
Abstract
Psychometrics of the Gratitude Questionnaire-6, which measures dispositional gratitude, was originally estimated in healthy college students. The purpose of this study was to examine the scales’ factor structure, convergent/divergent validity, and reliability among 298 AA adults at risk for CVD in the community. Analyses were performed using bivariate correlations, exploratory factor analysis, and confirmatory factor analysis. The scale demonstrated acceptable estimates for internal consistency (Cronbach’s α = 0.729). Our exploratory factor analysis results yielded a one-factor structure consistent with the original instrument, and the confirmatory factor analysis model was a good fit. Convergent/divergent validity was supported by the association with positive affect (coefficient = 0.482, 95% CI = [0.379, 0.573], spiritual well-being (coefficient = 0.608, 95% CI = [0.519, 0.685], and depressive symptoms (coefficient = −0.378, 95% CI = [−0.475, −0.277]. Findings supported the scale’s reliability and convergent/divergent validity among AAs at risk for CVD.
Positive Cardiovascular Health and African Americans
Cardiovascular disease (CVD) is the leading global cause of death, resulting in more than 17.9 million deaths per year, and is anticipated to grow to more than 23.6 million deaths by 2030 (Benjamin et al., 2019). In recent efforts to reduce CVD risk, the American Heart Association encouraged a focus on CVD prevention through the promotion of positive cardiovascular health (Benjamin et al., 2019). Although significant efforts are underway to improve population-wide cardiovascular health, the burden of this chronic disease remains high in the African-American (AA) population (Carnethon et al., 2017). Negative psychological factors such as depression and stress are prevalent among AAs and may be a contributing factor to CVD (Brewer et al., 2018; Sims et al., 2017). Positive psychological attributes, such as gratitude, are associated with improved cardiovascular outcomes and spiritual well-being (Mills et al., 2015; Millstein et al., 2016; Redwine et al., 2016), suggesting that this is a way to improve AA cardiovascular health.
A growing body of theoretical research suggests that gratitude may be a driving force of successful life outcomes such as well-being that broadens and builds over time (Fredrickson, 2004; Wood et al., 2009, 2010; Wood et al., 2008a; Wood et al., 2008b). Gratitude is defined in scientific literature as (a) an emotional response to other’s kindness, (b) a mood that focuses on what is cherished in life, or (c) a trait reflecting in a broader life’s orientation toward appreciating others (McCullough et al., 2002; Wood et al., 2010). Gratitude has emerged from the Positive Psychology Movement and provided a beneficial influence on well-being across cultures (Magallares et al., 2018). Examining these relationships is critical since it is known that an increase in negative psychological factors such as depression is a risk factor for developing CVD and positive factors such as gratitude, positive affect, and spiritual well-being are associated with better cardiovascular health (Mwendwa et al., 2013; Yaghoobzadeh et al., 2018). However, nothing is known about the relationships among positive and negative psychological factors such as gratitude, depression, positive affect, and spiritual well-being in AA adults. Efforts to increase gratitude, positive affect, and spiritual well-being may be of potential clinical value in preventing CVD in AA. Therefore, it is imperative to understand the interactions and impacts of these factors in AA at risk for CVD. However, a current limitation is the lack of a valid and reliable instrument to measure gratitude in AA.
The most widely used instrument to measure gratitude is the Gratitude Questionnaire-6 (GQ-6), comprised of six items (McCullough et al., 2002). The GQ-6 is a self-report questionnaire that is designed to assess people’s dispositional gratitude in everyday life (McCullough et al., 2002). The GQ-6 measures four domains of dispositional gratitude: (a) intensity, (b) frequency, (c) span, and (d) density (McCullough et al., 2002). The original psychometric analysis of the GQ-6 was conducted in two samples (n = 238 and n = 156) of undergraduate psychology students and (n = 1,228) adult volunteers and reported adequate construct validity and reliability (McCullough et al., 2002). Since the original psychometric study, the GQ-6 has been tested in different samples across the world including Chinese, Taiwanese, Filipino, Dutch, Chilean, and Spain (Chen et al., 2009; Froh et al., 2011; Jans-Beken et al., 2015; Kong et al., 2017; Langer et al., 2016; Magallares et al., 2018; Valdez et al., 2017; Zeng et al., 2017). However, no psychometric analysis has been conducted in a sample of participants of African descent. This study will be the first psychometric analysis in AA; to our knowledge, it will provide evidence for the validity and reliability OF GQ-6 in AA.
Purpose
Thus, the purpose of this study was to examine the scales’ factor structure, convergent/divergent validity, and reliability among 298 AA adults at risk for CVD in the community. Psychometric analysis of the GQ-6 in an AA sample will help determine whether this instrument measures gratitude similarly to other populations. The three aims are to (a) test the construct validity of the GQ-6 using exploratory factor analysis and confirmatory factor analysis, (b) examine convergent and divergent validity by assessing the relationship between GQ-6 and depressive symptoms, positive affect, and spiritual well-being (Kroenke et al., 2001; McCullough et al., 2002; Peterman et al.. 2002; Watson et al., 1988), and (c) assess the reliability of the GQ-6 using Cronbach’s coefficient.
From previous testing by McCullough et al. (2002), we hypothesized that (a) factor analysis would confirm the six items would reflect the latent variable, gratitude, (b) GQ-6 scores would be negatively correlated with depressive symptoms, positively correlated with positive affect and spiritual well-being, and (c) GQ-6 scores would demonstrate reliability (internal consistency) using Cronbach’s alpha.
Methods
Design and Sample
This cross-sectional study collected data via online and physical surveys. Participants were recruited between June and July of 2019, via three strategies: (a) social media platforms—Facebook, Twitter, LinkedIn, and Instagram, (b) distributing flyers to churches, hair salons, and barbershops in the southeastern United States, and (c) in person at the Florida Department of Health of Pinellas County and the Pinellas County Urban League. Inclusion criteria were: (a) adult age 18 years or older, (b) self-report as Black or AA, and (c) self-report with one of the following CVD risk factors: hypertension, hyperlipidemia, diabetes and prediabetes, smoking, overweight, or having a family history of early heart disease (50 years of age or less). Individuals were excluded from the study who met the following criteria: (a) not able to read or understand the material, (b) impaired vision, and (c) not able to speak English. The final sample consisted of 298 community-dwelling AA at risk for heart disease.
The study entitled The Grateful Heart and Soul was approved by a University Institutional Review Board (IRB #Pro00040664), which provided informed consent to participate in this non-intervention study. Participants completed demographic survey (age, gender, risk factor for CVD, race, education, religious affiliation, income, and primary care provider visit within 12 months) and then completed the GQ-6 (gratitude), Patient Health Questionnaire (PHQ-9; depression), Positive and Negative Affect Scale (PANAS; positive affect), and FACIT-Sp (Functional Assessment of Chronic Illness Therapy–Spiritual Well-being) questionnaires. Participants took an average of 13 minutes to complete the entire set of questionnaires, and 86% completed the survey online.
Measures
The Gratitude Questionnaire-6
The GQ-6, a well-validated, self-administered six-item scale is designed to measure dispositional (trait) gratitude (Froh et al., 2011; McCullough et al., 2002). The concept measured by the GQ-6 reflects four facets of dispositional gratitude: (a) intensity, (b) frequency, (c) span, and (d) density (McCullough et al., 2002). Each item is rated on a seven-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). Items three and six on the GQ-6 are reversed scored to reflect negatively worded items. Scores range from 6 to 42, with higher scores implying a greater level of dispositional gratitude and lower scores indicating a decreased disposition in gratitude (McCullough et al., 2002). The internal consistency of the GQ-6 in our sample was moderate, with a Cronbach’s α of 0.729.
The Patient Health Questionnaire-9
The PHQ-9 is a nine-item self-report instrument for determining criteria-based diagnoses of depressive symptoms over the past two weeks (Kroenke et al., 2001). The PHQ-9 scores each of the nine Diagnostic and Statistical Manual of Mental Disorders-IV as “0” (not at all) to “3” (nearly every day), and total scores range from zero to 27 (Kroenke et al., 2001). A major depressive episode is diagnosed using a diagnostic algorithm or a summary score (Kroenke et al., 2001). In our study, we utilized the summary score method. Any participants scoring positively for depressive symptoms (score 5 or higher) were encouraged to contact their primary care provider or licensed mental health provider. The PHQ-9 demonstrates high reliability and structural validity (Du et al., 2017). In our sample, the coefficient α was strong with α at 0.884.
The Positive and Negative Affect Scale
PANAS is a 20-item Likert scale that contains two mood scales, one that measures positive affect and the other that measures negative affect and are shown to be highly internally consistent and stable (Watson et al., 1988). We utilized the 10-item positive affect scale in this study. Positive affect scores range from 10 to 50, with higher scores representing higher levels of positive affect (Watson et al., 1988). The internal consistency of the PANAS (positive affect) score in our sample was strong, with α of 0.933.
The FACIT-Sp Modified for Non-Illness: Functional Assessment of Chronic Illness Therapy
A version of the FACIT-sp modified for non-illness (FACIT-sp12) is a 12-item scale designed to assess spiritual well-being in a population without chronic illness (Peterman et al., 2002). The FACIT-sp12 measures spiritual well-being experienced over the past seven days (0 = not at all to 4 = very much; Peterman et al., 2002). Scores range from 0 to 48; higher scores demonstrate an increase in spiritual well-being. Internal consistency reliability coefficient ranged from 0.81 to 0.88, and convergent validity estimates show moderate to strong correlations with other measures of spirituality and religiousness (Peterman et al., 2002). In this cohort, the coefficient α for FACIT-Sp was 0.928.
Demographic survey
The following items were used to provide descriptive data for the study: age, gender, heart disease risk factors, race, education, religious affiliation, income, primary care provider visits within the past 12 months.
Data Analysis
Descriptive statistics, frequencies, means with standard deviations were used to characterize the participants and scores of the questionnaires. Except for the exploratory factor analysis, all procedures replicated McCullough et al. (2002) original psychometric analysis to allow for a close comparison of the outcomes.
Construct validity (Aim 1)
From the original sample of 298 cases, the dataset was randomly divided into two separate and independent sub-samples using SPSS (Version 26). The first exploratory sample contained 149 cases for the exploratory factor analysis. The second, confirmatory sample of 149 was used as an independent, validation sample for the confirmatory factor analysis. A sample size of 84 was based on 80% power to detect a correlation of 0.30 using a two-sided hypothesis test at alpha = 0.05 and Pearson’s correlation test (Graybill, 1961; Guenther, 1977; Zar, 1984). While this procedure resulted in two smaller samples, it was essential to analyze the data using both exploratory factor analysis and confirmatory factor analysis with this sample of AA participants as the structure of the GQ-6 had not been previously established in AA. These sample sizes are similar to recent psychometric testing of the GQ-6 in Filipino participants (Valdez et al., 2017). In addition, it surpasses the recommended 4:1 ratio of subjects to items (MacCallum et al., 2001). In both our exploratory factor analysis and confirmatory factor analysis samples, the subject to item ratios were 25:1.
For the exploratory factor analysis, sampling adequacy was determined by a Kaiser–Meyer–Olkin (KMO; Field, 2018). Bartlett’s test of sphericity determined that the item-to-item correlations supported factor analysis (Field, 2018). Principal components analysis with a direct oblimin rotation was used in the exploratory factor analysis. Three decision rules guided the number of factors to retain: (a) Kaiser’s criterion (eigenvalues above 1), (b) analysis of the scree plot, and (c) the use of Horn’s parallel analysis (Horn, 1965).
Exploratory factor analysis was followed by confirmatory factor analysis using maximum likelihood estimation in the second validation sample (n = 149) using AMOS version 26 (Arbuckle, 2019). The multivariate normality was verified through Mardia’s coefficient. Bootstrapping using the Bollen-Stine procedure was utilized to handle non-parametric data (Byrne, 2001). Similar to the initial validation by McCullough et al. (2002), we examined chi-square, comparative fit index (CFI), and standardized root-mean-square residual (SRMR) fit statistics (Bentler, 1995).
Convergent and divergent validity (Aim 2)
In our second aim, correlation analyses were performed to test for convergent and divergent validity. Spearman’s rho was utilized to minimize the effects of violations of assumptions (positively skewed data), and confidence intervals were derived empirically using a bootstrapping procedure (Field, 2018). A priori α level of greater or equal to 0.05 was used to determine significance.
Reliability (Aim 3)
For the third aim, Cronbach’s α was calculated for the GQ-6 for the entire sample of 298 participants. Corrected item-total correlations were analyzed to ensure all correlation coefficients were between 0.3 and 0.9 (Field, 2018).
Results
Descriptive Statistics
Participants (n = 298) were primarily female (68.8%) and aged 43 ± 14 years. A majority of the sample self-reported either being overweight (44.6%) or having high blood pressure (23.2%). The sample was relatively well educated, with over half of the sample reporting that they had graduated from college (21.8%) or had a graduate degree (37.6%). A majority of the sample were Christian (82.9%) and visited their primary care provider within 12 months (82.6%).
Total GQ-6 scores were moderately high, with an average score of 37 ± 5. Average depression severity scores from the PHQ-9 was 6 ± 6, which is classified as mild depressive symptoms. Positive affect (PANAS) and spiritual well-being (FACIT-Sp12) were also moderately high, with an average score of 36 ± 9 and 37 ± 10, respectively.
Construct Validity (Aim 1)
Exploratory factor analysis
Bartlett’s Test of and the KMO supported the factorability of the matrix. The principal components analysis resulted in a one-factor solution, explaining 47.42% of the variance. The results of saturation weights are listed in Table 1. The extraction of the one-factor solution in this sample replicated the original instrument and provided evidence of a one-factor structure of the GQ-6 in AA at risk for CVD.
Exploratory Factor Analysis of the One-factor Solution by Principal Components Analysis (n = 149).
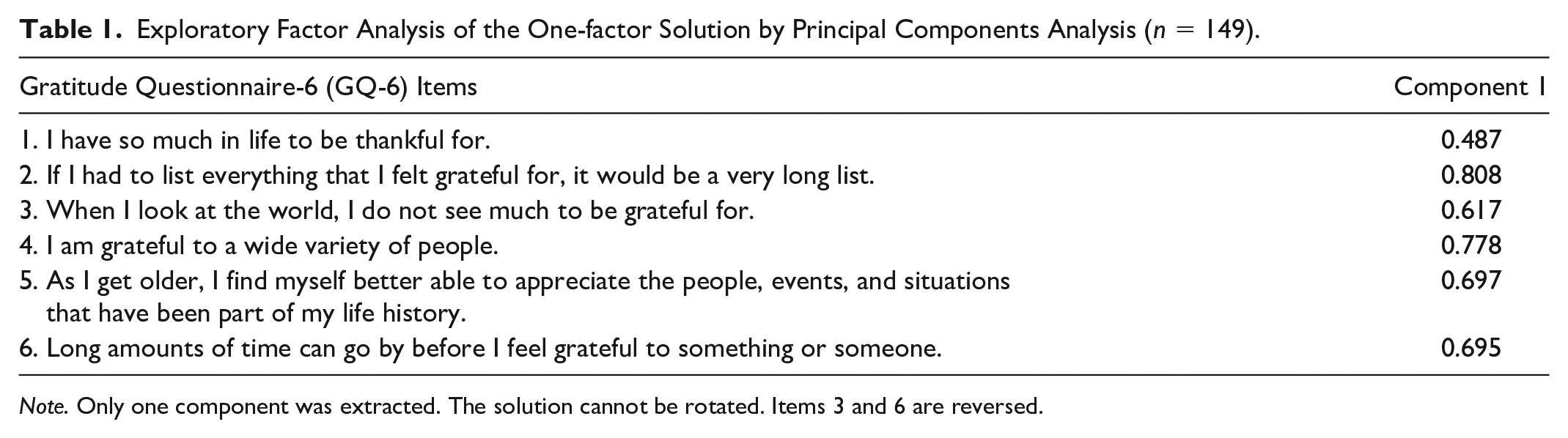
Note. Only one component was extracted. The solution cannot be rotated. Items 3 and 6 are reversed.
Confirmatory factor analysis
After the exploratory factor analysis, a confirmatory factor analysis using maximum likelihood estimation was conducted on the second sample (n = 149). Bollen–Stine’s bootstrapping procedure was used due to skewing, and the model fit was improved with 191 samples (Bollen–Stine bootstrap p = 0.05). Fit statistics were chi-square, χ2 (8, n = 149) = 18.16, p = 0.02. The CFI, 0.94, and the SRMR were 0.06 with error terms of items three and six correlated (reversed items of ingratitude) indicating that the one-factor model is a reasonable fit to the data (Figure 1).
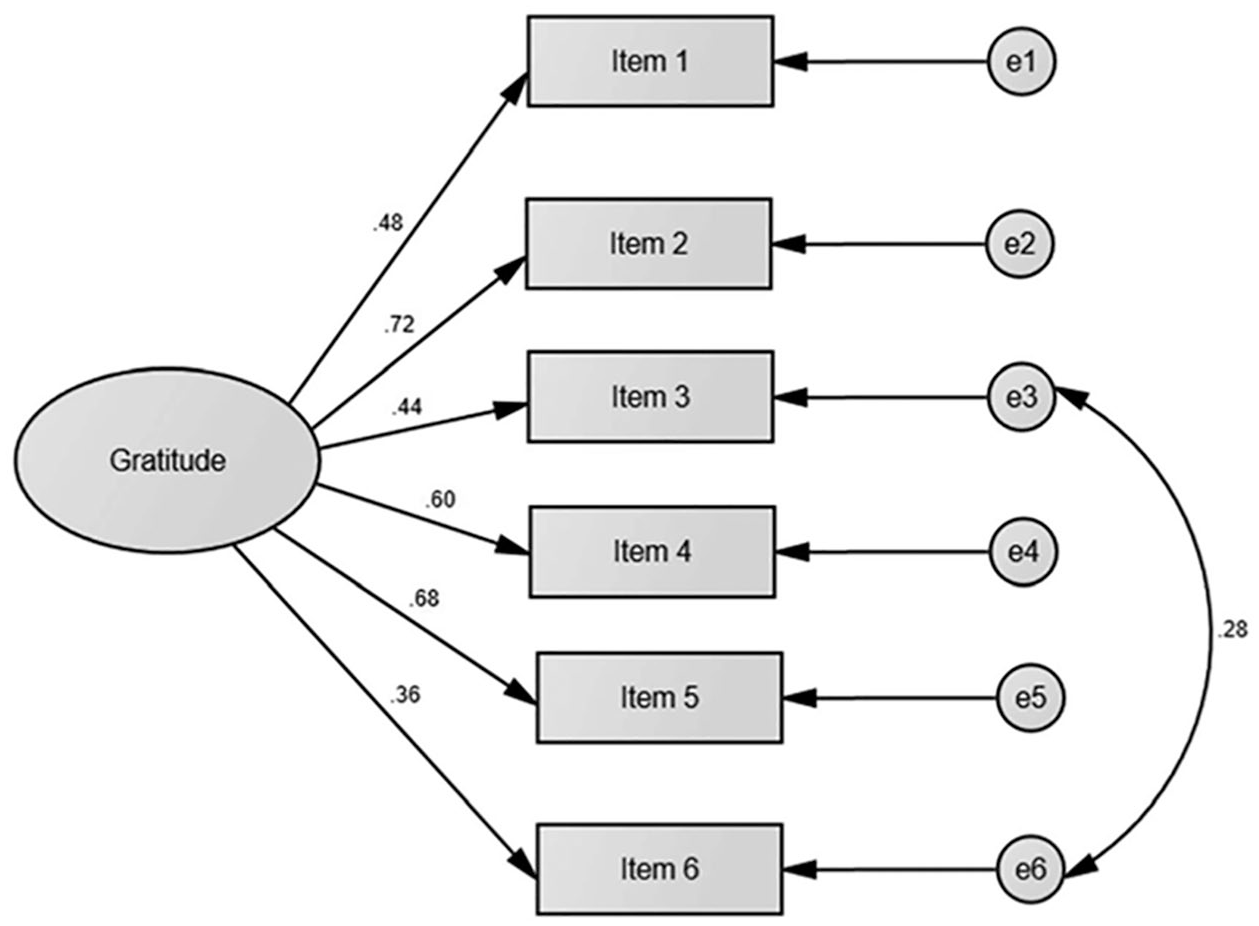
First Order CFA Model of the Gratitude Questionnaire-6. Standardized estimations of the model.
Convergent and Divergent Validity (Aim 2)
The relationship between the GQ-6 with the PHQ-9 (depressive symptoms), PANAS (positive affect), and FACIT-Sp12 (spiritual well-being) scores were examined using Spearman’s rho for the total sample (N = 298). GQ-6 scores were significantly correlated with the PHQ-9, PANAS, and FACIT-Sp (see Table 2) and in the expected directions supporting convergent and divergent validity.
Correlations Between the Gratitude Questionnaire-6 (GQ-6) and Other Constructs (N = 298).
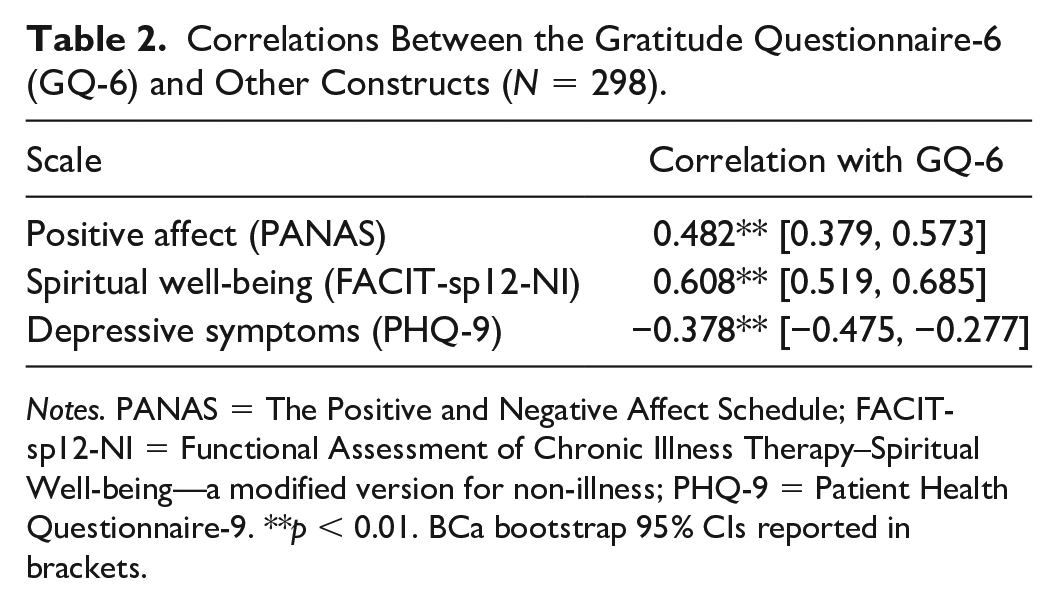
Notes. PANAS = The Positive and Negative Affect Schedule; FACIT-sp12-NI = Functional Assessment of Chronic Illness Therapy–Spiritual Well-being—a modified version for non-illness; PHQ-9 = Patient Health Questionnaire-9. **p < 0.01. BCa bootstrap 95% CIs reported in brackets.
Reliability (Aim 3)
The Cronbach α value for the GQ-6 was 0.729. Analysis of the item-total correlations ranged from 0.319 to 0.595, and the removal of any individual item of the GQ-6 did not improve the overall reliability of the scale. Once again, this was similar to the previous analysis of the GQ-6.
Discussion
The goal of this study was to psychometrically assess the GQ-6 in a sample of AA at risk for CVD and provide evidence for its validity and reliability in this population. As far as we know, this is the first study to analyze the psychometric properties of the GQ-6 in AA. Psychometric studies such as this one are needed to increase confidence that questionnaires such as the GQ-6 to measure gratitude in diverse groups. In the following section, we will discuss our findings in light of previous findings and suggest the next steps.
Results from the exploratory factor analysis yielded a one-factor structure consistent with the factor structure of the original scale from McCullough et al. (2002) and other psychometric studies in different countries (Jans-Beken et al., 2015; Kong et al., 2017; Magallares et al., 2018). However, the mean score on the GQ-6 in our sample was higher (ours versus theirs) than reported samples in the original study (McCullough et al., 2002). This is not unexpected, given the correlations between spirituality and gratitude was similar in the original sample, and our participants were 83% Christian.
When testing the construct validity of the GQ-6, the six-item, one-factor confirmatory factor analysis indicated that the model was a good fit when error terms for items three (“when I look at the world, I do not see much to be grateful for”) and six (“long amounts of time can go by before I feel grateful to something or someone”) were allowed to correlate. Correlated errors may arise from items that are very similarly worded or reverse-worded (Brown, 2015). In our sample, the correlated errors were the result of reversed-worded items. Previous studies of the GQ-6 in China and Spain also encountered similar correlated errors. However, their errors were due to similarly worded item content (Kong et al., 2017; Magallares et al., 2018). In these samples, the error terms of items four (“I am grateful to a wide variety of people”) and five (“as I get older, I find myself better able to appreciate the people, events, and situations that have been part of my life history”) correlated. These findings suggest that it may be necessary to evaluate the psychometric properties of the GQ-6 when using it in a diverse sample before conducting any analyses.
Correlations of the GQ-6 and several related constructs (depressive symptoms, positive affect, and spiritual well-being) were examined for evidence of convergent and divergent validity in our sample. As expected from previous studies, we found that gratitude is positively correlated with positive affect and spiritual well-being and negatively correlated with depressive symptoms in this sample of AAs (Chen et al., 2009; Jans-Beken et al., 2015; Langer et al., 2016; Magallares et al., 2018). These findings also support theoretical predictions by Wood et al. (2010), who hypothesized that dispositional gratitude has the potential to improve overall well-being and foster positive feelings. In our sample of predominantly Christian obese AA women with high blood pressure, spiritual well-being was significantly correlated with gratitude. Recent studies found that faithfulness to spiritual practices (i.e., gratefulness to God) in AA women who are obese with high blood pressure results in greater adherence to hypertension medication regimens and reductions in other CVD risk factors (diet and exercise; Abel & Greer, 2017; DeHaven et al., 2011). Furthermore, faith-based practices and gratefulness to God among community-dwelling hypertensive AAs are associated with normative beliefs—such as believing that God approved of their medication adherence (Lewis et al., 2010). This suggests future interventional opportunities using a gratitude intervention to increase spiritual well-being as a mechanism to improve self-care.
Our results support the GQ-6 is reliable in AAs with Cronbach’s α of 0.729. In our sample, the GQ-6 presented similar reliability to other validation studies, which reported Cronbach’s alphas between 0.70 and 0.80 (Chen et al., 2009; Langer et al., 2016; Magallares et al., 2018; Zeng et al., 2017). Taken together with the construct, convergent, and divergent validity evidence present here, this suggests that the GQ-6 is reliably measuring the latent construct, gratitude, in AAs.
One final finding needs further discussion. As detailed in our introduction, depression is a significant contributing risk factor of CVD in AAs (Brewer et al., 2018; Sims et al., 2017). In our sample, participants reported mild depressive symptoms (mean PHQ-9 score 6). Over time, depressive symptoms can negatively impact the cardiovascular system (Mwendwa et al., 2013). Dispositional depression and hostility are associated with inflammatory markers of CVD in AAs (Mwendwa et al., 2013). However, increasing gratitude is a potential means of non-pharmacologically mitigating depressive symptoms. Dispositional gratitude fosters protective factors against depression and serves as a psychological resource in decreasing CVD-related health risk from socioeconomic stressors (Hartanto et al., 2019; Wood et al., 2008b). Lastly, the results from this study suggest that further interdisciplinary research in gratitude is needed to better understand its contribution to the improvement of overall cardiovascular health in minority populations.
The limitations of this study include a convenience sample which may lead to a selective sampling, and the GQ-6 is a self-reported instrument that may introduce social desirability bias in the data. We attempted to mitigate these by first, recruiting in diverse areas instead of one location, including the Pinellas County Urban League, Florida Department of Health in Pinellas County, community centers, community events, churches throughout Florida for a heterogeneous sample of gender, age, education, employment status, and religious affiliation, and secondly by collecting the majority of the data from an anonymous online portal.
Overall, the adaptation of the GQ-6 in AA at risk for CVD showed excellent psychometric properties, similar to the original study and prior studies in other countries. The GQ-6 was determined to be a reliable and valid measure of dispositional gratitude. More importantly, this instrument can be used in clinical trials that seek to reduce depressive symptoms, improve positive affect, spiritual well-being, and reduce depressive symptoms that can impact CVD risk factors in AA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.