
Abstract
This study investigated the association between sociodemographic characteristics and public attitudes toward Tobacco 21 laws. Through a random telephone survey in 2017, 1,675 Kentucky adults were asked if they favored/opposed increasing the minimum legal age to purchase tobacco products from 18 to 21 years of age. Over half (57.9%) favored raising the minimum legal age for tobacco sales to 21 (95% confidence interval: [54.5, 61.2]). Multivariable logistic regression for weighted survey data was used to determine factors associated with support. In the adjusted analysis, older age, female sex, non-White, conservative political ideology (versus moderate), and support for a statewide smoke-free policy were each significantly associated with greater support for Tobacco 21. The results suggest multiple demographic and personal factors associated with support, even in a tobacco-growing state. Health care professionals, including nurses, must understand existing public attitudes to effectively advocate for tobacco policies in states with high tobacco use.
While tobacco control in the United States has made great strides over the past 50 years, leading to an estimated 8 million fewer premature deaths (Institute of Medicine [IOM], 2015), a large segment of the population continues to smoke/use tobacco and youth continue to initiate these behaviors, especially among those from rural communities and subpopulations of lower economic status. Among adults who become daily smokers, approximately 90% report first cigarette use before age 19 (U.S. Department of Health and Human Services [USDHHS], 2006, 2012). We also know that smokers who initiate earlier in life are less likely to quit, so policies that reduce or delay initiation could have a large impact on public health (Ahmad, 2005). Over the past few decades, effective tobacco control strategies have been implemented to reduce tobacco use, including higher tobacco taxes, strong smoke-free laws that include all workplaces and public places, and well-funded, sustained tobacco prevention and cessation programs (USDHHS, 2014). More recently, proponents have advocated that increasing the minimum legal age (MLA) to purchase tobacco products to 21 is a promising strategy to reduce smoking and other tobacco use among youth and save lives (IOM, 2015).
It is estimated that if the MLA for tobacco sales were raised to 21 years, smoking initiation could be reduced by 25% among 15- to 17-year-olds and by 15% among 18- to 20-year-olds, leading to nearly 250,000 fewer premature deaths and improved quality of life (Ahmad, 2005; IOM, 2015). Laws raising the MLA for tobacco sales to 21 years (i.e., Tobacco 21) are particularly important as they may protect adolescents who are vulnerable to nicotine addiction and subsequent neurological harm (USDHHS, 2012) as well as decreased likelihood of quitting tobacco use later in life (Kendler, Myers, Damaj, & Chen, 2013). Given nurses play a vital role in improving health and are regularly faced with the consequences of tobacco use among patients, families, and communities, understanding public health strategies to reduce tobacco use is warranted.
History of and Attitudes Toward Tobacco 21
Laws establishing a MLA for tobacco sales have been in existence since the 1880s, with half of the states in the United States adopting an MLA of at least 21 years in the 1920s (Apollonio & Glantz, 2016). Lobbying by the tobacco industry prompted states to lower the MLA to 16 or 18 years; the majority of the current state laws have an MLA of 18 years for most tobacco products (Apollonio & Glantz, 2016). Over the past 10 to 15 years, increasing the MLA for tobacco sales and advocating for Tobacco 21 laws has gained momentum in the United States. In 2005, Needham, Massachusetts, raised its MLA to 21 years and reported a 50% decline in youth smoking rates (Schneider, Buka, Dash, Winickoff, & O’Donnell, 2015). As of 2018, six states and at least 350 municipalities across over 20 states have raised the MLA to 21 years (Campaign for Tobacco-Free Kids [CTFK], 2018a). However, among the top tobacco-growing states (e.g., North Carolina, Kentucky, Tennessee, Virginia, South Carolina; CTFK, 2014), none have raised the MLA to 21 years.
Laws increasing the MLA reflect broad public support across the United States (Winickoff et al., 2016). The majority of U.S. adults strongly support raising the MLA for tobacco sales to 21 years, ranging from 65% to 75% (King, Jama, Marynak, & Promoff, 2015; Lee et al., 2016; Winickoff et al., 2016). Support for Tobacco 21 tends to be greater among older adults as compared with younger adults aged 18 to 20 years, although 65% of these younger adults respond favorably (King et al., 2015). Similarly, support tends to be highest among never smokers (69.9% among current cigarette smokers vs. 77.5% of never smokers; King et al., 2015) and females (73.2% among men vs. 76.7% of women; King et al., 2015; Winickoff et al., 2016). In regard to differences by political affiliation, there are similar levels of support for Tobacco 21 in states voting Republican versus Democrat in the last presidential election (Lee et al., 2016). However, these state-level indicators may not be reflective of personal-level data. To date, public opinion studies have looked at support across geographic regions (King et al., 2015; Lee et al., 2016; Winickoff et al., 2016), but none have specifically looked at support among individuals living in a tobacco-growing state such as Kentucky. Understanding attitudes toward Tobacco 21 in states with continued barriers to tobacco control can inform policy enactment and sustainability (USDHHS, 2014).
Purpose
As more communities and states enact Tobacco 21 laws, there is a need to identify potential sociodemographic factors that may influence attitudes toward the policy especially in states with tobacco use disparities like Kentucky, a tobacco-growing state with high rates of tobacco use and weak tobacco policies. Kentucky does not have a statewide smoke-free law; over one-third of Kentuckians are covered by local 100% smoke-free workplace laws (BREATHE, 2017). In addition, Kentucky is preempted from implementing Tobacco 21 at the community level, so statewide support among constituents needs to be understood. The purpose of this study was to assess whether demographic and personal factors (age, sex, education, children in the home, urban/rural status, smoking status and e-cigarette ever use), political party affiliation and ideology, voter registration status, and support for a statewide smoke-free law were associated with support for increasing the MLA for tobacco sales from 18 to 21 years in a tobacco-growing state.
Method
Design and Sample
We conducted a secondary analysis of cross-sectional data from the 2017 Kentucky Health Issues Poll (KHIP). KHIP is an annual opinion survey of Kentucky adults about ongoing concerns and timely policy issues that affect health in the Commonwealth. The KHIP is funded by Interact for Health and the Foundation for a Healthy Kentucky (FHKY) and data are publicly available (KHIP, 2017). The 2017 KHIP was conducted October 24 to December 2, 2017, by the Institute for Policy Research at the University of Cincinnati. At the time of this survey, there had not been Tobacco 21 advocacy campaigns in Kentucky.
A random sample of 1,692 adults from throughout Kentucky were invited to participate in phone interviews (861 landline and 831 cell phone). Both mobile and landline respondents for KHIP were selected at random, using probability sampling to limit potential selection bias. In 95 of 100 cases, the statewide estimates will be accurate to ±2.4%. Of those who participated, 1,675 completed the item that assessed degree of support for raising the MLA for tobacco products from 18 to 21; this subsample was used for the analysis reported here.
Measures
Support for statewide smoke-free and Tobacco 21 laws
First, participants were asked their opinion on smoke-free policy: “Would you favor or oppose a state law in Kentucky that would prohibit smoking in most public places, including workplaces, public buildings, offices, restaurants and bars?” Response options followed a 7-point Likert-type scale ranging from (1) strongly favor to (7) strongly oppose; the middle choice was (4) neither/not sure/don’t know. They were also asked “Do you favor or oppose increasing the minimum legal age to purchase tobacco products from 18 years to 21 years of age?” Response options were the same as above. For analysis purposes, given the bimodal distribution of responses for both policy variables, with more than 95% of participants choosing either one of the two most supportive categories or one of the two most oppositional ones, we dichotomized each of the two variables into “Favoring” versus “Opposing” with the “Unsure” responses in the middle of the scale combined with “Opposing” group. The convention of including those unsure with those opposed was chosen because it provides a conservative estimate of level of support for public policy.
Demographic and personal characteristics included age (years), sex (male/female), race, education, children in the home, county of residence and smoking status. Given the low prevalence of racial/ethnic minorities in Kentucky, race was coded as “White” versus “Other race.” For education, participants were asked the highest grade or year in school they completed. For the purpose of analysis, responses placed into the following categories: “high school or below,” “some college,” or “college degree.” The number of children living in the household below 18 years of age was recorded; we created an indicator variable for the presence of one or more minor child(ren) in the home (age of children was not asked). County of residence was recorded by the interviewer as a FIPS code and defined as rural or urban using Rural Urban Continuum Codes (U.S. Department of Agriculture, 2016).
Smoking status and e-cigarette use
For conventional cigarettes, two questions were used to determine smoking status: “Have you smoked at least 100 cigarettes in your lifetime” and “Do you smoke cigarettes every day, some days, or not at all?” Nonsmokers were those who had not smoked 100 cigarettes in their lifetime. Among those who answered “yes” to having smoked 100 cigarettes in their lifetime, participants responding “not at all” to the second question were coded as former smokers, while those who answered either “some days” or “every day” were current cigarette smokers. For e-cigarettes, only one item was asked: “Have you ever smoked electronic cigarettes?” Those who responded “yes” were coded as ever e-cigarette users.
Political party identification, ideology, and voter registration status
First, participants were asked, “Generally speaking, do you think of yourself as a Republican, Democrat, an Independent or what?” Next, participants were prompted, “We hear a lot of talk these days about liberals and conservatives. What about yourself—that is, in politics, do you generally think of yourself as a liberal, a moderate, or conservative?” An additional yes/no question was “Some people are registered to vote and others are not. Are you CURRENTLY registered to vote at your PRESENT address?”
Data Analysis
Methods appropriate for survey data, which reflect the sample weights, were used for descriptive, bivariate, and regression analysis. Frequency distributions were used to summarize study variables. The Rao-Scott chi-square test assessed the unadjusted bivariate associations between support for the Tobacco 21 policy and each of the personal and demographic characteristics. Logistic regression determined which factors predict support for the increase in MLA from 18 to 21 in the adjusted analysis. Potential predictors in the model included age, sex, race, education, children in the home, urban/rural status, smoking status, e-cigarette ever use, political party affiliation and ideology, voter registration status, and support for a statewide smoke-free law. Variance inflation factors were estimated to evaluate the presence of multicollinearity, and the Hosmer–Lemeshow (HL) goodness-of-fit test was used to assess model fit. Analyses were done using SAS, v. 9.4, with an alpha level of .05.
Results
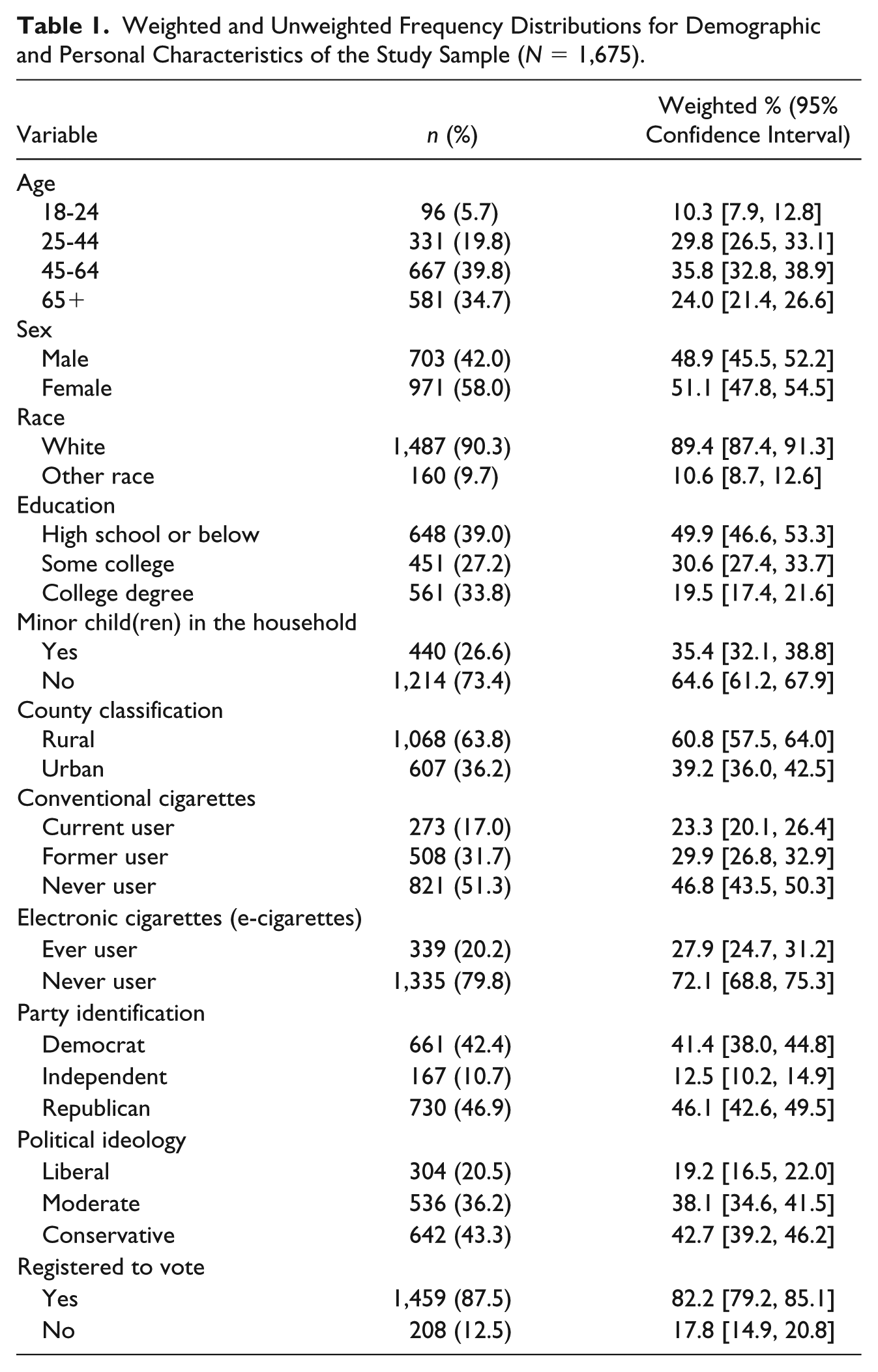
The weighted age distribution of the 1,675 participants indicated that 10% were 18 to 24 years, 30% were 25 to 44, 36% were 45 to 64, and 24% were 65 and above (Table 1). In the weighted summary, the majority of participants were female (51%) and most were White (89%). Half of those who completed the survey had a high school diploma or less education, 31% had attended some college, and the remaining 19% had a college degree. Most did not have minor child(ren) in the home (65%) and more than half lived in rural counties (61%). The largest percentage had never smoked conventional cigarettes (47%), while 23% were current smokers and 30% former smokers. About 28% had ever used e-cigarettes. In terms of political party identification, the largest weighted percentage was Republican (46%), followed by Democrat (41%) and Independent (13%). The largest subgroup for political ideology was conservative (43%), followed by moderate (38%), and then liberal (19%). Most who completed the survey were registered to vote (82%).
Weighted and Unweighted Frequency Distributions for Demographic and Personal Characteristics of the Study Sample (N = 1,675).
Most participants favored both tobacco control policies: a statewide smoke-free law and raising the MLA for tobacco sales in the state from 18 to 21 years. In the weighted sample, 71.0% were in support of a statewide smoke-free law (95% confidence interval: [67.8, 74.2]); 29.0% were either in opposition or unsure about the law. While there was less support for Tobacco 21 than for a statewide smoke-free law, 57.9% of participants supported Tobacco 21 (95% confidence interval: [54.5, 61.2]); 42.1% were opposed or unsure.
The personal and demographic variables associated with support for Tobacco 21 are shown in the unadjusted analysis columns in Table 2. The significant associations are with age, sex, electronic cigarette ever use, political party, ideology, and favorable assessment of a statewide smoke-free law. The percent in favor of Tobacco 21 by age category tended to increase with increasing age: Of those in the 18 to 24 years group, 50.5% favored this compared with 49.6%, 59.6%, and 68.6% in the 25 to 44, 45 to 64, and 65 and over groups, respectively (p < .001). Females were more supportive than males (67.5% vs. 47.8%, p < .001), and those who had ever used e-cigarettes were less in favor of Tobacco 21 than those who had not (48.7% vs. 61.4%,p = .002). In the unadjusted analysis, support for increasing the MLA to 21 was strongest among registered Democrats (63.1%), followed by Republicans (55.6%) and then Independents (45.8%; p = .006). The results were similar when comparing favorability across political ideology: 61.7% of those who were liberal supported Tobacco 21, compared with 60.9% of conservatives and 48.8% of moderates (p = .004). Finally, 62.9% of those who supported a statewide SF law were supportive of the Tobacco 21 policy, while of those who were not in favor of a statewide policy, only 45.3% supported raising the MLA to 21 (p < .001).
Unadjusted and Adjusted Associations of Demographic and Personal Characteristics and Support for a Smoke-Free Policy With Support for Tobacco 21 (n a = 1,550).
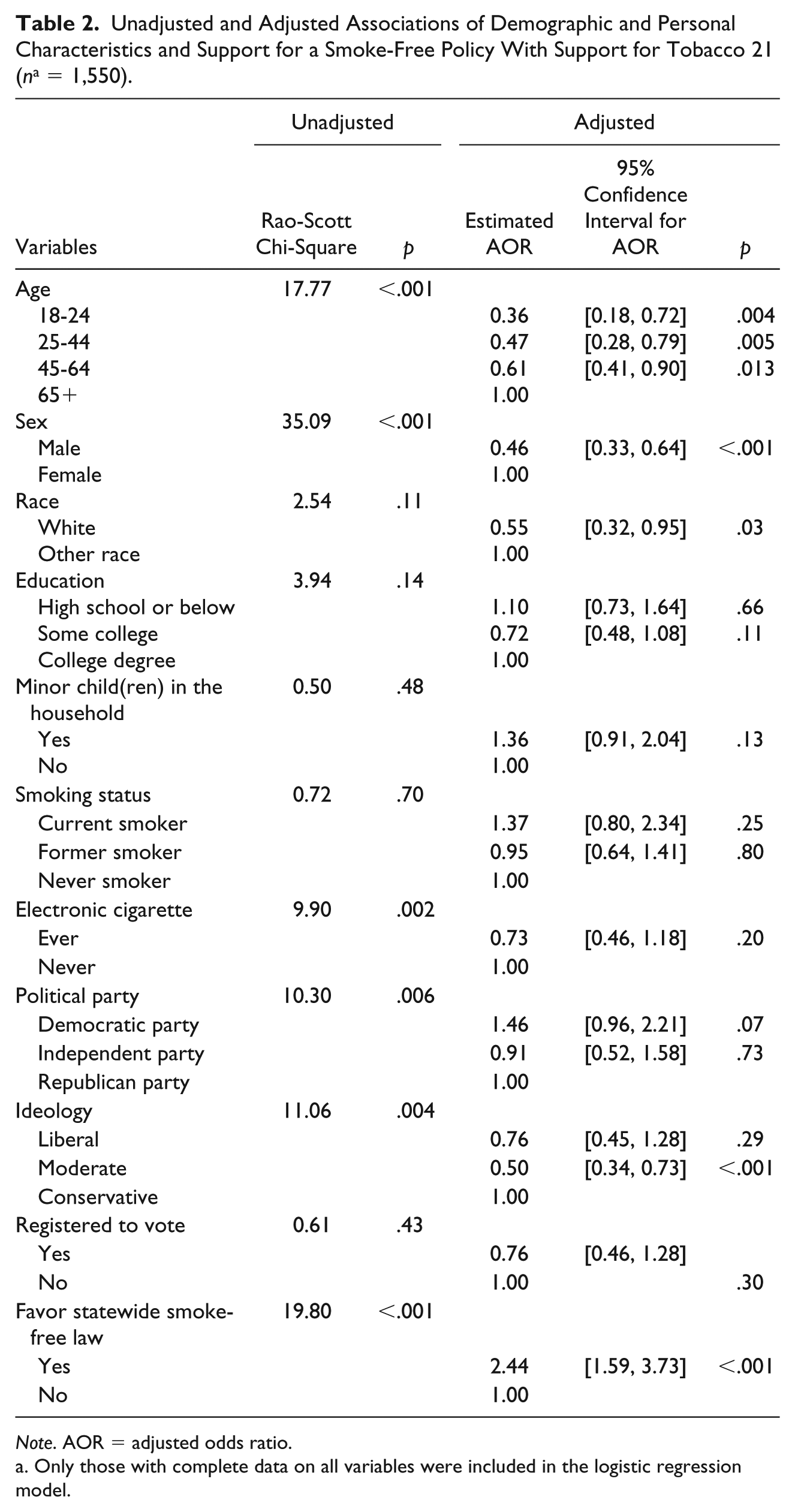
Note. AOR = adjusted odds ratio.
Only those with complete data on all variables were included in the logistic regression model.
The multivariable logistic weighted regression model to assess predictors of support for raising the MLA for tobacco sales to 21 years is shown in Table 2. The overall model was significant (likelihood ratio F = 9.3, p < .001), and the variable inflation factors were all less than 1.8, suggesting that multicollinearity did not distort regression parameters. The HL goodness-of-fit test was not significant, suggesting the model fit the data well (HL χ2 = 14.8,p = .063). The significant predictors of support for Tobacco 21 included age, sex, race, moderate political ideology (with conservative as the reference), and degree of support for a statewide smoke-free law. Compared with the participants aged 65 and older, those who were 18 to 24 were 64% less likely to support Tobacco 21, while those who were 25 to 44 were 53% less likely to support and those 45 to 64 were 39% less likely (Table 2). Males were 54% less likely than females to support this policy, and compared with minority participants, those who were White were 45% less likely to support Tobacco 21. Compared with those who identified as ideologically conservative, those who were moderates were 50% less likely to support the increase in MLA to 21. Those who favored a statewide SF law were 144% more likely to support Tobacco 21. Other variables in the model were not significantly associated with support for Tobacco 21.
Discussion
Even in a state historically known for tobacco production, high rates of tobacco use, and weak tobacco control policies (CTFK, 2018b), the findings of this study reinforce that the majority of U.S. adults support Tobacco 21. While the percent support for raising the MLA for tobacco sales to 21 years in Kentucky was lower (58%) than in previous research in other states (65% to 75%; King et al., 2015; Lee et al., 2016; Winickoff et al., 2016), nearly six in 10 Kentuckians support Tobacco 21. There is also a high level of support for a statewide smoke-free law among Kentuckians, which was associated with support for Tobacco 21. However, given the mixed support for tobacco control policies in a tobacco-growing state compared with previous national research (King et al., 2015), this study helps to further understand factors associated with support in a traditionally pro-tobacco state, which can help inform policy advocacy efforts in this setting.
Findings from this study reinforce current national research on factors associated with support for increasing the MLA for tobacco sales from 18 to 21. Females, non-Whites, and those 65 and older in Kentucky were more likely to indicate support for Tobacco 21, similar to previous research (King et al., 2015; Lee et al., 2016; Winickoff et al., 2016). Population-specific factors and demographics are critical to consider in developing, implementing, and sustaining laws that increase the MLA for tobacco sales (King et al., 2015; Lee et al., 2016; Winickoff et al., 2016). Future research is needed to determine the best ways to reach various demographics and specific populations that are not as supportive of tobacco policy change. Targeting advocacy and media messages to males, young adults, and Whites to promote support for Tobacco 21 would be particularly important. Public attitudes toward tobacco control interventions can inform policy development, implementation, and sustainability (USDHHS, 2014). Therefore, effective strategies for targeted messaging that impacts attitudes and opinions may be critical to the success of any Tobacco 21 policy initiative.
While there is limited research assessing differences in attitudes toward Tobacco 21 across political parties or ideology (Lee et al., 2016), we found that individuals who identified with being politically conservative were more likely to be supportive of Tobacco 21 relative to those identifying as moderate. However, there were no significant differences in support in the multivariable model when comparing self-reported political party. Previous state-level research reveals that voting Republican versus Democrat in the last presidential election was not associated with support for Tobacco 21 (Lee et al., 2016), but this study did not look at personal-level political party or ideology. Further research is needed to disentangle the influence of political party and ideology on support for Tobacco 21 laws, particularly in states with varying degrees of political support for tobacco policies in general.
Our study is the first to report an association between support for statewide smoke-free laws and greater likelihood for support of Tobacco 21. In Kentucky, public support for a statewide smoke-free law increased from 54% in 2011 to 71% in 2017 (FHKY, 2017). However, the state has yet to enact a statewide smoke-free law. Policymakers use public opinion polls to determine whether to support a policy and they report being greatly influenced by perceived constituent sentiment about tobacco control laws (O’Dougherty, Forster, & Widome, 2008). Given that our findings show that support for a statewide law predicts a greater likelihood of favoring fa Tobacco 21 law, garnering support for Tobacco 21 may be successfully tied to advocacy for a statewide smoke-free law. Furthermore, tobacco-growing states that have statewide smoke-free laws in place may be more ready to enact Tobacco 21 laws.
Interestingly, in the adjusted analysis, level of education, rurality, and smoking status were not associated with support for Tobacco 21, which contradicts the limited research on this topic (King et al., 2015; Lee et al., 2016; Winickoff et al., 2016). Tobacco users of all education levels, place of residence, and tobacco use status categories were as likely to support Tobacco 21 in this tobacco-growing state. Given these findings, broad-based appeals may be effective in promoting tobacco control policies, such as Tobacco 21, regardless of education, urban/rural status, or cigarette use. Previous research suggests that increasing public awareness about the addictive potential of even a few cigarettes might increase support for raising the MLA for tobacco sales to 21 (Winickoff et al., 2016). Further evaluating message framing among these groups is warranted.
The primary strength of this study is the relatively large number of survey participants recruited statewide. The inclusion of cell phones and landlines, as well as adjustment in the analysis for survey weights, further bolstered the representativeness of the sample for the underlying population in this disparate tobacco-growing state. The findings may have been limited by the availability of relevant variables and are not necessarily generalizable to other areas of the country. While there were several significant predictors of support for Tobacco 21, other factors (e.g., perceived addictive potential of tobacco use) may influence support but were not measured in this survey. These limitations reinforce the need for further research on factors associated with support for Tobacco 21 as state opinion polls are constrained in the number of relevant questions that are asked. Since the first municipality adopted Tobacco 21 in 2005, campaigns to raise the MLA to 21 have gained momentum across the nation (CTFK, 2018a). The findings of this study underscore support for both Tobacco 21 and a statewide smoke-free law in a tobacco-growing state with high rates of tobacco use and weak tobacco control laws. Factors that influenced support for Tobacco 21 in particular included age (with older participants more likely to be supportive), sex (with females more supportive), race (with minorities more likely to support), having a conservative political ideology (relative to a moderate one), and indicating support for a statewide smoke-free law. Further research is warranted to expand our understanding of the personal factors that may affect support for Tobacco 21, particularly in states with less support for tobacco policies. Results of this study can inform advocates, which often times includes nurses and other health care professionals, in their efforts to develop advocacy strategies to promote effective tobacco control policy campaigns.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.