
Abstract
Cognitive behavioral therapy (CBT) is often used to treat chronic pain; however, more information is needed about what are the most efficacious dose and delivery methods. The aims of this review were to determine (a) which CBT doses, delivery methods, strategies, and follow-up periods have been explored in recent intervention studies of individuals with chronic pain and (b) whether the outcomes described in the selected studies were consistent with recommendations by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials. The CINAHL, EMBASE, PubMed, PsycInfo, and SCOPUS databases were searched for randomized controlled trials published from 2009 to 2015 testing CBT for adults with chronic pain. Thirty-five studies were included in this review. Results revealed that CBT reduced pain intensity in 43% of trials, the efficacy of online and in-person formats were comparable, and military veterans and individuals with cancer-related chronic pain were understudied.
Chronic pain affects an estimated 100 million individuals in the United States (Institute of Medicine, 2011). Chronic pain (lasting ≥ 3 months) results from permanent changes in central nervous system processes and often occurs in sites that are distant from the site of the initial injury (Merskey, Bogduk, & International Association for the Study of Pain, 1994). Consequences of chronic pain include decreased quality of life (O’Connor, 2009), impaired sleep, decreased physical function, impaired family and social relationships, depression, and job loss (Breivik, Collett, Ventafridda, Cohen, & Gallacher, 2006). Cognitive behavioral therapy (CBT) is one non-pharmacological intervention that has been tested extensively as a treatment for chronic pain in randomized controlled trials to date. The overall objective of this integrative review is to explore the efficacy of CBT for the treatment of adults with chronic pain based on evidence from recently published randomized controlled trials.
The Complexity of Chronic Pain
Chronic pain is an inherently complex and subjective experience influenced by biological, psychological, and social factors (Ehde, Dillworth, & Turner, 2014). Chronic pain is difficult to treat because it often occurs alongside other symptoms such as sleep disturbance, anxiety, and depression (Attal, Lanteri-Minet, Laurent, Fermanian, & Bouhassira, 2011) that may increase pain severity and lead to further reductions in quality of life and physical function (Bair, Robinson, Katon, & Kroenke, 2003; Beesdo et al., 2010; Gupta et al., 2007; McCracken & Iverson, 2002). Anxiety and sleep disturbance co-occur in up to 45% and 53% of individuals with chronic pain, respectively (Kroenke et al., 2013; Tang, Wright, & Salkovskis, 2007; Taylor et al., 2007). In addition, depression has been shown to be associated with increased pain severity in 21% to 72% of cases (McWilliams, Goodwin, & Cox, 2004; Poole, White, Blake, Murphy, & Bramwell, 2009).
Due to the several co-occurring symptoms associated with chronic pain, optimal management of chronic pain is challenging. First line treatments for chronic pain include tricyclic antidepressants and combined serotonergic and noradrenergic antidepressants, calcium channel α2-δ ligands, and topical lidocaine (Dworkin et al., 2010; Park & Moon, 2010). However, meta-analyses suggest that only about half of patients experience clinically meaningful pain relief from pharmacological therapies (Bjordal, Klovning, Ljunggren, & Slørdal, 2007; Finnerup, Sindrup, & Jensen, 2010; L. A. Machado, Kamper, Herbert, Maher, & McAuley, 2009; G. C. Machado et al., 2015). Furthermore, many patients discontinue pharmacological therapy due to burdensome side effects, fear of addiction, or lack of efficacy (Broekmans, Dobbels, Milisen, Morlion, & Vanderschueren, 2010; McNicol, Midbari, & Eisenberg, 2013). Given the low efficacy of pharmacological therapies for chronic pain management, multidimensional approaches that include pharmacological and non-pharmacological treatment modalities are necessary to effectively manage chronic pain and the associated comorbid medical, psychological, and psychosocial conditions (American Academy of Pain Medicine, 2013; American Society of Anesthesiologists Task Force on Chronic Pain Management & American Society of Regional Anesthesia and Pain Medicine, 2010; Chou et al., 2009).
CBT for chronic pain is a non-pharmacological treatment that is typically delivered via individual or group counseling sessions that occur over several weeks (Ehde et al., 2014). CBT for chronic pain reduces pain perception and psychological distress by improving an individual’s ability to cope with their pain (Ehde et al., 2014; Kerns, Sellinger, & Goodin, 2011). Cognitive behavioral strategies for pain include, but are not limited to, cognitive restructuring, relaxation techniques, time- or quota-based activity pacing, and sleep hygiene. Cognitive restructuring involves identifying and reframing automatic negative thoughts, and their resulting behaviors in an effort to develop more adaptive coping thoughts and behaviors (Kerns et al., 2011). Relaxation training includes strategies such as deep breathing, progressive muscle relaxation, and visualization to reduce muscle tension and alter the perception of physical pain (Kerns et al., 2011). Activity pacing is a behavioral strategy used to help individuals schedule their activities based on time or quotas (rather than based on pain) to maximize their functionality despite persistent pain (Kerns et al., 2011). In addition, sleep hygiene refers to a variety of sleep scheduling, dietary, environmental, and activity strategies to improve sleep onset, maintenance, and quality (McCurry, Logsdon, Teri, & Vitiello, 2007).
Cognitive behavioral therapy for pain is based on the Gate Control Theory of Pain (Melzack & Wall, 1965). According to the Gate Control Theory, descending modulation from areas in the brain that govern thought (frontal cortex), emotions (limbic system), and regulatory processes (i.e., hypothalamus) influence pain transmission in the dorsal horn of the spinal cord via neurotransmitters, endogenous opiates, and hormones such as cortisol. Moreover, as an update to the Gate Control Theory, Neuromatrix Theory (Melzack, 1999) suggests that multiple sensory, cognitive, visual, and emotional inputs may disrupt the homeostasis-regulation patterns of the brain’s built-in matrix of neurons (the neuromatrix), producing a prolonged stress response (i.e., cortisol release). Due to this prolonged stress response, there may be an increase of muscle, bone, and neural tissue destruction that creates the conditions necessary for varying chronic pain conditions (Melzack, 1999). Preliminary evidence from functional magnetic resonance imaging trials suggest that CBT-induced structural changes in the prefrontal cortex may lead to the release of pain-inhibiting neurotransmitters which “gate” or block pain impulse transmission from the spinal cord to the brain (Jensen et al., 2012; Seminowicz et al., 2013) Thus, CBT-mediated descending inhibitory mechanisms result in decreased pain perception (Turk, Meichenbaum, & Genest, 1983).
A recent Cochrane systematic review (n = 42 articles) conducted by A. C. Williams, Eccleston, and Morley (2012) explored the efficacy of randomized controlled trials testing psychological treatments (CBT and behavioral therapy, respectively) for adults with chronic pain. The authors searched the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, and Psychlit databases from their inception to September 2011 using Medical Subject Heading terms such as “Pain,” “Psychotherapy,” “Cognitive therapy,” “Behavior therapy,” “Biofeedback (Psychology),” and “Mind-Body and Relaxation Techniques.” Results revealed that when compared with treatment as usual at post-treatment, CBT had a small effect on pain intensity and disability and a moderate effect on ratings of catastrophizing and mood (anxiety and depression). When compared with treatment as usual at follow-up (6-12 months post-treatment), CBT had no effect on pain intensity, a small effect on disability and mood, and a moderate effect on catastrophizing (A. C. Williams et al., 2012).
While strong evidence from the Cochrane review (A. C. Williams et al., 2012) demonstrates that CBT is effective for chronic pain compared with treatment as usual at post-treatment, more information is needed about whether CBT’s efficacy varies based on (a) the underlying pain etiology (such as cancer vs. low back pain), (b) “dose” (duration of therapy in weeks and number of hours) or delivery method, and (c) additional pain-related outcomes in individuals with chronic pain (Bernardy, Klose, Busch, Choy, & Hauser, 2013; Eccleston et al., 2014; Ehde et al., 2014; Macea, Gajos, Daglia Calil, & Fregni, 2010; A. C. Williams et al., 2012). It is important to target the most efficacious CBT delivery methods and doses to specific chronic pain populations to effectively utilize available CBT resources. Access to CBT treatment may be limited due to lack of transportation to the clinic, beliefs that only pharmacological treatments work for pain, the negative stigma associated with psychological therapy, and lack of trained providers (Ehde et al., 2014; D. A. Williams et al., 2010). Thus, targeting optimal doses and delivery formats to specific chronic pain populations may enhance the efficacy, acceptance, and availability of CBT for individuals with chronic pain.
The Cochrane review conducted by A. C. Williams et al. (2012) reported on key pain-related outcome variables, such as pain intensity, physical functioning, and mood, but did not report the effect of CBT on other pain-related outcome variables recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) such as fatigue, sleep impairment, satisfaction with treatment, and participant global impression of change at post-treatment and follow-up. The IMMPACT guidelines recommend that all chronic pain clinical trials contain six core outcome domains: (a) pain, (b) physical function, (c) emotional functioning, (d) participant rating of improvement, (e) symptoms and adverse events, and (f) participant disposition (Dworkin et al., 2005). Examining the efficacy of CBT for chronic pain on a variety of pain-related outcomes is important due to the many biological, psychological, and social influencing factors that may contribute to the chronic pain experience (Ehde et al., 2014). It is also beneficial for chronic pain trials to measure IMMPACT-related variables to evaluate the efficacy of different treatments across trials more readily (Dworkin et al., 2005). Thus, due to the known variability in CBT intervention design and delivery (A. C. Williams et al., 2012), the use of the IMMPACT domains will help determine the efficacy of the varying CBT interventions in this review on a spectrum of pain-related variables.
Purpose
The purpose of this integrative review was to determine which CBT doses (duration of therapy in weeks and number of hours), delivery methods, strategies, and follow-up periods have been explored in recent intervention studies and in which chronic pain populations. We also examined and compared these CBT intervention design features based on guidelines recommended by the IMMPACT (Dworkin et al., 2005). Overall, this integrative review furthers the results of the Cochrane review authored by A. C. Williams and colleagues (2012) by examining the efficacy of CBT for chronic pain based on: (a) specific durations and hours of treatment, (b) delivery method, and (c) a variety of IMMPACT-related outcomes. The information provided in this review will inform future research exploring new approaches for augmenting CBT’s effectiveness and expanding access to diverse chronic pain populations.
Method
Search Method
The CINAHL, EMBASE, PubMed, PsycInfo, and SCOPUS databases were searched for randomized controlled trials published between 2009 and 2015 testing CBT interventions in adults with chronic pain. The key search terms were cognitive behavioral therapy and chronic pain (Electronic Supplementary Table 1). Papers published between 2009 and 2015 were selected for this review because literature published before 2009 has already been summarized in several systematic reviews (Bernardy et al., 2013; Eccleston et al., 2014; Hofmann, Asnaani, Vonk, Sawyer, & Fang, 2012; Lunde, Nordhus, & Pallesen, 2009; Macea et al., 2010; A. C. Williams et al., 2012), and the focus of this review was to formulate updated conclusions surrounding the efficacy of CBT for chronic pain based on the most recent literature.
Inclusion and Exclusion Criteria
The inclusion criteria for the selection of the articles were (a) participants were above 18 years of age, (b) randomized controlled trial, (c) English language, (d) access to the full article, (e) published between 2009 and 2015, (f) contained outcome variable of pain intensity, (g) tested CBT interventions in individuals with chronic pain (present for ≥ 3 months) and (h) compared CBT against a control condition (i.e., standard care, education only, or exercise only). Excluded articles focused on acceptance and commitment therapy or mindfulness therapy. Acceptance and commitment therapy strives to increase functioning by improving psychological flexibility (Wicksell et al., 2013). Similarly, mindfulness therapy involves the acceptance of physical pain or psychological distress to decrease catastrophizing (Lakhan & Schofield, 2013). In contrast, CBT focuses on trying to teach individuals how to better control their thoughts and behaviors in relation to their pain (Kerns et al., 2011). Thus, acceptance and commitment therapy and mindfulness therapies were excluded in this review because when compared with CBT, these treatments decrease chronic pain severity via a slightly different mechanism.
Search Outcome
The initial search yielded 308 results. The number of studies from the CINAHL, EMBASE, PubMed, PsycInfo and SCOPUS databases were 41, 65, 63, 23, and 116, respectively (Electronic Supplementary Figure 1). After removing the duplicate articles, 185 unique studies were identified (no articles were excluded due to lack of access to the full text). Next, the inclusion and exclusion criteria were applied when examining the title and abstract, reducing the number of articles to 55. Excluded studies (a) were non-randomized controlled trials; (b) tested ACT, mindfulness, or other non-CBT interventions; (c) included non-adult populations or subjects that did not have chronic pain; and (d) did not include a pain intensity measure. Seventeen more articles were excluded following a full article review, leaving 38 articles. These 38 articles were critically appraised by the primary author using the CONSORT checklist to assess for risk of bias (Schulz, Altman, & Moher, 2010). For articles that the primary author identified as containing a high risk of bias, the primary author and his advisor further discussed the articles in question and decided whether to include them in the review. After CONSORT review, three additional articles were removed due to poor study quality (Castro, Daltro, Kraychete, & Lopes, 2012; Khan, Akhter, Soomro, & Ali, 2014; Linden, Scherbe, & Cicholas, 2014). An article authored by Castro et al. (2012) was removed because the authors did not fully explain the rationale for their choice of measures, the randomization procedure, or the statistical methods. The article authored by Khan et al. (2014) was excluded because the authors did not thoroughly describe the results of the study or the reliability and validity of the measures used. Last, an article authored by Linden et al. (2014) was removed because the authors did not elaborate on the statistical approaches used to analyze the measures, discuss the generalizability of the findings, or explicate the randomization process. After removing these three studies, 35 were retained and became the basis for this literature review.
Data Abstraction and Measurement Strategy
The following information was abstracted from the 38 studies: (a) sample size, (b) chronic pain population, (c) CBT intervention strategies, (d) control intervention design, (e) CBT dose (duration of therapy in weeks and number of hours), (f) follow-up period, (g) CBT delivery method, (h) pain intensity and other IMMPACT outcome measures, and (i) effects on IMMPACT/primary outcomes. A study was considered positive if the CBT intervention had a significant effect (p < .05; as reported by authors of included studies) on pain intensity in comparison with the control conditions. A study was considered positive for IMMPACT/primary outcomes if the CBT intervention had a significant effect (p < .05) on at least one IMMPACT-related variable (anxiety, depression, quality of life, global impression of change, physical function, sleep disturbance, or fatigue) or other primary outcome (as specified by the authors of the included trials) in comparison with the control condition. Similarly, if a study tested two different CBT interventions, the study was considered positive if either CBT intervention had a significant effect (p < .05) on pain intensity or at least one IMMPACT/primary outcome in comparison with the control condition. Positive studies were then categorized based on the population studied and CBT intervention characteristics (CBT dosage, strategies, delivery method, follow-up period).
Results
Abstracted information from the 35 studies is summarized in Table 1. Furthermore, details regarding the frequency of positive studies by population, CBT intervention characteristics, and outcome variables are highlighted in Tables 1 and 2, and Electronic Supplementary Tables 2 to 4.
CBT Randomized Controlled Trials Published 2009-2015.
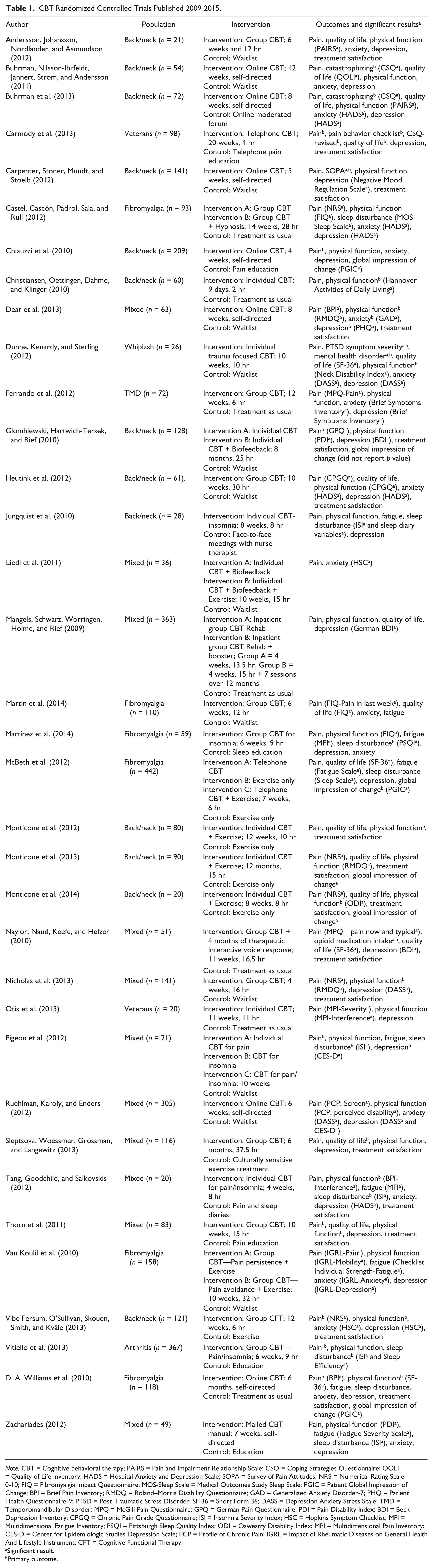
Note. CBT = Cognitive behavioral therapy; PAIRS = Pain and Impairment Relationship Scale; CSQ = Coping Strategies Questionnaire; QOLI = Quality of Life Inventory; HADS = Hospital Anxiety and Depression Scale; SOPA = Survey of Pain Attitudes; NRS = Numerical Rating Scale 0-10; FIQ = Fibromyalgia Impact Questionnaire; MOS-Sleep Scale = Medical Outcomes Study Sleep Scale; PGIC = Patient Global Impression of Change; BPI = Brief Pain Inventory; RMDQ = Roland–Morris Disability Questionnaire; GAD = Generalized Anxiety Disorder-7; PHQ = Patient Health Questionnaire-9; PTSD = Post-Traumatic Stress Disorder; SF-36 = Short Form 36; DASS = Depression Anxiety Stress Scale; TMD = Temporomandibular Disorder; MPQ = McGill Pain Questionnaire; GPQ = German Pain Questionnaire; PDI = Pain Disability Index; BDI = Beck Depression Inventory; CPGQ = Chronic Pain Grade Questionnaire; ISI = Insomnia Severity Index; HSC = Hopkins Symptom Checklist; MFI = Multidimensional Fatigue Inventory; PSQI = Pittsburgh Sleep Quality Index; ODI = Oswestry Disability Index; MPI = Multidimensional Pain Inventory; CES-D = Center for Epidemiologic Studies Depression Scale; PCP = Profile of Chronic Pain; IGRL = Impact of Rheumatic Diseases on General Health And Lifestyle Instrument; CFT = Cognitive Functional Therapy.
Significant result.
Primary outcome.
CBT Intervention Characteristics.
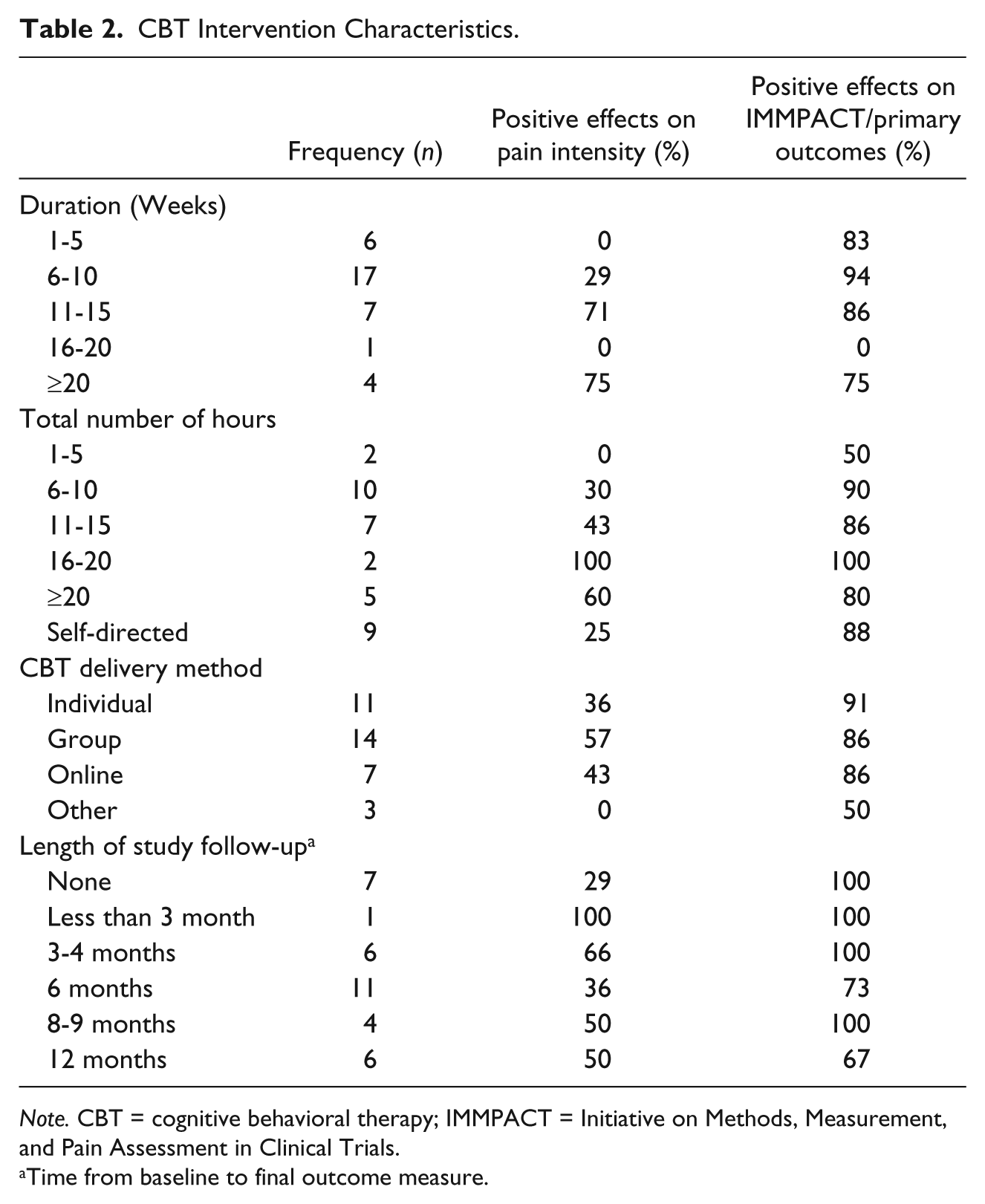
Note. CBT = cognitive behavioral therapy; IMMPACT = Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials.
Time from baseline to final outcome measure.
Populations
The chronic pain populations of focus in the 35 studies are described in Table 1 and Electronic Supplementary Table 2. The sample sizes (intervention and control group combined) of the included trials ranged from 20 (Monticone et al., 2014; Otis et al., 2013; Tang, Goodchild, & Salkovskis, 2012) to 442 (McBeth et al., 2012). Mean CBT group participant ages ranged from 39.57 (Ferrando et al., 2012) to 74.59 (Nicholas et al., 2013) years. The most frequently studied population was individuals with back/neck pain, followed by the mixed etiology and fibromyalgia populations. To clarify, the mixed etiology category contained studies of participants with various chronic pain conditions (i.e., back, knee, or joint pain). There also were no studies involving individuals with cancer-related chronic pain, and only two studies focused on military veterans with chronic pain. More than half of the studies testing CBT in patients with fibromyalgia and temporomandibular disorder showed significant reductions in pain intensity. Moreover, greater than 50% of the studies that tested CBT in military veterans and individuals with back/neck pain, mixed etiology, fibromyalgia, temporomandibular (one study), and whiplash associated with chronic pain (one study) demonstrated significant effects on the IMMPACT/primary outcomes studied, respectively.
CBT Intervention Characteristics
Tables 1, 2, and Electronic Supplementary Table 4 summarize the characteristics of the CBT interventions as described in the selected papers. More specifically, these tables summarize the delivery methods, doses (duration of therapy in weeks and number of hours), length of the follow-up periods, and strategies tested in the CBT interventions.
Delivery methods
Table 2 outlines the frequency of studies investigating various CBT delivery methods and the effects of each method on key outcome variables. The most frequently studied delivery method was group CBT, followed by individual and online CBT, respectively. Approximately 57% or less of the trials testing in-person delivery methods reported significant effects on pain intensity; however, more than 86% of these trials reported significant effects on IMMPACT/primary outcomes. Online CBT (CBT-OL) was also studied in seven trials, and 43% and 86% of these trials found significant effects on pain intensity and IMMPACT/primary outcomes, respectively. Furthermore, three studies tested CBT delivered via telephone or self-directed CBT manual (participants were mailed the CBT treatment manual and were asked to practice the CBT strategies on their own). Zero percent of the trials testing these formats reported significant effects on pain intensity, while 50% of the trials found significant results on IMMPACT/primary outcomes.
CBT dose
Table 2 displays the number of trials testing various CBT dosages based on the total number of weeks and hours of CBT received by study participants and the doses’ effects on pain intensity and IMMPACT/primary outcomes. The most frequently studied duration of CBT was six to 10 weeks (range = 2-52 weeks; Christiansen, Oettingen, Dahme, & Klinger, 2010; Monticone et al., 2013). Six to 10 weeks of CBT significantly reduced pain intensity in only 29% of the 17 trials, but had positive effects on IMMPACT/Primary outcomes in 94% of the studies. Results revealed that higher durations of CBT (more than 20 weeks) led to significant effects on pain intensity and the IMMPACT/Primary outcomes in 75% of the four trials testing this duration.
The most frequently studied total number of CBT hours was six to 10 total hours (range = 1-37.5 hr; Christiansen et al., 2010; Sleptsova, Woessmer, Grossman, & Langewitz, 2013). Results demonstrated that six to 10 total hours of CBT was effective decreasing pain intensity in 30% of trials; however, this dosage led to statistically significant results on IMMPACT/Primary outcomes in 90% of the 10 trials. Moreover, studies consisting of interventions testing less than six total CBT hours had positive effects on pain intensity and IMMPACT/Primary outcomes in 0% and 50% of two trials, respectively. However, interventions testing more than 20 total CBT hours demonstrated significant improvements in pain intensity and IMMPACT/Primary outcomes in 60% and 80% of five trials, respectively.
Furthermore, nine studies were found in which the CBT dose was defined by the participant (self-directed). In these studies, CBT was administered via the Internet or a self-directed manual that allowed the participants to use the software or CBT strategies for as much as they wanted. The trials testing a self-directed format revealed significant effects on pain intensity and the IMMPACT/Primary outcomes in 25% and 88% of the trials, respectively.
Follow-up period
Twenty-eight studies tested a follow-up period beyond the termination of the CBT intervention (Table 2). Most studies followed patients for 6 months (range = no follow-up to 1 year). Trials that tested a 6-month follow-up period reported significant effects on pain intensity and the IMMPACT/Primary outcomes in 36% and 73% of 11 trials, respectively. Moreover, only six studies tested a follow-up period of 12 months. Of these six studies, 50% and 67% of the trials reported positive effects on pain intensity and IMMPACT/Primary outcomes, respectively.
CBT intervention strategies
Electronic Supplementary Table 4 describes the CBT strategies used in the included trials. The most studied CBT strategy was cognitive restructuring (91% of trials), followed by pain/psychoeducation (80% of trials), relaxation (60% of trials), and activity pacing (60% of trials), respectively. However, the strategies of the CBT interventions varied widely across studies. Additional CBT strategies used in the included studies included biofeedback, hypnosis, sleep hygiene, assertiveness training, expressive writing, relapse prevention, goal setting, graded exposure, exercise, sleep restriction, and stimulus control.
Outcome Measures and Results
Table 1 and Electronic Supplementary Tables 3 and 5 describe the measures and results of the interventions as reported by the selected papers. In particular, Table 1 describes the IMMPACT outcomes studied and the significant results of the selected studies. Electronic Supplementary Table 3 summarizes the interventions’ effects on IMMPACT outcomes such as pain intensity, anxiety, depression, quality of life, global impression of change, physical function, treatment satisfaction, sleep disturbance, and fatigue. In addition, Electronic Supplementary Table 5 lists the most commonly used pain intensity measures in the selected studies.
Pain intensity and IMMPACT/primary outcomes studied
Table 1 lists the pain intensity and IMMPACT/Primary outcomes studied in the selected randomized controlled trials. The pain intensity measures utilized most commonly in these studies (Electronic Supplementary Table 5) included 0 to 10 rating scales (34% of trials), the Multidimensional Pain Index (17% of trials), the Brief Pain Inventory (14% of trials), the McGill Pain Questionnaire (8% of trials), and the Chronic Pain Grade Questionnaire (6% of trials).
In addition to pain intensity, other primary outcomes studied included anxiety, depression, post-traumatic stress disorder symptom severity, physical function, pain intensity, pain attitudes, pain behaviors, catastrophizing, mental health, global impression of change, opioid intake, sleep disturbance, and quality of life. However, only 8 out of 35 studies specifically targeted pain intensity as a primary outcome (Carmody et al., 2013; Chiauzzi et al., 2010; Glombiewski, Hartwich-Tersek, & Rief, 2010; Pigeon et al., 2012; Thorn et al., 2011; Vibe Fersum, O’Sullivan, Skouen, Smith, & Kvåle, 2013; Vitiello et al., 2013; D. A. Williams et al., 2010).
Intervention effects on pain intensity and IMMPACT/primary outcomes
Electronic Supplementary Table 3 highlights the number of trials testing various IMMPACT outcomes and the CBT interventions’ effect on the selected IMMPACT outcome variables. Pain intensity was measured in all of the trials, but only 16 of the 35 (43%) studies found significant effects. This percentage was lower than any other IMMPACT variable examined. Furthermore, CBT was shown to significantly improve IMMPACT/Primary outcome variables in 86% (30 out of 35) of the trials. Specifically, depression, anxiety, and physical function were the most frequently studied IMMPACT variables and were significantly improved by CBT interventions in 56% to 63% of the trials testing these outcomes. In addition, there were a higher number of studies reporting significant effects for the variables of sleep disturbance and global impression of change than any other outcome examined.
Discussion
This integrative review provides an overview of which CBT dose, delivery methods, follow-up periods, and strategies have been explored in recent intervention studies, and in which chronic pain populations. We also evaluated whether the CBT outcome variables described in the selected 35 studies align with those that have been recommended by the IMMPACT guidelines (Dworkin et al., 2005). Eight key findings emerged from the 35 randomized controlled trials: (a) additional studies are needed to test CBT interventions in individuals with cancer-related chronic pain and military veterans; (b) the optimal dose of CBT is unclear; (c) online cognitive behavioral therapy (CBT-OL) effectiveness may be comparable with traditional formats of CBT such as individual or group therapy; (d) less than 50% of the included trials reported positive effects on pain intensity; (e) future studies are needed to investigate CBT’s effects on anxiety, quality of life, sleep disturbance, treatment satisfaction, global impression of change, and fatigue in individuals with chronic pain; (f) additional research is needed to investigate mediators of pain intensity improvement following CBT treatment; (g) further studies are needed to examine the long-term efficacy of CBT for pain intensity in individuals with chronic pain; and (h) future research is needed to compare the efficacy of CBT treatment strategies. Additional details regarding these eight key findings are highlighted below.
The findings of this review revealed that the fibromyalgia, veteran, temporomandibular, arthritis, and cancer-related chronic pain populations were the least frequently studied. Surprisingly, results revealed that there were no trials testing CBT for individuals with cancer-related chronic pain. Due to the high incidence and debilitating consequences of cancer-related chronic pain, further research is needed to improve treatment in this population. In fact, 19% to 39.1% (Bennett et al., 2012) of individuals with cancer experience chronic pain due to the disease and its treatment (surgery, neurotoxic chemotherapy, radiation therapy; Smith et al., 2014). In addition, cancer treatment–related chronic pain commonly co-occurs with depression, anxiety, sleep disturbance, and physical impairment (Andersen & Kehlet, 2011; Belfer et al., 2013; Miaskowski et al., 2014; Mols, Beijers, Vreugdenhil, & van de Poll-Franse, 2014). While this current review revealed that there are no randomized controlled trials testing CBT for individuals suffering from cancer-related chronic pain, a meta-analysis authored by Tatrow and Montgomery (2006) revealed that cognitive behavioral strategies were effective in reducing pain (d = .49) and distress (d = .31) in individuals with breast cancer (Tatrow & Montgomery, 2006). In addition, Kwekkeboom and colleagues (2012) conducted a pilot randomized controlled trial to assess the efficacy of guided imagery and relaxation techniques in individuals with advanced cancer. This trial found positive significant results for CBT to treat the acute pain, fatigue, and sleep symptom cluster of cancer but was not included in this review because it did not specifically enroll individuals with chronic pain. Thus, there is preliminary evidence that CBT strategies are beneficial for individuals with cancer, but further research is needed to test CBT in individuals with cancer-related chronic pain.
Furthermore, due to improvements in battlefield armor, military medicine, and combat evacuation, a greater number of returning Operational Enduring Freedom and Iraqi Freedom veterans face the challenges of chronic pain (Clark, Bair, Buckenmaier, Gironda, & Walker, 2007). Nearly 50% of veterans report chronic pain (Gironda, Clark, Massengale, & Walker, 2006), and musculoskeletal pain is the most commonly reported pain complaint of returning Operational Enduring Freedom and Iraqi Freedom veterans (Higgins et al., 2014). In addition, military veterans are a unique chronic pain population due to their high incidence of comorbid post-traumatic stress disorder and traumatic brain injury (Lew et al., 2009). This triad of chronic pain, post-traumatic stress disorder, and traumatic brain injury is called post-deployment multi-symptom disorder. In fact, in a sample of Operational Enduring Freedom and Iraqi Freedom veterans (n = 340), 42.1% were diagnosed with post-deployment multi-symptom disorder (Lew et al., 2009). Despite the complexity of the chronic pain experience faced by military veterans, only two (Carmody et al., 2013; Otis et al., 2013) of the 38 studies tested a CBT intervention in military veterans. Due to the number of military veterans returning from overseas combat with chronic pain, additional randomized controlled trials are needed to explore the efficacy of CBT in this population.
Results revealed that the most commonly studied duration of treatment was six to 10 weeks, and the most frequently studied total number of CBT hours was six to 10. CBT effectiveness varied widely based on the total number of weeks and hours of CBT received by study participants. For example, when examining CBT effects at various dosages (treatment duration), the percentage of trials reporting positive effects for pain intensity range from 0% (1-5 weeks) to 75% (>20 weeks). In addition, there was only one study that compared one CBT dose with another (Mangels, Schwarz, Worringen, Holme, & Rief, 2009). This study demonstrated that a 4-week group CBT program did not result in significantly different participant ratings of depression or quality of life when compared with a 4-week group CBT program with subsequent booster sessions (seven additional CBT sessions over 12 months; Mangels et al., 2009). The lack of studies comparing CBT dosages in the current research evidence makes it difficult to recommend an optimal course of therapy. However, as randomized controlled trials show that six to 10 weeks and six to 10 total hours of CBT demonstrate positive effects on IMMPACT/Primary outcomes, perhaps a similar dosage should be defined as “standard” in future research. Defining a standardized CBT dose will allow for the comparison of CBT studies across trials.
Regarding the efficacy of online delivery methods, results of this review demonstrated that CBT-OL is effective for individuals with fibromyalgia (D. A. Williams et al., 2010), back/neck pain (Buhrman, Nilsson-Ihrfeldt, Jannert, Strom, & Andersson, 2011; Carpenter, Stoner, Mundt, & Stoelb, 2012), and mixed etiology chronic pain (Buhrman et al., 2013; Dear et al., 2013; Ruehlman, Karoly, & Enders, 2012). Specifically, randomized controlled trials suggest that CBT-OL is effective for the management of chronic pain based on the following: (a) CBT-OL significantly improves IMMPACT/Primary outcomes compared with a control condition, (b) CBT-OL’s positive effects persist more than 6 months beyond treatment completion (Buhrman et al., 2013; D. A. Williams et al., 2010), and (c) CBT-OL users are satisfied with the online format (Carpenter et al., 2012; Dear et al., 2013; D. A. Williams et al., 2010). These findings are consistent with prior systematic reviews that have demonstrated that CBT-OL significantly improves pain and pain-related outcomes such as anxiety and disability when compared with control conditions (Eccleston et al., 2014; Macea et al., 2010).
Analysis of CBT delivery methods revealed that there was a comparable number of CBT-OL and in-person CBT intervention studies reporting positive effects on pain intensity and IMMPACT/Primary outcomes. The efficacy of CBT-OL versus in-person CBT has been recently examined in a randomized controlled trial. While not included in this review because it compared two active CBT treatments, de Boer, Versteegen, Vermeulen, Sanderman, and Struys (2014) conducted a randomized controlled trial comparing CBT-OL with in-person group CBT in individuals with non-specific chronic pain and found that participants in the CBT-OL group had significantly greater reductions in catastrophizing, pain intensity, pain coping, and in some aspects of quality of life compared with group CBT. One limitation of this study was that more patients dropped out of CBT-OL treatment (33.3%) than group CBT treatment (6.7%). If patients dropped out due to perceived low efficacy, this may have compromised the study’s internal validity. Furthermore, a systematic review by Macea and colleagues (2010) uncovered a 26.6% dropout rate in 11 randomized controlled trials testing CBT-OL for chronic pain. Despite the higher dropout rates reported in CBT-OL trials, an online delivery method is a potential solution to the accessibility barriers inherent with individual or group CBT because it can be delivered via the participant’s personal computer, tablet, or smartphone. Additional research is needed to determine whether CBT-OL is equivalent or superior to in-person CBT and to determine CBT-OL’s efficacy as a treatment for various types of chronic pain.
This review revealed that CBT significantly improved pain intensity in 43% of the trials. The low number of positive trials may be related to study design limitations. First, pain intensity was only studied as the primary outcome in eight of the included trials. Thus, the CBT interventions of the included studies may have been designed to target a co-occurring psychological symptom and were not powered to detect changes in pain intensity. Second, 17 studies included in this review compared CBT with another active intervention and not with a true control group. This limitation has been previously described by A. C. Williams and colleagues (2012) in their systematic review which revealed that CBT was not effective in significantly reducing chronic pain intensity when compared with active controls (A. C. Williams et al., 2012). Third, internal validity threats such as attrition (Carpenter et al., 2012; Chiauzzi et al., 2010; Jungquist et al., 2010), invalid statistical conclusions due to small sample size, or multiple statistical analyses (Andersson, Johansson, Nordlander, & Asmundson, 2012; Dunne, Kenardy, & Sterling, 2012; Heutink et al., 2012; Jungquist et al., 2010; Liedl et al., 2011; McBeth et al., 2012; Monticone et al., 2014; Naylor, Naud, Keefe, & Helzer, 2010; Nicholas et al., 2013; Otis et al., 2013; Pigeon et al., 2012; Thorn et al., 2011; Vitiello et al., 2013; Zachariades, 2012) may have influenced the findings of these studies. For example, a negative trial authored by Chiauzzi et al. (2010) had a higher dropout rate in the CBT intervention group than in the control group, which may have decreased the statistical validity of the analyses. Future research designed to overcome limitations such as these are necessary to further assess the efficacy of CBT for pain intensity.
The IMMPACT guidelines recommend assessing pain intensity together with several other variables—physical functioning, emotional functioning, treatment satisfaction, and participant ratings of global improvement (Dworkin et al., 2005). Pain intensity, physical function, and depression were studied in over 75% of the trials. However, anxiety, quality of life, sleep disturbance, treatment satisfaction, global impression of change, and fatigue were all studied in less than 50% of the trials. Measuring the core IMMPACT domains in chronic pain in future trials may allow for the comparison of outcomes across trials, allow the pooling of data from different trials, and lead to the identification of optimal measures for these domains (Dworkin et al., 2005). Most importantly, inclusion of multiple IMMPACT-recommend outcome measures in future studies will allow researchers to describe CBT’s multifaceted benefits.
Furthermore, regarding IMMPACT variables, sleep, fatigue, depression, and anxiety improved in over 50% of the studies testing these variables. Perhaps there are specific pain-related variables that mediate improvements in pain intensity following CBT treatment in different pain populations. For example, a study conducted by McCracken, Gross, and Eccleston (2002) identified that improvements in pain intensity, pain interference, and depression were mediated by improvements in pain-related anxiety in individuals with chronic low back pain receiving CBT. As sleep, fatigue, depression, and anxiety significantly improved in a majority of the studies, perhaps these pain-related variables are ideal candidates to be targeted in future CBT interventions as mediators of pain intensity. For instance, pain intensity and anxiety both significantly improved following a 12-week group CBT intervention (Vibe Fersum et al., 2013). Similarly, pain intensity, anxiety, and fatigue all significantly improved after individuals with fibromyalgia engaged in a 10-week group CBT intervention (van Koulil et al., 2010). The identification of chronic pain mediators may help tailor specific CBT interventions and strategies for specific pain-related variables to ultimately improve pain intensity in individuals with chronic pain and increase the availability of limited CBT resources.
In terms of the lasting effects of CBT, 73% and 36% of the studies that evaluated outcomes at a 6-month follow-up period demonstrated sustained improvements in IMMPACT/Primary and pain intensity outcomes, respectively. Six studies were designed to evaluate the lasting effects of CBT at 12 months follow-up. Results demonstrated that over 67% and 50% of these studies revealed significant effects on IMMPACT/Primary outcomes and pain intensity, respectively. These findings are consistent with the Cochrane review published by A. C. Williams and colleagues (2012) which demonstrated that CBT had no significant effects on pain intensity 6 to 12 months post-treatment, but had a small and moderate effect on mood and catastrophizing 6 to 12 months post-treatment compared with treatment as usual. Overall, the results of this current review suggest that the benefits of CBT may extend at least 6 months from the start of therapy, but more studies are needed exploring whether effects can be sustained long term, and what types of maintenance programs may be required to maintain effects for improvements in pain intensity over time.
The strategies of the CBT interventions varied widely across studies. There were six studies designed to compare CBT treatment strategies (Castel, Cascón, Padrol, Sala, & Rull, 2012; Glombiewski et al., 2010; Liedl et al., 2011; McBeth et al., 2012; Pigeon et al., 2012; van Koulil et al., 2010), however, only three of these studies (Castel et al., 2012; Glombiewski et al., 2010; Liedl et al., 2011) compared CBT treatment strategies directly against one another. For example, a trial conducted by Castel et al. (2012) demonstrated that CBT (strategies included pain education, cognitive restructuring, sleep hygiene, assertiveness training, and activity pacing) plus hypnosis was superior in improving pain intensity and psychological distress compared with CBT alone in individuals with fibromyalgia. However, while not included in this review because the study did not contain a treatment as usual control group, a study conducted by Kerns et al. (2014) compared tailored individual CBT (used motivational enhancement strategies to encourage skill learning and practice) against standard individual CBT and found no significant differences in treatment adherence, pain intensity, physical function, or depression. Additional research is needed comparing CBT treatment strategies to determine whether a certain battery of strategies is most efficacious for individuals with chronic pain. The identification of optimal CBT strategies may lead to the development of a standard CBT protocol that can be tailored to specific chronic pain etiologies.
The limitations of this integrative review include the lack of a team approach to review and critically appraise the articles included in the study. Only the primary author reviewed the studies included in this review, thus increasing the risk of bias. It is also possible that we failed to find key studies testing CBT interventions for chronic pain. However, consistent key terms and limits were used to search each of the five databases (Electronic Supplementary Table 1). Last, limiting our search to papers published from 2009 to 2015 may have resulted in the exclusion of key papers that if included in this review, may have changed the scope of our findings.
In conclusion, this integrative review examined which CBT intervention characteristics and outcome variables have been explored in recent randomized controlled trials, and in which chronic pain populations. The results of this review demonstrated that CBT was effective for pain intensity in 43% of the trials and was an effective treatment for many pain-related variables recommended by IMMPACT such as physical functioning, anxiety, depression, and quality of life. Future research is needed to refine a standardized CBT dose and to test CBT interventions in understudied chronic pain populations such as military veterans and individuals with cancer treatment–related chronic pain. Furthermore, CBT-OL was shown to be particularly promising alternative to traditional CBT because the online delivery format was comparable with in-person CBT delivery methods for improving pain and pain-related symptoms. A logical next step based on the results of this review is to test a CBT-OL intervention in individuals with cancer treatment–related chronic pain or military veterans. If effective, CBT-OL could be further tested in combination with pharmacological interventions to improve pain and quality of life.
Footnotes
Acknowledgements
The authors thank Barbara Brush, PhD, ANP-BC, FAAN, and Debora Lauseng, Assistant Director, Academic and Clinical Engagement, Taubman Health Sciences Library, for their help with the literature search.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.