
Abstract
Women who smoke during pregnancy face psychosocial barriers to cessation, and women with opioid use disorder (OUD) face amplified barriers. We pilot tested a Perinatal Wellness Navigator (PWN) program for a group of high-risk perinatal women (N = 50; n = 42 with OUD) that consisted of (a) one-on-one tobacco treatment, (b) comprehensive assessment of cessation barriers, and (c) linkage to clinical/social services. Outcome measures were assessed at baseline and postintervention. Participants smoked 10 fewer cigarettes per day (p = .05) at postintervention and were less dependent on nicotine (p < .01). Mean postnatal depression scores (p = .03) and perceived stress (p = .03) decreased postintervention. Participants received at least one referral at baseline (n = 106 total), and 10 participants received an additional 18 referrals at postintervention to address cessation barriers. The PWN program was minimally effective in promoting total tobacco abstinence in a high-risk group of perinatal women, but participants experienced reductions in cigarettes smoked per day, nicotine dependence, stress, and depression.
Smoking during pregnancy increases the risk of multiple adverse outcomes, including premature birth, ectopic pregnancy, stillbirth, and sudden infant death syndrome (SIDS) (U.S. Department of Health and Human Services, 2014). Dangers of maternal smoking continue beyond pregnancy, as children exposed to secondhand smoke have an increased risk of asthma and other respiratory disorders, attention deficit hyperactivity disorder, poor neurocognitive performance, and SIDS (U.S. Department of Health and Human Services, 2006). Children born to mothers who smoke during pregnancy have a higher risk of tobacco dependence in adulthood than their peers (Buka, Shenassa, & Niaura, 2003; Shenassa, Papandonatos, Rogers, & Buka, 2015). In addition, the postpartum time period is a vulnerable point for relapse to tobacco use (Rockhill et al., 2016). Interventions are needed to promote smoking cessation during pregnancy and prevent postpartum smoking relapse.
Despite the well-acknowledged harms of maternal smoking, there have been minimal reductions in rates of prenatal and postpartum smoking in the past decade (Tong et al., 2013). The majority of smoking cessation interventions for pregnant women focus on individual behavior change, often through enhancing motivation. However, women who continue smoking during pregnancy tend to have psychosocial issues or social disadvantages. For example, smoking during pregnancy is higher among women who are of low socioeconomic status (Gilman, Breslau, Subramanian, Hitsman, & Koenen, 2008; Page, Padilla, & Hamilton, 2012; Tong et al., 2013); have co-occurring mental health issues (Page et al., 2012), such as depression (Gilman et al., 2008) and anxiety (Hauge, Torgersen, & Vollrath, 2012); did not access recommended prenatal care (Gilman et al., 2008); report stress or stressful life events (Al-Sahab, Saqib, Hauser, & Tamim, 2010; Hauge et al., 2012); or have experienced abuse or victimization (Mirjam, Berit, Siri, & Pål, 2009).
These disadvantages may be further exacerbated for perinatal women with co-occurring substance use disorders (Winhusen & Lewis, 2017). For example, the vast majority of women receiving medication-assisted treatment for opioid use disorder (OUD) report smoking cigarettes (Akerman et al., 2015; Chisolm et al., 2013). However, results of focus groups conducted with this population indicate that women wanted to stop smoking for themselves and their children, but report major life stressors and fear of addressing their dual dependencies (Fallin, Miller, & Ashford, 2016).
Tobacco treatment programs are needed that incorporate adequate supports to address these underlying psychosocial issues (e.g., social and economic disadvantage and co-occurring mental health issues; Stewart et al., 2011). In addition to being well-known barriers to smoking cessation (Twyman, Bonevski, Paul, & Bryant, 2014), stress, anxiety, and depression are independent predictors of adverse birth outcomes. Highly stressful life events reported during pregnancy are associated with shorter mean gestational age and an increased risk of preterm delivery (Hedegaard, Henriksen, Secher, Hatch, & Sabroe, 1996; Witt et al., 2014; Yost, Bloom, McIntire, & Leveno, 2005). Recent research confirms the impact of maternal stress and anxiety on perinatal outcomes (Beydoun & Saftlas, 2008; Glynn, Schetter, Hobel, & Sandman, 2008; Grigoriadis et al., 2018; Schetter, 2009; Torche, 2011; Wadhwa, Entringer, Buss, & Lu, 2011), including low birth weight, shortened gestation, and increased risk of premature birth. Women who are depressed during pregnancy are 1.4 times more likely to experience premature birth, 1.5 times more likely to have an infant with low birth weight, and 1.5 times more likely to have an infant with intrauterine growth restriction (Grote et al., 2010). Furthermore, the risk of depression-related premature birth is significantly higher among women of lower socioeconomic status (Grote et al., 2010).
For perinatal smoking cessation programs to be effective, it is necessary for programs to address the competing needs of pregnant women. We tailored and implemented a patient navigator program to tobacco treatment among pregnant women and women in the early postpartum period. Since the 1990s, hundreds of patient navigator programs have been implemented nationwide (Freeman, 2006; Paskett, Harrop, & Wells, 2011). These programs were designed to address the disproportionate cancer-related morbidity and mortality facing socioeconomically disadvantaged communities and racial/ethnic minorities through providing direct access to screening (e.g., free or low-cost mammography), reducing barriers to follow-up, and providing tailored education and outreach. Despite this widespread adoption of navigator programs for cancer screening and treatment, this model has rarely been implemented for cancer prevention in the context of tobacco treatment (Freeman, 2006). This program extends the work of Levinson and colleagues (2015) who implemented an innovative navigator approach to enhancing the treatment of tobacco dependence among low-income parents (Levinson et al., 2015).
The Perinatal Wellness Navigator (PWN) program filled a gap in services by providing evidence-based tobacco treatment, as well as navigation (i.e., comprehensive assessment and referrals to clinical and social services) to address barriers and promote facilitators to smoking cessation.
Purpose
The purpose of this evaluation was to (a) determine the impact of the PWN on smoking outcomes during pregnancy and the early postpartum period, (b) quantify referrals for social and clinical services that reduce participant barriers to smoking cessation and evaluate the impact of the PWN on maternal barriers to smoking cessation (e.g., depression and stress), and (c) describe participant experiences with the PWN intervention.
Method
Design
The study design is a program evaluation of a pilot PWN intervention. Several outcome measures were assessed via a longitudinal, repeated-measures strategy for program evaluation.
Participants/Sampling
All study participants were patients of the Department of Obstetrics and Gynecology within an academic medical center. We recruited from a clinic which serves a high volume of prenatal patients with tobacco use. This clinic also houses a large program designed to provide comprehensive treatment for pregnant and postpartum women with OUD. Any pregnant or postpartum patient from June to December 2017 who identified as a smoker at the point of care was approached by the study personnel (H.D.) for study recruitment. The first 50 patients who agreed to participate in the study, met eligibility criteria, and provided informed consent were enrolled in the PWN intervention. Participants were eligible for this study if they (a) were over the age of 18 or emancipated or had parental permission, (b) were current smokers (defined as 100 cigarettes in their lifetime and any cigarettes in the past 30 days), and (c) expressed interest in quitting smoking. Exclusion criteria included signs of serious mental illness such as schizophrenia, active psychosis, or bipolar with active mania. The study protocol was approved by the University of Kentucky institutional review board (IRB).
Data Collection/Measures
Smoking was measured by expired air carbon monoxide (EACO) using a Bedfont piCO+ smokerlyzer. Participants with an EACO of less than 10 ppm were considered to be nonsmokers.(Brose, Tombor, Shahab, & West, 2013). Self-report smoking was assessed with the question, “During the last 30 days, have you used any of the following [cigarettes]?”
Other smoking-related outcomes included nicotine dependence, number of cigarettes smoked per day, motivation to quit smoking, confidence in their ability to quit smoking, and secondhand smoke exposure in the home. Nicotine dependence was assessed using the Fagerstrøm Test for Nicotine Dependence (Heatherton, Kozlowski, Frecker, & Fagerstrom, 1991). The six-item scale is a reliable and valid measure of nicotine dependence (Heatherton et al., 1991).
Motivation was operationalized via the question, “How important is stopping smoking to you on a scale of 0 to 10?” Confidence was operationalized via the question, “How confident are you that you will quit smoking in the next month?”, with confidence options presented on a scale of 0 to 10, where 0 is “not confident at all” and 10 is “100% confident.” Self-report secondhand smoke exposure in the home was assessed with the question, “In the past 7 days (past week), how often were you exposed to secondhand tobacco smoke [in your house]?”
Additional outcome measures included maternal psychosocial factors, which were operationalized as depression, stress, and recovery capital. Depression was assessed via the Edinburgh Postnatal Depression Scale (EPDS). This 10-item validated scale examines clinical depressive symptoms in pregnant and postpartum women, with higher scores indicating more depressive symptoms (Gibson, McKenzie-McHarg, Shakespeare, Price, & Gray, 2009). Stress was assessed via the four-item Perceived Stress Scale (PSS4; Cohen & Williamson, 1988). The PSS4 has adequate reliability and is a useful measure for assessing perceived stress on short questionnaires (Cohen & Williamson, 1988).
Among participants who were enrolled in comprehensive OUD treatment, recovery capital was assessed via the Assessment of Recovery Capital (ARC) Scale (Groshkova, Best, & White, 2013). The ARC is a 50-item scale used to measure an individual’s recovery strengths. The scale is divided into 10 subscales that measure well-being across several domains, including physical health, psychological health, substance use, and social support. All items on the scale are dichotomous response items, thereby allowing a maximum score of 50, with higher scores indicating higher recovery capital (Groshkova et al., 2013). The ARC has adequate test–retest reliability and high concurrent validity with the World Health Organization Qualify of Life Scale (World Health Organization, 2004). Furthermore, a cutoff score of 27.5 predicts stable recovery, defined as greater than 5 years of sustained recovery (Groshkova et al., 2013).
Additional barriers to quitting were assessed via an accounting of tangible resources available to the participant, including safety and stability of housing, and reliability of access to transportation to health care appointments, child care, and food. Referrals for clinical and social services were recorded by the PWN following each study interaction. Following the encounter, the PWN documented information about the appointment by entering detailed notes into a disposition survey to capture any feedback from the participant on challenges, progress, or helpful contextual information.
Several secondary measures and data regarding patient demographics were collected as well. Demographic information included patient race, ethnicity, age, partner status, highest educational attainment, and household income.
Intervention
The PWN was a research team member with more than 20 years of experience working in behavioral health. First, the PWN delivered one-on-one evidence-based tobacco treatment based on Smoking Cessation and Reduction in Pregnancy Treatment (SCRIPT; Windsor et al., 2014), an evidence-based tobacco treatment curriculum for pregnant women. The PWN then conducted a thorough assessment of smoking cessation barriers (e.g., violence or victimization, stress, depression, and anxiety), which lasted approximately 30 min on average. Next, the PWN linked the participants to tailored community resources to address the identified barriers to optimize the potential for success. For example, for participants with high levels of stress, the PWN provided referrals to address underlying causes, such as unstable housing, unemployment, and relationships issues. Finally, the PWN referred patients to a smoking cessation group at the clinic for pregnant and postpartum women that was also based on the principles of SCRIPT (Windsor et al., 2014). After the first visit, the PWN scheduled a follow-up phone call and conducted a follow-up assessment 3 months later.
Procedures
We developed a comprehensive assessment and referral process for the PWN to use to guide assessment and referrals. In the preliminary phase of this study, the PWN formalized relationships with community partners for referral.
Furthermore, the project database manager created a comprehensive, user-friendly assessment tool administered through Qualtrics, which is an online survey software tool that can be used for data collection and analytics. Participants were guided to appropriate questions based on visit type (i.e., first visit, in-between phone call, or second visit), whether the participant was pregnant or postpartum, and whether the participant was concurrently in treatment for OUD. Critical results were revealed to the PWN in real time during the assessment. For example, if a participant reported current suicidal ideation or current physical violence or threat of violence, the PWN was notified for immediate action. At the end of the survey, the PWN was able to review a summary of all responses necessary to facilitate real-time referrals to clinical and social services. Furthermore, prior to the subsequent visit (a call or follow-up visit), the PWN could review the participant’s previous data and past referrals.
All primary and secondary outcome measures were collected pre–PWN intervention at baseline, and each measure was reassessed in each subsequent visit by the patient. All outcome measures were collected, at minimum, during baseline. For example, demographics were only collected at baseline. Patient identifiers were limited to an encrypted identification number, and crosswalks between identification number and patient identity were not accessible to study analysts.
Analysis
Outcome measure results collected at baseline (pre–PWN intervention) and in the final assessment (3 months following the baseline assessment) are included in this analysis. Participant scores and reports for the baseline and postintervention assessments were calculated. Change in mean scores from baseline to postintervention was analyzed via two-tailed Student’s t test for all continuous outcome measures. Change in secondhand smoke exposure from baseline to postintervention was analyzed via chi-square test. For sensitivity analysis, change in mean scores and secondhand smoke exposure from baseline to postintervention was also calculated only for participants who had both baseline and postintervention assessments.
Total referrals were counted at each assessment interval for study participants and stratified by referral type (i.e., cessation class, counseling or clinical social worker, parenting class, clothing bank, contraception or obstetric [OB] care, and other referrals). Quantitative analyses were conducted in Microsoft Excel and Stata v15.0, with a priori significance set at .05. Qualitative data were abstracted from the visit disposition data to increase richness of analysis (Rockwood, Fay, Hamilton, Ross, & Moorhouse, 2014). These verbatim descriptions were coded thematically using the qualitative text analysis function within Qualtrics.
Results
A total of N = 50 patients were enrolled in the PWN intervention, and all participants (N = 50) completed a baseline assessment. Most participants (n = 38) completed a follow-up intervention 3 months later, and few participants (n = 8) completed one or more telephone assessments in between the baseline and the postintervention period. The telephone assessments collected in between baseline and postintervention are not included in the analysis. Participants ranged from 19 to 41 years of age and were predominately White (98%) with a household income of less than US$20,000 per year (70%). Nearly half of the participants were single (46%). Approximately a third of the participants had a high school degree or a General Education Development (GED; 34%), and 26% had less than a high school education. Most participants in this study (84%) were recruited from an OB clinic that provided comprehensive care for pregnant women with OUD, and these participants were in concurrent OUD treatment.
Study participants reported smoking about 10 fewer cigarettes per day, on average, at the postintervention assessment (Table 1, p = .05). Dependence on nicotine also decreased following the intervention (p < .01). Expired CO decreased from baseline to postintervention assessment; however, this decrease was not statistically significant. Fewer participants at the postintervention assessment reported no secondhand smoke exposure in the home (52.00% at baseline vs. 39.47% at postintervention). In sensitivity analysis to limit baseline results to only those participants who completed both baseline and postintervention assessments, findings were similar; dependence on nicotine decreased in sensitivity analysis (Table 1, p < .01), as well as cigarettes smoked per day (p = .05).
Smoking and Smoke Exposure Outcome Measures.
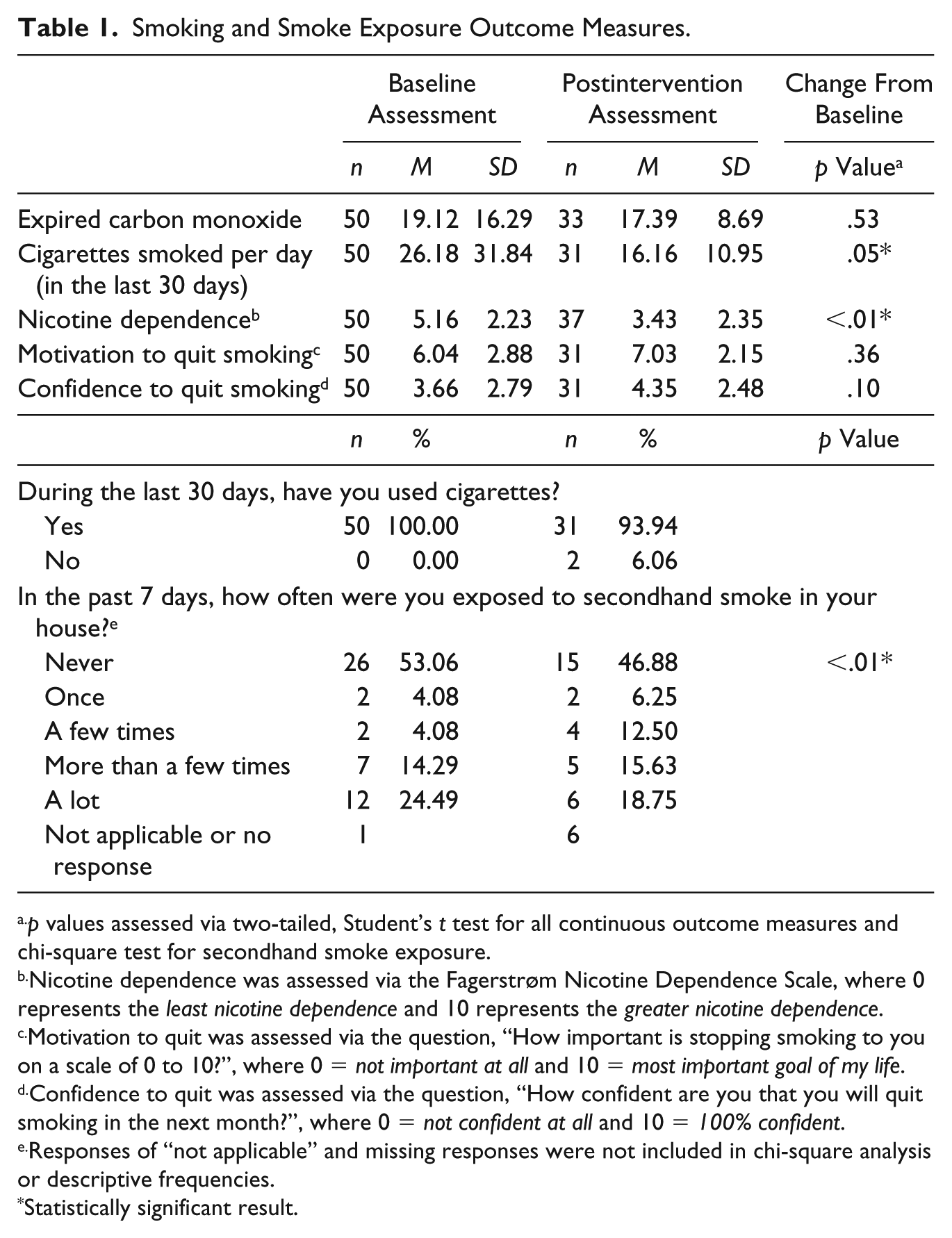
p values assessed via two-tailed, Student’s t test for all continuous outcome measures and chi-square test for secondhand smoke exposure.
Nicotine dependence was assessed via the Fagerstrøm Nicotine Dependence Scale, where 0 represents the least nicotine dependence and 10 represents the greater nicotine dependence.
Motivation to quit was assessed via the question, “How important is stopping smoking to you on a scale of 0 to 10?”, where 0 = not important at all and 10 = most important goal of my life.
Confidence to quit was assessed via the question, “How confident are you that you will quit smoking in the next month?”, where 0 = not confident at all and 10 = 100% confident.
Responses of “not applicable” and missing responses were not included in chi-square analysis or descriptive frequencies.
Statistically significant result.
The mean EPDS score at baseline (12.04) was indicative of widespread depression and anxiety among study participants, as scores of 12 and above are typically considered to require intervention. At the postintervention assessment, the mean EPDS score decreased to 9.47 (p = .03, Table 2), which was indicative of significantly reduced incidence of postnatal depression and anxiety. Similarly, participants reported significantly less perceived stress (p = .03) and slightly increased recovery capital (p = .09). Most participants at baseline (84.00%) and at postintervention (89.47%) were enrolled in concurrent OUD treatment. In sensitivity analysis to limit testing to participants who completed both baseline and postintervention assessments, findings were similar; mean EPDS score decreased from 11.79 at baseline to 9.47 (Table 2, p = .06), mean PSS score decreased but not significantly (p = .11), and mean recovery capital increased but not significantly (p = .17). Furthermore, of note, some participants were still pregnant at the time of follow-up, and others were already postpartum at baseline. Therefore, the observed reduction in stress and depression may not be entirely explained by delivery.
Psychosocial Outcome Measures and Referrals to Clinical or Social Services.
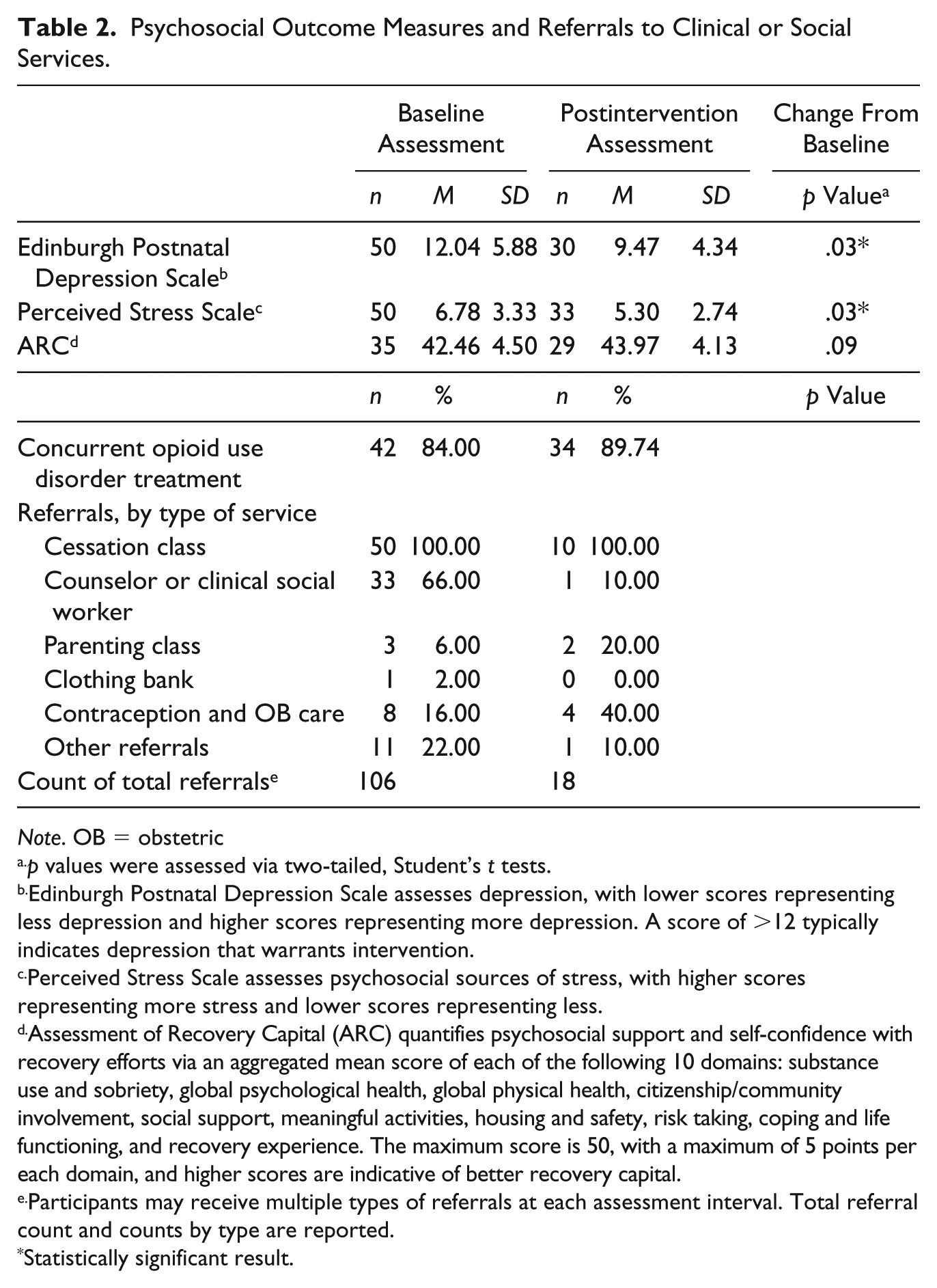
Note. OB = obstetric
p values were assessed via two-tailed, Student’s t tests.
Edinburgh Postnatal Depression Scale assesses depression, with lower scores representing less depression and higher scores representing more depression. A score of >12 typically indicates depression that warrants intervention.
Perceived Stress Scale assesses psychosocial sources of stress, with higher scores representing more stress and lower scores representing less.
Assessment of Recovery Capital (ARC) quantifies psychosocial support and self-confidence with recovery efforts via an aggregated mean score of each of the following 10 domains: substance use and sobriety, global psychological health, global physical health, citizenship/community involvement, social support, meaningful activities, housing and safety, risk taking, coping and life functioning, and recovery experience. The maximum score is 50, with a maximum of 5 points per each domain, and higher scores are indicative of better recovery capital.
Participants may receive multiple types of referrals at each assessment interval. Total referral count and counts by type are reported.
Statistically significant result.
All participants at baseline received at least one referral for clinical and/or social services, with a total of 106 referrals provided at baseline to all N = 50 participants and an additional 18 referrals provided at the postintervention assessment to a subset of n = 10 participants. The most frequent type of referral was to smoking cessation class at both assessment intervals, followed by referrals for counseling/social work at baseline and referrals for contraception/OB care at postintervention.
Experiences With the PWN Program
Participants consistently reported a desire to quit, yet struggled with co-occurring depression, stress, and substance use disorder. One disposition note stated, Patient has had significant family stress with little support. Patient reports depression and states this is because she is with her two young children alone with no respite. Patient’s mother has depression and cannot help. Patient reports having no cigarettes on this day and wanting to quit for her health and for her children’s health.
However, participants consistently reported that their motivation was not sufficient to enable them to quit smoking. According to one note, Patient reports she is “not doing very good at all” and has continued to smoke over a pack a day. Says she is unable to breathe when walking and even had a recent chest x-ray to rule out other issues. Patient says, “My motivation is very high but I still can’t stop. It is so frustrating. My want-to just doesn’t work.”
Another note stated, “Level of smoking remains steady although her desire to quit is still high.”
Co-occurring stress, anxiety, and depression were consistently documented as a barrier to smoking cessation. “Patient reports smoking one cigarette today and being disgusted she is smoking at all. Patient reports having periods of high anxiety and that smoking is her go-to to deal with anxiety. Goal is to be smoke-free by next follow-up.” Another example was as follows: “Patient is pregnant and has endocarditis. She was scheduled for a valve replacement when the hospital discovered she was a few weeks pregnant. Reports high anxiety and nervousness. Patient wants to stop smoking but uses it to manage stress.” According to another note, Patient reports smoking two packs per day and experiencing physical and verbal abuse by father of baby. Patient reports smoking to cope but wants to stop. She is unsure if she can, stating she has anxiety and has never been able to stop before.
Throughout the study, participants reported success with reducing cigarettes after seeking behavioral health support and alternative coping mechanisms for life stressors. One note stated, “Patient has been practicing more self-care and reports getting into crafts to cope with stress and attempt to decrease smoking. Patient has been going to counseling and taking meds appropriately. Patient reports she has decreased number of cigarettes.” According to another note, “Patient is proud she has cut down to one pack per day from three. Her CO level is 6 today. Patient father of baby [sic] has become verbally abusive and controlling. Patient reports coloring has helped her cope.”
Discussion
The pilot PWN intervention enrolled a high-risk population of pregnant or early postpartum patients who smoked and demonstrated significant reductions in cigarettes smoked per day by participants, as well as decreases in postnatal depression and stress.
A navigator model for tobacco treatment is particularly ideal during pregnancy and postpartum, given the concentration of psychosocial disadvantages facing this population. Pregnancy is commonly referred to as a “teachable moment” when motivation for behavior change is high (Olander, Darwin, Atkinson, Smith, & Gardner, 2016; Phelan, 2010). However, motivation is not sufficient for behavior change when pregnant women lack the capability or opportunity for change (Olander et al., 2016). Tobacco treatment interventions are needed that leverage this time of high motivation by providing realistic assistance to overcome cessation barriers.
This pilot program had minimal success with promoting total tobacco cessation. However, this program demonstrated success in reducing cigarettes per day and nicotine dependence. Results of a recent literature review indicated that reduction in cigarettes per day was associated with increased odds of future total cessation (Klemperer & Hughes, 2015). Furthermore, participants in the PWN pilot experienced a reduction in barriers to cessation (i.e., depression and perceived stress). Future studies are needed to test the effect of a longer, more intensive PWN intervention. In addition, future interventions should incorporate tailored interventions to promote smoke-free home policies. Among low-income smokers, the adoption of a smoke-free home policy is associated with increased smoking cessation, as well as an increase in cessation attempts and a reduction in cigarettes per day (Haardörfer et al., 2018).
There is a need to implement navigator programs within clinics that serve pregnant and postpartum women. Smoking has historically been overlooked as a “low priority issue” among women with co-occurring behavioral health issues (Prochaska, 2010; Schroeder & Morris, 2010). However, smoking abstinence is associated with a reduction in depression, anxiety, and stress and an improvement in mood (Taylor et al., 2014). Furthermore, among individuals with substance use disorders, smoking cessation has been associated with improved abstinence from other drugs and alcohol (Cavazos-Rehg et al., 2014; Kalman, Kim, DiGirolamo, Smelson, & Ziedonis, 2010; Prochaska, Delucchi, & Hall, 2004). Finally, among pregnant women with OUD, maternal smoking increases the likelihood and severity of neonatal abstinence syndrome observed in infants after birth (Jones et al., 2013), which provides further impetus for comprehensive clinical and social interventions that reduce barriers to smoking cessation and improve uptake and adherence to OUD treatment.
There were several limitations to this study. By design, the program did not employ randomization as study participants were recruited on a rolling basis for eligibility and enrollment was “first come, first serve.” Some participants (n = 12) completed the intervention but did not participate in postintervention assessment, which means that participants who were particularly motivated to quit smoking or improve health behaviors may be overrepresented in postintervention assessment results. In addition, participants facing the stigma of smoking while pregnant or in the early postpartum may underreport smoking-related behaviors; however, this concern is partially mitigated by testing for expired CO. There were also limitations regarding the analysis strategies employed in the statistical testing of assessment scores due to unbalanced baseline versus postintervention panels as well as small sample sizes, which means that statistical analysis had low power. Therefore, we could not discern statistically significant improvements when effect sizes were small. Despite these limitations, participation in the program resulted in reduced barriers to smoking cessation and improved psychosocial outcomes for this high-risk group of pregnant and postnatal patients.
Although the PWN program was minimally effective in promoting total tobacco abstinence, participants experienced a reduction in cigarettes smoked per day and nicotine dependence. Furthermore, participants experienced a reduction in stress and depression, which are major barriers to smoking cessation. The PWN intervention provided a necessary, innovative, and personalized service to address tobacco use in a high-risk group of pregnant and postpartum women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a March of Dimes Healthy Babies Are Worth the Wait grant.