
Abstract
Sleep disturbance is common in patients with heart failure and their family caregivers. The purpose of this study was to determine whether sleep disturbances of patients and their spousal caregivers predicted their own and their partners’ quality of life (QoL) in 78 heart failure patient–spousal caregiver dyads. Sleep disturbance was assessed using a composite score of four common sleep complaints. QoL was assessed by the physical and mental well-being subscales of the Short-Form 12 Health Survey. The multilevel dyadic actor–partner interdependence model analysis was used to determine the association between sleep disturbance and QoL. Each individual’s sleep disturbance predicted their own poor physical and mental well-being while spousal caregivers’ sleep disturbance predicted their partners’ mental well-being. Results indicated that patients’ mental well-being is sensitive to their spouses’ sleep disturbance. Interventions targeting improving sleep and QoL may have to include both patients and spousal caregivers.
Heart failure (HF) is a chronic disorder that requires lifelong management. Approximately 5.7 million Americans aged 20 years or older have HF, and the prevalence rate is expected to increase (Mozaffarian et al., 2016). Sleep disturbance, defined as having problems in either the qualitative aspects of sleep such as restfulness of sleep or in the quantitative aspect of sleep such as time taken to fall asleep and duration of sleep (Cohen, Menefee, Doghramji, Anderson, & Frank, 2000), is common in patients with HF. Among patients with HF, 44% reported having restless sleep, 41% had trouble falling asleep, 39% had early awakening, and 32% had trouble returning to sleep (Erickson, Westlake, Dracup, Woo, & Hage, 2003). In addition, sleep-disordered breathing (such as obstructive and central sleep apneas) occurs in 45% to 82% of patients with HF (Broström & Johansson, 2005). Family caregivers of patients with HF also reported changes in their sleep (e.g., midnight awakening and difficulty in returning to sleep after awakening) and sleeping arrangements (e.g., sleeping in a separate bed as patients need to sleep in upright position) related to their partners’ HF (Broström, Strömberg, Dahlström, & Fridlund, 2003). Anxiety related to their loved one’s HF and associated symptoms of dyspnea, apnea, snoring, coughing, and nocturia were reasons reported by caregivers for their disturbed sleep (Broström et al., 2003).
Sleep Disturbances and Quality of Life (QoL)
Sleep disturbances have been shown to be associated with poor QoL in general population (Baldwin et al., 2001), patients with HF (Johansson et al., 2010; Liu, Hung, Shyu, & Tsai, 2011; Manocchia, Keller, & Ware, 2001; Redeker & Hilkert, 2005), and in caregivers of patients with other conditions (Creese, Bédard, Brazil, & Chambers, 2008; Pawl, Lee, Clark, & Sherwood, 2013), The relationship has not been examined in caregivers of patients with HF. In addition, this relationship has never been examined with respect to the interdependence between individuals with close relationships such as patients and spousal caregivers.
The Interdependence Theory holds that interactions between individuals in a close relationship have an effect on their respective partners’ outcomes (Kelley & Thibaut, 1978). This suggests that individuals’ emotions, cognition, and behavior influence their partners’ as well as their own outcomes. Thus, it is important to examine the relationship between sleep and QoL in the context of both the patients and their caregiving partners (Rayens & Svavarsdottir, 2003). We predict that sleep disturbance in one partner will affect the QoL of the other partner.
Researchers in two studies examined the relationship between sleep and QoL (Read, Simonds, Kinali, Muntoni, & Garralda, 2010; Strawbridge, Shema, & Roberts, 2004). In the study by Read et al. (2010), the interdependence between the partners’ characteristics was not considered, the sample size was very small (10 dyads), participants had patient–parent relationships, and only correlational analysis was conducted (Read et al., 2010). In the study by Strawbridge et al. (2004), the analyses only accounted for the correlations between individual members’ characteristics. In this study of 405 couples, Strawbridge et al. reported that sleep problems in one partner predicted poor physical and mental health in their own as well as some aspects of their partners’ physical and mental health. In both of these studies, the assumptions of interdependence were not considered and the results do not fully reflect the effects of sleep disturbance on QoL (Kenny, Kashy, & Cook, 2006).
Dyadic analysis is the most appropriate approach for the study of individuals with a close relationship such as patient–caregiver. This approach accounts for the interdependence between dyad members and allows researchers to examine how the interdependence between individual members affects the outcomes at the dyadic level (McCarthy, Lyons, & Powers, 2011). Dyadic analysis can be used to investigate the influences of characteristics of each member of the dyad on his or her own and partner outcomes (Rayens & Svavarsdottir, 2003). No study has examined the association between sleep disturbance and QoL in individuals with interdependent relationships at dyad level.
Purpose
The purpose of this study was to examine whether individuals’ sleep disturbance predicted their own, as well as their partners’ QoL in HF patient–spousal caregiver dyads using the actor–partner interdependence model (APIM) dyadic analysis approach.
Method
Design, Sample, and Setting
This was a secondary analysis of cross-sectional data from a longitudinal study designed to determine the impact of family caregivers’ emotional distress on QoL, rehospitalization related to HF, and mortality in patients with HF (Chung, Pressler, Dunbar, Lennie, & Moser, 2010). The parent study included stable patients (consistent doses of HF medications for previous 3 months) with a confirmed diagnosis of chronic HF and their family caregivers. Patients 18 years or older who were able to read, write, and speak English were referred by nurses and physicians from outpatient clinics affiliated with two community hospitals and an academic medical center in Central Kentucky. The following are the inclusion criteria for patients: (a) not receiving active treatment for cancer; (b) no history of acute myocardial infarction or hospital admission in the prior 3 months; (c) no terminal illness or cognitive impairment; and (d) not referred for heart transplantation. In the parent study, caregivers were family members or significant others who provided care to eligible patients. Caregivers could not have (a) cognitive impairment, (b) HF, (c) cancer, (d) dementia or Alzheimer’s disease, or (5) terminal illnesses or any other major comorbid condition.
In the parent study, 143 patient–caregiver dyads completed the baseline assessment (Chung et al., 2010). In this article, we included 78 patient–spouse dyads who had no missing data on the main study variables of sleep disturbance and QoL.
Procedures
Approval from the institutional review board was obtained prior to data collection. Researchers approached eligible patients and caregivers either in the outpatient clinics or by phone. Patients had to identify their primary family caregivers. After screening eligibility of patients and their caregivers, the informed consent was obtained. Participants were asked to complete survey questionnaires of the study variables. Health conditions and demographic data (such as age, sex, and marital status) were collected. In addition, a research nurse obtained clinical information from participants using structured questionnaire, brief interview, and by reviewing patients’ medical charts.
Measures
Sleep disturbance
Because there was no standardized measure of sleep disturbance in the primary dataset, sleep disturbance score was computed from four common complaints related to sleep for this analysis: (a) changes in sleep pattern; (b) difficulty in sleeping; (c) frequency of trouble falling asleep, staying asleep, or sleeping too much; and (d) problems with restfulness of sleep. The items were selected because they reflect common aspects of disturbed sleep in patients and caregivers (Erickson et al., 2003; McCurry & Teri, 1996) and are common aspects assessed in sleep disturbance scales (Allen, Kosinski, Hill-Zabala, & Calloway, 2009; Hays, Martin, Sesti, & Spritzer, 2005; Lee, 1992).
The first item, change in sleep pattern was selected from the Beck Depression Inventory II (BDI-II) that is rated 0 to 6 on a Likert-type scale. Responses of “0,” “1 and 2,” “3 and 4,” and “5 and 6” were recoded, respectively, as 0, 1, 2, and 3 by following the BDI-II score coding. This recoded 4-point rating was converted to 0 to 100 scale as 0, 33.33, 66.66, and 100, respectively. The second item, difficulty sleeping because of HF was selected from the Minnesota Living with Heart Failure Questionnaire (MLHFQ). For spouses, a modified version of the MLHFQ was used. This item in spouses’ version asked whether they have difficulty in sleeping because of their partner’s HF. This item was rated on a scale of 0 (no difficulty) to 5 (very much difficulty), and responses were given composite scores of 0, 20, 40, 60, 80, and 100, respectively. The third item, having trouble falling asleep, staying asleep, or sleeping too much was selected from the Patient Health Questionnaire–9 (PHQ-9) and rated on a 4-point scale from 0 (not at all) to 3 (nearly every day). Responses converted into composite scores in the same manner as the first item. The fourth item asked about restfulness of sleep and was rated on 3-point Likert-type scale from 1 (very rested) to 3 (not rested at all). This item was developed by the primary investigator to assess sleep disturbance related to uninterrupted sleeping hours and taking a nap during the day. The responses for this item were recoded into composite scores of 0, 50, and 100, respectively.
The four item scores were averaged to achieve a total score that ranged between 0 and 100. Higher scores indicated higher level of sleep disturbance. The Cronbach’s alpha for reliability of the sleep disturbance scale was .76 for patients and .74 for spouses. Item–item correlations for patients were significant and ranged between .36 and .63. Item–item correlations for caregivers ranged between .21 and .64. All caregivers’ item–item correlations were significant except for the correlation between Item 2 (difficulty in sleeping) and Item 4 (restfulness of sleep). The item–item correlations without the correlation between Items 2 and 4 ranged between .47 and .64.
QoL
QoL was measured using the Short-Form 12 Health Survey (SF-12). The SF-12 is a short form of a validated generic QoL measure, the Medical Outcome Study health survey short form SF-36 (Ware, Kosinski, & Keller, 1996), which measures individuals’ perceptions of general functional health and well-being. Two standardized scores are generated from the SF-12; the physical well-being and the mental well-being (Ware et al., 1996). The physical well-being reflects the physical QoL addressed by physical health, physical functioning, bodily pain, and role limitations affected by physical health while the mental well-being reflects the mental QoL addressed by mental health, vitality, social functioning, and role limitations affected by mental health (Ware et al., 1996). The possible range for the standardized scores is 0 to 100 with higher scores indicating better QoL (Lim & Fisher, 1999). In heart and stroke patients, the SF-12 had Cronbach’s reliability alpha of .84 and .81 for the physical and mental well-being subscales, respectively, and its construct validity by hypothesis testing was supported (Lim & Fisher, 1999). Also, it had good test–retest reliability of .89 for physical well-being and .76 for the mental well-being among adults (Ware et al., 1996).
Data Analysis
All data analyses were performed using the Statistical Package for the Social Sciences Version 21 (SPSS Inc.®, Chicago, IL). A priori .05 alpha level was chosen as significance level. Descriptive statistics, including frequency distributions, means, and standard deviations, were calculated as appropriate to the level of measurement of the variables. Paired sample t test and chi-square test were used to compare patients and spouses in regard to their socio-demographic and study variables as appropriate to describe sample characteristics and to compare between included and excluded patients in terms of age, sex, and New York Heart Association functional class of patients. Pearson’s product–moment correlation was used to examine the correlations among variables of sleep disturbance, physical well-being, and mental well-being within patients and spouses. To conduct dyadic analysis, individual data were restructured into pairwise data, and grand mean scores and Z scores were created. The APIM with distinguishable dyads analyses were conducted for outcome of physical and mental well-being with sleep disturbance as predictor. The APIM allowed the examination of the effect of sleep disturbance of each member of the dyad on the aspects of QoL in both dyad members (Kenny et al., 2006). In the APIM, “the actor effect” was the individuals’ sleep disturbance prediction of their QoL, while “the partner effect” was the individuals sleep disturbance prediction of their partners’ QoL (Kenny et al., 2006).
Results
Characteristics of Patient–Spousal Caregiver Dyads
Seventy-eight patient–spousal caregiver dyads out of the 143 dyads in the parent study were included in this analysis. Comparison of the included versus excluded patients indicated there was no differences in age (62.2 ± 12.4 vs. 59.9 ± 12.6 years, p = .26) but there were more female patients (53.8% vs. 25.6%, p = .001) and more patients in New York Heart Association functional Classes III and IV (66.1% vs. 44.9%, p = .02) in the excluded patients than in the included patients. Among spouses, there was no significant difference in percentage of female spousal caregivers (74.4% vs. 75.8%, p = 1.0) between included and excluded spouses. However, caregivers included in the analysis were significantly older than the excluded caregivers (59.5 ± 12.3 years vs. 52.1 ± 15.9 years, p = .002).
Characteristics of patients and spousal caregivers are presented in Table.1. The mean age for the 78 dyads was 62.2 years (±12.4) for patients and 59.5 years (±12.3) for spouses. The majority of patients and spouses were Caucasian and about half had no more than a high school education. Patients’ and spouses’ education level and ethnicity were similar. Hypertension was the most common comorbid condition in both patients and spouses but more common in patients (77.8% in patients and 44.7% in spouses, p < .001). Half of the patients were New York Heart Association were in functional Class III or IV.
Characteristics and Comparisons Between Patients (n = 78) and Their Spousal Caregivers (n = 78).
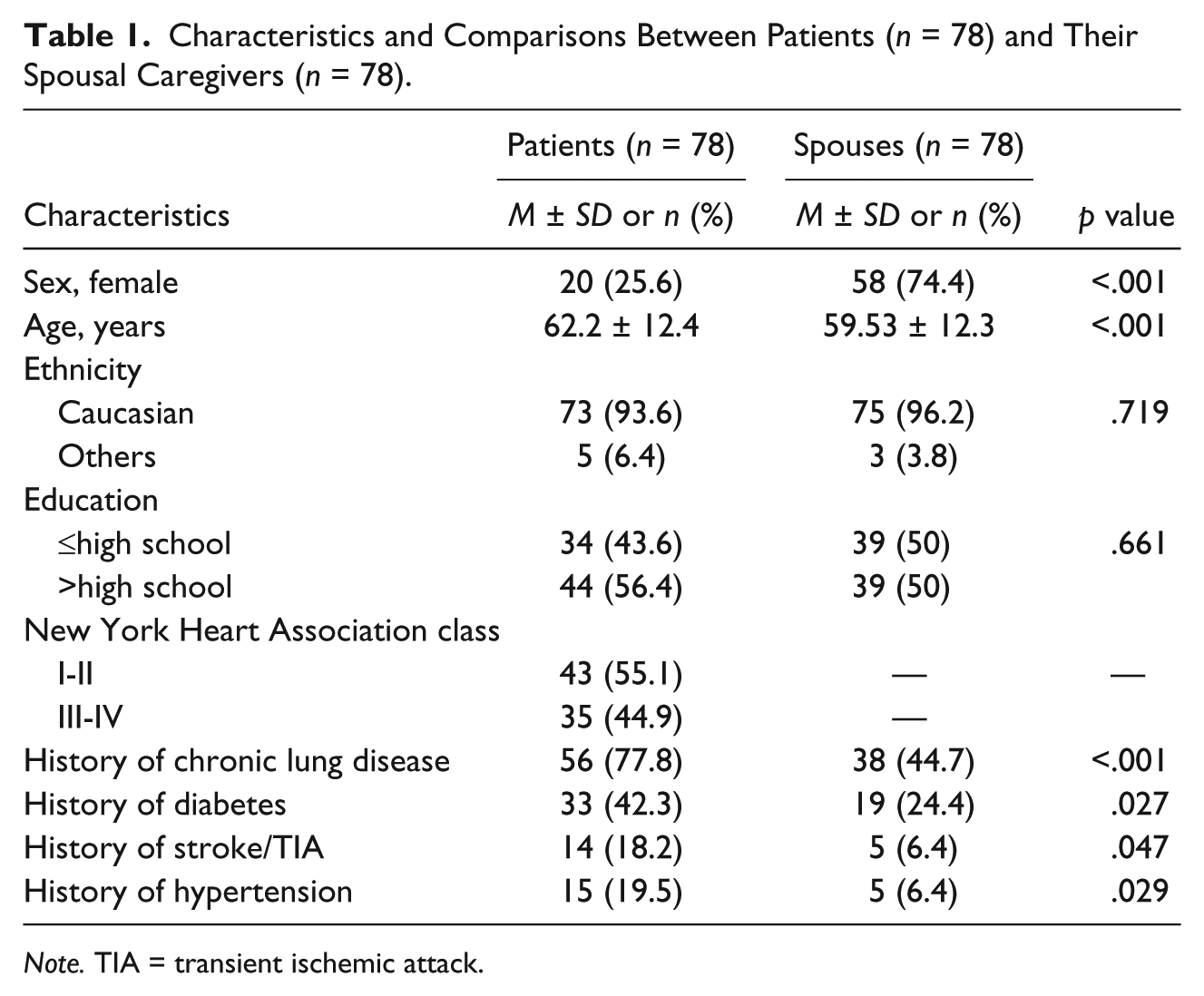
Note. TIA = transient ischemic attack.
Patients and their spouses had similar levels of sleep disturbance (Table 2). The mental well-being scores were similar between patients and spouses, but the physical well-being scores were significantly higher (better) in spouses (Table 2). Patients had mean physical well-being score of 35 with 92.3% of them having scores less than 50, which is considered poor. About 33% of patients had mental well-being scores less than 50. The percentage of spouses with scores less than 50 on physical and mental well-being were 62.8% and 33.3%, respectively. Physical well-being in spouses and mental well-being in both patients and spouses were considered moderately poor (slightly below the standard mean).
Comparisons Between Patients and Their Spousal Caregivers on Variables of Sleep Disturbance, Physical Well-Being, and Mental Well-Being.
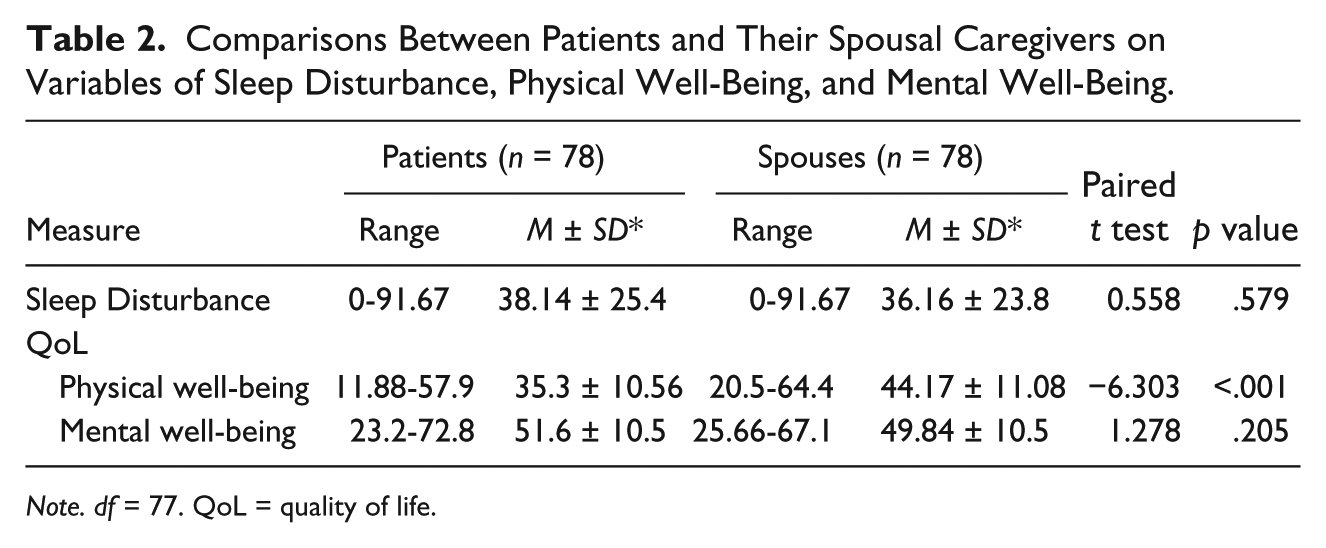
Note. df = 77. QoL = quality of life.
Sleep disturbance scores of patients and spouses were not significantly correlated (Table 3). Sleep disturbance in patients were significantly correlated with their physical well-being but not their mental well-being. Spouses’ sleep disturbance was significantly correlated with their own physical and mental well-being scores. There were no significant correlations between sleep disturbance scores of patients and spousal caregivers in regard to the spouses’ physical and mental well-being except that patients’ sleep disturbance was significantly correlated with spousal caregivers’ mental well-being (p < .01). Sleep disturbance scores were negatively correlated with age in spouses (r = −.220, p = .05) but not patients (r = −.203, p = .075).
Correlations Among Sleep Disturbance, Physical Well-Being, and Mental Well-Being in Patient–Spousal Caregiver Dyads.
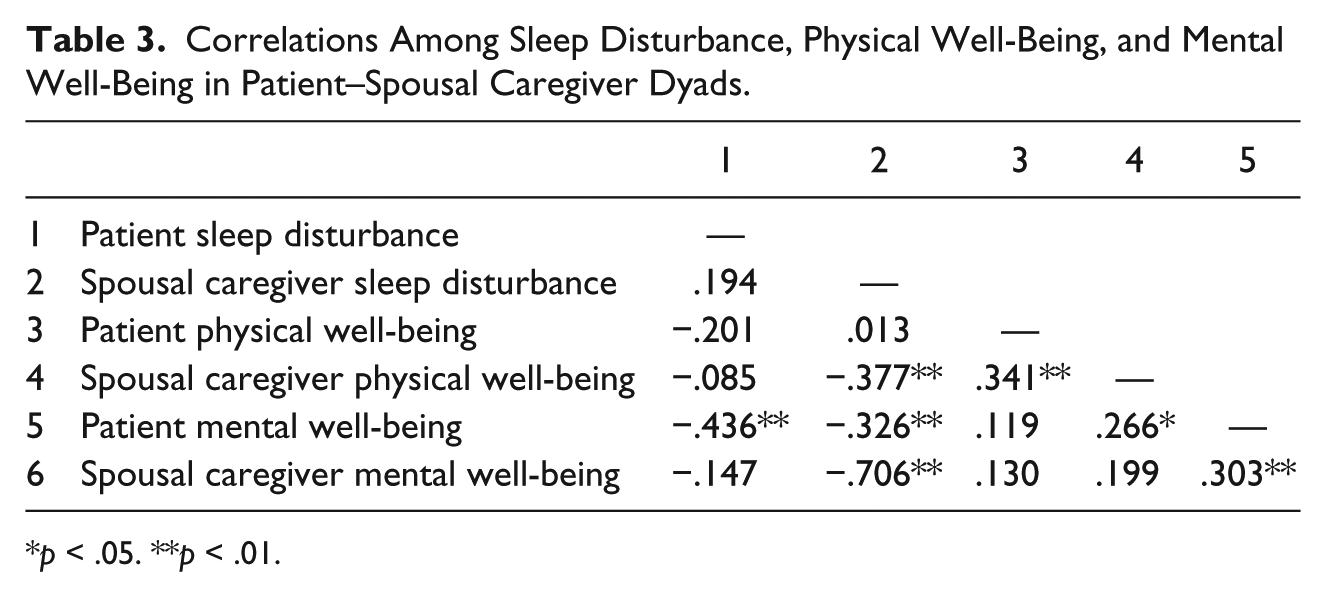
p < .05. **p < .01.
Association Between Sleep Disturbance and Physical Well-Being
Sleep disturbance exhibited only actor effects on physical well-being in both patients and spouses (Figure 1). This indicated that higher sleep disturbance in both patients and spouses predicted their own poor physical well-being. Sleep disturbance had no effect on the partner’s physical well-being in either patients or spouses (p values > .05).
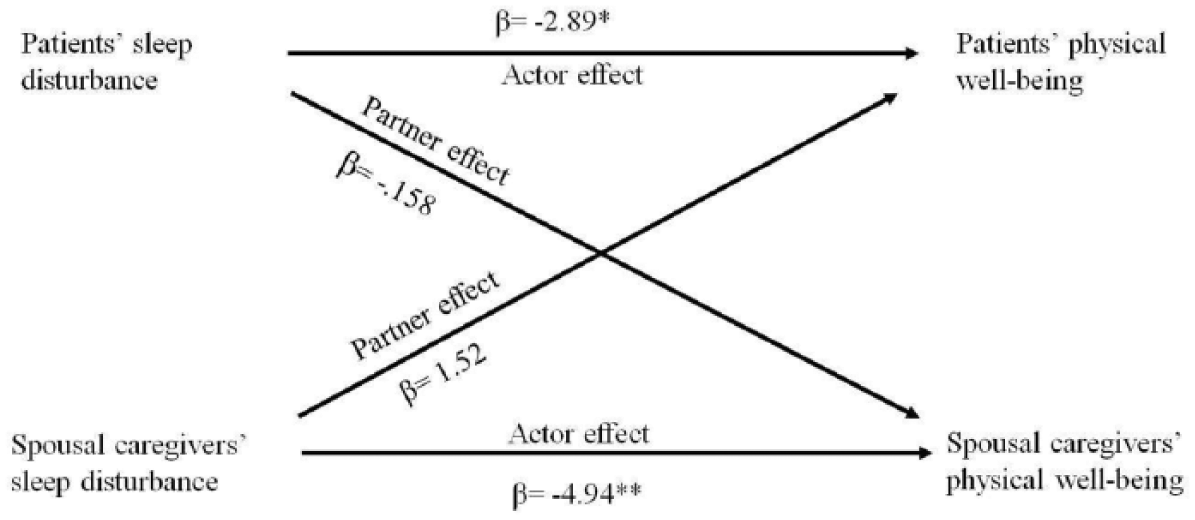
Sleep disturbance: The actor and partner effects as predictors of physical well-being using the actor–partner interdependence model with distinguishable dyads regression model.
Association Between Seep Disturbance and Mental Well-Being
Patient’s and spousal caregiver’s sleep disturbance exhibited an actor effect on mental well-being (Figure 2) meaning a high level of sleep disturbance predicted their own poor mental well-being. Patients’ sleep disturbance did not exhibit partner effects on spouses’ mental well-being (p = .451). For spouses, we found a significant partner effect of sleep disturbance on mental well-being. This indicates that patients whose spouse has higher sleep disturbance have poorer mental well-being.
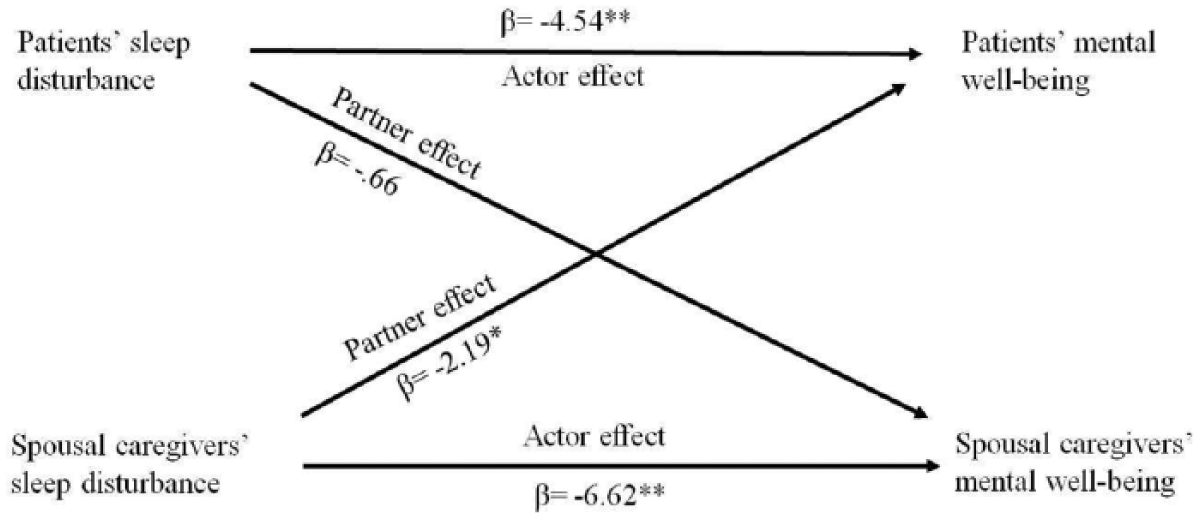
Sleep disturbance: The actor and partner effects as predictors of mental well-being using the actor–partner interdependence model with distinguishable dyads regression model.
Discussion
Using the APIM dyadic analysis, we found that sleep disturbance in patients and their spousal caregivers had negative association with their own physical and mental well-being aspects of QoL. As sleep disturbance increased, an individual’s own physical and mental well-being tended to be poorer. This finding is consistent with the results of previous studies of similar-aged married couples (Strawbridge et al., 2004) and in individual patients with HF (Johansson et al., 2010; Liu et al., 2011; Manocchia et al., 2001; Redeker & Hilkert, 2005). Strawbridge and colleagues (2004) found that sleep disturbances put individuals at risk for having poor physical and mental health. Likewise, Manocchia and colleagues (2001) in sample of 229 patients with HF found significant differences in all aspects of QoL using the SF-36 between patients with and patients without sleep problems. Subjectively measured sleep in HF patients has shown strong associations with the physical and the mental well-being aspects of QoL (Liu et al., 2011). Similarly, Johansson et al. (2010) found that the physical well-being was predicted by having difficulties in maintaining sleep and that the mental well-being was predicted by non-restful sleep. The association was also consistently found in caregivers of patients with breast cancer (Chang, Tsai, Chang, & Tsao, 2007), malignant brain tumors (Pawl et al., 2013), and Alzheimer diseases (Creese et al., 2008). In these studies, poor sleep scores were negatively correlated with overall QoL (Chang et al., 2007; Pawl et al., 2013) and with the physical and mental well-being aspects of QoL (Creese et al., 2008).
This relationship was also evident in a study by Redeker and Hilkert (2005) who objectively measured sleep duration and continuity using an electronic accelerometer (i.e., Actiwatch actigraph) in 61 patients with stable HF with reduced ejection fraction. They found that total awakening time after sleep onset was a significant predictor of physical function (i.e., SF-36) after controlling for covariates of age, gender, comorbidity, and New York Heart Association class and the duration of awakening bouts after the onset of sleep was significantly associated with the mental well-being.
There is no clear understanding of the mechanisms underlying how sleep disturbance affects QoL at individual level but sleep disturbance is known to be associated with fatigue (Broström, Strömberg, Dahlström, & Fridlund, 2001) and inadequate self-care behavior (Riegel, Dickson, Goldberg, & Deatrick, 2007) that may influence the QoL. Riegel and Weaver (2009) proposed that the effect of sleep disturbance on QoL is mainly through the effect on individuals’ cognitive abilities that in turn affect self-care and finally the QoL (Riegel & Weaver, 2009).
In the patient–spouse dyad, we found that individual’s sleep disturbance was not associated with their partner’s physical well-being. The physical well-being findings indicate that patients and spouses shown to be actor oriented (i.e., possessed only actor effect, (Kenny & Cook, 1999)) as their physical well-being was influenced by their sleep disturbance but not by their partners’ sleep disturbance.
An important finding of this study was that spousal caregivers’ sleep disturbance was negatively associated with patients’ mental well-being while sleep disturbance in patients had no association with spouses’ mental well-being. In the mental well-being analysis, spouses shown to be actor oriented (i.e., possessed only actor effect; Kenny & Cook, 1999). Patients were shown to be couple oriented as their mental well-being was influenced by their sleep disturbance as well as their spousal caregivers sleep disturbance (Kenny & Cook, 1999).
Consistent with our study, Strawbridge et al. (2004) found that spousal sleep problems put the partner at risk for having poor mental health. The odds ratio (OR) was 1.15 for having depressed mood if the spouse had sleep problems and 1.23 for poor or fair mental health. In physical health, spouses’ sleep problems were not significantly associated with partner feelings of having less energy than others on the similar age or feelings of being physically disabled. Contrary to our study, they reported that spouses’ sleeping problems were associated with the partner reporting fair or poor health. In that study, physical health was measured by a one item self-rating of general health not specifically the physical health. Thus, ratings may reflect all aspects of the health, not only the physical.
This is the first study to examine relationships at dyad level and was not designed to identify the mechanism by which sleep disturbance in the spouses may affect the patients’ mental well-being aspect of QoL. However, one potential hypothesis is that sleep disturbance decreases the ability of spousal caregivers to support their ill family member especially to provide psychological support.
Our study had many strengths including that it was the first study to examine the relationship between sleep disturbance and QoL at dyad level using the APIM dyadic approach. However, the study has some limitations. First, although we created a sleep disturbance score using multiple aspects of sleep disturbance and provided some reliability testing, it was not a well-established measure of sleep disturbance. Second, several aspects of sample may limit the conclusions that can be drawn. While the sample was patient-spousal caregiver dyads living in the same home, it was unknown whether patients and spouses slept together. The sample consisted of community-dwelling patients with stable HF, and the majority were Caucasian. Additional research is needed with a broader sample of patient–caregiver dyads. Third, this was a cross-sectional study which prevents the establishment of the causality in these relationships. Finally, other variables such as age, depression, anxiety, caregiving burden, and quality of patient–spouse relationship that may have associations with QoL were not controlled in the analyses. Future studies should consider how these variables influence the relationships between sleep disturbances and QoL.
Several implications can be derived from the findings of this study. It provided more evidence that patients and their spousal caregivers have interdependent relationships that influence each other’s outcomes. In this respect, health care professionals should assess for sleep disturbance in both patients and their spouses. Implications for research include the need to focus on a dyadic approach to QoL in patients with HF and their spousal caregivers. In addition, studies are needed on the long-term effects of sleep disturbance on dyads’ outcomes. Furthermore, studies are needed to determine why patients’, but not spousal caregivers’, mental well-being was sensitive to their partners’ sleep disturbance.
This study demonstrated the interdependence between patients with HF and their spousal caregivers sleep disturbance on outcomes. In this study, the actor effect of sleep disturbance in members of the dyad on their physical and mental well-being was evident. In addition, sleep disturbance in spousal caregivers exhibited partner effect on mental well-being of patients. These findings suggest that patients with HF would gain more benefit from dyad-focused interventions that provide equal attention to the caregiver as a mean of improving physical and the mental well-being.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH) or the National Institute of Nursing Research (NINR). This work is submitted to the Graduate School at University of Kentucky in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Nursing from the College of Nursing.
Declaration of Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Kentucky, College of Nursing Faculty Research Support Grant (Chung, M. L., principal investigator [PI]); NIH/NINR (1K23NR010011-01, Chung, M. L., PI); and NIH/NINR (1P20NR010679, Moser, D. K., PI and P-20 Center director).