
Abstract
We aim to investigate nurses’ feelings of comfort or discomfort with three different types of touch: task-oriented contact, touch promoting physical comfort, and touch providing emotional containment. A questionnaire was administered to a sample of 198 nurses. We present results of multiple regression analysis identifying some antecedents of nurses’ feelings of comfort with touch, namely, attachment style, worry, gender, and length of service. Worry is negatively associated with task-oriented contact and touch promoting physical comfort. Attachment security and length of service are associated with comfort with touch aimed at emotional containment; female nurses feel more comfortable than male nurses in performing this type of touch. Practical implications of findings are discussed in relation to the promotion of focused training courses for practitioners who are willing to improve the quality of care services.
Since the mid-1950s (Frank, 1957; Hall, 1955, 1959), the affective component of touch was recognized both for its effects and social meaning. Even though initial studies in the field underlined that touching is governed by unwritten, conventional, cultural, and gender-dependent rules, it has been stated that, in general, individuals have a greater need for touch during illness or psychological distress (Burton & Heller, 1964; DeWever, 1977).
During the early 1990s, scholars proposed a more complex definition of touch in nursing, introducing and formalizing also its psychological and social effects, namely, supporting, helping patients cope with illness (Bottorff, 1993), comforting, reassuring, and encouraging (Adomat & Killingworth, 1994). In addition, scholars (El-Kafass, 1983; Estabrooks, 1989) underlined that some patients may manifest an increased need for touch because of the isolation and separation from their families, due to severe or terminal illness, age, or chronic pain. Even though its benefits are recognized, the widespread adoption of nonnecessary touch is not proven (Gleeson & Timmins, 2005) and there is a profound lack of overall accepted clear guidelines. Moreover, at the present time, nurse’s engagement in nonnecessary, affective touch is left to nurse’s personal initiative, sensitivity, and degree of responsiveness to the patient’s needs. While several organizational stressors hindering touch practices are identified since the early 1990s (Adomat & Killingworth 1994; Connor & Howett, 2009; Estabrooks, 1989; Estabrooks & Morse, 1992; McCann & McKenna, 1993), there is a need to clarify the role of variables of individual difference in supporting or preventing nurses to perform touch. Estabrooks’s (1989) studies show that three different variables, namely, nurse variables, patient variables, and contextual variables, can exert an impact on nurse’s experience of touch. A recent review on the use and effectiveness of nursing touch (Gleeson & Timmins, 2005) indicates that studies have mainly focused on three areas: nurse’s use of touch, the impact of touch, and the experience of touch. Overall, the literature on touch has not systematically investigated the role of individual differences and how these can affect nurses’ perceptions of their use of touch.
This article aims to fill this gap, by investigating the association between nurses’ attachment style and inclination to worry and their feelings of comfort with touch practices in their daily activity. Our sample includes nurses from four different departments: palliative care, intensive care, oncology, and geriatrics. In fact, according to literature (El-Kafass, 1983; Estabrooks, 1989), patients hospitalized in the above-mentioned departments manifest an enhanced need for touch. This study is concerned with nurses variables of individual difference, namely, attachment style and worry associated with feelings of comfort or discomfort with three components of touch practices: task-oriented contact, touch promoting physical comfort, and touch providing emotional containment (Pedrazza, Minuzzo, Berlanda, & Trifiletti, 2015; Pedrazza, Trifiletti, Berlanda, Minuzzo, & Motteran, 2015).
Touch in Nursing
Definitions of Touch
Touch is an essential and often unavoidable part of nursing practices, which can develop in three different types of action: task-oriented contact, touch promoting physical comfort, and touch providing emotional containment (Pedrazza, Minuzzo, et al., 2015). According to Montagu (1971), touching is an essential part of nonverbal communication; in addition, the experience of touch stimulation for the human being, considered as an open system, is essential to survival, balance, and human development (Weiss, 1992).
From the early 1970s, to the early 1990s, scholars came up with different definitions of touch (Routasalo, 1999) according to type of practice, context, patients’ characteristics and needs, and nurses’ goals: necessary and nonnecessary touch (Barnett, 1972), instrumental and expressive touch (Watson, 1975), instrumental and empathic touch (Gadow, 1984), procedural and expressive touch (Mitchell, Habermann-Little, Johnson, VanInwegen-Scott, & Tyler, 1985), and spontaneous, pragmatic, and silent touch (Karr, 1985). These first attempts to synthesize and to formalize differentiated but interconnected acts, attitudes, and behaviors, organized and performed to more fully assist patients, gained the growing attention of the scientific and professionals’ community. Definitions of touch were associated with its effects on patients’ behavior and on their reported attitude changes. It was experienced as therapeutic, but its explicit purpose was not to heal (Routasalo, 1999). Research was also extended to the patients’ perception of/and responses to touch (Day, 1973; DeWever, 1977).
During the 1990s, scholars recognized and defined additional types of touch, with specific reference to its psychological and social functions, such as comforting, helping the patient cope with illness (Bottorff, 1993), caring, reassuring, and encouraging (Adomat & Killingworth, 1994).
Since 1989 (Estabrooks), intensive care unit (ICU) nurses know protocols and normative patterns of touch for intensive care patients. In fact, several patient populations may manifest enhanced need for adequate touch in a safe and supporting environment. According to different scholars (Adomat & Killingworth, 1994; Bottorff, 1993; Bush, 2001; Estabrooks, 1989; Routasalo & Isola, 1998), appropriate touch can improve the health status of older adults in general and specifically of long-term patients, older hospitalized patients, and terminally ill patients.
In the early 1990s, scholars began to explore the different components of touch practices (Bottorff, 1993) and their effects (Estabrooks & Morse, 1992).
Qualitative and explorative research highlighted the fact that not only personal factors but also organizational variables could be identified as potential stressors impeding and even hindering touch practices with specific reference to cancer patients.
Conceptualization of Touch in Nursing
The experience of touch is located on a continuum from negative to positive outcomes, depending on nurses’ intention and awareness. Scholars distinguish nonintentional from intentional touch (Chang, 2001), task-oriented contact from touch promoting physical comfort, and touch providing emotional containment (Pedrazza, Minuzzo, et al., 2015; Pedrazza, Trifiletti, et al., 2015). These conceptualizations refer to different but strongly interconnected dimensions: nurses’ awareness of/and/in the process, and the objective/intention nurses have when they experience and put into practice attitudes, acts, and behaviors pertaining to the complex performance of touch. The conceptualization grows in complexity in Connor and Howett’s model of touch (2009), where different personality and social dimensions of nurses and contextual variables are put into place. As the authors underline, among nurses’ personal factors influencing touch, we can enumerate stress levels, shared meaning of touch, and extent of trust relationship. The touch continuum the authors propose differs slightly from the previously mentioned ones, and looks at touch from new perspectives: an objective one, where nonintentional touch can be recognized within a procedure-centered performance, and a subjective one, where intentional comfort grows, for patients and nurses, within a patient-centered acts/and actions sequence. In line with this last conceptualization, scholars (Estabrooks, 1989; Estabrooks & Morse, 1992; Gleeson & Timmins, 2005) emphasize that nurses’ experience of touch can be ascribed to three different origins: nurse variable, patient variable, and contextual variables. Even though capturing only marginal attention from researchers, the “nurse variable” has been categorized in very similar ways throughout scientific literature: perceived stress (Adomat & Killingworth, 1994; Aiken, Clarke, Sloane, Sochalski, & Silber, 2002; Connor & Howett, 2009), tolerance and trust in relationships, values (Routasalo, 1999), cultural and familial background (Estabrooks, 1989; Estabrooks & Morse, 1992), personal experience, and training.
Touch in Health Care Practices
Estabrooks (1989) underlines that patients experiencing chronic pain, terminally ill patients, and elderly patients benefit consistently from adequate touch because of their often long-lasting experience of social deprivation. Touch is an essential part of caregiving and has been proved to contribute to meet these specific patient’s needs: it reduces pain, agitation behaviors in patients with dementia (Kim & Buschmann, 1999), and it provides comfort in older adults residing in nursing homes (Kolcaba, Schirm, & Steiner, 2006). Compassionate touch, feasible and effective, assists providers in achieving the reducing of antipsychotic medications (Catlin, 2015). Touching as a therapeutic event is not as simple as a mechanical procedure or a drug because it is above all an act of communication (Montagu, 1971), it is a powerful tool for nonverbal communication. The methods used in compassionate touch combine specific touch techniques—including focused touch, hand massage, slow stroke back massage, and foot massage—with the quality of presence (Catlin, 2015).
Cutaneous stimulation has been shown to be useful in reducing pain (see Pedrazza, Minuzzo, et al., 2015). Touch improves quality of life in patients with metastatic cancer at the end of life and is associated with beneficial effects, such as pain reduction and sleep quality (Toth et al., 2013). In a study by Karagozoglu and Kahve (2013), patients reported lower anxiety scores after being touched by nurses during chemotherapy. The importance of human touch (Adams, White, & Beckett, 2010) to balance the high-technology of today’s health care practices was also confirmed. A large and growing body of research justifies the use of massage therapy for pain management in the acute care setting. Massage therapy was effective in blood pressure, heart rate, respiration rate, and O2 saturation in patients with congestive heart failure (Jamali, Ramezanli, Jahromi, Zare, & Poorgholami, 2016). Using tactile massage may give nurses a tool in their work, may change their caregiving practice, and may increase their own and their patients’ well-being in a stressful environment as the short-term emergency ward (Airosa, Falkenberg, Öhlén, & Arman, 2016).
Kübler-Ross (2008) claims that gentle hand pressure is the most effective form of communication with dying patients. In general, touch is an essential part of caregiving and an excellent way of communicating attention, sympathy, closeness, reassurance, and presence (see Routasalo, 1999). Hand massage is a simple comfort intervention that can be incorporated readily into routine nursing care activities and conveys caring through touch, individual attention, and presence (Kolcaba et al., 2006). Touch promotes adaptation of institutionalized elderly to the new environment of the nursing home. As an intervention, hand massage promotes comfort and facilitates communication between care recipients and caregivers. Touch is experienced as positive both from patient as from nurses if it is appropriate to the situation (Hollinger-Smith & Buschmann, 1993) and not discrepant with the needs of individuals. It can be experienced as positive if it does not impose more intimacy than desired. Not all touch is perceived as a positive intervention by patients even if it was intended so by nurses (Davidhizar & Giger, 1997).
Variable of Individual Difference Preventing Nurses to Feel Comfortable Using Different Types of Touch
Up-to-date literature (Pedrazza, Minuzzo, et al., 2015; Pedrazza, Trifiletti, et al., 2015) points out that the ease with touch influences job satisfaction in a positive way. The recently identified types of touch, above all the one providing reassurance, psychological support, and psychological containment, can elicit stress. This type of touch accounts for the psychological dimension that prompts actions to distance oneself emotionally and cognitively from one’s work, presumably as a way to cope with the work overload (Maslach, Schaufeli, & Leiter, 2001). Touch implies closeness and sometimes intimacy and it cannot therefore be taken for granted that nurses are always willing to engage in it (Edvardsson, Sandmann, & Rasmussen, 2003). Connor and Howett (2009) signalize that nursing students, when asked to care for difficult or offensive patients, often disengage from intentional comfort touch because they feel pushed outside their comfort zone.
Among others, nurses’ main requirements to feel comfortable using touch are the following: a sense of inner balance and the need for supportive environment (Airosa et al., 2016). In fact, even though a number of different aspects influencing positive touch practices are mentioned, a great concern seems to be about affective inner balance (Andersson, Wändell, & Törnkvist, 2007). Also, organizational restraints seem to exert a considerable impact on touch: technical and stressful environment, perceived high demands, and work overload (Airosa et al., 2011; Yang et al., 2001). Adomat and Killingworth (1994) interviewed nurses in ICUs and showed that stressors were mainly related to organizational pressure rather than to involvement of caring for critical patients. Furthermore, they underline that some nurses become mechanical in their patient encounters and that they engage only in task-oriented touch. Very interesting for the purpose of our study are Whiteside and Butcher’s (2015) exploration and critical review of factors influencing perception and use of touch in nurses. They show that above all, male nurses report they feel uneasy, fearful, and anxious in relation to touching females (see also Gleeson & Higgins, 2009). Even though those feelings may be consequences of gender-based stereotypes (Paterson et al., 1996), they account also for the features attachment theory–based research has identified as general caregiving deficits (B. C. Feeney & Collins, 2001; Mikulincer & Shaver, 2007) and barriers to sensitivity and responsiveness. Attachment literature and nursing studies of touch practices agree in viewing the uneasy and generally unpleasant feelings in closeness with “generalized others” and patients, as one of the most widespread variables of individual difference, which can hinder intentional comfort touch.
Touch Through the Prism of Attachment
Touch literature has proven that nurses may feel uncomfortable and under pressure to use this type of intervention (Gleeson & Timmins, 2005). Kruijver, Kerkstra, Bensing, and van de Wiel (2000) show that nurses use blocking behaviors such as avoidance and distancing when stressed or faced with problems.
The previously described enriched conceptualizations of touch allow us to look at variables of individual difference, which support or hinder different types of touch. It is worth recalling that the attachment system includes a set of beliefs and expectations about relationships, the self, and others, which supports any type of dyadic interaction. The perception of each relational transition is filtered through the lens of individual representations of the self and of the “generalized other” stored within the so called IWM, internal working models of attachment developed during infancy. Expectations and causal attributions, activated by/and/within each interpersonal transition, are affected by those representations and seem to be sufficiently stable over time, influencing personal feelings of comfort and discomfort in closeness. The attachment theory (Mikulincer & Shaver, 2007) explains how secure, anxious, and avoidant attachment styles differently affect human interactions. This theoretical framework allows us to look at touch practices as moving on a continuum from “allowing closeness with ease” to “perceiving closeness as threatening.” Closeness to the patient is related, on one hand, to nurses’ objectives (such as task-oriented objectives or comforting and reassuring patients) and, on the other hand, to the degree nurses allow closeness. Secure attached subjects are less involved in responding to their own needs, they perceive less discomfort by witnessing another person’s distress and pain, and they do not perceive interdependence, involved in providing care, as uncomfortable or even threatening. In contrast, the long-lasting and recurrent feelings of discomfort insecure subjects perceive in closeness can produce emotional overload and burnout. Anxious people are usually comfortable with closeness but they are characterized by a lack of intra- and interpersonal regulatory skills; avoidant subjects typically maintain what they perceive as a safe distance from their interlocutor and tend to perceive great discomfort in responding responsively to suffering interlocutors (Collins, Ford, Guichard, & Allard, 2006; Mikulincer & Shaver 2007).
Touch, Caregiving System, and Attachment Style
Physical touch requires sensitivity, responsiveness, and great involvement on the part of nurses because it implies physical, cognitive, and emotional proximity to the patient (Pedrazza, Minuzzo, et al., 2015). Attachment style is a key variable in activation and functioning of the caregiving system. A key part of the caregiving system’s strategy (Mikulincer & Shaver, 2007) is the adoption of an empathic stance toward another person’s need. Moreover, according to attachment theory (Mikulincer & Shaver, 2007), facing another person’s suffering can evoke two different types of affective response in the caregiver: empathic compassion and personal distress. Studies on attachment security and insecurity demonstrate that all forms of sensitive, responsive, and compassionate care across the life span and different contexts have a common basis and resemble each other (Mikulincer & Shaver, 2007). Kolcaba’s (1994, 2001) comfort theory describes nursing as the process of identifying patients’ comfort needs and addressing them through the development and implementation of appropriate nursing interventions. In this context, physical touch can play a key role.
The extent to which nurses feel comfortable about the use of touch may affect both the frequency and quality of nursing touch-based interventions. According to Kolcaba (1991, p. 238), we defined comfort as “the state of having met the basic human needs for ease, relief, and trascendence.” According to Platts, Tyson, and Mason (2002), attachment security or insecurity could function as conceptual bridges linking early experience with the development of schemata and representations. They argue that individual differences in attachment orientation can be related to differences in schemas/thoughts/representations people hold referring to each social/interpersonal domain. Platts et al. (2002) suggest that researchers should develop more interest in studying actual beliefs people with different attachment styles hold. Our study is concerned with the interpersonal domain consisting in the nurse–patient relationship. Important results from studies on compassion and empathic behavior show that avoidant attachment predicts lower levels of compassion (Mikulincer et al., 2003) and helping behavior, whereas attachment anxiety is linked with personal distress (van Ijzendoorn & Zwart-Woudstra, 1995).
Worry as Risk-Associated Factors for Distress at Work in Caring
We assume that nurses can perceive feelings of discomfort facing particular touch practices thereby undermining some aspects of the quality of care. As mentioned, the perceived personal distress could in fact prevent nurses from engaging in compassionate behaviors. The long-lasting perception of feelings of discomfort and personal distress may induce the practitioner to reflect in a persistent way on those feelings, looking for reasons and coping strategies. Recurrent self-focused thinking leads to worry.
Worry involves recurrent stream of thoughts and images associated with unpleasant affect. We assume that worry is relevant to our study because it involves the analysis of the present and it is also concerned with preoccupation for future possible events (Watkins & Baracaia, 2001). We assume nurses may respond to discomfort feelings at work with worry. Performance stressors such as those induced by social-evaluative threat elicit more worry than a stressor without the explicit evaluative component (Zoccola & Dickerson, 2012). Such stressors may elicit and maintain negative thoughts immediately and also days later. It can be therefore interesting to identify to which extent touch is associated with nurses’ worry behavior.
Worry and Attachment Insecurity
According to Nolen-Hoeksema and Morrow (1993), motivations and thoughts related to worry are important because they often are the reason for persevering in this behavior. Our attachment system is activated in facing events and situations perceived as threatening or negative. Nurses who are burned out, or simply worried, can perceive touch practices as threatening or negative components of their daily nursing experience. We argue that it is important to investigate some aspects of the metacognitive dimension of worry. These include the self-reported feelings and thoughts associated with low and high levels of worry, when touch practices become salient. In the present study, self-reported thoughts and feelings associated with high or low levels of worry are examined utilizing the Attachment Style Questionnaire (ASQ; J. A. Feeney, Noller, & Hanrahan, 1994). This scale is a useful tool because it is concerned with beliefs associated with security, anxiety, and avoidance concepts sedimented in our representations. Those thoughts are consistent and stable in adulthood over time and social/interpersonal domain. Internal working models organize beliefs over time and shape individuals’ expectations, perceptions, reactions, and behaviors (Ein-Dor, Mikulincer, & Shaver, 2011). We are interested to investigate thoughts and concepts associated with high or low scores in worry, which are pertinent to the interpersonal domain of the nurses–patients relationship.
Purpose
Touch perception among nurses has received only marginal attention in nursing research (Gleeson & Timmins, 2005). Pedrazza, Trifiletti, et al. (2015) develop the nurses’ Comfort With Touch Scale. This scale highlights three types of touch: task-oriented contact elicited the highest level of comfort, followed by touch aimed at promoting physical comfort and touch providing emotional containment. These studies suggest that the three dimensions of touch reflect three different degrees of affective and cognitive proximity to the patient. Feeling comfortable with emotional closeness probably helps to establish a positive and rewarding interaction with patients, and this probably acts as a buffer against stress. Attachment security allows individuals to feel comfortable in closeness and in autonomy. Insecure subjects, however, whether avoid closeness or they fear it, feel preoccupied and worry about it. Attachment style represents the most important variable of individual difference, which supports/hinders and regulates interpersonal psychological processes regarding any type of social domain: familial, social, peers, and professional domain (Pedrazza, Berlanda, Trifiletti, & Bressan, 2016). It also accounts for differences in the perception of threat. Closeness to patients can represent a threatening event, above all for insecure people. We therefore assume that the level of worry and concern from both secure and insecure subjects can help us to glance into nurses’ experience of touch.
Our aim is to understand how and to what extent attachment style and worry exert an impact on nurses’ engagement in different touch practices, such as task-oriented touch, touch promoting physical comfort, and touch providing emotional containment, in contexts where touch is needed (El-Kafass, 1983; Estabrooks, 1989).
Hypotheses
We assume a differentiated effect of worry and attachment style on nurses’ comfort in performing the three types of touch. Specifically, we hypothesized that worry would be more strongly related to task-oriented touch and touch promoting physical comfort (Hypothesis 1), while adult attachment should be more strongly related to emotional containment (Hypothesis 2).
Task-oriented touch is an integral part of nurses’ job and is therefore evaluated. Although providing physical comfort through touch is not explicitly included among nurses’ duties, it is likely to be perceived as strictly functional to the provision of care and, therefore, as a component of performance that is evaluated. Nurses who report higher levels of worry should be more concerned about evaluation of their performance and feel less at ease with the above-mentioned components of touch.
Touch aimed at emotional containment implies not only a physical but also an emotional proximity to the patient. Adult attachment should play a more important role in determining comfort with this type of touch than worry because it represents the most fundamental individual variable for the regulation of social relationships.
Method
Procedure
A self-report questionnaire was administered to a convenience sample of registered nurses, working in the departments of palliative care, intensive care, oncology, and geriatrics in several hospitals of Veneto and Friuli Venezia Giulia (Northeast Italy). The final sample included 198 nurses. Researchers provided subjects with explanations and asked for signing of informed consent forms.
Participants were contacted in April 2013 during a 2-day pain management training course held by one of the authors. They were given the questionnaire at the end of the first day and asked to return it on the following day. The research was presented as a survey on nurse’s skills and well-being at work. Ethical approval was obtained from the ethics committee of the researchers’ institution. Informed consent was obtained from each participant after having explained the nature and purpose of the study. Subjects were also informed that data obtained from the questionnaire would be used only for research purposes. Participation was entirely voluntary; participants were informed about their right to withdraw or refuse to give information at any time without incurring any penalties. The anonymity and confidentiality of answers were guaranteed.
Measures
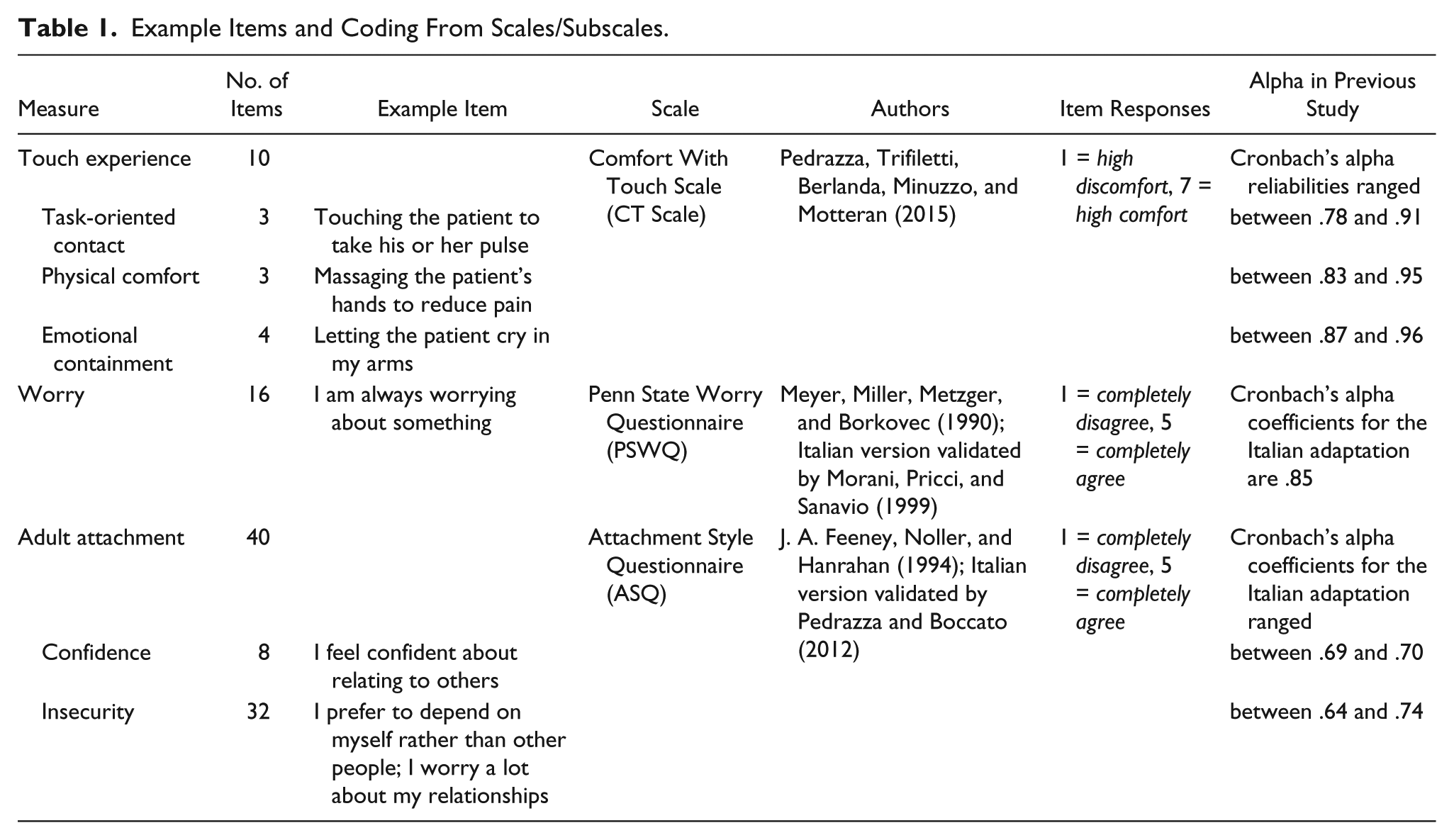
The survey questionnaire contained the following validated measures: Touch Experience, Worry, and Adult Attachment (see Table 1). Responses are given on a Likert-type scale.
Example Items and Coding From Scales/Subscales.
Data Analysis
The collected data were analyzed using the SPSS statistical software package, Version 21.0.
PRELIS (LISREL 8.7) was used for the imputation of missing data with the expectation–maximization (EM) algorithm. Only 2.48% of the total responses were missing scores (demographics were not submitted to missing data imputation). According to Schafer and Graham (2002), maximum likelihood imputation (EM algorithm) provides more accurate estimates of population parameters than list-wise deletion or mean substitution.
First, for each variable, a composite score was computed by averaging the respective items. Pearson correlation was used to examine the association between variables. To test whether nurses reported similar levels of comfort in relation to task-oriented contact, touch promoting physical comfort and touch aimed at emotional containment paired t test were applied. Finally, multiple linear regression analyses were carried out: touch aimed at emotional containment, touch aimed at promoting physical comfort, and task-oriented contact were dependent variables. We included in the regression models worry, confidence, and insecurity attachment as predictors, and we added length of service and gender as covariates. Age was not included in regression analyses because (as shown in Table 3) its correlation with length of service was .90. Including two highly correlated variables may generate multicollinearity. We chose length of service, as we deemed it as more interesting than age for this context. Due to missing data on length of service and gender variables, sample size in multiple regression models was reduced (N = 186). Post hoc calculation of power (two-tailed) indicates that for a multiple regression model with five predictors and α = .05, power (1 − β) equals .99.
Results
Sample
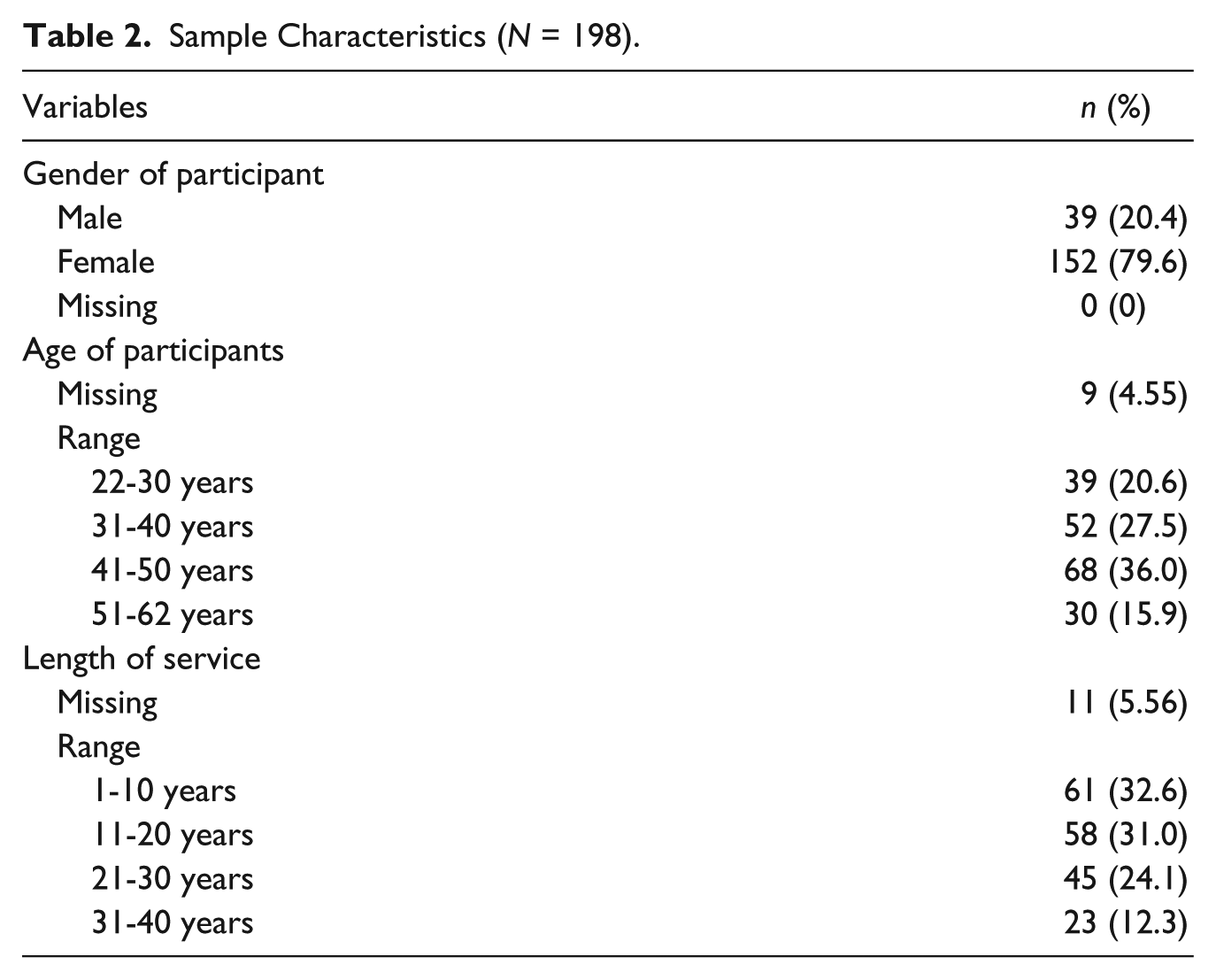
Our sample included 198 nurses (82.5% return rate). Demographic data are summarized in Table 2. The mean age was 40.46 years (SD = 9.63, range = 22-62). The mean length of service was 16.75 years (SD = 10.76, range = 1-40).
Sample Characteristics (N = 198).
Descriptive Statistics, Internal Consistencies, and Correlations
Descriptive statistics, internal consistencies, and correlations for the study variables are reported in Table 3. Nurses present high levels of self-perceived comfort with task-oriented touch, whereas they feel less at ease to touch the patient to provide support and containment. Paired samples t tests indicate significant differences between task-oriented touch and touch aimed at promoting physical comfort (p < .001, [0.854, 1.173]), between task-oriented touch and touch aimed at providing emotional containment (p < .001, [1.413, 1.831]), and between touch aimed at promoting physical comfort and touch aimed at providing emotional containment (p < .001, [0.411, 0.805]).
Descriptive Statistics, Alpha Values, Correlations, and Confidence Intervals for the Study Variables (N = 198).
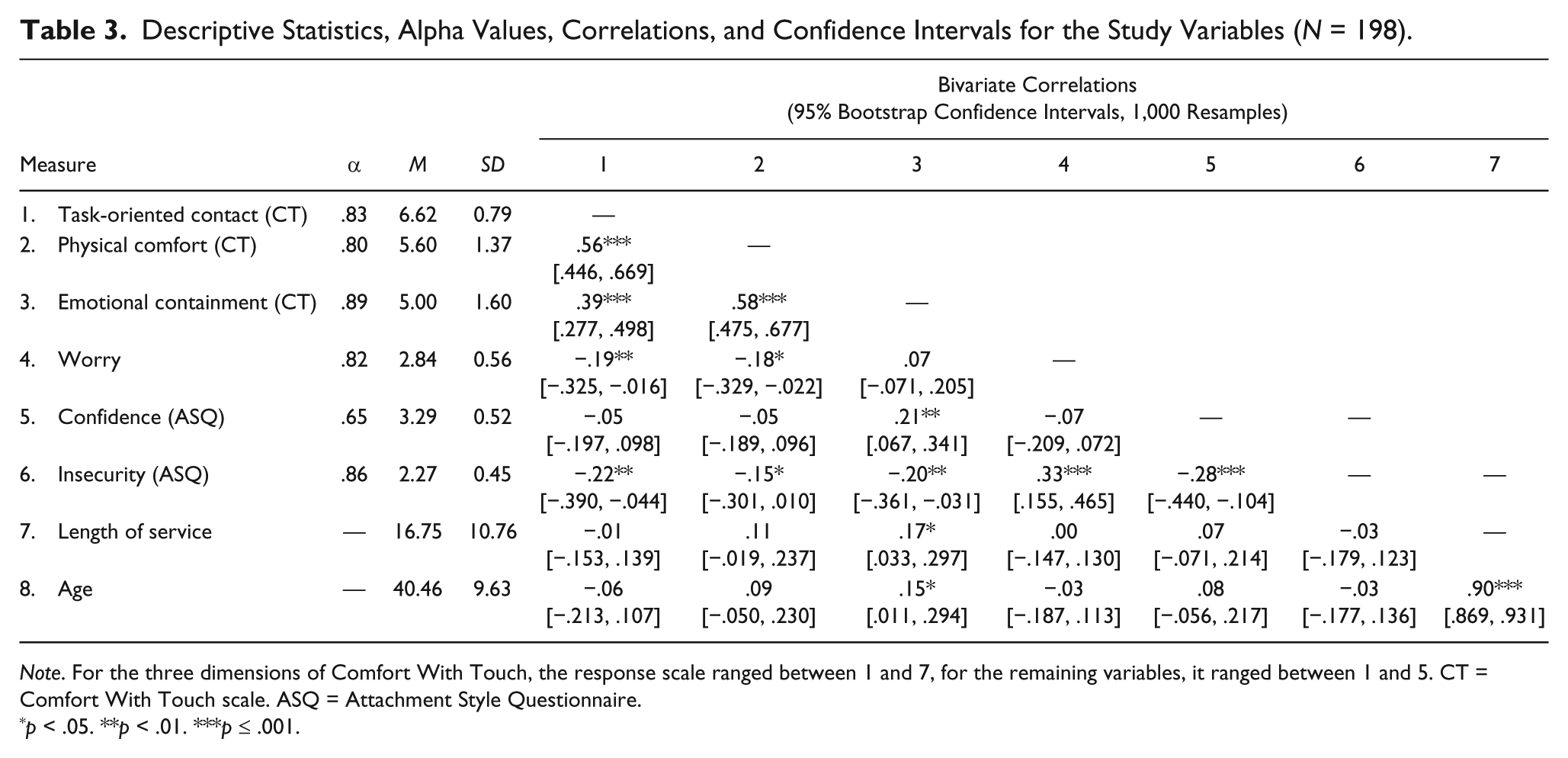
Note. For the three dimensions of Comfort With Touch, the response scale ranged between 1 and 7, for the remaining variables, it ranged between 1 and 5. CT = Comfort With Touch scale. ASQ = Attachment Style Questionnaire.
p < .05. **p < .01. ***p ≤ .001.
Multiple Regression Analysis of Variables on Comfort With Touch
The regression analysis with task-oriented contact as dependent variable (Table 4), F(5, 186) = 3.30, p < .010, R2 = .08, shows that insecurity, and partially worry, compromises task-oriented contact. For the touch aimed at promoting physical comfort (Table 5), F(5, 186) = 2.68, p < .050, R2 = .07, 7% of the variance in the score were predicted by worry. The regression analysis, with the touch aimed at emotional containment (Table 6), F(5, 186) = 5.25, p < .001, R2 = .13, shows that insecurity compromises this type of contact, while confidence, greater length of service, and female gender facilitate the comfort with emotional containment touch.
Multiple Regression Analysis of Nurses Variables on Task-Oriented Contact (N = 186).
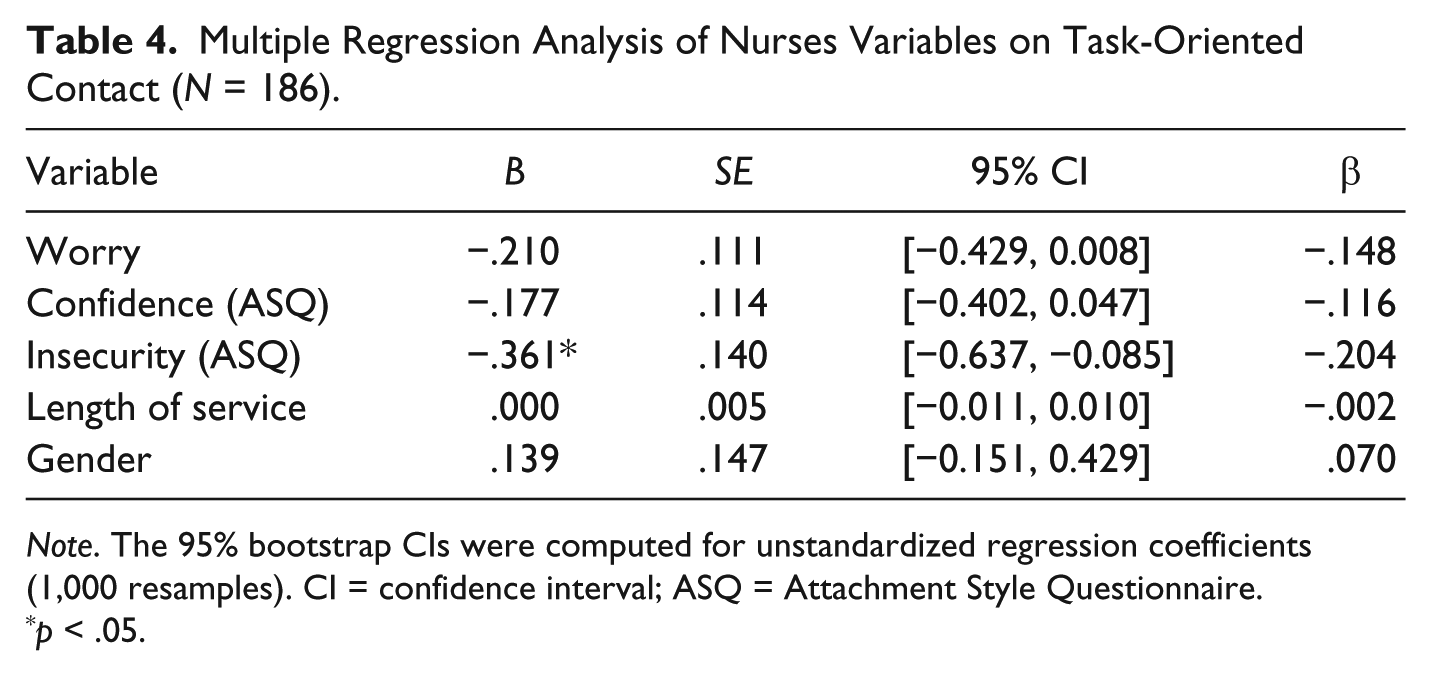
Note. The 95% bootstrap CIs were computed for unstandardized regression coefficients (1,000 resamples). CI = confidence interval; ASQ = Attachment Style Questionnaire.
p < .05.
Multiple Regression Analysis of Nurses Variables on Touch for Physical Comfort (N = 186).
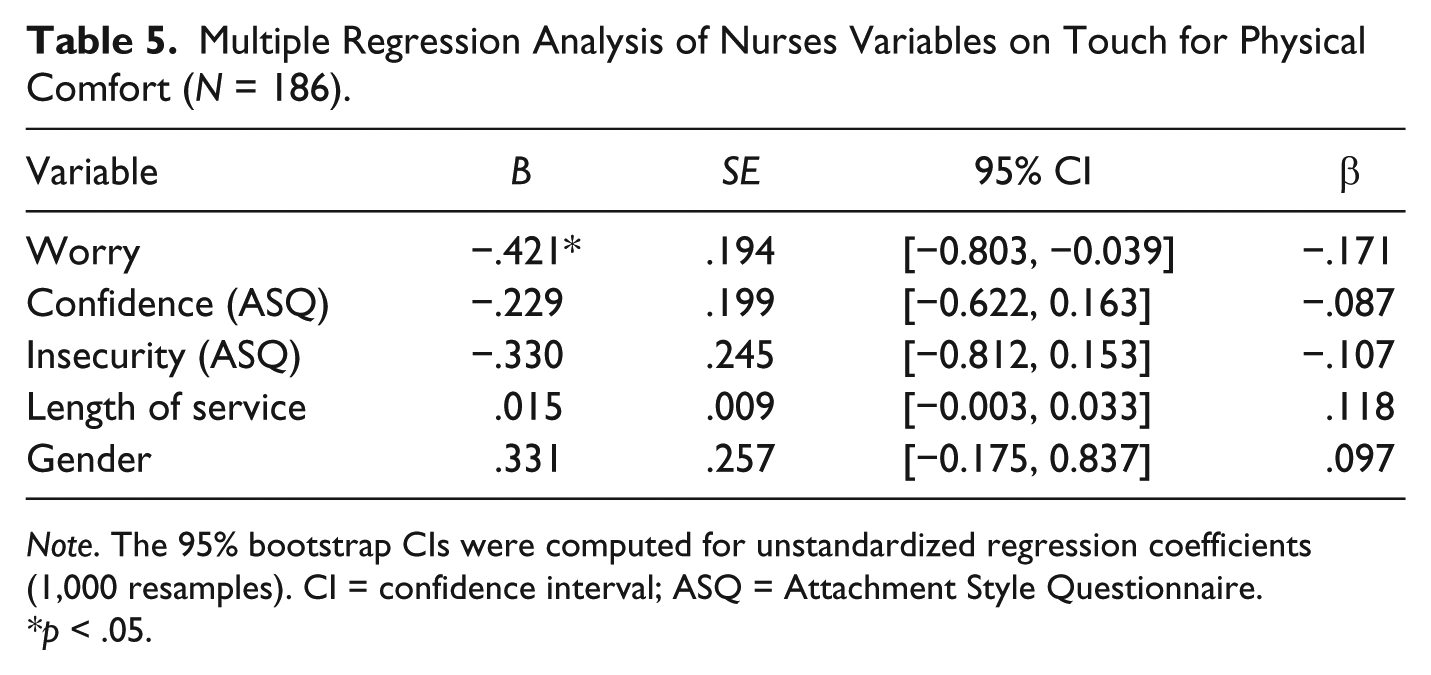
Note. The 95% bootstrap CIs were computed for unstandardized regression coefficients (1,000 resamples). CI = confidence interval; ASQ = Attachment Style Questionnaire.
*p < .05.
Multiple Regression Analysis of Nurses Variables on Touch for Emotional Containment (N = 186).
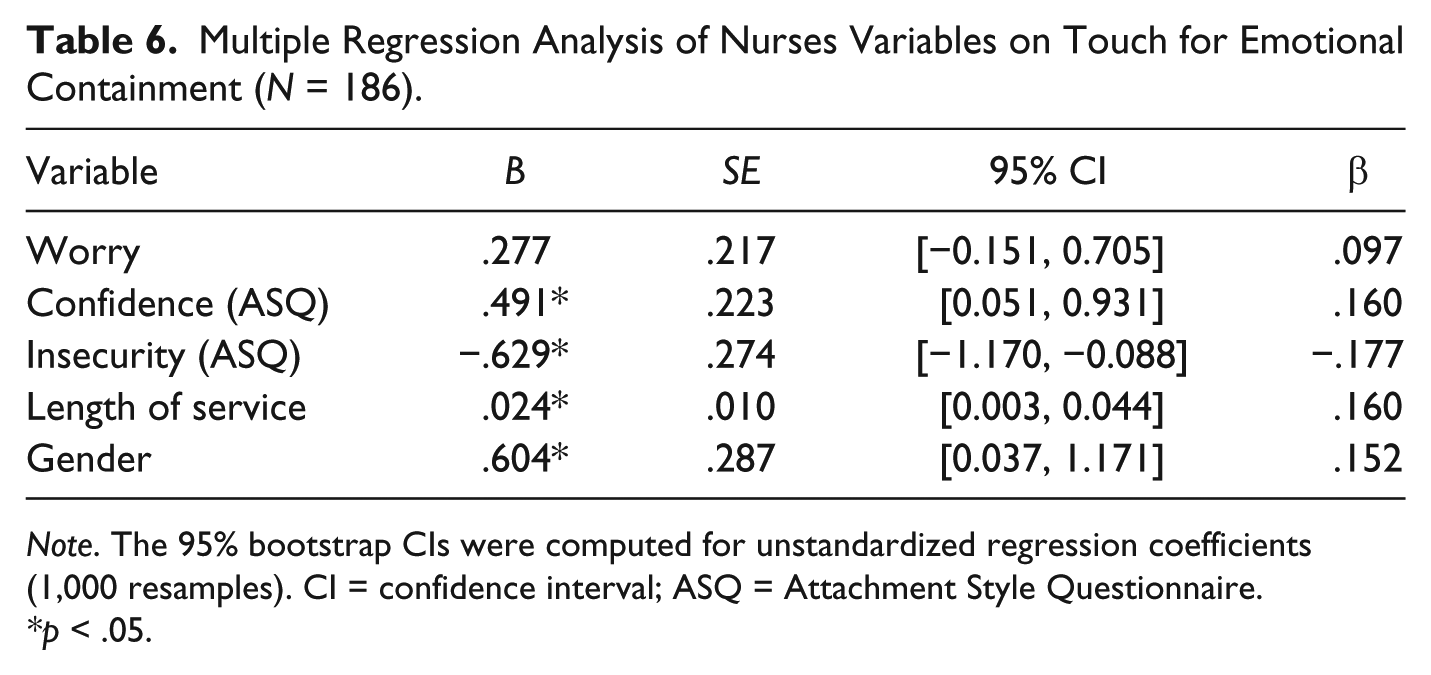
Note. The 95% bootstrap CIs were computed for unstandardized regression coefficients (1,000 resamples). CI = confidence interval; ASQ = Attachment Style Questionnaire.
*p < .05.
Discussion
The present study feels a gap in literature concerning the understanding of the effects of variable of individual difference influencing touch. In fact, previous studies, focused on nurse’ variables (Gleeson & Timmins, 2005) influencing touch, were concerned with personal experience (Estabrooks & Morse, 1992), perception of unease and feeling uncomfortable with touch (Gleeson & Timmins, 2005; McCann & McKenna, 1993), familial background (Northouse & Northouse, 1998), personal meaning attributed to touch, locus of control (Hollinger-Smith & Buschmann, 1993), and age (Adomat & Killingworth, 1994; Caris-Varhallen, de Gruijter, Kerkstra, & Bensing, 1999; Edwards, 1998). In the present study, we explored the feelings of comfort/discomfort of nurses in performing three types of touch (Pedrazza, Trifiletti, et al., 2015) and their relationship to worry and attachment style.
Hypothesis 1 was confirmed. Task-oriented touch was related to attachment insecurity and to worry (marginal effect). Insecure caregivers are more likely to experience difficulties than secure ones, both in closeness with the patient and in being evaluated for their work. The dyadic, interpersonal nature of the caregiving process may induce insecure subjects to perceive this interaction as a burden or even as a threat (Mikulincer & Shaver, 2007; Tsilika, Parpa, Zgogianni, Kouloulias, & Mystakidou, 2015). In addition, insecure subjects are particularly sensitive to social judgment and the awareness their work practices are observed and evaluated contributes to the building up of worry; in fact, task-oriented touch refers to touch aimed at carrying out specific nursing tasks or procedures.
There was a strong association between worry and touch promoting physical comfort. Even though touch for physical comfort is generally recognized as an important practice, nurses may feel effective and efficient in focusing primarily on task-oriented touch, thus avoiding to providing patients with comfort touch. This last type of touch is not included in protocols; however, nurses could feel worried because of the commonly recognized value, that is, of massage and, in general, of comfort touch associated practices.
Hypothesis 2 was confirmed. Attachment security is associated with feelings of comfort with touch for emotional containment. The perception of comfort with this type of touch is also associated with the female gender and with length of service. The closeness implied in touch for emotional containment is perceived as threatening by insecure subjects. When close to others, they are typically focused on their own attachment needs and thereby oriented to controlled motives for providing care. This type of touch implies on the part of the nurse responsiveness, confidence in own ability to cope with stress/pain and fear, patients can feel and express. It also implies the willingness to help and to provide patients with support. Secure attachment generates confidence and the person’s ability to feel comfortable in maintaining relationships. In addition, secure attachment style is characterized by positive working models in which a person has self-confidence and trust in relationships with others. Securely attached nurses feel comfortable in supporting and encouraging suffering patients. Those abilities and competences are less likely to be exhibited by insecure subjects and by inexperienced nurses; on the contrary, they are likely to be mastered over a long period of service.
Female nurses grow up and interiorize stereotypical features ascribed to women: Nursing is a female-dominated profession and caring is one of the most commonly and intergenerationally transferred competences. In fact, gender differences could be ascribed to group membership and therefore probably drawn from widespread and long-established stereotypes. The first one refers to the image of men as less effective than women in engaging effectively in caring and nurturing practices; the second one accounts for the widespread and often reported fears of male nurses, whose use of touch could be misinterpreted or even perceived as sexual inappropriateness. In addition, according to a recent literature review (Whiteside & Butcher, 2015), men feel uncomfortable and embarrassed in relation to touching female patients because of shared stereotypes, that is, women are supposed to be quieter, harmless, and more sensitive and responsive than men.
Our results suggest that one should create conditions to support nurses to face challenges in nursing practice both at the first stage and also during their career, through supplementary training courses and implementation of higher education study courses. One should prevent nurses from feeling uncomfortable or troubled in their daily practice due to worry or anxiety activated by evaluative practices and outcome evaluation procedures. Experience exchange practices with expert nursing peers and counseling could offer effective support to all.
Male nurses should be supported in the implementation of their ability to cope with stress in front of female patients.
Nurses, grown in work experience, recognize the value of touch aimed at emotional containment, and have probably learned to be effective in providing support and containment during their career (Mikulincer & Shaver, 2007). Some large cancer centers in the United States have started to integrate touch and massage therapy into conventional settings (Russell, Sumler, Beinhorn, & Frenkel, 2008). We suggest the implementation of differentiated training opportunities to secure and insecure nurses, allowing them to contribute to improving the general quality of care. Insecure and male nurses could benefit from an in-depth analysis of their unease in closeness during supervision to increase the number of coping strategies they rely on, managing the nurses–patient relationship. Specific training opportunities should be devoted to encourage the building of a professional stereotype including sensitiveness and responsiveness to mitigate the impact of the current gender-stereotype.
We recognize some limitations of the present study: (a) We relied exclusively on self-reports, and participants may not necessarily be aware of their perceptions and thoughts or may respond in a socially desirable way, (b) the great majority of the sample was female and this might limit the generalizability of our results, and (c) the nested nature of data was not taken into account, given the lack of information about nurses’ departments.
Further studies should be aimed to analyze touch experience in samples including a consistent number of male subjects. Surveys should explore which types of touch are experienced as most problematic in different contexts and subgroups, thus providing useful information for interventions aimed to preserve nurses’ well-being at work and thereby the quality of care. It is true that research should also target representative samples of different cultural contexts. As we assessed variables of individual difference, we strongly believe that our results can be replicated also in different contexts. In fact, research findings into adult attachment (Mikulincer & Shaver, 2007) and worry (Davey & Wells, 2006) literature show that these variables of individual difference should have similar effects across different national and cultural contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.