
Abstract
The purpose of this scoping literature review was to understand what is known about how the rural profile influences beliefs regarding telehealth utilization. Rural nursing theory (RNT) provided a framework for the review. Search criteria were limited to peer-reviewed studies conducted in Europe, the United States, Canada, Australia, and New Zealand. A variety of search terms related to patient telehealth perceptions generated 213 unique articles, of which 10 met the inclusion criteria. Included studies incorporated qualitative methodologies and were from Australia, Canada, Sweden, or the United States. The review highlighted four themes related to the rural profile’s influence on telehealth beliefs: importance of familiar relationships, concerns with privacy and confidentiality, acceptance of limited access to care, and resourcefulness and frugality. These themes echo concepts within RNT. Nurses and other health professionals must acknowledge the rural profile’s influence on a person’s decision to use telehealth in order to provide optimal care.
Health inequities in rural areas of the United States and other developed nations are well documented (Aggarwal et al., 2021; Anderson et al., 2015; Behrman et al., 2021; Lutfiyya et al., 2012; Matthews et al., 2017). A perfect storm of a lagging rural economy, a lower investment in resources, including health care and education, and geographic isolation have ultimately resulted in downstream consequences of poorer health outcomes in rural areas (Thomas et al., 2014). According to the Centers for Disease Control and Prevention (CDC), rural areas experience higher rates than urban areas for the five leading causes of death in the United States: chronic lower respiratory disease, cancers, unintentional injury, heart disease, and stroke (Moy et al., 2017; Yaemsiri et al., 2019).
Telehealth has been promoted as an innovative tool to improve access to care for rural populations (Lum et al., 2019; Nelson, 2017; O’Kane, 2020). Telehealth encompasses telemedicine consults, mHealth tools such as remote monitoring, and patient portal access. The term also includes provider-to-provider communications (e.g., store and forward mechanisms, project ECHO). Most relevant to rural patients is the ability to have virtual appointments with providers who may not be located within the patient’s geographic area. Primary care clinics have been able to set up remote visits with specialists, allowing patients to confer from the privacy of their primary care provider’s office on matters ranging from mental health to dermatology to cardiac care. This model has been well-accepted and has been used extensively in the U.S. Veterans Affairs health system (Jacobs et al., 2019; Lum et al., 2019) as well as in geographically remote regions for years (Lee et al., 2019).
The onset of the COVID-19 pandemic in March 2020 dramatically shifted telehealth operations. Regulatory rules within the United States’ and other nations’ health systems were adjusted to allow providers to charge for remote telehealth encounters based from the patient’s home, as it was deemed unsafe for patients to travel to their providers’ offices. This global “demonstration project” has revealed that telehealth can be highly effective in certain circumstances. Policies are being reconsidered to allow for video-based and audio-only telehealth encounters in the home setting to be reimbursed at the same rate as in-person visits (Brotman & Kotloff, 2021; Lee et al., 2020; Mishori & Antono, 2020). However, recent literature has reported that during the COVID-19 pandemic rural populations were accessing telehealth services at lower rates than the general population (Chu et al., 2021; Hsiao et al., 2021; Jaffe et al., 2020; Jewett et al., 2022; Poeran et al., 2021; Quinton et al., 2021). This finding is particularly interesting because prior to COVID-19 rural areas tended to use telehealth slightly more than urban areas (Chu et al., 2021). It must be emphasized that previous to COVID-19, patients who used telehealth—most frequently to connect with a specialist—were overwhelmingly doing so at a local primary care office. With COVID-19, telehealth suddenly shifted to the home. Previous research has indicated that rural dwellers have less access to the internet and are less likely to use health information technologies such as patient portals and mHealth applications (Bhuyan et al., 2016; Greenberg et al., 2018). While lack of broadband access and digital literacy have emerged as possible answers to this puzzle, researchers have suggested that there are underlying factors beyond internet access that must be considered (Jaffe et al., 2020; Jewett et al., 2022). One factor the literature has largely failed to recognize is the distinct rural health-seeking profile. In the COVID-19 era, with the onus on the individual instead of the clinician in terms of deciding to use telehealth, understanding the rural profile becomes a critical component of providing equitable health care. Rural Nursing Theory (RNT) is an applicable framework to explain rural populations’ unique approach to health and health-seeking behaviors.
Rural Nursing Theory
Developed in the last quarter of the twentieth century, RNT is based on the premise that nursing practice in a rural environment is different from that in an urban place (Lee et al., 2022). The three current propositions of RNT state:
(a) Rural residents define health as being able to do what they want to do; it is a way of life and a state of mind; there is a goal of maintaining balance in all aspects of their lives. However, older rural residents and those with ties to extractive industries are more likely to define health in a functional manner—to work, to be productive, and to do usual tasks.
(b) Rural residents are self-reliant and make decisions to seek care for illness, sickness, or injury depending on their self-assessment of the severity of the present health condition and of resources needed and available.
(c) Health care providers in rural areas must deal with a lack of anonymity and much greater role diffusion than providers in urban or suburban settings (Lee & McDonagh, 2018, pp. 52–53).
Concepts such as distance, self-reliance, resilience, informal networks, informed risk, hardiness, privacy, being a conscientious consumer, trust, and community support are all important components of RNT (Lee & McDonagh, 2018; Lee et al., 2022; Montgomery & Paré, 2018) that help to distinguish differences between rural and urban populations in terms of how health is defined and how health care is sought.
Objectives
Due to the recent shift in telehealth delivery, there is a potential knowledge gap in the research regarding how the rural profile may influence the adoption of telehealth technologies. The objective of this scoping review is to understand the state of the science relative to rural beliefs and attitudes toward the utilization of telehealth. The specific research question is as follows: What is known from the literature about how the unique rural profile contributes to beliefs about and preferences for telehealth use?
Key Terms
Telemedicine, telehealth, eHealth, and mHealth are often used interchangeably. Broadly, telehealth has been defined “as the delivery and facilitation of health and health-related services including medical care, provider and patient education, health information services, and self-care via telecommunications and digital communication technologies” (NEJM Catalyst, 2018, para. 1). For the purposes of this literature review, telehealth is used as the generic term for all digitally mediated health-related interactions between the provider or health care organization and the patient. This includes patient portal use, web- or video-based communication with a provider, and remote monitoring devices. It does not include audio-only communication via telephone with a provider.
The term rural profile is used in this review to specifically denote the qualities of rural residents that contribute to a unique perspective on health and health-seeking behaviors as delineated by RNT. Other authors have used similar terms such as rural attitude or rural culture (Thomas et al., 2014; Thurman et al., 2019). The rural profile includes attitudes, behaviors, and beliefs such as self-reliance, hardiness, and stoicism. It does not include the predisposing demographics or social structure factors, such as sex, age, geography, income, or family size.
Rural can mean different things to different people. While authors should operationalize rural within their studies, this is not always the case. Study-specific definitions of rural will be included when available.
Methods
A scoping literature review was undertaken in order to understand the extant literature regarding how the rural profile may influence perspectives of telehealth utilization. Scoping reviews are an appropriate method to summarize findings within a heterogeneous or ill-defined area of research in order to assess the state of the science and identify any gaps (Peters et al., 2015; Tricco et al., 2018). While there is a large body of research on telehealth access in rural areas, the state of the science regarding the rural profile’s influence on telehealth beliefs and preferences for use in rural areas is unclear and thus a scoping review is a necessary first step. The PRISMA-ScR checklist was used as a guideline (Tricco et al., 2018). To be included in the review, relevant literature needed to include qualitative, quantitative, or mixed methods findings explicitly related to rural residents’ attitudes or beliefs within the context of telehealth utilization. Only peer-reviewed studies were included. Due to the paucity of literature on RNT, articles did not have to reference RNT. Studies that only focused on the provider or organizational perceptions of telehealth utilization, policy briefs, commentaries, theses and dissertations, and other gray literature were excluded.
A comprehensive literature search was conducted using the following databases between May and July 2022: CINAHL, Medline, Academic Search Complete, Anthropology Plus, APA PsycArticles, Social Sciences Full Text, and PubMed. Delimiters included the English language and the geographic area of Europe, Australia/New Zealand, the United States, or Canada. Studies conducted prior to 2007 were excluded due to rapid advancements in telehealth implementation that began in 2007 with the advent of the iPhone, the conclusion of the first Veterans’ Health Administration study on telehealth, and substantial investment in rural broadband in the United States (Nesbitt & Katz-Bell, 2018). All terms were required to be found in the title or abstract. The first set of search terms used was (telehealth OR telemedicine OR eHealth OR mHealth) AND rural AND (patient perceptions OR patient attitudes). The second search included (telehealth attitudes OR telehealth perceptions) AND rural. A final search used only the PubMed database with the terms rural AND (telehealth OR telemedicine OR eHealth OR mHealth) AND (preference OR utilization). In addition to searching databases, manual citation searching was conducted using reference lists from the previously identified relevant literature.
Data charting included the following key elements: setting, including the definition of rural, if available; study sample characteristics; objectives; methods; and findings. Findings not relevant to the study objective were not included in the charting (e.g., findings from clinicians who were also interviewed, or findings that related to patient satisfaction). The findings were then synthesized into themes within extant RNT constructs.
Results
Selection of Sources
The aim of this scoping review was to understand the state of the science relative to rural attitudes and beliefs regarding telehealth utilization. A total of 312 records were found. After duplicates were removed (n = 99), there were 213 unique records. Of these, 176 were eliminated after the title/abstract review for the following reasons: being a conference abstract, protocol, or commentary (n = 9); involving only provider/organization perspectives (n = 73); not taking place in the delimited geographic area (n = 16); not rural (n = 14); not related to telehealth (n = 7); not including data on rural attitudes and perceptions toward utilizing telehealth (n = 49); data were collected prior to 2007 (n = 8). The remaining 34 articles were reviewed in full, of which 24 were eliminated due to insufficient descriptions of attitudes and perceptions toward utilization of telehealth in the rural context. Because this is a scoping review, articles were not eliminated based on quality or scientific rigor. In total, 10 articles met the inclusion criteria and were included in this review (Figure 1).
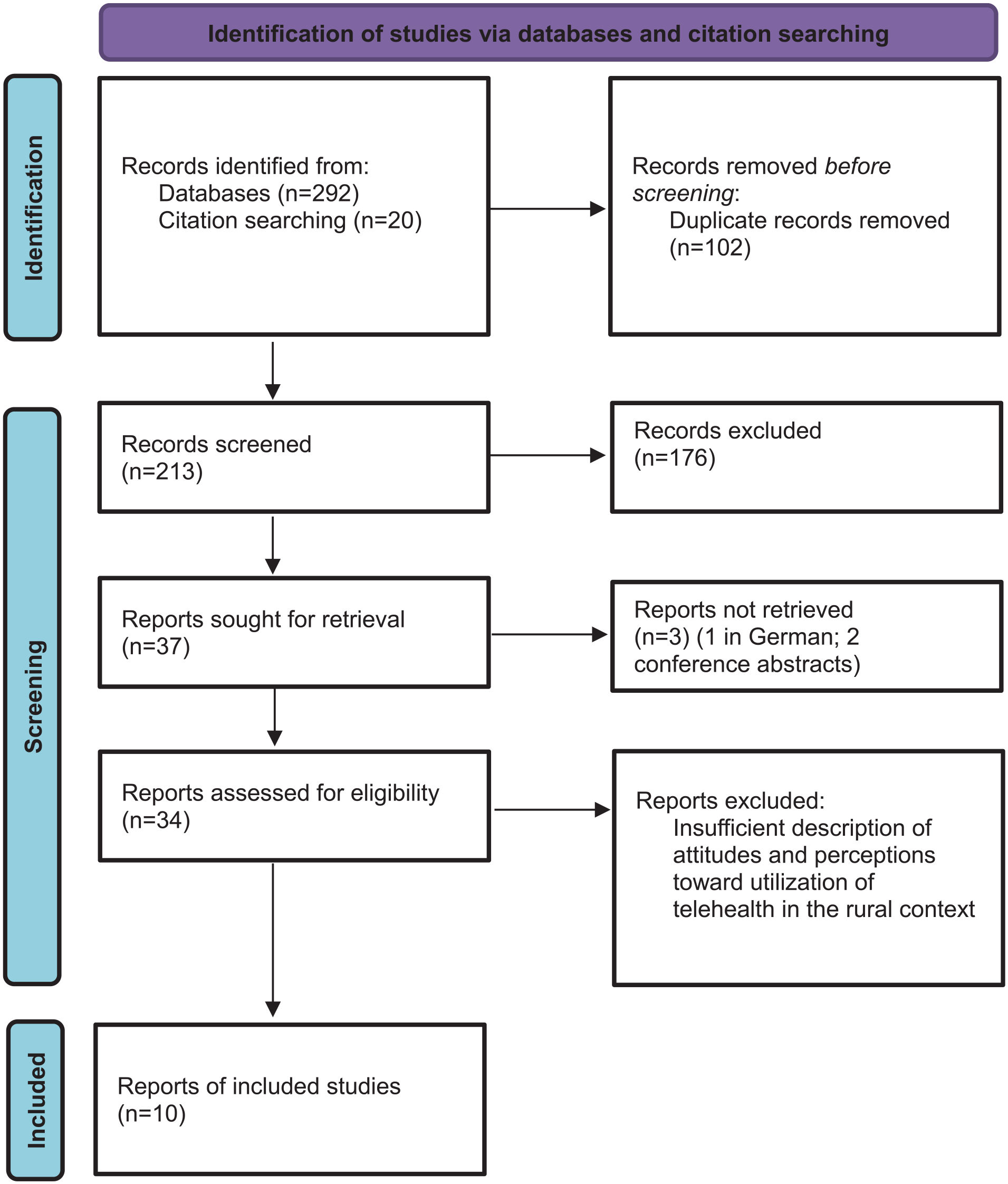
Study Inclusion Flow Diagram.
Characteristics of Sources of Evidence
The 10 articles were based on studies conducted in the United States (Alexander et al., 2021; Hubach et al., 2020; Sundstrom et al., 2020), Canada (Gibson et al., 2011; Rush et al., 2019), Sweden (Lindberg et al., 2021), or Australia (Bradford et al., 2015; Campbell et al., 2019; Rasekaba et al., 2021; Sabesan et al., 2014) (Table 1). All were published between 2011 and 2021 indicating a relatively recent interest in understanding how the rural profile may be associated with preference for and utilization of telehealth. Only one article referenced COVID-19 (Hubach et al., 2020) as a potential driving force for increased utilization of telehealth in rural populations.
Literature Review Findings.
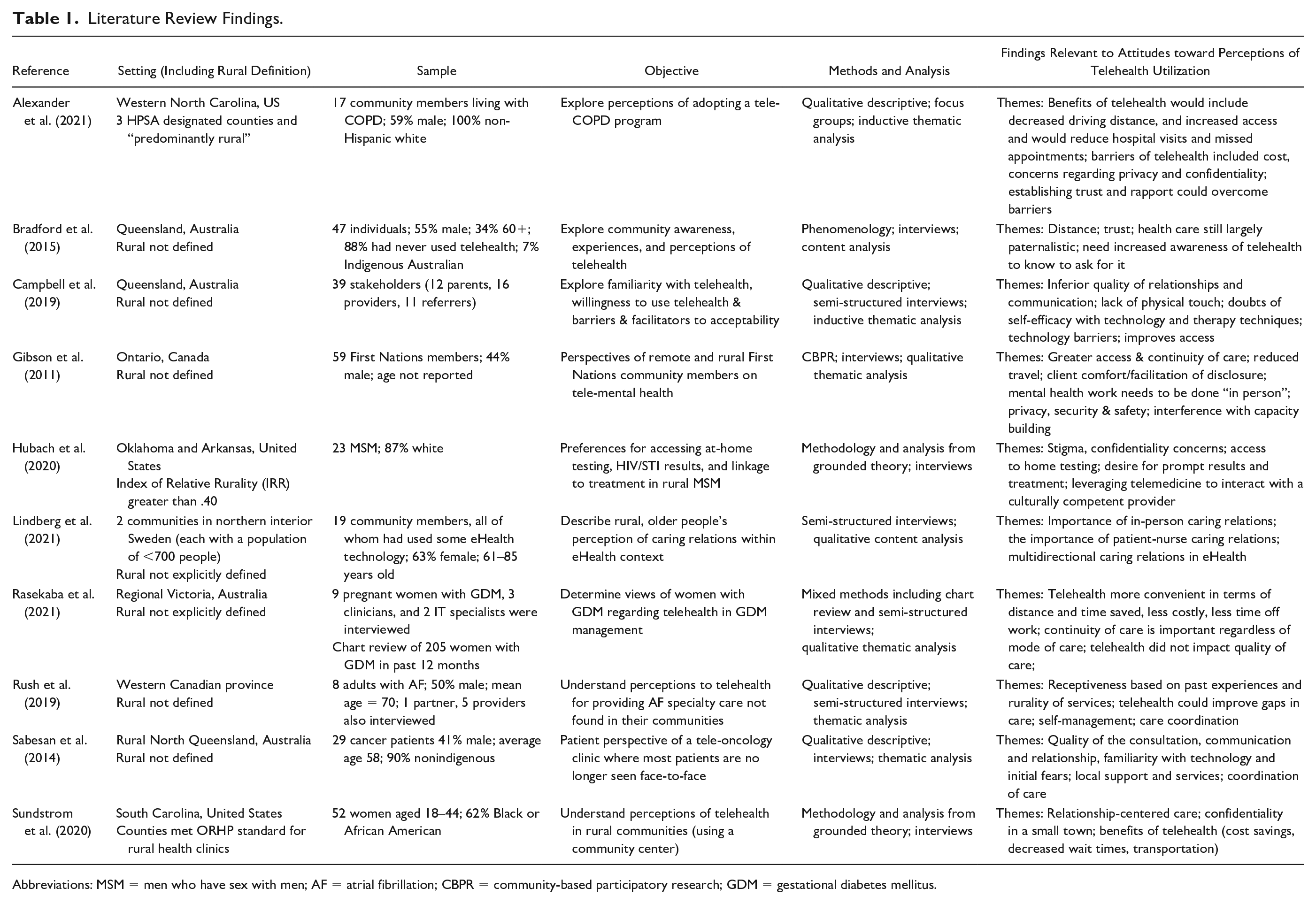
Abbreviations: MSM = men who have sex with men; AF = atrial fibrillation; CBPR = community-based participatory research; GDM = gestational diabetes mellitus.
None of the articles used RNT and only one (Rasekaba et al., 2021) referenced the use of a theoretical framework to undergird the analyses. All of the studies used qualitative or mixed methods designs. The objectives, and thus the methodologies, varied across studies. Methodologies included qualitative descriptive (Alexander et al., 2021; Campbell et al., 2019; Lindberg et al., 2021; Rasekaba et al., 2021; Rush et al., 2019; Sabesan et al., 2014), community-based participatory research (Gibson et al., 2011), phenomenology (Bradford et al., 2015), and grounded theory (Hubach et al., 2020; Sundstrom et al., 2020). In all cases, a variation of inductive thematic analysis was used to synthesize findings. Only two articles explicitly operationalized rural (Hubach et al., 2020; Sundstrom et al., 2020). Two articles mentioned steps taken to ensure the credibility and rigor of their studies (Gibson et al., 2011; Rush et al., 2019).
Sample sizes ranged from 8 to 59 individuals. There was diversity in the populations of interest among the articles. While all populations were deemed rural, individual studies focused on women seeking reproductive health care (Rasekaba et al., 2021; Sundstrom et al., 2020), adults with chronic disease (Alexander et al., 2021; Rush et al., 2019), individuals receiving cancer care (Sabesan et al., 2014), men who have sex with men (Hubach et al., 2020), Indigenous communities (Gibson et al., 2011), older adults (Lindberg et al., 2021), and parents and other stakeholders of pediatric allied health care (Campbell et al., 2019). Only one study enrolled rural community members at large (Bradford et al., 2015). It is important to note that participants in all studies acknowledged the benefits of telehealth for both the greater population, as well as for their own rural communities. No studies found that the majority of participants expressed an unwillingness to engage with telehealth technologies.
Synthesis
Importance of familiar relationships
Rural people value the familiarity of their relationships with health care providers in their communities, and they appreciate how small communities facilitate these relationships (Shreffler-Grant, 2022; Thurman et al., 2019; Weinert et al., 2005). This theme was nearly universal in the review and it speaks to the RNT concepts of trust and familiarity. Within the First Nations’ culture, Gibson et al. (2011) reported there was a general feeling that trust could not be established in a virtual context due to the lack of physical contact and thus telehealth was at times construed as inappropriate. Some parents in Campbell et al.’s (2019) study echoed these concerns regarding their children’s virtual appointments with allied health professionals.
Sundstrom et al. (2020) studied rural women’s perceptions of seeking reproductive health care via a community telehealth center. The participants in this study expressed concern over the ability to trust a provider via telehealth and described mediated communication as impersonal. Older rural adults in Lindberg et al.’s study also believed that face-to-face interactions were critical for establishing authentic, caring relationships (Lindberg et al., 2021). The recent focus on digital solutions at the local clinics even made some participants wary of using local in-person health care since staff were being hired for their digital competence instead of their interpersonal skills.
Rural individuals often indicated that they would be comfortable using telehealth after they had initially met the provider face-to-face (Alexander et al., 2021; Gibson et al., 2011; Lindberg et al., 2021; Rasekaba et al., 2021; Rush et al., 2019; Sabesan et al., 2014). Alternatively, during telehealth interactions that took place within a clinic setting, having a local nurse or medical assistant was seen as comforting to some patients (Gibson et al., 2011; Rush et al., 2019; Sabesan et al., 2014).
Findings from Hubach et al.’s (2020) research describing preferred methods of HIV/STI screening in a sample of rural men who have sex with men are somewhat discordant with the other articles. In this study, participants struggled with stigma from their local providers and the fear of being outed within their communities. For participants in this study, it was difficult to form close relationships with the local providers and having the option to use telehealth to communicate with an LGBTQ-affirming provider was seen as a benefit.
Concerns with privacy and confidentiality
Lack of anonymity is one of the original concepts from RNT (Long & Weinert, 2022). The related concepts of privacy and confidentiality remain important factors in terms of health-seeking behaviors among rural populations (Swan & Hobbs, 2018). In this review, even though people living in rural areas were accustomed to the lack of anonymity in their communities, some were concerned with the privacy and confidentiality of their health information and how the mediated use of technology may infringe upon their privacy. In total, 4 of the 10 studies raised confidentiality and privacy concerns related to telehealth. There are some nuances that will be important to note, particularly concerning how telehealth services are delivered and the relative risks of familiarity versus confidentiality in a small town.
If telehealth was offered in a community location, some people expressed concern that everybody in town would know their business. There were concerns about people being able to overhear their conversations even if the encounter took place in a private office (Gibson et al., 2011; Sundstrom et al., 2020). Some participants in the reviewed studies expressed apprehension about their conversation being recorded without their knowledge; that others would be listening in on the other end; and voiced concerns regarding data theft (Alexander et al., 2021; Sundstrom et al., 2020). These concerns are also related to the concept of trust, and participants described the need for reassurance that the technology would not violate their privacy (Sundstrom et al., 2020).
Alternatively, telehealth could be seen as protecting privacy and confidentiality. Hubach et al. (2020, p. 472) noted that “accessing care locally could mean attending clinics where community members worked and create opportunities for confidentiality to be breached.” In small communities, it is difficult to remain anonymous. Thus, telehealth may create a safer, more private environment than face-to-face encounters for stigmatized health concerns.
Acceptance of limited access to care
According to RNT, place shapes one’s broader worldviews, leading to an acceptance of the limitations of living in a rural area (Lee & McDonagh, 2018). In Rush et al.’s study on telehealth perspectives for older rural adults with atrial fibrillation, patients who were satisfied with their current rural health services could not articulate how telehealth would improve care (Rush et al., 2019). The authors described this as “a rural mindset that was accepting of what they had and pride in looking after themselves, suggesting subtle resistance to the intrusiveness of telehealth” (Rush et al., 2019, p. 139). Lindberg et al. (2021) noted that some of their participants would rather wait until the local doctor was available at the rural clinic instead of using telehealth for perceived nonurgent concerns. Other individuals living in remote areas were willing to travel over the course of several days to meet with a specialist as they did not consider any alternative ways to receive health care (Bradford et al., 2015).
This acceptance of living in a rural area incorporates the concept of self-reliance. Rural residents understand that living in a rural area means there will be limited and sparsely distributed resources. This sense of self-reliance also reinforces an insider–outsider perspective. Some study participants had a difficult time understanding the benefits of telehealth—an “outsider” technology—and therefore expressed an unwillingness to use it (Bradford et al., 2015; Campbell et al., 2019; Rush et al., 2019). Other participants commented that implementing telehealth services would limit capacity-building efforts within the rural community (Gibson et al., 2011).
Resourcefulness and frugality
According to RNT, the concepts of resources and distance impact health-seeking behaviors (Lee et al., 2019). Rural characteristics include resourcefulness and frugality (Mennenga et al., 2022), and participants in most of the studies endorsed using telehealth because it was economical (Alexander et al., 2021; Bradford et al., 2015; Gibson et al., 2011; Rasekaba et al., 2021; Sundstrom et al., 2020). Telehealth is a particularly useful tool to reduce travel time and costs. Telehealth could alleviate the transportation issues that some rural residents indicated were a barrier to receiving care especially if they did not have their own vehicle or had to travel many hours while not feeling well (Bradford et al., 2015; Rasekaba et al., 2021; Sabesan et al., 2014; Sundstrom et al., 2020).
In addition to saving time and money, telehealth was also able to alleviate some of the emotional stresses associated with visiting a provider’s office. Participants often reported feeling less vulnerable and more relaxed interacting with their providers through telehealth (Bradford et al., 2015; Campbell et al., 2019; Gibson et al., 2011; Hubach et al., 2020; Sundstrom et al., 2020). Telehealth also allowed participants to avoid long waits in potentially crowded waiting rooms (Sabesan et al., 2014; Sundstrom et al., 2020).
The RNT concept of self-reliance connects to the theme of resourcefulness and frugality. The adage “necessity is the mother of invention” is mentioned in Jakobs’ (2022) discussion of self-reliance in frontier communities. Connecting to health care in a way that is not only more cost-effective but also potentially gives the patient more autonomy and flexibility, demonstrates this independent spirit and the ability to get by with limited resources.
Discussion
In this scoping review, 10 studies addressing how the rural profile influences beliefs about telehealth utilization were identified. Four themes were developed: the importance of familiar relationships, concerns with privacy and confidentiality, acceptance of limited access to care, and frugality and resourcefulness. These themes contained robust RNT concepts including trust, familiarity, lack of anonymity, place, self-reliance, resources, and distance.
Similar themes are found in the larger body of literature regarding rural health-seeking behaviors (Brown & Schafft, 2019; Cheesmond et al., 2019; Fennell et al., 2018; Lee et al., 2022; Thurman et al., 2019). A pervasive “rural deficit” discourse has led some rural individuals to feel they are second-class citizens and has emphasized the unwritten cultural norms regarding power relationships and inclusion and exclusion practices in rural communities (Simpson & McDonald, 2017). This distrust or mistrust of newcomers and outsiders (and by association, the technology they bring) may contribute to slower adoption of telehealth in rural areas (Brown & Schafft, 2019; Lee et al., 2022).
In addition, rural communities are generally closely knit due to limited social networks and scarce resources (Keller & Owens, 2020; Maclaren, 2018; Phillips & McLeroy, 2004). There is a relative lack of anonymity, and according to RNT, a general expectation among both clinicians and patients is that they will know one another on both a professional and personal level (Glover, 2019; Paré et al., 2022; Scharff, 2022). Therefore, interactions with health care providers tend to be more relational than transactional (Farmer et al., 2012; Scharff, 2022), which may also lead to a preference for in-person health care interactions. Conversely, this sense of tight community may also encourage some individuals to use telehealth when they realize that doing so would alleviate some pressure on their local health care staff and free up availability for other patients in the community who may need the in-person care more urgently (Lindberg et al., 2021).
Implications for Policy, Practice, and Research
There is an assumption that people living in rural areas will utilize telehealth if they have the technological capabilities, in terms of infrastructure and digital literacy. Thus, recommendations for programs and policies are focused on increasing broadband access and providing people with the appropriate resources they need in order to use telehealth (DeGuzman et al., 2020; Shaw et al., 2021). This review indicated that equipped with these resources, many rural people are amenable to telehealth because of the associated time and financial savings. However, clinicians and policy makers also need to understand that the unique rural profile shapes beliefs about telehealth utilization. Again, due to this perception of being “less than,” and similar to other disparate groups, a trusting rapport needs to be established between providers and rural community members in order to make telehealth an effective and acceptable form of care delivery. Lindberg et al. (2021) and Currie et al. (2015) have suggested that health care administrators, nurses, and clinicians should consider framing telehealth not as replacing traditional care, but as supplementing it. That is, individual clinicians should be using a mix of in-person and telehealth interactions instead of relying on separate telehealth-only teams. The initial in-person visit prior to engaging in telehealth seems to be important for many rural people in order to establish trust and rapport and assuage any concerns about breaches of privacy. Similarly, having trusted local nurses or clinicians present during a telehealth encounter originating from a local clinic may be an essential strategy to encourage telehealth adoption. The review also indicated the dearth of data available regarding the rural profile and perceptions of telehealth utilization. While the intent of the study was not to assess actual utilization, future research efforts could explore the relationship between the rural profile and telehealth uptake.
Limitations
There are several limitations to this scoping review that must be acknowledged. First, search criteria were limited to developed nations that have large rural populations. Understanding rural perceptions of telehealth access in developing countries was not the intent of this review. However, the delimiters placed on geography could have excluded some relevant studies. Second, there was a paucity of literature regarding how the rural profile may impact telehealth acceptance and utilization using the defined search terms. Future work could undertake a more systematic review, particularly now that the COVID-19 pandemic has prompted numerous studies related to telehealth implementation in rural settings. It may be helpful to include audio-only telehealth as a search term to broaden results and inform findings. Third, all but one of the evaluated studies examined marginalized populations which limits generalizability.
Conclusion
The results from this scoping review revealed that there is a large gap in the knowledge base pertaining to how the rural profile contributes to beliefs about telehealth utilization. RNT is an applicable, yet underutilized, a middle-range theoretical framework that could be used to explore this topic further. Understanding how the rural profile can influence a person’s decision to use telehealth under various circumstances is not only important for nurses and other health care professionals but is critical to public health initiatives as well. The improvements in broadband access in rural areas will certainly help alleviate barriers to health care for some individuals. But unless rural health-seeking behaviors are accounted for when implementing telehealth programs, it is likely that the disparity in access to health care will only increase.
Footnotes
Authors’ Note
The author Kristin Pullyblank is also affiliated with Decker College of Nursing and Health Sciences, Binghamton, NY.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.