
Abstract
People with advanced Parkinson’s disease (PD) are living at home being cared for by a family member. Decisions about health care and living preferences are made in a family context. The aims of the study were to (a) examine the types and timing of the decisions being made by dyads (person with Parkinson’s [PWP] and caregiver) in advanced PD; and (b) explore perceived decision quality relative to specific decisions made. A mixed methods design of semi-structured dyad interviews followed by individual completion of decision measures twice at six months apart was utilized. Decisions involved obtaining more services in the home, moving into assisted living communities, maintaining as is, and initiating hospice. There was high decision quality as reflected by low decisional conflict and regret without statistical differences within the dyad. The findings provide insight into the nature of decisions dyads face and suggest ways that health care providers can support decision-making.
Parkinson’s disease (PD) is a common neurologic progressive disease. It is estimated that there are approximately 1 million people in the United States living with PD and up to 10 million worldwide (Parkinson’s Disease Foundation, 2017). While the trajectory of PD is highly individualized, nonetheless, it is progressive and downhill in nature. Advanced PD refers to the time in the illness trajectory when symptoms are more disabling, more assistance with activities of daily living is required, assistive devices are needed, and living alone is not usually an option (Parkinson’s Disease Foundation, 2017). Advanced PD is generally defined as Stage 4 or 5 on the Hoehn and Yahr Disability Scale, a common tool used by clinicians (Goetz et al, 2004). The Hoehn and Yahr Scale has been widely used for decades and primarily assesses motor function, with Stage 4 being severely disabled and Stage 5 being wheelchair or bedbound unless assisted (Hoehn & Yahr, 1967). As the illness progresses into the advanced stages, the person requires more family support with activities and the increasing number of symptoms they experience (Agarwal & Fleisher, 2016; Bunting-Perry, 2006; Habermann & Shin, 2017). The rate of nursing home placement is low in advanced PD, with prevalence estimates ranging between 1% and 8% worldwide (Hoegh, Ibrahim, Chibnall, Zaidi, & Grossberg, 2013; Keranen, Martikainen, Keranen, & Marttila, 2013). Thus, the majority of care is delivered by family members (either spouses or adult children) in the home.
Importance of a Dyad Perspective in Decision-making
The literature examining PD management and illness experiences primarily have taken the perspective of either the person with Parkinson’s (PWP) or the primary caregiver. This largely remains true in the literature examining advanced stages of PD and palliative care needs, with the majority of research focusing on the primary caregiver (Boersma et al., 2017; Goy, Cater & Ganzini, 2008; McLaughlin et al., 2010). A few studies have included both PWPs and caregivers, but these studies have not required that both the PWP and caregiver participate thus the samples are not necessarily matched dyads (Fox et al., 2017; Giles & Miyasaki, 2009). More recently, the impacts of the disease duration, stage, symptoms and relationship and quality have been examined to predict caregivers’ health, depression, and strain (Carter, Stewart, Lyons, & Archbold, 2008; Lyons, Stewart, Archbold & Carter, 2009; Martinez-Martin et al., 2008; Tanji et al., 2008). While this literature begins to explore the interface between PWPs and their caregivers, it does so within the limitations of not looking at the dyad, defined as PWP and primary caregiver, equally and mutually. Given that the illness experience occurs within the context of a family, and more specifically a dyad, studies that utilize a dyadic perspective are needed. The need to study dyads has been highlighted in the literature across chronic illnesses and across the stages of illnesses (Badr & Acitelli, 2017; Menne, Tucke, Whitlach, & Feinberg, 2008; Schmid, Allen, Haley & DeCoster, 2010; Whitlatch, Judge, Zarit, & Femia, 2006). An area particularly worthy and in need of dyadic studies is in advanced chronic illnesses (Meeker, Waldrop & Schneider, 2014) and more specifically in the area of decision-making in advanced illness in elderly populations (Hanson & Winzelberg, 2013). There has been limited research involving dyads with advanced PD, especially given the amount and length of care given by the primary family member; but one study suggests that the progressive physical complications such as falls and choking influence concerns that the dyad has for the future and may influence decision-making (Habermann & Shin, 2017). No specific research studies have been identified that examine the types of decisions being made in advanced PD nor do any studies that examine satisfaction with decisions in PD dyads exist. Dyadic decision-making experiences research remains very limited, and the existing literature is a few studies involving lung cancer or cardiac implantable electronic device dyads (Fowler et al., 2018; Miller, Sullivan & Lyons, 2017)
Purpose
Guided by the Ottawa Decision Support Framework (ODSF), the purpose of this study was two-fold: (a) to examine the types and timing of the decisions being made by dyads in advanced PD; and (b) to explore perceived decision quality relative to specific decisions made. Understanding the nature including the specific types of decisions being made in dyads with advanced PD and how those decisions were perceived will provide a framework to develop interventions to support decision-making in advanced stage illness.
Conceptual Framework
Aspects of the ODSF guided the study. The ODSF is a middle-range theory that supports patients and family members to make health and health-related social decisions that aligns well with the research purpose of this study (Ottawa Hospital Research Institute, 2018). The ODSF contends that people’s decisional needs will affect decision quality, which ultimately affects actions or behavior and use of health services. Decisional needs in this framework is defined as including but not limited to decision type, timing of decisions, and dyad characteristic’s. Decision quality is operationalized as the outcomes or absence of high levels of regret and conflict. The ODSF has been used as a framework to develop decision aids that can be utilized in interventions with patients. While intervention was beyond the scope of this study, several measures that are congruent and were developed as a result of the framework were employed in this study. Specifically, the Decision Self-Efficacy Scale, the Decision Conflict Scale (DCS), and the Decisional Regret Scale (DRS) were utilized to measure decision quality. These measures will be described in the method section.
Method
The study utilized an exploratory sequential mixed methods design to incorporate the strengths of both qualitative and quantitative research (Creswell, 2009; Clark & Ivankova, 2016; NIH Office of Behavioral and Social Sciences, 2018). More specifically, the study was a qualitative-quantitative driven one, where specific decisions were explored through in-depth qualitative interviews followed by quantitative measures regarding the specific decision. Given that the study had a qualitative priority, sample size was based on reaching informational redundancy (Sandelowski, 1995). The aim related to the nature of decisions was measured through the qualitative semi-structures interviews, while the decisional quality was measured via the specified scales mentioned previously. After obtaining Institutional Review Board approval and written consent from both members of the dyad, demographic data were jointly collected from the dyad on the first occasion (time 1). Other sources of data were collected on two occasions (time 1 and time 2), approximately 6 months apart. A six-month timeframe was chosen to demonstrate if it was feasible for the advanced stage PWP still being cared for in the home without loss to institutionalization or death. Semi-structured interviews were conducted with the dyad at both time intervals while each participant completed quantitative measures independently at both time intervals. Semi-structured interviews lasted on average for 30 minutes. The interviews focused on changes or progression in symptoms, new symptoms developing, concerns about the future may bring, and a specific health care or life/social decision made in the last 6 months. The dyadic interview resulted in an identified decision made in the past 6 months. This identified decision was then utilized as the decision to complete the quantitative measures on.
Three questionnaires were administered relative to decision-making. The Decision Self-Efficacy Scale measures belief in one’s ability to make decisions, including participating in shared decision-making. The scale contains 11 items that are related to self-confidence in decision-making and are rated on a 5-point Likert scale from not at all confident (0) to very confident (4). The Cronbach’s alpha for the scale reported in the previous study was 0.92 (O’Connor, 2002). Examples of items include “Get the facts about the benefits of each choice,” “Figure out the choice that best suits me,” and “Delay my decision if I feel I need more time”. The Decisional Conflict Scale (DCS) measures uncertainty in choosing options, factors contributing to uncertainty in decision-making, and effective decision-making (expressing satisfaction with the choice). There are 16 items on the scale with a 5-point Likert scale from strongly agree (0) to strongly disagree (4). Higher scores indicate more conflict with a decision. The DCS has been widely used in more than 200 studies including recent research with dyads in cognitive impairment (Fowler et al., 2018). The stem of the introduction was individualized with the decision that the dyad had identified; thus, the responses were given in the context of the specific decision. Examples of items include “I am clear about what to choose”, “I feel I have made an informed choice”, and “I am satisfied with my decision”. The Cronbach’s alpha of the scale in the previous study was 0.78 (O’Connor, 2010). The Decisional Regret Scale (DRS) measures “distress or remorse after a [health care] decision” (Brehaut et al., 2003). It is a 5-item scale with a 5-point Likert scale from strongly agree (1) to strongly disagree (5). The stem of the introduction was individualized with the identified dyad decision. Examples of items include “It was the right decision” and “The decision was a wise one”. Higher scores indicate more regret with a decision. Cronbach’s alphas have been reported in the range of 0.81–0.92 (O’Connor, 2003).
Lower conflict and lower regret scores suggest decisions are informed and consistent with personal values. Informed decisions and decisions consistent with one’s values are indicative of decisional quality in the ODSF (Fowler et al., 2018; Ottawa Hospital Research Institute, 2018).
The qualitative arm of the study utilized a qualitative descriptive approach (Sandelowski, 2000, 2010). Qualitative description is used when descriptions of phenomena or when a summary in everyday terms is desired. The goal is to stay close to the data and not be highly interpretive (Sandelowski, 2000). Either the principal investigator or one of two research assistants that were trained in using the interview guide conducted all interviews. All interviews were transcribed verbatim by a professional transcriptionist and checked for accuracy by a research assistant. Interview coding began after a few interviews were conducted and continued through the data collection period. Prior to the second interview with the dyad at time 2, the first interview was reviewed in order to identify areas that might benefit from additional follow up. Two of the authors conducted coding of the interviews individually, and the process continued with comparisons between the two coders until consensus was reached. In qualitative descriptive designs, coders are more likely to reach consensus and agree with themes, given that the interpretation is low inference and one is staying close to the data and remaining true to the facts (Sandelowski, 2000). Member checking was used to ensure the rigor of study findings (Creswell, 2016; Sandelowski, 1986). The level of two coders’ experiences in advanced PD was different, so they reflected their roles and experiences during the period of data analysis to ensure researcher reflexivity (Creswell, 2016).
Quantitative data analyses were performed using SPSS version 24 (IBM Corp., Armonk, NY). Descriptive statistics were performed to describe sample characteristics. T-tests were utilized for analyzing differences in within and across time scores on the three decisional measures. Significance level was set for less than <0.05.
Participants
Participants were recruited from Parkinson’s support groups and other Parkinson’s-related activities in community-based settings (such as senior centers) and from one movement disorder specialty practice in the Mid-Atlantic region of the United States. In order to be eligible, participants with PD had to be on anti-Parkinson’s medications, be totally dependent on assistive devices for mobility, be able to participate in interviews, and have a family member who resided with them who was willing to participate in the study. Exclusion criteria for the dyad include either member being on prescribed memory enhancing medications, having a history of psychiatric illness, or having any known reason where they might be unable to participate for the 6-month duration of the study. Potential participants received an explanation of the study. Upon expressing a willingness to participate, they were scheduled for consent and data collection. Interviews were scheduled in either their home or a place of their choice such as a local church where the support group met. At the prearranged date and time, the study was re-explained and time was provided for questions to be answered before written informed consent was obtained from each participant.
The sample consisted or 15 dyads (N = 30) who were either married, partnered, or living together at the time of the study. Participants with PD (n = 15) were on average 75.33 years of age (range 58-89; SD = 9.81) whereas the family member was 68.87 years of age (range 33-80; SD = 11.99). Mean years together was 41.4 years (range 1-61; SD = 15.47). Of the 15 participants with PD, 11 were male, whereas 5 of the family members were male. The sample was predominately Caucasian (93.3%), with one couple being African-American. All participants had some level of college education, with the mean being slightly over 15 years. None of the participants with PD were currently employed; approximately half had retired due to disability. Two family members worked outside of the home part-time. For the participants with PD, the mean time from diagnosis was 9.73 years (range 4-23 years; SD= 4.59) and the time for dependency on assistive devices was 5.93 years (range 1-19 years; SD= 4.54). Of these participants, two (13.3%) described themselves as homebound and an additional person described herself as chair-bound which is reflective of a Stage 5 on the Hoehn & Yahr. The remaining 12 participants with Parkinson’s were Stage 4.
Results
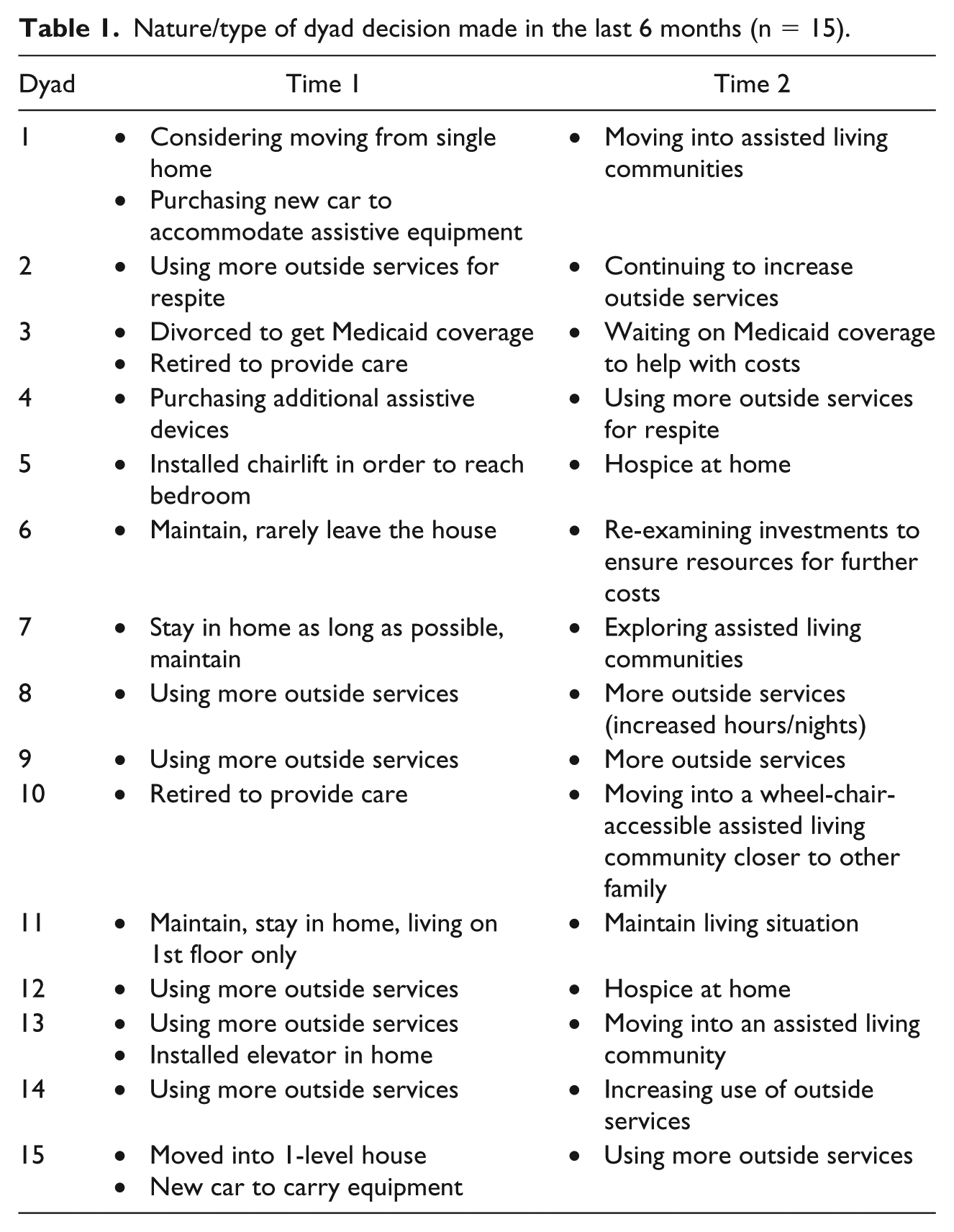
Qualitative results will be presented first followed by the statistical results. Content analysis of the qualitative data resulted in the identification of four major themes: (a) obtaining more help and services in the home, (b) moving into assisted living communities, (c) maintaining as is, and (d) initiating hospice. These themes will be described and are further illustrated in Table 1 by dyad and interview time.
Nature/type of dyad decision made in the last 6 months (n = 15).
Obtaining More Help and Services in the Home
For many participants, obtaining outside services was a way of being able to stay in their homes and ensure safety of the participants with PD. For family members, leaving the person with PD by themselves even for short periods of time was no longer an option, as they feared that they could fall or need something that they could not access. Obtaining outside services had associated costs that influenced the number of days and hours the services were received. Occasionally, other family members helped with the financial costs. As discussed by a partnered couple whose other family members lived out of state:
And the only thing that has changed drastically I guess is I’ve had to enlist the nurse much more, and that’s because his mother has come to me and said you need some time for yourself. I’ll pay for the nurse to come, and so I thought okay, well, I appreciate that. I’m using the nurse Fridays and Saturdays, like I said, and that’s pretty recent. That’s been in the last couple months. I was fearful to leave him alone for two, three, four hours at a time…. Now, it does free me up, but mind you, part of my brain is still there, so it doesn’t matter that I’m physically not there, I’m still mentally there. So it’s not a 100% reprieve.
For another married couple in their late 70s, the decision was made as the participant with PD was receiving rehabilitation after surgery at a skilled facility. As discharge became more imminent, obtaining in home help was going to be required.
Well, as far as change is concerned we have a nurse’s aide who helps us. She’s scheduled to come three times a week. For the most part, she does Tuesday, Thursday and Saturday. Those mornings from 9:00 to 12:00 are for toiletry.
And showers. I brush my teeth myself but she’s there to help me. As far as showering I’m able to sit down on a shower chair in the bathroom and take care of myself. She helps dry me. She helps get me dressed. She helps make lunch. But she’s here only three hours.
It gives me time to go out. I do the shopping, exercise, get gas, and do little errands while she’s here.
Obtaining and utilizing outside services was the most common of the themes identified across the sample.
Moving into Assisted Living Communities
Several families were undergoing living changes during the course of the study, which involved moving into an assisted living community where the continuum of care was available. Often in these families, they had previously made a living arrangement change that they had thought would be their last one. The first example demonstrates this in that the couple had retired to the area and bought the house that they thought they would remain in. Seven years later, they are relocating back to where they have additional family.
We have been indecisive about selling the house for a while. But he has continued to get weaker and weaker. We don’t use over half of the house because he can’t access it. We are paying for yard work and all of the maintenance. So we finally said it is time. We are moving into an assisted living community back close to where our son lives. He will be able to help us more and we will have the services that are needed.
Another example involved a couple who had a multi-level home. They had done extensive adaption to the home including having an elevator installed to transport him between the three levels. They shared that this was approximately a $70,000 project during the first data collection. Six months later at time 2, they had sold their house and were moving to a nearby retirement community. Their decision had been influenced by his declining health/mobility (participant with PD) and recent new health concerns for the wife.
Maintaining as Is
For some participants, staying and maintaining in the home was what they were focused on. While there usually was an acknowledgement that this might not be possible long-term, in their narratives, maintaining things as they are currently was common. For some, they had previously modified their homes or only lived in certain areas to accommodate the participant with PD. A couple that had lived together for many years that recently legally married said:
And our decision is that we’ll probably stay where we are because it’s a two-story home, but we only use the first floor and the second floor when our grandchildren visits.
We made a decision way back in the beginning and we did some things…we changed the toilets in our bathroom to a handicapped toilet; we took out the tub in one bathroom and put a shower…a walk-in shower. These were all things that we were saying that was going to have to be done and we went ahead and did them…trying to stay in the house as long as possible.
Others, while acknowledging staying in the home as their preference, also spoke about a lack of knowledge being a problem.
Well, we haven’t made any real decisions. We have talked about it. And, I guess lack of knowledge, we can’t make the decisions. And so, we’ve both would prefer to stay home as long as we can. That part, I’ll say. But as to making any decisions, we haven’t made them because we don’t know enough about what decisions to make.
Thus some participants demonstrated on both time intervals a preference to remain in the home, and yet uncertainty as to if that would be possible.
Initiating Hospice
Initiating hospice services occurred in two families during the duration of the study. Other families spoke about the possibility in the future. These conversations usually occurred in the context of moving into assisted living or retirement communities where the full continuum of care would be available. For the two families who initiated hospice, the decision was jointly made by the dyad and with additional consultation with their adult children. As explained by a wife caring for her husband, both in their late 80s:
We now have around the clock help, which I had to have because I was getting very tired. It became imperative. And then we have an aide who comes in in the morning and then somebody until 9:00 at night and then from 9:00 until 7:00. Now I have somebody from hospice, a lovely guy. Yeah, but I find it’s very often a two-person job because, for instance, we had just gotten this lift and sometimes you need two people to help with that (referring to a Hoyer lift). We have been here 38 years. This is where we are staying.
For the second couple also in their 80s:
I had the aide three mornings during the week but really could not afford more. We talked about it and felt it was time for hospice. It has been a big help with having the hospital bed.
Statistical Analysis
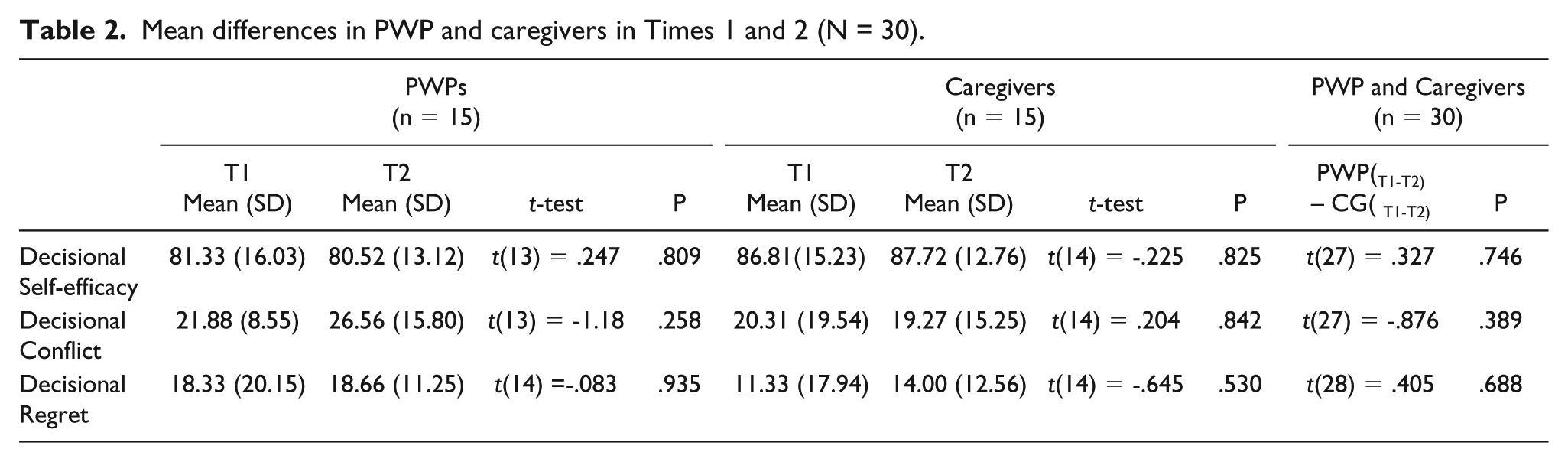
There were no significant differences in any of the three decisional scales for the PWP or the family member when comparing time 1 and 2. There were also no significant differences when comparing scores on the decisional scales between the PWP and the family member (Table 2). Overall means for the decisional regret and decisional conflict scores were low as evidenced in Table 2 (out of 100). Self-efficacy scores were in the high range (out of 100).
Mean differences in PWP and caregivers in Times 1 and 2 (N = 30).
Discussion
Findings from this mixed method study demonstrate the nature and timing of decisions dyads with advanced PD are faced with, including the more common decisions made and the perceived quality of those decisions. Dyads are making living and social arrangements due to the progressive disease they are experiencing. Many of the dyads are maintaining in their homes by increasing the outside help and services they use. This includes a variety of services and assistive/equipment devices. For some of the dyads, this strategy was being utilized at time 1 and again successfully at time 2, six months later. For others, six months later, they were making different living arrangements including selling their homes and moving into retirement or assisted living communities. The decision to make changes in living arrangements in PD has been identified in the previous literature (Habermann & Shin, 2017). In advanced stages of PD, the desire to stay in the home as long as possible, which was demonstrated in this study, has been identified previously (Habermann & Shin, 2017). In mild to moderate disease, caregivers of PWP identify future concerns regarding the housing/living situation, and whether they could care for the spouse in the advanced stages in the home (Boersma et al., 2017).
For other dyads, the desire was maintaining as is without making living changes for as long as possible. In some cases, this resulted in living in limited areas of the home due to safety and access issues. Some participants acknowledged they were not making any major decisions as they did not have the knowledge regarding what decisions needed to be made. This notion of needing more information has been noted in a previous study (Habermann & Shin, 2017).
For a few families, initiation of hospice services had been requested by the family. Other families acknowledged the need of hospice services as a potential need in the future. Interestingly, the families were requesting and initiating the process with the providers rather than the providers suggesting these services to the family.
No significant differences were found on paired t-test between the PWP and of the family member on any of the three decisional scales or within participants between time 1 and time 2. Overall, participants had very low regret and conflict scores, and the scores were lower than reported in other samples (Fowler et al., 2018). These low scores were also occurring in cases even where six months later new decisions had to be made. There are several plausible reasons for these results. This was a small sample, and while assumptions of normalcy were met, a larger sample might yield different results. The sample was also highly educated (at least some level of college), had long established relationships as a dyad (mean over 40 years), and was predominately Caucasian. Whether a sample with less education, less established relationships, or more ethnic diversity would have yielded different results cannot be determined. The majority of participants with Parkinson’s were male; however, this is consistent with the prevalence of PD being greater in males. Another explanation for no significant differences on paired t-test may be that six months is not a long enough period of time, given the highly individualized way the disease progresses. Recent announcements for funding in the areas of advanced illness management involving both patients and caregivers have recommended a minimum of a year (Patient Centered Outcome Research Institute, 2017). Participants had high self-efficacy scores, suggesting they had confidence in their decisions, and this was substantiated by the qualitative data. Overall, they were satisfied with their decisions. Perhaps they felt they were making the best decisions at any given time based on the knowledge they had.
Even though the quantitative findings showed no statistical significance, the qualitative data suggest the decisions had significant financial costs. Outside services including in home help/assistance are out of pocket expenses in the United States. These services are not affordable for everyone, as evidenced by dyad three. This couple had actually divorced so that they no longer had shared assets and he would be able to receive federal assistance (Medicaid) for health care. While divorced, they continued to live together and she continued to be his primary caregiver. Even for dyads that have the financial resources (such as money to install an elevator) in the hopes of staying in the home, having then to make a later change in living arrangements such as buying into a retirement community is very expensive.
Future research areas are two-fold. Longitudinal studies that engage dyads with advanced PD for a minimum of a year are needed to identify other potential areas of decision-making over time. Research involving the use of decisional aids that can be utilized by the dyad are needed. Development of health and social living decisional aids, which could be tailored to help the decision-making needs, plan the next steps, and facilitate shared decision-making both within the dyad and with the dyad and health care provider need to be developed and tested empirically. This work would be congruent with the ODSF that was utilized in this study.
This study advances our knowledge of what advanced Parkinson’s dyads have to manage and make decisions regarding. As such, it contributes to the advanced chronic illness literature but more specifically to our understanding of dyadic management of chronic illness in older adults. The study also suggests areas where family care in advanced PD can be optimized and thus is informative to health care providers. Decisions were being made in the context of the dyad with occasional support from other family members. Little to no discussion, education, or information sharing was being done among health care providers, PWP, and their family member. Given that primary and/or specialty providers are not addressing decision needs, this is an area that nurses, particularly, advanced practice nurses, could address. By augmenting their knowledge about expected disease progression, prognostic indicators, and the types and timing of potential decisions to be made, nurses could address a knowledge gap and support the family in their decision-making process. The most informed decisions can be made by nurses providing accurate and evidence-based information to PWP and their family member. This in the end can save time, and minimize the need to revisit decisions and the financial strain for the dyad.
This study had a sample size of 15 dyads of a person with advanced PD and their family member because informational redundancy was reached. However, a larger sample may have resulted in different statistical results. The sample was homogenous, and thus results are limited by this.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.