
Abstract
Depression can disproportionately affect low-income women. The purpose of this study was to explore the chronicity of depressive symptoms in a sample of 276 low-income inner-city mothers of children with high-risk asthma. The aims were to identify factors (asthma health status, stress, social support) associated with change in depressive symptomatology over 12 months as well as to ascertain what factors are most consistently associated with depressive symptoms. Using latent growth curve analysis, demographic variables, asthma severity, stress, and social support failed to explain changes in depressive symptomatology. The growth curve models, however, were predictive of Center for Epidemiologic Studies–Depression Scale (CES-D) scores at distinct time points indicating that higher daily stress and lower social support were associated with increased depressive symptoms. Our data highlight the chronic nature of depressive symptoms in low-income mothers of children with poorly controlled asthma. Integrating questions about caregiver psychological state across all clinical encounters with the family may be indicated.
Keywords
Depression is a serious health and behavioral health problem disproportionately affecting women (Ronzio & Mitchell, 2010). Women of childbearing age, in particular those who are low-income, unemployed, have physical health problems, or are raising children with behavioral or physical health difficulties, are especially at risk for developing depression (Centers for Disease Control, 2010; Manuel, Martinson, Bledsoe-Mansori, & Bellamy, 2012; Rosenthal, Learned, Liu, & Weitzman, 2013). Prevalence rates for depressive symptoms among women with young children range from 10% to 48% and it is estimated that one in 10 children have mothers experiencing depression in any given year in the United States (Ertel, Rich-Edwards, & Koenen, 2011; Manuel et al., 2012). Depressive symptoms are associated with widespread functional impairment and profound difficulties in fulfilling work and home life responsibilities (Pratt & Brody, 2008). The effects of depression are also evident throughout the family with maternal depression negatively affecting mother–child interactions as well as children’s behavior and development (Minkovitz et al., 2005; Sohr-Preston, & Scaramella, 2006; Surkan et al., 2014). Protracted maternal depression may yield especially devastating effects on child growth, with longitudinal research showing children of chronically depressed mothers to be more likely to have behavioral problems, lower social competence, decreased electroencephalogram (EEG) brain activation, and vulnerability to psychopathology (Ashman, Dawson, & Panagiotides, 2008).
Maternal Depressive Symptoms: Implications in the Care of Children With Asthma
Childhood asthma is one of the most common childhood health conditions, and over a decade of research has shown that mothers of children with asthma have elevated rates of depressive symptoms compared with the broader caregiver population (Bartlett et al., 2004; Shalowitz et al., 2006). Reducing psychological distress experienced by caregivers is highly significant as maternal depressive symptoms are consistently related to increased child morbidity and health care utilization (Pak & Allen, 2012). Even when accounting for asthma severity, caregivers who experience high levels of depressive symptoms are 30% more likely to report an emergency department (ED) visit by their child than caregivers with low depressive symptomatology (Bartlett et al., 2001). Although it is not known whether depression causes asthma morbidity, or if it is the experience of raising a child with high-risk asthma that heightens vulnerability to depressive symptoms, there is general consensus that the presence of depressive symptoms may limit the caregiver’s capacity to effectively monitor the child’s symptoms and implement recommended therapies, potentially resulting in poor asthma control and avoidable emergency services for child asthma (DiMatteo, Lepper, & Croghan, 2000; Tibosch, Verhaak, & Merkus, 2011). Investigations addressing how chronic maternal depression affects the trajectory of child asthma are scarce, but one prospective study found baseline maternal depressive symptoms predicted childhood asthma symptoms 6 months later in low-income urban African American families (Otsuki et al., 2010).
Previous studies examining predictors of maternal depressive symptoms indicate that stressors including socioeconomic disadvantage are often related to depressive symptoms in mothers (Giallo, Cooklin, & Nicholson, 2014; Manuel et al., 2012; Mulvaney & Kendrick, 2005; Siefert, Finlayson, Williams, Delva, & Ismail, 2007). In addition, it is clear that social support may protect against depressive symptoms (Manuel et al., 2012; Mulvaney & Kendrick, 2005). However, models testing risk and protective influences on depressive symptoms among low-income mothers of young children with poorly controlled asthma are limited, and even less is known about the trajectory of depression symptoms in this vulnerable population.
Purpose
Consequently, the purpose of this longitudinal study was to explore the chronicity of depressive symptoms in a sample of inner-city mothers of children with high-risk asthma and to identify factors (asthma health status, stress, social support) associated with change in depressive symptomatology. A secondary aim was to ascertain what factors are most consistently associated with depressive symptoms in caregivers over time.
Method
This secondary data analysis is part of a larger prospective randomized controlled trial (RCT) approved by the Johns Hopkins University Medical Institution and the University of Maryland Medical Institutional Review Boards (Butz et al., 2014). Recruitment of children with asthma occurred between December 2008 and January 2010, using a Health Insurance Portability and Accountability Act (HIPAA) waiver to identify and contact families by mail to determine their interest and eligibility in the study. Eligibility criteria for the children included ages 3 to 10 years; diagnosis of persistent asthma by a physician, reported controller medication use, and two or more ED asthma visits over 12 months. Children meeting these criteria are considered high risk or having uncontrolled asthma (United States Department of Health and Human Service [USDHHS], 2007). Children were excluded if they had other major respiratory conditions including cystic fibrosis. Three hundred caregivers and their children were enrolled in the RCT after eligibility was determined, written informed caregiver consent was obtained, and child verbal assent (age ≥ 8 years) completed.
After completing a baseline questionnaire, all children and their caregivers were randomly assigned to either a Pediatric Asthma Alert Intervention (PAAL) designed to enhance adherence to guideline-based care or an attention control arm (Butz et al., 2012, 2014). Although both groups received home visits, the intensity and focus of these visits varied. Children assigned to the control group received three nurse home visits focused on home-based asthma education targeting asthma triggers, asthma medications, device training for peak flow meter and spacer technique, as well as assistance with arranging follow-up asthma care with the child’s primary care provider (PCP). Children assigned to the PAAL group also received nurse visits for asthma education but in addition, the nurse accompanied the child and parent to the child’s follow-up PCP visit for asthma. The nurse provided feedback to the child’s PCP about the child’s asthma health, pharmacy refill data, and salivary cotinine level. Caregivers and children were followed over 12 months with in-home survey data collection occurring at baseline (T1), 6 months (T2), and 12 months (T3). Only biological mothers (276/300; 92%) of the children were included in the current analysis.
Measures of Demographic Covariates
Sociodemographic data were collected at the baseline time point and included child gender (0 = male; 1 = female), maternal education level (0 = high school/General Educational Development [GED] or less, 1 = more than high school education), income level (ordinal variable ranging from less than US$10,000 to US$40,000 or more), employment (0 = yes, 1 = no), marital status (0 = single, 1 = not single), as well as child age that was treated as a continuous variable.
Asthma Severity
Asthma severity was measured at baseline enrollment using National Asthma Education and Prevention Program (NAEPP) Guidelines (USDHHS, 2007). Caregivers reported on their child’s symptoms days and nights over the prior 14 days and nights over the previous 30 days, and child activity limitations due to asthma. Children were categorized as mild intermittent, mild persistent, moderate persistent, or severe persistent, with mild intermittent used as the reference group in the analyses.
Asthma Control
Asthma control, a measure of impairment and risk, was assessed at each data collection time point and per NAEPP Guidelines was based on caregiver report of daytime and nighttime frequency of symptoms of coughing, wheezing, and shortness of breath or difficulty breathing and albuterol use in the past 2 weeks (USDHHS, 2007). Children were categorized as poorly controlled, not well controlled, or well controlled.
Social Support–Emotional/Informational
Social support was measured at all time points using an eight-item subscale from the Medical Outcomes Study that focuses on the availability of emotional/informational support (Sherbourne & Stewart, 1991) The 5-point Likert-type scale has scores ranging from 8 to 40, where higher values indicate greater perceived social support. The baseline internal consistency for this study was .95.
Stress Variables
Caregivers were administered two measures of stress at each data collection period. Caregiver life stress was assessed using a 10-point Visual Analog Scale (VAS). The mothers reported their perceived level of daily life stress on a scale of 1 to 10 with “1” defined as no stress at all to “10” reflecting the highest level of stress. Asthma management stress, defined as stress related to caring for a child with asthma, was also assessed using a 10-point VAS. The anchors included “1” defined as no stress at all to “10” reflecting the highest level of stress. The psychometric qualities of the VAS have been studied by Lesage and colleagues who found evidence of interconcept validity and discriminative sensitivity (Lesage & Berjot, 2011; Lesage, Berjot, & Deschamps, 2012). The VAS has also been used in a community study of older adults living with HIV and found to have a positive relationship with the Perceived Stress Score (Webel et al., 2014).
Depressive Symptoms
Maternal depressive symptomatology was ascertained using the 20-item self-report Center for Epidemiologic Studies–Depression Scale (CES-D) at each data point (Radloff, 1977). Respondents identify the frequency of symptoms within the past week using a scale of 0 to 7 days with the following responses: 0 = less than a day, 1 = 1 to 2 days, 2 = 3 to 4 days, and 3 = 5 to 7 days. The total summed score on all 20 items is used to measure levels of depressive symptomatology in general populations in the community as well as in psychiatric populations. The total score is treated as a continuous variable in our analyses but in addition it was coded as a dichotomous variable based on CES-D scores (0 for a total score <16 and 1 for ≥16) with a score of 16 often indicating clinically significant depression (Radloff, 1977) for descriptive purposes. The CES-D has excellent internal consistency (Cronbach’s α >.85) and has shown high sensitivity (.95) and specificity (.70) in predicting depressive disorders in low-income minority women (Myers & Weissman, 1980; Thomas, Jones, Scarinci, Mehan, & Brantley, 2001). The internal consistency for the current study was .89.
Data Analysis
The outcome variable of interest was the level of maternal depressive symptomatology, measured at baseline (T1), 6 months (T2), and 12 months (T3). Control variables measured at (T1) were treatment group assignment (intervention vs. attention control), child’s age, mother’s education level, marital status, employment, and asthma severity. Time-varying covariates in the model were measured (T1), (T2), and (T3) and included social support, daily life stress, asthma caregiving stress, and asthma control level. No evidence of multicollinearity was observed among the continuous predictors entering the model (highest correlation was for daily life stress and asthma caregiving stress at T3, r = .44). Results are reported using an alpha level of .10 with associated 95% confidence intervals.
Latent growth curve modeling (LGCM) using Mplus Version 6 was performed to examine changes in maternal depressive symptomatology over time (Muthén & Muthén, 2011; Preacher & Coffman, 2006). Data in LGCM are described by latent change factors (i.e., means and slopes) that estimate both group-level change and individual-level change. Intercept values were estimated by fixing factor loadings at each time point to 1. Values were then estimated by assigning fixed factor loading representing time (baseline, T1; 6 months, T2; 12 months, T3). Maximum-likelihood estimation with robust standard errors (MLR) was used to address missing data that never exceeded 10% for any variable. Based on α = .05 and β = .80, a priori power analysis indicated a minimum sample of 217 for testing the structure of the LGCM (root mean square error of approximation [RMSEA] < .10), and a minimum sample of 152 for testing individual parameters (b > 0; Preacher & Coffman, 2006).
The fit of the model to the data was estimated using both sample- and population-based indices (Hu & Bentler, 1999). Sample-based indices used were the chi-square test of goodness of fit, the relative chi-square statistic that accounts for sample size, the Akaike information criteria (AIC), and the standardized root mean square residual (SRMR); ratios of 3:1 for the relative chi-square are indicative of good fit, lower AIC values indicate improved fit between nested models, and an SRMR < .08 is indicative of good fit. Population-based indices used were the RMSEA, with values <.06 preferred, and the comparative fit index (CFI) and the Tucker–Lewis index (TLI) with preferred values over 0.90.
Results
Maternal and Child Demographic Characteristics
Maternal and child characteristics are seen in Table 1. The children (N = 276) were primarily male (59%), African American (96%), with an average age of 5.9 years (range = 3-10). The maternal caregivers were predominantly single (73%), unemployed (45%), and completed a high school education or higher (71%). The majority (51.7%) earned less than US$10,000 per year. Selected health, stress, and social support characteristics are presented in Tables 2 and 3. Asthma morbidity of the children was high and consistent with expectations based on study eligibility criteria. The children were predominantly categorized with severe persistent asthma (n = 109, 39.8%), followed by mild persistent (n = 104, 38%), moderate persistent (n = 48, 17.5%), and mild intermittent (n = 13, 4.7%). Asthma control improved over the 12 months (Table 3) with the number of children characterized as having poorly controlled asthma decreasing from 93.8% at T1 to 61.6% at T2 and T3.
Demographic Characteristics of 276 Children and Mothers.
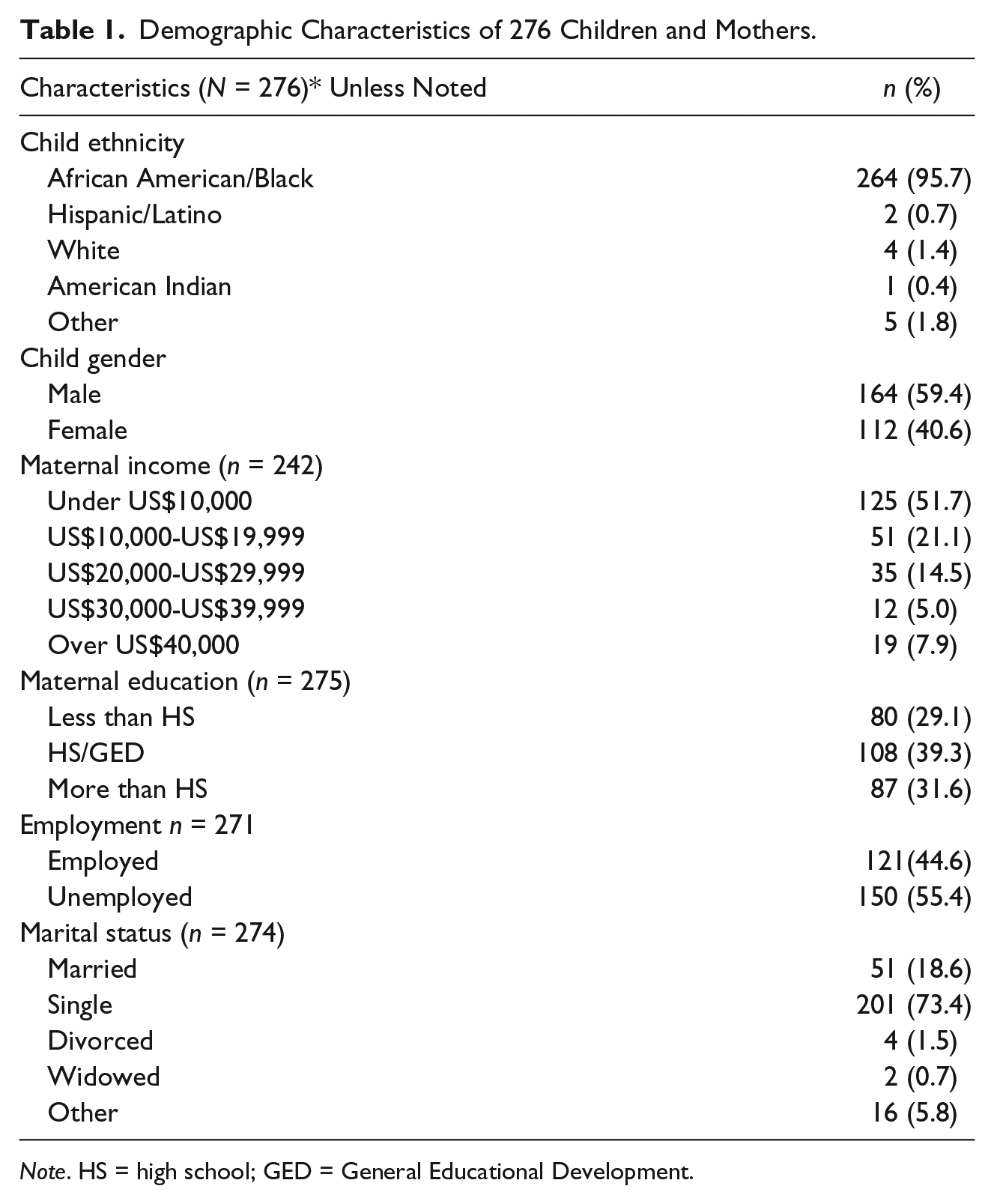
Note. HS = high school; GED = General Educational Development.
Changes in Mean CES-D, Stress, and Social Support Scores Over Time.
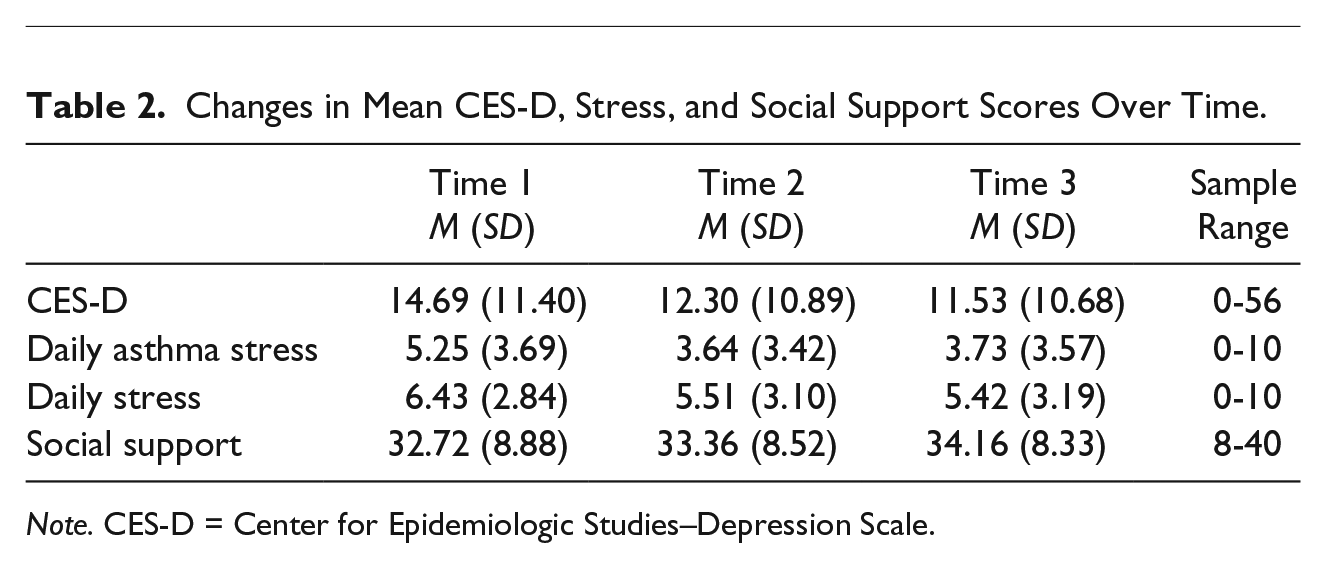
Note. CES-D = Center for Epidemiologic Studies–Depression Scale.
Descriptive Statistics for Asthma Severity, Asthma Control, and CES-D Over Time.
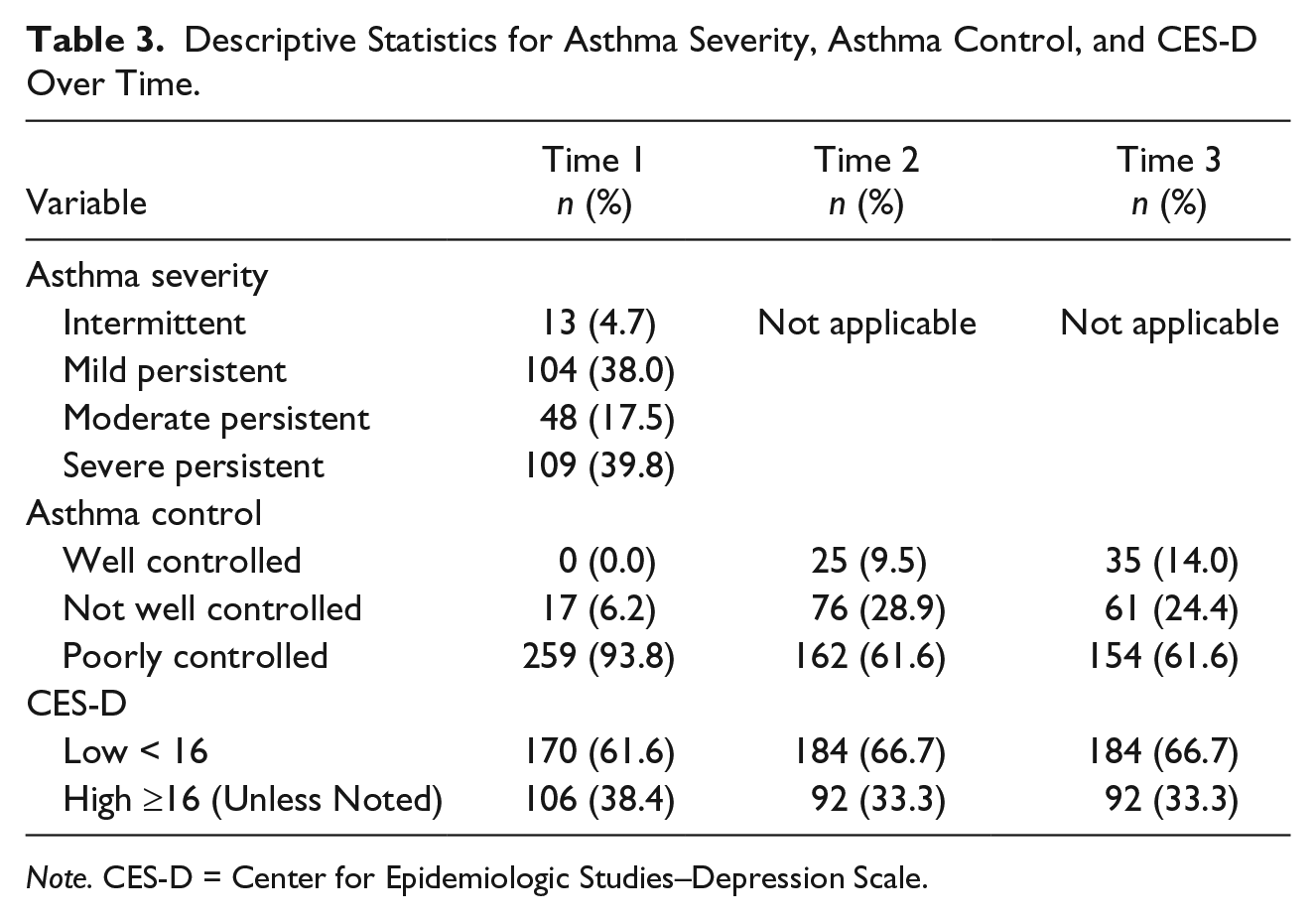
Note. CES-D = Center for Epidemiologic Studies–Depression Scale.
The presence of clinically significant scores on the CES-D (16 or higher) varied between 38% at T1 to 33% at both T2 and T3 time points. On average, CES-D mean scores in the full sample decreased over time from 14.70 (SD = 11.55) at T1 to 12.47 (SD = 10.77) at T2 to 11.69 (SD = 10.66) at T3, with statistically significant differences between T1 and T2 (p < .001) and between T1 and T3 (p < .001). Caregiver Daily Stress scores also decreased from T1 (M = 6.43, SD = 2.86) to T2 (M = 5.57, SD = 3.11) to T3 (M = 5.36, SD = 3.19); changes in mean scores between T1 and T2 and between T1 and T3 were significant (p < .001 for both). Asthma caregiving stress demonstrated a similar trend with a baseline mean of 5.23 (SD = 3.70), a T2 mean of 3.66 (SD = 3.46), and a T3 mean of 3.72 (SD = 3.54); significant decreases in mean scores were observed between T1 and T2 as well as T1 and T3 (p < .001 for both). Small but statistically significant improvements in mean social support scores were also observed between T1 (M = 32.72, SD = 8.88) and T3 (M = 34.36, SD = 8.18; p = .003) and between T2 (M = 33.56, SD = 8.53) and T3 (p = .04).
LGCM Results
LGCM analysis was used to assess changes in maternal depressive symptomatology over time as a function of daily life stress, asthma caregiving stress, asthma control, and social support. An unconditional model using only depressive symptoms over time was tested first. Results for the intercept and slope were 14.41 (p < .001) and −1.75 (p = .08), respectively, indicating that the mean depressive symptom score was greater than 0 over time; the average slope was negative, suggesting a decrease in depression scores over time. Baseline control variables and time-varying covariates were added to create a second latent growth curve (LGC) model. Results for the second model indicate acceptable fit as evidenced by an RMSEA of .06, high values for CFI (.93) and TFI (.86), and an SRMR of 0.03. Results for the second model show a significant positive intercept (I = 13.07, p = .03) and a positive but nonsignificant slope (S = 5.55, p = .14), suggesting no significant variation in depression scores after adding time-varying covariates to the model. The only significant parameter estimates for the control variables were a positive slope for the intervention group (b = 1.39, p = .04), suggesting increasing depressive symptom scores for mothers randomized to the intervention group relative to mothers in the control group and a negative slope for employment (b = −1.48, p = .04), which reflects decreasing depressive scores over time for unemployed mothers relative to mothers who were working. The absence of significant relationships between depressive scores slope and intercept with child age, gender, income, education, marital status, or asthma severity suggests changes in depressive symptoms over time are not affected by these control variables.
Although the time-varying factors (stress, social support, asthma control) did not predict change in depressive symptoms over the 12 months (slope = 5.55, p = .14), we were also interested in the relationship of these factors to caregiver symptomatology at each distinct data collection period. Higher daily life stress was significantly associated with increased maternal depressive symptoms at T1 (b = 1.87, p < .001), T2 (b = 1.42, p < .001), and T3 (b = 0.94, p < .001). Asthma caregiving stress was not associated with maternal depression at T1 (b = 0.01, p < .96) or T2 (b = −0.09, p = .63); however, a significant relationship between asthma stress and maternal depressive symptomatology was found at T3 (b = 0.41, p < .02), with higher asthma stress predictive of greater depressive symptomatology. Asthma control level was not associated with depression scores at any time point (p > .05). However, higher social support was significantly associated with lower maternal depressive symptomatology at all three time points; b = −0.29 (p < .001) at baseline (T1), b = −0.24 (p < .001) at 6 months (T2), and b = −0.39 (p < .01) at 12 months (T3).
Discussion
Study findings highlight the chronic nature of depressive symptoms in low-income, inner-city caregivers of children with poorly controlled asthma. Over one third of caregivers of young children with asthma reported significant depressive symptomatology across the three time points (33%-38%; Horwitz, Briggs-Gowan, Storfer-Isser, & Carter, 2007). Our observed rate of clinically significant depressive symptoms is greater than what was found in a comparable population (25%; Kub et al., 2009) but less than other research using an 11-item version of the CES-D in which nearly half (47%) of caregivers endorsed clinically significant levels of depressive symptomatology (Bartlett et al., 2001). Moreover, the reported prevalence rates are notably higher than what was found in other research with low-income mothers with young children. In a 5-year study of impoverished African American families, Manuel and colleagues (2012) found maternal depression varied between 15% and 21% over time. Minkovitz and colleagues (2005) observed a comparable rate variation (15.5%-17.8%) in mothers of children followed from birth to age 3.
A novel aim of our study is its focus on elucidating factors driving change in depressive symptomatology over time. However, the selected sociodemographic, asthma caregiving stress, life stress, and social support variables failed to achieve significance in explaining change in depressive symptoms across the 12-month study period. This finding was unexpected and it is most likely attributed to the statistically significant but small differences in depressive symptoms over time in our sample. That is, as caregiver depressive symptoms remained relatively stable across the 12-month follow-up, especially from T2 (6-months) to T3 (12-months), variability in the sample was quite restricted and offered little opportunity for the selected variables to predict change in depressive symptoms. Instead, each factor entering the model explained a portion of the observed variance in depressive symptoms. However, caregiver employment status did predict change in symptomatology, with employed mothers experiencing more depressive symptoms over time. It is possible that the elevated symptom level reflects stress associated with meeting employment demands while also parenting a child with high-risk asthma. Another explanation is that maintaining employment and managing a child’s asthma may be especially challenging for this sample of women who are primarily single parents.
A notable strength of our study findings is that at each distinct time, the model was a good fit to the data. Specifically, R2 values were high (T1 = 56%, T2 = 56%, T3 = 59%), indicating the model was very predictive of CES-D scores. Caregiver perception of daily life stress in particular was the strongest predictor of caregiver depressive symptoms. Other studies of low-income urban mothers similarly found life stressors and chronic stressors linked to depressive symptoms (Kub et al., 2009; Manuel et al., 2012; Shalowitz et al., 2006). Poverty and substandard housing in underresourced communities are often significant predictors of depression (Suglia, Duarte, & Sandel, 2011). Among 824 African American mothers living in the poorest census tracts in Detroit, risk factors for depressive symptoms included food insufficiency and deteriorated housing (Siefert et al., 2007).
The observed associations among child asthma severity, asthma control level, asthma caregiving stress, and caregiver depressive symptoms were also intriguing. Baseline asthma severity was not predictive of caregiver depressive symptoms, nor did we observe a relationship between asthma control and depression at any of the data points. In contrast, a modest association between perception of asthma stress and depression was found at the 12-month time point. It is unclear as to why asthma stress was significant only at the 12-month time point unless it could be related to ending of the study and support of the home visiting nurses that both groups of study participants received. Perceptions of asthma stress may not reflect disease severity or level of control but could perhaps relate to practical problems related to care of children with a chronic illness such as obtaining medication fills, maintaining health insurance coverage and adhering to medical appointments (van Oers et al., 2014). These findings differ from our previous research on quality of life (QOL) outcomes in this population in which impaired QOL was associated with poor asthma control (Bellin et al., 2015). Studies have also found that illness-related characteristics of the child were not related to anxiety or depression in mothers or fathers. In a sample of mothers bringing their children to an ED with low acuity illness, mothers reported poorer health status for themselves but not their children (Grupp-Phelan, Whitaker, & Naish, 2003). Tu and colleagues studied 1,696 mother–child dyads examining the relationship of maternal depressive symptoms and child asthma attacks over time. For the mothers with no depressive symptoms at 5 months, child asthma attacks since birth did not contribute to new depressive symptoms 1 year later. Poverty, however, was linked to increased maternal depressive symptoms (Tu, Perreault, Séguin, & Gauvin, 2011). Our finding that asthma control was not predictive of depressive symptoms at any time point lends further support to our position that health status indictors are not necessarily the driving force of psychological symptoms in this caregiver population, rather daily “life” stress may be the major contributor to maternal depression.
Similar to other studies, we observed social support to predict caregiver depressive symptoms across time. In our sample of impoverished caregivers of children with poorly controlled asthma, greater access to emotional/informational support was associated with lower depressive symptoms at each time point. These findings support previous work among low-income mothers, which have found both from qualitative and quantitative studies that a persistent theme for low-income mothers is a protective influence of informational support and emotional support on health outcomes (Dyer, Stein, Rice, & Rotheram-Borus, 2012; Israel, Farquhar, Schulz, James, & Parker, 2002; Keating-Lefler, Hudson, Campbell-Grossman, Fleck, & Westfall, 2004).
There are potential limitations associated with this study. Generalizability of the findings may be limited due to the purposeful selection of families of children with poorly controlled asthma (Bellin, Osteen, Collins, Butz, & Kub, 2014). It is possible that model results may differ among caregivers of children with controlled asthma. In addition, our sample was comprised of mothers who could be followed over 12-months and thus, it may not represent the larger population of low-income inner-city caregivers. Given the reliance on self-report data, it is possible that same source bias may have contributed to the observed significant findings. In addition, the use of a single global indicator of daily life stress may limit the ability to ascertain the particular stressors linked to depressive symptoms. The contextual factors affecting inner-city families are diverse in scope and include housing instability, exposure to pollution, rodent and cockroach infestation in home dwellings, food and utilities insecurity, residence in high crime areas, parenting stresses, and poor physical health (Cadigan & Skinner, 2015; Manuel et al., 2012; Matheson et al., 2006). We were unable to address all contextual factors in this study. To effectively build tailored practice interventions among caregivers experiencing depressive symptoms, teasing out the particular sources of daily life stress is needed.
Assessing the prevalence and chronicity of depressive symptoms in low-income mothers is important in understanding asthma morbidity in children. Over a decade ago, mothers reported that their own mental health symptoms affect their ability to care for their children (Grupp-Phelan et al., 2003). Routine assessments of stress levels and changes in family roles and routines may be an important step in determining if caregivers could benefit from a referral to psychological services (Bowden et al., 2015). Screening questions to assess depressive symptoms in EDs or primary care practices have been recommended since 2008 by the American Academy of Pediatrics Task Force and the Bright Futures practice guidelines (Pak & Allen, 2012). Given our findings of a chronic nature of depressive symptoms in mothers of children with poorly controlled asthma, regular assessment of caregiver symptoms in clinical encounters with this population is critical. A single assessment during an initial intake visit with the family may not be sufficient. Instead, integrating questions about caregiver psychological state across all clinical encounters with the family is indicated, especially for working single mothers. With the growing emphasis on home visits for management of chronic diseases such as asthma, there is an opportunity to build these assessments into home visiting protocols as well as make referrals to community-based resources to reduce experiences of life stress. Finally, it is important for health care providers to remember that families are dealing with multiple levels of life stress and that caring for a child with a chronic illness is just one stressor. It would be important to remedy those stresses associated with child care as much as possible. From a practical perspective, it may include readjusting clinic schedules to better accommodate families’ schedules (Malm-Buatsi et al., 2015).
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by a National Institute of Nursing Research, National Institutes of Health (NIH) Grant NR010546.