
Abstract
This comparative and correlational study examined personal and social-cognitive factors related to physical activity in middle-aged women with (n = 37) and without (n = 67) type 2 diabetes (T2D). Compared with those without the condition, women with T2D attained less accelerometer-measured moderate, t = −3.35(89.40), p = .001, and vigorous physical activity, t = −2.76(59.30), p = .008, and moderate-to-vigorous physical activity (MVPA), t = −3.50(91.19), p = .001, and had lower physical activity self-efficacy, t = −2.6(101), p = .01, and perceived benefits of physical activity, t = −2.4(51.0), p = .02. For the total sample, greater MVPA was related to White race, not having diabetes, lower body mass index, fewer comorbidities, less depressive symptom severity, no smoking status, more positive attitudes, higher self-efficacy, and greater perceived benefits. Enhancing attitudes, self-efficacy, and benefits may increase MVPA in middle-aged women with T2D.
Women during middle age are at increased risk of developing diabetes and associated cardiovascular disease (CVD; Centers for Disease Control and Prevention [CDC], 2011; Towfighi, Saver, Engelhardt, & Ovbiagele, 2007). One lifestyle behavior reported to reduce the risk of developing type 2 diabetes (T2D) and related CVD complications is physical activity (Delahanty & Nathan, 2008; Mosca et al., 2011; Oguma & Shinoda-Tagawa, 2004). For women to achieve health-related benefits, the U.S. Department of Health and Human Services (USDHHS; 2008) and the American Heart Association (Mosca et al., 2011) recommend at least 150 min per week of moderate-intensity physical activity or at least 75 min per week of vigorous-intensity physical activity or a comparable combination of moderate- to vigorous-intensity physical activity (MVPA) 3 or more days per week. Despite this recommendation, the majority of women lack sufficient participation in and are unable to maintain physical activity, and those with diabetes report being less active than those without the condition (Poomsrikaew, Berger, Kim, & Zerwic, 2012; Wilbur, Chandler, & Miller, 2003).
Due to the lack of participation by middle-aged women, interventions to increase physical activity are strongly recommended to prevent or manage diabetes and reduce the risk of associated CVD. To design effective interventions to increase physical activity, a thorough awareness of the factors that influence this behavior among middle-aged women is imperative. The Social-Cognitive Theory (SCT; Bandura, 1977) and Theory of Planned Behavior (TPB; Ajzen, 1991) identify certain personal and social-cognitive factors as being associated with physical activity. Data from several empirical studies involving middle-aged women (Ayotte, Margrett, & Hicks-Patrick, 2010) and adults with diabetes (Allen, 2004) support the proposed theoretical relationships, and researchers have used constructs from both SCT and TPB when examining predictors of physical activity in inactive middle-aged women (Barg et al., 2012). However, the authors found no studies specifically focusing on comparing middle-aged women with and without T2D on the factors related to physical activity. An awareness of any differences in factors associated with physical activity between middle-aged women with T2D and those without the condition is important to determine whether intervention based on theories, such as the SCT and TPB, needs to be tailored to address any unique needs of the former group.
Correlates of Physical Activity in Women and Adults in General With Diabetes
Factors examined in this study were selected from two frameworks used extensively in research related to physical activity in adults, the SCT (Bandura, 1977) and TPB (Ajzen, 1991). A main contention of SCT is that a person interacts with the environment. As a result, the person receives social support from others, some of whom may be actually participating in a specific behavior (role modeling), and develops self-efficacy or the confidence to engage in the behavior, while considering the perceived consequences or benefits of behavioral enactment (outcome expectations). The TPB, however, purports that attitudes toward the behavior, self-efficacy, and subjective norms, defined as the perceived social pressure or support, are associated with behavior. Both theories indicate that personal and social-cognitive factors influence behavior.
Personal factors can be both demographic and health-related. Studies involving women in general (Cleland et al., 2010; Olsen, 2013) and adults of all ages with and without diabetes (Morrato, Hill, Wyatt, Ghushchyan, & Sullivan, 2007; Plotnikoff et al., 2006) indicated that the following specific demographic factors influence physical activity: age, race, marital status, educational level, annual household income, and employment status. Health-related factors associated with physical activity among women in general include long-term illness such as diabetes, poor health, and body mass index (BMI; Cleland et al., 2010; Olsen, 2013). For adults with diabetes, these same factors, along with comorbidity index, depressive symptom severity, and smoking status, are related to physical activity (Morrato et al., 2007; Plotnikoff et al., 2006).
Various social-cognitive factors are associated with physical activity. Studies involving adult participants indicate that these factors include attitudes toward physical activity, physical activity self-efficacy, benefits of physical activity, and social support for physical activity (adults with diabetes of all ages, Allen, 2004; middle-aged adults, Ayotte et al., 2010; middle-aged women, Im, Lee, Chee, Stuifbergen, & the Mapa Research Team, 2011; African American women ≥35 years of age, Murrock & Madigan, 2008; women of all ages, Speck & Harrell, 2003; middle-aged adults, White, Wojcicki, & McAuley, 2012). Poomsrikaew and colleagues (2012) found that physical activity self-efficacy and benefits differed by both sex and age with women being more influenced by self-efficacy than men and middle-aged adults having greater perceived expected benefits than younger adults. In a comprehensive review of the evidence focusing on the maintenance of regular physical activity among women in general, age, race, marital status, socioeconomic status (educational levels and annual household income), BMI, self-efficacy, benefits, and social support were identified as being associated with physical activity (Speck & Harrell, 2003).
Only one previous study was found comparing adults with diabetes with those without the condition on any social-cognitive factors and physical activity (Plotnikoff, Karunamuni, & Brunet, 2009). Using a sample of 2,311 Canadian adults with and without diabetes and controlling for age and sex (covariates), the study found that adults with diabetes had more negative attitudes, along with fewer perceived benefits and less social support (Plotnikoff et al., 2009). Meta-analysis of social-cognitive factors and physical activity has been difficult due to the variability of the physical activity measures and social-cognitive scales (Allen, 2004). A notable gap in the literature is the lack of examination of the association of social-cognitive factors with MVPA measured by accelerometry (Allen, 2004; Plotnikoff, Lubans, Trinh, & Craig, 2012).
To our knowledge, differences in social-cognitive factors associated with physical activity between middle-aged women with T2D and those without the condition have not yet been clearly identified. Therefore, the main purpose of this comparative and correlational study was to examine personal and social-cognitive factors related to physical activity in middle-aged women with T2D compared with those without the condition. Specific research questions were as follows:
Method
Sample and Setting
For this comparative and correlational study, a convenience sample of middle-aged women was recruited from four primary care clinics in an urban Midwest setting over a 7-month period. Women who met the following criteria were included in the study: (a) between 45 and 64 years of age; (b) able to read, write, speak, and comprehend English; and (c) able to respond affirmatively to the question “Are you able to walk independently for at least 10 min during an activity such as grocery shopping?” Diagnosis and/or treatment by a health care provider for T2D was determined initially by self-report and then confirmed by chart audit. Women who reported that they were pregnant were excluded from the study.
Measures
A self-administered pencil–paper survey was used to assess all personal and social-cognitive factors, except for the directly measured BMI. Personal factors were both demographic and health-related. Demographic factors included age, race, marital status, educational level, annual household income, and employment status. Health-related factors included diagnosis of T2D, BMI, comorbidity index, depression symptom severity, and smoking status. Social-cognitive factors included attitudes toward physical activity, physical activity self-efficacy, benefits of physical activity, and social support for physical activity. Physical activity of the middle-aged women who participated was assessed by both self-report and accelerometer. Table 1 lists the instruments used to measure the variables along with their reliability and validity.
Study Variables, Instruments, Reliability, and Validity.
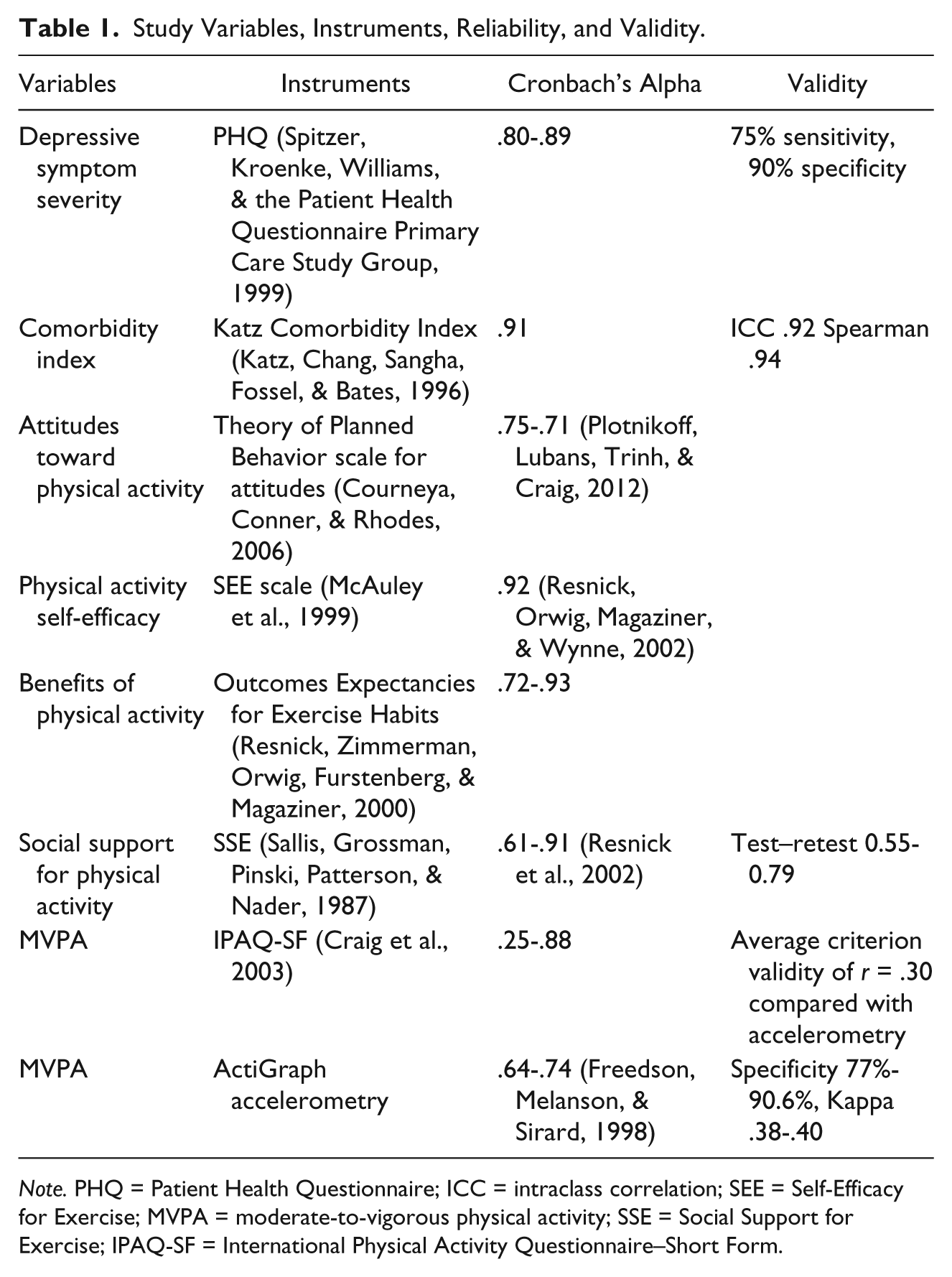
Note. PHQ = Patient Health Questionnaire; ICC = intraclass correlation; SEE = Self-Efficacy for Exercise; MVPA = moderate-to-vigorous physical activity; SSE = Social Support for Exercise; IPAQ-SF = International Physical Activity Questionnaire–Short Form.
Demographic factors
Age was measured in full years from 45 to 64. Women could select more than one response choice for race and only one response choice for marital status, educational level, annual household income, and employment status.
Health-related factors
Diagnosis of T2D was the health-related factor of greatest interest. Duration of diabetes in years, use of oral medication for diabetes (0 = no, 1 = yes), and use of insulin (0 = no, 1 = yes) were also assessed for the middle-aged women with T2D.
BMI
Weight and height of each woman were measured twice by the first author, who successfully completing 2 days of formal training in biometrics prior to the study. A doctorally prepared exercise physiologist and researcher having expertise in this area conducted the training. BMI was calculated by entering the average of the two measured weights and heights into the online CDC (2009) adult BMI calculator.
Comorbidity index
Comorbidity index was measured by each woman’s response to the 17-item Katz version (Katz, Chang, Sangha, Fossel, & Bates, 1996) of the Charlson Comorbidity Index (CCI; Charlson, Pompei, Ales, & MacKenzie, 1987). The Katz version of the CCI was scored using an online version of Microsoft Excel Macro software program (Hall, Ramachandran, Narayan, Jani, & Vijayakumar, 2004). The program utilizes the weighting of 17 comorbidities from 1 to 6 and determines a composite comorbidity score based on age by adding 1 point for each decade after 50 years. The composite comorbidity score was treated as a continuous variable ranging from 0 to 43 (Hall et al., 2004).
Depressive symptom severity
Depressive symptom severity was measured as a continuous variable by responses to the nine-item Primary Care Evaluation of Mental Disorders Patient Health Questionnaire–9 (PHQ-9; Spitzer, Kroenke, Williams, & the Patient Health Questionnaire Primary Care Study Group, 1999). Cut-point scores for depressive symptom severity were (a) 0 to 4 for minimal, (b) 5 to 9 for mild, (c) 10 to 14 for moderate, (d) 15 to 19 for moderately severe, and (e) 20 to 27 for severe (Kroenke et al., 2009). For depression symptom severity scores of 10 or greater, a protocol was followed that included a telephone call and mailed letter to each woman (a) stating the risk of depression, (b) requesting that she speak to her primary care provider about this possibility, and (c) listing sources of mental health assistance.
Smoking status
Smoking was measured by a response choice of yes or no. The single-item question was “Do you currently smoke tobacco?”
Social-cognitive factors
All social-cognitive factors were measured as continuous variables. Scores for each of the individual social-cognitive factors were summed and divided by the number of items in the measure to determine an average score. Higher scores indicated a higher perceived value for that particular social-cognitive factor. For this study, Cronbach’s alphas for the attitudes toward physical activity, physical activity self-efficacy, benefits of physical activity, and social support for physical activity were .81, .90, .91, and .86, respectively, which indicated strong internal consistency reliability.
Attitudes toward physical activity
Attitudes toward physical activity were measured by women’s responses to six items. The item responses were on a continuum from harmful (1) to beneficial (7), useless (1) to useful (7), unimportant (1) to important (7), boring (1) to fun (7), and painful (1) to pleasurable (7) (Courneya, Conner, & Rhodes, 2006).
Physical activity self-efficacy
Physical activity self-efficacy was measured by women’s responses to 10 items on the Self-Efficacy for Exercise (SEE) scale that assesses confidence in the ability to overcome barriers associated with physical activity (McAuley et al., 1999; Resnick & Jenkins, 2000). Response choices ranged from I am not confident (1) to I am very confident (7). One item was added to the SEE to assess incontinence, which has been identified as a significant barrier to physical activity among middle-aged women (Brown & Miller, 2001).
Benefits of physical activity
Benefits of physical activity were measured with the nine-item Outcomes Expectancies for Exercise (OEE) scale (Resnick, Zimmerman, Orwig, Furstenberg, & Magaziner, 2000). Item response choices ranged from strongly disagree (1) to strongly agree (7).
Social support for physical activity
Social support for physical activity was measured by responses to the 13-item Social Support for Exercise (SSE) scale (Sallis, Grossman, Pinski, Patterson, & Nader, 1987). Responses were scored from never (1) to very often (6) with a seventh response of does not apply (7). As suggested by Sallis et al. (1987), scores of 7 were recoded to 1 and negative items were reverse coded. While the original SSE divides responses by family and friends, the instrument used in this study focused only on someone important to me to allow for a more global measurement of social support from anyone rather than a specific type of person. This change was made in response to a cross-sectional study indicating a lack of difference in social support for physical activity by family versus friends in middle-aged and older women (Eyler et al., 1999).
Physical activity
The self-report tool, the International Physical Activity Questionnaire–Short Form (IPAQ-SF), measured physical activity in minutes per day, whereas the accelerometer measured physical activity in minutes per hour. The IPAQ-SF measured moderate, vigorous, and walking intensity of physical activity. The accelerometer measured light-, moderate-, and vigorous-intensity physical activity.
Self-report
The IPAQ-SF, which was designed for use with young and middle-aged adults, assessed self-reported MVPA over the past 7 days (Craig et al., 2003). Across six studies from 10 countries including the United States, the IPAQ-SF demonstrated average criterion validity of r = .30, similar to most physical activity measures (Craig et al., 2003).
Scoring of the IPAQ-SF followed the recommendations described in the 2005 Guidelines for Data Processing and Analysis of the IPAQ. Cleaning of data included truncating vigorous, moderate, and walking minutes per day exceeding 3 hr to 180 min. This method allowed for a maximum of 21 hr per week of MVPA while controlling for outliers. Outliers of more than 960 min of summed walking and MVPA per day were excluded from the study. Walking was considered to be a moderate physical activity. Therefore, minutes of vigorous and moderate physical activity were summed with minutes of walking time to create MVPA for the IPAQ-SF.
Accelerometer-measured
Physical activity was measured in counts per minute by a uniaxial accelerometer, the ActiGraph GT1M (ActiGraph LLC, Fort Walton Beach, Florida). The accelerometer was set to collect data at 60-s intervals. Sufficient data collection was considered to be 4 days with at least 10hr of wear time per day and at least 1 day being a weekend day (Trost, McIver, & Pate, 2005). Matthews, Ainsworth, Thompson, and Bassett (2002) found 80% reliability with 3 to 4 days of accelerometer monitoring for at least 10 hr in a 7-day period.
The ranges of physical activity intensity used for this study and established by Freedson, Melanson, and Sirard (1998) included (a) light (500-1,951 counts/min), (b) moderate (1,952-5,724 counts/min), and (c) vigorous (≥5,725 counts/min). The MeterPlus™ software program (Version 4.2, Santech, San Diego, California) was used to analyze the accelerometry data and to convert the data from counts per minute to minutes of light-, moderate-, and vigorous-intensity physical activity per hour.
Procedures
Investigators received Institutional Review Board approval from both the health care agency associated with the clinics and the university and adhered to procedures established for the protection of human subjects. Multiple methods of recruitment were used, including posters, recruitment flyers, and business cards in examination rooms.
At the initial appointment, which occurred in a private clinic room or at a home visit, the study was explained to each individual woman. Women who were interested in enrolling in the study signed the consent form. Once enrolled, each woman was asked to complete a self-administered paper and pencil survey and to have her weight and height measured.
Women were asked to wear a small light-weight accelerometer on the right hip attached to an elastic waist band at least 10 hr daily on 7 consecutive days and to remove the accelerometer only for sleeping and water activities, such as showering or swimming. Upon verbal agreement, each woman received two telephone calls (2nd day and 5th day) during the week to assess accelerometer wear time and address any issues or concerns.
At the second clinic appointment or home visit with the woman, the accelerometer data were downloaded onto the computer. During the download, data were assessed for valid days and wear time and a graphical output of the data was presented to the woman. A continuous 20 min of 0 counts was considered to be non-wear time (Healy et al., 2007). If the data were not sufficient, the woman was asked to re-wear the accelerometer for another 7 consecutive days. Missing survey data from the initial visit were flagged. Women were asked to review their flagged survey data and complete any missing information. Each woman was asked to complete the IPAQ-SF (Craig et al., 2003).
Analysis
Data were analyzed using the SPSS (Version 21.0). A significance level of .05 was set for the two-tailed analyses. Data were analyzed initially for the total sample of middle-aged women using descriptive statistics and correlations. Comparison testing between the women with and without T2D involved t tests and chi-square tests to evaluate the continuous and categorical variables, respectively. Correlations were used to identify variables associated with MVPA. Pearson and Spearman correlation coefficients were reported for continuous and categorical data, respectively. Missing data were assessed and found to be random effect. No imputation of missing data was utilized.
Due to the small number of women in some categories describing the sample, response choices were combined to create a new category for descriptive data analysis. For race, women were categorized as either “White” or “non-White.” Marital status response choices, including widowed, divorced/separated, and never married, were combined to create a category of “not married/partnered.” Educational levels of some high school education and high school graduate were combined to create a category of “high school graduate or less.” Annual household income was combined to create three categories: “<US$25,000,” “US$25,000 to <US$65,000,” and “≥US$65,000.” Employment status response choices of employed full-time and employed part-time were combined to form the category of “employed.” Response choices of retired, unemployed, and unable to work were combined to form the category of “not employed.”
Results
Of the 104 women who completed the surveys, 37 (35.6%) were confirmed as having T2D by chart audit. Of the 37 women with T2D, duration of the condition ranged from less than 1 year to 25 years with a mean duration of 10.3 (SD = 6.3) years. Of the 37 women with T2D, 29 (76.3%) and 17 (44.7%) reported taking oral anti-diabetes medications and insulin, respectively.
Demographic Factors
For the total sample of women, average age was 53.9 (SD = 5.1) years. For women with T2D and those without the condition, average age was 54.2 (SD = 5.0) and 53.7 (SD = 5.2) years, respectively. Descriptive statistics for all demographic factors except age are listed in Table 2. Differences between middle-aged women with T2D and those without the condition occurred only for race with more non-White than White women having the diagnosis.
Descriptive Statistics for Demographic Factors of the Total Sample of Women (N = 104) and Comparison of Those With (n = 37) and Without (n = 67) T2D.
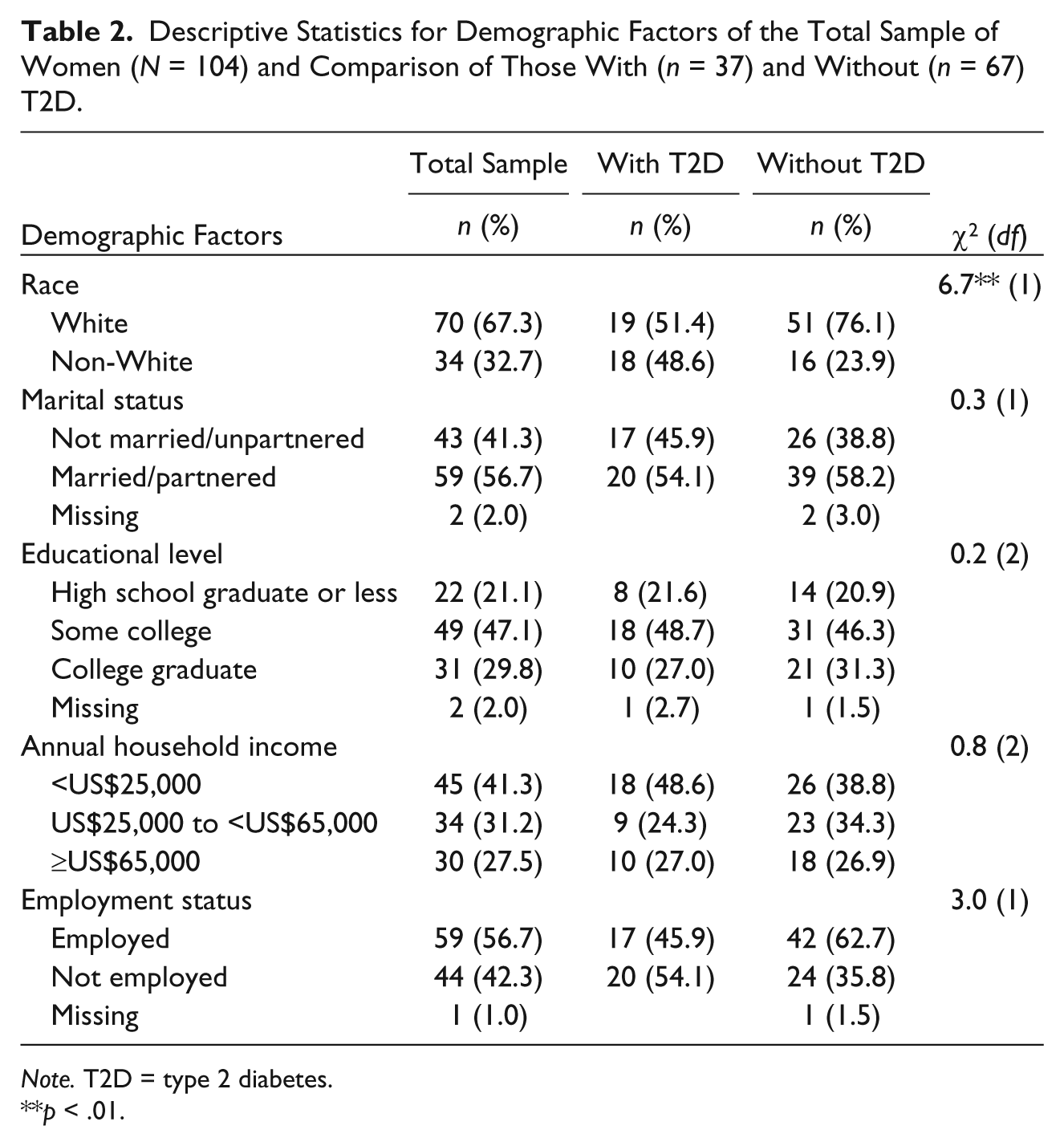
Note. T2D = type 2 diabetes.
p < .01.
Health-Related Factors
Descriptive statistics for all health-related factors except smoking status are noted in Table 3. Women with T2D differed from those without the condition in health-related factors by having higher BMI, 37.4 (SD = 8.2) versus 29.6 (SD = 6.6), and comorbidity index, 3.2 (SD = 1.9) versus 1.1 (SD = 1.7), respectively. For comorbidities, 43 (39.4%) women reported having none, 29 (26.6%) reported one or two, and 37 (33.9%) reported three to seven. Depression symptom severity scores on the PHQ-9 were minimal (n = 64, 58.7%), mild (n = 29, 26.6%), moderate (n = 10, 9.2%), moderately severe (n = 5, 4.6%), and severe (n = 1, 0.9%). Sixteen (14.7%) women scored above 10 on the PHQ-9 and received letters regarding the findings. Of the 103 women who responded to the question about smoking status, the majority (n = 87, 84.5%) did not smoke tobacco. Women with T2D and those without the condition who did not smoke numbered 32 (86.5%) and 35 (50.9%), respectively. The between-group differences in smoking status were not statistically significant.
Descriptive Statistics for Health-Related, Social-Cognitive, and Physical Activity Factors of the Total Sample of Women (N = 104) and Comparison of Those With (n = 37) and Without (n = 67) T2D.
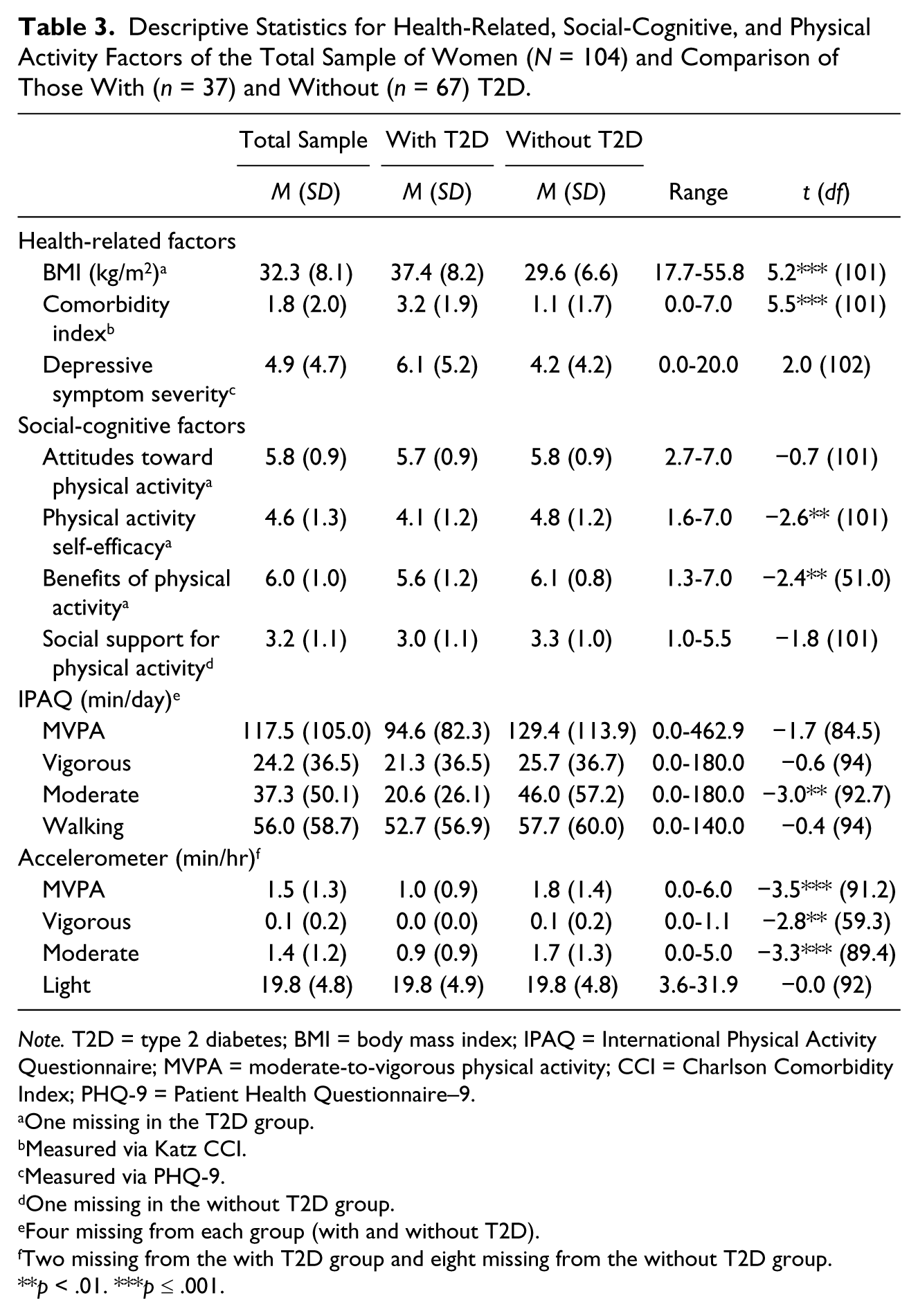
Note. T2D = type 2 diabetes; BMI = body mass index; IPAQ = International Physical Activity Questionnaire; MVPA = moderate-to-vigorous physical activity; CCI = Charlson Comorbidity Index; PHQ-9 = Patient Health Questionnaire–9.
One missing in the T2D group.
Measured via Katz CCI.
Measured via PHQ-9.
One missing in the without T2D group.
Four missing from each group (with and without T2D).
Two missing from the with T2D group and eight missing from the without T2D group.
p < .01. ***p ≤ .001.
Social-Cognitive Factors
As noted in Table 3, women with and without T2D differed in only physical activity self-efficacy and perceived benefits of physical activity. Women with T2D had, on average, lower physical activity self-efficacy, 4.1 (SD = 1.2), and perceived benefits of physical activity, 5.6 (SD = 1.2), than those without the condition, 4.8 (SD = 1.2) and 6.1 (SD = 0.6), respectively.
Physical Activity
Self-report
Table 3 includes descriptive statistics for physical activity measured by self-report. Statistically significant between-group differences in physical activity occurred only for moderate-intensity physical activity with women having T2D reporting fewer minutes per day than those without the condition, 20.6 (SD = 26.1) versus 46.0 (SD = 57.2), respectively.
Accelerometer
Table 3 includes descriptive statistics for physical activity measured by accelerometer. Women with T2D significantly differed from those without the condition by attaining lower MVPA, 1.0 (SD = 0.9) versus 1.8 (SD = 1.4); moderate physical activity, 0.9 (SD = 0.9) versus 1.7 (SD = 1.3); and vigorous, 0.0 (SD = 0.0) versus 0.1 (SD = 0.2), respectively.
Correlates of MVPA
Correlates of MVPA for the total sample of middle-aged women are listed in Table 4. Of all demographic, health-related, and social-cognitive factors, the only correlate of self-reported MVPA measured via the IPAQ-SF was educational level, and the significant relationship occurred in both the total sample and the women without T2D (r = .275, n = 63, p = .029, 95% confidence interval [CI] = [−.489, −.029]). For the total sample of 94 middle-aged women with sufficient accelerometer data, MVPA was positively correlated with White race, attitudes toward physical activity, physical activity self-efficacy, and benefits of physical activity. A negative correlation was found in the total sample between MVPA and T2D diagnosis, BMI, comorbidity index, depressive symptom severity, and smoking status. None of the other demographic, health-related, and social-cognitive factors was significantly correlated to accelerometer-measured MVPA in the total sample.
Pearson Correlations (r) Between Continuous Factors and MVPA for the Total Sample of Women.
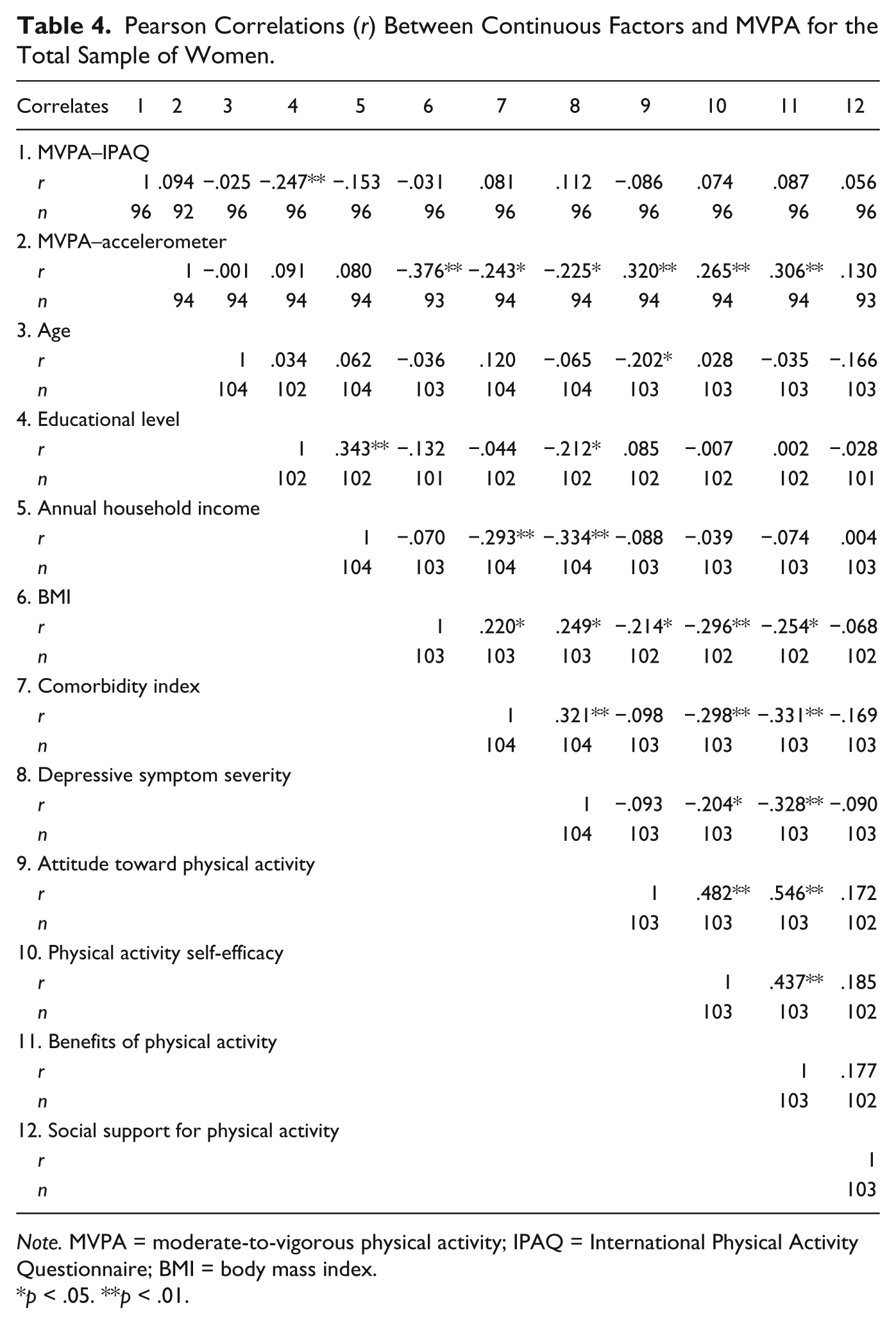
Note. MVPA = moderate-to-vigorous physical activity; IPAQ = International Physical Activity Questionnaire; BMI = body mass index.
p < .05. **p < .01.
For the 59 women without T2D with sufficient accelerometer data, MVPA was positively correlated with attitudes toward physical activity (r = .278, p = .033, 95% CI = [.024, .499]), and negatively correlated with BMI (r = −.309, p = .017, 95% CI = [−.524, −.058]) and smoking status (r = −.288, p = .027, 95% CI = [−.507, −.035]; 0 = no and 1 = yes). None of the other demographic, health-related, and social-cognitive factors was significantly correlated with accelerometer-measured MVPA in the women without T2D.
For the 35 women with T2D with sufficient accelerometer data, MVPA was negatively correlated with taking insulin (r = −.346, p = .042, 95% CI = [−.609, −.014]) and positively correlated with attitudes toward physical activity (r = .388, p = .021, 95% CI = [.063, .639]). None of the other demographic, health-related (including duration of diabetes or oral medication use), or social-cognitive factors was significantly correlated to accelerometer-measured MVPA in the women with T2D.
Discussion
Research Question 1
Findings of a greater percentage of non-Whites in middle-aged women with T2D compared with those without the condition are similar to CDC (2011) data reports about race. Despite their high educational levels, 45 (41.3%) women reported having annual household incomes of less than US$25,000, which is close to the 2013 U.S. Poverty Guideline of US$22,350 for a family of four (USDHHS, 2013). The lack of statistically significant between-group differences in age, educational level, annual household income, and employment status could be attributed to the narrow age range of recruitment.
The CDC (2012) defines overweight for adults as a BMI between 25 and 29.9 and obesity as a BMI ≥ 30. Therefore, the average BMI of middle-aged women in this study was associated with the obesity category. Findings of higher average BMI and comorbidity index in middle-aged women with T2D compared with those without the condition have been previously reported (Shai et al., 2006). Findings of a lack between-group differences in depressive symptom severity conflicts with a study indicating that depression is more prevalent among women with diabetes, as compared with those without the condition (Pan et al., 2010). However, the present study did not assess for provider treatment of depression in the women. The 13% of self-reported smoking among the middle-aged women with T2D was slightly lower than national studies indicating that 15% to 20% of women with diabetes smoke (Karter et al., 2008). Perhaps, participating in a study eliciting information about physical activity was more appealing to non-smokers.
With regard to the social-cognitive factors, the mean score for attitudes toward physical activity was close to the maximum scale score of 7 and had low variability, possibly resulting in an inability to detect significant differences. The high mean score, however, indicates that middle-aged women with and without T2D greatly value physical activity whether or not they participate in it. This study’s findings of lower benefits of physical activity in middle-aged women with diabetes compared with those without the condition are similar to those of previously conducted comparative research involving adults with and without diabetes (Plotnikoff et al., 2009). In contrast, however, the latter study showed no differences in physical activity self-efficacy and greater barriers to physical activity between adults with and without diabetes.
Although the results indicate that raising awareness of benefits may be a beneficial approach to increasing minutes per day of MVPA in middle-aged women, especially those with T2D, additional research is needed to assess knowledge gaps that women with T2D have about the benefits of physical activity and whether these perceptions can be changed through interventions. The scale used to measure benefits of physical activity in this study was not specific to a particular health condition, such as T2D. Instruments specifically focused on measuring perceptions related to physical activity in women with T2D may need to be developed to enhance the relevance of the information obtained. The finding that women with and without T2D had no differences in social support for physical activity is somewhat contradictory to results from other investigations, in which social support emerged as a significant factor for increasing physical activity in African American and Hispanic women (Murrock & Madigan, 2008; Perez, Fleury, & Keller, 2010).
The middle-aged women spent the majority of their MVPA time engaging in moderate-intensity physical activity. On average, based on their self-reported physical activity, the women without T2D met the USDHHS (2008) recommendations, whereas those with the condition did not. According to the accelerometer findings, neither group was sufficiently active enough to meet the USDHHS (2008) recommendations. Differences between the women with T2D and those without the condition are clinically significant because research indicates that physical activity decreases BMI and risk of CVD (Loprinzi & Cardinal, 2013; Zheng et al., 2009). The low level of physical activity attained by women with T2D potentially limited their ability to acquire health benefits associated with adequate engagement in the behavior. Thus, lower perceptions of benefits from physical activity paralleled their lower level of attainment, compared with women without the condition.
Research Question 2
A significant correlation occurred between White race and accelerometer-measured MVPA, reflecting findings similar to those reported by the CDC (2014). Educational level correlated negatively with MVPA measured by the IPAQ-SF for both the total sample and for women without T2D, but not for those with the condition; this finding was not supported by the accelerometer data or in other studies (Cleland et al., 2010; Morrato et al., 2007; Plotnikoff, Mayhew, Birkett, Loucaides, & Fodor, 2004). In a study by Cleland and colleagues, the behavior varied in women by context with the lower socioeconomically disadvantaged performing less leisure and more transportation-related physical activity than women of higher socioeconomic status. In the current study, women with higher levels of education may have had more sedentary occupations than those who were less educated. Thus, assessing context of physical activity, such as specific occupation or work environment, is an important consideration for future research.
Similar findings of a negative correlation between three factors, including diagnosis of diabetes, BMI, and depressive symptom severity, and MVPA were noted in another study. The only difference was that the current study involved measuring MVPA by accelerometers, whereas the other study did not (Morrato et al., 2007).
Findings that BMI and depressive symptom severity were not correlated to accelerometer-measured MVPA in the middle-aged women with T2D are surprising. This occurrence could be explained by the small sample size, the high average BMI, and the lack of sufficient MVPA in the women with T2D. For the middle-aged women with T2D, the negative correlation between taking insulin and MVPA measured by accelerometer could be explained by a fear of hypoglycemia as demonstrated in other research (Brazeau, Rabasa-Lhoret, Strychar, & Mircescu, 2008). Findings concerning smoking and MVPA measured by accelerometer for the total sample and the women without T2D were similar to those from a systematic review that noted a negative association between smoking and self-reported physical activity, particularly among women compared with men, as evidenced in 61% of the reviewed studies (Kaczynski, Manske, Mannell, & Grewal, 2008).
Findings of a high correlation between attitudes toward physical activity and accelerometer-measured MVPA for the total sample, for women without T2D, and for those with the condition indicate that having a positive attitude toward physical activity is important for increasing the behavior. In a 15-year longitudinal study of 1,427 Canadian adults, attitudes significantly predicted self-reported physical activity (Plotnikoff et al., 2012). While physical activity self-efficacy was correlated with only accelerometer-measured MVPA in the total sample, findings from other studies support its importance as a predictor of self-reported physical activity in middle-aged adults (White et al., 2012), women (Perez et al., 2010; Speck & Harrell, 2003), and adults with diabetes (Allen, 2004).
The study has both limitations and strengths. One limitation involves the use of two theoretical models that have the potential to differ conceptually. Generalizability may also be limited due to the small sample size, convenience sampling, and inclusion of only women from the Midwestern United States. In addition, due to the study’s descriptive design, the significant p values do not indicate cause–effect relationships. An important strength is the objective measurement of MVPA via accelerometer. Measurement of physical activity by both self-report and accelerometer was helpful to assess feasibility and reliability when used with middle-aged women. Because the results on the correlates of MVPA differed depending on whether MVPA was measured via self-report or accelerometer, the reliability of self-report is questionable. Prince and colleagues (2008) found that women’s physical activity was from 100% to 4,024% (M = 138%) higher when measured by self-report, as compared with accelerometers. These discrepant findings underscore the importance of using objective measures of physical activity with middle-aged women in future research.
The study identified several demographic, health-related, and social-cognitive factors that are associated with MVPA among middle-aged women, including those with T2D. Because of its significant relationship with MVPA in the total sample of women, those without T2D, and those with the condition, attitudes toward physical activity emerged as a major social-cognitive factor associated with the behavior. The findings that middle-aged women with T2D differ from those without the condition in race, BMI, comorbidity index, physical activity self-efficacy, benefits of physical activity, and MVPA are all important to consider when designing future interventions to increase MVPA. Because physical activity self-efficacy and perceived benefits are significantly lower in women with T2D, as compared with those without the condition, interventions to increase these two modifiable social-cognitive factors may be important for increasing MVPA in middle-aged women with T2D.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author’s dissertation study was funded by Blue Cross Blue Shield of Michigan Foundation, Michigan State University Graduate School and College of Nursing, and the State of Michigan Nurse Corps Initiative. The other authors received no financial support for the research, authorship, and/or publication of this article.