
Abstract
HIV continues to impact people of color disproportionately. In 2015, Black Americans accounted for 42% of those living with HIV, and Latinx individuals accounted for 30% of new diagnoses. Using a sample of 364 people of color, demographic data, HIV testing history, and interactions with health care providers were collected. Over half of the participants (59.3%) had never been offered an HIV test, and only 19% reported a provider had offered an HIV test once, followed by 14% who have had a provider offer an HIV test more than once. Participants who were offered an HIV test once were 13.23 times more likely to report a history of HIV screening, and those offered an HIV test more than once were 18.02 times more likely to report a history of HIV testing. Participants who reported feeling a “little” judged were 6.85 times less likely to report being screened for HIV.
Despite considerable progress in the fight against HIV, it remains a significant public health issue. An estimated 1.1 million people are living with HIV in the United States. Of these living with HIV, approximately 156,000 (13.3%) were unaware of their infection. 1 In 2019, about 31,000 new HIV infections were reported in the United States, with persons of all races, genders, and sexual orientations represented. 2 The effects of HIV continue to disproportionately fall on Black individuals, who comprise 41% of those living with HIV despite comprising only 13% of the US population. 3 Gay and bisexual men of color have proportionally higher rates of HIV than any other group, with three times the incidence. 4 A systematic review examining HIV between 2006 and 2017 reported that Black transgender women had the highest HIV prevalence (56.3%). 5 Furthermore, among the races and ethnicities evaluated, Black Americans had the highest mortality rate linked with HIV. 6
Latinx individuals are also disproportionately burdened with HIV. Hispanic/Latinx accounted for 30% of all HIV infections in 2019 yet represented only 18% of the US population. 7 Hispanic/Latinx males are four times more likely to have HIV/AIDS and twice as likely to die from it than non-Hispanic white males, according to data from the Centers for Disease Control and Prevention (CDC). 7 Hispanic/Latinx women experienced a similar increase in HIV rates relative to non-Hispanic white women: in 2019, Hispanic/Latinx women were four times as likely to have HIV/AIDS. Additionally, as many as 25% of Hispanic/Latinx transgender women are HIV positive. 5
Lack of knowledge regarding one's HIV status, particularly among Hispanic/Latinx men who have sex with other men (MSM), is a significant concern regarding HIV/AIDS rates among Hispanics/Latinos. This may result from underreporting individual risk factors or fewer opportunities to get tested. 6 In addition, the disproportionate burden of HIV among Black and Hispanic/Latinx communities in the United States illustrates the need for targeted preventive efforts and explicit endorsement from medical professionals.
There are several methods for preventing HIV infection, including using condoms during sex, preexposure prophylaxis (PrEP) for HIV prevention, viral suppression among those living with HIV, and routine testing. The CDC recommends that everyone aged 13 to 64 receive HIV testing at least once in their lifetime. However, individuals at increased risk benefit from more regular screening. For example, the CDC recommends that sexually active MSM and users of illicit drugs be screened for HIV at least once a year, with those considered at the highest risk getting tested every three to six months.
Despite screening recommendations, many people are unaware of their HIV status. Approximately 13% of the 1.2 million people (156,000 people or about 1 in 7) living with HIV in the US are unaware of their status. HIV testing is an essential first step in stemming the spread of HIV and lowering HIV-related morbidity and mortality. Furthermore, a lack of awareness of one's HIV status accounts for approximately 37% of new HIV diagnoses. 8 Because of the potential lack of understanding about HIV, many people are fearful or in denial about getting screened for the virus. However, if medical professionals take an opt-out approach to screening, they may be able to move beyond barriers and begin a conversation about care.
Opt-out testing is an approach to HIV care in which screening is part of routine medical care. 9 With this approach, the clinician discusses the benefits of HIV screening with the patient and offers the choice to accept or reject the test. However, many providers continue to follow an opt-in approach, which operates under the assumption that if the test is needed, the patient will request it, placing the burden of initiating HIV screening on the patient. In addition, an opt-in testing approach is frequently cited as a barrier to identifying individuals who are unaware of their infection, making it more challenging to connect them with appropriate prevention or treatment plans of care.10,11
Opt-out testing has proven to be instrumental in increasing the rate of HIV testing, 12 moving us one step closer to achieving the Ending the HIV Epidemic (EHE) initiative goals. 13 The first goal of EHE is to diagnose all patients with HIV as early as possible. 13 Moreover, previous research has shown that missed clinical opportunities are a significant barrier to decreasing the rate of infections. In a study by Liggett et al., patients typically met with their health care provider four to five times before receiving their HIV diagnosis. 14 Their findings suggest that an opt-out testing approach may lead to earlier identification; and quicker access to pre-exposure prophylaxis or antiretroviral therapy (ART) for viral suppression.
Purpose
Marion County, located in central Indiana, is one of 48 counties throughout the United States to be included in Phase 1 of the EHE initiative. The initiative was announced in 2019 to reduce the incidence of HIV by 75% by 2025 and by 90% by 2030. 13 HIV testing is a critical component of EHE; therefore, understanding how health care providers can improve the HIV testing rate among at-risk populations is essential. Aligning with the EHE initiative, the present study was developed to better understand patient and provider communication and the resulting influence on HIV testing. Specifically, we wanted to know whether there is a link between provider-initiated HIV testing and self-reported history of HIV testing among persons of color in Indiana.
Methods
A cross-sectional study examining predictors of HIV testing among Black and Latinx individuals in Indiana was conducted from March 19th through April 16th, 2021. Inclusion criteria are as follows: (a) at least 18 years of age, (b) current resident of Indiana, and (c) identify as Black or Latinx. Participants were required to read a study summary and provide electronic consent before accessing the survey.
Participants were recruited via Qualtrics participant panels. The use of Qualtrics participant panels allows for the collection of data from traditionally hard-to-reach populations while also providing an incentive for completion. 15 In fact, past research has demonstrated that Qualtrics panels more accurately reflect the US population than other recruitment methods. 16 Furthermore, this approach assists in ensuring that participants meet the inclusion criteria, thereby preventing those who do not from contributing to the study. Each participant received an incentive for their time and participation. The distribution of incentives was managed by Qualtrics. The study was deemed exempt and the Indiana University Institutional Review Board approved all materials and procedures (protocol #2007595098).
An attention check question was integrated into the survey to help ensure high-quality responses. This approach has been described in survey literature and has proven to help address quality issues in online survey completion. 17 The question developed for this study asked participants to select one specific response from four options. If the participant did not answer the question as directed, they were removed from the survey and not included in the final analysis. A total of 426 participants initiated the survey prior to close. In total, 52 participants did not complete at least 90% of the survey, and an additional ten did not pass the instructional attention question resulting in a final sample size of 364.
Measures
Demographic variables measured included gender, race and ethnicity, age, and sexual identification. Participants were asked to identify the race and ethnicity they most closely identified with by selecting one of the following options: Black/African American/African Diaspora, more than one race including Black/African American/African Diaspora, Hispanic/Latino or Spanish; More than one race including Latin/Hispanic/Spanish, more than one race including Latin/Hispanic/Spanish. The categories of Black and Latinx were created owing to a smaller number of responses in the multiracial options. Sexual identification was assessed with one question developed for this survey. Participants were asked to select one of seven options (straight, gay, lesbian, bisexual, asexual, questioning/unsure, or other).
Previous sexually transmitted infection testing
Previous sexually transmitted infection (STI) testing was assessed with one question developed for this survey where participants were asked to answer the question have you ever been tested for any sexually transmitted infections (syphilis, gonorrhea, chlamydia for example), and were instructed to pick one of three options (no, yes, I do not know).
Provider-initiated HIV screening
Whether a health care provider has offered an HIV test was assessed by one question developed for this survey. Participants were asked has a healthcare provider (physician, nurse, nurse practitioner, etc.) ever offered to give you an HIV test and instructed to pick one of the following four options: (1) offered an HIV test once, (2) offered HIV test more than once, (3) not offered HIV test, (4) unsure if provider offered HIV test.
Feeling judged when offered HIV test
To understand if participants felt judged when offered an HIV test, they were asked the question, when a healthcare provider offered you an HIV test, did you feel like they were judging you? Potential responses are as follows (1) did not feel judged at all, (2) did not really feel judged, (3) felt a little judged, and (4) definitely felt judged.
Data Analysis
Statistical analysis was conducted in three phases. First, study variables were analyzed descriptively via univariate analysis. Second, chi-square tests examined the association between each predictor variable and the dependent variable. Finally, the relationship between the dependent variable (history of HIV testing) and independent variables (race and ethnicity, gender, sexual identification, STI testing, the provider offered HIV test, feeling judged when offered HIV test) was explored using a binary logistic regression model. All data analyses were conducted using SPSS version 28, and the statistical significance level was set at p < .05. Due to a low representation in specific sexual identification categories, gay, lesbian, bisexual, asexual, and questioning/unsure were combined to make one LGBTQ+ variable. A power analysis was conducted using G*Power 3.1.9.2 to estimate the necessary sample size and indicated that 337 participants would provide sufficient statistical power to detect a medium effect size between the independent and dependent variables. 18 Assumptions of chi-square and logistic regression tests were checked prior to analysis.
Results
The participants' most common race or ethnicity was Black (67.3%, n = 245), and 8.2% (n = 30) identified as multiracial, including Black. This was followed by 17.3% (n = 63) and 7.1% (n = 26) who identified as Latinx and as more than one race including Latinx, respectively. Most participants were between 18 and 24 years old (51.1%, n = 186), and a majority identified as female (64.6%, n = 235). For education level, 34.1% of the participants reported completing high school (n = 124) and 23.4% (n = 85) reported completing some college but not attaining a degree. Most participants identified as straight (74.7%, n = 272), 14.3% (n = 52) identified as bisexual, and 4.7% (n = 17) identified as lesbian. Over half of the respondents (53.6%, n = 195) have never been tested for HIV, and 22.5% (n = 82) have been tested once. A summary of participant demographics can be found in Table 1.
Participant Demographics of HIV Testing among Black and Latinx Individuals in Indiana (N = 364).
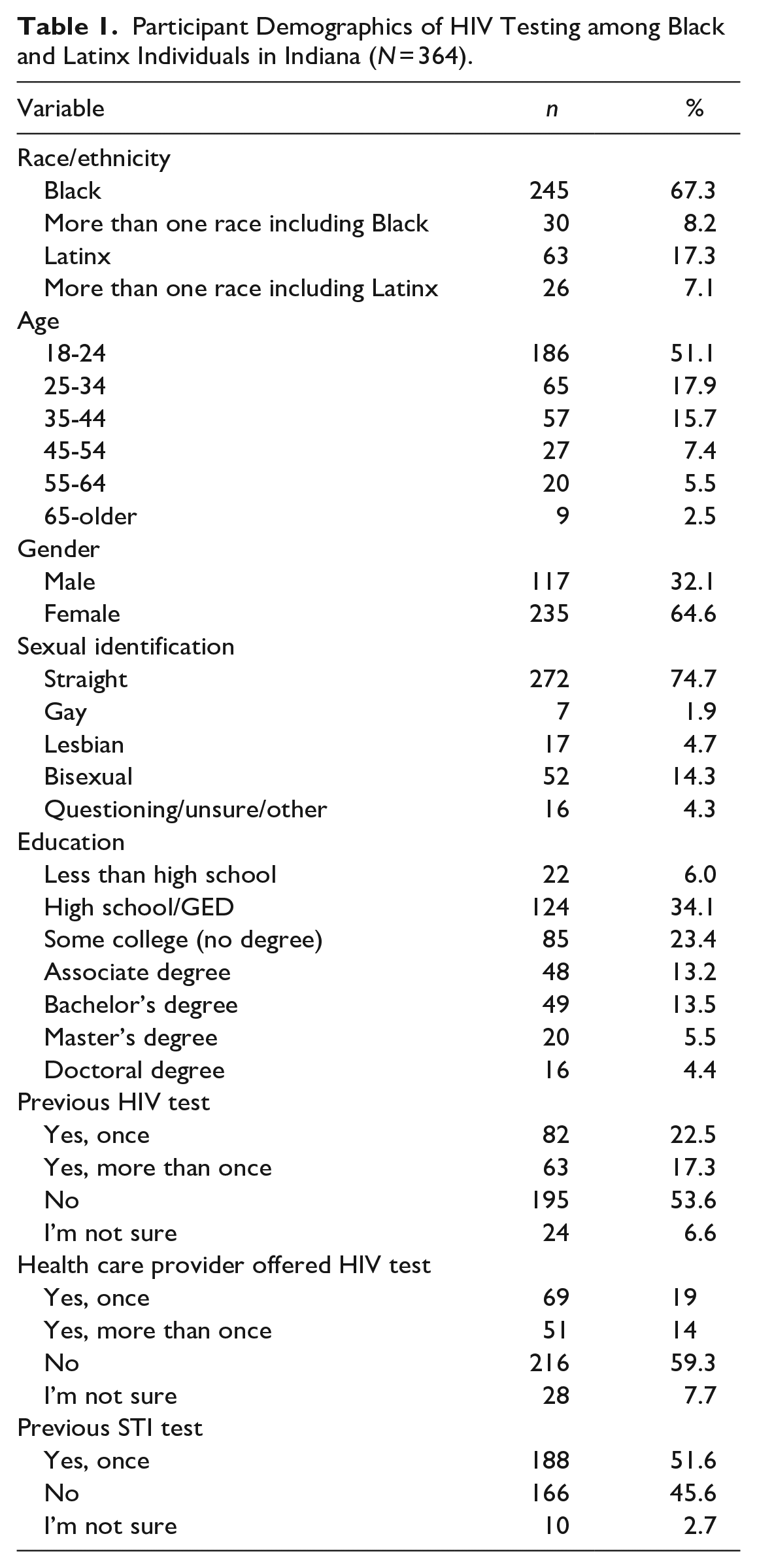
Most participants stated that a health care provider never offered them an HIV test (59.3%, n = 216), and 69 (19%) reported that a health care provider had once offered them an HIV test. Only 14% (n = 51) had a health care provider offer them an HIV test more than once. The majority reported not feeling judged “at all” when offered an HIV test (17.3%, n = 63) and 7.7% (n = 28) reported “not really” feeling judged when offered an HIV test. Over half of the participants (54.6%, n = 188) reported receiving an STI test.
A chi-square test for association was conducted between previous STI testing and a history of HIV screening. All expected cell frequencies were greater than five, and there was a statistically significant association between STI and HIV testing (χ2(2) = 106.5, p < .001), with a strong relationship between STI and HIV testing (Cramer’s V = 0.541, p < .001). A chi-square test was also used to examine the association between reporting a history of health care providers offering an HIV test and previous HIV screening. All expected cell frequencies were greater than five, and there was a statistically significant association between a health care provider offering an HIV test and being tested for HIV (χ2(2) = 84.8, p < .001). In addition, there was a medium association between the two variables (Cramer’s V = 0.483, p < .001). Chi-square tests examining race, gender, and feeling judged did not yield significant results.
A binary logistic regression was performed to ascertain the effects of race and ethnicity, gender, health care provider offering HIV testing, sexual identification, health care providers giving the opportunity to ask health-related questions, previous STI testing, and feeling judged when offered an HIV test on the likelihood that participants have been tested for HIV. The model was statistically significant (χ2(14) = 180.2, p < .001), and explained 54% (Nagelkerke R 2 ) of the variance in HIV testing and correctly classified 79.3% of cases. Sensitivity was 64.1%, specificity was 89.5%, positive predictive value was 80.5%, and negative predictive value was 78.7%. In total, 4 of the 13 predictor variables were statistically significant (provider offered HIV test once, provider offered HIV test more than once, I felt a little judged when offered HIV test, and previous STI test).
Participants who had a health care provider offer them an HIV test once had 13.23 higher odds of being tested for HIV (95% confidence interval [CI] [5.093, 34.387]). Participants who were offered an HIV test more than once had an 18.02 higher odds of being tested for HIV (95% CI [6.065, 53.566]). Individuals who reported feeling a little judged had 6.85 times lower odds of being tested for HIV (95% CI [1.80, 26.32]) compared with those who did not feel judged obtaining an HIV test. Furthermore, participants who reported previous STI screening had 15.87 higher odds of being tested for HIV (95% CI [8.017, 31.422]) compared with those who have never been screened for STI’s. Binary logistic regression results can be found in Table 2.
Logistic Regression Predicting Likelihood of HIV Testing among Black and Latinx Individuals in Indiana (N = 364).
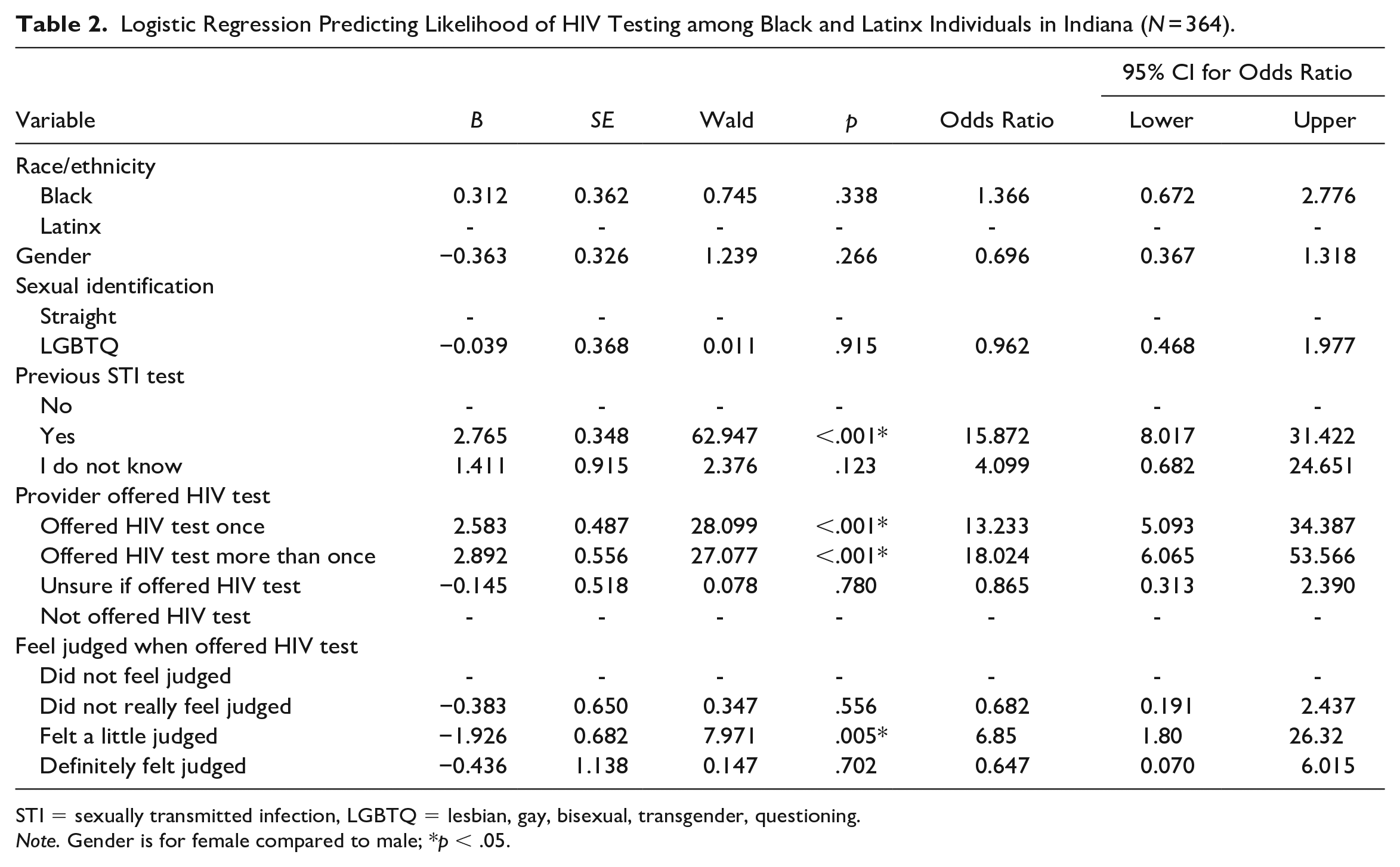
STI = sexually transmitted infection, LGBTQ = lesbian, gay, bisexual, transgender, questioning.
Note. Gender is for female compared to male; *p < .05.
Discussion
According to recent research, the number of new cases of HIV has decreased dramatically among most populations. 6 However, people of color represent the most significant proportion of new diagnoses. Therefore, the EHE initiative focuses on expanding prevention and screening measures to decrease HIV incidence by 90% by 2030. One of the primary steps in addressing the epidemic among people of color is identifying those unaware of their status. Because approximately 14% of people of color are unaware of their HIV-positive serostatus, increasing efforts to screen individuals is essential in reducing the spread of HIV.8,19
Negative experiences with a health care provider are often cited as a reason to avoid HIV testing. 20 This particularly is cited alongside stigma and discrimination, being uncomfortable or hesitant discussing the topic, and fear. 21 Therefore, perhaps the most clinically relevant finding from our study is the importance of provider communication concerning the uptake of HIV testing. With better provider-initiated, whole-person approaches to HIV testing, a reduction in stigma and fear of HIV could be realized by initiating a conversation between provider and patient. Health care providers may find this an excellent opportunity to promote open communication. Proactive sexual health conversations can significantly impact the patient/provider dynamic, where the patients are no longer responsible for inquiring about HIV care, and health care providers can lead the discussion.
There are several ways to begin the conversation, but establishing a trusting, open, and nonjudgmental atmosphere and developing a courteous relationship are critical. HIV screening rates among Black and Latinx patients in the United States are unacceptably low. Our study found that participants who reported previous HIV testing were significantly more likely to have their provider offer them an HIV test during a health care visit. Results from our study indicate that participants who had their primary care provider offer an HIV test to them once had a 13.23 increased likelihood of testing for HIV. However, those participants who had a provider offer HIV testing more than once were 18.02 times more likely to report HIV testing. These findings support previous studies that found that using an opt-out approach to HIV testing is an effective way to improve uptake. 22
Providers must be educated on the significance of addressing the topic of sex and sexual health, particularly in the context of HIV, to lower transmission rates and promote a culture of whole-person health. A great deal of the literature describes how a provider's sense of discomfort contributes to their ability to screen every patient for HIV.23,24 While conversations about HIV and sexual health may be uncomfortable, practicing communication skills and fine-tuning them can ultimately help improve patient outcomes. Providers who conveyed HIV prevention information judgment-free were more likely to have patients who reported being tested for HIV. In contrast, providers who delivered HIV prevention education in a way regarded as judgmental by patients were less inclined to have people test for it. These results underscore the significance of the patient/provider relationship. Stigma and prejudice against persons living with HIV have previously been shown to deter them from getting tested for the virus.25,26
There is still much progress to be made when it comes to HIV testing and other sexual health screenings for marginalized racial and ethnic groups. Too frequently, these communities are excluded from the conversation, leaving them without appropriate care and assistance. However, there are some promising efforts underway that are attempting to alter this. EHE is one initiative that aims to improve HIV screening and treatment by combining various disciplines. To reduce new HIV infections by 90% by 2030, EHE has developed a series of targets geared toward HIV prevention. One of the main goals is to make people aware of their condition and link them to treatment or prevention plans. According to a recent study by Hutchinson and Dhairyawan, obtaining an HIV test is often stigmatized due to cultural HIV and STI stigma. 26 Many individuals who have acquired a late HIV diagnosis interact with health care providers and do not receive an HIV test. Many people who find out they have HIV late in the progression report that, in previous interactions with health care providers, no testing was ever offered. Therefore, breaking down barriers to universal HIV screening should be a top priority.26,27
According to our results, receiving prior STI screening was associated with a considerably higher chance of having been tested for HIV. A recent study examining STI testing after an HIV diagnosis found that most participants had interacted with HIV/STI services more than once before their HIV diagnosis, and most reported a positive STI diagnosis prior to their HIV diagnosis. 28 With the introduction of PrEP, providers and patients have access to an efficacious prevention plan. And to reach those at the most significant risk of HIV acquisition, we must also examine the process of STI screening and recognize that individuals diagnosed with an STI also have an increased risk of HIV acquisition.
The present study has some limitations worth noting. First, only Black and Latinx men and women from Indiana were included in the study. Therefore, we cannot compare the experiences of men or women who do not identify as Black or Latinx or who live outside Indiana. The study's cross-sectional design means we can describe relationships between the variables; however, we cannot determine causality. The results of this study are also unable to describe the content of the conversation between the health care provider and the patient regarding HIV. Future research focusing on the context of the HIV screening conversation is required to understand how clinical conversations influence HIV screening. Concerning the identification of race and ethnicity, the way demographic questions were constructed, we can describe our participant population in terms of Black and Latinx, including those who identify as multiracial, including Black or Latinx. However, we cannot describe those who may identify as Afro-Latino. Despite the noted limitations, this study found that there may be a positive relationship between Black and Latinx people whose health care provider offers HIV screening and those who report a history of HIV screening. Future research is required to better understand how the content and tone of conversations concerning HIV among Black and Latinx individuals influence linkage into the HIV continuum of care.
Footnotes
Author’s Note
Anita Ohmit is now affiliated with Indiana Minority Health Coalition, Indianapolis, IN, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by a grant from the Indiana Minority Health Coalition