectful, intimidating, or humiliating: With certain nurses there’ll be a lot more of, well did you do this? did you do that? It’s less I’m giving report to you and more like I’m checking on what you did. The question is well, did you really know the patient and . . . trying to figure out if you messed up on something. It’s not just a question, it’s a loaded question. (SB18)
Other nurses said they caught themselves engaging in a probing style of questioning when they had mistrusted the offgoing nurse. This occurred when they had previously been assigned patients that they felt had received poor quality care and subsequently obtained handoff from the same nurse. In this kind of situation they perceived both their patients and themselves at risk. “Part of the anxiety of taking over someone else’s shift is not knowing what they didn’t do, forgot to do, that is going to end up in your lap unexpectedly.” (SBMA09)
Offgoing nurses may resort to defending themselves and felt that important information could get lost when they felt flustered or unable to think. Thus, they hastened the process to end report quickly. Oncoming nurses sometimes sensed defensive reactions to their questions and disengaged when this happened. Tape-recording handoffs was a common strategy for avoiding specific nurses. Others tried to correct themselves and said, To be brutally honest . . . my frustration comes out before I can catch it . . . Can you tell me this? Can you tell me that? . . . I show it in my tone that I am getting frustrated and impatient. Sometimes I can tell that they are starting to get defensive, so I am like, oh am I sounding frustrated? Oops ok so I tone it down. (SB08)
Nurses’ openness to feedback about the quality of handoff information was often complicated. Every participant stated they valued direct and honest feedback. In contrast, when asked how they gave feedback to other nurses, most participants admitted that they just asked more questions rather than telling the nurse directly that the information was inadequate. Thus, asking questions could become an indirect way to give negative feedback and contributed to the tension that questioning could engender.
Leaving the handoff with an incomplete picture often delayed oncoming nurses because they lacked the necessary information needed for safe care: I’m looking after people that I don’t really know enough about . . . [digging through the record] takes me off the floor for longer, which I don’t think is good for patient’s safety . . . you’re behind already . . . your attention is taken with other things, when it should have been patients. So it just makes me feeling really ill equipped to do my job well. (SB08)
Discussion
Results indicate that information gathering and synthesizing processes occurring intra-shift impact the effectiveness of handoff information. Nurses emphasized that without a grasp of the story by the end of their shift, their ability to jointly paint a full picture at handoff was jeopardized; that is, the offgoing nurse lacked the necessary complete information. Disruptions in the practice environment often impeded nurses in their quest to grasp the story.
These results extend prior research. Indeed, other scholars have supported the concepts of grasping the story including cueing-in to critical details as important factors in promoting patient safety. Benner and colleagues describe a nurse’s clinical grasp as a skill and means that a nurse has a solid clinical understanding of patients’ status (Benner, Hooper-Kyriakidis, & Stannard, 1999; Benner, Hughes, & Sutphen, 2008). Having such a grasp directs a nurse to assess, plan, and intervene. Clinical grasp promotes forethought, so that nurses can anticipate patient risks, recognize and detect unexpected changes, and take necessary action (Benner et al., 1999, 2008). Weick (1995) describes extracted cues as “the seeds from which people develop a larger sense of what may be occurring” (p. 50). When nurses possessed this level of information, they were in a stronger position to prevent errors, reduce patient risks, detect when patients were deteriorating, and identify and intercept hazards.
Maintaining patient safety intra-shift and during handoff requires individual and collective responsibility (Collins et al., 2011; Flemming & Hubner, 2013; Rasmussen, 2003; Reason, 1990; Weick, 1995; Weick & Sutcliffe, 2007). The processes we observed in this study illustrate the intersection of multiple levels of responsibility, as individual, organizational, and dyadic dynamics can support or challenge safety. Planning and executing safe patient care take time, including time to think. Nurses often struggled with organizational pressures in balancing efficiency-thoroughness trade-offs, potentially posing risks to patient care (Hollnagel, 2004).
Our results have several implications for nursing practice. Leaders need to value nursing knowledge by supporting improvements in the practice environment, which is relatively inexpensive (Aiken et al., 2011). Nurse managers could shadow nurses during their work and engage staff nurses in identifying problems in the practice environment. A good practice environment includes positive working relations, open dialogue between staff, adequate staffing resources, sufficient time to spend with patients, and continued learning for nurses and quality improvement for patient care (Aiken et al., 2011; Kutney-Lee, Lake, & Aiken, 2009).
Findings from our study suggest that the handoff exchange may be improved by decreasing distractions and noise, providing dedicated handoff time, minimizing concomitant meetings, and providing a structured but flexible written tool. Other researchers have found and argued for similar improvements (Abraham et al., 2014; Collins et al., 2011; Flemming & Hubner, 2013; Holly & Poletick, 2014; Johnson et al., 2012; Kerr et al., 2011; Matney, Maddox, & Staggers, 2014; Meissner et al., 2007; O’Connell et al., 2008; Randell et al., 2011; Riesenberg et al., 2009; Staggers et al., 2011; Staggers, Clark, Blaz, & Kapsandoy, 2012; Staggers & Jennings, 2009; Strople & Ottani, 2006; Welsh et al., 2010). Nurses began to develop a standardized tool during the study. Nurses would benefit from educational interventions such as giving and receiving feedback, conflict management, and hospital programs about the impact of individual behaviors on patient safety (Budin, Brewer, Chao, & Kovner, 2013).
Future research needs to consider improvement interventions that target the different processes involved in grasping the story intra-shift and painting a full picture at handoff. Comparing patient outcomes from handoffs conducted on units with good and poor practice environments is needed. Research is needed to examine handoffs and outcome measures.
Study limitations included a small sample size in one institution. Non-participants may have different perspectives. The differences in handoff report content between RNs and LVNs were not explored. We did not have data for establishing an empirical link to outcomes. Establishing such causality remains a central challenge for the field. The study strengths included 87 handoff observations and 24 in-depth nurse interviews. In sum, this study contributes to understanding the complexity of handoffs in the actual practice setting.
The handoff is clearly situated within a more complex practice environment. If processes within the practice environment fail to support the value of nursing knowledge, the handoff itself will reflect such disparity and patients are potentially at risk. Investing in good practice and handoff environments benefits both patients and nurses. In optimal environments, nurses are more likely to have and utilize resources that support their promotion of patient safety.
Footnotes
Acknowledgements
The authors thank the nurses for their support of this study and Adele Clarke, PhD, for invaluable comments on previous drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary investigator received funding for a research award from the Alpha Eta Chapter, Sigma Theta Tau International. This material is a result of work supported by resources from the Department of Veterans Affairs (VA) Medical Center San Francisco. No funding from VA was received for this project. The fourth author received support from the National Centre for Advancing Translational Sciences, National Institutes of Health (NIH), through UCSF-CTSI Grant KL2TR000143. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the VA or NIH.