
Abstract
Emerging adults with diabetes, particularly in underserved communities, represent a growing but less studied population whose needs may differ from older adults. This study investigated perspectives of underserved emerging adults regarding diabetes self-management influences and provider interactions. Focus groups and interviews with emerging adults in a safety-net health care setting were conducted to identify perspectives regarding self-management influences and patient-provider interactions. Diabetes was perceived as a psychological burden complicated by busy lifestyles and competing responsibilities. Lack of resources, especially financial barriers, also limited self-management. Participants often perceived diabetes visits as standardized encounters providing access to diabetes supplies but desired additional guidance appropriate to their needs and life-stage. Participants valued encouragement and positive ongoing provider relationships for tailored informational and emotional support and support from family and peers. Providers and health care systems adapting to provide or facilitate this support will be better able to optimize diabetes management at and between visits.
Keywords
Emerging adulthood is a distinct developmental stage of transition from adolescence to full adulthood. Emerging adulthood (ages 18-29 years) is characterized by demographic diversity and instability as individuals seek to become self-sufficient. 1 Emerging adults coping with a chronic disease such as diabetes confront additional life challenges, particularly for a disease which requires an extensive degree of ongoing self-management and health system engagement. 2 The incidence of type 1 and type 2 diabetes among children and adolescents continues to increase, especially among racial and ethnic minority youth. 3 With this increasing number of youth with diabetes, more emerging adults will be living with diabetes.
Emerging Adulthood and Diabetes Care Challenges
The period of emerging adulthood presents a critical time for the development of lifelong habits of self-care behaviors for a population that will be managing diabetes and seeking to mitigate potential complications of diabetes for many years. Research to date suggests diabetes outcomes are less than optimal for emerging adults with diabetes (EAWD). Many EAWD do not achieve target HbA1c, and engagement in self-care behaviors has been observed to be less than optimal.4-6 For emerging adults with type 1 diabetes, HbA1c may peak in late adolescence with increasing, though not optimal, control through emerging adulthood. 5 For emerging adults with type 2 diabetes, HbA1c may increase over emerging adulthood. 6 Poor psychosocial outcomes such as diabetes-related distress are higher among EAWD compared to other adults with diabetes. Younger adults (21-44 years) with type 2 diabetes are less likely to engage in follow-up care compared to older adults, and emerging adults with type 1 diabetes are less likely to engage in follow-up after transitioning to adult care.7-9 For underserved EAWD, health outcome disparities may be even more pronounced. For instance, minority and socioeconomically underserved EAWD are more likely to have poorer diabetes self-management, higher loss to follow-up and higher HbA1c after transition to adult care, and greater diabetes-related distress relative to other EAWD.10-12
Gaining a better understanding of challenges that EAWD confront within adult care systems will allow tailoring of interventions to provide care and guidance appropriate to their life circumstances. While a growing but limited body of research has provided some insight into challenges, a significant amount of EAWD research and intervention focuses on the transition from pediatric to adult care. Less is known about EAWD needs within adult care settings, particularly among underserved EAWD. Current research suggests that factors such as balancing life priorities and diabetes management, economic barriers, the degree of support, and the quality of relationships with health care providers may impact diabetes self-management and perceptions of adult care services among EAWD.9,13-15
However, further insight into the experiences of EAWD, particularly in underserved communities, is necessary to improve EAWD care. The purpose of this study was to investigate the needs and experiences of underserved EAWD within adult care through exploration of perspectives of EAWD receiving care within a safety-net health care system to gain insight to better serve this population. In particular, the aims of this study were focused on investigating perceptions of EAWD regarding (1) factors that influence their diabetes self-management, (2) interactions with their adult diabetes care providers (defined as physicians, advanced practice nurses and physician assistants, nurses, and other health care support staff) during diabetes appointments, and (3) wants and needs during their diabetes care visits to support diabetes management.
Methods
Study Design and Participant Recruitment
The study used a qualitative descriptive design. 16 Study participants were recruited from a diabetes care center within an urban public safety-net hospital in Georgia, USA. As a safety-net hospital, the majority of care is provided to individuals living in medically underserved communities—communities that might not otherwise have access to health care. Most patients are individuals with limited income and who are underinsured or lack medical insurance, particularly individuals from racial and ethnic minority groups. Care is provided regardless of ability to pay. At the diabetes clinic used in this study, patients are typically scheduled for regular follow-up 2 to 4 times annually. During visits, the medical assistant assesses vital signs, and the patient then meets with their designated nurse to review medications, blood glucose values, and any issues since their last visit. The endocrinologist covering clinic that day will then see the patient, review the collected information, and make medication adjustments.
This study was approved by the Emory University Institutional Review Board (IRB00109307) and given administrative approval from the hospital system prior to study activities. A list of eligible participants was generated from electronic health records from November 2018 to November 2019. Based upon seminal work regarding emerging adulthood and a preliminary demographic review of the diabetes clinic patient population, 1 patient eligibility for recruitment included those aged 18 to 30 years with a diagnosis of type 1 or type 2 diabetes. To ensure participants could speak to the adult care experience within this public care setting, recruitment was limited to diabetes clinic patients who had attended an appointment in the hospital’s diabetes care center or primary care clinic within the past year (365 days). Patients not speaking English, patients with developmental delays or acute mental health concerns, or patients recently diagnosed with diabetes (within the past year) were excluded.
Recruitment letters were sent to 118 patients with a return card for patients to indicate interest or disinterest in participation. The research team made follow-up calls to participants not responding to the letter invitation. Additional recruitment occurred via flyers at the diabetes clinic and referrals by diabetes clinic staff. A total of 36 eligible patients expressed interest in the study and were contacted by phone to provide additional study information and to schedule focus groups. If EAWD could not be scheduled for a focus group or preferred an individual interview, an individual interview was scheduled. EAWD received reminder letters after being scheduled for the study and a reminder call the day prior to their scheduled visit.
Data Collection
Focus groups and interviews were held in a private classroom or diabetes clinic office at the hospital. After written consent was obtained, participants completed a brief demographic questionnaire. Focus groups began with a brief introduction, including an explanation of the study purpose and establishment of ground rules to ensure orderly and robust discussion. 17 The focus group moderator/interviewer used a semi-structured interview guide with 3 key questions and probes corresponding to the following 3 study aims: What makes it harder/easier to manage diabetes? How would you describe your current interactions with your health care team at diabetes care visits? What would an ideal visit to support you in managing diabetes look like? A research assistant was present at focus groups to serve as notetaker. Participants received $25 cash compensation for their time.
Data Analysis
Data analysis consisted of a 6-step process of data organization/preparation, initial review of data, coding, description, representation, and interpretation. 18 Interviews and focus groups were transcribed verbatim from audio recordings of the discussions, with the exception of one focus group which was not recorded due to moderator error. Recording transcripts (notes for the unrecorded focus group) were imported into MAXQDA 2020 software (Berlin, Germany). Both deductive and inductive coding were used to analyze data. 19 After an initial analysis of transcripts, three conceptual deductive topics of focus were derived from the study aims: Influences on Diabetes Self-Management, Perceptions of Current Interactions with Providers During Visits, and Wants and Needs for the Diabetes Care Visit. Transcript text was then coded inductively to identify themes within this categorization framework, and a codebook was created to refine and organize codes. Coding was performed by the primary author and reviewed by a second study team member. Iterative concept mapping and tables were used to help identify, organize, and collapse codes throughout data analysis, and case by topic matrices were created to aid in visualization and analysis of research findings.18,20 Memos and reflective note-taking were used to document observations and decision-making processes.
Results
Description of the Sample
A total of 14 EAWD participated. Two focus groups were held with emerging adults with type 2 diabetes and one with emerging adults with type 1 diabetes (4 participants, 5 participants, and 2 participants, respectively). Three EAWD (one with type 1 diabetes and two with type 2 diabetes) participated in individual interviews. Mean duration of focus groups and interviews was 46 minutes and ranged from 41 minutes to 84 minutes. Demographic data are summarized in Table 1. On average, participating EAWD were 27 years old and had been diagnosed with diabetes for nine years. All participants self-identified as Black and two reported their ethnicity as Hispanic/Latino. Most were women, and most worked at least part-time. Among those who knew their HbA1c, mean HbA1c was 9.1%.
Participant Demographics (n = 14).
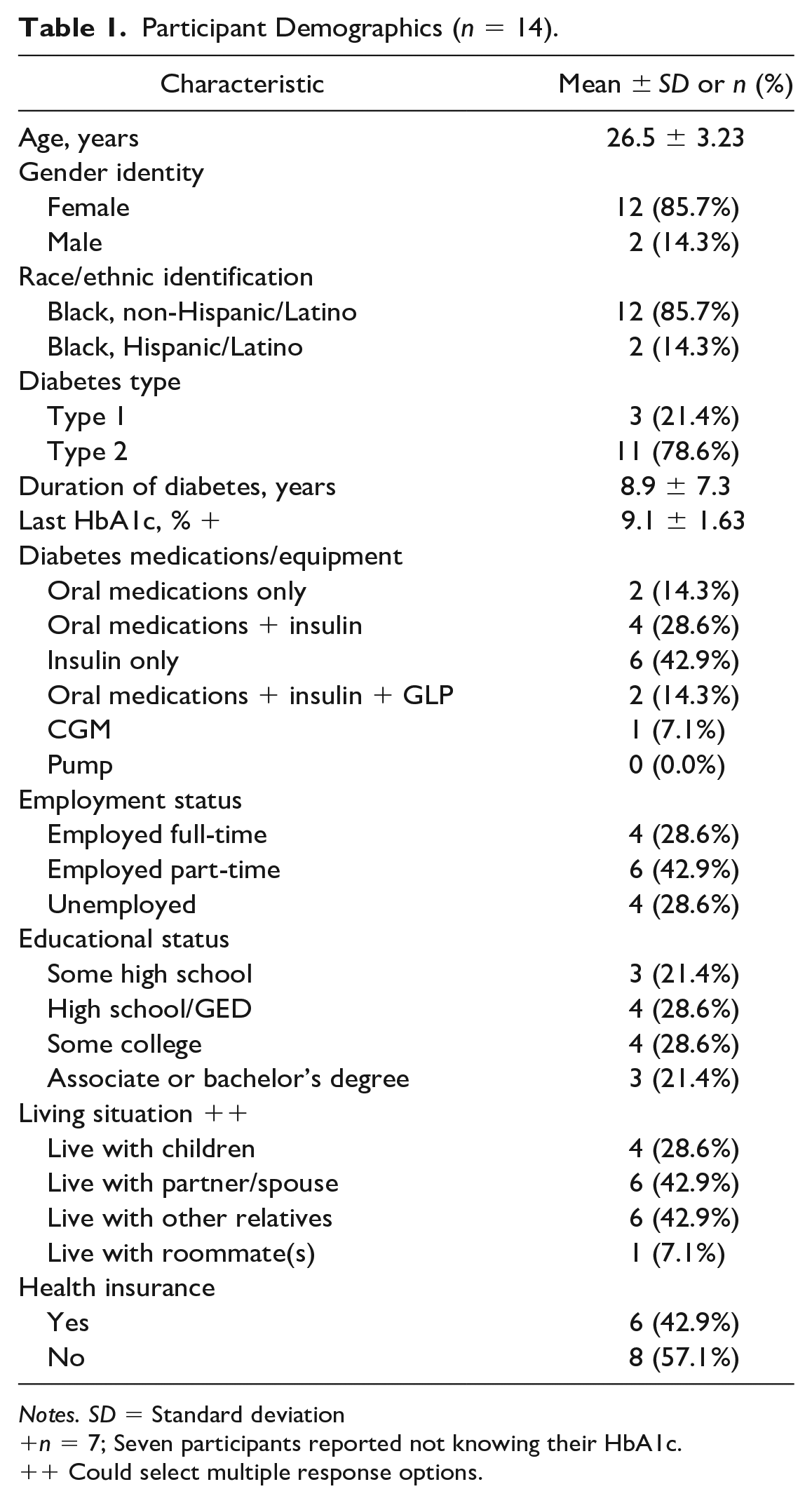
Notes. SD = Standard deviation
n = 7; Seven participants reported not knowing their HbA1c.
+ Could select multiple response options.
Qualitative Findings
During focus groups and interviews, EAWD described factors influencing diabetes self-management, their perceptions of their current diabetes visit interactions, and their wants and needs during their diabetes visits.
Influences on diabetes self-management
The main factors that EAWD perceived to influence diabetes self-management were the emotional burden of diabetes, active busy lives, access to resources, and family. These main factors are presented in Table 2 with a summary description of each factor and participant quotes reflecting these influences. Most factors served as barriers to self-management. The emotional burden of dealing with diabetes daily, especially as an EAWD, was often described as a deterrent to self-management tasks. As one EAWD commented, “Diabetes is like a job. It’s hard work” (EAWD #2). EAWD described balancing and reprioritizing diabetes self-management needs with work, social, and family activities. Work, especially, was identified by most EAWD as a responsibility that interfered with diabetes self-management or that was adversely impacted by the need to manage diabetes: “If I am called in to work a double, I have to push my meals. . .I’m just reworking my schedule” (EAWD 13). Likewise, limited access to resources, particularly financial resources limiting access to health insurance, healthy food, and medication, within and outside the health care setting, was a major barrier. Comparing her health care to that of friends with insurance, one EAWD remarked, “I think that’s important, having good insurance that goes somewhere” (EAWD #7). Several observed that, as an EAWD, one loses resources available within pediatric care, including health insurance and assistance navigating health care systems.
Factors Influencing Diabetes Self-Management.
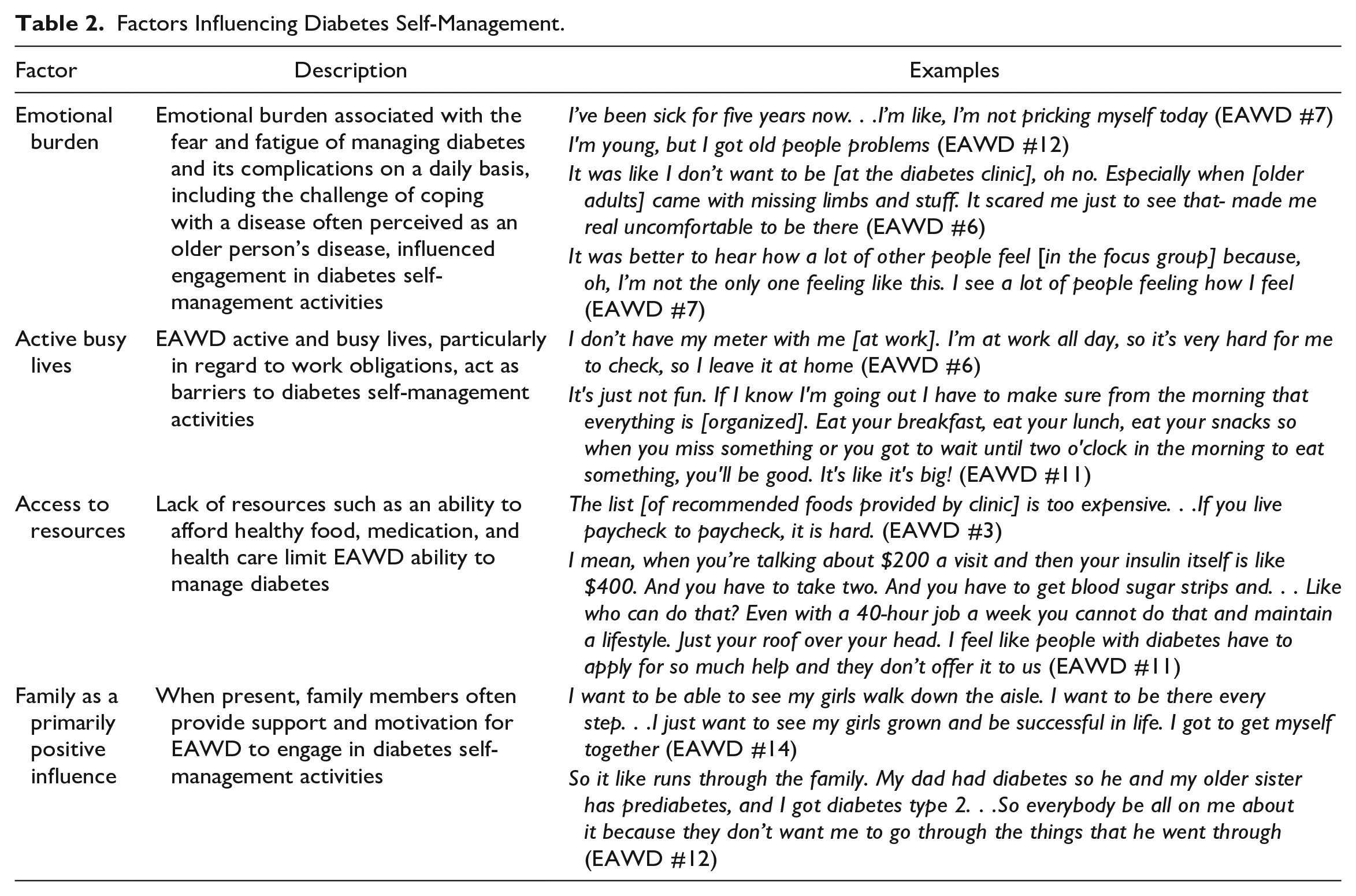
While EAWD identified more barriers to self-management than facilitators of self-management, at times the emotional burden associated with fear of and desire to avoid complications sometimes served as motivation for self-management: “I should have been doing better, so this [hospitalization] will never happen again. I be like, I probably going to die or something, so I be like, just force myself to do it. But I’m tired of [diabetes]” (EAWD #6). The family was also described as a primarily positive influence on self-management.
Perceptions of current interactions with providers during diabetes care visits
When asked to describe their current diabetes visit interactions, participants’ responses led to identification of the following three major themes: (1) routine nature of the visit, (2) value for time spent, and (3) tangibles and knowing where you stand.
Routine nature of the visit
Many EAWD believed they hear the same messages at each visit and perceived visits as rather routine, with most of the effort to manage diabetes occurring outside the clinic on one’s own time. One participant noted, “[I am] pretty much waiting for them to tell me what I already know” (EAWD #4). As one individual observed, “Yeah, it’s a lot by myself, but I don’t mind being independent. I have my refills, my numbers look good, then I’m good” (EAWD #13). Another remarked, “I’ve been coming to the diabetes center for four to five years, so it’s like the same thing, but mostly it is on me” (EAWD #7).
Value for time spent
Participants discussed the value of the diabetes visit, particularly in relation to opportunity cost when time is limited. Almost all EAWD mentioned the wait time to be the most unsatisfactory part of appointments. Given the limited time with providers and information gained, several EAWD thought that their time was not always well spent, especially when they had other obligations and when they believed what was accomplished at visits could be conducted in a more efficient, streamlined manner. One EAWD described that the best part of the visit was, “Going home, cause you are already in there for about 10 hours. They give you new medicine and just tell you the same thing over and over again” (EAWD #9). Online appointments and appointments outside of 9 am to 5 pm work hours were suggested as alternatives. Several EAWD mentioned they had either stopped coming to appointments because of perceived inertia of care or came only for medication refills.
Tangibles and knowing where you stand
When asked about goals for the visit, participants indicated that they came for the following three main purposes (1) for diabetes supplies, (2) to know where they stand regarding diabetes control and complications, and (3) to hear good news. For some, the only reason they came was to obtain diabetes supply refills. For the majority, knowing their numbers and their progress in reducing their HbA1c was the primary goal for the visit. An EAWD described what she wanted from her visit: “Nothing really. Just to be seen and see what’s wrong with me, if something is wrong with me, see what’s wrong with me, and that’s it, and go home” (EAWD #12). Many also acknowledged that they came to the visit hoping to hear good news or to avoid bad news: “As long as I know things aren’t getting worse, I’m okay” (EAWD #4).
Wants and needs for the diabetes care visit
Participants discussed their thoughts regarding their needs and wants beyond their current provider interactions at visits. The following three themes identified included: (1) need for tailored guidance, (2) beyond content: caring relationships and positivity, and (3) continuity and communication between visits.
Need for tailored guidance
EAWD indicated that, while they may perceive diabetes care visits as an “in and out” experience and do not necessarily approach the visit with the expectation of acquiring new information and skills that can be applied to facilitate self-management at home, they need and appreciate personalized guidance for self-management that works for them and addresses their unique concerns. Several EAWD observed that when they were first diagnosed, information was new and informative:
The first time, they had a talk about it, so that was pretty helpful. They talked about diabetes and all the things that can happen having diabetes, so that was very helpful. After that they just do a reminder of what they talk about and all the things you’re supposed to do to keep your body, keep your body right. (EAWD #12)
However, many felt that self-management advice was no longer useful. “I think, yeah, they see you, tell you what you need to hear, but it don’t really somewhat help sometimes in a ways. . .. It feels like they’re more of a cookie cutter type” (EAWD #6). A desire for personalization included guidance on a range of topics including medication management, nutrition, physical concerns, and exercise. For instance, one EAWD noted, “I don’t take as much medicine as they tell me to take. They prescribe too much. I don’t eat as much as they prescribe. My sugar would be too low if I took as much as they gave me” (EAWD #3). Another commented, “I need them to be relatable and logical like let’s just be real. . .A person eats differently than their grandma. We don’t know what we’re going to eat until we’re about to cook” (EAWD #11).
A few EAWD described being appreciative when they did receive helpful self-management advice specific to their situation. For example, one participant noted that her nurse gave useful tips on how to curtail her snacking habit while also being prepared for low blood sugars, and another found reviewing her daily meals and blood sugars with her nurse to identify associations between diet and blood sugars helpful for understanding dietary management.
Beyond content: Caring relationships and positivity
In addition to the need for specific advice, all EAWD desired providers who conveyed that they care about individual patients. EAWD wanted to feel like they were not just numbers or part of the job. Caring was described in several forms. For some, this meant taking time to allow EAWD to ask questions and to communicate in a way patients could understand:
I learn from looking. You can tell me anything but if I didn’t visually see it I don’t understand. Take your time with us we are paying to see you for more than 5 minutes. No rush. We need help. (EAWD #3)
For many, caring meant trying to understand the patient and his or her experience:
It would be better if [providers] were diabetics. Because [providers are] reading the books. Knowledge is different than experience. So different. You can read about low blood sugar. You can tell the symptoms of low blood sugar. But when you’re living with low blood sugar. It is not even half of what they put in a book. . .. They’re like “Oh, if your sugar’s dropping, get something quickly.” Yeah, I’m trying. . .. I feel like if at least one person was a diabetic in there, it would make so much more sense. It would click. You would understand why we can’t do this. (EAWD #11)
Caring relationships not only influenced emerging adults’ perceptions of quality of care but enhanced receptivity to provider messaging. As one individual observed,
Receiving the information is easier from someone who seems like they care. If they don’t care, it’s like, should I listen to you? I mean I will but it’s not as much—it’s not as welcoming as something from someone that you prefer to be around. (EAWD #13)
All EAWD wanted providers to frame messages in a positive perspective, and all felt that encouragement was important: “Number one thing, please encourage us. PLEASE. That’s the first thing. It’s just the icing on the cake, encouraging us. Other than that, I don’t have a second or third [request]” (EAWD #9). Not only were EAWD eager for encouragement and acknowledgment of progress achieved, but they reported frustration when the message they received was framed in the negative (for instance, not meeting HbA1c goals, being at risk for limb loss) especially when that message was not followed up with a solution or advice for positive health outcomes:
Good news [is when the doctor tells] them they have diabetes, but when you say they have diabetes, oh I can help you keep it low, or I can help you keep it at a good level. You give them bad news when you say, oh you have diabetes and that’s it. You’ve got diabetes and tell them more bad things like your A1c is high, you’ve got to get this low. A doctor that gives the news away but don’t help deliver it, like help with the process. (EAWD #12)
Continuity and communication between visits
Several EAWD indicated a caring relationship was easier to establish when they consistently see the same provider. Moreover, communication and access to providers between visits was described as fostering both the provider relationship and EAWD ability to receive tailored guidance for self-management. Several EAWD observed that they could benefit from just-in-time provider guidance for diabetes management (e.g., day-to-day decision-making, medication concerns, sick day management) and were frustrated when they could not gain timely access to providers between visits:
You’ve got to call them, they leave a message, and it takes them weeks to reply back and you are like, I don’t even need the answer anymore. It’s difficult to even talk to them so I don’t even bother anymore, I just Google it. (EAWD #6)
Conversely, EAWD reflected on how impactful it was (or could be) if providers called to check on them: “She [the nurse] sounds like she cares. . .You know, you’re supposed to call in and give them your blood sugar. She’s calling me. And I love that because it’s like I’m not just a patient” (EAWD #11).
Discussion
Participants in this study of EAWD receiving diabetes care in a safety-net public health care system identified several factors impacting their diabetes self-management. The emotional burden of dealing with diabetes as an EAWD was particularly salient and compounded by busy lives, competing priorities, and multiple responsibilities with limited access to resources to support diabetes management. While EAWD often viewed access to diabetes supplies and awareness of their diabetes health status as key components of their visits, their desire for (individually tailored) informational and affective support from providers emerged in discussion of EAWD needs at diabetes visits. The health care system for these EAWD served both as a facilitator and barrier to participants’ self-management needs, providing access to care and supplies but not always leaving participants satisfied with quality of care.
The findings support previous research identifying significant psychosocial burden for EAWD, particularly underserved EAWD, and serve as additional evidence that emotional health is related to self-management behavior and health outcomes.21-23 Therefore, addressing emotional burden merits further attention. Interpersonal relationships seem to be a potential source of resilience and motivation for EAWD, and interventions related to relationship building may offer some solutions. EAWD have described a desire for connection, rapport, understanding, and collaborative person-centered care as components of EAWD-provider interaction.13,24 In this study, EAWD identified dual roles for providers in supporting both self-management skills and psychosocial well-being. EAWD overwhelmingly and adamantly reported the need for positivity and encouragement from providers as much as they prioritized the need for specific informational content, which suggests affective support related to diabetes burden, as much as informational support and medication management, maybe a vital component of diabetes care for EAWD.
Other EAWD peers with diabetes may also serve as an interpersonal resource. A notable finding from all focus group interactions was EAWD desire for further social connection with other EAWD who can understand their experiences. Prior studies have reported EAWD need to feel that they are not alone in their challenges managing diabetes. 22,25 This suggests that interventions such as those facilitating support networks with other EAWD during the transition from pediatric to adult care may be beneficial when extended beyond the transition of care. Such interventions may be especially important for many EAWD isolated in their diagnosis as EAWD and unable to establish networks through activities such as pediatric diabetes camps. Given the barriers to self-management identified by EAWD within this health care system, implementation of these interventions should accommodate busy schedules and financial constraints.
Like other EAWD, participants in this study report that activities and responsibilities associated with emerging adulthood and the added task of managing diabetes on a daily basis create additional burden in the mid of competing priorities.9,25 However, the nature of these responsibilities may differ. For instance, college has been described as a challenge to diabetes management among younger emerging adults with type 1 diabetes.9,26 In the current study, most participants had not or were not attending college and were slightly older on average. For these EAWD, work was described as a predominant challenge to self-management activities. However, in a study of urban minority EAWD, the workplace was perceived as primarily supportive of self-management. 27 Perhaps because participants in the prior study were slightly more educated, they may have had jobs offering more psychosocial/structural support and flexibility for diabetes self-management. In contrast, many participants in the current study held jobs in construction, fast food, and industries with potentially less flexibility for self-management. This indicates the nature of the influence of work and other responsibilities on diabetes management and, conversely, of diabetes on ability to engage in these roles should be assessed when caring for underserved EAWD.
While EAWD clearly articulated a need to address the emotional burden of diabetes, they also indicated the importance of informational support when appropriately provided. Specific, practical, actionable, and age-appropriate guidance could enhance the perceived value of visits and increase the likelihood of regular follow-up to improve outcomes. For instance, among this population of EAWD, it may be important to provide guidance and medical management tailored to being a working adult and maintaining or obtaining employment while managing diabetes. Soliciting concerns about acute and long-term complications (such as fear of inducing hypoglycemia while avoiding hyperglycemia) and then providing actionable information within the context of the emerging adults’ lives may help EAWD feel heard and facilitate self-efficacy despite social and economic barriers limiting sense of agency. Given the daily challenges of managing diabetes and desire for more care continuity, EAWD may benefit from interventions ensuring EAWD can connect with diabetes care providers outside of routine visits and can reliably access timely advice and support. As many EAWD are actively engaged with “instant access” technologies such as internet that provide ready access to information, digital technology may be an apt means to facilitate these interactions.21,28
Although the study provided insight into perceptions of EAWD regarding diabetes self-management challenges and diabetes care visits within a public hospital setting, there were several limitations. The participants may not represent the full diversity of EAWD in safety-net care, particularly since participation was limited by difficulties recruiting, especially male EAWD, EAWD with type 1 diabetes, and younger EAWD. Two factors that may have contributed to recruitment challenges were identified from the study itself: active, sometimes unpredictable lives as well as a lack of sense of connectedness to the health care system. Additionally, while focus groups provided insights into important dynamics of social interaction among these EAWD, and while the moderator attempted to encourage robust discussion and differing opinions during focus groups, focus group discussion could have been influenced by group dynamics biasing the discussion. Use of individual interviews served as a supplementary data collection method to counterbalance potential group dynamic biases.
In future research to improve care for EAWD, additional purposive sampling may provide better insight for comparison among different subsets of EAWD within safety-net care. For instance, differences in experiences of emerging adults with type 1 diabetes versus type 2 diabetes, as well as differences between EAWD having transitioned from pediatric diabetes care versus those diagnosed as adults were not fully explored within this limited sample.
Alignment of health care services with concerns of EAWD is vital to improving quality of care. This study suggests EAWD need mental health and social services that address emotional health, provide strategies for managing diabetes along with other responsibilities, and link EAWD to social support and financial resources. Access to follow-up between appointments by a consistent provider may be challenging in safety-net care but important, as this study contributes to literature endorsing person-centered care for EAWD.9,29 Essential elements of person-centered care encompass communication, empathy, respect, shared decision-making, individualized and holistic care, building therapeutic relationships, and a goal of meaningful living. 30 While safety-net care may face staffing and resource challenges in addressing some EAWD needs, some aspects of person-centered care that EAWD desire may not necessarily be resource-intense. Providers able to provide empathetic affective support and tailored informational guidance by focusing on successes and possibilities and soliciting EAWD input and feedback to ensure interactions address what is meaningful to EAWD will enhance the value of diabetes visits and care. Ultimately, such actions have the potential to decrease health care burden and improve outcomes for EAWD across their lifespan.
Footnotes
Acknowledgements
The authors would like to thank Breanna Berry, MPH, from Emory School of Public Health, for assistance with patient recruitment, focus groups facilitation, and data transcription.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.