
Abstract
Members of marginalized communities experience health disparities or inequities and are underrepresented in health research. Community engagement in research is a catalyst for researchers to address health disparities while prioritizing community needs and strengthening community capacity. There is limited knowledge on how to engage underrepresented communities throughout the research process, particularly on initiating a partnership and planning research with a community. The purpose of this reflection piece is to share individual cases of research engagement within four communities: immigrant postpartum women, rural residents engaged in farming, low literate and non-English speaking adults, and individuals with intellectual disabilities in the United States. In each case, we explain how we initiated partnerships with the communities, continued to integrate community feedback to guide research questions, and implemented tailored methodologies. Finally, we discuss commonalities and differences in approaches used, tailoring within, and lessons learned when working with these diverse, underrepresented communities during the research process.
Keywords
Members of marginalized communities who experience health disparities or inequities are underrepresented in health research. Examples of these communities include immigrants, residents of geographically remote areas, subgroups of racial and ethnic minorities, and people with disabilities (Shaghaghi et al., 2011). A number of contextual factors, including social (e.g., being on dependent visa), cultural (e.g., valuing independence and self-sufficiency), geographic (e.g., residing in a rural area), linguistic (e.g., being non-English speaking), or cognitive (e.g., having intellectual disabilities [IDs]) contribute to their underrepresentation in health research. These communities are often excluded in health research due to challenges with research access, recruitment, and retention (Semaan, 2010; Sydor, 2013). Without the inclusion of underrepresented communities in health research, the health disparities experienced by these communities are likely to persist. Therefore, investigators must implement socially, culturally, and contextually appropriate strategies to engage these communities in the research process.
Community engagement in research is a catalyst for researchers to address health disparities while prioritizing community needs and strengthening community capacity (Ahmed & Palermo, 2010; Boutin-Foster et al., 2008; Gebbie et al., 2003). According to the Patient Centered Outcomes Research Institute (2018), to engage communities means to recognize community members as “equitable partners—as opposed to research subjects” and to involve them “from planning the study, to conducting the study, and disseminating study results.” However, a substantial amount of research has documented known barriers for researchers and participants that contribute to the poor research participation of communities. Participant barriers have included distrust of the research community (Corbie-Smith et al., 2002; Yancey et al., 2006), lack of knowledge or awareness of health research (UyBico et al., 2007), concerns over confidentiality and privacy (Levkoff & Sanchez, 2003), fear that participation in research study could result in loss of health services (Levkoff & Sanchez, 2003), and ineffective informed consent process (Flory & Emanuel, 2004; Killien et al., 2000). Researcher barriers have included difficulty locating potential participants (Moorman et al., 1999; Nápoles-Springer et al., 2005), personal biases (Ejiogu et al., 2011; Shavers-Hornaday et al., 1997), and cultural differences between researchers and participants (Corbie-Smith et al., 2002; Killien et al., 2000).
To facilitate the involvement of underrepresented communities in health research, a growing body of literature has provided strategies to maximize recruitment, sampling, and retention (Bonevski et al., 2014; Ellard-Gray et al., 2015; Shaghaghi et al., 2011). These strategies include establishing community advisory boards, which inform effective research approaches such as participant recruitment strategies (Corbie-Smith et al., 2004), and offering transportation and childcare support, which reduce resource-related barriers to research participation (Ellard-Gray et al., 2015). Furthermore, to advance translational research and improve health outcomes, particularly among communities experiencing health disparities, Michener et al. (2012) have advocated for the need to build a pipeline of community engagement researchers, starting from pre-college students to doctoral students, residents, and postdoctoral fellows.
The implementation of existing strategies to engage underrepresented communities in research, such as using community advisory boards or providing transportation and childcare support, often requires researchers to possess extensive financial (e.g., multiple funding mechanisms) and human (e.g., multiple research assistants) resources, as well as pre-existing social capital (e.g., organizational support and established relationships with community stakeholders; see examples in Centers for Disease Control and Prevention, 2011). These prerequisites may pose substantial barriers for novice researchers or for those without prior relationships with communities of interest. Therefore, accessible (i.e., ready-to-use), community-specific strategies must be developed to support researchers who are interested in engaging in research with underrepresented communities. In addition, a critical aspect of community engagement research is planning the research with community partners, prior to writing a grant or defining the research agenda (Michener et al., 2012). To plan research with the community, researchers must first initiate and establish partnerships with the community. However, the literature has offered researchers limited practical guidance for initiating and building partnerships with underrepresented communities and for incorporating community members as experts to identify community assets, needs, and priorities.
The purpose of this reflection piece is to provide practical examples and accessible strategies used in research studies conducted within four underrepresented communities, including immigrant postpartum women, rural residents engaged in farming, low literate and non-English speaking adults, and individuals with an ID in the United States. In the following section, we present four research study cases. In each individual case, we present an account of the engagement process from the perspective of the investigators who undertook the community engagement. For each of the four cases presented, research activities were vetted with and received approval from the investigators’ University Institutional Review Board prior to formative data collection with each community.
Individual Cases
Engaging Immigrant Postpartum Women
Context
In 2017, 23% of all births in the United States were to immigrant women (Pew Research Center, 2019), many of whom are socially isolated and rarely represented in health research (Falah-Hassani et al., 2015). Immigrant women in the present study are spouses of international students or workers and often hold dependent visas that restrict their working capacity. For several reasons, many of these women are left homebound after giving birth. For example, visa-based work restrictions substantially reduce their social interactions. Moreover, language barriers, cultural differences, transportation limitations, and overwhelming uncertainties may cause immigrant mothers to stay close to the same-ethnic community as a survival strategy (Cho et al., 2005). Although this strategy allows immigrant mothers to receive material or informational support from their community, it distances immigrant mothers from the broader society. Finally, in cases when professional childcare is unaffordable and family support is unavailable, immigrant mothers are stranded at home due to intensive childcare demands.
Strategies
Although I share similar cultural and linguistic backgrounds with participants in my study, I had no prior relationships with the local immigrant mother community. Therefore, my engagement started with building relationships with the community through the help of a gatekeeper, over the course of six months. This gatekeeper, a nurse researcher colleague who facilitated my entry into the community, was an active and respected community member. To establish an initial connection, the gatekeeper and I visited five Chinese immigrant mothers at their homes and temporarily helped with childcare. During the visits, I presented myself as someone who shared a similar cultural and immigrant background. To position mothers as experts in their own lives, I stated the purpose of my visit as learning from someone experienced with being an immigrant mother in the United States. Over the initial visits, mothers provided me access to multiple online Chinese mother groups on the messaging application WeChat. The mothers used the groups to exchange parenting strategies and share interpersonal relationship struggles. Access to these online groups allowed me to assess the dynamics and needs of this community. In these online groups, mothers were very supportive of and responsive to each other, though they sometimes shared inaccurate health information or advice that could be harmful. In response to this observation, I proposed to write weekly blogs about the groups’ common concerns on maternal-child health and to share these blogs via the WeChat mother groups. The proposal was well received by the mothers, and they provided me with many topics for future blogs, including postpartum depression. While serving and interacting with the community, I came to realize that postpartum distress among immigrant mothers emerged as a significant unmet need but was rarely addressed in the literature. Before constructing research plans and applying for funding, I directly asked mothers whether postpartum distress was something they would like me to study and received strong support. One mother exclaimed, “Finally someone is paying attention to this [postpartum distress], this is very important, and I fully support it!” I had no difficulties with recruitment, and some mothers volunteered to distribute my study flyers in their online groups. Given the sensitive topic and the fact that these mothers had few opportunities to share their experiences, I used qualitative interviews to collect data. Many participants appreciated the interviews and found them to be supportive. One participant shared, “You are actually the first one to hear these things in such details. . .. Like I said before, why many moms probably like tell you things —it’s a reflection.”
Engaging Rural Farming Residents
Context
At the start of the 20th century, 41% of the US workforce was employed in production agriculture (farming), while today that number is less than 2% (Dimitri et al., 2005; United States Department of Agriculture, 2019). This reduction in agricultural employment occurred in response to economic changes, mechanization, and technological advances in farming (Dimitri et al., 2005; National Public Radio, Robert Wood Johnson Foundation, Harvard T. H. Chan School of Public Health, 2019), leaving farmers hidden to researchers, policy-makers, and health advocates. Farmers often live in sparsely populated, geographically remote communities (Ryan et al., 2019) that lack reliable broadband or cellular service (Humphreys, 2019). Moreover, they usually work alone for long, variable hours (Aplass et al., 2004; Ryan et al., 2019). Cultural traits associated with farming, such as independence, privacy, and self-sufficiency, also limit farmers’ willingness to engage with others, including researchers (Fuller et al., 2009).
Strategies
I am a fourth-generation farmer who grew up in the midwestern United States. Since I no longer work or live on a farm, my ability to engage farmers in research relies on building relationships in local farming communities, starting with community gatekeepers. Many farmers belong to their local Farm Bureau, a county-level advocacy group that promotes policies to support agriculture and farming (American Farm Bureau Federation, 2020). As such, the president of the Farm Bureau is a potential community gatekeeper. I initiated a connection with this gatekeeper by emailing the president of the Farm Bureau for my county of interest and introducing myself as a registered nurse who grew up on a farm. The president provided me an opportunity to establish further connections with the farming community at the next Farm Bureau meeting.
I used multiple strategies to build credibility and trust with the farming community over a nine-month period. To connect with them, I introduced myself as fourth-generation farmer who has ties to the local community and understands what it is like to be a farmer. I acknowledged that my background gave me insight into rural and farming life, although I also showed my respect for farming culture, expressing that I was no longer an expert and that I needed to learn from them. To demonstrate my commitment to serve the community, I shared my interest in supporting farmer’s attainment of health and well-being and asked what issues they felt were the greatest priorities in their community. I also began visiting the community on a monthly basis, at minimum, to establish a regular and visible presence. During these visits, I shopped at local businesses and drove around the county. This process allowed me to stay current on local issues and the community to become familiar with my vehicle. I was invited to present farmer health information at the annual Farm Bureau district meeting, which included members from a seven-county region. These efforts facilitated relationship building, as farmers began sharing stories about their struggles in farming, particularly those associated with economic uncertainties and fear of losing their farms. One member stated, “We need you here, now more than ever.” After the annual meeting, I was invited to write a monthly column about farmer health in the Farm Bureau newsletter. I was also asked to host an informal women’s group every three to four months in their local community. This group has become a source of information and resources for health and well-being and allows the women to feel connected and less isolated.
Engaging Low Literate and Non-English-speaking Adults
Context
The Hmong are an underrepresented Asian subpopulation in research because of their inability to read and write in English or Hmong. The Hmong are refugees originally from Southeast Asia, and their relocation to the United States was a result of their involvement in the Vietnam War. More specifically, they were recruited by the Central Intelligence Agency to fight communists in Laos during the Vietnam War (Hamilton-Merritt, 1993). The Hmong traditionally have an oral culture. Although Christian missionaries developed a Romanized Alphabet (RA) writing system in the 1950s, most Hmong do not know how to write and read in this system (Duffy, 2007). Of the Hmong population in the United States, 42% have limited English proficiency, which is defined as communicating in English “less than well.” Approximately 260,000 Hmong live in the United States, with the highest concentrations in California, Minnesota, and Wisconsin (Pfeifer et al., 2012). Consequently, the Hmong, even those willing to participate in research, are excluded because most research requires the ability to read and write in English or in their native language.
Strategies
Although I was raised in the Hmong community in the United States, my Hmong background does not guarantee access to the Hmong community as a researcher. Acknowledging that my position as a researcher may elicit some discomfort or distrust, I volunteered at two community centers that serve a large Hmong population as the first step to building trust. This volunteer service began before any development and implementation of research, and it continued for two years. On a weekly basis, I tutored in a middle- and high-school after school program. On a monthly basis, I volunteered for a senior program held in the evening. During this volunteering, community members disclosed detailed personal information to me, indicating that they trusted me and acknowledged my commitment to helping Hmong community members. When members of the community center learned that I was a nurse, I received frequent requests for health information and resources outside my usual volunteer activities. These volunteer opportunities also allowed me to learn about the vulnerabilities (e.g., being poor or having language barriers resulting in lack of access to health care) of the Hmong community, thus providing insight into how the research process can be tailored to address cultural and linguistic needs. For example, rather than providing a written informed consent document to Hmong members, I developed oral consent that incorporated members’ inputs, including usage of language and presentation of study information. In addition, I tailored my data-collection tool to be consistent with the Hmong’s oral culture—using audio and visuals to collect health information. As a result of the culture- and language-centered research process, the interviews with Hmong participants often lasted longer (between 60 minutes and 120 minutes) than typical interviews and showed higher levels of engagement from participants. Moreover, participants frequently and spontaneously shared experiences unrelated to health condition topics (e.g., cultural factors that may impact health behaviors in general, and the impact of the Vietnam War on their well-being) and identified additional needs of the community (e.g., need to focus more on improving interpreter services). The abundance and level of information shared with the researcher by participants highlights their desire for someone to listen to their concerns.
Engaging Individuals with Intellectual Disabilities
Context
Down syndrome (DS) is the most common genetic cause of IDs (Mefford et al., 2012). Of every 691 live births, one is a child with DS, representing approximately 3,000 to 5,000 DS births in the United States annually (Parker et al., 2010). Characterized by the presence of an extra partial or whole copy of chromosome 21 (Stancliffe et al., 2012), DS and its clinical indicators include poor muscle tone and significant delays in physical and cognitive development (Stancliffe et al., 2012). People with DS are often dependent on others in order for them to fully participate in society. A necessary requirement, for example, is to ensure transportation so that a person with DS can participate in leisure activities, given that these individuals are frequently unable to drive. Employment and housing are additional areas wherein people with DS rely on support from their social networks. These individuals are largely underrepresented in research, with most studies on people with DS examining data generated through interviews with family members or friends of individuals suffering from the condition. This underrepresentation is unsurprising because research involving people with DS and IDs is generally confronted with a number of practical and ethical challenges (Iacono, 2006), such as obtaining informed consent (Cameron & Murphy, 2007), selecting appropriate data collection techniques (Jurkowski, 2008), and addressing obstacles arising from the cognitive abilities of people with IDs (Iacono, 2006).
Strategies
Although I had some prior knowledge of and experience with caring for people with IDs, I had a limited understanding of the needs and history of the local community of people with DS. Over a three-to-four-month period, I used the following strategies to build connections with the local community. To observe and learn about this community in detail, I participated in Buddy Walk, a public event for raising awareness and funds for programs that benefit people with DS and their families. I chose to participate in this event because it was an established program recognized by the community and required no prior relationship with the community. During the three Buddy Walks that I attended, I had conversations with relatives and friends of individuals with DS about their everyday lives in order to grasp the needs and dynamic of this local community. Subsequently, to develop initial connections with the local community of people with DS, I volunteered in an achievement center for people with DS. While volunteering at the center, I worked directly with people with DS and had conversations with their parents or other family members during drop-off and pick-up periods.
The initial connections formed with a few people with DS and their families granted me access to more community members. For example, the mother of a person with DS with whom I conversed with frequently introduced me to her private online support group for families of people with DS. Unexpectedly, she voluntarily facilitated my study recruitment by posting the study recruitment flyer on her online support group. As a result of this introduction of my study and me as a researcher to the local community, members of the community reached out to me, showing interest in participating in the research. Data collection on a social network traditionally involves a network inventory survey. However, apprehensive about the cognitive functioning barriers of conducting research with people with IDs, I tailored my data collection method for my research on social networks of people with DS. The data collection process entailed constructing a social network map together with DS individuals and their family members, facilitated by a social network visualization software. Although the software was not originally developed for people with DS, I chose to use it to construct social network maps rather than engaging network inventory surveys to encourage and support participant engagement in the data collection process.
Analytical Process
To facilitate reflections across cases, we examined the cases using techniques of thematic analysis as discussed by Braun and Clarke (2006). First, we familiarized ourselves with the data by reading each case description. In the beginning, the case descriptions of each person did not follow a specific guideline. Second, we generated initial codes by summarizing the text on an abstract level and identified potential themes by sorting the initial codes to determine if they fit the overall themes. We then checked whether the text aligned with the final themes. Lastly, we described the themes.
Results
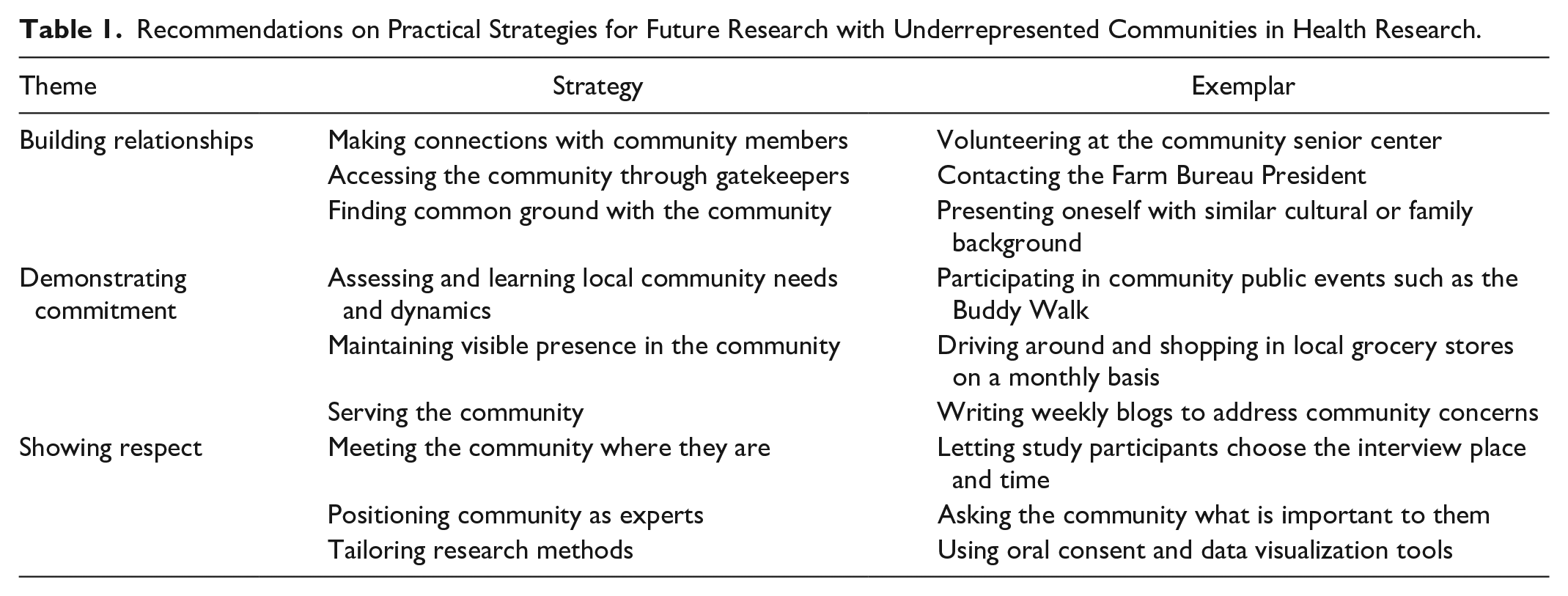
The processes that investigators used across cases to engage underrepresented communities in research aligned into three themes: (a) building relationships, (b) demonstrating commitment, and (c) showing respect (Table 1).
Recommendations on Practical Strategies for Future Research with Underrepresented Communities in Health Research.
Building Relationships
Initiating partnerships with underrepresented communities began with relationship building, primarily because the investigators did not have prior relationships with the community. Strategies for building relationships involved making connections with individual community members, accessing the community through gatekeepers, and finding common ground with the community. The decision to approach the community directly through individual members or indirectly through gatekeepers depended upon the nature of the community and the availability of gatekeeping persons. Importantly, relationship-building was a dynamic process that continued for the duration of the research. Although relationship-building typically involves some extent of reciprocity, the investigators made sure that there was no sense of coercion felt among the communities involved, particularly in cases whereby there were no gatekeepers in place. Spontaneous, voluntary outreach from community members to the researchers reinforced confidence that coercive means were not used. Investigators shared some common ground with the community, such as being a parent or having a similar cultural or family background. These commonalities signaled to the community that the investigators understood their lived experience. However, these commonalities did not grant investigators access or sustain the initial connections with members of the community. Thus, the next process, demonstrating commitment, is essential for ongoing, sustainable community engagement.
Demonstrating Commitment
Before entering the community, all investigators had a general knowledge of the context and needs of these underrepresented communities, but their knowledge of specific local communities was limited. The key action that demonstrated commitment was assessing or learning the needs and dynamics of local communities. Methods for assessing community needs were related to the availability of existing resources (e.g., having a vehicle to drive to the community) of the investigators. Similarly, methods for maintaining a visible presence in the community were influenced by these factors as well as by the characteristics of the communities. For example, innovative methods such as establishing a virtual presence provided an alternative option, as was the case with the immigrant postpartum women’s community. Finally, demonstrating commitment required service to the community by addressing unmet health needs. At times, the communities’ unmet needs were so substantial, however, that serving the community became overwhelming to the investigators. In such circumstances, investigators had to balance their duties and draw boundaries between their roles as researchers and clinicians.
Showing Respect
Consistent with the principles of community engagement (Centers for Disease Control and Prevention, 2011), showing respect involved positioning the communities as experts to determine research priorities and methods. There were various ways to share power with the communities. Investigators asked community members what was important to them or proposed and sought community feedback on study topics based on observations or conversations with selected individuals representing the community. Showing respect also required investigators to be considerate and thoughtful about small, everyday concerns that might not occur to researchers but are important to members of the communities, such as conducting interviews at places of participants’ choosing and being flexible with interview times. Furthermore, when traditional research process (e.g., written consent) or data collection methods (e.g., self-report surveys) presented challenges for certain underrepresented communities, investigators needed to be adaptive about ways (e.g., using data visualization tools) to continuously support and engage study participants in the research process.
Discussion
Engaging underrepresented communities requires an ongoing and reciprocal process of relationship negotiation with the community. Through this process, we learned several lessons about underrepresented communities and the approaches to engage these communities in the research process. These lessons reflect the contextual realities of the communities in which they reside and may provide practical strategies for research directions and methodological considerations for future studies (see Table 1).
Engaging underrepresented communities can be challenging. However, it is not true that these communities prefer not to be engaged. In fact, through our interactions with four communities, we learned that members of these communities wanted to participate in the research process. They liked being interviewed and believed that it was important for researchers to understand and tell their stories. In addition, we learned that these communities were resilient. They wanted us to capture their knowledge, resources, cultural identities, happiness, and gratefulness, and not only the adversities that may have been more apparent to researchers. This lesson reminds us that our job as nurse researchers includes storytelling in a way that brings attention to communities’ assets and strengths as well as to their unmet health needs and limitations. Acknowledging the existing socio-cultural resources within communities is essential for building capacity and implementing strength-based community health promotion (Brough et al., 2004). By working to engage these communities, their experiences, needs, and resilience are recognized by more researchers, promoting greater representation of underrepresented communities in health research.
Underrepresented communities are highly connected within their own network. Members of underrepresented communities attribute significant value to their networks, which bridge exchangeable resources, offer a sense of belonging, and generate cultural identities. This has also been observed in other vulnerable communities, including low-income parents (Curry & Holter, 2015) and LGBT communities (Ceatha et al., 2019). Community organizations and events carry symbolic meaning to members of underrepresented communities and provide a venue of recognition. Moreover, these organizations and events can become a point of entry for researchers to build connections and assess community dynamic and needs.
Members of underrepresented communities can be highly connected while experiencing isolation in their everyday life. Our interviews with participants tended to be lengthy, and the topics of conversation often went beyond the purpose of the interview. Through this process, we realized that we had become a source of companionship for our participants. Similarly, Mills et al. (2013) have found that workers of home-visiting parent support programs reduced participants’ loneliness, particularly for those with small social networks. In some cases, the interview topics covered material that participants rarely disclosed to their friends or families. Having in-depth, non-judgmental conversations about these topics validated and normalized their experiences.
Many underrepresented communities are vulnerable due to their literacy levels (e.g., limited literacy), language proficiency (e.g., non-English), or differences with mainstream culture. As a result, they may not fully understand the research process and may feel that their contribution is unimportant, thereby hindering research participation. As illustrated in the studies with Hmong participants and participants with ID, when the researchers tailored the research process, however, including data collection (i.e., the use of a visual or audio techniques) and informed consent process (e.g., oral vs written), it provided a means through which participants could engage fully in the research project. For example, the Hmong participants were offered verbal consent instead of written consent, consistent with their oral culture. While verbal consent and audio- or video-assisted data collection or consent procedures are not new, they require researchers to be mindful and cognizant of the culture and characteristics of their study participants (George et al., 2013; Hutchison et al., 2007; Lawton et al., 2017).
One of the most critical components of negotiating relationships with underrepresented communities was establishing and maintaining trust throughout the research process (McDonald, et al, 2008). Trust is a complex concept whose meaning varies within and across relationships (Resnik, 2010). Yet in all situations, trust involves a willingness to make oneself vulnerable to others (Tschannen-Moran & Hoy, 2016). Demonstrating competence and acting with honesty, integrity, and transparency increases research participants’ beliefs that their well-being will be protected, which allows them to expose their vulnerabilities through study participation (Tschannen-Moran & Hoy, 2016). Although trust was not measured in presented cases, the personal stories, interview lengths, personal investments in recruitment, and invitation of researchers to serve these communities were indicators that we succeeded in developing credibility and trust with these underrepresented communities.
Engaging communities in research begins by building relationships with the community. The relationships with communities must be continuously negotiated and maintained by researchers’ actions of demonstrating commitment and showing respect. In addition to enhancing researchers’ abilities to address health disparities while prioritizing community needs, community engagement provides a lens of resilience that facilitates identifying strengths and health promotion strategies grounded contextually in a community’s microsystem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.