
Abstract
We assessed the feasibility and acceptability of examining breast/chest feeding attitudes among African Americans in South Carolina using an explanatory sequential, mixed methods approach. We surveyed 50 pregnant African American women during their ob-gyn appointment (Phase I), followed by qualitative interviews with four African American couples (N = 8) (Phase II), and integrating quantitative–qualitative data through joint display (Phase III). Phase I supported the feasibility of recruiting pregnant African American women for our study. However, for Phase II, more research is needed to support the feasibility of recruiting couples from the quantitative phase. The Iowa Infant Feeding Attitude Scale demonstrated moderate reliability (α = 0.68). Participants intending to exclusively breastfeed (M = 65, SD = 5.79) had higher scores than those intending to exclusively use formula (M = 50, SD = 4.37, p < .001). The six qualitative themes (Phase II) and data integration (Phase III) identified cultural considerations for future research.
According to the American Academy of Pediatrics, U.S. infants should be exclusively fed at the breast/chest (only human milk and no other foods/liquids) for 6 months with continued breast/chest feeding for 1 year or longer following the introduction of solid foods (Eidelman et al., 2012). Breast/chest feeding includes feeding a child at the breast/chest or with expressed human milk from the parent or a donor. However, while approximately 86% of White infants in the United States are fed at the breast/chest at some point in their infancy, only 69% of Black infants are ever breastfed (Beauregard et al., 2019). The greatest breast/chest feeding disparities among Black and White populations in the United States are in the Southeast region (Anstey et al., 2017), including South Carolina. Disparities in breast/chest feeding are particularly troubling given the internationally recognized benefits for both parents and their children (World Health Organization, 2017).
Need for a Greater Understanding of Reasons for Racial Disparities in Breast/Chest Feeding
The U.S. Surgeon General (U.S. Department of Health and Human Services, 2011) and the U.S. Preventive Services Task Force (Bibbins-Domingo et al., 2016) have both called for further research to identify the factors that contribute to racial disparities in breast/chest feeding and to develop effective interventions. A substantial number of qualitative (Asiodu et al., 2017; Barbosa et al., 2017; Deubel et al., 2019; LoVerde et al., 2018) and quantitative (Beauregard et al., 2019; Dunn et al., 2015; Fleurant et al., 2017; Oniwon et al., 2016; Riley et al., 2016) studies have focused on barriers, perceptions, and/or knowledge related to breast/chest feeding among ethnic minority women; however, reasons for the lack of breast/chest feeding among African Americans are not yet fully understood (Asiodu et al., 2017). Although a few scholars have used mixed methods approaches to examine these questions (Kamoun & Spatz, 2018; Kim et al., 2017; Munn et al., 2018), researchers can produce a more complete picture of the root causes of breast/chest feeding disparities through a mixed methods design. By integrating quantitative and qualitative findings about the breast/chest feeding experiences and perceptions of African American women, scholars and researchers can develop more culturally responsive and meaningful interventions for these populations (Bacchus et al., 2016). Thus, our goal for this formative study was to use a mixed methods approach to discover unique cultural nuances that might help explain potential underlying reasons for racial and ethnic disparities in breast/chest feeding among African American women. We aimed to gather formative data on African American’s attitudes toward breast/chest feeding that could affect future mixed methods studies and interventions strategies (Czajkowski et al., 2015).
Purpose
This formative study assessed the feasibility and acceptability of using an explanatory sequential mixed methods approach to examine breastfeeding attitudes among African American women and their support partners in South Carolina. Our primary objectives were to assess study feasibility, acceptability, and identify any unanticipated barriers that would be critical to resolve prior to conducting a larger scale study and/or future intervention. Our secondary objective was to interpret our quantitative, qualitative and integrated quantitative–qualitative findings within the context of this exploratory investigation. Although we used the terms “women” and “breastfeeding” at the time of recruitment and data collection, we acknowledge that not all individuals who breast/chest feed identify as women or mothers. Therefore, we use human milk and other gender-inclusive language except when providing direct quotes from our study participants or citing other authors who use other terms.
Methods
Study Paradigm
Our study was guided by a pragmatic research paradigm (Biddle & Schafft, 2015; Creswell & Tashakkori, 2007; Feilzer, 2010). The philosophical underpinnings of this paradigm suggests that “there are singular and multiple realities that are open to empirical inquiry and [pragmatism] orients toward solving practical problems in the real world” (Feilzer, 2010, p. 8). This paradigm advances scientific knowledge through the use of research design and adaptable methodological approaches that yield practical and useful outcomes (Biddle & Schafft, 2015).
Study Design
Our study employed a cross-sectional two-group design. We used an explanatory sequential design to obtain a general understanding of breast/chest feeding through quantitative statistical analysis and then further explored the quantitative results using a qualitative methodology (Creswell & Clark, 2011). The quantitative and qualitative data were then “mixed” or integrated (Fetters et al., 2013) to obtain more comprehensive knowledge about how breast/chest feeding attitudes may serve as an underlying reason for low rates of breast/chest feeding among African Americans.
In the quantitative phase (Phase I), we surveyed pregnant African American women about their breastfeeding attitudes, maternal history, and sociodemographics related to their infant feeding intentions. In the qualitative phase (Phase II), we explored African American women’s experiences with and preferences for feeding their new infants using qualitative interviews with the African American women and their identified support partners (e.g., spouses, significant others, grandmothers, etc.). In the mixed methods phase (Phase III), we integrated the quantitative and qualitative data at the interpretation and reporting level in two ways: integration through narrative and a joint display. First, we integrated the data through narrative using a contiguous approach, by which we report both the quantitative and qualitative findings in separate sections of this manuscript (Fetters et al., 2013). Second, we integrated the data through the use of a joint display, which visually provides a side-by-side comparison of the quantitative and qualitative data to uncover new insights or nuanced inferences beyond the separate quantitative and qualitative findings (Creswell & Clark, 2011; Fetters et al., 2013). This study was reviewed and approved by the Institutional Review Boards of the University of South Carolina and formerly Palmetto Health (currently Prisma Health) hospital system.
Setting
We conducted Phase I at one of the hospital-affiliated clinics that provides comprehensive ob-gyn care. The hospital is one of the largest health systems in South Carolina and provides comprehensive care to over 300,000 patients. The clinic is located in one of the largest metropolitan statistical areas (MSA) in South Carolina and primarily serves racially diverse and economically disadvantaged women. We conducted Phase II in the personal homes of eligible participants who resided in the same MSA as Phase I participants.
Sample
For the Phase I questionnaire, we used a convenience sampling method. Eligible participants had to self-report being (a) pregnant at the time of study, (b) African American, (c) 18 years or older, (d) a resident of South Carolina, and (e) able to speak English.
For the Phase II interviews, we recruited a purposive sample of dyads of African American women and their self-identified support partners. To be eligible, participants had to (a) have had a child in the past 24 months, (b) self-identify as African American, (c) be 18 years or older, (d) be a resident of South Carolina; and (e) speak English. Support partners were identified by the eligible women and could be anyone the woman identified as being supportive of her as a mother (e.g., spouse, friend, parent, etc.). Support partners also had to be 18 years or older and residents of South Carolina.
We asked Phase I participants to provide their contact information if they were willing to (a) participate in a follow-up interview and (b) invite one support person (e.g., expectant father, friend) to join them for a subsequent interview in Phase II. We obtained contact information from six women in Phase I and subsequently invited them via email and/or text messaging to participate in Phase II interviews. We also recruited potential interview participants by emailing African American colleagues, community members, and by posting the study flyer on Facebook and Twitter. The flyer included a direct hyperlink to a Web-based form for interested participants to screen for eligibility and sign up to be contacted by a member of our study team. In total, 23 additional women shared their contact information by completing our web-based sign-up form. Among 29 total interested women, none of the Phase I participants were interviewed in Phase II due to nonresponse.
Measurement
For Phase I, we developed a self-report, quantitative questionnaire that consisted of close-ended questions. The questionnaire assessed participant sociodemographics (multiple choice: age, relationship status, education level; insurance status, enrollment in Women, Infants, and Children [WIC]), maternal history (multiple choice: number of children, previous experience with breast/chest feeding), plans for feeding their new infant (multiple choice: breastfeeding and/or formula), reasons for their feeding decision (select all that apply: e.g., convenience, plan to return to work), actual and preferred sources of information on infant feeding (select all that apply: e.g., websites, providers), and plans for returning to work (multiple choice). We also included the Iowa Infant Feeding Attitudes Scale (IIFAS) to measure participants’ breastfeeding attitudes and perceptions. The IIFAS is a 17-item scale that has been validated with participants in the United States (de la Mora et al., 1999) and is commonly used in breast/chest feeding research (de la Mora et al., 1999; Ho & McGrath, 2010; Holbrook et al., 2013). Each item is rated using a 5-point Likert scale (strongly disagree to strongly agree). The potential scores for the IIFAS range from 17 to 85 with lower scores indicating positive attitudes toward formula feeding and higher scores indicating positive attitudes toward breastfeeding (de la Mora et al., 1999). The questionnaire consisted of a total of 42 questions, including the IIFAS.
For Phase II, we developed a semistructured interview guide based on previous literature on African American women and breast/chest feeding. After each interview, we also provided participants with a questionnaire adapted from the Phase I survey. Questionnaires distributed to the participants who had recently given birth were revised to reflect participants’ postpartum experiences with infant feeding. We also created a modified version of the questionnaire for the support partners to complete, which consisted only of sociodemographic questions and the IIFAS scale. The Phase II questionnaires for the participants who had recently given birth and their support partners consisted of a total of 42 and 22 questions, respectively.
Data Collection
For Phase I, questionnaire data were collected from April to June 2015. Potential participants were approached by either one of the coprincipal investigators (co-IPs) (TMF, JRJ) and/or an undergraduate nursing student who was trained in human subjects research. The co-PIs were a doctorally prepared African American social worker and a maternal/child health nurse (PhD and EdD, respectively). We asked potential participants about their interest in completing the questionnaire in paper format while they were waiting for their scheduled ob-gyn appointments. Once we screened participants for eligibility and they agreed to participate, we gave the participants the self-administered questionnaire and asked them to complete it. The questionnaire did not request any protected health information. The study co-PI(s) remained in the waiting room until participants completed their questionnaires in the event any participant had any questions about the study. After completing the questionnaire, the study co-PIs provided the participants a $10 cash stipend.
For Phase II, the study co-PIs conducted face-to-face, qualitative interviews from January to March 2016 with the selected participants. We interviewed each dyad of participants together in their homes. After the completion of the interview, we also asked participants to complete the revised questionnaires. All participants were given a $20 cash stipend for completion of the interviews and questionnaires. All interviews were audio recorded.
Outcome variables
Our primary study outcomes were study feasibility and acceptability. For Phase I, we defined feasibility as the recruitment of 50 pregnant, African American women from the hospital-affiliated, ob-gyn clinic for Phase I (quantitative). Given the formative nature of this study, an a priori sample size calculation was not appropriate. However, our targeted sample size of 50 aligned with the range of recommended and observed sample sizes for feasibility and pilot studies (Billingham et al., 2013). For Phase II, we assessed the feasibility of recruiting of a subsample of African American women from Phase I and their support partner for qualitative interviews. We set our goal to recruit 20% of Phase I participants (plus their identified support partner, n = 10 dyads) for Phase II. We evaluated acceptability as the participant responses to the follow-up email and texting procedures used to invite Phase I and other interested participants to take part in the Phase II interviews. For secondary outcomes, we evaluated the psychometric properties of the of the IIFAS tool (Phase I) and assessed barriers and facilitators of breastfeeding through the qualitative interviews (Phase II) and mixed methods integration (Phase III).
Data Analysis
For the Phase I questionnaire, our main outcomes of interest were breast/chest feeding attitudes and infant feeding intentions. We conducted descriptive statistics on all sociodemographic, maternal history, breastfeeding attitudes, and infant feeding intention variables. We measured breastfeeding attitudes by IIFAS scores and infant feeding intentions by a single questionnaire item asking participants how they planned to feed their new infant: breast (i.e., human milk), bottle (i.e., formula), or both. To assess psychometric properties, we calculated Cronbach’s α to assess the reliability of the IIFAS in our sample. While formal hypothesis testing is not a primary goal of formative research (Lee et al., 2014), we also conducted a series of descriptive and bivariate analyses (independent t-tests, one-way ANOVA, chi-square tests, as appropriate) to evaluate the predictive validity of the IIFAS by sociodemographics, maternal history and infant feeding intentions. We also explored infant feeding attitudes by sociodemographics, maternal history, and breastfeeding attitudes. We used Stata 15 (StataCorp, 2017) to conduct analysis. A p-value < .05 indicated statistical significance.
For Phase II interviews, a professional transcriptionist transcribed all of the interviews. We reviewed the transcripts for accuracy and removed participant names to ensure confidentiality. We conducted an inductive thematic analysis in order to identify emergent codes and themes across the qualitative data (Braun & Clarke, 2006). We used an affective coding method, versus coding, which identifies processes, structures, and concepts that may be in direct conflict with one another (Saldaña, 2015). Commonly used in policy and education research, this method is appropriate for investigations of phenomena, such as breast/chest feeding, that may elicit strong conflicts, competing goals, and/or opposing norms within, among, and between participants (Saldaña, 2015).
For the first iteration, two doctoral students independently generated initial codes from the interview data as dichotomies (e.g., us vs. them) and compared the codes across the transcripts. The full research team (doctoral students and co-PIs) discussed the first iteration codes, and for the second iteration, each member independently compared, sorted, and grouped the versus codes. Next, the full team discussed and organized the versus codes into thematic categories. For the third iteration, team members condensed redundant versus codes into appropriate categories. For the final iteration, the full team reached 100% consensus on the final versus codes and thematic categories and used in vivo codes from the original transcripts to describe them. We maintained a detailed audit trail to document our research methods and processes (Cohen & Crabtree, 2006), including researcher reflexivity.
For Phase III mixed methods analysis, we developed a joint display to examine how the Phase II qualitative data could provide greater insights into IIFAS items that indicated neutral participant responses in Phase I. Based on the distribution of the IIFAS scores in our Phase I sample, we defined a “neutral response” as any IIFAS item for which the participants’ mean score was 3–3.5 (score range: 1–5). For the IIFAS items with neutral responses, we created a “statistics-by-themes matrix” (Guetterman et al., 2015) of the IIFAS scale items that indicated neutral mean scores from Phase I by qualitative quotes from Phase II that were related to the IIFAS items with neutral mean scores. Quotes were classified as either being “congruent” or “noncongruent” with each corresponding IIFAS item.
Reflexivity Statement
The first (TMF) and last author (JRJ) served as co-PIs of their first funded study focused on promoting breast/chest feeding among African American women. At the time of study, TMF was an assistant professor and health disparities researcher and J.R.J. was a clinical assistant professor and maternal/child nurse. Authors TMF and EHH were mothers who had breastfeeding experience at the time the data were collected and analyzed. Authors CAN and EC were doctoral students in nursing science and public health, respectively, at the time of study. Prior to beginning their doctoral programs in South Carolina, CAN was a nurse-midwife born and raised in Nigeria and EC was a physician born and raised in Turkey. All other authors (TMF, CMT, EHH, JRJ) were African American women who were born and raised in South Carolina.
Results
Phase I: Quantitative Results
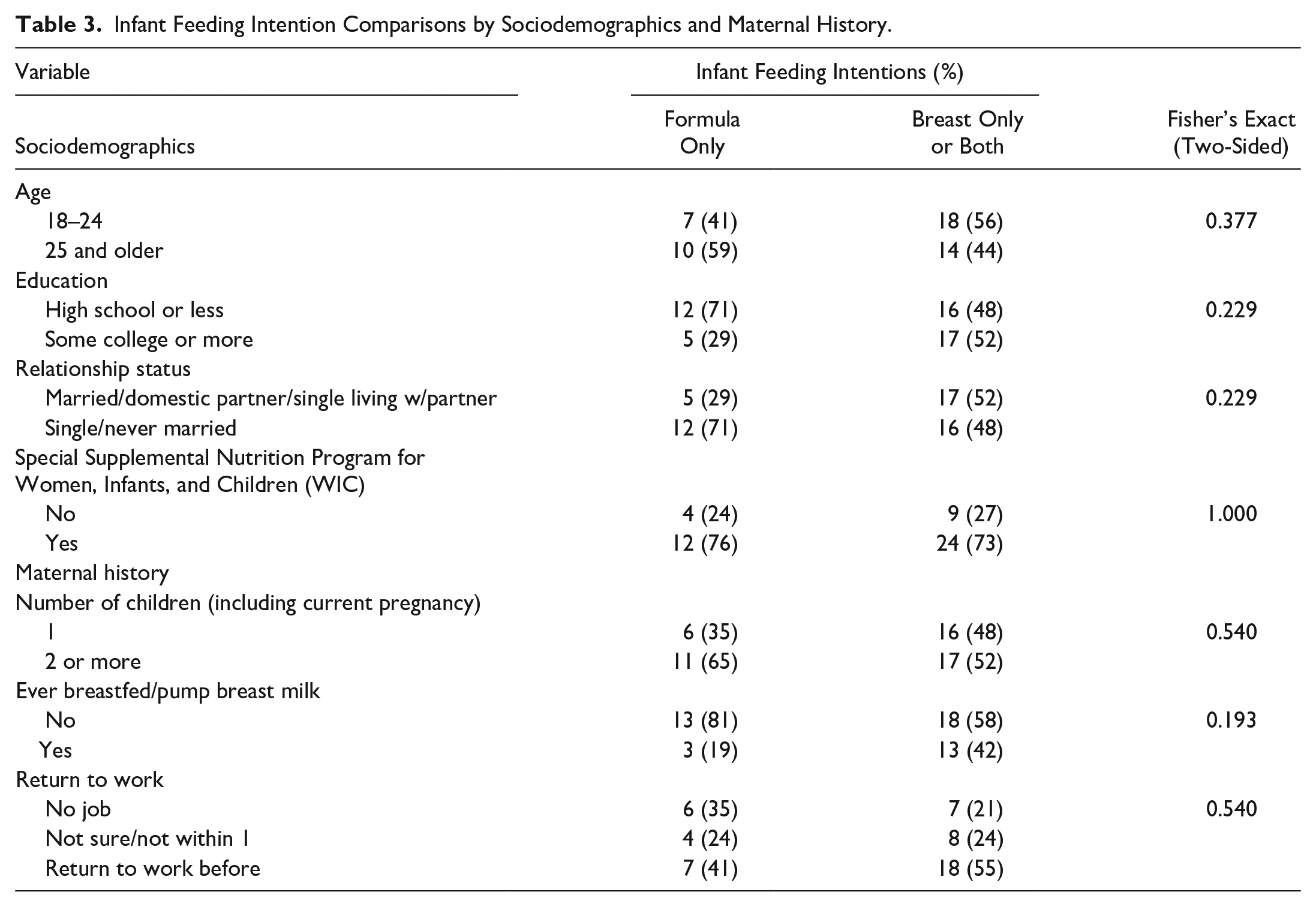
Fifty women (N = 50) were recruited for Phase I and completed the questionnaire. Half (n = 25) of the women were 18–24 years old and 40% (n = 20) graduated from high school or received a GED. About half reported being single and never married (n = 27, 54%) and most were enrolled in Medicaid (n = 45, 90%) and WIC (n = 37, 74%) (Table 1). We display differences in breast/chest feeding attitudes by sociodemographics and maternal history in Table 2, and infant feeding intentions by sociodemographics, maternal history, and breast/chest feeding attitudes in Table 3.
Sociodemographic Characteristics, Maternal History, Infant Feeding Intentions and Breastfeeding Attitudes of the Women’s Clinic Questionnaire (Phase I) and Qualitative Interview Samples (Phase II).
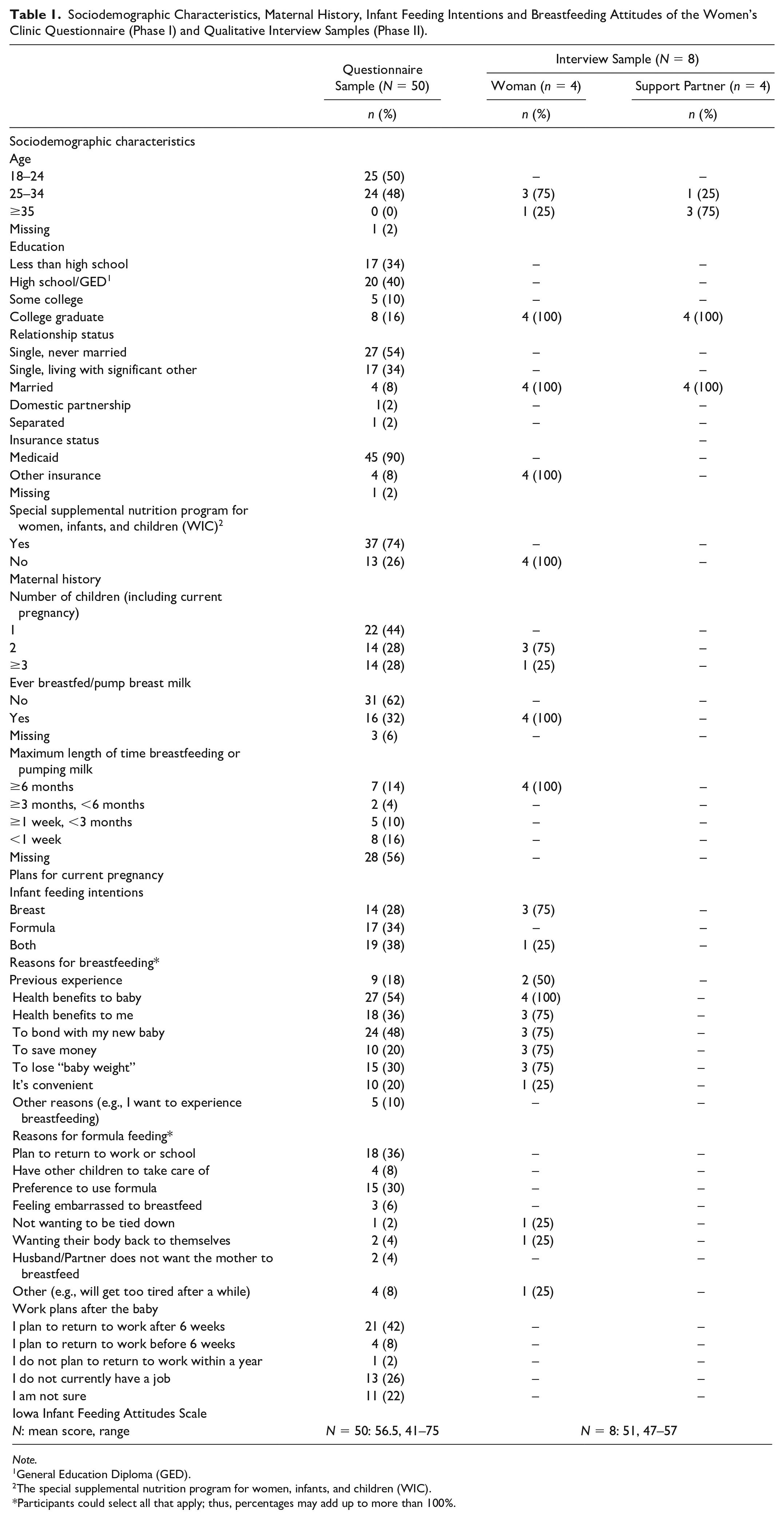
Note.
General Education Diploma (GED).
The special supplemental nutrition program for women, infants, and children (WIC).
Participants could select all that apply; thus, percentages may add up to more than 100%.
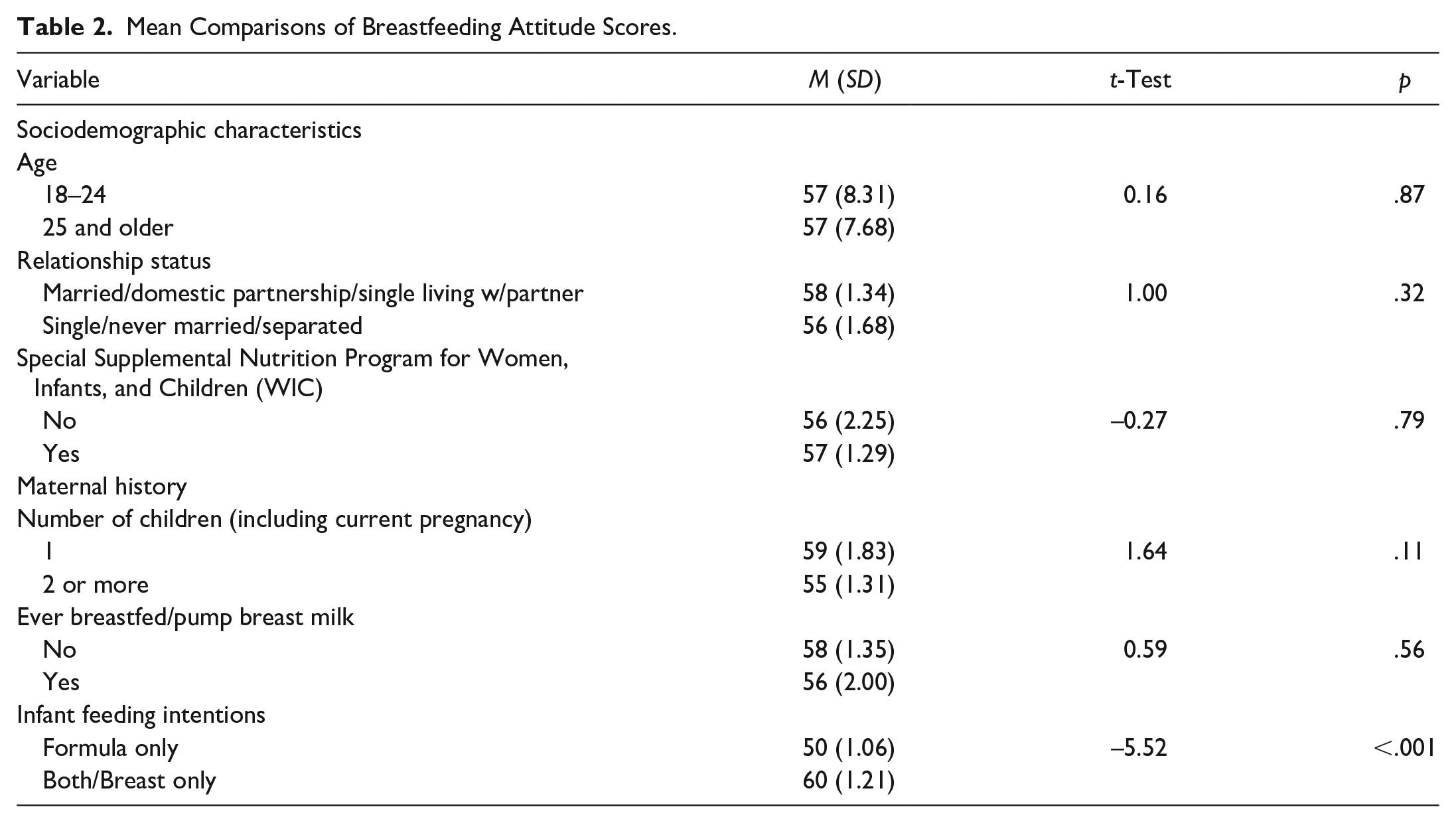
Mean Comparisons of Breastfeeding Attitude Scores.
Infant Feeding Intention Comparisons by Sociodemographics and Maternal History.
IIFAS instrument reliability and validity
Participant breastfeeding attitudes, as measured by the IIFAS, had moderate reliability (α = 0.68) in our sample, which is consistent with the range of Cronbach’s alpha coefficients (0.68–0.86) previously reported in the initial validation studies (de la Mora et al., 1999) and similar to a previous study that reported Cronbach’s alpha of 0.70 among African American participants (Jefferson, 2017).
The sample had a mean IIFAS score of 57 (SD = 7.8, range: 41–75). One-way ANOVA results showed statistically significant differences in IIFAS scores based on the number of children that a participant had, F(2, 47) = 4.78, p = .013. Post hoc comparisons using Bartlett’s test with a Bonferroni correction showed statistically significant lower IIFAS scores—indicating more negative breastfeeding attitudes—among participants who had more than one child. Specifically, participants with ≥3 children (including their current pregnancy) had significantly lower IIFAS mean scores (M = 52, SD = 6.19) than participants having their first child (M = 59, SD = 8.61, p = .019) or second child (M = 59, SD = 5.90, p = .041). We also found significant differences in IIFAS scores by infant feeding intentions, F(2,45) = 25.45, p < .001. Post hoc comparisons using Bartlett’s test with a Bonferroni correction showed higher mean IIFAS scores for participants who intended to exclusively breastfeed (M = 65, SD = 5.79) versus those who intended to exclusively use formula (M = 50, SD = 4.37, p < .001) or both human milk and formula (M = 58, SD = 6.27, p = .002). Among WIC participants (n = 37), we also observed those who intended to exclusively breastfeed (M = 64, SD = 6.12) scored significantly higher than those intending to exclusively use formula (M = 51, SD = 3.40, p < .001).
Phase II: Qualitative Results
We recruited four dyads (N = 8) to participate in the qualitative interviews, consisting of African American women and their support partners, all of whom were male spouses. Interviews lasted between 31 and 58 minutes (average time = 45 minutes). All women participants (n = 4) were college graduates, did not receive WIC and had breastfed at least 6 months or longer. All male support partners were also college graduates (n = 4) and most were 35 years or older (n = 3) (Table 1).
For Phase II, we identified six interrelated thematic categories that emerged from the participant interviews (Table 4). Overall, participants felt that an African American woman’s decision to breastfeed was influenced by interrelated factors at multiple levels: individual (sacrifice vs. opportunity: “It’s about your baby. It’s about what breastfeeding does.”), interpersonal (woman’s job vs. team effort: “. . .my husband is on board. We’re a team effort.”), health care systems/providers (pushing formula vs. pushing breastfeeding: “I don’t remember getting any education about ‘nursing’ in the doctor’s office.”), African American community (contemporary practice vs. cultural traditions: “You know my mom formula fed. Her mother formula fed. That’s all they know.”), and broader society (White vs. Brown Babies: “. . .when you see images of breastfeeding, it’s not Black women”; Sexual pleasure vs. actual purpose: “They’d rather have the sexual pleasure from the breast, instead of the actual purpose of it”).
Quotations Illustrating Major Themes and Versus Codes from Qualitative Interviews with the African American Couples (N = 8).
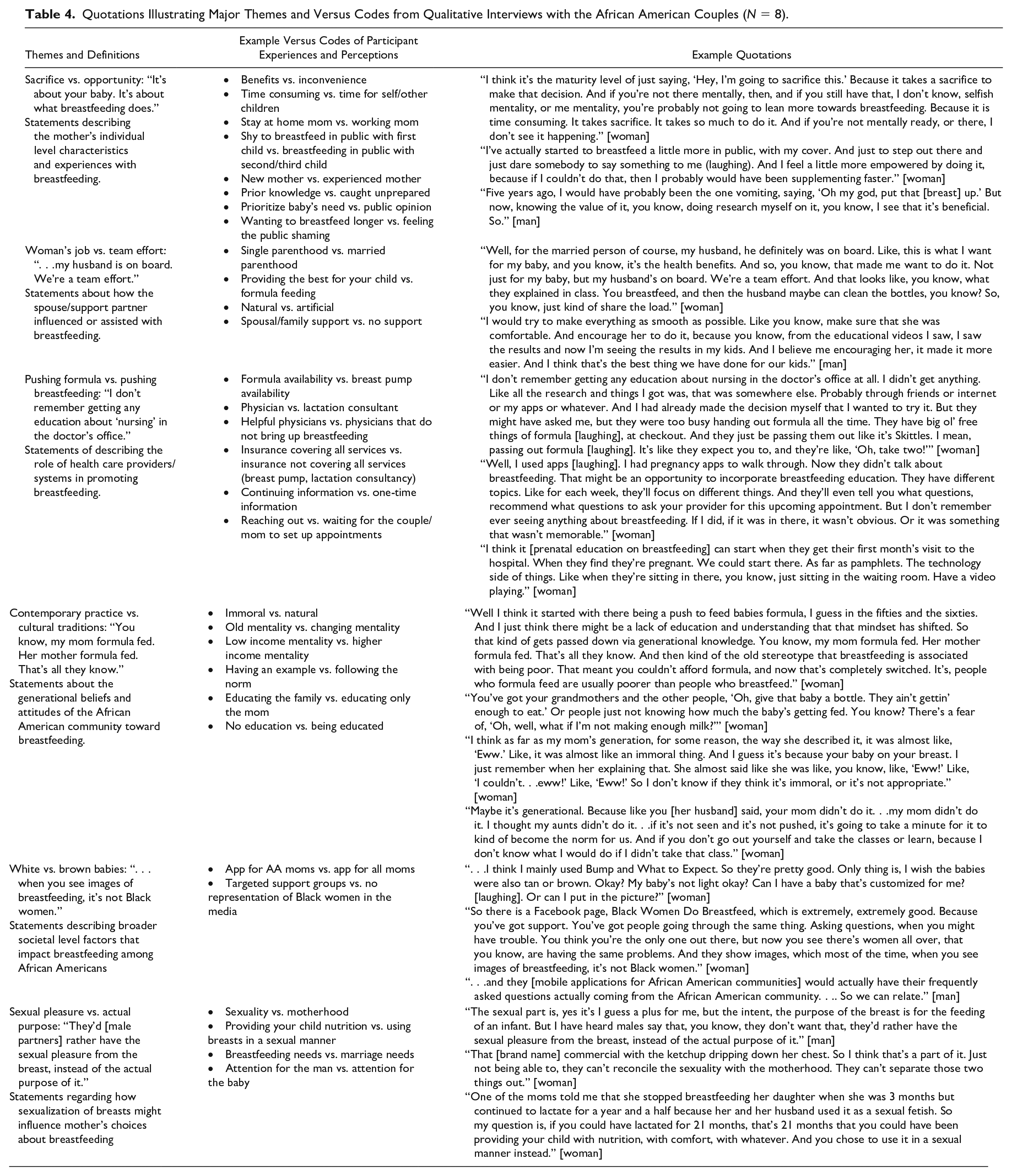
Sacrifice vs. opportunity
The African American women participants shared both positive and negative experiences with breastfeeding, emphasizing the complexity of breastfeeding being both a sacrifice and an opportunity. Participants described mutually deciding as a couple to breastfeed prior to the birth of their new infant. Key factors that influenced their decision to breastfeed included breastfeeding their previous child(ren), financial considerations, and the couples’ shared belief that breastfeeding was the best choice for their new infant: I mentioned my friend. Like, we had a heart to heart. And she just reminded me and got me back grounded, and took me back to like the foundation of what it’s about. It’s about your baby. It’s about what breastfeeding does. It’s about the benefits. It’s about the health benefits. It’s about the bond. It’s about, she just made me, she brought me back to where I needed to be. So that is what kept me going. The support. And then when she got me to thinking about my baby again, and what it’s going to do for him. And then that prepared me mentally to just fight it through. [woman] Because it takes a lot of maturity as well. It takes support from your family, your spouse mainly also pushing you to do it. And I think it’s the maturity level of just saying, “Hey, I’m going to sacrifice this.” Because it takes a sacrifice to make that decision. [woman]
Woman’s job vs. team effort
Couples described breastfeeding as a “team effort” and not simply the woman’s role. The African American women participants shared that the support from their male spouses played an essential role in their ability to initiate and continue breastfeeding in the face of multiple challenges: Yeah, breastfeeding was the best choice. Especially when we were having two kids both in daycare, and you still, you have to deal with those expenses. So like you said, why not get something free when it’s available? [man] The number one thing that I would say is get the men on board. Because obviously these women are following behind their head of house or whatever garbage big White Jesus been telling them. So, if you can get their husbands on board, I think you can probably get the women to breastfeed. Or the boyfriend or the spouse or whoever. Because I think that’s really where it’s coming from. They aren’t doing it because they don’t have support. [woman]
Pushing formula vs. pushing breastfeeding
Participants expressed that their health care provider had little to no effect on their decision to breastfeed. They expected to receive breastfeeding education from their health care providers; however, this expectation was not met. Furthermore, participants shared that their providers promoted formula feeding. They also talked about receiving breastfeeding education from prenatal classes or other pregnancy-related resources (e.g., mobile phone applications), as well as from select family members and friends: [Participant talking about their ob-gyn] I don’t even think they asked me if I was going to breastfeed. This time he asked, but he couldn’t even recommend a good pump. I mean, he just was completely oblivious to what I should do. I actually ended up turning to my supervisor, who’s an extended breastfeeder, and I got a lot of my questions answered from her. Our pediatrician who is a nurse practitioner is also a certified lactation consultant. So I did a meeting with her, and got a lot of information about what I needed. [woman]
Contemporary practice vs. cultural traditions
When asked about the reasons why many African American women do not breastfeed, participants shared that breastfeeding did not seem to be a celebrated practice in African American families. They thought that the reality of many African American women being working women made it difficult for them to breastfeed. Participants said there seemed to be a lot of tension around breastfeeding in the African American community, where it is alternately perceived as “nasty,” “immoral,” “gross,” “unnatural,” “natural,” or “best choice”: Because my mom, she didn’t breastfeed me. And she was married, and she also had three other children. So it could be like, it’s very convenient to formula feed your baby. Very convenient. And then she also made a gesture, like, “Ooh, I just couldn’t, ooh! So I don’t know if they think it’s—” [woman] “Nasty, or—?” [man interjects] “Yeah, immoral or something like that.” [woman]
Participants also discussed the generational aspect of negative perceptions around breastfeeding. They shared that their mothers and other older family members did not breastfeed and, in some ways, discouraged them from doing so. Even though the participants did not allow these negative perceptions to influence their own decision to breastfeed, they believed that these negative perceptions were being passed down generationally and were a reason for low rates of breastfeeding among African Americans. They also highlighted how these negative perceptions of breastfeeding were often reinforced because few African American female or male role models served as positive examples of breastfeeding.
White vs. brown babies
Participants noted that breastfeeding was presented and celebrated as a “norm” for women in the broader U.S. society; however, little attention has been given to the diversity of women’s experiences. African American women participants noticed a lack of images in popular media and mobile applications showing African American women breastfeeding; as a result, participants said it was hard to relate to the information provided: You think you’re the only one out there, but now you see there’s women all over, that you know, are having the same problems. And they show images, which most of the time, when you see images of breastfeeding, it’s not Black women. [woman]
Sexual pleasure vs. actual purpose
Participants also felt that society viewed women’s breasts as sexual objects. Along with acknowledging breasts as a source of sexual pleasure, they referred to breasts as natural “bottles,” describing the main purpose of breasts as “feeding of a baby.” They thought that the sexualization of breasts forced African American women to reserve their breasts for sexual pleasure in intimate relationships versus providing for the nutritional needs of their children: Also just not wanting that interaction. Like, they don’t want to be touched. . .. From my family, my mother said she didn’t like the feeling of it, so she didn’t do it. And she never taught my sisters to do it. So that’s why they don’t do it. They say the same thing. They didn’t like the touching of the, somebody touching their boobs like that. [man] They didn’t want anybody who wasn’t a man touching their boobs. . .. Yeah, I think it’s very different. I think they have sexualized their bodies to the point where they cannot, it’s not extricable from there. They can’t, that duality is not possible. The mother and the spouse part of it just can’t coexist. [woman]
Phase III: Integrating the Quantitative and Qualitative Results
In Table 5, we present our joint display of the Phase I and Phase II data integration. Under the quantitative results headings we display 8 of the 17 IIFAS scale items for which Phase I participants reported neutral mean scores. Under the qualitative heading, we display quotes from the Phase II participants that address the IIFAS statement. For four of the eight IIFAS items in Table 5, participants did not specifically discuss the content of those items (e.g., human milk is lacking iron, mothers who formula feed miss one of the great joys of motherhood, etc.) during the qualitative interviews. For the remaining four IIFAS items, there were both congruent and/or noncongruent responses that aligned with the quantitative responses.
Joint Display of Exemplar Quotes from the Qualitative Interviews that Provide Context to the Quantitative Breastfeeding Attitudes Items with Neutral Mean Scores.
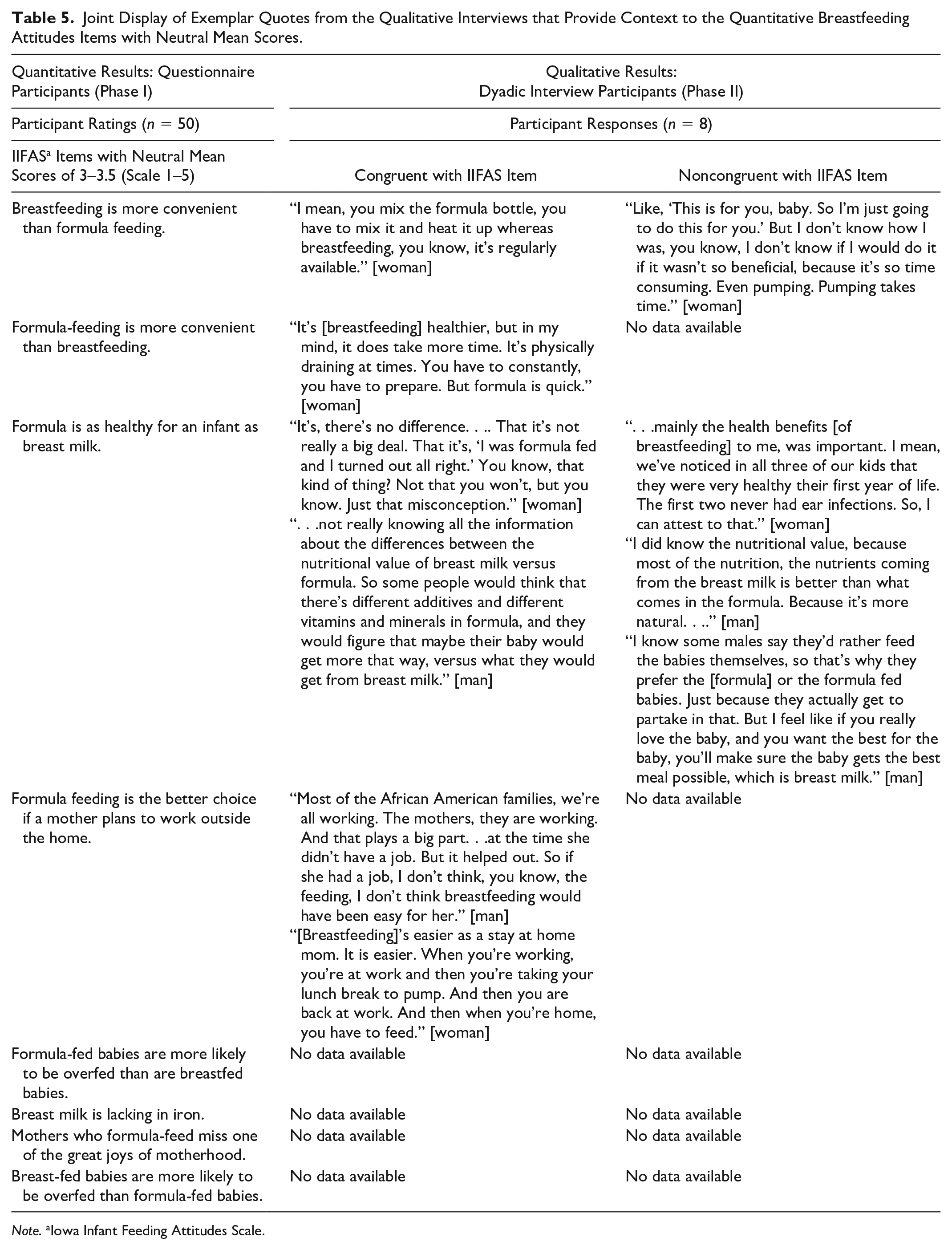
Note. aIowa Infant Feeding Attitudes Scale.
Regarding the convenience of formula feeding versus breastfeeding, participants’ responses reflected a diversity of perceptions about convenience; they described breastfeeding as “regularly available” but also “time-consuming.” For the IIFAS item addressing formula feeding being more convenient than breastfeeding, participants described breastfeeding as being “physically draining” and noted that it “takes more time. . .but formula is quick.” Interview participants stressed that human milk was healthier than formula, but they also mentioned that some people in their communities believed that there are no nutritional differences between formula and human milk, potentially explaining the neutral score on this item. The final IIFAS item indicating a neutral response was about formula being a better choice for mothers who work outside the home. The congruent responses noted that most African American mothers work and that work plays a significant role in their ability to breastfeed. Participants stated that “breastfeeding is easier as a stay-at-home mom.”
Discussion
This formative study evaluated the feasibility and acceptability of recruiting African American women and their support partners to participate in mixed methods research to obtain a greater understanding of Africa Americans’ beliefs and attitudes about breast/chest feeding. For quantitative Phase I, we met our feasibility goal of recruiting 50, pregnant African American women to complete our questionnaire. We believe that four key elements of our recruitment methods contributed to the success of meeting this goal: (1) broad study eligibility criteria; (2) research team remaining onsite during data collection; (3) low participant burden to complete questionnaire; and (4) immediate receipt of financial stipend following questionnaire completion.
For Phase I, the IIFAS indicated moderate reliability for assessing breastfeeding attitudes in our study sample which aligns with previous studies (de la Mora et al., 1999; Jefferson, 2017). The results also suggest the predictive validity of the IIFAS. Similar to previous research (de la Mora et al., 1999; Ho & McGrath, 2010; Kim et al., 2017), the IIFAS was significantly associated with participants’ intention to exclusively breastfeed and differentiated between those desiring to breastfeed versus formula feed. We also identified statistically significant differences in participants’ attitudes based on the number of children they had and enrollment in WIC. Regarding number of children, we posit those participants may have felt that exclusively breast/chest feeding a newborn would be difficult while also having to tend to other children. Regarding WIC, we speculate that those who were in WIC may have received breast/chest feeding education or support that may have positively influenced their breastfeeding attitudes and intentions to exclusively breastfeed. While an a priori sample size calculation was not required for this formative study, we were able to identify these statistical differences between key variables where the strength of the relationship was not impacted by the size of the sample. However, these statistically significant findings, as well as the nonsignificant differences, should be further investigated in a larger, appropriately powered study.
For Phase II, we fell below the feasibility criteria we established for the qualitative interviews. The intent of using the explanatory sequential design was to gain a deeper understanding of selected Phase I participant responses on the questionnaire—particularly their initial infant feeding intentions versus actual feeding behaviors in a qualitative interview following birth of their new baby. Unfortunately, we experienced challenges with recruiting for Phase II interviews, as only 6 (8.3%) versus our goal of 10 (20%) out of 50 participants from Phase I, provided their contact information for the subsequent Phase II interview. For those who provided their information, their loss to follow-up was likely due, in part to two key factors. First, while our broad study eligibility criteria of being pregnant at the time of study made it highly feasible to recruit for the Phase I questionnaire, it may have served as an unintended barrier to recruiting from Phase I to Phase II because we likely recruited women at various stages of their pregnancy (e.g., 12 weeks vs. 30 weeks). Depending on how far along the Phase I participants were in their pregnancy may have impacted some of their willingness to participate in Phase II. The heartbreaking reality of pregnancy loss or related complications could also account for some of the Phase I participants’ lack of response. Unfortunately, we did not record the number of weeks pregnant for each participant. Second, the lack of response to our email and text invitations suggests that Phase I participants did not find these procedures acceptable. Future research should explore ways to remain in touch with Phase I participants until Phase II recruitment begins, as well as connecting with participants through phone calls in addition to texting to reduce loss to follow-up.
We also did not meet our goal of 10 couples from Phase I for the Phase II qualitative interviews. While saturation is the most common and preferred standard used to support qualitative sample sizes, we do not claim to have achieved saturation in this sample. However, our sample and findings can be evaluated within the context of the principles of information power. Directly aligned with our pragmatic study design, information power outlines five key dimensions to be considered: (1) breadth of the study aim; (2) sample specificity; (3) use of established theory; (4) quality of dialogue; and (5) analysis strategy (Malterud et al., 2016). Information power argues that “the more information the sample holds, relevant to the actual study, the lower number of participants is needed (Malterud et al., 2016, p. 1759).” Based on this premise and concept’s five dimensions, we deem that our study reflects moderate information power, which could have been enhanced by recruiting a larger, more diverse sample of African American couples of various relationship structures (e.g., domestic partnership, in a relationship, married, living with a partner). Findings from our qualitative interviews most accurately describe infant feeding experiences of African American mothers in South Carolina who were married to African American men and had a child ≤24 months versus African American mothers in South Carolina more generally. Despite this, a key strength of our qualitative analysis is our use of versus coding which allowed us to provide some new ways of understanding the breast/chest feeding challenges faced by African American women. These findings can serve as preliminary data for further investigation and corroboration.
Our identified themes from the Phase II interviews and results of the quantitative-qualitative data integration provided important cultural context that should be considered in designing a future mixed methods study and/or pilot intervention. African American women with strong support systems, including partner support, are more likely to choose to breastfeed (Gross et al., 2017; Jones et al., 2015). Participants in the qualitative phase of this study confirmed this by emphasizing how the instrumental and emotional support of their spouses was critical to their ability to initiate and continue breast/chest feeding. The themes that emerged from the qualitative data indicated important barriers to breast/chest feeding in African American communities: lack of appropriate support for working mothers, lack of culturally tailored breastfeeding promotion, lack of breastfeeding education and encouragement from health care providers, longstanding misconceptions of breastfeeding within African American communities, and the sexualization of women’s breasts. Other studies have also documented that health care providers did not engage enough with pregnant African American women about breastfeeding and, at times, had an oppositional stance (Spencer et al., 2015).
Results from our integrated data suggested that participants perceived breastfeeding as both convenient and time-consuming (versus formula). For example, in the joint display, participants shared that formula feeding was viewed as a somewhat more convenient, or at least more reasonable, choice for working African American women. Compared to women from other racial/ethnic groups, African American women are more likely to return to work earlier (Beauregard et al., 2019; Shealy et al., 2005; Spencer & Grassley, 2013;), more likely to have jobs with insufficient maternity leave and less flexibility, and find the workplace to be an unsupportive environment (Johnson et al., 2015; Steurer, 2017). Our integrated results also indicated that participants reported mixed perceptions as to whether formula is as healthy for newborns as human milk. Common practices of in-hospital formula introduction to African American infants and the marketing of infant formula may play a role in these perceptions. For example, McKinney et al. (2016) found that the Black/White gap in breastfeeding duration could be reduced by nearly 2 weeks if hospital formula introduction was eliminated. While formula is a critical infant feeding option for families to have, the formula industry’s aggressive marketing and advertisements—particularly to African American communities—are designed to send mixed messages to the consumer about the challenges of breastfeeding (Freeman, 2019; Kaplan & Graff, 2008; Valaitis & Shea, 1993).
Our study had some limitations. Due to logistical and financial constraints, our quantitative and qualitative sample sizes were relatively small, which limits generalizability. Our Phase III data integration should also be interpreted with caution, given that our Phase I and Phase II participants differed sociodemographically. Additionally, some of the qualitative participants were known and connected via social media to the study co-PIs. All participants were recruited from South Carolina; therefore, their perceptions and attitudes may differ from African Americans in other geographic locations.
In conclusion, our results suggest the feasibility of recruiting pregnant, African American women to a mixed methods study to gain a greater understanding of the low rates of breast/chest feeding in the African American community. However, modifications to the recruitment methods and study procedures from the quantitative to qualitative phases would be needed to increase and diversify recruitment and retention, as well as to enhance study acceptability. Our formative findings highlight the importance of considering African American’s differences in beliefs and attitudes based on age, education, socioeconomic factors, and relationship status when developing future breast/chest feeding studies and interventions. Future studies should also further investigate how the number of children, WIC enrollment, plans for returning to work and perceived nutritional value of human milk versus formula may shape African American women’s breast/chest feeding attitudes and infant feeding intentions. Applying mixed methods approaches and including more diverse samples (e.g., relationship status) of African American women and their support partners is also critical to better understanding underlying belief systems and designing effective interventions that can improve the initiation and overall experience of African Americans who desire to breastfeed.
Footnotes
Acknowledgements
This study was funded by a University of South Carolina Institute for African American Research Fellowship (2014–2015). We would like to thank Dr Dana Dehart for reviewing initial drafts of this manuscript. We would also like to thank the nurse managers at Palmetto Health who graciously worked with us and all the families who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an Institute for African American Research Fellowship at the University of South Carolina.