
Abstract
The purpose of this study was to examine whether parental self-efficacy (PSE) is associated with change in infant weight-for-length z score (WLZ) from age 3 to 12 months. Data were drawn from the Infant Care, Feeding, and Risk of Obesity study, conducted with low-income, African American mother–infant dyads (n = 127). PSE was measured at infant age of 3 months. Infant anthropometrics were measured at infant age of 3 and 12 months, WLZ change between these time points was calculated, and infants stratified into WLZ change categories (expected, excessive, or slow). To analyze the data, ANCOVA, multiple regression, and post hoc techniques were used. Controlling for infant birthweight, PSE at 3 months was associated with infant WLZ change (η2 = 0.05, p = .04). Mothers of infants who exhibited excessive growth had higher PSE than mothers of infants who exhibited slow growth (Tukey-adjusted p = .03). This finding suggests that infants of mothers with high PSE may have increased obesity risk, but more research is needed.
Health care providers monitor infant weight gain closely by following the growth trajectory of an infant between birth and 12 months of age. Traditionally, the primary concern of providers was the infant whose weight fell off the growth curve (i.e., failure to thrive); however, pediatricians and other pediatric health care providers are becoming increasingly aware that infants whose growth exhibits an upward crossing of percentiles have greater risk for childhood obesity and subsequent cardiometabolic consequences (Druet et al., 2012; Vogelezang et al., 2019; Woo, 2019). Some factors contributing to this excessive growth pattern are clear in the literature. For example, formula-fed infants and those from low socioeconomic status (SES) families tend to experience a greater rate of weight gain compared with breast fed infants or those from middle or high SES families (Gibbs & Forste, 2014; Li, Magadia, Fein, & Grummer-Strawn, 2012). In addition, African American infants tend to experience excessive weight gain as compared with Caucasian infants (Shinn, Tangney, Busche, Sharp, & Mullen, 2018; Taveras, Gillman, Kleinman, Rich-Edwards, & Rifas-Shiman, 2010). Biological factors such as race or ethnicity cannot be changed, however, psychosocial factors have the potential to be modified if an association with infant weight gain is identified.
Parental self-efficacy (PSE) is an understudied psychosocial factor associated with infant feeding and growth (Bahorski et al., 2018). PSE is the belief a parent has in their ability to accomplish the tasks of parenting and is an important predictor of parental decision making during infancy (Fong et al., 2018; Liyana Amin, Tam, & Shorey, 2018; Salonen et al., 2009). Parents with high PSE are more likely to make a successful transition to parenthood, be more confident in their parenting decisions, and be better emotionally adjusted (Coleman & Karraker, 1997; Liyana Amin et al., 2018; Salonen et al., 2009). Research has demonstrated that infants and toddlers (up to age 2 years) of parents with higher PSE are more likely to have healthier dietary practices such as increased intake of fruits and vegetables, and decreased intake of sugar sweetened beverages (Koh et al., 2014; Spence, Campbell, Crawford, McNaughton, & Hesketh, 2014; Xu, Wen, Rissel, Flood, & Baur, 2013). Furthermore, high PSE has been associated with parenting behaviors, which may prevent obesity such as positive feeding styles (Barrett, Thompson, & Bentley, 2016; Salarkia, Omidvar, Zaeri, Zeinab, & Neyestani, 2016) and the ability to overcome barriers to prevent obesity in their children (Kahlor, Mackert, Junker, & Tyler, 2011). For these reasons, it is plausible that an association between PSE and infant growth gain may exist.
To our knowledge, no prior study has examined the assocation between PSE and infant growth. Only one cross-sectional study has reported a trend for PSE to be positively associated with infant body mass index score (BMI) in a group of well-educated, middle SES, Caucasian American mother–infant dyads, but this association did not reach statistical significance (Stifter, Anzman-Frasca, Birch, & Voegtline, 2011). It is possible that PSE will be more closely associated with infant growth among infants who are at greatest risk for excessive weight gain such as those from low SES or minority race.
Purpose
Due to evidence that PSE is associated with many aspects of parenting and the dearth of literature regarding PSE specific to infant weight gain, this study was undertaken. The purpose was to examine whether PSE is associated with infant weight-for-length z score (WLZ) change in a group of first-time, low-income, African American mother–infant dyads.
Method
Design/Participants
This correlational study was a secondary analysis conducted with data from the Infant Care, Feeding, and Risk of Obesity Study (Infant Care) (NIH/NICHD RO1 HD042219-02, Bentley et al., 2003). These data were collected between 2003 and 2007 from first-time, low-income, African American mothers and their infants. The aim of the Infant Care study was to identify the constellation of household, caregiver, and child characteristics associated with the risk of childhood obesity (Bentley et al., 2003). All participants were recruited between birth and infant age of 3 months from Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) centers in central North Carolina. First time, African American mothers between the ages of 18 and 35 years and their infants were eligible if the infant was born greater than 35 weeks gestation with a birthweight between 2,500 and 4,500 g and without any medical complications (i.e., Down Syndrome, cerebral palsy). Infants diagnosed with failure to thrive or conditions that may interfere with feeding or growth (i.e., cleft lip/palate, severe food allergy) were ineligible. The cohort of mother–infant dyads (n = 217) was followed from infant age of three months to 18 months. Each mother provided consent for herself and her infant at study enrollment.
The current study used a subset of the Infant Care data; mother–infant dyads with infants who had complete weight and length measurement at the 3 and 12 month time points were included (n = 128). Permission for use of the Infant Care data was obtained from the principal investigator. The Infant Care study and the current study were approved by the appropriate university institutional review board.
Measures
Infant WLZ scores
Infant Care study personnel conducted home visits with the dyads at each time point. Study personnel were trained in collecting infant weight and length. Infants were weighed in a dry diaper on a digital scale (Tanita BD-585 Digital Baby Scale) with weight recorded to the nearest 10 g. Recumbent length was measured using a portable length board (O’Leary Length Board) to the nearest 0.1 cm by a two-person team. All measures were performed 3 times and the mean used in analyses. This method of measurement is consistent with that used to collect anthropometric data in the National Health and Nutrition Examination Survey (NHANES) and was used in development of the World Health Organization (WHO) reference data for infant growth (Centers for Disease Control and Prevention, 2017; De Onis et al., 2004).
For the current analysis, z scores were calculated based on the WHO reference data for the 3-month and 12-month time points. Z scores are a standard deviation score and considered the best method to analyze anthropometric data in research (WHO, 2017). To exam infant growth in this study, WLZ at 3 months was subtracted from the WLZ at 12 months to create growth change variable. To classify infants into categories based on this change, the method suggested by Ong, Ahmed, Emmett, Preece, and Dunger (2000) was used. In this method, a z score change of > –0.67 and < 0.67 is considered expected growth, whereas a change outside these parameters is either excessive or slow growth (z score change > 0.67 is considered excessive growth and < 0.67 considered slow) (Ong et al., 2000). Many studies have used this method to stratify infants into those who exhibited excessive growth, expected growth, or slow growth. Prior studies have consistently shown that infants who exhibited excessive growth, according to this definition, have greater risk for obesity later in childhood (Nanri et al., 2017; Sutharsan, O’Callaghan, Williams, Najman, & Mamun, 2015; Zhou et al., 2016). Therefore, this method was chosen for the current study as a measure of infant WLZ change through the first year of life.
PSE
The Parenting Sense of Competence Scale (PSOC) was used in the Infant Care study to measure PSE and satisfaction with parenting. Mothers completed this tool at the first study time point, infant age of 3 months. Developed by Gibaud-Wallston and Wandersman in the 1970s, the PSOC consists of two subscales, efficacy and satisfaction (Gibaud-Wallston, 1977). For the current study, only the eight-question efficacy subscale was used (Table 1), which measures “parents’ perception of the degree to which they have the acquired skills and understanding to be a good parent” (Gibaud-Wallston, 1977, p. 39). Each question had a Likert-type scale with six responses that ranged from strongly disagree (given a score of 1) to strongly agree (given a score of 6). The score from each question was summed providing a total score ranging from eight (indicative of a low sense of PSE) to 48 (indicating a high sense of PSE). No cut-off score for high versus low PSE has been identified for the PSOC. The scale has been deemed valid and reliable for use in mothers of infants with alpha coefficients ranging from .68 (Gilmore & Cuskelly, 2009) to .8 (Gibaud-Wallston, 1977; Ohan, Leung, & Johnston, 2000). In the subset of the Infant Care data used in the current study, the alpha coefficient demonstrated acceptable internal reliability (α = .70).
Efficacy Subscale of the Parenting Sense of Competence Scale.
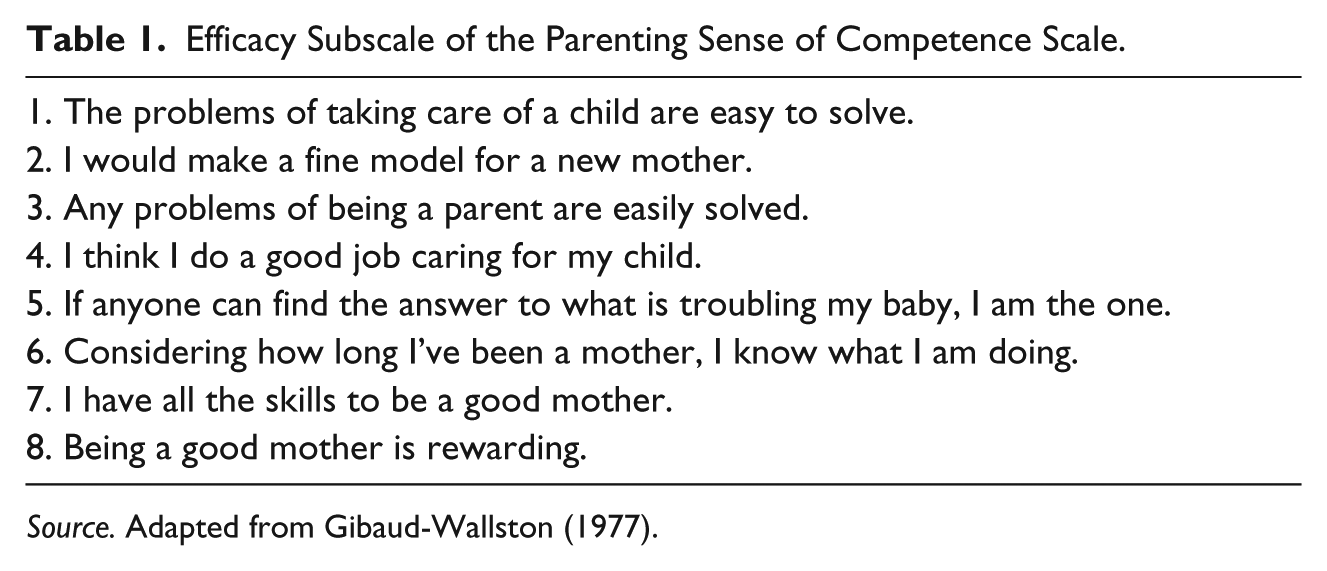
Source. Adapted from Gibaud-Wallston (1977).
Covariates
Variables from the Infant Care data set were included as potential covariates if prior research suggested that the variable may be important when examining infant growth. Covariates included infant birthweight, infant temperament, maternal sociodemographic factors (age, marital status, education level), maternal BMI, maternal depression level, maternal perception of infant weight status, ever breastfed, duration of breastfeeding if breast fed, and age at first complementary food. At the first Infant Care visit, mothers self-reported her infant’s birthweight as well as her age, marital status, and education level. Also, at the first visit, maternal height and weight were measured by the Infant Care–trained research personnel and used to calculate BMI.
Mother’s perception of her infant’s temperament was measured using two subscales of the Infant Behavior Questionnaire–Revised (IBQ-R); activity level and distress to limitations. These two subscales were chosen because prior analysis found an association with WLZ in the Infant Care sample (Slining, Adair, Goldman, Borja, & Bentley, 2009). Prior studies have demonstrated reliability of the IBQ-R in the Infant Care data set (Slining et al., 2009; Wasser et al., 2011). Maternal risk for depression was collected via self-report using the Center for Epidemiologic Studies Depression scale (CESD). The alpha coefficient in this subset of the Infant Care data demonstrated internal reliability (α = .85).
At each Infant Care visit, mothers were asked to indicate their perception of their infant’s weight status per one of the following categories: very overweight, overweight, normal weight, underweight, and very underweight. For the current study, this response was compared with the infant’s weight-for-length percentile based on age and sex per the WHO growth charts. Infants whose weight-for-length was > 90th percentile were considered overweight, infants between the 10th and 90th percentile were considered appropriate, and infants < the 10th percentile were considered underweight. A dichotomous variable was created indicating whether the mother’s perception of the infant’s weight for length was concordant with the infant’s percentile, coded as “yes” if concordant, or “no” if discordant.
At each study time point, mothers completed a 3-month infant diet history. The infant dietary history questionnaire was created by the Infant Care researchers for use in the study and was modeled after the tool used in the Infant Feeding Practices Study II (Fein et al., 2008). From data at the first study visit (infant age of 3 months), mothers reported whether her infant was ever breastfed then a dichotomous variable was created for ever breast fed. For breastfed infants, mothers were asked at the 3-month visit and each subsequent visit whether she was still breastfeeding her infant, if not, she reported the age of her infant, in months, when breastfeeding was discontinued. A variable with duration of breastfeeding in months was created for this study. Finally, age of first complementary food (any food or drink other than breastmilk for formula) was gathered through analysis of the infant feeding history questionnaire. This questionnaire included a list of foods and drinks, mothers were asked to indicate whether her infant had received any of these products during each month of life. Data were extracted to create a variable indicating the age in months the infant first received a complementary food.
Data Analysis
Sample size
Of the 128 infants with complete WLZ data, one maternal PSE score at 3 months was missing. Therefore, analyses were conducted on the 127 mother–infant dyads with complete data. A detectable effect size computation (G*Power Version 3.1.9.2) was conducted given the sample size available in the Infant Care data set with complete infant WLZ data (n = 127). Assuming a linear regression model for the numerical outcome of PSE, three coefficients (WLZ trajectories [three trajectories] and birthweight), a significance level of 0.05, and with 80% power, the detectable effect size is 0.08 (R2), a small-to-medium effect (Cohen, 1988).
Analyses
Initial bivariate analyses were conducted to determine which covariates to control for in adjusted models testing the association between PSE and WLZ categories. For continuous variables, analysis of variance (ANOVA) and partial eta square were calculated, and for categorical variables, chi-square tests and Cramer’s V were calculated. To test the hypothesis that PSE is associated with WLZ trajectories, analysis of covariance (ANCOVA) was calculated, adjusting for any covariates that were significant in the initial analyses. If the overall model was significant, follow-up multiple regression analyses were calculated to determine which WLZ trajectories were different while adjusting for significant covariates. Partial eta square was used as a measure of effect size. R and R Studio Version 3.4.3 were used for all analyses (RStudio Team, Boston, MA, 2016).
Results
Descriptive statistics of the sample are presented in Tables 2 and 3. This subsample was, in general, similar to the full Infant Care sample, no significant differences among any variables existed. This group of mothers were primarily single, overweight, and about half had education beyond high school. Infant feeding practices indicated that most mothers (73.4%) initiated breastfeeding with a mean duration of 4 months. Of note, no mothers were exclusively breastfeeding at infant age of 3 months. Mean age of complementary food introduction was 2.7 months. PSE scores of mothers at infant age of 3 months ranged from 23 to 48 (M = 38.5, SD = 4.6). Infant WLZ change categories from 3 to 12 months were as follows: 46.1% exhibited expected growth, 35.9% exhibited excessive growth, and 18.0% exhibited slow growth.
Descriptive Statistics, Continuous Variables (n = 128).
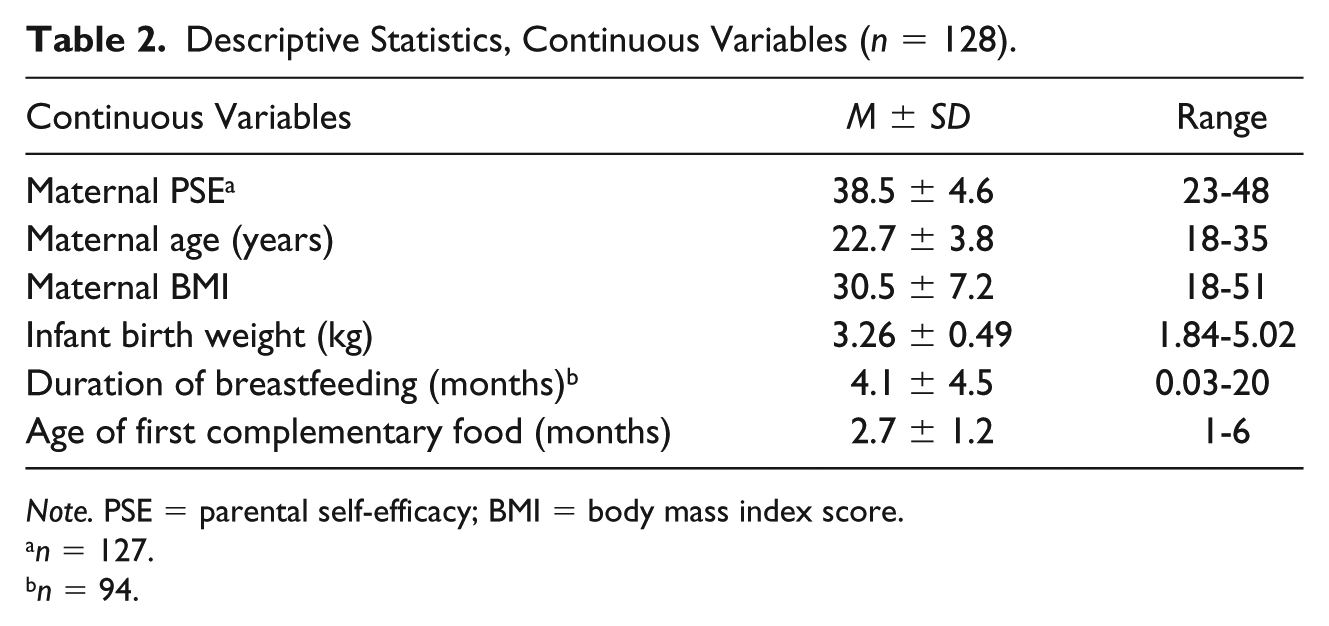
Note. PSE = parental self-efficacy; BMI = body mass index score.
n = 127.
n = 94.
Descriptive Statistics, Categorical Variables (n = 128).
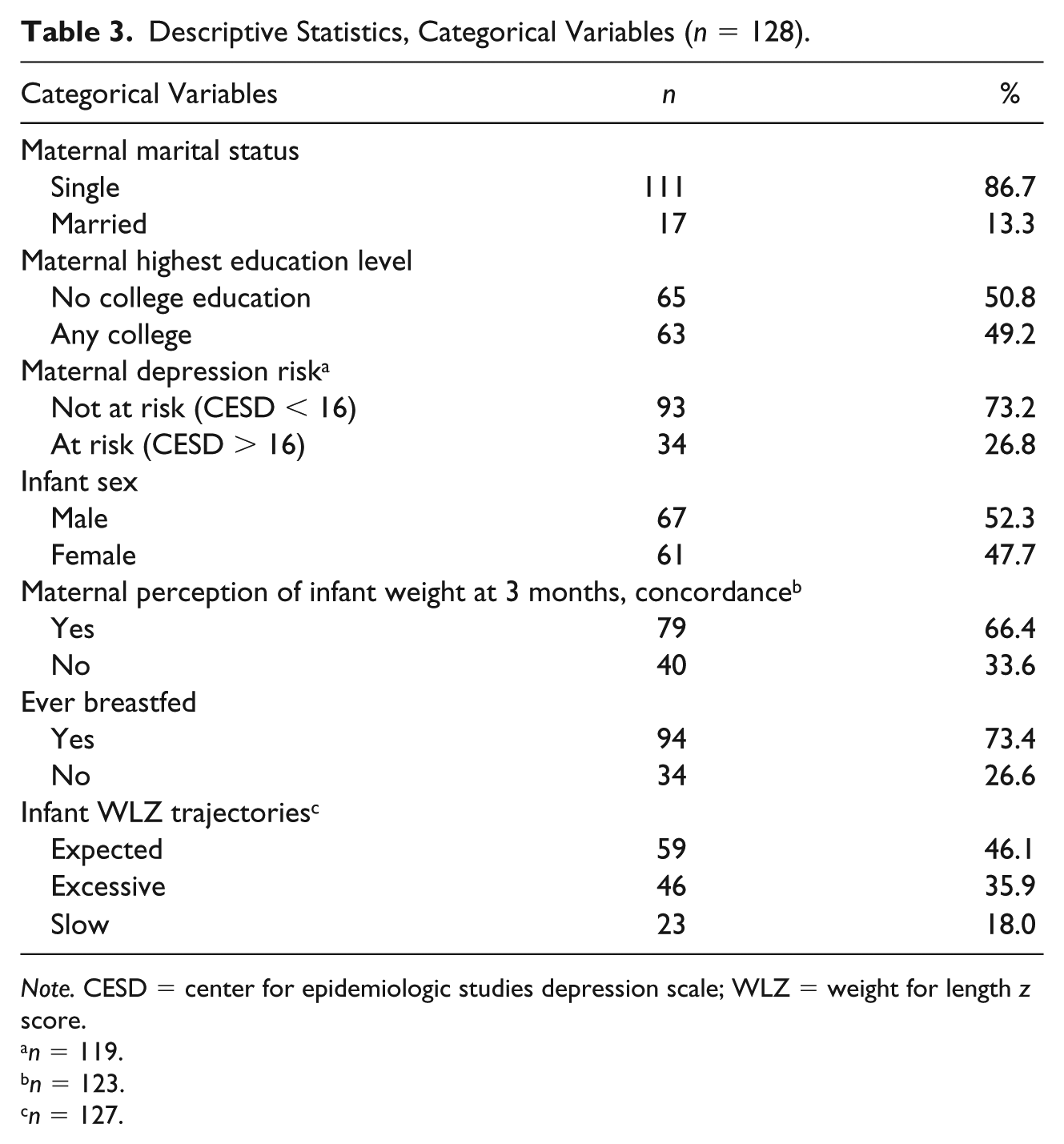
Note. CESD = center for epidemiologic studies depression scale; WLZ = weight for length z score.
n = 119.
n = 123.
n = 127.
Association Between WLZ Change and Covariates
All covariates were analyzed individually for an association with each WLZ category (Table 4). Infant birthweight was the only covariate significantly associated with the WLZ change; a medium association was seen (η2 = 0.1, p = .001). Average birthweight for the infants who exhibited excessive WLZ change was 3.45 kg, which was significantly greater than the birthweight of infants who exhibited slow WLZ change (M = 3.03 kg, p < .01) or expected WLZ change (M = 3.21 kg, p < .01). Maternal perception of infant’s weight status (V = 0.21, p = .07) and perception of infant’s distress to limitation (η2 = 0.04, p = .063 months showed a small to medium effect on infant WLZ change, but were not statistically significant. No relevant associations were observed with the remaining covariates, including the infant feeding practices.
Association Between WLZ Change Categories and Covariates (n = 128).
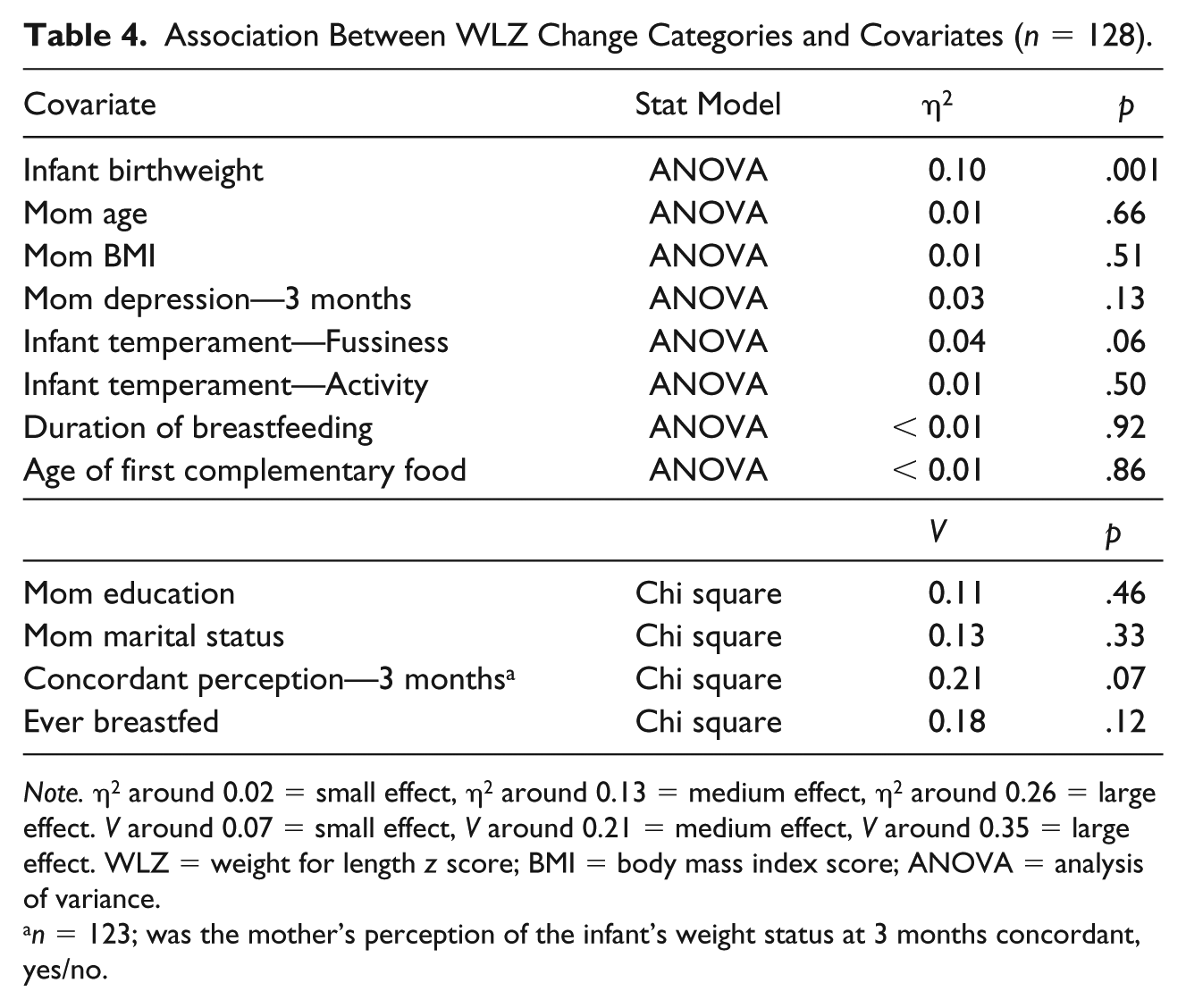
Note. η2 around 0.02 = small effect, η2 around 0.13 = medium effect, η2 around 0.26 = large effect. V around 0.07 = small effect, V around 0.21 = medium effect, V around 0.35 = large effect. WLZ = weight for length z score; BMI = body mass index score; ANOVA = analysis of variance.
n = 123; was the mother’s perception of the infant’s weight status at 3 months concordant, yes/no.
Association Between PSE and WLZ Change
Using ANCOVA, the association between PSE and WLZ change category was examined while controlling for infant birth weight. Results of this model indicated a significant, small to medium association (η2 = 0.05, p = .04). Additional analyses were done to examine this association further. Multiple regression analysis and post hoc comparison showed that the significant difference in PSE at 3 months was between mothers of infants with excessive WLZ change as compared with mothers of infants with slow WLZ change (Table 5). Mothers of infants with excessive WLZ change reported PSE approximately three points higher than that of mothers with infants who exhibited slow WLZ change (Tukey-adjusted p = .03; Table 6). The association among the other categories was not significant. PSE scores of mothers of infants with excessive WLZ change were, on average, one point higher than that of mothers with infants with expected WLZ change, and PSE scores of mothers of infants who exhibited expected WLZ change were two points higher than those of mothers who exhibited slow WLZ change.
Regression Model for PSE at 3 Months and WLZ Change (n = 127).
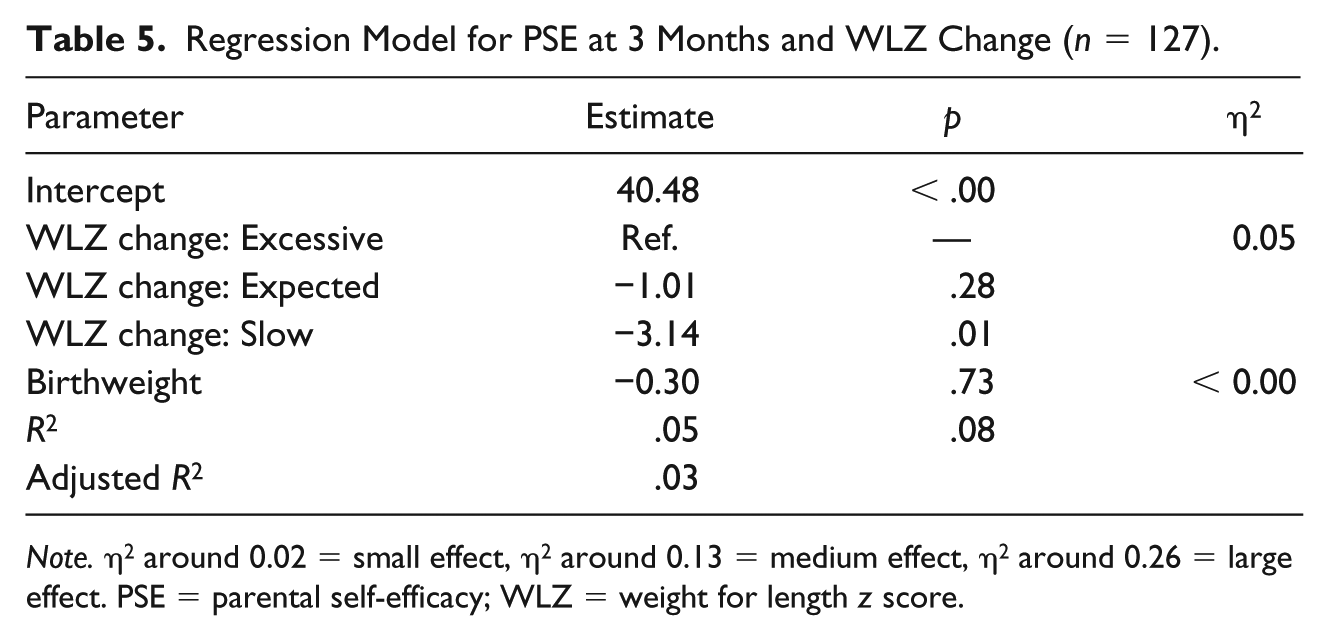
Note. η2 around 0.02 = small effect, η2 around 0.13 = medium effect, η2 around 0.26 = large effect. PSE = parental self-efficacy; WLZ = weight for length z score.
Model-Estimated Differences in Mean PSE Between WLZ Categories.
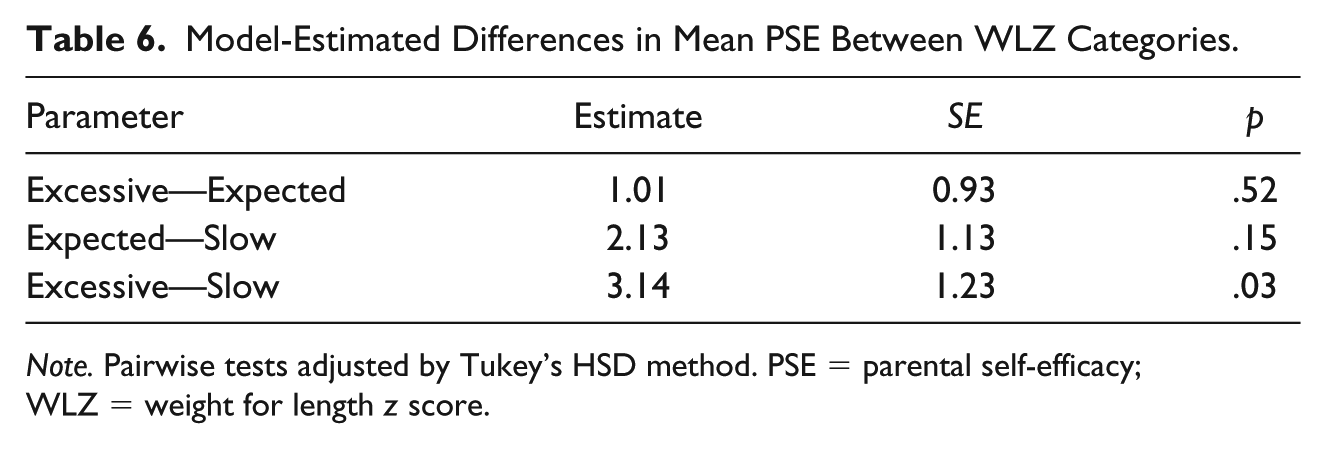
Note. Pairwise tests adjusted by Tukey’s HSD method. PSE = parental self-efficacy; WLZ = weight for length z score.
Discussion
In this sample of first-time, low-income, African American mother–infant dyads, we found a significant association between PSE and infant WLZ change from 3 to 12 months. In general, mothers who reported higher PSE at infant age of 3 months, had infants with a greater WLZ change from 3 to 12 months. Although only significant between infants whose WLZ change was classified as slow compared with those whose WLZ change was classified as excessive, the mean PSE score rose across each infant WLZ change category (Figure 1) implying a linear association between PSE and WLZ. This group difference in PSE scores remained while controlling for infant birthweight.
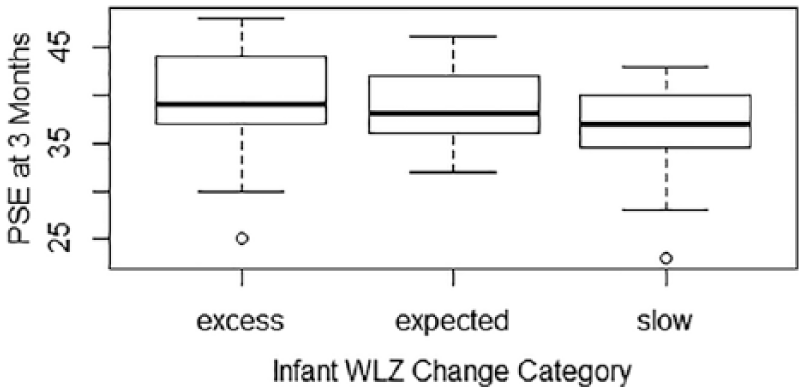
Boxplot of PSE at 3 months versus infant WLZ change categories.
To our knowledge, the current study is the first to examine the association between PSE and WLZ change. Researchers in a prior cross-sectional study reported a nonsignificant trend for PSE to be positively associated with infant BMI, but this study did not examine the association of PSE with BMI change (Stifter et al., 2011). Examining the change in infant growth across time, rather than weight status at any single time point, is important because this change is the most reliable predictor of obesity risk (Druet et al., 2012; Vogelezang et al., 2019; Woo, 2019). The association between PSE and WLZ change found in this study appears counterintuitive because high PSE was associated with a negative health outcome. This contradicts prior research that has found high PSE to be associated with positive outcomes such as successful transition to the parenting role, healthy feeding practices, and greater engagement in obesity prevention strategies, as compared with low PSE (Coleman & Karraker, 1997; Koh et al., 2014; Liyana Amin et al., 2018). Reasons for this discrepancy are unclear, however, cultural beliefs and practices of the population must be considered. Research regarding PSE in African American mothers is sparse, and beliefs regarding parenting and infant growth may vary from populations of other race or ethnicity. It is possible that the positive association between PSE and excessive WLZ change is at least partially attributable to cultural perception.
Prior research has shown that in the African American culture, a heavier infant is viewed as healthy and a sign of good parenting (McGarvey et al., 2006; Radzyminski & Callister, 2016). A qualitative study by McGarvey and colleagues (2006) reported that low-income, African American mothers expressed an attitude that “overweight or obesity in children are genetic and related to a ‘solid’ (implying healthy) physical build rather than adiposity” (McGarvey et al., 2006, p. 278). In addition, using the entire sample of the Infant Care data, low-income, African American families used the term “greedy” in a positive way to describe babies who are strong and healthy (Thompson, Adair, & Bentley, 2014). Consequently, African American mothers with high PSE may value a heavier infant and consciously, or subconsciously, engage in practices that promote an excessive infant growth. It is also possible that the significant association of PSE and excessive infant WLZ change is attributed to parents having an inaccurate perception of their infant’s growth.
Prior research suggests that mothers often have a skewed perception of their child’s weight (Hager et al., 2012; Thompson et al., 2014). In a study of predominately (70%) African American mother–toddler dyads, 94% of mothers of overweight toddlers and 60% of mothers of normal weight toddlers evaluated their toddlers as being smaller than their WLZ percentile (Hager et al., 2012). Using the entire Infant Care sample, Thompson and colleagues (2014) found that mother’s perception of infant WLZ was skewed, more so as the infant aged. Consistent with these prior studies, 33% of mothers in the current study had a perception of their infants’ weight status that was discordant with the infant’s actual weight for length percentile, however, this concordant or discordant perception was not significantly associated with WLZ change. Maternal knowledge and perception of healthy infant growth patterns in African Americans should be considered in future research as it may influence the association between PSE and WLZ change.
Prior studies have found an association between infant growth and infant feeding practices. Infants who were never breastfed, breastfed for a short duration (less than 6 months), or received complementary foods prior to 4 months of age tend to experience excessive growth (Gibbs & Forste, 2014; Li et al., 2012; Wen, Kong, Eiden, Sharma, & Xie, 2014). Feeding practices of the current sample were similar with average breastfeeding duration of 4 months and average age of complementary food introduction of 2.5 months. The results of this study failed to support previous findings as there were no significant associations between feeding practices and WLZ change. The feeding practices of this sample were homogeneous with few infants experiencing feeding practices that protect against excessive growth, this could have precluded a significant association. Future research should consider examining this association in a sample of diverse African American mother–infant dyads from all SES to determine if the association between infant feeding practices and WLZ change differs, and whether the association with PSE changes.
A strength of this study was the ability to access and use longitudinal infant weight and length data from the Infant Care data set, which provided the ability to examine WLZ change rather than WLZ at a single time point. In addition, research personnel collected data in the participants’ homes and were trained in collecting infant anthropometric measurements. This is an advantage over using data self-reported data from mothers. Although only a subset of the Infant Care sample was available for analysis in the current study due to attrition, important baseline characteristics did not significantly differ by attrition and the number of participant data available was sufficient to yield a small to medium effect of the associations examined.
This study does have limitations. The age of the data must be considered as it was collected at least 12 years prior to these analyses. However, current infant feeding practices and growth of low-income, African American infants are similar to that in the 2000s making this data set valuable for the current study (Davis, Li, Adams-Huet, & Sandon, 2018; Shinn et al., 2018). The lack of infant length at birth in the Infant Care data set precluded an assessment of WLZ change from birth to 12 months of age. Previous studies have found that catch-down or catch-up growth as a result of the uterine environment, may occur during the first few months of infancy (Taal, Vd Heijden, Steegers, Hofman, & Jaddoe, 2013; Woo, 2019), however, it is unknown in the current study whether this affected the WLZ change measured from 3 to 12 months. Similarly, PSE has been shown to increase the longer one has parented. The first measurement of PSE in the Infant Care data set was at infant age of 3 months. Without a measure prior to that time, it is unknown whether PSE changed during pregnancy, at birth, or in the postpartum period. In addition, the PSOC tool measures PSE as opposed to self-efficacy specific to feeding or infant growth. To our knowledge, a valid and reliable tool to measure self-efficacy for infant feeding or growth does not exist, such a tool may provide different results, but this cannot be examined from the Infant Care data set. Finally, it is well reported that maternal characteristics, such as gestational weight gain and gestational diabetes mellitus, have influence on infant weight gain (Hales & Barker, 2013), however, no pregnancy data were available in the Infant Care data set. These data could have contributed to infant growth, yet could not be considered in the current study.
The current study is the first to examine the association between PSE and infant WLZ change across the first year of life in a group of low-income, African American mother–infant dyads. This is an important area for study because African American infants are at risk of excessive weight gain in the first year of life, placing these infants at risk of childhood obesity (Shinn et al., 2018; Taveras et al., 2010). PSE is a modifiable risk factor that can be assessed by clinicians in clinical practice. Prior research suggests that increasing PSE has positive maternal and infant outcomes, however, findings in the current study suggests otherwise. Contributors to the development of PSE in first-time mothers warrants additional study, particularly among populations at high risk for obesity such as African Americans and those of low SES.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Association of Pediatric Nurse Practitioners, 2017 Research Foundation Grant. The Infant Care, Feeding, and Risk of Obesity study was supported by NIH/NICHD RO1 HD042219-02 (PI: Bentley).