
Abstract
Childhood obesity is a serious health issue, associated with medical comorbidity and psychosocial impairment that can persist into adulthood. In the United States, youth with intellectual and developmental disabilities are more likely to be obese than youth without disabilities. A large body of evidence supports the efficacy of family-based treatment of childhood obesity, including diet, physical activity, and behavior modification, but few interventions have been developed and evaluated specifically for this population. We highlight studies on treatment of obesity among youth with intellectual and developmental disabilities, including both residential/educational settings as well as outpatient/hospital settings. All interventions were delivered in-person, and further development of promising approaches and delivery via telenursing may increase access by youth and families. Nursing scientists can assume an important role in overcoming barriers to care for this vulnerable and underserved population.
In the United States, rates of obesity in children have more than doubled over the past 30 years (Ogden, Carroll, Kit, & Flegal, 2012, 2014). For youth between 2 and 19 years of age, the prevalence of obesity was 17% in 2011 and 2014 (Ogden et al., 2016). Obesity is a result of an energy imbalance in which excess calories are consumed and too few are expended over time, influenced by various genetic, environmental, and behavioral factors (Fiese & Jones, 2012; Kellou, Sandalinas, Copin, & Simon, 2014). Youth with obesity are more likely to have risk factors for cardiovascular disease, namely high blood pressure or high cholesterol (Dong, Wang, Wang, & Ma, 2015; Saner, Simonetti, Wühl, Mullis, & Janner, 2016), and as children with obesity grow into adolescence, they are at greater risk for prediabetes and diabetes (Centers for Disease Control and Prevention, 2011). In addition, youth with obesity are at risk for related health problems including sleep apnea and joint problems, as well as psychological challenges, namely poor self-esteem and stigmatization (Bazzano et al., 2016; Cornette, 2008; Halfon, Larson, & Slusser, 2013). The psychological toll of childhood obesity is substantial, and obesity has been reciprocally linked to anxiety and depression (Kalarchian & Marcus, 2012; Luppino et al., 2010; Puder & Munsch, 2010; Pulgarón, 2013; Vander Wal & Mitchell, 2011). Stigma linked to childhood obesity intensifies if obesity persists into adulthood, with obesity factoring into discriminatory practices in employment (Agerström & Rooth, 2011) and bias in health care settings (Puhl & Heuer, 2009). Taken together, the impact of these medical and psychosocial implications of childhood obesity should not be taken lightly.
Since the late 1970s, family-based approaches to treatment of childhood obesity have predominated (Epstein, Paluch, Roemmich, & Beecher, 2007; Sung-Chan, Sung, Zhao, & Brownson, 2013), and research findings support their short- and longer-term efficacy (Berge & Everts, 2011; Epstein, Myers, Raynor, & Saelens, 1998; Hoelscher, Kirk, Ritchie, & Cunningham-Sabo, 2013; Jelalian & Saelens, 1999; Kalarchian et al., 2009). Family-based approaches include a focus on education, diet, physical activity, and behavior modification, targeting both the child and parent for behavior change. Parental involvement is associated with weight loss in children, and studies suggest that use of a wide range of behavior change techniques improves weight outcomes (McLean, Griffin, Toney, & Hardeman, 2003). Furthermore, there is support for working exclusively with the parent for child weight management. Research has shown that targeting parents only was superior to targeting parents and children (Golan & Crow, 2004; Golan, Kaufman, & Shahar, 2006), whereas other studies have yielded comparable results for approaches that do and do not target children (Boutelle, Cafri, & Crow, 2011; Janicke et al., 2008).
Despite evidence suggesting increased prevalence of obesity among people with disabilities (Mikulovic et al., 2011; Weil et al., 2002), surprisingly little attention has been paid to treatment of obesity among youth with disabilities (Maïano, Normand, Aimé, & Bégarie, 2014). Furthermore, some genetic conditions associated with intellectual and developmental disabilities, such as Down syndrome and Prader–Willi syndrome, include overeating and weight gain as associated characteristics (Must et al., 2014). In the present report, we review select interventions targeting weight and healthy eating among youth with disabilities. Disabilities are broadly conceptualized to include a range of physical, mental, and behavioral impairments, which we refer to collectively as intellectual and developmental disabilities.
The studies reviewed here suggest that evidence-based strategies can be adapted to address eating and weight among youth with intellectual and developmental disabilities. Moreover, given the challenges of attending in-person and potential burden of travel for families, we assert that these tailored interventions can be effectively delivered to parents via telehealth. An approach increasing in acceptance and popularity, telehealth is the use of telecommunications (including telephone, Internet, text-messaging, and video conferencing technologies) to provide medical information and care. We contend that there is an emerging role for telenursing in treatment of obesity in this vulnerable and underserved population.
Obesity Among Youth With Intellectual and Developmental Disabilities
Some researchers have called attention to a dearth of studies investigating obesity among children with disabilities (Fleming et al., 2008; Grondhuis & Aman, 2014; Phillips et al., 2014; Slevin, Truesdale-Kennedy, McConkey, Livingstone, & Fleming, 2014). Nonetheless, population-level prevalence data suggest that obesity levels within this group are higher than in youth without intellectual and developmental disabilities. For example, using a nationally representative sample of 9,619 youth in the United States, a recent study found the prevalence of obesity among adolescents with autism and other learning and behavioral disabilities to be 20.4% compared with 13.1% among youth without these disabilities, a significant difference even after controlling for sociodemographic factors and birth weight (Phillips et al., 2014). Obesity was highest among the autism subgroup, and adolescents with either a developmental disability or obesity had a higher prevalence of common neurological, dermatological, gastrointestinal, and respiratory conditions/symptoms than adolescents without. Another nationally representative sample found prevalence of obesity in children with intellectual disabilities to be nearly twice the prevalence for those without, 28.9% as compared with 15.5% (Segal et al., 2016). After adjusting for age, sex, race/ethnicity, and poverty level, the prevalence remained significantly greater among children with intellectual disabilities. These studies suggest elevated rates of obesity among children and adolescents with disabilities relative to the general population. A recent systematic review and meta-analysis documented that adolescents with intellectual disabilities are 1.8 times more at risk for obesity than adolescents without, noting variations as a function of geographical region, recruitment setting, additional diagnoses, and definition of obesity (Maïano, Hue, Morin, & Moullec, 2016).
Maintaining a healthy weight may be particularly challenging for youth with intellectual and developmental disabilities whose capacity for self-management may be limited relative to those without disabilities. For example, less structured environments can pose challenges, as they may require a level of autonomy and decision-making skills that exceed developmental capabilities of youth in this population, particularly if they lack self-efficacy for healthy eating and physical activity (Curtin et al., 2013) or if their disability is associated with impaired satiety (e.g., Prader–Willi syndrome; Cassidy, 1997). Deficits in self-determination skills among adolescents and young adults with developmental disabilities may also adversely affect health-related choices (McGuire & McDonnell, 2008).
Youth with intellectual disabilities may be less likely to engage in physical activity (Salaun & Berthouze-Aranda, 2012) and may also have less access to environments in which physical activity is encouraged (Chen, Kim, Houtrow, & Newacheck, 2010). Furthermore, characteristics of certain developmental disabilities—namely poor motor control, need for supervision, poor social skills, and difficulty learning—have been linked to less time spent engaged in physical activity (Must, Phillips, Curtin, & Bandini, 2015). In a study comparing 38 adolescents with intellectual disabilities to 60 without, fewer adolescents with disabilities reported that they have someone with whom to engage in physical activity and fewer believed that activity would be good for their health, whereas more perceived that physical activities were too hard to learn and more reported a dislike of individual physical activities, relative to adolescents without (Stanish et al., 2016).
Many youth with intellectual and developmental disabilities experience medication-related weight gain, which can also contribute to the onset or exacerbation of obesity. Psychotropic medications such as antipsychotics, antidepressants, and anticonvulsants are often prescribed to treat comorbid psychiatric and behavioral disorders. Psychotropic medications are rarely weight neutral, often altering appetite, changing food preferences, or slowing metabolism (Correll, 2007). For example, clozapine, an atypical antipsychotic used to treat aggression, depression, and anxiety, poses risk for weight gain (Gressier, Porcelli, Calati, & Serretti, 2016). Other commonly prescribed atypical antipsychotics include olanzapine and quetiapine, and both are also associated with risk of weight gain (Martínez-Ortega et al., 2013). Antidepressant (Serretti & Mandelli, 2010) and anticonvulsant medications (Tanamachi et al., 2015; Wirrell, 2003) have been associated with weight gain as well.
Finally, caregivers play a key role in managing child eating and weight, and the challenge of “comparative severity” may be a factor in approaches to weight management among youth with disabilities (Grondhuis & Aman, 2014). For example, when already tackling the behavioral challenges of autism in the context of family life, parents may be relatively less likely to consider obesity a priority area. Moreover, some parents may be unaware of the serious, long-term consequences of obesity and may feel guilt over preventing a child with a disability from enjoying a pleasurable food (Rimmer, Rowland, & Yamaki, 2007).
Clearly, youth with intellectual and developmental disabilities constitute a distinctive subgroup of the obese population. Some unique considerations may be specific to the disability, such as the physical, behavioral, and/or mental impairments associated with the condition; potential need for increased environmental supports to facilitate healthy eating and activity; and medication-related weight gain. Others factors, such as diet, physical activity, behavior modification, and parenting, are important in treating all youth with obesity, but become even more salient for youth with intellectual and developmental disabilities.
Treatment of Obesity Among Youth With Disabilities
The complexities of disability may interact with and compound the challenges of addressing obesity in youth (Grondhuis & Aman, 2014; Rimmer, Yamaki, Davis, Wang, & Vogel, 2011). For example, Modell and Valdez (2002) call for more focused supervision and teaching when engaging children with intellectual disabilities in a behavioral intervention due to reduced intellectual and communication abilities. Although the literature is limited for youth with disabilities, a systematic review suggests that a combination of techniques (e.g., nutrition education, diet, physical activity) may be most effective in targeting weight loss for youth with intellectual disabilities (Maïano et al., 2014).
Below, we describe exemplar interventions that have been developed and evaluated specifically for managing weight and eating among youth with intellectual and developmental disabilities. Given the dearth of published literature in this population, we aim to highlight examples of effective interventions to stimulate further research. Our inclusion criteria were that the intervention incorporated diet (as opposed to physical activity only) and was delivered to a population of youth with intellectual or developmental disabilities. We describe studies conducted in residential/educational settings before presenting interventions delivered in outpatient/hospital settings (see Table 1 for overview of studies).
Select Intervention Studies for Treatment of Weight and Eating Among Youth Within Intellectual and Developmental Disabilities.
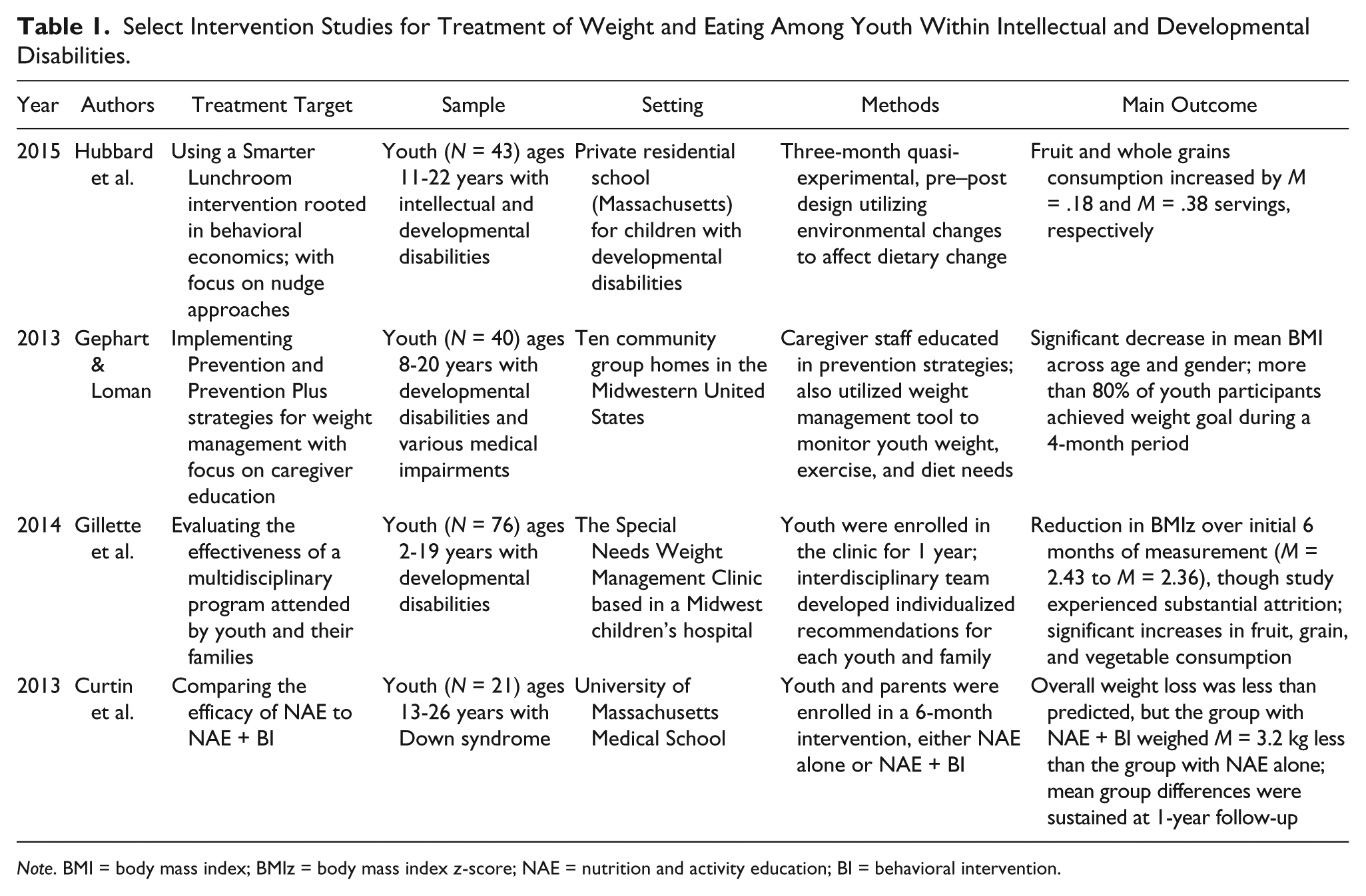
Note. BMI = body mass index; BMIz = body mass index z-score; NAE = nutrition and activity education; BI = behavioral intervention.
Children and adolescents with developmental disabilities who live in residential schools and group homes may be at particular risk of overeating and weight gain if the environment does not adequately support healthy eating. Hubbard and colleagues (2015) investigated the impact of a Smarter Lunchroom intervention, rooted in behavioral economics, for 43 youth aged 11 to 22 years with obesity and developmental disabilities living in a residential school. The 7-month study incorporated specific modifications for this population, including explaining the menu items using pictures and preparing the cafeteria environment using stories which describe situations in advance to improve behavioral response. The intervention also capitalized on the cafeteria environment to encourage changes through “nudging,” which encourages autonomy and choice among participants, rather than a forced menu change. For example, fruits were made easy to access and arranged attractively on the serving line, whereas peanut butter and jelly sandwiches were hidden and available only after consideration of the entrees offered on the menu. From pre- to post-intervention, children chose more whole grains and fruit while opting for fewer refined grains. These preliminary data suggest the efficacy of this approach for improving food selection and consumption choices for children with developmental disabilities. However, the effects of individual components of the intervention and the intervention impact on child weight status remain unknown.
While Hubbard et al. (2015) intervened in a residential school, Gephart and Loman (2013) evaluated strategies for weight management delivered to 40 youth aged 8 to 20 years with developmental disabilities living in group homes in a Midwestern educational/residential center. In a pre- to post-design, 48 staff caregivers were provided with weight management education, a communication tool for youth weight indices, weight and physical activity goals, dietary orders, and monthly follow-up communication. Youth were categorized based on body mass index (BMI) percentile (underweight [<5%], healthy weight [5%-84%, overweight [85%-94%], and obese [≥95%]), and results suggested that the intervention strategies were useful for weight management over a 4-month period. At post-intervention, more than 80% of the youth achieved their weight goal, with an overall decrease in weight status. However, this decrease was driven primarily from change in the healthy weight category, in which 96% of children met their goal to maintain their body mass index (BMI) percentile over the course of the study; this group also showed the largest overall decrease in BMI. Although an improvement in daily fruit consumption and vegetable consumption was documented, the investigators noted that parents and caregivers provided high-calorie snacks. Thus, results suggest that more intensive interventions may be needed for youth with developmental disabilities who are already obese, and highlights the need for educating both parents and caregivers.
Other investigators have focused on interventions delivered in an outpatient setting. Gillette and colleagues (2014) developed a hospital-based Special Needs Weight Management Clinic in which children and their families took part in a multidisciplinary treatment approach. Seventy-six children with special needs (e.g., autism, intellectual disabilities, Down syndrome, Prader–Willi syndrome) aged 2 to 19 years and their families met with an interdisciplinary treatment team, including a clinical child psychologist, nurse practitioner, dietitian, and occupational therapist, for an intake session and five follow-up sessions over a 12-month period. After the baseline assessment, the treatment team collaborated to develop behavioral and dietary recommendations tailored to each child and family. The program led to an increase in the variety of foods consumed by the child, as well as an increase of fruits and vegetables, as reported by parents. At the 6-month assessment, the intervention also resulted in a decrease in body mass index z-score (BMIz). There was, however, substantial withdrawal from the study over the first 6 months, with families often citing time or travel constraints as reasons for missing follow-up appointments. Thus, this study documents the promise of a tailored approach delivered on an outpatient basis while also highlighting potential challenges of clinic-based treatment.
Curtin and colleagues (2013) also conducted a study in an outpatient setting. Participants were 21 youth and young adults with Down syndrome (ages 13-26 years) who lived at home but hoped to transition to independent living. In a controlled design, families were randomized to a 6-month nutrition and activity education with or without parent behavioral intervention. The 16-session program was based in family-based behavioral intervention modified to address the unique cognitive needs of participants. The education component consisted of a nutrition program designed by a dietitian, which utilized pictures to enable diet planning and “coins” to facilitate understanding of discretionary calories. A physical therapist also evaluated the participants’ ability to complete required physical exercises, which were described for participants using illustrations and simple text. Parents assigned to the education with behavioral intervention condition also received instruction on behavior monitoring, positive reinforcement, goal setting, and modeling. At 6 months, mean body weight in the group receiving education plus behavioral intervention for parents was 3.2 kilograms lower than in the group that did not include parents, with differences sustained through 1-year follow-up. Positive changes in vegetable intake and activity were also observed. Strengths of this study include the randomized design documenting the importance of parent training and support over and above diet and physical activity education alone for youth and young adults with Down syndrome.
Considered together, these studies suggest that for youth with disabilities, the living environment and caregivers become particularly salient in overcoming the challenges to managing eating and weight. All interventions made specific adaptations to ensure intervention was accessible to children with intellectual and developmental disabilities. These included ensuring that protocols are easy to follow and understand, structuring the living environment to support healthy diet and lifestyle changes, and providing nutrition education for parents or caregivers. Indeed, individuals who lack training in weight management may be receptive to adaptations for youth with intellectual and developmental disabilities. For example, family-based behavioral obesity intervention has been recently adapted for pilot delivery among youth on second-generation antipsychotic medications with medically induced weight gain, a substantial proportion of whom had developmental disabilities (Nicol et al., 2016). Preliminary results suggest that the adaptations made to the content and delivery of the intervention not only positively impacted weight but also were rated with high satisfaction by participants.
It should be noted that the studies highlighted in Table 1 included relatively small, heterogeneous samples and included nonrandomized, uncontrolled designs. Thus, additional research using large, diversified samples in randomized, controlled studies is warranted to further evaluate adaptions to intervention content and delivery methods for behavioral treatment to address obesity in youth with intellectual and developmental disabilities. Moreover, many of the extant studies have been conducted in research settings, and the intensity of family-based behavioral intervention (often delivered in-person, weekly over a period of several months) and associated training may not be feasible or sustainable in routine care settings. Therefore, it is critical to identify models through which practitioners can deliver obesity intervention, and families of youth with disabilities can engage in such intervention. Expert committee guidelines outline the strong promise of pediatric primary care as a setting for obesity services, and nurses are well positioned to deliver the recommended screening and intervention approaches (Barton & U.S. Preventive Services Task Force, 2010; Oude Luttikhuis et al., 2009; Spear et al., 2007).
The Role of Nursing in Addressing Obesity
Nurses have been called to the front lines for prevention and treatment of childhood obesity (Berkowitz & Borchard, 2009) and can play an important role in advancing evidence-based care of youth with intellectual and developmental disabilities. Nurses are key health care providers for children in outpatient, inpatient, and residential settings, which can support continuity of care. Maintaining continuity of care is particularly important when considering the role of the nurse in establishing relational continuity, which provides the patient with a sense of predictability and consistency (Haggerty et al., 2003). In addition to guidelines for all pediatric primary care providers (Barton & U.S. Preventive Services Task Force, 2010; Oude Luttikhuis et al., 2009; Spear et al., 2007), nurses are encouraged to provide early identification, intervention, and continuity of care for youth with overweight or obesity (National Association of Pediatric Nurse Practitioners, 2009, 2015).
Despite these clear guidelines, however, studies of obesity service delivery indicate that evidence-based guidelines are rarely implemented and that primary care providers report barriers broadly related to training and implementation processes. For example, providers report concerns regarding inadequate skill levels for addressing obesity or lack of treatment options (Flower, Perrin, Viadro, & Ammerman, 2007; Holt et al., 2011; Klein et al., 2010; Rausch, Perito, & Hametz, 2011; Spivack, Swietlik, Alessandrini, & Faith, 2010). They also report need for greater training in weight-related counseling (Bleich, Bennett, Gudzune, & Cooper, 2012) and nutrition (Adams, Kohlmeier, & Zeisel, 2010), as well as tools for identifying and treating obesity (Block, DeSalvo, & Fisher, 2003; Forman-Hoffman, Little, & Wahls, 2006; Jay et al., 2008; Vetter, Herring, Sood, Shah, & Kalet, 2008). Additionally, providers report concerns with the amount of time associated with intervention delivery (Story et al., 2002). Notably, studies that involve training primary care providers to deliver a specific set of obesity-related recommendations suggest that focusing on a subset of care strategies may be deliverable and impactful in primary care settings (Jay et al., 2010).
Recent efforts with nursing students indicate that brief training can enhance their knowledge and skill in delivering screening and initial intervention for obesity among youth and families (Kolko et al., 2017). Given that nurses receive limited training in addressing behaviors among youth with disabilities, this could be incorporated into obesity-related education for nurses. For instance, monitoring, positive reinforcement, goal setting, and parenting strategies may be discussed in the context of youth with disabilities and may be helpful for addressing weight management in this population. In addition, given that training approaches are efficacious in live (i.e., in-person) and web-based methods (Kolko et al., 2017), incorporating technology may increase reach and scalability, and offers cost-effective opportunities to review and reengage with training materials (Miller, Sorensen, Selzer, & Brigham, 2006; Sholomskas et al., 2005).
Intervention Delivery via Telehealth
Telehealth may prove to be a cost-effective way to deliver interventions to this underserved population of youth and families. The Internet has been effectively utilized to deliver weight loss (Tate, Wing, & Winett, 2001) and maintenance interventions (Wing, Tate, Gorin, Raynor, & Fava, 2006), achieving comparable outcomes at a lower cost (Meenan et al., 2009). Email or text messages have also been demonstrated to be beneficial for weight loss (Shapiro et al., 2012) and have shown to be a successful medium for delivering care to an adolescent population as well (Sharifi et al., 2013; Smith, Kerr, Howie, & Straker, 2015). For example, a telehealth intervention utilizing a mobile ambulatory clinic has shown promise for an urban youth population (Slusser, Whitley, Izadpanah, Kim, & Ponturo, 2015). Indeed, a recent meta-analysis suggests the efficacy of telehealth interventions across a variety of technologies for the treatment of childhood obesity (Turner, Spruijt-Metz, Wen, & Hingle, 2015).
Emerging research suggests that telehealth treatment of obesity may extend to youth with intellectual and developmental disabilities. For example, in a pilot study investigating the efficacy of weight loss diets for adolescents with developmental disabilities, tablet computers were successfully used to track dietary intake and physical activity, as well as to allow for video chat sessions with a registered dietitian (Ptomey et al., 2015). Patients and their parents video chatted with a registered dietitian weekly for 2 months, with 80% attendance. In addition, patients utilized their tablet computers to track dietary intake 83% of the time, with an overall improvement in diet quality. In terms of the patients’ experience engaging with technology, 95% reported that the tablet was enjoyable and easy to use, although parents reported that only 42% of youth were able to utilize the tablet without assistance. However, additional studies in this area are lacking.
Nurses can play an important role in delivery of interventions via telehealth. Telenursing, a subtype of telehealth, is an emerging field in which nurses provide care to patients via telecommunication devices (Kumar, 2011). Telenursing has been effectively utilized across a variety of technological mediums and treatment programs, and it positively influences the patient’s perception of accessibility to care as well as speed of access (Hagan, Morin, & Lépine, 2000). In a program to prevent weight-related diseases through the use of short messaging services (SMS), telenursing users demonstrated greater knowledge of the subject material than non-telenursing users (Pangan et al., 2011). In a separate study assessing user perceptions of a telenursing service, users reported appreciating the clarity of nurses’ responses to questions (Hagan et al., 2000). Users also saved an average of 5 hr of time in accessing the nurses via telephone as opposed to going in-person to their primary care provider. Given the importance of time, cost, and accessibility in determining whether patients pursue and sustain care of chronic conditions such as obesity (Gillette et al., 2014; Kim et al., 2010), telenursing offers promising benefits in this regard. Maintaining the continuum of care under the same treatment team, while alleviating stressors associated with travel to the treatment location, is a potentially significant benefit.
Challenges to using telehealth in this vulnerable and underserved population are similar to those associated with the implementation of technology in general. Barriers may include issues related to accessing the Internet and using computers, as well as concerns about maintaining privacy of health care information. For efficient and effective use of telehealth for intervention delivery, nurses must develop and maintain their own comfort level and ability to use telehealth while maintaining good rapport with patients (Dowell, Stubbe, Scott-Dowell, Macdonald, & Dew, 2013). Longer-term challenges for sustained use of telehealth can be multifaceted, including nurses’ concerns regarding increased workload. For patients to stay engaged in self-management, they must perceive that telehealth is useful to them. Therefore, technologies will need to be developed that maximize provider and patient engagement in the telehealth intervention over time (Or et al., 2011).
Depending on the type of intellectual or developmental disability, parents and caregivers will need to evaluate the potential benefits relative to the risks of implementing family-based weight management interventions via telehealth. For example, parents may experience opposition from their child, including physical aggression, requiring a more intensive level of support and training from a certified behavior analyst. Thus, it is critical to include appropriate screening of families and access to an interdisciplinary treatment team in the development of telehealth protocols.
Summary and Future Directions
Despite evidence that youth with intellectual and developmental disabilities are at increased risk for overweight and obesity compared with youth without disabilities, relatively few interventions have been developed and evaluated for managing weight and eating in this population. To stimulate future work, we have highlighted available research, stressing the importance of creating a healthy environment among youth whose capacity for self-management may be limited. We suggest that telenursing holds promise for increasing access among parents and caregivers who may find participation in in-person sessions to be burdensome when caring for a child with a disability. Nonetheless, telehealth also includes challenges and barriers. Developing partnerships among key stakeholders including nurses, families, and policy makers will be critical to developing effective training and treatment protocols. Creative approaches are needed for delivery of childhood obesity prevention and treatment (Pratt, Stevens, & Daniels, 2008), and novel approaches may need to be tailored to the type of disability, as different physical, mental, and behavioral impairments may require specific intervention strategies. Interdisciplinary interventions that show evidence of feasibility and preliminary efficacy for weight management among youth with intellectual and developmental disabilities should be evaluated by nurse scientists in prospective, randomized, controlled studies including diverse samples.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.