
Abstract
Family caregivers of persons with bipolar disorder experience considerable stress. Yet, studies have not examined whether their stress differs by race and gender. This preliminary analysis of baseline data from 228 African American and White family caregivers of adults with bipolar disorder who were enrolled in a randomized controlled trial examined race and gender differences on two validated self-report measures of psychological stress (caregiver burden and caregiver reactions) and an electrocardiography device used to capture heart rate variability (HRV). No statistically significant differences were found by race or gender on either measure of psychological stress. African American caregivers had significantly lower scores on two indices of HRV compared to White caregivers. Women had significantly lower scores on one index of HRV compared to men. Low HRV indicates greater stress and mortality risk. Future research should include HRV to measure caregiver stress and implement relevant interventions.
Bipolar disorder affects nearly 2.8% of American adults each year (National Institute of Mental Health [NIMH], 2017). Most people diagnosed with bipolar disorder are cared for by family members. The unpredictable, cyclical nature of bipolar disorder makes caregiving particularly challenging and burdensome for these family members. Few studies have examined psychological and physiological stress responses to caregiving for a family member with bipolar disorder, and none have specifically examined whether differential stress responses occur by race or gender.
Caregiver Characteristics
Female caregivers contribute more time to caregiving and experience greater amounts of stress and strain than male caregivers (Sharma et al., 2016). Furthermore, female caregivers of people with mental illness often have multiple roles and experience more disruption in their work and social life because of caregiving than men (Sharma et al., 2016). Female caregivers are more likely to lose income, lose job benefits, and reduce work hours due to caregiver responsibilities (Lahaie et al., 2013). In the caregiving literature, the majority of studies are among women (Sharma et al., 2016). Thus, there is limited information on the experience of male caregivers, particularly highly distressed caregivers such as those caring for persons with bipolar disorder.
In studies comparing White and African American caregivers, African Americans generally provide more caregiving hours and perform more caregiver tasks than White caregivers (Kaufman et al., 2010; Pinquart & Sörensen, 2005). However, African American caregivers report lower levels of burden and depression than White caregivers (Cuellar, 2002; Janevic & Connell, 2001; Pinquart & Sörensen, 2005). The stress appraisal and coping theory (Lazarus & Folkman, 1984) suggests a person appraises, or evaluates, the personal significance of a potential stressor. African American caregivers tend to appraise caregiving as less stressful but are more cognitively impaired and in worse physical health than White caregivers (Pinquart & Sörensen, 2005; Shah et al., 2010).
African Americans feel they have no choice in taking on the caregiving role, which is compounded by full time employment outside of the home (American Association of Retired Persons [AARP] & National Alliance for Caregiving, 2020). This feeling of obligation is related to a deeply rooted expectation in African American culture to assume care for a family member or friend (Pharr et al., 2014). Transition into the caregiver role can be a continuous hardship for several years because of role engulfment and loss of identity (Skaff & Pearlin, 1992). Chronic stress endured by these caregivers leads to a physiologic burden. There are no identified studies on racial differences in cardiovascular physiological stress markers in highly distressed caregivers. Therefore, this study examined racial differences in measures of heart rate variability (HRV) in highly distressed caregivers of people with bipolar disorder.
Heart Rate Variability
HRV reflects the ability of the heart to adapt to stressors and can be used as an objective measure of stress (Kim et al., 2018; Moss & Shaffer, 2016). The autonomic nervous system is the most prominent physiologic factor that determines heart rate through the brain–heart connection (Thayer & Sternberg, 2006). The autonomic nervous system is comprised of the sympathetic nervous system, associated with active and mobile functions, and the parasympathetic nervous system, associated with rest functions (Thayer & Sternberg, 2006). Specifically, the cardiac vagal nerve is the parasympathetic contribution to cardiac regulation (Laborde et al., 2017; Thayer & Sternberg, 2006).
Normally, the sympathetic and parasympathetic nervous systems are in balance to maintain homeostasis (McEwen, 2000; Thayer & Sternberg, 2006). However, stressors affect homeostasis by increasing energy demand on bodily systems through activation of the sympathetic nervous system (McEwen, 1998; Selye, 1956). The sympathetic nervous system speeds the heart rate through the release of epinephrine and norepinephrine and the parasympathetic nervous system slows the heart rate rapidly through the release of acetylcholine (Moss & Shaffer, 2016). Thus, a dynamic autonomic balance must be maintained to preserve cardiovascular health.
Time domain and frequency domain indices of HRV capture different sources of autonomic control. Time domain indices include the standard deviation of all intervals between normal sinus beats (SDNN) and the square root of the mean of the sum of squares of the differences between adjacent normal sinus beats (RMSSD). SDNN is influenced by sympathetic and parasympathetic nervous system activity (McCraty & Shaffer, 2015). RMSSD is highly influenced by the parasympathetic nervous system (Shaffer & Ginsberg, 2017). Frequency domain indices quantify power distribution of the heart signal. Spectral components include high frequency power, low frequency power, and very low frequency power. High frequency is a measure of parasympathetic nervous activity. Low frequency is a measure of sympathetic nervous and baroreflex activity (Ernst, 2017; Moss & Shaffer, 2016; Shaffer & Ginsberg, 2017). Very low frequency is likely influenced by the renin angiotensin system and physical activity with some influence by both the parasympathetic and sympathetic nervous systems. However, there is some uncertainty around the physiologic mechanism underlying the very low frequency (Ernst, 2017; Moss & Shaffer, 2016). Total power is the sum of each spectral band. The low to high frequency ratio reflects sympathetic versus parasympathetic nervous system activity, or sympathovagal balance (Moss & Shaffer, 2016; Shaffer & Ginsberg, 2017).
Autonomic imbalance is linked to increased cardiovascular morbidity and all-cause mortality (Fang et al., 2020; Moss & Shaffer, 2016). High HRV scores are indicative of resilience and a healthy adaptive response. Low HRV scores are indicative of a maladaptive autonomic response and comprised cardiovascular health.
Purpose
The purpose of this study was to (a) determine whether there were differences by race and gender on measures of psychological stress (caregiving burden and caregiver reactions) and (b) determine whether there were differences by race and gender on measures of physiological stress (HRV—seven indicators) among family caregivers of adults with bipolar disorder. The HRV indices are as follows: (a) standard deviation of interbeat intervals of normal sinus beats, (b) square root of the mean squared distance of adjacent normal sinus beats, (c) total spectral power, (d) high frequency power, (e) low frequency power, (f) ratio of low to high frequency power, and (g) very low frequency power.
Methods
Design and Sample
This study was a preliminary analysis of baseline data from a randomized controlled trial of family caregivers of adults with bipolar disorder conducted in Northeastern Ohio from 2017 to 2021. The Case Western Reserve University Institutional Review Board approved this research. Participants were recruited from the community including libraries, grocery stores, eateries, universities, and social media. The parent study evaluated the effects of family caregiver participation in selection of self-management interventions on mental and physical health over time. Inclusion criteria for the randomized controlled trial are as follows: (a) English speaking; (b) age ≥ 18 years old; (c) have a family member with bipolar disorder; (d) have cared/supported them for at least 6 months in the last year; and (e) capable of performing informed consent and participating in study procedures. Caregivers in the role for at least six months have adapted to the role, caregivers in the role less than six months may experience additional stress due to the adjustment. Participants were excluded from the parent study if they had knowledge of another family member in the same household enrolled in the study were pregnant, had a pacemaker, or lived outside of the study area.
This preliminary analysis used baseline data to examine gender (male vs. female) and racial (African American vs. White) differences on measures of stress response. The sample sizes for other racial and gender groups were too small for comparisons to be made. In total, 21 participants did not identify as African American or White and three participants did not specify a gender. Additionally, one participant enrolled, but did not complete baseline data collection. These participants were not included in the analyses.
The gold standard for short-term HRV measurement is at rest for a total of at least 5 minutes (Shaffer & Ginsberg, 2017). Participants that had an electrocardiogram recording less than 5 minutes were not included in the analyses. Additionally, artifacts (missed beats, unclear reading) are a major area of concern when analyzing electrocardiography data because they can distort time and frequency domain measurements of HRV (Shaffer & Ginsberg, 2017). Participants with high artifact (20%–80%) or undetectable HRV indices were not included in the analyses. The total sample in this study consisted of a convenience sample of 228 African Americans and White participants. We performed sensitivity analysis using G Power software (Erdfelder et al., 1996) given the sample size of 228 and we had adequate power to detect a small to medium effect size.
Procedures and Measures
Study data were collected and managed using REDCap electronic data capture tools hosted at Case Western Reserve University. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing the following: (a) an intuitive interface for validated data entry; (b) audit trails for tracking data manipulation and export procedures; (c) automated export procedures for seamless data downloads to common statistical packages; and (d) procedures for importing data from external sources (Harris et al., 2009).
Caregiver characteristics
Demographic characteristics in-cluded age, race/ethnicity, gender, education, and personal income.
Caregiver burden
Caregiver burden was measured by the 31-item Involvement Evaluation Questionnaire (IEQ) (Schene & Van Wijngaarden, 1992). The IEQ is well validated and reliable. In a sample of 223 primary caregivers of people with schizophrenia, the Cronbach’s alpha (α) was 0.86 (Gonçalves-Pereira et al., 2017). Furthermore, the IEQ was correlated with the Zarit Burden Interview (ZBI) to establish convergent validity. A significant correlation was found (r = 0.63, p < .0001). In a multicountry study on caregiving (Van Wijngaarden et al., 2000), various language translations of the IEQ had good internal consistency (α = 0.87–0.91) and test–retests reliability (ICC = 0.81–0.99).
The IEQ has four domains: tension (nine items), worrying (six items), supervision (six items), and urging (eight items). Four items are not included in the domains: two questions on coping, one question on personal interest, and one question on caregiver/recipient relationship changes. The caregivers rated each domain item on a 5-point Likert scale from 0 (never) to 4 (always). The 27 domain items were used for analysis. A total score was calculated by summing the scores. Total scores ranged from 7 to 108 (M = 48.57, SD = 19.50). The possible range for the scale is 0–116. Higher scores indicate greater caregiver burden. The scale had good internal consistency in our sample (α = .91).
Caregiver reactions
Caregiver reactions were evaluated using the Mood Disorder Burden Index (MDBI) reaction subscale (Martire et al., 2009). The MDBI reaction subscale is a 32-item measure to assess caregiver burden in family members and friends of adults with bipolar disorder or major depressive disorder. The 32 items capture reactions to event occurrences. Reliability of the scale was established in a sample of 161 caregiver of older adults with major depressive disorder or bipolar disorder. The Cronbach’s alpha (α) for the 32-item subscale was .91 (Martire et al., 2009). The reaction subscale was correlated with the ZBI, which is often used to measure general caregiver burden. The correlation between the MDBI reaction subscale and the ZBI was large and positive (r = .65, p < .001). The MDBI reaction subscale was also correlated with caregiver rewards and had a low, nonsignificant correlation (r = –.07) indicating no association between burden and rewards (Martire et al., 2009).
The MDBI has three core domains and a fourth optional domain: patients’ mood symptoms (20 items), caregivers’ worry about the future (3 items), caregivers’ interpersonal difficulties with the patient (4 items), and burden associated with patient’s mood disorder treatment (optional 5 items). The caregivers rated reactions to each event on a 5-point Likert scale based on bothersome or upset feelings ranging from 0 (not at all) to 4 (extremely). The subscale scores ranged from 0 to 128 (M = 55.72, SD = 24.71). The possible range for the subscale is 0–128. Higher scores indicate more bothered or upset feelings related to care recipient behaviors. The subscale had good internal consistency in our sample (α = .93).
HRV measurement
HRV was measured and recorded using the BioRadioTM. The BioRadioTM is a portable electrocardiography device. Participant’s wrists and hands were cleansed with alcohol and three electrodes were applied: left wrist, right wrist, and back of the hand. The leads were attached to a receiver that captured data via Bluetooth on the data collector’s computer. HRV was recorded for approximately 5–10 minutes during spontaneous breathing. The gold standard for short term HRV measurement is 5 minutes at rest (Moss & Shaffer, 2016; Shaffer & Ginsberg, 2017). After data collection, artifact and ectopic beats were removed from the recording before calculating the seven HRV scores (SDNN, RMSSD, total spectral power, high frequency power, low frequency power, ratio of low to high frequency power, very low frequency power) using Vivosense software.
Low SDNN scores have been associated with greater morbidity and mortality (Hillebrand et al., 2013; Nolan et al., 1998). Low RMSDD scores have correlated with unexplained death in epilepsy patients (DeGiorgio et al., 2010). Low levels of low frequency power have been associated with vascular resistance. Low levels of high frequency power have been associated with stress, anxiety, and worry (Shaffer & Ginsberg, 2017). Low levels of very low frequency power have been associated with adverse cardiovascular events (Huang et al., 2017), post-traumatic stress disorder (Shah et al., 2013), and inflammation (Lampert et al., 2008). Generally, lower scores on each HRV measurement have been associated with adverse health outcomes (Shaffer & Ginsberg, 2017).
Analysis
This preliminary analysis used baseline data from a larger study to examine gender and racial differences on measures of stress response. This study focused on racial (White vs. African American) and gender (male vs. female) differences. Frequency distributions, outliers, and missing data were examined using the Statistical Package for the Social Sciences (SPSS), version 27. HRV indices were natural logarithm transformed for analyses because of skewed data. Natural logarithm (ln) transformations of HRV indices occur commonly in the literature because data are often not normally distributed and interfere with computing parametric analyses (Ellis et al., 2008; Nunan et al., 2010).
General linear model (GLM) analyses were conducted to examine the effects of gender and race on stress responses. Separate GLMs were built for each dependent outcome variables (caregiver burden, caregiver reactions, lnSDNN, lnRMSSD, lnLF, lnHF, lnLFHF, lnVLF, lnTP). Scores for the participants were entered into the appropriate models with gender and race for between subject comparisons. The models were computed using α = .05. There were no extreme outliers as assessed by inspection of boxplot. Data were normally distributed as assessed by skewness and kurtosis values of residuals (Kline, 2015). There was homogeneity of variances as assessed by Levene’s test for equality of variances (p = .09–.96)
Results
Caregiver Characteristics
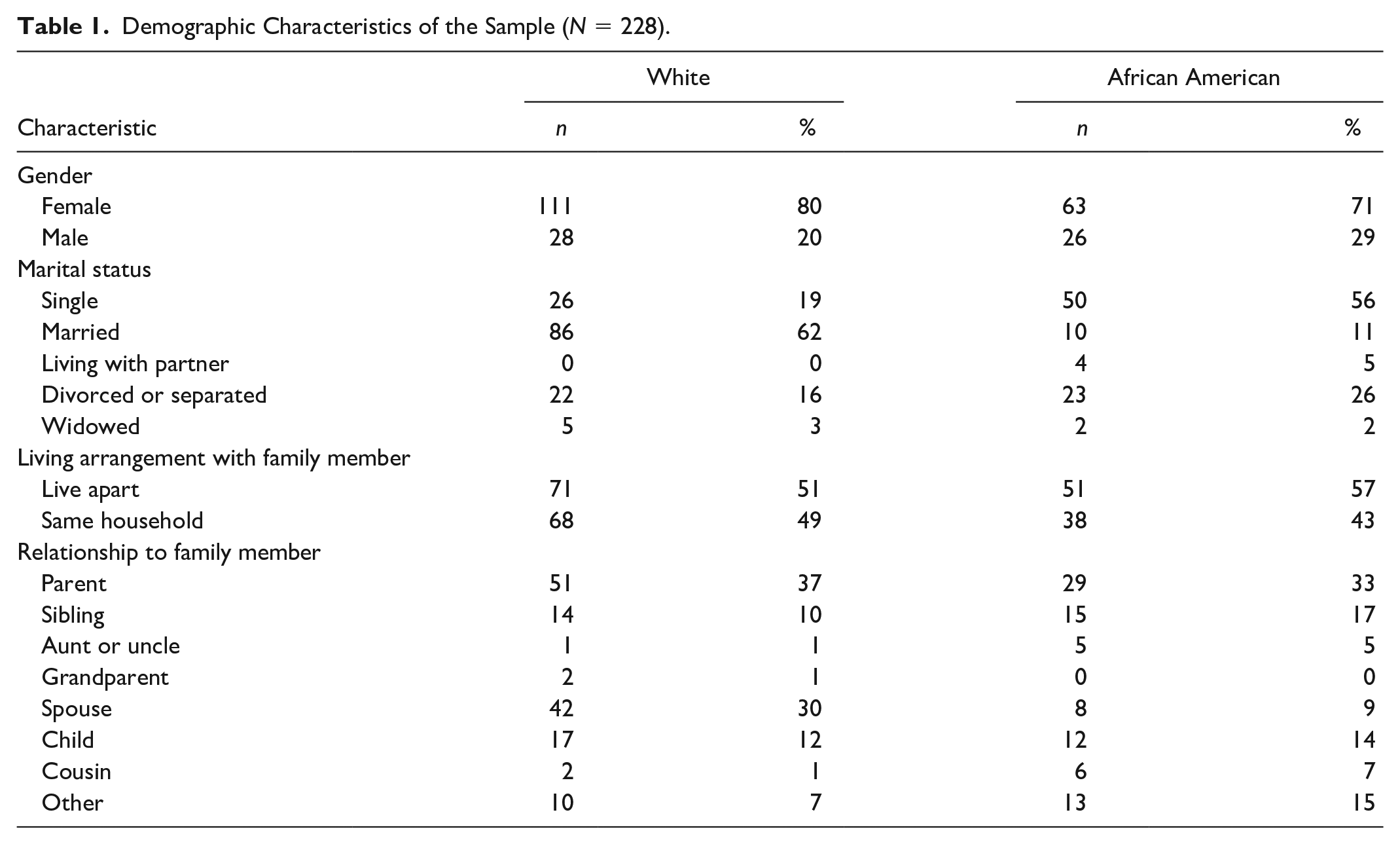
African American participants were between the ages of 19 and 74 years (M = 50.74, SD = 12.37). The majority of African American participants identified as female (71%), single (56%), reported individual annual income <$20,000 (73%), and completed some college or less (70.8%). White participants were between the ages of 18 years and 87 years (M = 52.93, SD = 14.16). The majority of White participants identified as female (80%), married (62%), reported individual annual income of at least $30,000 (55%), and completed college or held advanced degrees (66.2%). Descriptive characteristics of the sample are displayed in Table 1.
Demographic Characteristics of the Sample (N = 228).
Psychological Stress Response
The results of the GLM statistical analyses for psychological stress variables are presented in Table 2, which include means, standard deviations, and two-way ANOVA statistics for caregiver burden and caregiver reactions scores.
Means, Standard Deviations, and Two-Way ANOVA Statistics for Psychological Variables.
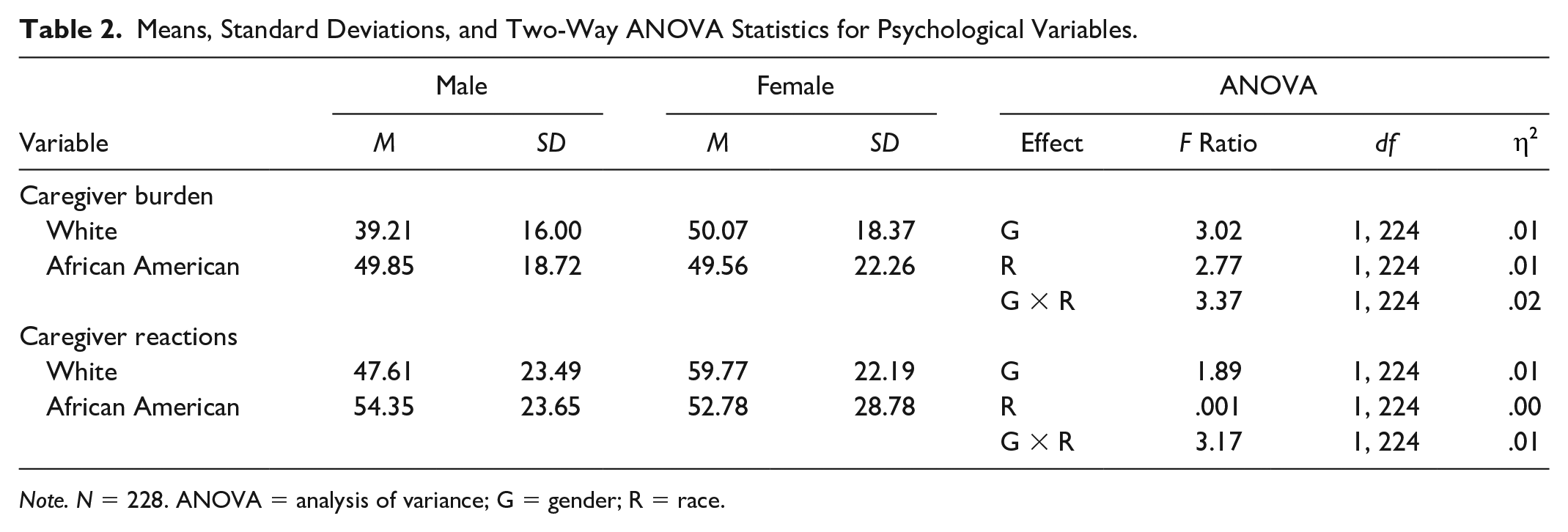
Note. N = 228. ANOVA = analysis of variance; G = gender; R = race.
Caregiver burden
There was no statistically significant interaction between gender and race for caregiver burden scores, F (1, 224) = 3.37, p = .07, partial
Caregiver reactions
There was no statistically significant interaction between gender and race for caregiver reactions scores, F (1, 224) = 3.17, p = 0.08, partial
Physiological Stress Response
Heart rate variability time domains
As displayed in Table 3, there was not a statistically significant interaction between gender and race for lnSDNN scores, F (1, 224) = .93, p = 0.34, partial
Means, Standard Deviations, and Two-Way ANOVA Statistics for HRV Time Domains.
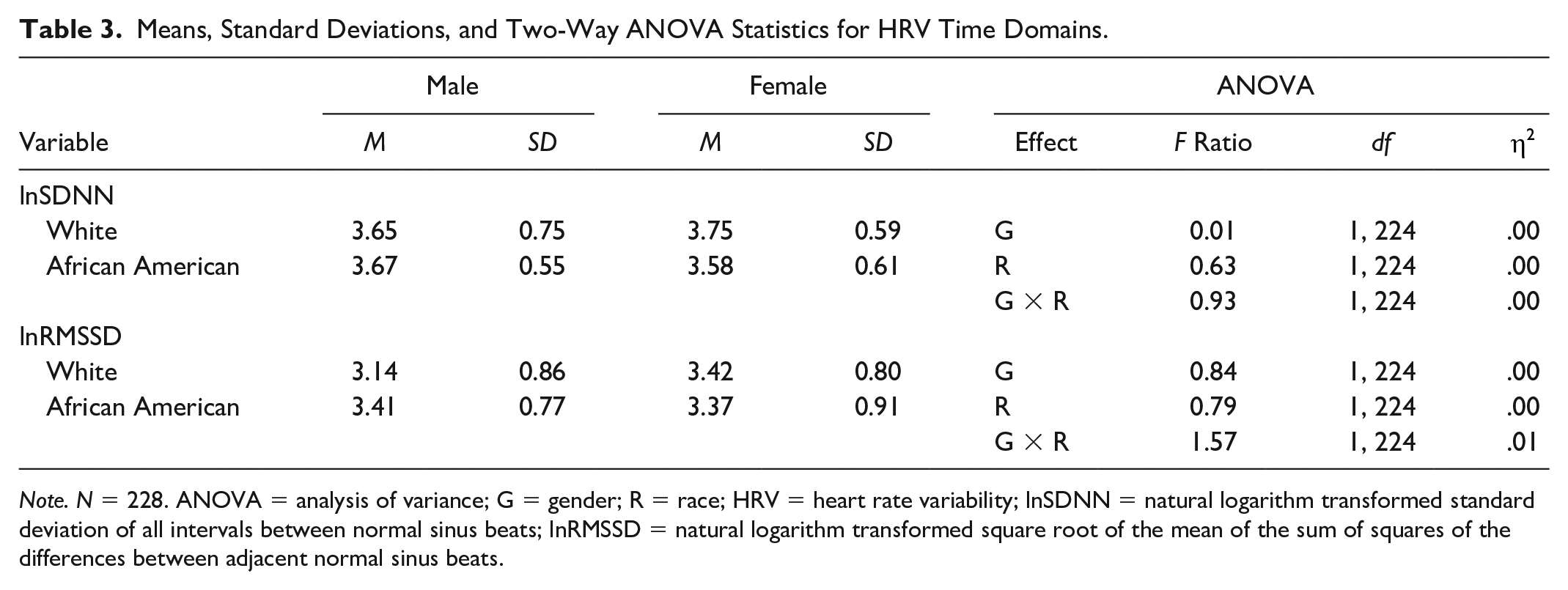
Note. N = 228. ANOVA = analysis of variance; G = gender; R = race; HRV = heart rate variability; lnSDNN = natural logarithm transformed standard deviation of all intervals between normal sinus beats; lnRMSSD = natural logarithm transformed square root of the mean of the sum of squares of the differences between adjacent normal sinus beats.
There was no statistically significant interaction between gender and race for lnRMSSD scores, F (1, 224) = 1.57, p = 0.21, partial
Heart rate variability frequency domains
As displayed in Table 4, there was no statistically significant interaction between gender and race for lnLF scores, F (1, 224) = .00, p = 0.99, partial
Means, Standard Deviations, and Two-Way ANOVA Statistics for HRV Frequency Domains.
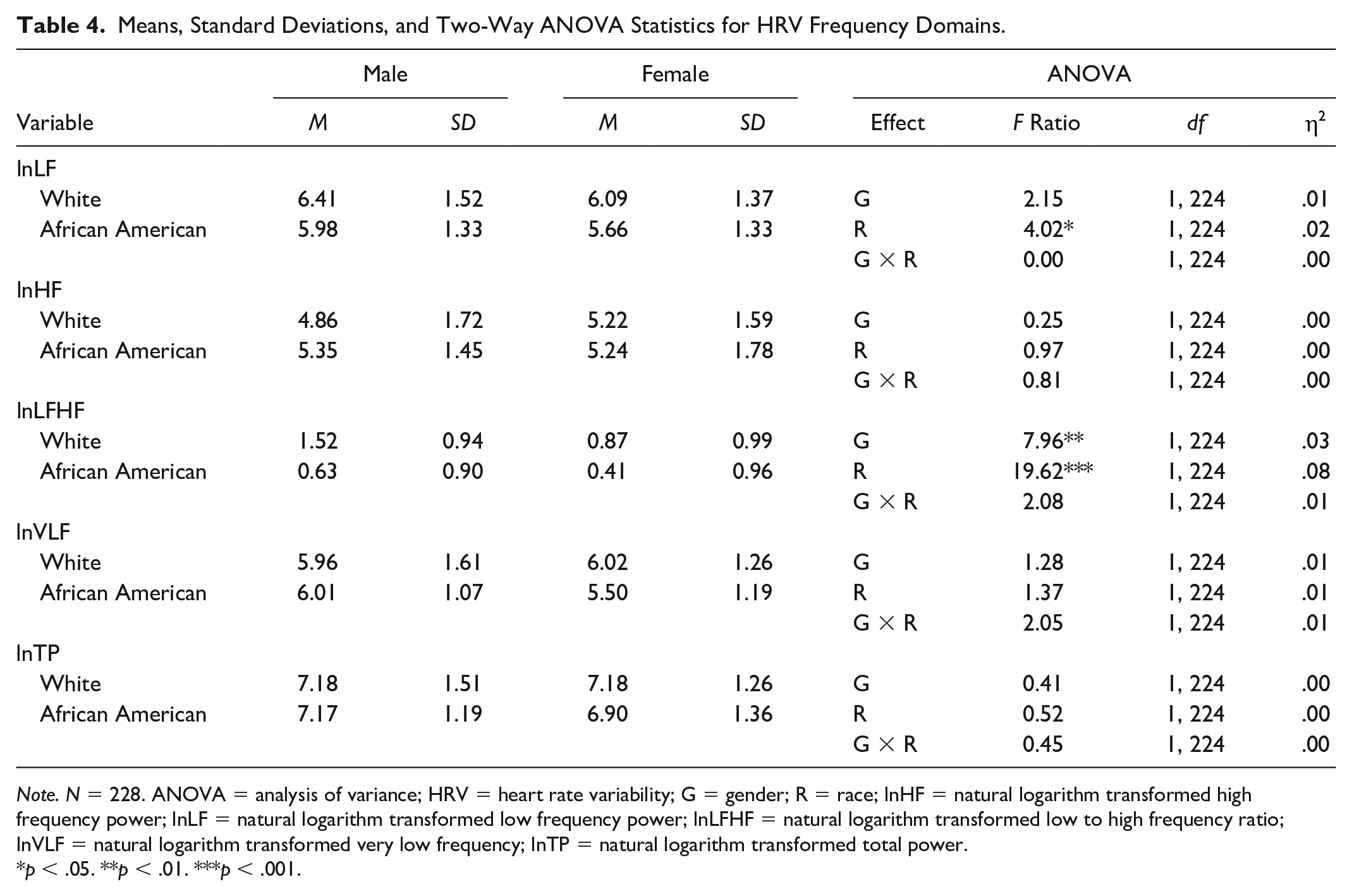
Note. N = 228. ANOVA = analysis of variance; HRV = heart rate variability; G = gender; R = race; lnHF = natural logarithm transformed high frequency power; lnLF = natural logarithm transformed low frequency power; lnLFHF = natural logarithm transformed low to high frequency ratio; lnVLF = natural logarithm transformed very low frequency; lnTP = natural logarithm transformed total power.
p < .05. **p < .01. ***p < .001.
There was no statistically significant interaction between gender and race for lnHF scores, F (1, 224) = .81, p = 0.37, partial
There was no statistically significant interaction between gender and race for lnLFHF scores, F (1, 224) = 2.08, p = 0.15, partial
There was no statistically significant interaction between gender and race for lnVLF scores, F (1, 224) = 2.05, p = 0.15, partial
There was no statistically significant interaction between gender and race for lnTP scores, F (1, 224) = .45, p = 0.50, partial
Discussion
This is the first known study to explore HRV, a noninvasive physiologic measure of stress, as a major research focus in caregivers of people with bipolar disorder. Findings from this study demonstrated racial and gender disparities in HRV. We found African American participants had significantly lower scores in low frequency power and ratio of low to high frequency power domains of HRV than White participants. The low frequency power band largely reflects baroreceptor activity (blood pressure regulation) and sympathetic nervous system activity (adaptability) when measured at rest (Ernst, 2017; Moss & Shaffer, 2016; Shaffer & Ginsberg, 2017). In light of what the power band captures, our findings are consistent with known disproportionate cardiovascular disease risks among African Americans (Carnethon et al., 2017). Our findings also suggest the caregiving experience might have a greater physiological cost among African Americans.
Our findings are consistent with a study examining physiologic regulation in middle aged adults that found significantly higher levels of allostatic load, or physiologic dysregulation, in African American men and women compared to White men and women (Tomfohr et al., 2016). Our findings are also consistent with the CARDIA study that found African American adults had significantly lower levels of low frequency power and a lower ratio of low to high frequency power than their White counterparts (Sloan et al., 2008). However, Hill et al. (2015) performed a systematic review and meta-analysis to examine ethnic differences in resting HRV and found African Americans had higher HRV than Whites. The review did not include the HRV domains where we found differences.
We found females had a significantly lower ratio of low to high frequency power than males. The ratio reflects sympathetic versus parasympathetic nervous system activity, or autonomic balance (Moss & Shaffer, 2016; Shaffer & Ginsberg, 2017). A higher ratio is indicative of sympathetic dominance and a lower ratio is indicative of parasympathetic dominance (Moss & Shaffer, 2016). Our findings are consistent with the notion that males tend to have more sympathetic activity than females (Dart et al., 2002). A recent meta-analysis on gender differences in HRV demonstrated similar findings, showing greater sympathetic, or baroreflex activity, in males compared to females in a sample of healthy middle aged adults (Koenig & Thayer, 2016).
In examination of psychological stress, findings from this study emphasize the burden experienced by caregivers of adults with bipolar disorder, regardless of race and gender. This was an interesting finding as studies have reported racial differences in caregiver burden and appraisal with African American caregivers reporting less psychological burden or distress compared to White caregivers (Janevic & Connell, 2001; Kaufman et al., 2010; Pinquart & Sörensen, 2005). Additionally, studies have found females caregivers generally experience significantly higher levels of caregiver burden than male caregivers (Mulud & McCarthy, 2017; Sharma et al., 2016; Swinkels et al., 2019). In our sample, 56% of African American participants were single and 62% of White participants were married. There could be potential differences in psychological stress by marital status. A study on family caregivers of adults with disability found caregivers who were single had higher levels of caregiver stress (Kim, 2017).
The current study had a large sample size (N = 228) and was unique in its application of HRV as a primary research focus in caregivers of people with bipolar disorder. However, there are some limitations to note. We were limited to the existing sample comprised mostly of African American and White caregivers, which allowed us to only make comparisons between these racial groups. Future research should incorporate HRV and examine caregivers from other racial and ethnic groups. Study participants lived in Northeastern, OH and may not be representative of the entire population, although Northeast Ohio is an ideal setting given its demographic composition, including minority representation that exceeds the State of Ohio, United States (United States Census Bureau, 2010).
This study was a preliminary analysis of baseline data from a randomized controlled trial, which might not capture participants who would have participated in a cross-sectional study. The nature of this study also limited the selection of measures and study variables. However, the available measures were reliable and valid indicators of psychological and physiological stress. In the examination of physiological stress, we cannot tease out caregiver stress from other stress in one’s life. Lastly, time of day, body mass index, blood pressure, and heart rate were not considered in the context of HRV but may be explored in future research.
Findings from this study identify the relevance of using HRV when examining stress in diverse samples of caregivers to inform biobehavioral pathways of stress and develop interventions to reduce racial/gender disparities, such as HRV biofeedback. Future research should consider individual characteristics other than race and gender when examining stress in this population to provide insight on factors that may influence the relationship between psychological and physiological stress responses and race and gender. Characteristics might include age, marital status, and individual annual income. This recommendation emphasizes the need for nurse scientists to utilize theoretical frameworks that account for biobehavioral mechanisms. Caregiving and HRV are relevant areas for nurses to gain further training to employ techniques that reduce stress and improve health outcomes for highly distressed caregivers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute of Nursing Research, National Institutes of Health [Grant number R01NR016817-S].