
Abstract
Guided by Individual and Family Self-Management Theory, the purpose of this cross-sectional study was to describe patient care activities that family caregivers endorsed and performed while visiting their family member in the ICU. We found that caregivers wanted to be involved in ICU patient care and had preferences for the care they wanted to perform with their critically ill family member. More than 80% preferred to perform tasks related to daily grooming, communication, and education. Of note, many caregivers expressed interest in holistic healing activities (i.e., music and art), and yet, less than 50% of caregivers reported participating in these activities. The discrepancy between the number of care activities that respondents desired to perform compared to the number of care activities they reported performing represents an important opportunity to shift research and practice improvement efforts toward more tailored family engagement interventions and recognition of family caregivers as essential partners in care.
Intensive care unit (ICU) survivors require ongoing support throughout their recovery from critical illness. Family caregivers of ICU survivors assume considerable caregiving responsibilities that can have persistent negative effects on their health and overall quality of life, which in turn, can impact their ability to support their family member (Cameron et al., 2016; Choi et al., 2011; Douglas & Daly, 2003; Hickman & Douglas, 2010). Actively involving caregivers in direct patient care at the bedside early in the ICU experience has the potential to improve both patient and caregiver outcomes (Burns et al., 2018; Choi et al., 2016, 2018). Current critical care practice guidelines call for actively engaging family caregivers in bedside care; however, few evidence-based strategies exist to operationalize this recommendation (Brown et al., 2015; Davidson et al., 2017; Olding et al., 2016). The purpose of this study was to explore caregivers’ preferences for participation in patient care as well as their actual contributions to patient care while visiting their family member in ICU. The results from this study add to a growing body of literature that highlights the importance of evaluating individual family caregiver characteristics and preferences to support their safe and effective participation in direct patient care in the ICU (Brown et al., 2015; Mitchell et al., 2016; Olding et al., 2016; van Beusekom et al., 2016).
Family Caregiver Participation in Patient Care in the ICU
Approximately 5.7 million critically ill patients are admitted to ICUs each year in the United States (SCCM, 2021). Advancements in clinical treatments and technological interventions have decreased inhospital mortality rates for ICU patients by 50% in the past 25 years. Currently, approximately 80% of patients survive their ICU experience (Brinkman et al., 2013; Kasza et al., 2013). The majority of patients who survive a critical illness require significant help with activities of daily living and depend on family caregivers for support. While family caregivers have identified positive aspects of their ICU caregiving experience (Tate & Choi, 2020), they are often unprepared to assume burdensome caregiving responsibilities after the patient returns home (Choi et al., 2018; Levine & Reinhard, 2016; Stayt & Venes, 2019). Ongoing caregiving responsibilities can have persistent negative effects on caregivers’ quality of life (Cameron et al., 2016; Choi et al., 2011; Douglas & Daly, 2003; Hickman & Douglas, 2010). Notably, caregivers of ICU patients experience symptoms of anxiety (15%–24%), depression (5%–36%), and posttraumatic stress disorder (PTSD) (35%–57%). They also report fatigue and difficulty sleeping. This sequela of symptoms has been termed Post Intensive Care Syndrome-Family (PICS-F) (Davidson & Harvey, 2016; van Beusekom et al., 2016). PICS-F can have a negative impact on a caregiver’s quality of life and their ability to support an ICU survivor (Cameron et al., 2016; Choi et al., 2011; Davidson & Harvey, 2016; Douglas & Daly, 2003; Hickman & Douglas, 2010).
There is emerging evidence that negative physical and psychosocial caregiving consequences can be mitigated by actively engaging caregivers in the ICU experience early on in their caregiving trajectory (Burns et al., 2018; Choi et al., 2016, 2018). The ICU admission is an optimal time to begin to prepare caregivers for future caregiving roles. Caregivers want to be actively involved in patient care in the ICU; however, there is a paucity of literature on family caregiver preferences for how they would like to contribute to their family member’s care (Wong et al., 2020, 2021). Current ICU practice involves passive forms of family caregiver engagement in patient care such as the health care team sharing information about the patient with the family and eliciting information about the patient, involving family in decisions about the patient’s treatment options, and promoting family presence at the bedside (Brown et al., 2015; Davidson et al., 2017; Olding et al., 2016). A growing body of research suggests that active involvement in patient care has the potential to improve long-term caregiver outcomes, as well as patient outcomes (Brown et al., 2015; Cameron et al., 2016; Mitchell et al., 2016; Olding et al., 2016; van Beusekom et al., 2016).
ICU nurses have limited evidence-based strategies to promote appropriate, individualized caregiver participation in bedside care. Research to inform evidence-based strategies is limited as few studies have examined family perspectives about involvement in ICU patient care or explored specific activities actually performed by family caregivers (Brown et al., 2015; Olding et al., 2016). Assessing family experiences in direct care and their preferences is a first step toward developing tailored interventions for involving family in patient care. Therefore, the purpose of this study was to explore caregivers’ preferences for participation in patient care as well as their actual contributions to patient care while visiting their family member in ICU. We also describe the relationships among demographic, psychological, clinical factors, and caregiving behaviors.
Theoretical Framework
The study was guided by selected elements of Sawin & Ryan’s Individual and Family Self-Management Theory (IFSMT) (Ryan & Sawin, 2009). Family includes anyone who provides the majority of physical, emotional, and/or financial support to a patient, regardless of biological or legal relationship (Ryan & Sawin, 2009; Tate & Choi, 2020). Self-management is a purposeful incorporation of health-related behaviors into a family’s daily life. In the ICU, family caregivers assume responsibility for caring for their critically ill family member in collaboration with clinicians. There are contextual factors that may influence caregiver health-related behaviors and their ability and desire to participate in ICU patient care. These contextual factors may include the complexity of patient care, their ability to be present, and their perspectives about care. In this study, contextual factors include caregivers’ demographics, preferences for involvement, and psychological health (global health and well-being and acute stress) as well as the clinical characteristics of the patient. These contextual factors influence family caregiving behaviors (proximal outcomes), such as their readiness and capacity to participate in caregiving activities (Figure 1).
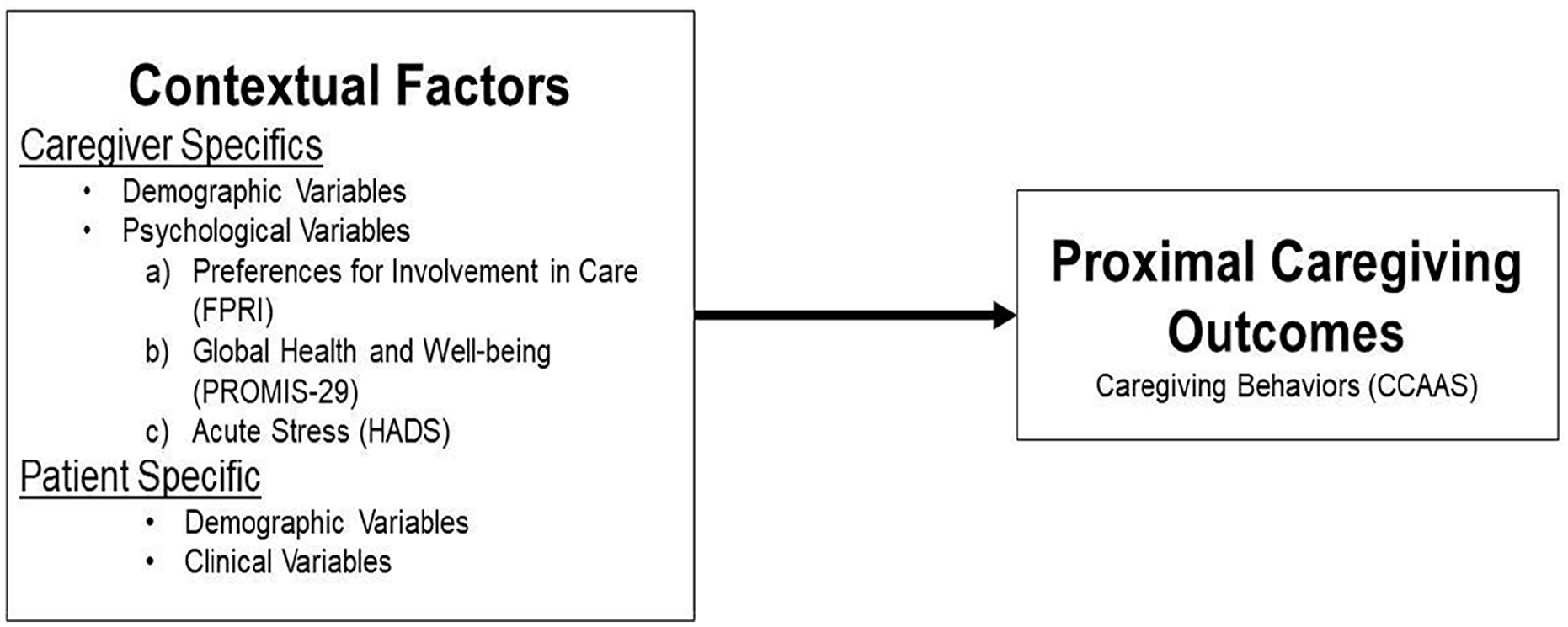
Conceptual model.
Methods
Design and Sample
This descriptive study used a cross-sectional, correlational research design. The study was approved by the Institutional Review Board at the University of Nebraska Medical Center. A convenience sample of ICU family caregivers and the patients they cared for who were admitted to any of the six adult or pediatric ICUs were recruited from a large tertiary medical center located in Omaha, NE. The medical center endorses 24 hour open visitation, but specific family engagement practices vary between units and clinicians, and there are no definite ICU family engagement policies. Data were collected from November 2017 to July 2018. Individuals who were at least 19 years of age or older, able to understand and speak English, present at the bedside during time of enrollment, and identified by the bedside nurse as a primary caregiver for an adult or pediatric ICU patient were asked to participate. Individuals were excluded if they had a preexisting neurocognitive impairment (as reported by the bedside nurse) or profound vision or hearing loss that would preclude variable measurement.
Measures
Caregiver demographic variables
Caregiver demographic variables were collected using an investigator developed 17-item instrument that assessed demographic characteristics of the caregiver including age, sex, race/ethnicity, marital status, relationship to the patient, employment status, and previous caregiving experiences.
Caregiver psychological variables
Caregiver psychological variables included preferences for involvement in care, global health and well-being, and acute stress. They were assessed using the Family Preferences Index (FPRI) (Li, 2002), PROMIS-29 (Hays et al., 2009; Schnall et al., 2017), and Hospital Anxiety and Depression Scale (HADS) (Mykletun et al., 2001). The FPRI is a 14-item instrument that measures the caregiver’s personal choice about providing care to the hospitalized patient. A total score is calculated. Given the construction of this measure, reliability statistics cannot be calculated, but it has sufficient construct validity (Li, 2002). The PROMIS-29 is a 29-item health related quality of life instrument, which includes four items on seven domains (physical function, anxiety, depression, fatigue, sleep disturbance, ability to participate in social roles and activities, and pain interference) as well as a 0–10 numeric rating pain intensity scale. Scores on each domain are population normed on a T-score metric with mean of 50 and standard deviation of 10. It has a reported Cronbach’s alpha of 0.87 to 0.97 (Schnall et al., 2017). The HADS contains 14-items and two subscales (anxiety and depression). Each item is ranked on a 0–3 Likert scale. Subscale score ranges are 0–21; 0–7 = normal; 8–10 = borderline; scores of 11 or greater are considered moderate to severe anxiety/depression. It has a subscale variance of 24%–36% and Cronbach’s alpha of 0.73 to 0.85 (Mykletun et al., 2001).
Proximal caregiving behaviors
Proximal caregiving outcomes were assessed using the Caregiver Care Activities Assessment Scale (CCAAS), which was developed by the investigators (Hetland et al., 2017). We specified caregiver behaviors using a list of 27 common ICU patient care activities that a nurse may offer a caregiver to perform. To enhance content validity, five current ICU nurses were consulted to review the appropriateness patient care activities listed on the CCAAS. The instrument assesses that (a) whether the caregiver would prefer to perform the care by themselves or would they prefer the nurse perform the care; (b) whether the caregiver has performed the care during their loved one’s ICU stay; if so, how often, if not, their level of comfort with the care if asked to perform it by nursing staff.
Patient demographic and clinical variables
Clinically relevant patient variables were abstracted from the patients’ electronic medical records (EMRs) using an investigator developed patient demographic form, which assess demographic and clinical characteristics of the patient. Severity of illness was measured using the Acute Physiology, Age, Chronic Health Evaluation (APACHE) III score and the Carlson Comorbidity Index using EMR data from the 24 hours prior to study enrollment. Mental status was measured using the Glasgow Coma Scale. Sedative exposure is a method for aggregating sedative and opioid medication doses from disparate drug classes commonly administered to critically ill patient (Tracy et al., 2019). For this study, it was operationalized as a sedation intensity score and sedative dose frequency for the 24-hour period prior to study enrollment. We used a standardized chart review method to measure the number of lines, tubes, and equipment for each patient. To assure the reliability of the abstracted EMR data, 25% of the cases were assessed for interrater reliability.
Procedures
Advertisements about the study were posted in waiting rooms designated for family caregivers of ICU patients. Also, information about the study was disseminated among ICU nursing staff. ICU nurses were asked to provide a postcard with study information to all caregivers at the bedside. These postcards were also available in the designated ICU family waiting areas. With these recruitment mechanisms, caregivers were asked to contact the principal investigator directly via telephone if interested in participating. In addition, research assistants with ethical access made daily rounds in the ICUs to identify available caregivers. If the caregiver was interested in participating, trained research assistants sought written informed consent in a quiet private space. Data were collected via a face-to-face interview by trained research assistants at a single time point during a patient’s admission to the ICU. Data collection took approximately 30 to 45 minutes to complete. To compensate for time spent, each subject received a $5 hospital meal ticket for participating.
Data Analysis
The measures and patient information collected were entered directly into REDCap. Prior to analysis, data were exported into SPSS Version 25, where the measures were scored, and descriptive statistics were calculated on all study outcomes. Comparisons of mean scores on proximal caregiving outcomes across categorical caregiver variables were made using analysis of variance (ANOVA) models with Tukey tests for paired comparisons. Spearman correlations were utilized for testing associations between continuous caregiver variables and caregiving behaviors. An a priori p-value of .05 was used to indicate significance.
Results
Sample Characteristics
Demographic, psychological, and clinical characteristics of the 127 enrolled caregiver-patient dyads are described in Tables 1–3. Participants were enrolled an average of 6.1 days (SD = 8.7; range = 0 to 62) days after patient admission to the ICU. Caregivers had a mean age of 51.8 (SD = 15.6), the majority of which were White (82.7%) and female (77.2%). The patients’ average Apache III score was 45.9 (SD = 22.5), and there was a range of 2–14 lines or tubes present (Mean = 6.9, SD = 2.8). The average Sedation Frequency score was 14.6 (SD = 17.9), and Sedation Intensity had an average of 11.3 (SD = 14).
Caregiver Demographic Variables (N = 127) a .
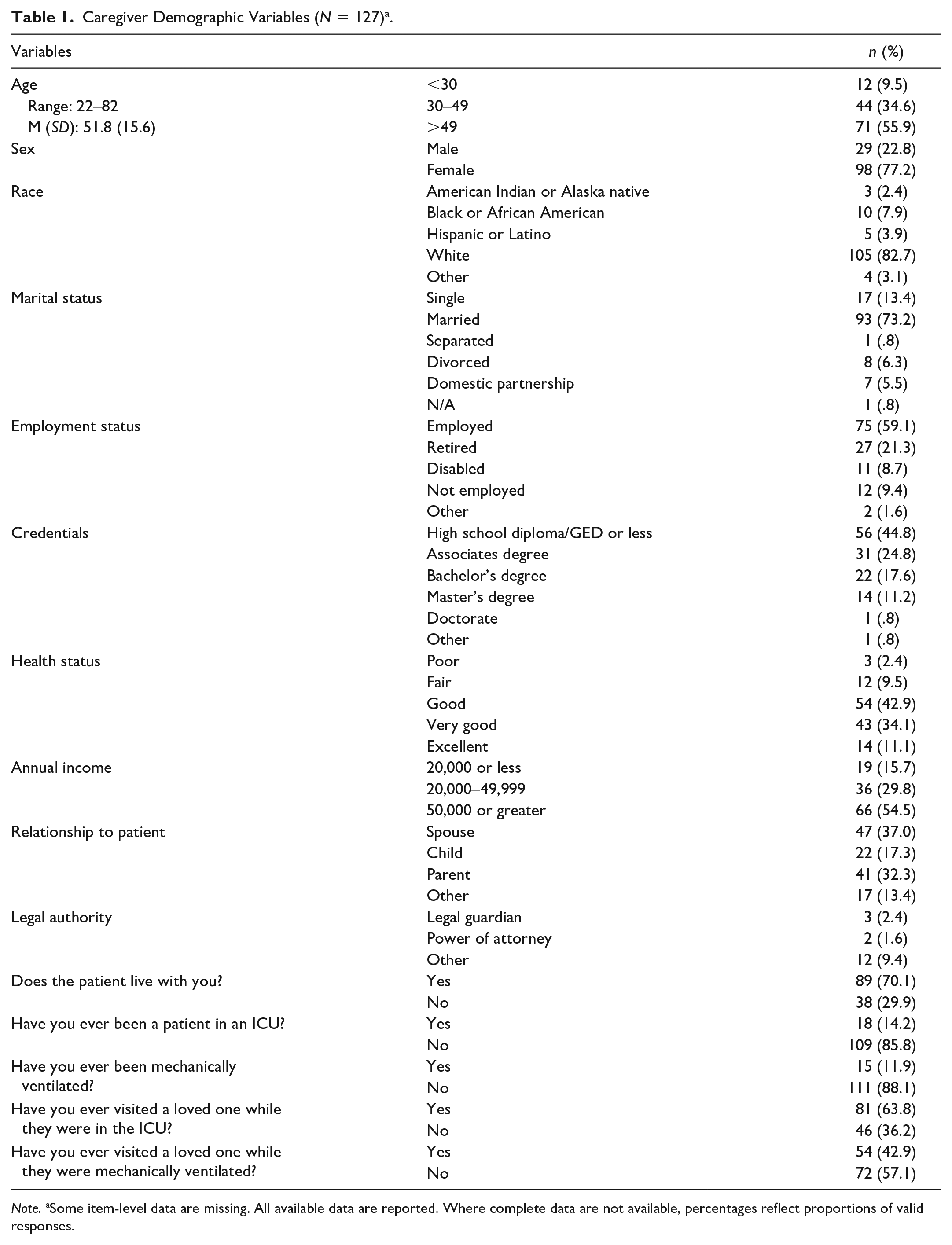
Note. aSome item-level data are missing. All available data are reported. Where complete data are not available, percentages reflect proportions of valid responses.
Caregiver Psychological Variables (N = 127) a .
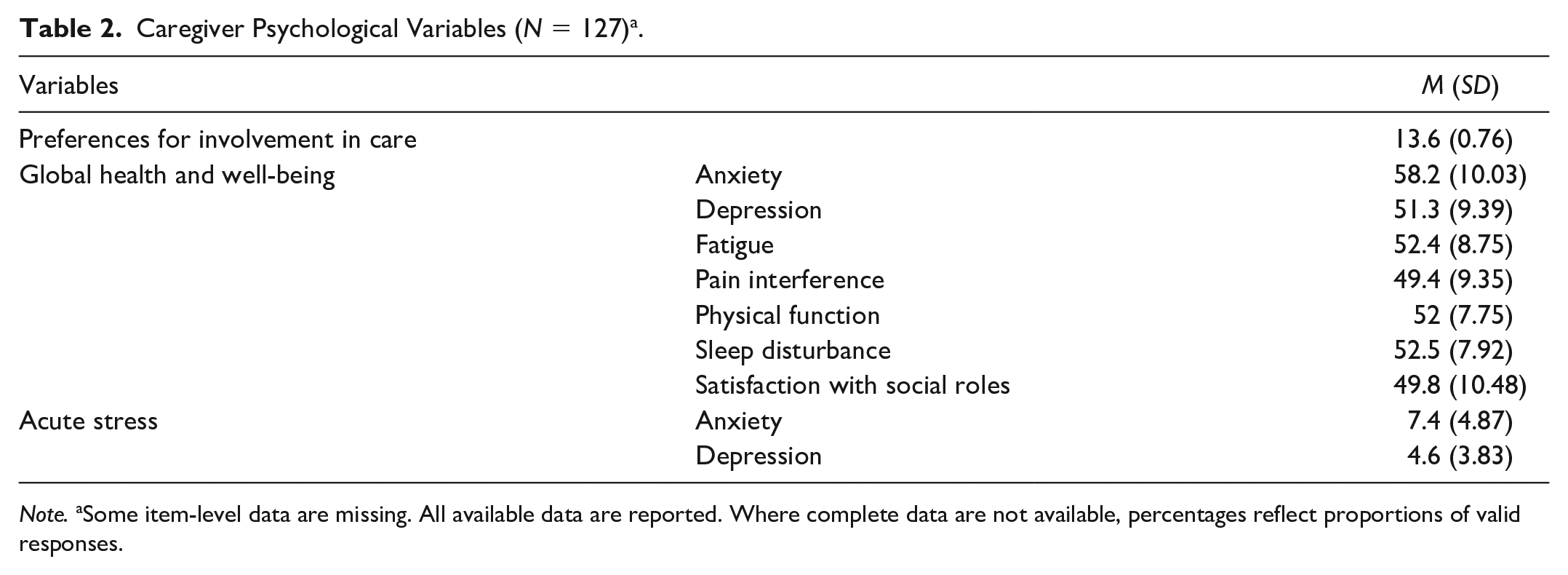
Note. aSome item-level data are missing. All available data are reported. Where complete data are not available, percentages reflect proportions of valid responses.
Patient Demographic and Clinical Variables (N = 127) a .
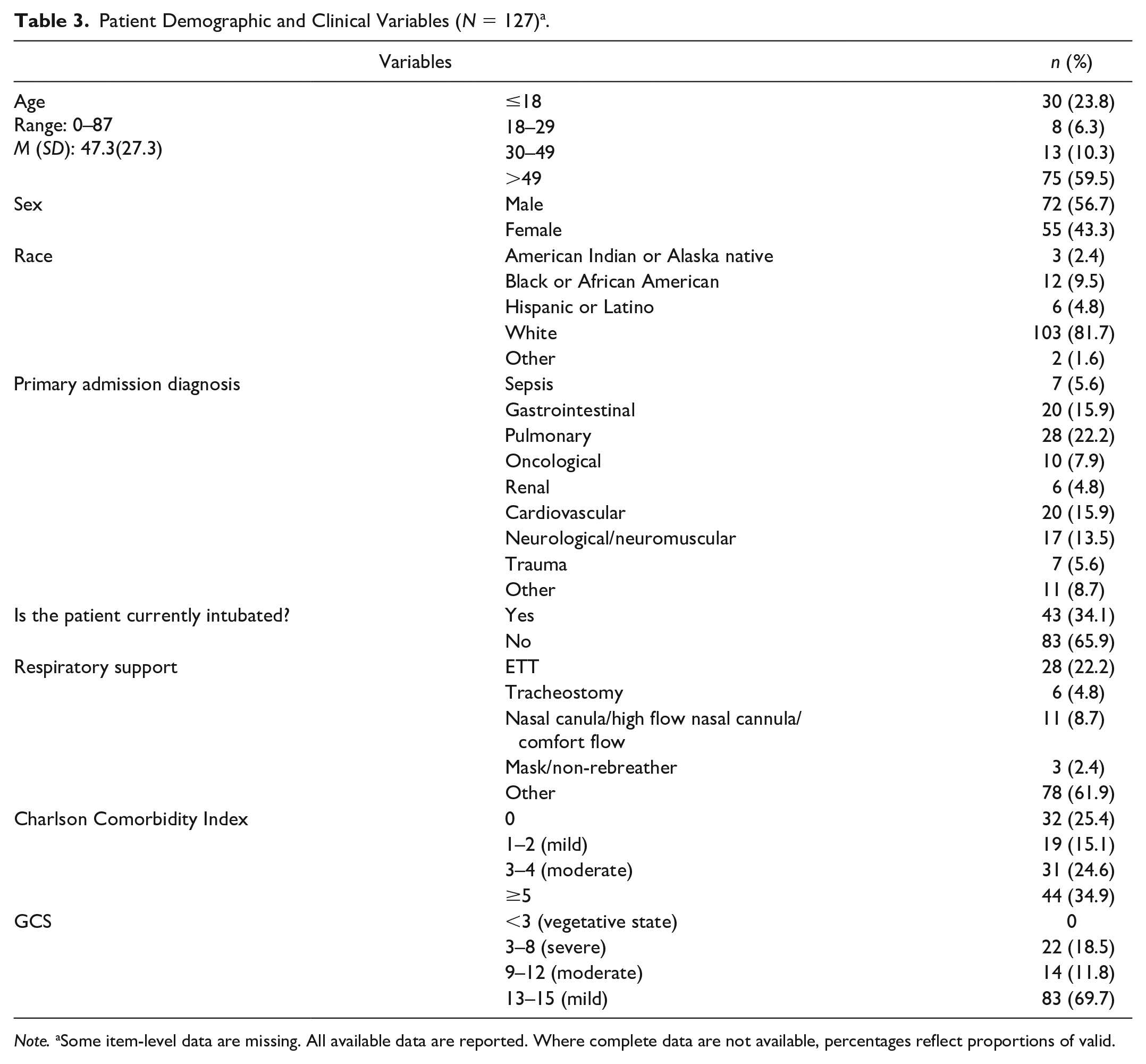
Note. aSome item-level data are missing. All available data are reported. Where complete data are not available, percentages reflect proportions of valid.
Caregiving Behaviors
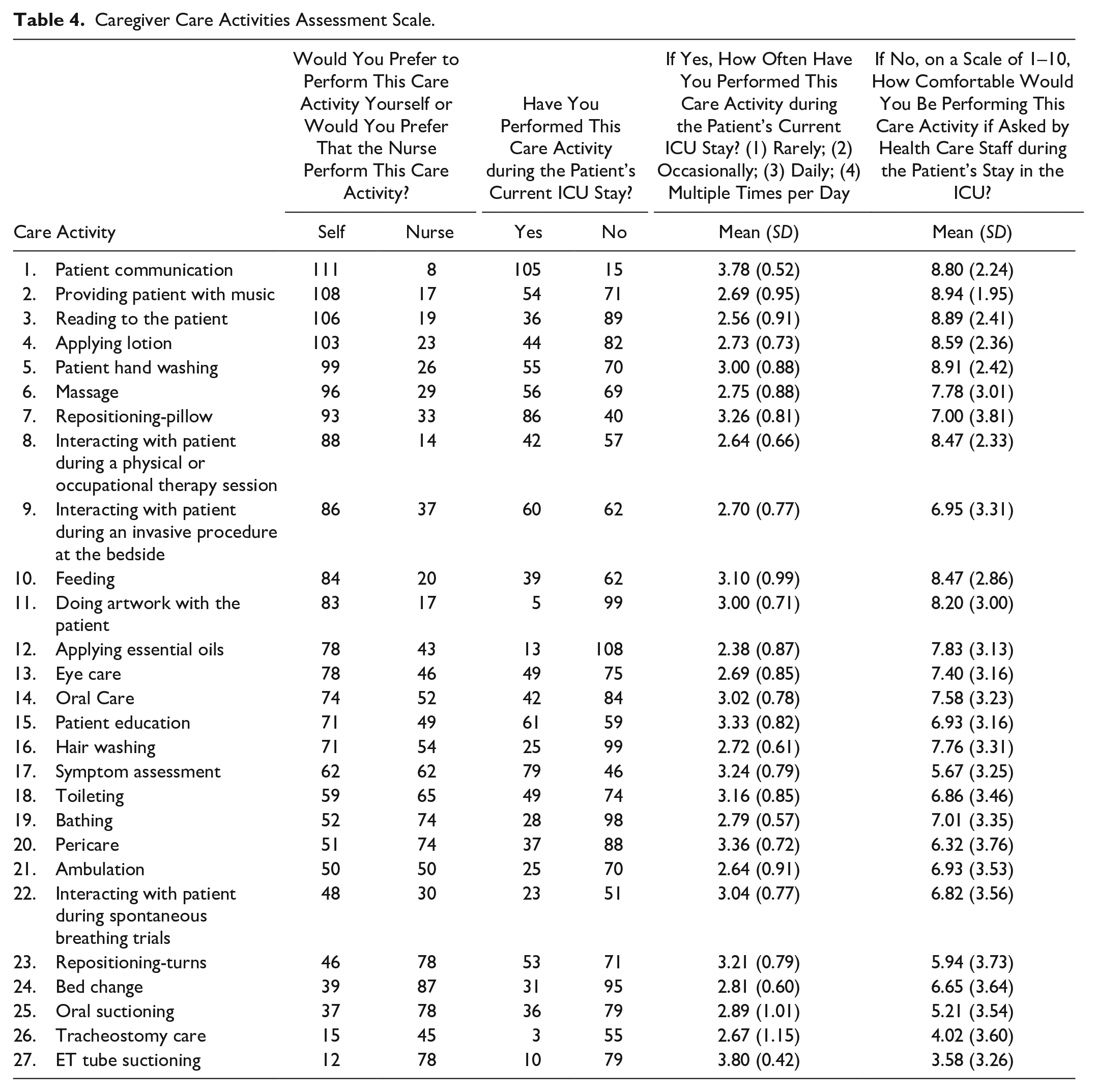
Preferences and frequency of performing the 27 care activities described in the Caregiver Activities Assessment Scale are shown in Table 4, sorted based on the most preferred actions. The activities caregivers most preferred to perform themselves are patient communication (93%), providing music (86%), and reading to the patient (85%); least preferred activities are oral suctioning (32%), tracheostomy care (25%), and ET tube suctioning (13%). Figure 2 presents activities ordered by the widest deviation between preferred and performed activities. Although 108 caregivers preferred to provide music to the patient, only 54 performed the activity. Of the 106 caregivers that preferred to read to the patient, only 36 performed the activity. The largest difference is seen in preference for doing artwork with the patient. Artwork was performed by only 5 caregivers out of the 83 that expressed interest in doing so.
Caregiver Care Activities Assessment Scale.
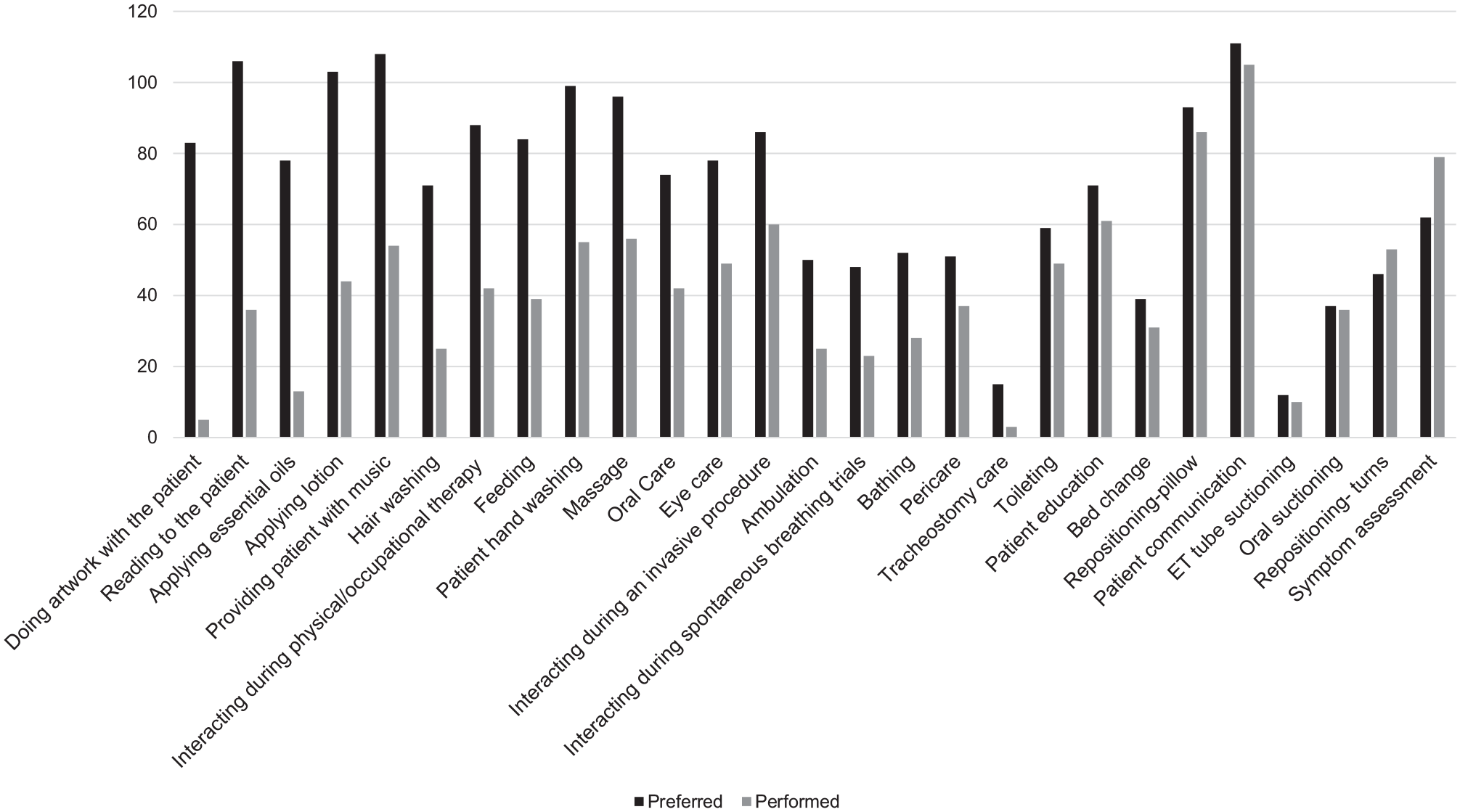
Caregiver preference of care activities to perform versus care activities actually performed in the ICU.
Relationships among Caregiver Demographic Psychological Variables, Clinical Variables, and Caregiving Behaviors
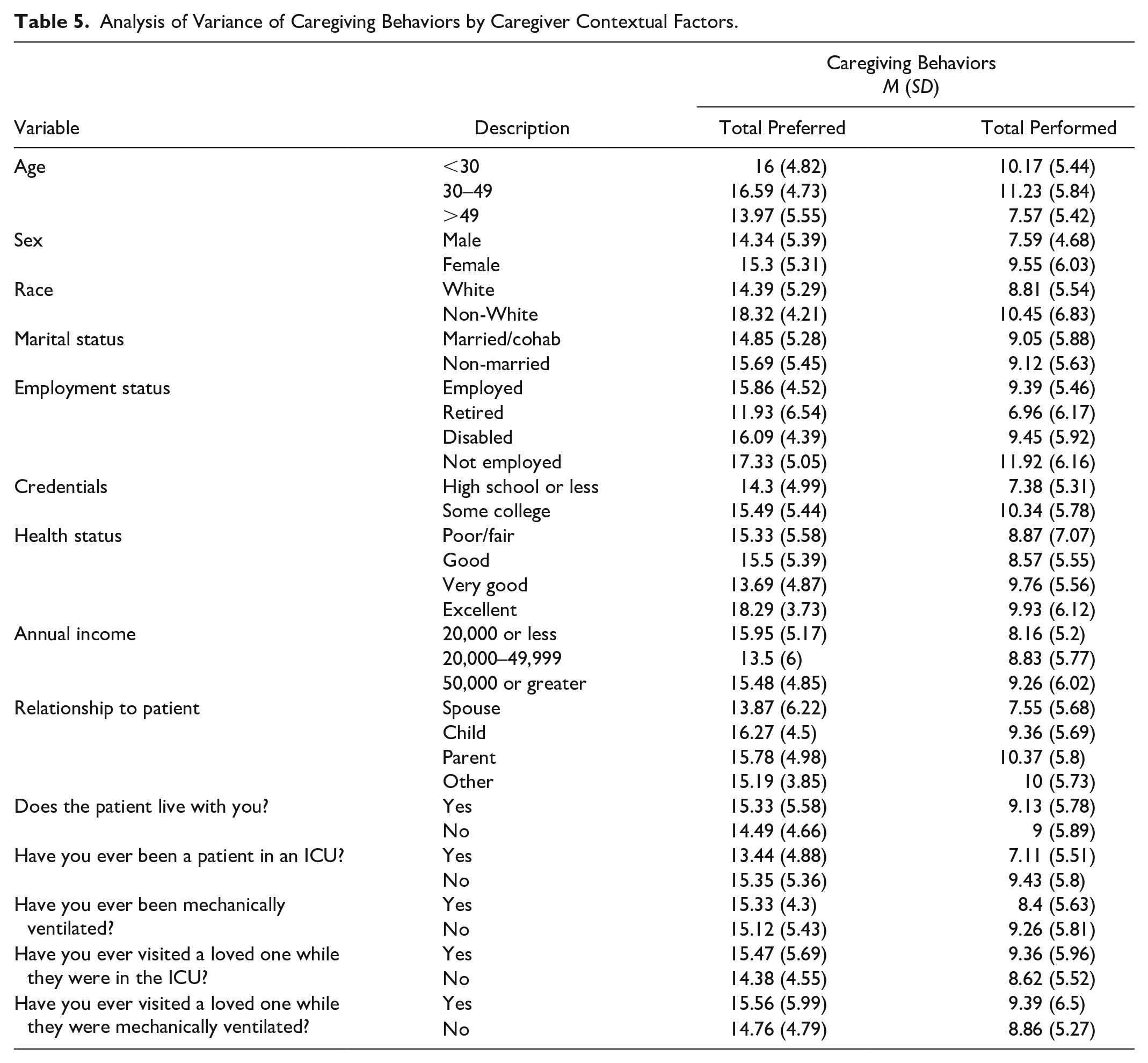
Tables 5 and 6 present relationships among caregiver contextual factors and caregiving behaviors (total preferred and performed activities). ANOVA models found caregiver age to be a significant predictor of caregiving behaviors, with those in the 30 to 49 age range having significantly higher total preferred (p = .027) and performed activities (p = .003) than those that are 50 and older. Race was a significant factor in total preferred activities with non-White caregivers preferring to perform significantly more activities than White caregivers (p = .001). Caregivers that were either employed or unemployed had significantly higher preference totals than retired caregivers (p = .004 and .014, respectively). Although no difference was found in preferences based on caregiver education, those with a college degree did perform more activities than caregivers without a degree (p = .004). Health status of the caregiver was found to influence preferences (p = .033), with those in excellent health having the highest number of preferred activities. The FPRI was found to have a small, but positive correlation with total preferred activities (r = .186, p = .037), while measures of caregiver mental health did not have any significant correlations with total preferred care activities.
Analysis of Variance of Caregiving Behaviors by Caregiver Contextual Factors.
Correlations between Caregiver Contextual Factors and Caregiving Behaviors.
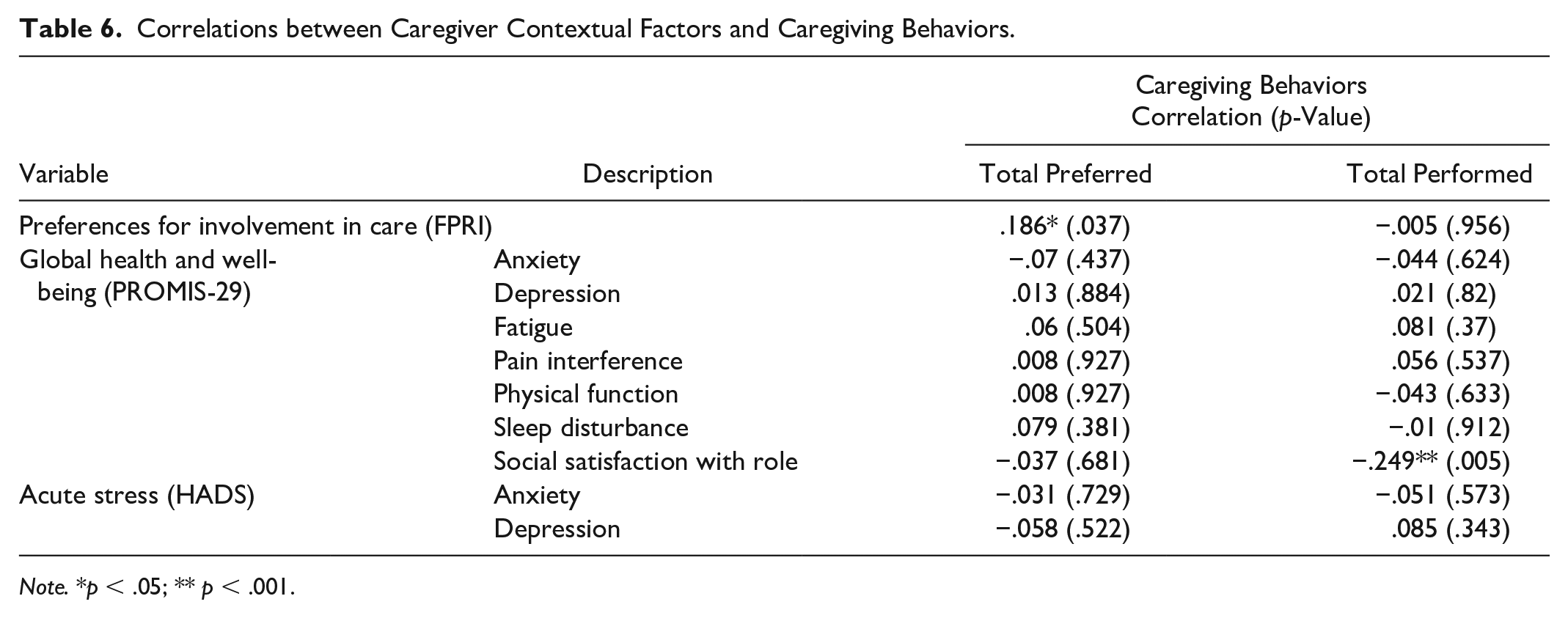
Note. *p < .05; ** p < .001.
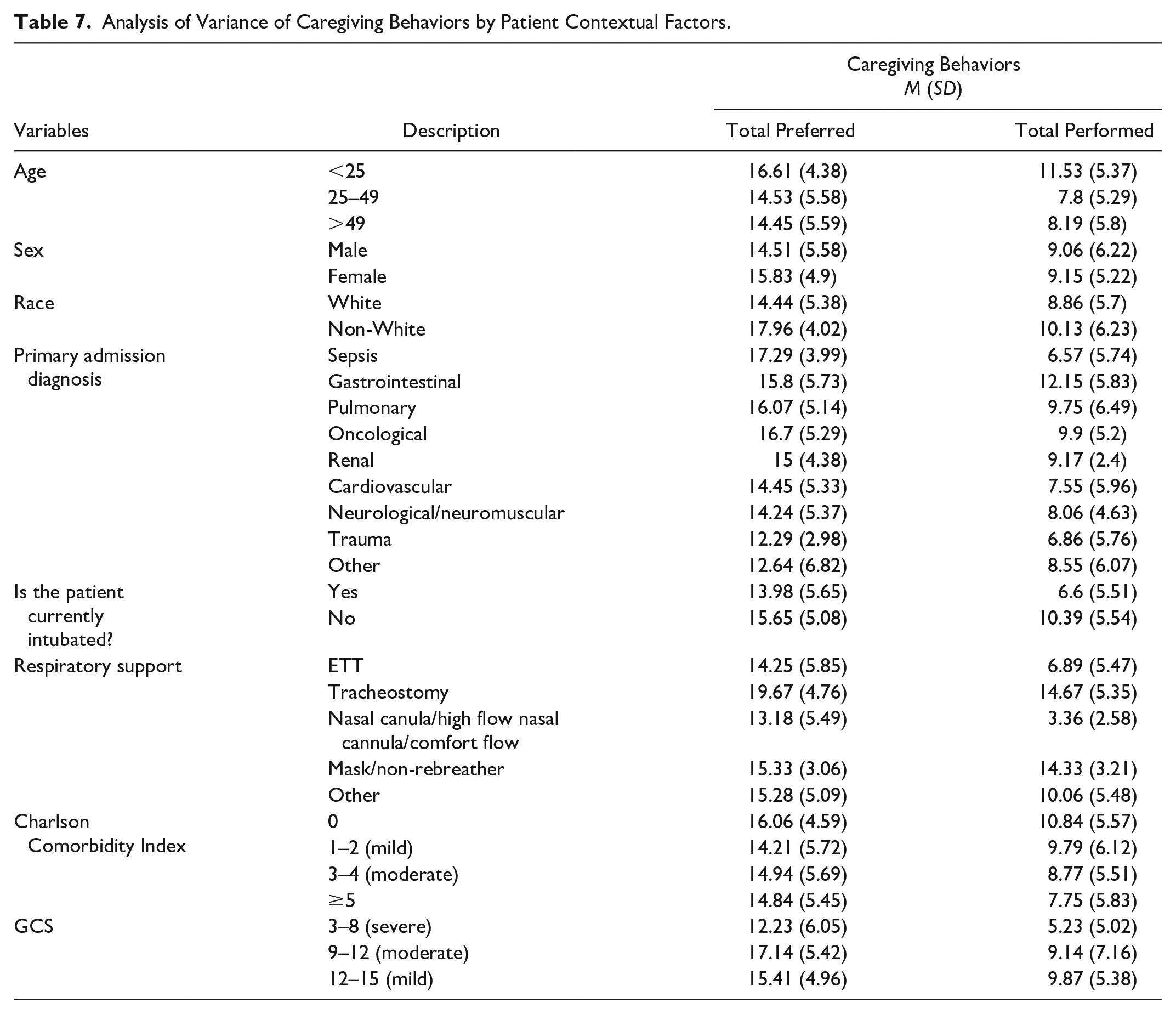
Relationships among patient contextual factors and caregiving behaviors are shown in Tables 7 and 8. Although patient age was not correlated with total preferences, it was significantly correlated with total activities performed, with caregivers of patients less than 25 years old performing an average of 11.5 care activities, significantly more than caregivers of patients over 49 (p = .011). Caregivers of patients that were intubated performed significantly less care behaviors (p < .001); approximately 4 more care activities were performed by the caregiver when the patient was not intubated. Significantly lower care preferences (p = .013) and performing of activities (p = .003) were seen in patients in the severe category of the Glasgow Coma Scale, indicating caregivers may prefer to be less involved in patients with the lowest mental status. Significantly fewer performed activities were observed in cases with higher sedation frequency (r = −.346, p < .001), higher sedation intensity (r = −.325, p < .001), and a greater number of lines or tubes present (r = −.279, p = .002).
Analysis of Variance of Caregiving Behaviors by Patient Contextual Factors.
Correlations between Patient Contextual Factors and Caregiving Behaviors.
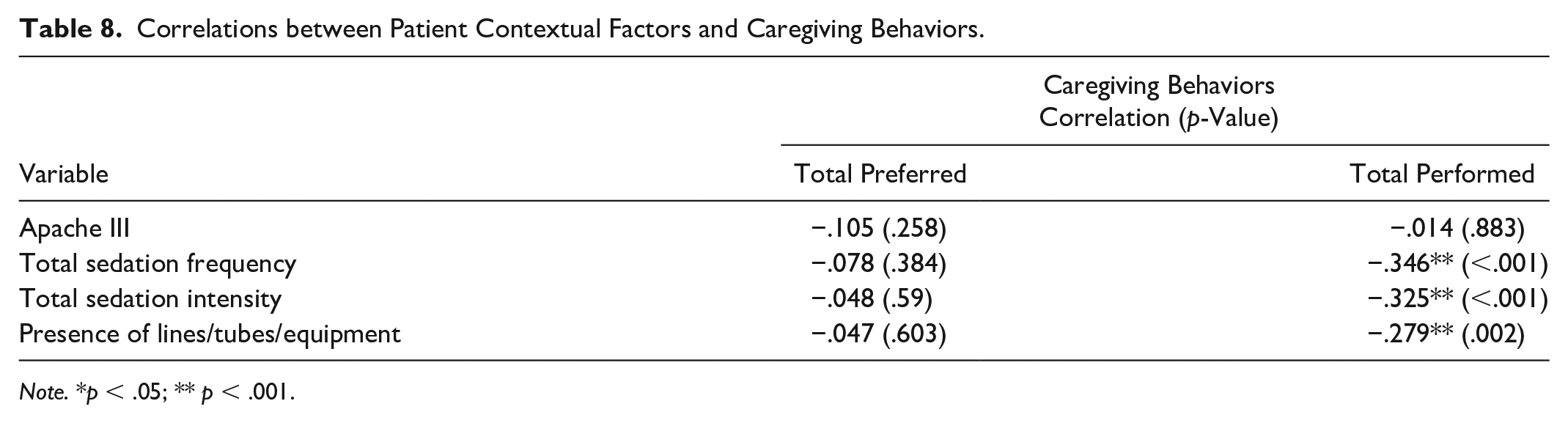
Note. *p < .05; ** p < .001.
Discussion
This study aimed to investigate caregivers’ preferences for participation in patient care, as well as describe their actual contributions to patient care while visiting their family member in the ICU. In addition, we explored the relationships among demographic, psychological, clinical factors, and caregiving behaviors. Similar to previous studies, family respondents in this study expressed a desire to be involved in the care of their family member while in the ICU (Garrouste-Orgeas et al., 2010; McAndrew et al., 2020b; Wong et al., 2020; Wyskiel et al., 2015b). Of note, our study is one of few that elicited family caregivers’ preferences for specific care activities. Specifically, more than half of the caregivers in our sample preferred to perform care activities related to daily grooming, integrative healing, communication, education, and bedside therapies and procedures. By and large, nurses support family caregiver involvement in these noninvasive care activities at the bedside (Hetland et al., 2017, 2018). However, we identified a discrepancy between the numbers of care activities that respondents desired to perform compared to the number of care activities they reported performing at the bedside. This discrepancy may be due to previously documented barriers that can negatively affect family engagement in patient care, such as a lack of established tools and evidenced-based interventions to effectively operationalize family member’s participation in care, as well as inadequate family caregiver education and training (Hetland et al., 2017, 2018; McAndrew et al., 2020b). We recommend future studies apply robust qualitative approaches to elicit more about the activities that nurses and family caregivers agree are practical and appropriate for family caregivers to complete, and determine optimal ways to promote these activities at the bedside. Similarly, further exploratory work is required to understand the care activities that family caregivers are interested in completing but are not able to complete. This will help identify what may prevent caregivers from completing these activities (e.g., not receiving education and training to safely complete task; task is considered too complicated; inadequate time to complete) and inform continued development of evidence-based practice guidelines for active family involvement in patient care.
More than half of our sample expressed a desire to participate in low risk, holistic care activities such as providing the patient with music, reading to the patient, applying essential oils, and doing artwork together, and yet fewer than 50% of caregivers reported participating in these activities at the bedside. This may be due to clinicians’ misconceptions about the value of these holistic cares, an adult ICU culture that fails to have a deep understanding of how to diminish the emotional and cognitive shock induced by critical illness, and a lack of institutional support for incorporating these holistic cares as part of daily routines in the ICU. Holistic healing cares are simple, noninvasive, appropriate for the large majority of patient/caregiver relationships, and can address physical, emotional, and psychological symptoms in both the patient and family caregiver. For example, family caregivers have previously described the importance of their role in helping maintain their critically ill family member’s psychosocial and emotional well-being (Wong et al., 2020). Caregivers have also expressed the value of being present and feeling like they are contributing (Blom et al., 2013). However, there is a lack of literature investigating the actual use of holistic healing techniques in the ICU. Future studies should explore holistic care activities as opportunities to promote family caregiver participation in patient care and examine how that engagement impacts patient and caregiver outcomes. Child Life programs, a pediatric model of care that addresses the psychosocial concerns that accompany hospitalization, hold promise for engaging family caregivers in adult ICUs. ICU clinicians need support from other professionals with expertise in psychology and integrative health and healing to create a more gentle, caring, and responsive environment for critically ill adult patients and their families (O’Brien et al., 2015).
To productively engage family caregivers in patient care, we first need to increase both clinicians and caregivers’ awareness of opportunities for family caregiver engagement. Clinicians need readily available bedside assessments to help them elicit individual caregiver’s preferences for performing patient care activities. We recommend building upon the instrument used in this study to elicit family preferences as a starting point to help align family needs and preferences with specific nursing interventions and patient care activities. In this study, despite individual caregiver differences in baseline contextual factors, when provided with a list of ways to be involved in care, respondents clearly articulated their preferences. This is an important finding as it points to the value of efforts to elicit family caregiver preferences. In a recent quality improvement initiative, investigators posted a family involvement menu in the patient’s room and allowed families to pick the care activities they wanted to be involved in (Wyskiel et al., 2015b). Families reported an enhanced ability to cope and improved communication and information sharing. While this menu was a useful tool, harnessing technology to embed such a tool in the EMR giving caregivers an opportunity to record their participation in care activities is a key advancement to fully operationalizing caregivers as active partners in care.
A surprising finding was that caregivers in our study reported feeling that they would be comfortable performing tasks that they had not yet had the opportunity to perform. On a 10-point scale, they reported a mean comfort level of 5 or above for 25 out of the 27 tasks listed. A systematic review of patient and family-centered care interventions that included a meta-analysis of outcomes reported that interventions resulted in a decrease in ICU length of stay; no studies found increased ICU cost or increased resource use (Goldfarb et al., 2017). In light of high patient acuity and increasing ICU nurse workload, our results support efforts to engage motivated and willing caregivers at the bedside to perform daily care tasks. Family participation in care can also help increase nurse availability for critical thinking, patient assessment, and care coordination; enhance clinician-family relationship building and create opportunities for early education for post ICU discharge (Wyskiel et al., 2015a, 2015b). Additional studies should be conducted to further examine the impact of active family participation in care on measures of clinicians workload and satisfaction.
With a mean preference score (FPRI) of 13.6 and PROMIS-19 anxiety and depression scores that were close to the population norm, caregivers in our sample were preinclined to participate and not overly stressed. This is an important consideration when interpreting our study findings since previous studies have highlighted caregiver reports of insecurity and poor caregiver mental health as a barrier to their participation in patient care. Future research should engage family caregivers and clinicians in the development of routine assessment strategies that help inform caregiver willingness to and readiness for participation in caregiving activities. There is also a need for research that investigates the optimal education, preparation, and support for family caregivers to engage in ICU care and how these relate to patient and family outcomes. Leveraging simulation-based training and education for caregivers of ICU patients may be a strategy to support better preparation of family caregivers for the patient’s transition home after their hospitalization (Arnold & Diaz, 2016). Future studies should explore the feasibility, acceptability, and outcomes of simulation as well as virtual educational modalities that address the emotional, psychological, and cognitive issues related to caregiving and the impact on PICS-F. Providing caregivers with the training and support to facilitate patient recovery after critical illness remains an important and understudied area of science.
The complexity of family engagement in care speaks to the importance of theory driven research. In a recent review of ICU family-centered interventions, only 33% were guided by a theoretical framework. Our study is novel in that to our knowledge, it is the first ICU study to apply components of the IFSMT to the study of ICU family engagement (Ryan & Sawin, 2009). Although originally developed with chronic illness in mind, IFSMT serves as a unique guide to study how patient, family, and health care professional factors, and cultural and environmental components of the ICU, influence family engagement in care. Framing ICU family engagement intervention development within the constructs of the IFSMT encourages consideration of the ways in which individual caregiver attributes influence their willingness, readiness, preparation, and preferences for participating in patient care. Theory supports precise measurement and creates a roadmap to explore a specific intervention’s mechanism of action (Melnyk & Morrison-Beedy, 2012). This is where family engagement science must evolve if we are to be successful in the development of interventions that promote appropriate, individualized caregiver participation in bedside care.
There are several limitations to this study. We recruited our study subjects using convenience sampling from a single site possibly limiting the diversity and generalizability of our findings. We used a cross-sectional design and recruited family caregivers at a single time point during a patient’s ICU admission. Caregivers were enrolled between 0 and 62 days of patients’ ICU admission. Therefore, it is possible that some family caregivers could have performed care activities after they completed our study measures. The self-report nature of our study measures may influence the reliability and validity of our measurements. We included caregivers of both adult and pediatric patients. These caregiving populations may have different preferences and access to resources for engagement that may have affected our results. Finally, although caregivers were given an opportunity to provide open-ended comments about their responses, few took this opportunity to share more. Including one-on-one interviews with caregivers is recommended in future studies to further understand the discordance between what caregivers are able to and what they want to do to support the patient in the ICU.
Conclusions
Interventions that enable caregivers to actively participate in patient care in the ICU are urgently needed to mitigate the negative symptom sequelae experienced by family caregivers during and after the ICU and to better prepare them for new caregiving demands after hospital discharge (Davidson et al., 2017; McAndrew et al., 2020a). Because ICU family engagement science is still emerging, evidence-based, standardized tools to evaluate family caregiver characteristics and preferences have yet to be established, leaving clinicians with few tools and resources to support family involvement in care. Before tailored interventions can be developed, we must further explore family caregivers’ perspectives about involvement in the ICU so we can better understand family preferences and develop tools and interventions to support families as partners in ICU care. This is essential, as not all family caregivers will want to participate or feel safe to do so. The results from this study add to a growing body of literature that highlights the importance of evaluating individual family caregiver characteristics and preferences to support their safe and effective participation in direct patient care in the ICU (Brown et al., 2015; Mitchell et al., 2016; Olding et al., 2016; van Beusekom et al., 2016). Future studies should explore family preferences on holistic healing activities and ways to involve families in the delivery of this type of care. Further, we must also examine the impact of family involvement on nurse workload in addition to its impact on patient and caregiver outcomes. It is critical that clinicians and researchers recognize the importance of family partnership in the ICU; this must guide our future research and practice improvement efforts.
Footnotes
Author Contributions
B.D.H., K.A.K., and B.J.P. contributed to the conception and design of the study. B.D.H. and J.M.H. contributed to the acquisition of the data. B.D.H., N.S.M., C.E.C., and K.A.K contributed to the analysis and interpretation of the data. All authors contributed to the drafting and revision of the manuscript for important intellectual content and approved the final version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Nurses Foundation.