
Abstract
New recommendations for hypertension (HTN) diagnosis and treatment highlight the role of self-care activities in managing blood pressure (BP). This cross-sectional study investigated the predictive validity of the Hypertension Self-Care Activity Level Effects (H-SCALE) measure and examined the relative and cumulative effects of HTN self-care adherence on BP. We pooled baseline data from three studies (N = 79), resulting in a gender and racially balanced sample. Partial correlations determined the relative effects of individual self-care behaviors on BP. We modeled the relationship between adherence to self-care behaviors and BP control using logistic regression. Physical activity had the greatest correlation with systolic BP. Adherence to each additional self-care behavior increased the odds of systolic BP control by 88% (95% confidence interval (CI) = [1.20, 2.96]) and diastolic BP control by 74% (95% CI = [1.10, 2.75]). Results provide further evidence that the H-SCALE is a valid assessment tool and should be adopted by clinicians to aid in improving BP management.
Hypertension (HTN) remains the leading cause of premature death in the United States (National Center for Health Statistics, 2017), with the highest prevalence rates observed in the southern states (Fang, Gillespie, Ayala, & Loustalot, 2018). Risk factors for HTN such as prediabetes and overweight/obesity are increasing in the U.S. population (Booth et al., 2017), including younger adults, thus increasing their risk for HTN at younger ages. Substantial gaps exist in individuals’ awareness, diagnosis, and treatment related to HTN (van Kleef & Spiering, 2017), which have invigorated efforts to address HTN nationally and globally (Frieden & Jaffe, 2018). Recent U.S. data indicate that use of antihypertensive medication among those who report a diagnosis of HTN is approximately 62% (Fang et al., 2018); among those receiving antihypertensive therapy in the United States, blood pressure (BP) control is just below 50% (Wall et al., 2018). However, these numbers do not reveal whether people with HTN are rigorous in following their medication regimen or what other lifestyle activities they may engage in to help manage their BP. Lifestyle behaviors play an important role in primary prevention of HTN (Bavikati et al., 2008) as well as secondary prevention as a complement to medication therapy in improving BP control (Lloyd-Jones et al., 2010).
Revised HTN Guidelines and Opportunities for Behavioral Counseling
In late 2017, the American College of Cardiology revised guidelines on HTN diagnosis and treatment for adults (Whelton et al., 2018). These new guidelines altered the HTN diagnostic criteria to identify those who are most at risk of developing HTN, and the guidelines recommend medication therapy earlier in the disease process. Based on these new criteria, overall HTN prevalence estimates among U.S. adults increased from 32% to 46%; the percentage of patients who need treatment with antihypertensive medication(s) (Stage 1 for those with systolic blood pressure [SBP] ≥130 mmHg and diastolic blood pressure [DBP] ≥80 mmHg and Stage 2 for individuals with SBP ≥140 mmHg and DBP ≥90 mmHg) increased from 34% to 36% (Muntner et al., 2018). Recommended treatment for individuals with elevated BP (SBP between 120 and 129 mmHg with DBP <80 mmHg) focuses solely on self-care behaviors, rather than medication (Whelton et al., 2018), shifting the treatment burden from pharmacotherapy to more time-intensive behavioral counseling. To effectively manage or control elevated BP, clinicians will require easy and valid tools to assess patients’ HTN self-care activities to provide appropriate recommendations and reach treatment goals. Moreover, patients with Stage 1 or Stage 2 HTN also need to focus on self-care behaviors in addition to antihypertensive medication adherence as medication alone (even when taken appropriately) is insufficient for BP control in many cases (Yaxley & Thambar, 2015).
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) identified six self-care activities related to weight management, diet, physical activity, moderate alcohol consumption, cessation of smoking, and following antihypertensive medication regimens (U.S. Department of Health and Human Services, 2004). More recently, the recommendations for diet and physical activity were confirmed by the American College of Cardiology and American Health Association Working Group of Lifestyle Management (Eckel et al., 2014). Lifestyle recommendations were absent from the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC8), which focuses on antihypertensive medication protocols based on available pharmacotherapies and addresses more intensive therapies when comorbidities are present (James et al., 2014).
Consistent with JNC7 lifestyle guidelines for BP management, the Hypertension Self-Care Activity Level Effects (H-SCALE) questionnaire assesses levels of adherence to antihypertensive medication, physical activity engagement, eating a healthy diet (based on the Dietary Approaches to Stop Hypertension [DASH] diet), weight management, and avoiding alcohol and tobacco (Warren-Findlow, Basalik, Dulin, Tapp, & Kuhn, 2013; Warren-Findlow, Coffman, & Karp, 2018; Warren-Findlow, Reeve, & Racine, 2017). Prior studies using the H-SCALE have assessed self-care adherence rates among community-dwelling and primary care patients with HTN. H-SCALE adherence levels varied, ranging from 12% for high DASH diet quality to 30% to 35% for weight management, approximately 50% for medication adherence, and 37% to 52% for physical activity adherence. Adherence rates were highest for primary and secondary tobacco exposure (71%-82%). Adherence to moderate alcohol consumption using gender-specific cut points ranges from 90% to 93% (U.S. Department of Health and Human Services, 2004). The H-SCALE has been used by more than 100 clinical researchers and students around the world to assess HTN self-care behaviors. It has been translated into French, Persian, Chinese, Thai, Nepalese, and Turkish, to name a few. A validated Spanish version is available from the author. The H-SCALE measure is based on self-reports and is easy to administer.
Purpose
The goal of the present study was threefold: one, to further assess the predictive ability of the H-SCALE with respect to SBP and DBP management; two, to examine the relative effects of the various HTN self-care behaviors on SBP and DBP to determine potential counseling priorities; and three, to investigate the relationship between cumulative adherence to HTN self-care activities and control of SBP/DBP. To our knowledge, no current measure exists that provides an overall adherence score for all JNC7-recommended self-care behaviors. This article contributes to clinical practice by giving health care providers evidence to address patient questions regarding “Which self-care behavior should I focus on to get the greatest effect on my BP?” “How much self-care is enough to achieve control of my BP?” and “How much more benefit will I get by being adherent to additional self-care behaviors?”
Method
Participants/Data Collection
This cross-sectional study pooled baseline data from three intervention studies conducted in North Carolina that assessed BP and self-care activities using the H-SCALE. Two studies included participants enrolled in intervention programs testing isometric exercise training (IET) to lower BP. The first was a community-based study of 22 individuals with HTN randomized to a group-based IET program, a home-based IET program, or a delayed control group (Gordon et al., 2018). Adults, aged 21 to 60 years with resting BP between 130/81 and 160/100 mmHg and/or who were prescribed antihypertensive medication, were recruited via email from a major university. In the second study, eight participants were recruited by clinic staff from an outpatient cardiopulmonary rehabilitation clinic of a major hospital, and these participants had diagnosed HTN and/or cardiopulmonary disease. Participants were randomized to either a control group or an IET intervention group. The third study was conducted in a low-cost, primary care clinic where adult patients with HTN (n = 49) who were taking at least one antihypertensive medication were recruited by clinic staff. Patient participants received a brief intervention designed to improve health literacy related to medication adherence and weight management (Warren-Findlow, Coffman, Vinoski Thomas, & Krinner, 2019). In all three studies, H-SCALE data were collected using paper-based surveys by trained research assistants. All participants had a diagnosis of HTN according to previous HTN guidelines (BP >140/90 mmHg). Prior publications with these individual samples did not report or analyze H-SCALE data and its association with BP. Ethical approval for all three studies was obtained from the University of North Carolina at Charlotte Institutional Review Board.
Measures
The H-SCALE consists of six subscales (31 items) which correspond to the six recommended domains of HTN self-care (Warren-Findlow et al., 2017; Warren-Findlow & Seymour, 2011). Five of the subscales measure frequency of engagement in self-behaviors over the past week; items in these subscales began with the stem, “How many of the past 7 days did you . . . ?” and have response options ranging from 0 to 7 days. The sixth subscale, which assesses weight management, is designed to measure strength of agreement to activities over the past 30 days.
Medication adherence was assessed with three items. A sample item is, “How many of the past 7 days did you take the recommended number of BP pills?” Responses were summed (range = 0-21). Respondents with a score of 21 were considered adherent. We use a more restrictive and thus conservative cut point (100%) than what has been the standard (80%; based on the proportion of pills taken from pills prescribed; Brown & Bussell, 2011; Osterberg & Blaschke, 2005) as we are not accounting for the number of antihypertensive medications prescribed, any comorbidities, or other factors influencing medication adherence.
Diet was assessed with 11 items (Warren-Findlow et al., 2017); this subscale (termed the DASH-Q) assesses nutritional intake consistent with the DASH diet. Responses were summed (range = 0-77), and participants with a score of 52 or higher were considered adherent (eating a high-quality diet consistent with DASH nutritional recommendations). DASH-Q cut points were established using a previously validated measure to determine diet quality and nutrition risk among older adults (see Warren-Findlow et al., 2017, for additional details).
Physical activity was measured with two items that assess aerobic physical activity; items were summed (range = 0-14). Participants who score an 8 or better were considered adherent and reported physical activity levels consistent with national recommendations of 150 min per week of moderate-intensity physical activity (Piercy et al., 2018).
Tobacco exposure was assessed with two items to determine personal smoking habits and exposure to environmental tobacco smoke. Responses were summed (range = 0-14). Only scores of zero were considered adherent.
Weight management consists of 10 items that measure activities that are undertaken to reduce or manage weight, such as reading food labels or reducing portion sizes. Responses range from “strongly disagree” to “strongly agree” using a 5-point Likert-type scale. Responses were summed (range = 10-50). Participants who reported that they agreed or strongly agreed with all 10 items (score ≥40) were considered to be adherent to effective weight management practices.
Alcohol intake was assessed with three items. The average number of days per week that the participant drinks were multiplied by the typical number of drinks that a person had in one sitting, to create a continuous variable ranging from zero to infinity. In this study, we followed JNC7 guidelines, categorizing adherence to moderate alcohol consumption among men as ≤2 drinks/day (scores of 14 or less over the 7-day response period) and ≤1 drink/day for women (scores of 7 or less).
For all subscale scores, we allowed for one to two missing responses. Across all subscales and respondents, we were missing 0.15% of responses (four out of 2,607). In all instances, having complete data for the subscale would not have altered the respondent’s level of adherence for any behavior.
Cumulative adherence was calculated by summing adherence values (0 or 1) from the six subscales (range = 0-6). For this sample, we allowed for one missing value, as we only have DASH-Q responses from 22 participants. We termed this construct the H-SCALE index.
Demographic characteristics of age, race, and gender were self-reported. Race was categorized as White, African American, or Hispanic.
SBP and DBP were measured via individual study protocols (Gordon et al., 2018). BP was obtained by trained research assistants (either Kinesiology or Nursing students) using an automated oscillometric sphygmomanometer (American Diagnostic Corporation, Adview 9000 Hauppauge, NY) or by following the American Heart Association (AHA) protocol using a manual sphygmomanometer (Pickering et al., 2005). At least two measures were obtained and then averaged together. Controlled SBP was categorized as SBP <130 mmHg. DBP control was categorized as DBP <90 mmHg. As all participants were enrolled prior to the revision in HTN diagnosis guidelines (Whelton et al., 2018), we applied the older standard for BP control.
Data Analysis
Descriptive statistics were used to analyze sample characteristics. Each H-SCALE subscale was scored and tested for internal consistency using a Cronbach’s alpha. We used the continuous form of each subscale score to perform unadjusted and adjusted correlations with SBP and DBP to determine the relative effect of a specific behavior. Adjusted correlations included the other H-SCALE subscales as well as age, race, and gender. We also performed correlations between the H-SCALE index and SBP and DBP, adjusting for participants’ demographic characteristics.
To assess the cumulative effect of self-care adherence, we performed unadjusted and adjusted logistic regression to model the average effect of increasing self-care adherence on control of SBP and DBP. Relationships were adjusted for age, race, and gender.
Results
Participant Characteristics
Participants (N = 79) were on average in their mid-50s (mean age = 54.1, SD = 9.5), 54% were female, and approximately equal numbers of participants were White (34%), African American (33%), or Hispanic (30%). Average SBP and DBP were 134.1 and 86.5 mmHg, respectively. Only 39% of participants had their SBP controlled and 66% had controlled DBP. Participants with data on all six H-SCALE behaviors (n = 22) were adherent to a mean of 3.4 behaviors versus those with five H-SCALE behaviors (n = 57) had a mean of 3.1.
Characteristics of H-SCALE Subscales
Internal consistency of the H-SCALE subscales ranged from α = .56 for tobacco use (which contains only two items) to .90 for the alcohol intake subscale. Analyses suggest that internal consistency for the DASH-Q subscale would be improved if the item “How many days of the week do you eat pickled vegetables?” was removed (α = .67 vs. .73). The other subscales had good internal consistency with Cronbach’s alphas >.70.
HTN Self-Care Adherence by Age, Gender, and Race
Table 1 presents H-SCALE subscale scores by level of adherence. For the pooled sample, adherence rates to individual self-care behaviors were highest in the alcohol and smoking subscales (89% and 82%, respectively). Lowest adherence was reported in the DASH-Q subscale (18%, n = 22). Adherence to other self-care behaviors ranged from 39% for weight management to 56% for medication adherence. Analyses by age, gender, and race indicated few significant differences. Only medication adherence prevalence differed significantly by race, with African Americans having substantially lower levels of medication adherence as compared with Whites and Hispanics.
Hypertension Self-Care Adherence Levels of Age, Gender, and Race.
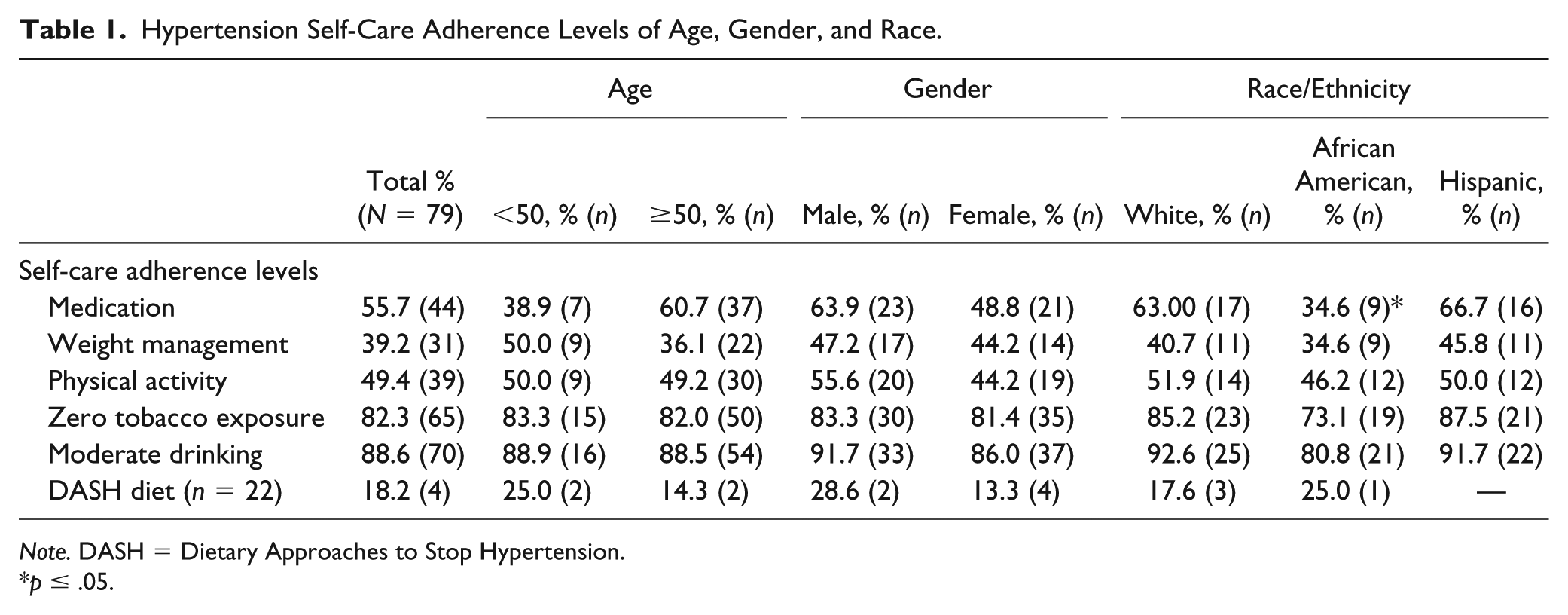
Note. DASH = Dietary Approaches to Stop Hypertension.
p ≤ .05.
In terms of overall adherence to the set of self-care behaviors, there were no significant differences by age, gender, or race with respect to the mean number of behaviors to which participants adhered (data not shown).
H-SCALE Subscales and BP
All H-SCALE score correlations were theoretically consistent with SBP and DBP (see Table 2). Higher adherence scores for four of the six subscales have a negative relationship with increasing BP. For tobacco and alcohol, where lower scores indicate greater adherence, the relationship with increasing BP is positive. H-SCALE subscale scores were significantly correlated with SBP in two of the six domains. Medication adherence (mean = 18.70 ± 4.56) had a modest but significant correlation with SBP and DBP; however, after adjusting for demographics and the other H-SCALE subscales, the relationships between medication adherence and SBP and DBP were not significant. Physical activity (mean = 7.11 ± 4.08) had a statistically significant, moderate correlation with SBP, r(79) = −.32, N = 79, p < .01, in the unadjusted model. This relationship was attenuated but remained significant after controlling for demographics and the other H-SCALE subscale scores. The DASH-Q subscale had a moderately strong relationship with DBP, but the sample was too small to achieve sufficient statistical power. These results suggest that the predictive validity of the individual subscales is solid, given the limitations of the small sample.
H-SCALE Subscale and Overall Index Correlations With Systolic and Diastolic BP Adjusted for Age, Gender, and Race (N = 79).
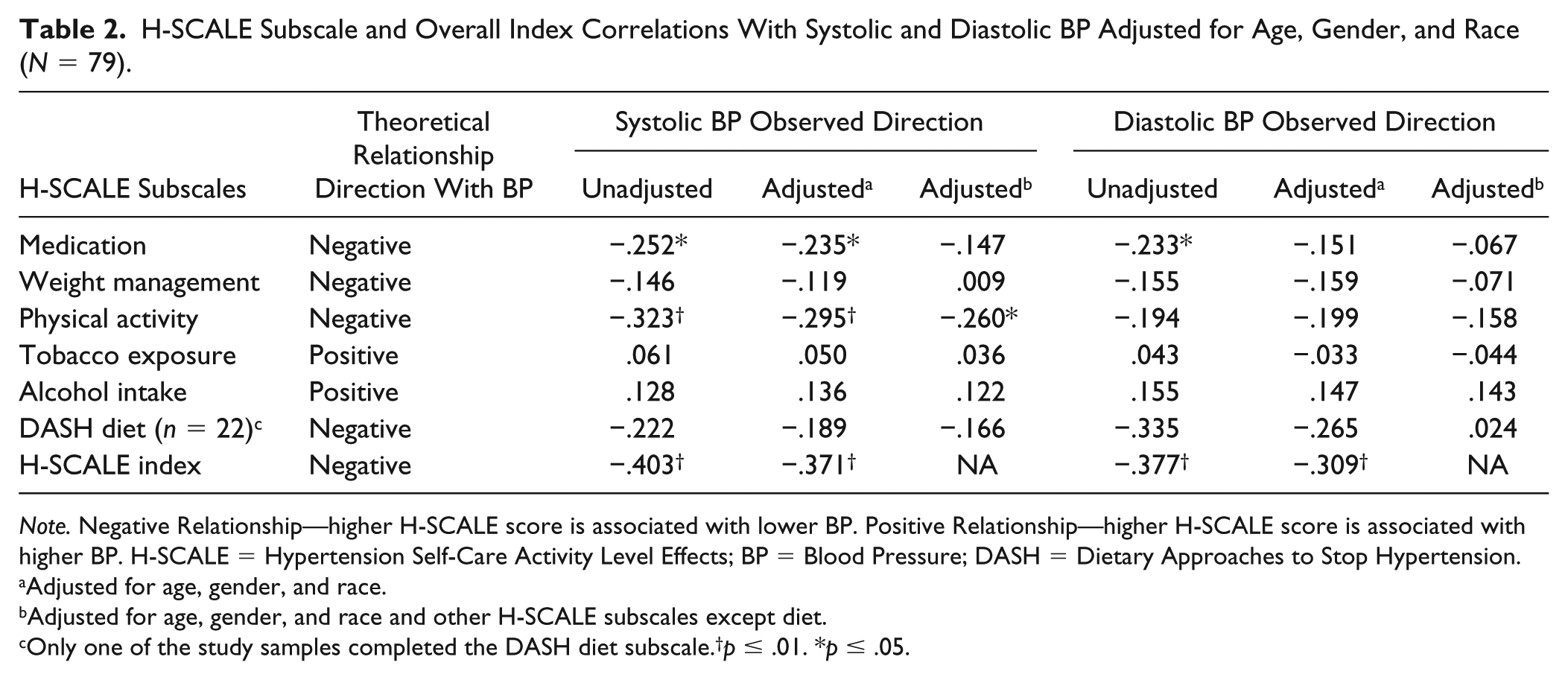
Note. Negative Relationship—higher H-SCALE score is associated with lower BP. Positive Relationship—higher H-SCALE score is associated with higher BP. H-SCALE = Hypertension Self-Care Activity Level Effects; BP = Blood Pressure; DASH = Dietary Approaches to Stop Hypertension.
Adjusted for age, gender, and race.
Adjusted for age, gender, and race and other H-SCALE subscales except diet.
Only one of the study samples completed the DASH diet subscale.†p ≤ .01. *p ≤ .05.
In comparison with other behaviors, physical activity had the strongest correlation with SBP. Results for physical activity correlations with DBP were not significant.
The H-SCALE index (mean = 3.20 ± 1.25) had a modest but significant correlation with SBP in unadjusted, r(79) = −.40, N = 79, p < .01, and adjusted, r(73) = −.37, N = 79, p < .01, analyses. Results were similar for the H-SCALE index and DBP in terms of strength of the association, significance, and attenuation after adjusting for demographic characteristics.
Cumulative Effects of Adherence to HTN Self-Care Behaviors
Table 3 presents unadjusted and adjusted (by age, gender, and race) odds ratios (ORs) and 95% confidence intervals (95% CI) for the cumulative effects of H-SCALE adherence levels on control of SBP and DBP. On average, the odds of having controlled SBP (<130 mmHg) increased by 84% (95% CI = [1.19, 2.82]) for each additional self-care activity where adherence was achieved. The odds of having controlled DBP (<90 mmHg) increased with every additional adherence score on average by 76% [1.15, 2.69]. These associations are slightly modified when controlled for age, gender, and race but remain statistically significant.
Cumulative Effects of Hypertension Self-Care Behavior Adherence on BP Control (N = 79).
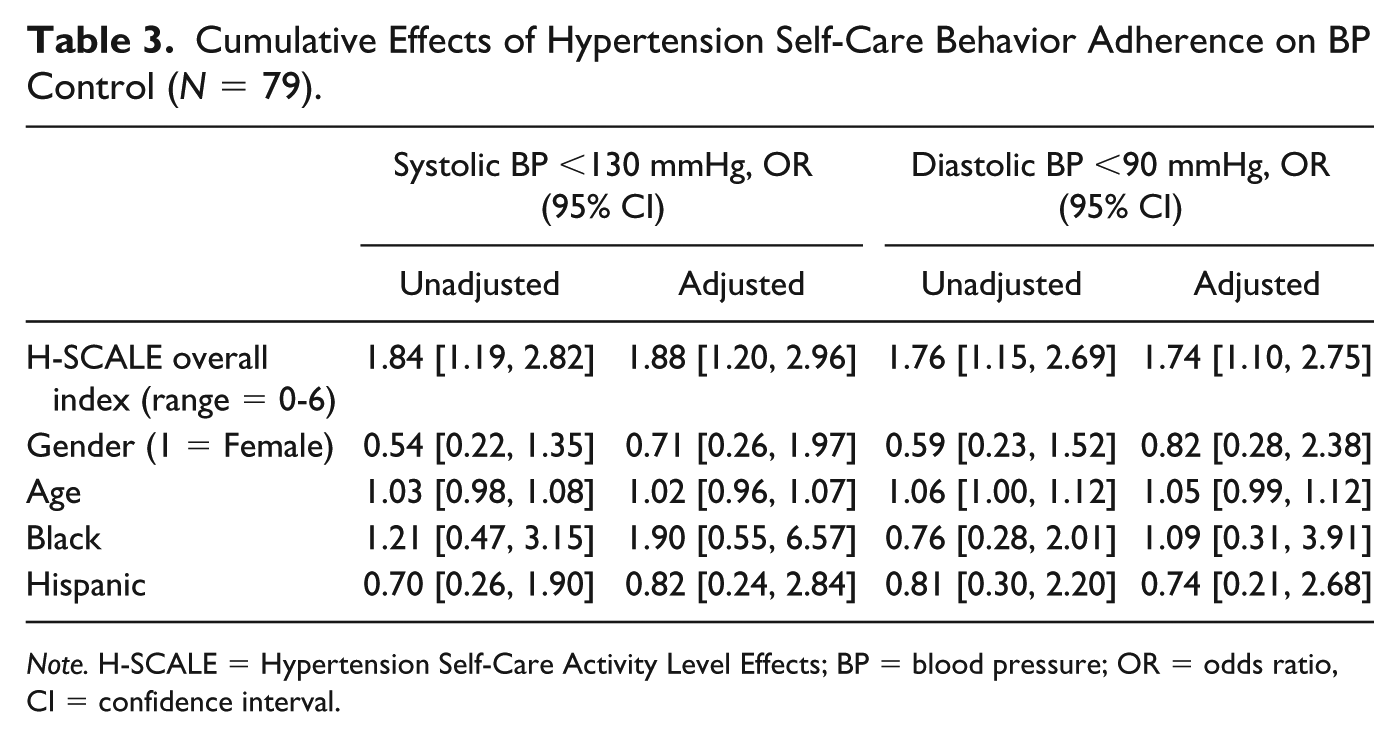
Note. H-SCALE = Hypertension Self-Care Activity Level Effects; BP = blood pressure; OR = odds ratio, CI = confidence interval.
Discussion
New guidelines for HTN diagnosis and treatment have heightened the need for data on lifestyle behaviors among individuals with SBP >120 mmHg (Whelton et al., 2018). Current population-based data are limited and insufficient for behavioral counseling purposes. Although other tools measure factors that contribute to HTN self-care behaviors such as motivation and self-efficacy (Han, Lee, Commodore-Mensah, & Kim, 2014) or barriers to adherence (Morisky, Green, & Levine, 1986), the H-SCALE directly assesses levels of adherence to the recommended activities related to BP management.
In comparison with prior studies using the H-SCALE, H-SCALE scores for this sample were consistent with previous studies for medication, weight management, and physical activity mean scores (Warren-Findlow et al., 2013; Warren-Findlow & Seymour, 2011). Participants in the current pooled sample reported less tobacco exposure (M = 1.05 days vs. 2.90 days) than a sample of primary care patients with HTN (Warren-Findlow et al., 2013). However, the pooled sample reported twice as much alcohol intake as the former primary care sample (M = 2.93 compared with 1.46). Participants in the current study reported eating a better quality diet than participants with HTN in the national sample used to develop the DASH-Q (39.55 vs. 35.49) (Warren-Findlow et al., 2017).
Compared with population-based studies of adherence with respect to lifestyle behaviors, the study sample was consistent with national samples on meeting aerobic physical activity guidelines (Piercy et al., 2018) and moderate alcohol consumption (Esser et al., 2014). Tobacco exposure rates were mixed; actual rates of smoking were lower than national rates, but tobacco exposure rates were driven by higher secondhand smoke exposure levels (Centers for Disease Control and Prevention, 2019). Diet adherence levels are difficult to compare, but our results are not inconsistent with extant literature indicating very low adherence to the DASH diet in the community (Epstein et al., 2012; Folsom, Parker, & Harnack, 2007). Similarly, there are no directly comparable estimates of weight management activities, but our findings are consistent with studies reporting on weight loss practices (Burroughs et al., 2010) and food label reading among individuals with HTN (Lewis et al., 2009).
Overall, H-SCALE adherence levels did not differ based on demographics. Results indicated significantly lower medication adherence levels among African Americans compared with Whites and Hispanics. These findings were consistent with previous research examining racial and ethnic differences (Gerber, Cho, Arozullah, & Lee, 2010; Holmes et al., 2012; van der Laan et al., 2017) and gender differences in medication adherence (Holt et al., 2013). Our results conflict with prior studies that have reported significant differences between race/ethnicities, gender, and age groups with respect to adherence to HTN-related health behaviors (Abegaz, Shehab, Gebreyohannes, Bhagavathula, & Elnour, 2017; Epstein et al., 2012; Minges et al., 2017). The African Americans in our sample reported lower rates of zero tobacco exposure consistent with recent statistics, indicating that half of non-Hispanic Black nonsmokers had secondhand smoke exposure based on self-reports and serum cotinine levels (Tsai et al., 2018).
Psychometrically, the H-SCALE subscales demonstrate sufficient internal consistency, given the sample size and number of items per subscale. We found indications that the internal consistency of the DASH-Q subscale could be improved by removing one item, which is reverse scored, but we elected to retain that item, given that our sample was already limited for this subscale.
Furthermore, all H-SCALE subscale scores are theoretically consistent with BP. This finding is especially important for the DASH-Q as the original version of the diet subscale was problematic (Warren-Findlow et al., 2013), resulting in substantial revisions with more rigorous development (Warren-Findlow et al., 2017). The results from this study suggest that those prior issues have been addressed. Furthermore, increasing adherence to individual self-care behaviors as determined by the H-SCALE index is associated with management of SBP and DBP according to clinical guidelines.
Relative to the other self-care behaviors, aerobic physical activity had the strongest correlation with BP in the present study. This finding is partially consistent with previous research using the H-SCALE (Warren-Findlow et al., 2013). The magnitude of the relationship in this study was stronger than a previous sample of primary care patients (Warren-Findlow et al., 2013). While two of the three samples we used were participants enrolled in exercise interventions, those interventions were strength-based in nature, and we used only baseline data for our analysis. However, those participants reported higher levels of physical activity and may have self-selected into those studies, potentially biasing our results.
Despite clinicians’ focus on medication to treat BP, medication adherence prevalence was only approximately 56%, and adherence was not strongly correlated with SBP or DBP once we controlled for other self-care activities. One possible interpretation is that some participants may prefer to engage in other lifestyle behaviors to avoid having to take medication or take it in the recommended dosage. Cost and side effects of antihypertensive medications, and poor relationships between patients and providers are significant factors contributing to nonadherence (Tedla & Bautista, 2016; van der Laan et al., 2017). However, no studies on medication adherence assess patients’ other HTN self-care activities. Larger samples are needed to see whether this finding remains consistent and what other factors might influence this relationship.
Tentatively, based on these results, clinicians should focus on counseling patients to “move more” in conjunction with following prescribed medication regimens. Diet appears to have the next greatest effect, which is consistent on research with the DASH diet (Juraschek, Miller, Weaver, & Appel, 2017).
Our study is the first to present an overall adherence index for the recommended HTN self-care behaviors according to JNC7 guidelines. The 73% to 80% (DBP and SBP, respectively) increased odds of BP control for adherence to each additional behavior contribute to the evidence supporting the importance of counseling individuals on HTN self-care behaviors and on helping them to achieve adherence. Notably, the 95% CIs are narrow despite the small sample size and the difference in the number of outcomes between SBP and DBP.
Researchers should interpret our study findings with a few caveats. Larger sample sizes will be needed for further validation of the DASH-Q and for evidence of the validity and usefulness of the H-SCALE overall score of self-care behavior adherence. The use of cut points to establish adherence is controversial, given that participation in health behaviors is conceptually on a continuum. However, our criteria for adherence align as much as possible with established clinical or policy recommendations for health. In addition, having a particular goal with respect to a health behavior addresses patients’ desire to know the minimum or sufficient level of effort to exert to achieve BP control. We were unable to control for the number of antihypertensive medications that participants may have been taking, the presence and severity of other comorbidities, and/or prior cardiovascular events, which affect more clinically specific guidelines for BP diagnosis and BP treatment goals. Furthermore, we had incomplete data on body mass index, a key contributor to HTN development.
Some notable strengths of this study include the balanced racial and ethnic representation, gender equivalency, and diversity of settings and health status across the three samples. Importantly, the H-SCALE assesses the comprehensive set of recommended HTN self-care behaviors. These data permit us to evaluate and control for the full range of activities that influence BP. We were able to obtain BPs at baseline concurrent with the self-care data, which increased evidence for the predictive value of the H-SCALE subscales.
Future studies will include larger samples and also recruit individuals who meet the category of elevated BP, who have not yet been prescribed antihypertensive medications. Lifestyle activities may be particularly important to this population so that they can avoid the need for medication therapy. Additional studies should also examine alternative scoring methods for the H-SCALE overall index such as weighting the subscale adherence levels. We are also interested in pursuing further research on the relative effect of physical activity on BP and including strength training items in the H-SCALE to better align with guidelines calling for strength training 2 days per week.
We found additional data to support the psychometric robustness and validity of the H-SCALE. The preliminary results for the DASH-Q suggest that it will be similarly sound. Relative to the other self-care behaviors, physical activity had the greatest correlation with SBP, consistent with existing evidence for HTN lifestyle recommendations (Eckel et al., 2014). Findings suggest that the H-SCALE is a valuable tool for assessing HTN self-care activities and is strongly associated with BP management. We also demonstrated that the H-SCALE overall index for self-care behavior adherence is a valid and useful measure for determining the effects of self-care adherence on BP control.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors received partial financial support for this research from the University of North Carolina Charlotte.