
Abstract
A recent increase in children living with grandparents places more children at increased risk for emotional, psychological, or behavioral problems. This study used the Resiliency Model of Family Stress, Adjustment, and Adaptation to examine how children’s living situation, parental monitoring, child’s resourcefulness, and perceived support affect depressive symptoms and perceived family functioning. Of participants, 36% (n = 56) lived with their parents only, 44% (n = 69) lived with a grandmother as their primary caregiver, and 20% (n = 31) lived in a multigenerational household. Results indicate parental monitoring and support affected perceptions of family functioning. Subjective support and resourcefulness affected depressive symptoms. No effects were found from living situation and demographic factors. Resourcefulness had the strongest effect on depressive symptoms, with a 3-point decrease in symptoms for each incremental increase in resourcefulness. This study provides insight into factors influencing children’s depressive symptoms and perceived family functioning, and provides direction for the development of future interventions.
Keywords
According to 2014 U.S. Census data, 4.8 million children are being raised in some capacity by their grandparents, a number that has significantly increased since the 2000 Census report (U.S. Census Bureau, 2016). Child protective services have increased their reliance on grandparents to care for children removed from the home as an alternative to placing the child in foster care (Winokur, 2009). The conditions and adverse life events that result in children being raised without parents in their grandparent’s home, such as trauma, incarceration, prenatal exposure to drugs or alcohol, and poor parental attachment, place these children at increased risk for emotional, psychological, or behavioral problems that create challenges for how well the family functions (Kelley, Whitley, & Campos, 2011; Scarcella, Ehrle, & Geen, 2003). Grandchildren who are raised by their grandparents are more likely to demonstrate poor mental health, emotional symptoms, conduct problems, hyperactivity, inattention, peer conflict, and aggression compared with their peers (Dunifon, 2013; Goodman, 2012; Scarcella et al., 2003). Protective factors such as parental monitoring, child resourcefulness, and social support may reduce psychological problems in the grandchild and improve how the family functions (Armstrong, Birnie-Lefcovitch, & Ungar, 2005; Yu et al., 2006; Zauszniewski, Bekhet, & Bonham, 2010). There has been a wealth of research examining the impact of grandchild caregiving on grandmothers, but less attention has focused on the grandchildren’s outcomes related to their living situation. This is critical, because children’s living situation and personal and social resources can have a direct impact on their behavior and influence how they perceive their situation (Vingilis, Wade, & Seeley, 2002). Thus, the purpose of this study was to examine how grandchildren’s living situation (being raised by grandmother, living in a three-generation home, or living in a separate residence from grandmother) affects grandchildren’s depressive symptoms and perceptions of family functioning, and whether parental monitoring, child’s resourcefulness, and perceived support influence these outcomes.
Living Situation
A child’s living situation affects his or her well-being. Nearly one third of grandchildren raised by grandmothers have mental health problems, including internalizing behaviors such as social withdrawal, depression, inattention, hyperactivity, and anxiety, or externalizing behaviors such as noncompliance, conduct problems, and aggression (Dunifon, 2013; Goodman, 2012; Scarcella et al., 2003; Smith & Palmieri, 2007). These problems directly affect the child’s academic functioning and ability to form positive attachments with peers and other adult figures (DeSocio & Hootman, 2004). Adolescents in families with married biological parents report more parental monitoring and less family conflict than children not living with their biological parents (Shek, Xie, & Lin, 2014; Wagner et al., 2010). They also have less depression, fewer emotional problems, and better overall health than children living in single-parent homes or with grandparents but not parents (Bramlett & Blumberg, 2007). There have been few studies comparing well-being in children raised by grandparents, often grandmothers only, with children living in three-generation homes, or with parents apart from grandparents, as this article does.
Depressive Symptoms
According to the Centers for Disease Control and Prevention (2013), one in five children living in the United States experiences a mental health disorder, and about 2% of children 3 to 17 years of age are clinically depressed. The 2011-2012 National Survey of Children’s Health identified factors associated with childhood emotional problems: being non-Hispanic White, female, older, and facing adverse circumstances (e.g., living with someone with mental illness or drug and alcohol problems, experiencing parental death, incarceration or divorce, or witnessing domestic violence; Balistreri & Alvira-Hammond, 2016). While these problems are not unique to children being raised by grandparents, many children raised by grandparents have experienced these circumstances that can increase their risk for psychological distress compared with children in the general population (Goodman, 2012; O’Hora, Dolbin-MacNab, & Tech, 2015; Poehlmann, 2003; Smith & Palmieri, 2007). Furthermore, many grandchildren raised by grandparents feel neglected and abandoned by their parents and presume that they are a stressor to them (Kelley et al., 2011).
Children with psychological distress, fewer family resources, and less supportive home environments have shown high internalizing and externalizing behavioral problems (Kelley et al., 2011). Regardless of gender, custodial grandchildren showed more behavior and emotional problems than normative samples (Smith & Palmieri, 2007). Among children raised by grandparents, disrupted family processes were associated with more mental health symptoms in youth across gender and race (Yorgason et al., 2014). For children raised by grandmothers, the grandmother’s mental health and a structured home environment supporting appropriate behavior and academic success had a positive impact on grandchildren’s behavior and protected against the development of psychological disorders (Goodman, 2012; Pilkauskas & Dunifon, 2016).
Family Functioning
Children’s and adolescent’s perceptions of their family’s functioning are associated with their mental health. Among high school students, worse family functioning was associated with greater depression, suicidal ideations, and intentional self-harm behaviors (Martin, Rotaries, Pearce, & Allison, 1995). Adolescent-reported perceptions of their family’s functioning accounted for a significant amount of variance in their depressive symptoms and self-esteem (Ciao, Accurso, Fitzsimmons-Craft, Lock, & Le Grange, 2015). In their qualitative study of 20 adolescents raised by grandmothers, Downie, Hay, Horner, Wichmann, and Hislop (2010) identified that concerns about their grandmother’s health and financial and environmental stresses, and difficulties adjusting to the grandmother’s parenting style may affect older children’s mental health and influence their perceptions of how their family functions. Despite feeling rejected by their parents, many identify their grandmothers as the most constant, stable person in their lives and demonstrate resilience (Sands, Goldberg-Glen, & Shin, 2009).
Parental/Guardian Monitoring and Support
Practices such as parental monitoring and providing support are important modifiable behaviors that present opportunities for the parent or guardian to have a positive impact on a child’s well-being (Coley & Hoffman, 1996; Dishion, Nelson, & Kavanagh, 2003; Yap & Jorm, 2015; Yap, Pilkington, Ryan, Kelly, & Jorm, 2014; Zhou, Sandler, Millsap, Wolchik, & Dawson-McClure, 2008). Lowe and Dotterer (2013) found that youth who identified having a positive warm relationship with either their mother or father also reported having higher levels of parental monitoring, intrinsic motivation, and lower levels of school trouble. To date, little research has compared family functioning of youth being raised by their grandmothers as primary caregiver with those who live in homes with multiple adult generations or their parents.
Parental monitoring is defined as a guardian’s knowledge of their child’s whereabouts, peer groups, school activities, and use of free time, and it includes parents establishing expectations, boundaries, and consequences for socially unacceptable behaviors (Bacchini, Concetta, & Affuso, 2011; Lowe & Dotterer, 2013). Parental monitoring is recognized as a critical parenting practice for effective child adaptive outcomes (Coley & Hoffman, 1996; Dishion et al., 2003; Lowe & Dotterer, 2013; Slesnik et al., 2012; Yu et al., 2006). Teens who reported higher levels of family functioning also reported more interpersonal connectedness and satisfaction with their parent–child relationship (Slesnik et al., 2012). Adolescents at high risk for behavioral problems are those who spend time with peers in unsupervised setting and live in homes with lower levels of parental monitoring (Bacchini et al., 2011; Pettit, Bates, Dodge, & Meece, 1999). Parental monitoring and less exposure to violence predicted less violent behaviors by elementary and middle school children (Singer, Flannery, Guo, Miller, & Leibbrandt, 2004).
There is evidence to suggest that parental monitoring influences mental health outcomes (Bacchini et al., 2011; Dillon, Pantin, Robbins, & Szapocznik, 2008). The emotional and interactional quality of the parent–child relationship shapes the structure of the family and influences the way the child learns to regulate and express their emotions (Schwartz et al., 2012). Schwartz et al. (2012) reported that higher levels of parental aggressive behavior, in contrast to positive parental behaviors, predicted higher levels of depression and anxiety in adolescents. Parenting strategies focused on warmth, parental monitoring, peer groups, discipline, communication, healthy behavior, and good academic performance are essential in reducing adolescent risk for depression or anxiety disorder (Yap et al., 2014).
Resourcefulness
Resourcefulness refers to a set of cognitive-behavioral self-help skills (positive thinking, goal setting, problem solving, planning, and cognitive reframing) that enhance one’s ability to cope with adversity (Rosenbaum, 1980; Zauszniewski, 1995; Zauszniewski & Bekhet, 2011). Resourcefulness is hypothesized to improve one’s capacity to manage stress and thus reduce the effects of family demands on depressive symptoms and overall functioning (Musil, Zauszniewski, Burant, Toly, & Warner, 2015; Rosenbaum, 1980; Zauszniewski, 1995). In adolescents and school-aged children, greater resourcefulness has been associated with fewer depressive symptoms and the ability to deal more effectively with stress (Chang, Zauszniewski, Heinzer, Musil, & Tsai, 2007). Resourcefulness skills can be taught (Rosenbaum, 1990) and may be a potential intervention for children at risk for depression and problems in family functioning. Ronen and Rosenbaum (2009) taught resourcefulness skills to a group of highly aggressive ninth graders, and the intervention group demonstrated reduced objective and subjective aggression rates compared with baseline and control group; thus, resourcefulness might be a potential intervention strategy with these children and adolescents.
Conceptual Framework
This study used the Resiliency Model of Family Stress, Adjustment, and Adaptation to conceptualize how the stressors placed on the family system might influence the well-being of children based on the context of their living situation. The model considers the challenges and demands that family systems experience and how resources and problem solving/coping can affect individual or family adaptation and well-being (McCubbin, Thompson, & McCubbin, 1996). According to this model, a failure to alleviate or resolve family demands through resources (social support and parental monitoring) and coping (resourcefulness skills) may increase the likelihood of negative outcomes such as compromised mental health and poor family functioning. Therefore, we hypothesized that greater support, parental monitoring, and higher resourcefulness would be associated with fewer depressive symptoms and fewer problems in family functioning, regardless of family structure.
Method
Design
This is a secondary data analysis from the fourth wave of an Institutional Review Board (IRB) approved longitudinal study that examined the health and well-being of Ohio grandmothers; grandchildren were included at the fourth-time wave. At this time wave, we recruited grandchildren of study participants and asked the grandchildren about social support, depressive symptoms, family functioning, resourcefulness, and parental monitoring. These findings have not been reported elsewhere.
Sampling
Grandmothers from an ongoing National Institutes of Health (NIH)-funded study of grandmothers as caregivers to grandchildren were contacted about potentially enrolling their grandchildren in an expansion of the original study. Grandchild recruitment entailed obtaining information from the grandmothers about the grandchild and the child’s guardian, followed by letters to the grandchild’s guardian and the grandchild, an opt-out postcard, and, for those interested in participating, a written informed consent for the guardian and a child assent form.
In total, 171 grandmothers enrolled in the study provided one or more names of grandchildren who were under the age of 16 as potential participants, from which 281 recruitment letters were sent to parents/guardians. Of the parent/guardians, some were grandmother study participants raising their grandchildren, others were parents living in a multigenerational home with the grandmother and grandchild, and some were parents who lived with their children apart from the grandmother. Inclusion criteria were as follows: grandchild of a grandmother enrolled in the larger study, age 8 to 19, parent/guardian consent and grandchild assent to participate, and ability to read and write English, and understand the study questions.
Recruitment of children was a challenge; some grandchildren were too young to participate, others had aged out of study eligibility, and some parents/guardians were reluctant to have their children participate even though the children’s grandmothers were study participants. To facilitate parent/guardian understanding of the request, sample surveys were sent with the original mailings to grandchildren so that parents and/or guardians could preview the surveys prior to the interview. From this, 157 grandchildren completed Time 1 surveys, representing 89 distinct families. Most surveys (n = 125) were returned by mail and the rest (n = 32) were completed by phone as originally planned, an IRB-approved protocol modification to allow the convenience of mailed responses. Children received a US$15 incentive for completing the questionnaire.
The demographic characteristics of the grandchildren (N = 157) are reported in Table 1. Over half (n = 93; 59%) were female. The sample was composed of adolescent and latency-age children (M = 12.5 years, range = 8-19 years). Nearly half (n = 72; 46%) were being raised by a grandmother, 17% (n = 27) lived in a multigenerational home, and 37% (n = 58) lived with their parents and no grandparents. We used grandmothers’ self-reported race as a possible indicator of grandchild racial background; grandmothers were 67.5% (n = 106) White, and 31.2% (n = 49) non-White, and 1.3% (n = 2) did not report race.
Means and Standard Deviations of Study Variables by Living Situation.
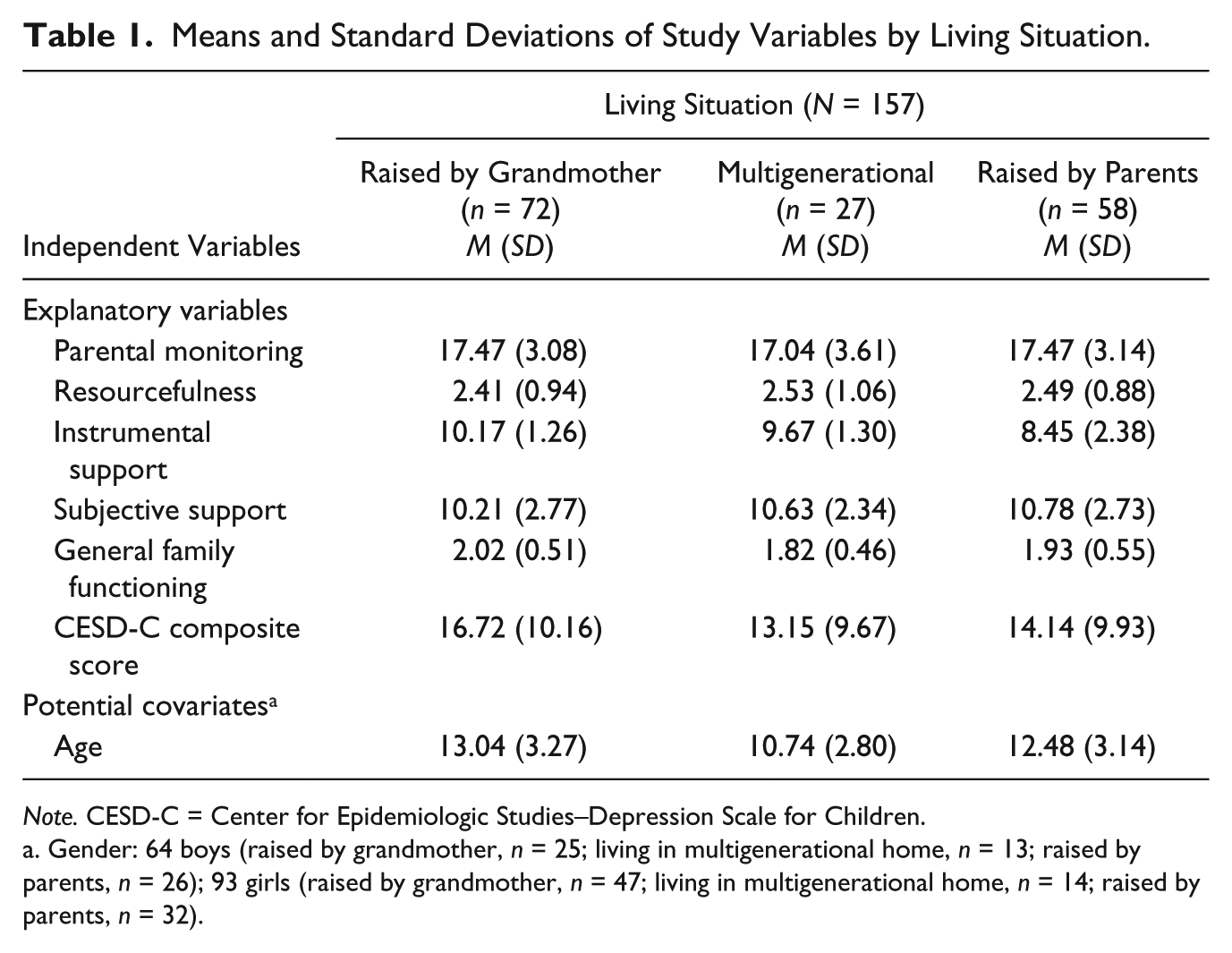
Note. CESD-C = Center for Epidemiologic Studies–Depression Scale for Children.
Gender: 64 boys (raised by grandmother, n = 25; living in multigenerational home, n = 13; raised by parents, n = 26); 93 girls (raised by grandmother, n = 47; living in multigenerational home, n = 14; raised by parents, n = 32).
Measures
All measures were formatted for self-administration and were pilot tested on a convenience sample of racially and ethnically diverse children, aged 8 to 16 years (22 girls and 28 boys), from urban and suburban communities. The pilot indicated that children across a range of age and abilities could complete the questionnaire.
Resourcefulness was measured by the Children’s Resourcefulness Scale (Zauszniewski et al., 2010). Resourcefulness is a learned set of cognitive-behavioral and self-control skills to help individuals deal with life stressors (Zauszniewski et al., 2010). This self-report 10-item scale measures the tendency to use self-control techniques to solve behavioral problems using a 6-point Likert-type scale. Scores range from “not at all like you” to “very much like you,” and questions included items such as “If something is too hard for me, I do something else” and “When I know what I want for my birthday, it’s hard for me to wait until then to get it.” A high composite score indicated greater resourcefulness (Zauszniewski et al., 2010). This scale demonstrated acceptable reliability and validity with a Cronbach’s alpha of .72.
Social Support was measured by the Duke Social Support Index (DSSI) using two subscales: Subjective Social Support (seven items) and Instrumental Support (12 items) (Koenig et al., 1993). Originally designed to assess older adults’ perceptions, the index is easy to use and measures subjective support with questions such as “Do you feel listened to by family and friends?” and “Do family and friends understand you?” with response options of “hardly ever,” “some of the time,” or “most of the time.” The Instrumental Support subscale asks, “Do family and friend ever help you out in the following ways?” such as “help you out with money?” “provide companionship to you?” and “prepare or provide meals for you?” with response options of “yes” or “no” for each. Cronbach’s alpha was .75 for the Instrumental and .67 for Subjective Support, consistent with other studies (Saameño, Sánchez, Castillo, & Claret, 1996).
Family Functioning was measured by the General Family Functioning subscale of the McMaster Family Assessment Device (MFAD; Baños, 2011; Epstein, Baldwin, & Bishop, 1983; Ridenour, Daley, & Reich, 1999). Respondents rated 12 statements according to how well they describe their family, using a 4-point Likert-type scale, with responses of “strongly agree,” “agree,” “disagree,” and “strongly disagree” (Baños, 2011; Epstein et al., 1983); higher scores represent more problems in family functioning. Cronbach’s alpha was .70 in this study. The FAD has been used with children and has shown adequate test–retest reliability, criterion validity in dysfunctional families, and sensitivity and specificity with adults and children (Bihum, Wamboldt, Gavin, & Wamboldt, 2002; Miller, Epstein, Bishop, & Keitner, 1985).
Parental/Guardian Monitoring was measured by the Parental Monitoring Scale (Singer et al., 2004). Parental monitoring is the degree to which a parent is aware of their children’s whereabouts and social groups (Singer et al., 2004). Respondents rated responses on a 4-point Likert-type scale, with “0” meaning “never/not important” and “3” meaning “always/very important.” This scale has demonstrated consistently good reliability: Cronbach’s alpha of .77 (Singer et al., 2004).
Depressive Symptoms were measured with the Center for Epidemiologic Studies–Depression Scale for Children (CESD-C). This 20-item self-report scale measures depressive symptomatology during the past week in children 7 to 17 years of age (Radloff, 1977). Each item is rated on a 4-point scale, with 0 = rarely or none of the time (less than 1 day) to 3 = most or all of the time (5-7 days). The measure has a cutoff score at which depressive symptoms are considered significant. Higher scores indicated more depressive symptoms. This measure has demonstrated good reliability with a Cronbach’s alpha = .86 and test–retest reliability (r = .85).
Potential covariates included grandchild age (in years), gender, and living situation (being raised by their grandmother, living in a multigenerational home, or living with parents apart from grandparents). Based on expert recommendation, we chose not to ask grandchildren their race but report the race of the grandmothers who participated in the study.
Data Management and Analysis
Data were collected using telephone interviews and written mailed questionnaires. Data were entered into a database using double data entry, cleaned, and assessed for normality. Analysis was conducted with SPSS 23 and included descriptive statistics, reliability analysis, and the SAS mixed model procedure. A mixed model regression approach was used as some families had more than one child respond, and thus the data were not independent. We conducted two sets of mixed model multiple regression analyses. The first model determined how subjective and instrumental support, resourcefulness, and child perceptions of parental monitoring explained grandchild’s (a) depressive symptoms and (b) perceived family functioning. The second mixed model examined whether grandchild age, gender, and living situation (raised by grandmother, living in a multigenerational home, or living with one or more parents apart from a grandmother) confounded the effects identified in the first mixed regression model.
Results
Given that ANOVA is not robust against the violation of the assumption of independence (more than one grandchild in a family may have participated), we do not report F-test statistics comparing the explanatory variables (resourcefulness, parental monitoring, support, depressive symptoms, and family functioning) between grandchildren based on their living situation. There were differences between living situation groups for age; grandchildren living in a multigenerational home were statistically significantly younger (10.74 years) than those being raised by grandmothers (13.04 years) or living with their parents (12.48 years).
Effect of Explanatory Variables on Depressive Symptoms
Table 2 shows the mixed models analyses testing the predictors of depressive symptoms with and without covariates. The explanatory variables remained stable even after covariates were added to the model. Depressive symptoms were inversely affected by resourcefulness (unstandardized B = −3.15, p < .0001) and subjective support (unstandardized B = −1.06, p = .0005), with parental monitoring approaching significance in both models. Resourcefulness had the strongest effect on depressive symptoms. In Model 2, for every incremental increase in resourcefulness, depressive symptoms decreased by 3.15 points. Intraclass correlations (not shown) for the multiple family members were r <.001, indicating no significant family-level effects.
Mixed Models of Depressive Symptoms (CESD-C).
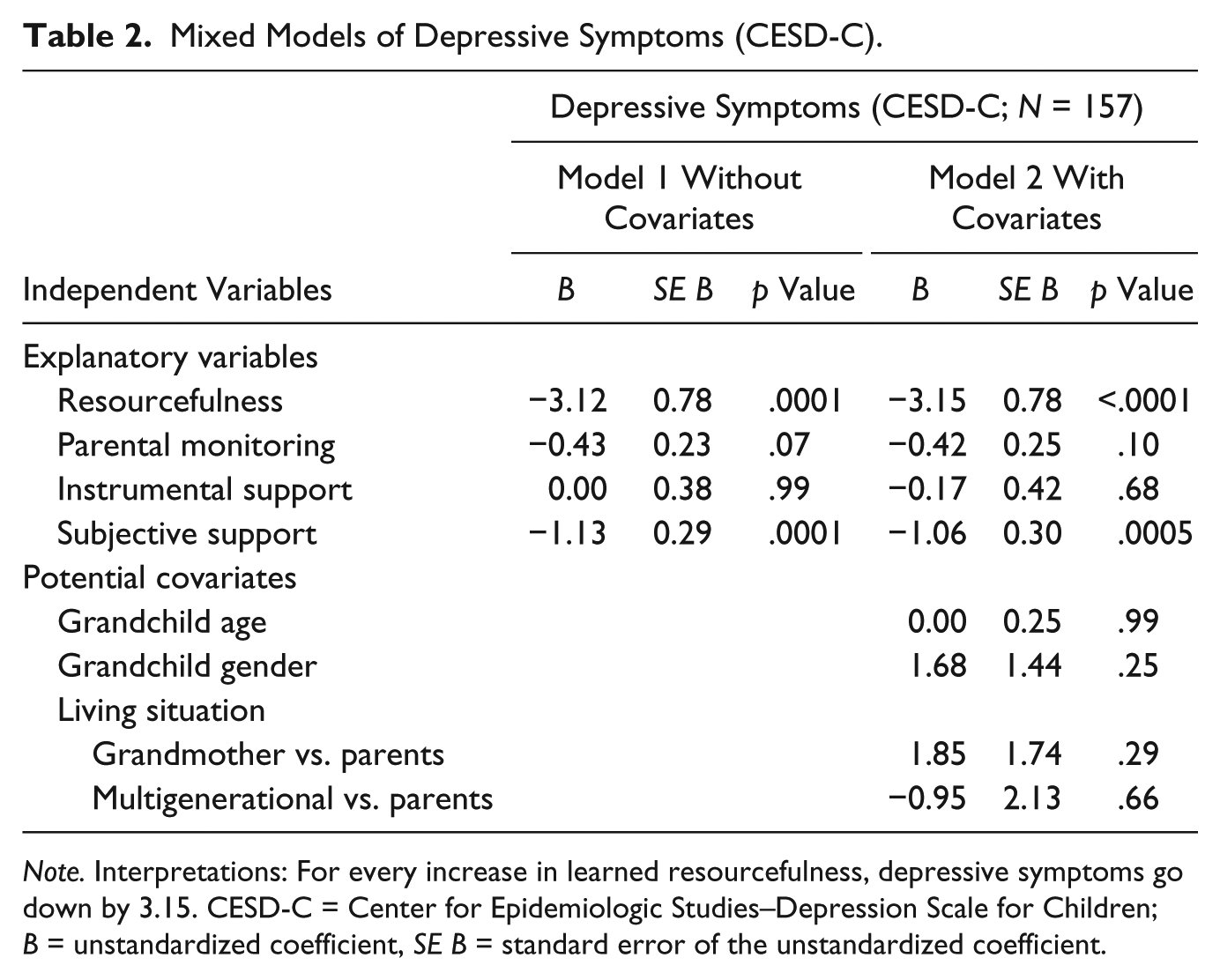
Note. Interpretations: For every increase in learned resourcefulness, depressive symptoms go down by 3.15. CESD-C = Center for Epidemiologic Studies–Depression Scale for Children; B = unstandardized coefficient, SE B = standard error of the unstandardized coefficient.
Effect of Explanatory Variables on Perceived Family Functioning
Table 3 represents the mixed models analyses testing the predictors of perceived family functioning with and without covariates. The explanatory variables remained stable even after covariates were added to the model. Perceptions of more problems in family functioning were modestly influenced by less parental monitoring (unstandardized B = −0.04, p = .007), instrumental social support (unstandardized B = −0.06, p = .005), and subjective social support (unstandardized B = −0.08, p < .0001). The child’s level of resourcefulness approached significance (unstandardized B = −0.07, p = .08). Intraclass correlations (not shown) for multiple family members were r <.001, indicating no significant influence from family-level effects.
Mixed Models of Family Functioning (FAD General Functioning).
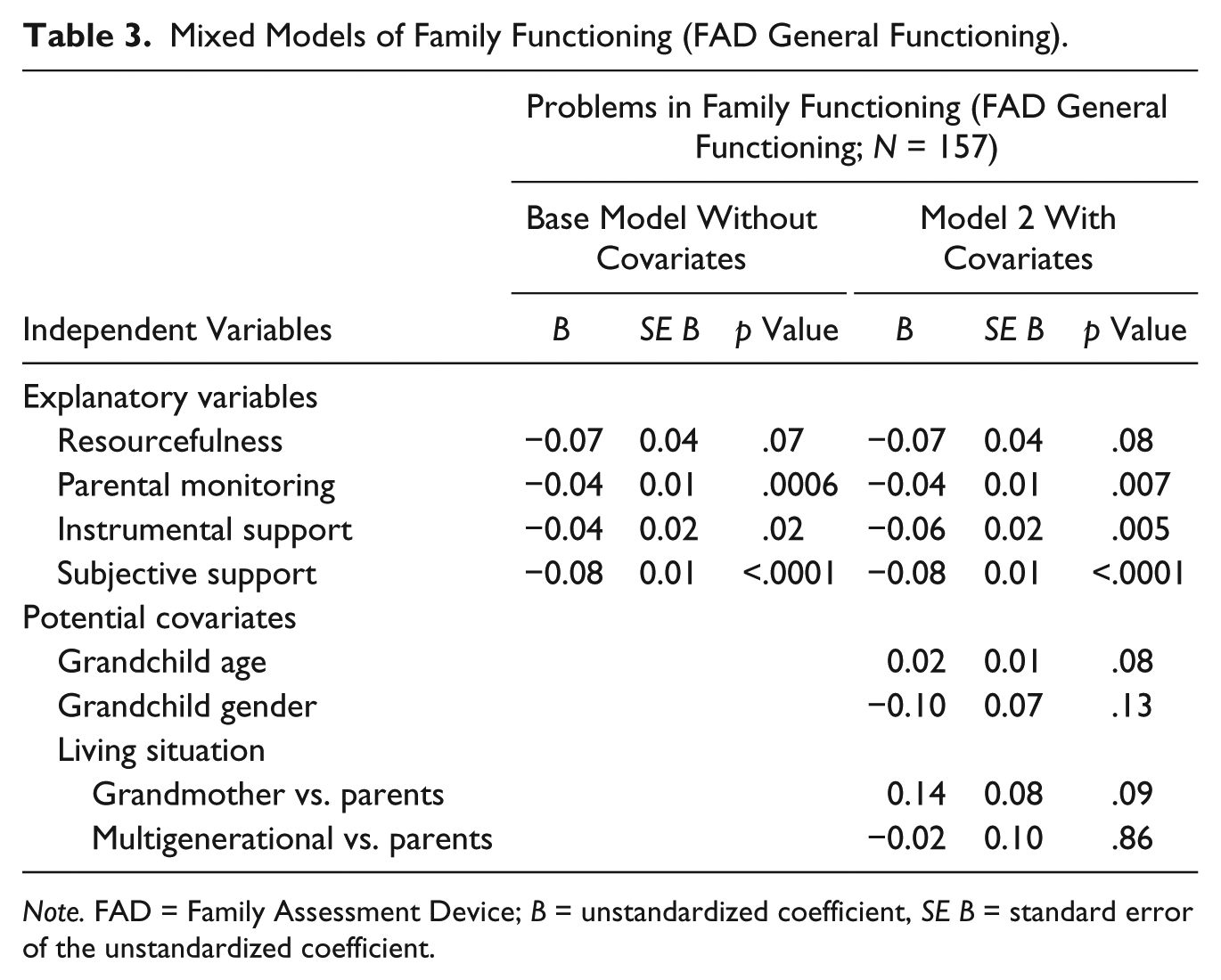
Note. FAD = Family Assessment Device; B = unstandardized coefficient, SE B = standard error of the unstandardized coefficient.
Discussion
We hypothesized that greater support, parental monitoring, and higher resourcefulness would be significantly associated with both fewer depressive symptoms and fewer problems in family functioning. Fewer depressive symptoms were significantly associated with greater subjective support and higher resourcefulness; however, they were not significantly associated with either parental monitoring or instrumental support. Family functioning was significantly associated with parental monitoring, instrumental support, and subjective support; however, resourcefulness did not achieve significance, but the p value could be interpreted as a trend (.08). Thus, the hypotheses related to fewer depressive symptoms were partially supported, and those related to better family functioning were almost fully supported.
The inverse association between resourcefulness and depressive symptoms is well established in samples of young, middle-aged, and older adults in both English-speaking (e.g., Bekhet, 2014; Musil, Jeanblanc, Burant, Zauszniewski, & Warner, 2013; Toly & Musil, 2015) and non-English-speaking (e.g., Chung et al., 2012; Huang, Wang, Lin, & Chen, 2018; Kao et al., 2016) populations. Resourcefulness has been negatively correlated with depressive symptoms in adolescents (Huang & Guo, 2009; Yang, Lai, Yen, Hsu, & Zauszniewski, 2016) and school-aged children (Chang et al., 2007; Zauszniewski et al., 2010). Thus, our study results are consistent with previously reported findings.
In this study, resourcefulness was the strongest predictor of depressive symptoms even in the presence of relevant covariates. This finding has implications for intervention development of resourcefulness skills in children and adolescents to prevent or manage depressive symptoms. The Children’s Resourcefulness Scale used in this study is conceptually different from how resourcefulness in adults has been more recently conceptualized and measured. Specifically, children’s resourcefulness is conceptualized in terms of problem-solving and self-control skills, which would parallel the “personal” resourcefulness component of the adult conceptualization of resourcefulness, which now also includes a “social” resourcefulness component that involves seeking social support (Zauszniewski, Lai, & Tithiphontumrong, 2006). The contribution of both resourcefulness and subjective social support to the explanation of depressive symptoms suggests the concepts are related but not redundant.
Resourcefulness was not found to be as strong of a predictor of family functioning in the study reported here, although the results suggest that there is a trend toward statistical significance. This appears to be the first time that children’s resourcefulness was examined as a predictor of a family outcome. Previous research has examined the relationship between parenting styles and support with children’s or adolescent’s resourcefulness. The children of parents who were more accepting and more involved were more resourceful regardless of the level of supervision or strictness of the parents (Türkel & Tezer, 2008). Williams-Wheeler (2011) reported that children’s resourcefulness could be predicted from the parent’s communication style and reasoning patterns. Leung and He (2010) found a positive association between parental support and greater child resourcefulness. Finally, Preechawong and colleagues (2007) found that family functioning influenced adolescent’s resourcefulness. Our findings may deserve further examination in terms of the directionality of the predictive relationship to disentangle which characteristics of individual family members may affect the family and vice versa.
Subjective support was the only variable to be a significant predictor of both depressive symptoms and family functioning. Our findings are similar to past research (Lester, Watson, Waters, & Cross, 2016) that identified significant inverse relationships between family connectedness with depressive symptoms and emotional difficulties in adolescents. Family connectedness or perceived closeness to parents is similar to subjective support and includes the perceived caring of family, feeling loved and wanted by family members, and satisfaction with relationship to family (Lester et al., 2016; Luthar & Latendresse, 2005). This connectedness is believed to be protective of mental health and is fostered by communication between parent/guardian and the child or adolescent (Lester et al., 2016). Attachment to the parent or guardian helps to provide the child or adolescent with a feeling of comfort during periods of stress, change, and uncertainty (Dubois-Comtois, Cyr, Pascuzzo, Lessard, & Poulin, 2013), and a safe base to explore the world and develop their autonomy (Damour, 2016). Another protective factor for child and adolescent well-being is parental presence in the home before and after school, at dinner time, and in the evenings (Lester et al., 2016; Luthar & Latendresse, 2005). Instrumental support affected only the child’s perception of how well the family functions but did not affect their depressive symptoms.
Parental monitoring was significantly related to family functioning but not significantly related to depressive symptoms. Knowing the whereabouts of one’s children and their friends, and having clear expectations for when to return home are an important facet of better family functioning. Higher parental monitoring scores suggest clear communication between the adult caretaker and the child/youth as well as clear consequences when the monitoring expectations are not met. The lack of significant relationship between parental monitoring and depressive symptoms may be due to small sample size. Although depressed children often have fewer friends and less participation in activities outside the home than their nondepressed peers which may result in fewer occasions for monitoring, the relationship between parental monitoring and depressive symptoms has been supported elsewhere (Bellamy & Hardy, 2015).
We did not examine the relationship between family functioning and depressive symptoms. In one study, perceived family functioning mediated the relationship between depressive symptoms and help-seeking beliefs, which may indicate family functioning increases help-seeking behaviors in those with higher depressive symptoms (Keeler & Siegel, 2016). Family-based interventions to decrease children’s depressive symptoms might target both the child and the parent/grandparent, with interventions aimed at increasing children’s resourcefulness and helping adults to find ways to enhance support, respectively.
The covariates of age, gender, and living situation demonstrated no effects on depressive symptoms, but there were suggestions of possible influences on family functioning. Older grandchildren and those living with grandmothers showed a tendency toward more problems in family functioning (p < .10), but larger sample sizes might be needed for a significant effect to become apparent. An important point is that being raised by a grandmother did not dispose a grandchild to mental health problems.
While the sample size was adequate for the number of variables included, the sample was obtained from one Great Lakes state which might limit its generalizability to other locales. Furthermore, the challenges of recruiting grandchildren into the study through their grandmother may introduce sampling bias that could distort the findings. Because we recruited through the grandmother, there were siblings and possibly cousins who participated. Although we found no effect from this lack of statistical independence, it would be enlightening to examine family effects if there were sufficient families. Our sample also ranged widely in age, from as young as 8 to 19. It is possible, that with larger subsamples in each age range, more robust patterns would emerge. Finally, we did not ask the grandchild participants their race, which might be relevant.
Despite the limitations, we believe that this study adds to the literature about children’s depressive symptoms and family functioning across a range of children and adolescents, including those who may or may not have diagnosed mental health problems. What seems to matter to children’s mental health is feeling loved and supported and having skills to cope with adversity, including the problem-solving and self-control skills that constitute resourcefulness. Nurses and frontline practitioners are uniquely positioned to teach these skills to children and adolescents as well as to coach those who are closely involved in child rearing. Indeed, the children and adolescents indicated that guardians who supply emotional support and practical help and set limits evoke the perception that their family is working well. The importance of parental attention to their children’s activities, whereabouts, and companions is a critical indicator of good family functioning and may affect child mental health as well. Thus, our findings give nurses and other frontline practitioners new guidance in addressing the socioemotional needs of their patients and understanding how better to help them manage depressive symptoms and family instability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the grants “Intergenerational Caregiving to Youth at Risk” and “Grandmothers, Caregiving, Families and Transitions” from the National Institute of Nursing Research/National Institutes of Health (ROI-NR05067).