
Abstract
Although family caregivers who use both the personal and social resourcefulness skills have the best health outcomes, it is unknown whether their tendency toward personal or social resourcefulness varies by their care recipient’s condition. This cross-sectional study of existing data from 234 caregivers of persons with various conditions examined five item pairs from the Resourcefulness Scale© with responses capturing personal and social resourcefulness in relation to anxiety, anger, sadness, indecision, and financial distress. Caregivers were categorized by the recipient’s condition (amyotrophic lateral sclerosis, cancer, dementia, mental illness, Parkinson’s disease, stroke, traumatic brain injury, other, or multiple conditions). Findings showed that across most groups, caregivers used both personal and social resourcefulness when angry, sad, or indecisive and personal resourcefulness when anxious or managing money. Caregivers of persons with cancer, traumatic brain injury, stroke, and mental illness differed. The findings provide a basis for future clinical trials across diverse caregiver groups.
The most recent statistics on family caregiving in the United States show an increase by 9.5 million between 2015 and 2020 representing a total of 53 million caregivers and more than one in five Americans (AARP & National Alliance for Caregiving, 2020). The study included family caregivers of persons with long-term physical conditions, memory problems, emotional, behavioral, or mental health issues, developmental and intellectual disorders, and short-term medical conditions. In addition, over the past five years, the findings indicated that a greater number of family caregivers (45% compared to 38%) were providing care for persons with multiple comorbid conditions (AARP & National Alliance for Caregiving, 2020). Most importantly, the study revealed that the health of these family caregivers was much worse than it was five years prior (AARP & National Alliance for Caregiving, 2020).
Regardless of the care recipient’s medical condition, the impact of caregiving on the caregiver’s health may be reflected in the caregiver’s feelings of anger, anxiety, sadness as well as their ability to make decisions and to manage financial distress. Caregiving events and demands and care recipient behaviors and symptoms have been found to affect caregiver health and quality of life adversely across informal caregiver populations. For example, the effects of anger, anxiety, and sadness on health outcomes have been examined in caregivers of persons with dementia (Liu et al., 2015; Steffen & Merritt, 2012; Watson et al., 2018), mental illness (Zauszniewski & Bekhet, 2014), multiple sclerosis (Pooyania et al., 2016), cancer (Schumacher et al., 2008), heart failure (Chung et al., 2020), and a mixture of chronic conditions (Moss et al., 2019). Research has also appraised the challenges faced by family caregivers regarding indecisiveness in studies of caregivers of persons with dementia, Parkinson’s disease, traumatic brain injury (TBI), and other chronic illnesses (Lewis et al., 2000; Whitlatch, 2008). Finally, studies have investigated the impact of financial strain and burden on the family caregiver’s self-care ability and overall health and quality of life among caregivers of persons with dementia (Liu et al., 2019; Turner et al., 2015), cancer (Balfe et al., 2016; Ferrell & Kravitz, 2019), cardiovascular disease (Mochari-Greenberger & Mosca, 2012), and mixed samples of family caregivers (Götze et al., 2014; Lai, 2012).
Collectively, the health and quality of life of family caregivers of persons with various health conditions may be compromised as they experience feelings of anger, anxiety, sadness, indecisiveness, and financial distress while providing care and support for their family members. Yet, research findings show that caregivers have better physical and mental health when they use resourcefulness skills (Zauszniewski et al., 2009; Zauszniewski & Burant, 2020; Zauszniewski et al., 2016). Research shows that persons who are flexible and able to use both the personal and social resourcefulness skills interchangeably have better health outcomes than those who use either the personal or social resourcefulness skills alone; those who use neither the personal or social resourcefulness skills have the worst health outcomes (Zauszniewski, 1996).
Theoretical Framework
Applying Zauszniewski’s midrange theory of Resourcefulness and Quality of Life©, resourcefulness is a compendium of cognitive-behavioral skills for coping with adversity (Zauszniewski, 2018). The skills constituting resourcefulness are of two types: personal or self-help skills and social or help-seeking skills (Zauszniewski, 2016, 2018). While examples of personal resourcefulness include problem-solving, organization, positive affirmation, cognitive reframing, and intentional behavior change, social resourcefulness skills include reliance on others, social exchange, and professional guidance. The personal and social resourcefulness skills are affected by process regulators that affect one’s health and quality of life, which may include perceptions, thoughts, and feelings. In general, process regulators may be cognitive, affective, motivational, or volitional factors, which provide the context in which resourcefulness skills may be used (Zauszniewski, 2016, 2018). In the study reported here, process regulators were operationalized by the item stems that reflected contexts of anger, anxiety, sadness, indecisiveness, and financial distress. The caregivers’ use of personal and social resourcefulness skills in response to those five process regulators were compared across groups of caregivers of persons with various conditions.
Purpose and Research Question
Although resourcefulness has been studied in caregivers of persons with mental illness or dementia (Zauszniewski et al., 2009, 2016), comparisons on the use of specific personal and social resourcefulness skills have not been explored among caregivers of persons with various health conditions. Determining similarities and dissimilarities among caregivers of persons with various health conditions can facilitate tailoring of Resourcefulness Training© interventions to meet diverse caregiver needs and promote their health. This study examined patterns of responses of caregivers of persons with various health conditions to items focusing on anger, anxiety, sadness, indecisiveness, and financial distress to establish their use of personal and social resourcefulness skills. Accordingly, the research question was the following: “Do family caregivers of persons with various health conditions differ in their tendency to use personal and social resourcefulness skills with their responses to feelings of anger, anxiety, sadness, indecisiveness, and financial distress?” Data for this analysis were taken from an online caregiver studies that examined burden of care (Zauszniewski et al., 2020b) and mental health (Zauszniewski et al., 2020a), which was approved by the University Institutional Review Board following an expedited review.
Methods
Design and Sample
This descriptive secondary data analysis used data from a cross-sectional study from which a convenience sample of 234 family caregivers of adults was recruited through social media platforms that included Twitter and Facebook (Fox et al., 2020). Inclusion criteria for the parent study specified that the caregivers must be age 18 years and older, caregiving for a minimum of six months, and able to read and understand English. There was no specification for the care recipient’s health condition. However, the caregivers had to be providing care for their family member for at least three days per week. The type of care they may have provided was any of the following: bathing, dressing, grooming, toileting, transferring to chair or bed, walking, climbing stairs, eating, shopping, cooking, managing medications, using the phone, doing housework, doing laundry, helping with transportation, or managing finances. The parent study excluded parents/caregivers of children and formal/paid caregivers.
Detailed information regarding demographic characteristics of the sample are published elsewhere (Zauszniewski et al., 2020a) and only summarized here. Caregiver ages ranged from 23 to 79 years, with an average age of 54 years (SD = 10.59). The majority of the caregivers were women (95%), White Caucasian (88%), and married/partnered (73%). Approximately 51% had a college or graduate degree and 56% reported an annual income greater than $40,000, with 12% reporting an annual income exceeding $100,000.
The family caregivers were categorized by their care recipient’s health condition as in the parent study (Zauszniewski et al., 2020a). The nine categories alpha order were amyotrophic lateral sclerosis (ALS) (N = 20), cancer (all types) (N = 14), dementia (all types) (N = 43), mental illness (all types) (N = 10), multiple conditions (N = 79), other conditions (including broken limbs, infections, problems related to aging, etc.) (N = 21), Parkinson’s disease (N = 22), stroke (N = 12), and TBI (N = 13). Because the sample sizes across the 9 categories were unequal and some were small, their adequacy was limited to descriptive analyses (i.e., frequencies and percent) of the 10 resourcefulness items.
Measures and Data Collection
For this secondary analysis, data obtained on the Resourcefulness Scale© from the 234 family caregivers who took part in the parent study (Zauszniewski et al., 2020a) were used. Although the Resourcefulness Scale© (Zauszniewski et al., 2006) consists of 28 items on a 6-point Likert Scale, to which respondents indicate the degree to which an item is characteristic of them; this analysis only used the data on 10 of its items. The 28-item Resourcefulness Scale© captures two dimensions of resourcefulness: personal (16 items) and social (12 items). The Resourcefulness Scale© has been reported as reliable and valid with an internal consistency estimate of Cronbach’s alpha = .83 and construct validity indicated by confirmatory factor analysis verifying the presence of two subscales reflecting personal and social resourcefulness, which were moderately correlated (r = .41, p < .001) (Zauszniewski et al., 2006). The Cronbach’s alpha for the 10 items used in this analysis = .70.
The Resourcefulness Scale© is constructed with an item stem to provide a context (e.g., anger, anxiety, sadness, indecisiveness, or financial distress) for use of a particular resourcefulness skill, and a response that describes either a personal (i.e., self-help) or social (i.e., help-seeking) resourcefulness skill. For this analysis, five items in which the item stems reflected similar contexts (i.e., anger, anxiety, sadness, indecisiveness, and financial distress) were selected from each subscale, totaling 10 items. For example, two item stems put the respondent in the situation of being anxious with many things to do. The response for the personal resourcefulness item indicates independently planning what needs to be done while the response to the social resourcefulness item reflects asking for others’ help.
To facilitate making comparisons across the nine caregiver groups, the item responses were collapsed from the original 6-Likert alternatives into dichotomous categories reflecting whether the use of a specific personal or social resourcefulness skill was characteristic or not characteristic of the respondent. Thus, each caregiver respondent was coded on each of the 10 items as if using the personal or social resourcefulness skill was like them or not like them and it could be determined whether they used one or the other skill, or neither or both of them.
Data Analysis
Caregivers across these nine health conditions were compared in their use of resourcefulness skills in relation to anger, anxiety, sadness, indecisiveness, and financial distress. Using frequencies and percent, we aimed to determine whether differences existed across the nine caregiver groups in their use of personal resourcefulness, social resourcefulness, both forms of resourcefulness, or neither form of resourcefulness in response to the five contexts. However, the unequal sample sizes among the nine caregiver groups precluded the performance of tests of statistical significance. Thus, the findings would be informative for providing future direction for comparative and experimental studies of family caregivers that may lead to the tailoring future Resourcefulness Training© interventions.
Results
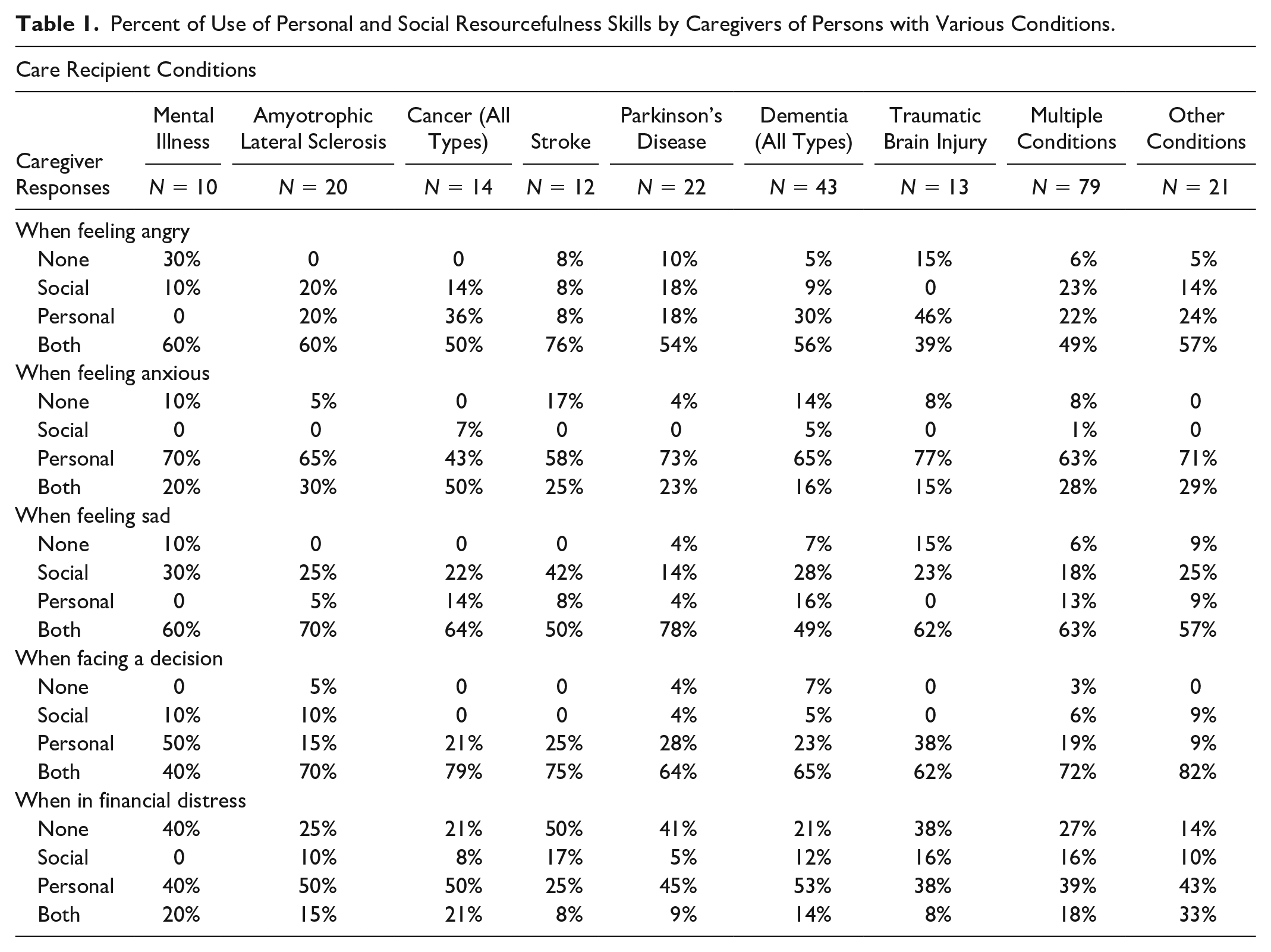
Table 1 displays the percent of family caregivers within the nine health conditions categories by care recipient condition who reported the use of both personal and social resourcefulness skills, either personal or social resourcefulness skills, or neither the personal or social resourcefulness skills when feeling angry, anxious, sad, indecisive, and financially distressed. The results are reported for each of these five contexts.
Percent of Use of Personal and Social Resourcefulness Skills by Caregivers of Persons with Various Conditions.
Family Caregiver Responses to Anger
The tendency to use both personal and social resourcefulness skills was found for family caregivers of persons with amyotrophic lateral sclerosis or cancer; none of them reported not using the personal or social resourcefulness skills. In fact, with the exception of caregivers of persons with TBI, there was a pattern across the other caregiver groups toward using both personal and social resourcefulness skills for anger management (49%–79%). Caregivers of persons with TBI tended to use personal resourcefulness (46%) while none in this category gravitated toward using social resourcefulness. In comparison with the other groups, the greatest percent of family caregivers of persons with mental illness (30%) reported they did not use either personal or social resourcefulness skills to deal with anger. In addition, no caregivers in this category reported using personal resourcefulness skills.
Family Caregiver Responses to Anxiety
There were no family caregivers of persons with cancer or other conditions who reported using neither the personal or social resourcefulness skills when experiencing anxiety. With the exception of caregivers of persons with cancer, who were inclined to use both personal and social resourcefulness skills (50%), the other caregiver groups reported using personal (58%–77%) rather than social resourcefulness skills (<7%). In fact, there were no family caregivers of persons with mental illness, amyotrophic lateral sclerosis, stroke, Parkinson’s disease, TBI, or other conditions, who reported using social resourcefulness skills when feeling anxious.
Family Caregiver Responses to Sadness
Interestingly, there was a pattern across all nine caregiver groups for using both personal and social resourcefulness skills with response to feelings of sadness (49%–78%). For three groups of family caregivers, including caregivers of persons with amyotrophic lateral sclerosis, cancer, and stroke, none reported using the personal or social resourcefulness skills. No family caregivers of persons with mental illness or TBI reported using personal resourcefulness skills. In fact, across all nine groups of family caregivers, the percent use (14%–42%) of social resourcefulness skills exceeded the percent use of personal resourcefulness skills when experiencing feelings of sadness.
Family Caregiver Responses to Indecisiveness
In response to making a decision, there were no family caregivers of persons with mental illness, cancer, stroke, TBI, or other conditions who said they did not use at least one of the two forms of resourcefulness. In addition, no family caregivers of persons with cancer, stroke, or TBI reported using social resourcefulness skills when faced with decision-making. With the exception of caregivers of persons with mental illness who gravitated toward use of personal resourcefulness skills (50%), the greatest percent (62%–82%) of family caregivers across the other eight groups reported they used both the personal and social resourcefulness followed by using personal resourcefulness (9%–38%) more frequently than social resourcefulness skills to overcome indecisiveness.
Family Caregiver Responses to Financial Distress
With the exception of family caregivers of persons with stroke in which the largest percent (50%) reported using neither personal nor social resourcefulness skills, a greater percent of caregivers in the remaining eight categories defined by their care recipient’s condition, reported using personal resourcefulness skills (25%–53%) in comparison with social resourcefulness skills when experiencing financial distress. In comparison with the other four contexts (anger, anxiety, sadness, indecisiveness, and financial distress), family caregivers across all nine groups had the largest percent (14%–50%) reporting they did not use either the personal or social skills constituting resourcefulness.
Discussion
This study examined similarities and differences in the use of resourcefulness skills used by family caregivers of persons with various health conditions. The personal and social skills constituting resourcefulness have been defined within the midrange theory of Resourcefulness and Quality of Life© (Zauszniewski, 2018). Within that theory, process regulators provide a context that influences one’s use of personal or social resourcefulness skills. In this study, process regulators consisted of anger, anxiety, sadness, indecisiveness, and financial distress.
The findings indicated that while family caregivers of persons with various conditions have some commonalities in their use of personal and social resourcefulness skills in response to feeling angry, anxious, or sad, or when faced with decision-making or financial distress, there are also some differences. Critical examination of those similarities and differences is important for moving forward with future research that will lead to the tailoring interventions to meet the caregivers’ needs and contexts. Indeed, research has shown that persons who use both the personal and social skills constituting resourcefulness have the best health outcomes (Zauszniewski, 1996). Thus, if it is known that family caregivers of persons with a specific condition or facing a particular situation have a tendency to not use social resourcefulness skills (i.e., not seek help from family, friends, or professionals), these skills might be emphasized more strongly during Resourcefulness Training©.
The study findings showed that the majority of family caregivers of persons with various health conditions had a tendency to use both personal (self-help) and social (help-seeking) resourcefulness skills when experiencing anger, sadness, and indecisiveness. Few studies have examined coping strategies used by family caregivers to manage anger. Studies examining family caregiver experience of sadness or depression and decision-making are more abundant. However, no studies were found that examined the simultaneous use of self-help and help-seeking skills for caregiver management of feelings of anger or sadness or when making a decision.
Seeking help in the form of social support groups has been reported as a beneficial way for family caregivers to express anger and share management strategies (Diehl et al., 2003; DuBenske et al., 2014). Likewise, social support groups have been found to reduce depressive symptoms in family caregivers of persons with heart failure, dementia, and physical disabilities (Barutcu & Mert, 2016; Chu et al., 2011; Zhong et al., 2020). In other caregiver research, anger arising from the caregiving situation was mediated by the caregiver’s personal resources, including self-efficacy and emotion-focused coping (Crespo & Fernández-Lansac, 2013). In addition, interventions that include self-help strategies similar to those constituting personal resourcefulness (e.g., positive self-talk, emotion regulation, and self-monitoring) were found to be effective for managing anger and depression (Coon et al., 2003).
Research indicates that family caregiver decision-making is a complex process that requires the use of both self-help and help-seeking behaviors. Caregivers of persons with dementia have expressed the need for support from both health professionals and experienced family caregivers in order to make better decisions for themselves and their care recipient (Truglio-Londrigan & Slyer, 2019). Caregivers of persons with TBI have also identified the need for outside help with decision-making (Knox et al., 2016). However, family caregivers characterized as vigilant decision-makers (i.e., those who consider alternatives, collect information, and weigh alternatives) have had better caregiver outcomes than those less vigilant (Wackerbarth & Tarasenko, 2018). Thus, the study reported here is the first to highlight the tendency of the majority of family caregivers of persons with various conditions to use both self-help and help-seeking skills, which constitute personal and social resourcefulness, for managing feelings of anger and sadness and when making a decision.
The study findings also indicated a tendency across all caregiver groups toward less frequent use of help-seeking skills than self-help skills when confronted with feelings anger, anxiety, indecisiveness, or financial distress. This finding may be explained by research that has identified an association between difficulties or delays in seeking help with caregiver worry and self-criticism. That is, caregivers tend to internalize their caregiving situation, viewing it as their responsibility, even though it may be beyond their control. They experience tension associated with decision-making, conflicting emotions, including anger and frustration, and concern about financial hardship, all of which have been found to correlate with avoidance of help-seeking in dementia caregivers (Ng et al., 2021).
In addition, research with caregivers of persons with cancer has shown that more than one-third have alexithymia, that is, a difficulty in describing their emotions and feelings, and high alexithymia has been associated with low help-seeking (Hasuo et al., 2020). However, our findings also showed a tendency for most caregiver groups to use help-seeking as well as self-help strategies when experiencing sadness. Indeed, the protective effects of social support for caregiver mental health have been well documented. Similar to help-seeking behavior, seeking social support, including affectionate support, emotional/informational support, and positive social interaction and participation have been associated with fewer depressive symptoms in caregivers of persons with various conditions (Sibalija et al., 2018).
Finally, this study revealed a proclivity toward use of personal resourcefulness (self-help) rather than social resourcefulness (help-seeking) skills across most caregiver groups when faced with anxiety or financial distress. Consistent with our findings, Tschanz et al. (2013) reported that dementia caregivers predominately used intrapersonal coping strategies and sought social support only rarely to sometimes, indicating their preference for personal rather than social resourcefulness. While informative, this distinction may not adequately address the distinction between personal and social resourcefulness, as the latter includes seeking emotional support and tangible counsel or assistance.
Personal financial strain has been identified as a relevant stressor across diverse caregiving context, including late-life frailty (Kang, 2020), dementia (Liu et al., 2019), cancer (Thomas et al., 2019) and TBI (Sabella & Suchan, 2019). Yet, there is limited empirical research to support a tendency for use of personal rather than social resourcefulness. Casado (2008) examined a diverse sample of caregivers and found that the sense of need for financial support, and subsequent willingness to seek assistance, was more strongly associated with caregiver-related factors than care-recipient factors, including type of chronic condition. Lee and Zurlo (2014) showed that positive social support significantly lessens the experience of financial strain, but relative to social resourcefulness, their study did not examine whether or how that support was solicited.
Generalizability of the study’s findings is limited by several factors. As a secondary data analysis of existing data, the recruitment of the family caregivers was beyond the researcher’s control. Convenience sampling and the use of online recruitment and data collection may have produced a biased sample of family caregivers. In addition, the data analyses were limited by the unequal numbers of family caregivers across the various recipient conditions. As the sample sizes for some of the health conditions were small, this prohibited the use of more advanced statistic beyond frequencies. Future studies should target increasing the samples of condition groups that were smaller in the current convenient sample. Additional subjects would allow the use of chi squares to explore further the caregiver responses differences among the care recipient conditions.
Although data were available within the existing dataset on the measures of personal and social resourcefulness regarding the five specific contexts, the items did not force the caregivers to choose one or the other skill (i.e., personal or social resourcefulness) for a given context. However, allowing the family caregivers to respond separately to one item capturing use of personal resourcefulness and another capturing use of social resourcefulness, enabled us to evaluate their interchangeable use of either the personal or social resourcefulness skills. Although forcing the caregivers to choose between the personal and social resourcefulness skills may have been informative, it would have been inconsistent with seminal research findings that suggest the importance of using both sets of skills (Zauszniewski, 1996).
Yet, this was the first study to compare family caregivers of person with various conditions on their use of personal and social resourcefulness skills in coping with commonly occurring emotions, such as anger, anxiety, and sadness, and in managing decision-making and financial distress. As such, the findings are foundational for future research to compare the use of resourcefulness skills in equal samples of caregivers of persons with various health conditions in which tests of significance can be performed, which may inform future development and tailoring of Resourcefulness Training© interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the Frances Payne Bolton School of Nursing research fund to Dr Jaclene A. Zauszniewski.