
Abstract
Sleep disturbance is prevalent among caregivers of people living with dementia. However, gaps exist about caregivers’ sleep patterns before and during their caregiving trajectory. This exploratory secondary analysis using a qualitative descriptive approach aimed to (1) identify and describe current caregivers’ patterns of change in sleep before and during caregiving, and (2) understand caregivers’ perceptions of their current sleep compared to their pre-caregiving sleep. We conducted semi-structured interviews with 19 caregivers taking part in a larger randomized controlled trial. Participants were female (n = 11), white (n = 13) and on average 63 years of age. Interview questions focused on caregivers’ sleep patterns. The interviews were audio-recorded using a videoconferencing platform and ranged from 20 to 45 minutes. We conducted thematic analysis of the interview transcripts. Three distinct caregiver-sleep profiles emerged from the qualitative data: changed and dissatisfied, changed and satisfied, and unchanged and dissatisfied. Caregivers whose sleep was categorized as changed reported a difference when comparing their current sleep pattern to their pre-caregiving sleep pattern. This was usually a change from good to poor sleep. Caregivers whose sleep was unchanged had poor sleep pre-caregiving and continued to have poor sleep during caregiving. Caregivers also reported being satisfied or dissatisfied with their current sleep pattern, defined in terms of distress and impairment. These three subtypes highlight the heterogeneity of caregivers’ sleep experiences and debut a useful clinical framework with which to identify, categorize, and target caregivers at risk for sleep disturbance, many who may be ready to engage in behaviors to improve their sleep. Knowing caregivers’ sleep profiles will enable health care providers and researchers to determine caregivers’ needs and readiness for interventions then work collaboratively with them to improve their sleep problems.
Keywords
Insomnia is difficulty falling asleep, or staying asleep, or having early morning awakenings and being unable to return to sleep even with ample sleep opportunity accompanied by daytime clinical distress or functional impairment. 1 Up to two-thirds of caregivers of persons living with dementia (PLwD) experience insomnia-like sleep problems.2,3 In addition, one recent systematic review found that caregivers of PLwD lose between 2.4 hours and 3.5 hours of sleep weekly compared to their age-equivalent non-caregiver counterparts. 4 Since the prevalence of insomnia in adults ranges between 17% and 60%,5,6 it is likely caregivers’ sleep disturbances can predate their caregiving responsibilities. However, there are gaps in the literature regarding when caregivers begin to experience sleep problems along their caregiving trajectory.
Causes of caregivers’ sleep disturbance are multifactorial. Caregiver-specific causes could include employment and chronic health conditions which can precede caregiving. Since approximately 60% of family caregivers report being employed, it can be deduced that most caregivers are employed when they become caregivers. 7 Moreover, more than 50% of caregivers have a chronic condition such as hypertension, diabetes, or heart disease; since most chronic conditions develop with time, it is also likely that many caregivers begin the role of having at least one chronic health condition. 8
Non-caregiver-specific causes of caregivers’ sleep disturbance include caregiving responsibilities, and behavioral and psychological symptoms exhibited by the PLwD.9,10 Caregivers for PLwD provide extensive assistance, which can range from instrumental activities of daily living to more hands-on activities of daily living, often for a long duration. 7 The level of care and the type of care can increase caregivers’ risk for sleep disturbance. 10 During this time, PLwD may also have behavioral and psychological symptoms of dementia, including sleep disturbance, 11 which may affect caregivers’ sleep. PLwD may awaken caregivers at night to ask for assistance or perform activities without the caregivers’ knowledge.12-14 Over time, caregivers may become hypervigilant and have difficulty falling or staying asleep.15,16,17
Purpose
Sleep disturbance is prevalent among caregivers of PLwD and can lead to numerous adverse outcomes;18,19 therefore, tailored interventions are needed to address caregivers’ sleep problems. However, it is important to understand caregivers’ sleep patterns before and during caregiving because the process used to develop and tailor an intervention may differ based on the timing and cause of the sleep disturbance. To address these gaps pertaining to caregivers’ sleep in relation to their caregiving trajectory, this study sought to (1) identify and describe profiles of current caregivers’ sleep patterns before and during caregiving, as well as (2) understand their perception of their sleep quality relative to their pre-caregiving sleep.
Methods
Design
An exploratory secondary analysis with a qualitative descriptive approach was used to capture caregivers’ sleep characteristics and experiences and categorize the sleep data into different sleep groups.20,21 A qualitative descriptive design allows for exploration of caregivers’ situations with minimal interpretation for development or tailoring of future interventions. 20 Data collection involved conducting semi-structured interviews with caregivers of PLwD, a method that created a collaborative interview process within which researchers and participants could co-construct knowledge. 22 Author GB developed the interview guide based on the Modified Spielman 3P model of Insomnia, 23 topics identified from existing literature, and discussions with the research team, which qualitative research experts reviewed to ensure its readability and fit with study objectives. However, in the tradition of qualitative research, the final guide evolved after an initial iteration of data collection as additional insights emerged. Broadly, the semi-structured interview asked about the characteristics of the caregiver’s sleep pattern before caregiving, their current sleep pattern, the factors associated with their previous and current sleep pattern, and their perceptions about their current sleep pattern (Table 1). The Emory University Institutional Review Board granted ethical approval for the study (IRB00092812).
Sample Interview Questions.
Participants
Participants were caregivers of PLwD who were participating in a randomized controlled trial (NCT03033875) to examine the effects of an online psychoeducational intervention, Tele-Savvy, compared to Healthy Living or Usual Care on caregivers’ competence and mastery. 24 To be included in the main study, participants had to be informal caregivers (family/friends) of community-dwelling PLwD who are providing unpaid assistance for an average of 4 hours per day. Participants were excluded if they had plans to place the PLwD in a residential community within the next 6 months and did not have access to a computer or mobile device with adequate internet connection. Participants provided informed consent at the baseline, which also included being contacted for an optional follow-up interview after completing the 6-month data collection visit. For this specific study, after one of the first three interviewees reported no sleep problems, we purposefully interviewed caregivers who had an Insomnia Severity Index (ISI) score of at least 5, which indicates the presence of some insomnia symptoms. 25
Recruitment
Initially, any caregiver who expressed willingness to be interviewed was emailed a description of the interview study after they completed the 6-month data collection visit of the parent study. A follow-up email was sent to those who responded, providing options of dates and times for a videoconference interview. Once scheduled, participants were sent calendar invitations with the Zoom link. Interviews took place between February 2019 and December 2019.
Data Collection
Measures
Sociodemographic information was collected using a sociodemographic questionnaire (age, sex, ethnicity, educational level). The ISI is a 7-item instrument that assesses self-perception of insomnia symptoms as well as the degree of concerns or distress caused by those symptoms over the previous 2 weeks. 25 The total ISI score range is 0-28 points, with higher scores indicating greater insomnia severity. 25
Interviews
GB conducted all of the interviews. Interviews ranged from 20 to 45 minutes. At the conclusion of the interviews, participants were compensated with a $30 gift card to a local store. Interviews were digitally recorded via the videoconferencing application and professionally transcribed verbatim. The transcripts were compared with the recordings to check for accuracy. Caregivers’ names were changed to pseudonyms to maintain anonymity and confidentiality. Only the de-identified transcripts were used for coding.
Analysis
Descriptive statistics (means, ranges, frequencies) were computed for the demographic information using SPSS (Statistical Package for Social Sciences, version 26). Five authors (G.B., F.E., K.B., C.P., K.Y.) trained in qualitative methods and steeped in the sleep and /or caregiving literature conducted all analyses. These five individuals coded the first four transcripts individually. After the initial four transcripts were analyzed, the team met and discussed the codes and arrived at consensus for the development of the codebook. At least 2 authors coded each of the remaining 15 transcripts using the codebook. Each pair of coders met and discussed any discrepancies and then reached consensus. After the other 15 interviews were coded, the completed code sheets were reviewed for areas of disagreement. When there were areas of conflict, at least 3 of the 5 agreed on the code and supporting statement(s). The team used thematic analysis iteratively to summarize the data. 26 Thematic analysis involved the researchers reviewing the text in detail to familiarize themselves with the data to identify patterns, generate initial codes, and to search for “themes” which were then organized, defined, and named. These themes enabled the integration of findings from data, theory, and previous findings. An audit trail was used to document all processes and collaborations and data decisions. 26
Credibility and Rigor
To further foster rigor of data collection and enhance data analysis, brief field notes were taken during interviews, and reflexive journaling was done after each interview.21,27,28 Acknowledging how the background and values of the researcher can influence the research as well as bracketing preconceptions and assumptions at the beginning of this project and throughout the project through reflexive journaling minimized potential bias.29,30 The reflexive journal included entries that recorded the primary researcher’s (GB): (a) reason for undertaking the research, (b) beliefs regarding sleep experienced by caregivers and PLwD, (c) role as a Black nurse practitioner and researcher, and (d) potential role conflicts with participants. To establish another element of rigor, we reduced the likelihood of introducing bias at the analysis stage by (a) having four researchers independently code the initial transcripts, (b) conducting peer debriefings, and (c) incorporating a third research colleague to assist with resolving discrepancies. To promote credibility of the data, participants were chosen who had experience of the phenomena under study. An “audit trail” of fieldwork procedures, methodological decisions, and data analysis was also maintained. 31 All these components helped to establish the trustworthiness of this study.
Results
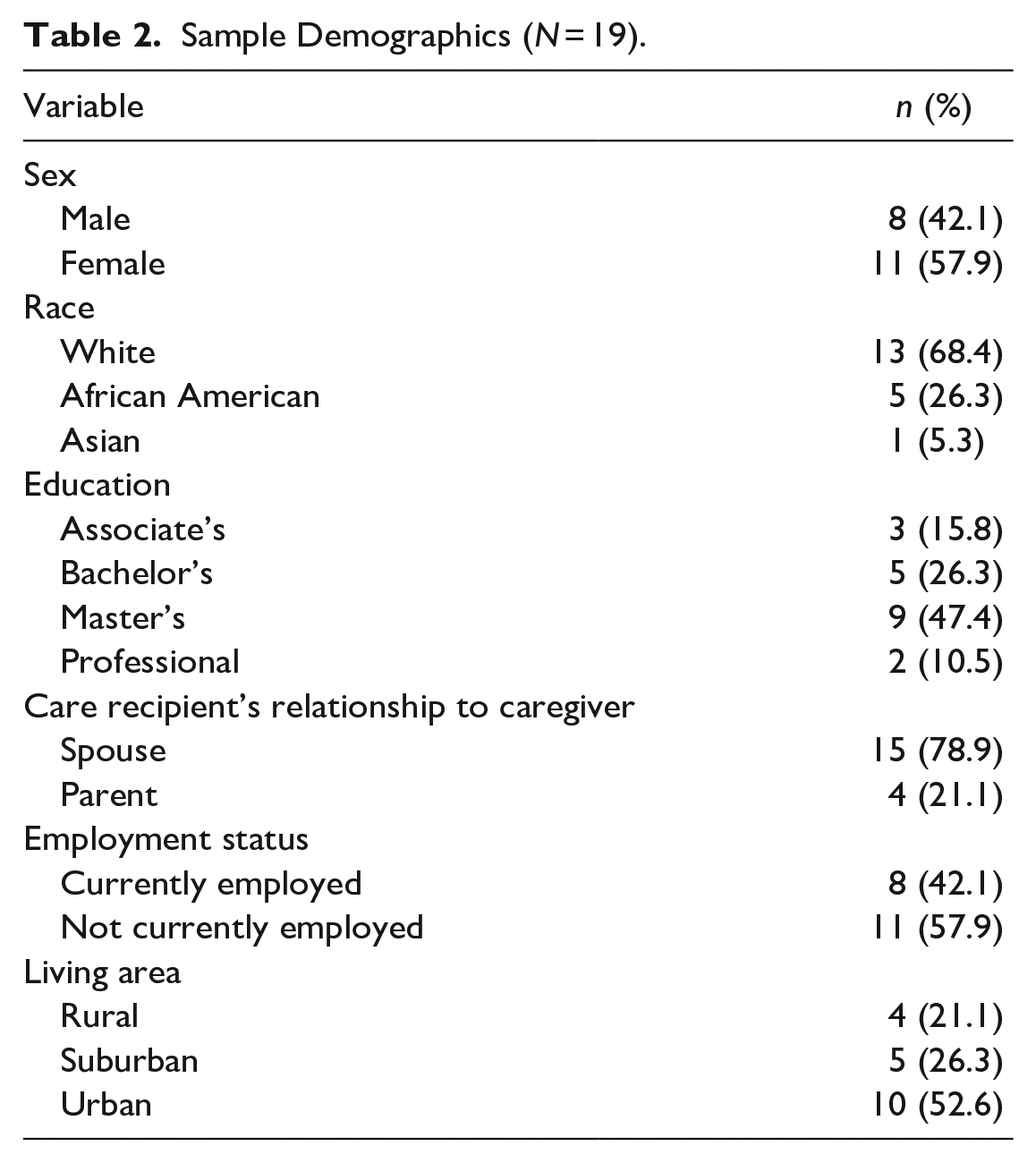
Nineteen caregivers participated in this study; most were female (n = 11) and white (n = 13). On average, caregivers were 63 years of age (SD [Standard Deviation] ± 8.23) and provided care for an average of 2.71 (SD ± 2.07) years. On the measure of insomnia severity (ISI), caregivers scored 11.52 (SD ± 6.26), suggestive of mild insomnia. Table 2 further illustrates caregivers’ demographic characteristics.
Sample Demographics (N = 19).
Caregiver Sleep Profiles
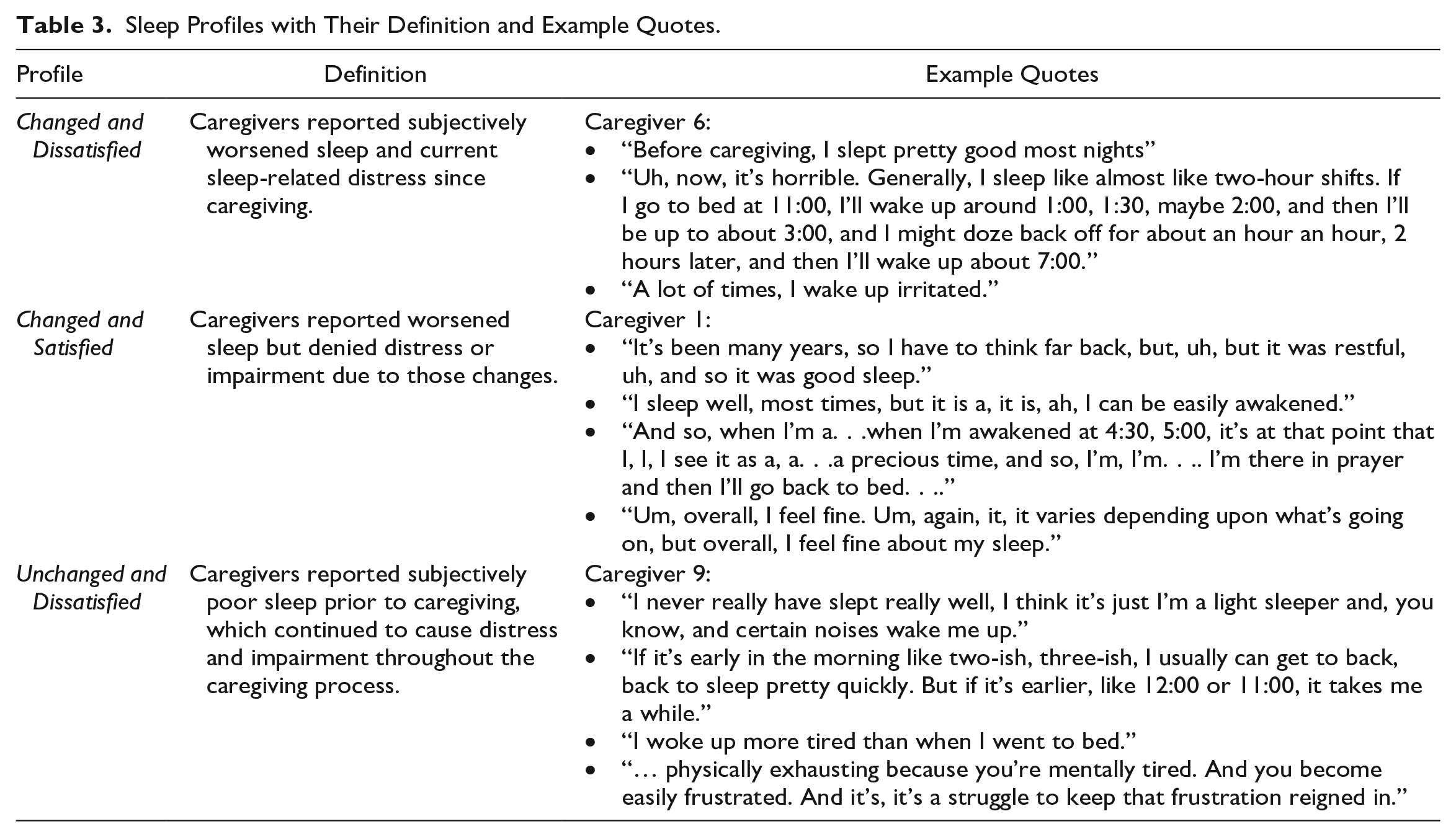
We identified 2 categories based on caregivers’ descriptions of pre-caregiving compared to current sleep pattern (changed and unchanged) and 2 categories based on their appraisals of their current sleep relative to the pre-caregiving sleep (satisfied and dissatisfied). These categories generated the following 3 distinct caregiver phenotypes: (a) changed and dissatisfied, (b) changed and satisfied, and (c) unchanged and dissatisfied. Caregivers of the changed and dissatisfied type reported subjectively worsened sleep and current sleep-related distress since beginning caregiving. Caregivers of the changed and satisfied type similarly reported worsened sleep but denied distress or impairment due to those changes. Conversely, caregivers of the unchanged and dissatisfied type reported subjectively poor sleep prior to caregiving, which continued to cause distress and impairment. Table 3 provides additional explanations of the categories with example quotes from caregivers’ interviews.
Sleep Profiles with Their Definition and Example Quotes.
Changed and Dissatisfied Profile
These caregivers reported subjective changes in their sleep and decline in their level of satisfaction with these changes after they became caregivers. Specifically, they noted difficulties with falling asleep, restless sleep, and sleep fragmentation, citing nighttime vigilance and mental stress associated with caregiving. For instance, one husband, Caregiver 6, reported sleeping in “two-hour shifts” to check on his wife who slept in another room. A wife, Caregiver 18, mentioned that she was “on the alert, because during the night, [she] would wake up because every time he moved, [she] didn’t know if he was going to the washroom; was he getting dressed? Was he trying to leave? Um, he was so confused. . ..” She also recalled an incident of wandering while she napped, noting, “he did wander, ah, one night, one early evening, and, um, got lost and was missing for an hour or so. And ever since then, I had been on alert. . ..” Caregiver 4, a daughter, reported mental stress associated with her role: “it’s just, you know, stretched different ways and my mind is just constantly going, so it is hard to kind of wind down, um, settle down and, and sleep.” Others reported feeling nervous about their care recipient’s (CR) inability to self-regulate their chronic health conditions at night. One son, Caregiver 17, admitted to difficulties maintaining sleep because he knew his mother was unable to adequately manage overnight changes in blood sugar. He noted:
She wears a continuous glucose monitor. It’s networked with my phone. So, if her sugars are low or high, I would get like beeped on my phone. A signal would go off and I would have to either give her, if it was low, I would give her something to eat, and if it was high, I’d have to give her insulin. Even if I were sleeping, that would wake me up, I’d say an average of every other night. And sometimes, I’d have to wait, I didn’t just go back to sleep, I would wait up until, her sugar levels were normal again, make sure, ‘cause sometimes, getting it back up, it didn’t always work. And you’d have to get more food and take a little bit of time.
Caregivers reported impairments in wakefulness, including daytime fatigue, anxiety, amotivation, difficulties concentrating, irritability, and issues completing activities of daily living resulting from their sleep changes.
Changed and Satisfied Profile
These caregivers reported good sleep before caregiving. They admitted that while their sleep schedules now varied nightly, they slept well most nights despite new disturbances. Overall, these caregivers reported feeling “fine overall” and were not “very concerned” about their sleep. Caregiver 1, a daughter, put it simply, saying, “I feel fine about my sleep.” She said she frequently awakened early in the morning but used these awakenings to read the bible and pray, which left her feeling satisfied with her sleep. Caregiver 10, a wife, was currently having “pretty good” sleep, sharing: “most nights, I do wake up” … “and, um, tend not to go back to sleep for a little while. Lots of times, I’ll move into the, um, couch, on the couch.” However, she noted that her sleep is “pretty good sleep. It’s not restless. I don’t toss and turn.” Another wife, Caregiver 2, also expressed that while she had good, regular sleep before caregiving, she started experiencing more irregular, superficial sleep with caregiving with which she reported no dissatisfaction.
Unchanged and Dissatisfied Profile
These caregivers short sleep duration and poor sleep quality before caregiving. They described their pre-caregiving sleep as erratic, restless, and fragmented, often implicating their work responsibilities and schedules. For instance, Caregiver 8, a wife, noted that “we [her and her husband (the PLwD)] started [a] business and, so that, that kind of level of stress contributes to poor sleep to start with because you’re always very busy.” Caregiver 19, a husband, noted, “I could be working late at night, or I could be having to get up super early in the morning.” Other factors that affected their pre-caregiving sleep patterns included: noise from the PLwD’s continuous positive airway pressure machine, the death of a loved one, being unable to “calm the brain down,” nocturia, and psychological challenges including anxiety, alcohol use, and historical trauma. These caregivers were and remained dissatisfied with their sleep. Among this subtype of caregivers, poor sleep had daytime consequences, including fatigue, exhaustion, and negative affects like crankiness, nervousness, and panic. For example, Caregiver 17 reported, “I’ll wake up like sort of jittery and like panicky a little bit. And I, and I wake up really tired,” or Caregiver 12 who stated that, “I’m just so tired, I doze off,” and “it, it just, physically causes me to feel uncomfortable.”
As a result of poor sleep, some caregivers also used prescription or over-the-counter medications or alcohol to manage their sleep problems. Caregiver 19 said:
I was on, Trazadone, Trazadone, briefly. . .but it, it made me a loopy, goofy mess. . .. It was very, very uncomfortable. It wasn’t a very, pleasant medication for me. It didn’t really work. I had better luck taking Benadryl or Pseudoephedrine, Sudafed, which I can look at a bottle of Sudafed and it puts me to sleep.
Caregiver 15, a wife, also used medication to sleep but she appeared conflicted about taking the prescribed medication. She said:
I try not to take ‘em [Ambien], in the last several months I’ve only taken them once, it was the night before the first day I had to be back [to work], this past week. . .. I just wanted to make sure I slept through the night and woke up. So, yeah, that’s the only time I’ve really had a complete night’s sleep.
Other caregivers denied using pharmacological sleep aids and instead used sleep hygiene principles, stimulus control techniques, exercise, and/or adjusting their work schedules, to try to improve their sleep.
Discussion
This study is among the first to identify and describe caregiver sleep profiles before and during caregiving, drawing directly from lived experiences of caregivers of PLwD. Three distinct caregiver sleep profiles emerged from the qualitative data: changed and dissatisfied, changed and satisfied, and unchanged and dissatisfied. These profiles highlight the heterogeneity of caregivers’ sleep experiences and debut a useful clinical framework with which to identify, categorize, and target caregivers at risk for or already experiencing sleep disturbance, some of whom may be ready to engage in behaviors to improve their sleep.
Drawing from the Modified Spielman’s 3P model, 23 caregivers in the unchanged and dissatisfied profile most prominently identify predisposing and precipitating factors of their sleep disturbance. These factors were present before caregiving and included early life trauma, death of a loved one, and significant work stress. Some caregivers in the unchanged and dissatisfied profile reported using medications, but they didn’t have much success with them or used them inconsistently to experience any significant improvement in their sleep. Some also used some behavioral techniques but without much success, as they remained discontented with their sleep quality. These sleep-distressed and dissatisfied caregivers may have more motivation to pursue and engage in behavioral treatment than caregivers who deny any distress associated with their sleep, thus even if caregiver burden remains constant, they may respond more readily to evidence-based sleep interventions, such as Cognitive Behavioral Therapy for Insomnia (CBTI), where both motivation and insight into clinical concerns predict treatment success. 32 Of note, none of the caregivers who were dissatisfied mentioned referral to or being treated by a behavioral sleep medicine provider. This reflects what is seen in the literature with referral rates for CBTI being low among primary care providers and lower in patients older than 45 years compared to patients younger than 45 years. 33
CBTI is a first-line behavioral treatment for insomnia.32,34 The principles of CBTI include behavioral modifications such as stimulus control, sleep consolidation, sleep hygiene, relaxation training, and cognitive therapy. The goal of CBTI is to adjust sleeping habits and use cognitive strategies to change thoughts, feelings, and expectations concerning sleep. Treatments tailored to caregivers recognizing their unique role, including adaptations to CBTI, may help to increase treatment effectiveness and engagement. 9 Adaptations may include teaching caregivers about stress management, managing behavioral and psychological symptoms of dementia, and including the PLwD in the treatment sessions. For example, the cognitive therapy sessions of CBTI for the unchanged and dissatisfied caregivers could integrate ways to restructure unhelpful sleep thoughts with developing new coping strategies for dealing with past trauma, work stress, and other non-caregiving stressors. For the changed and dissatisfied caregivers, these sessions could focus on the coping strategies for the stressful situations that accompany caregiving.
Since CBTI is a behavioral intervention, intervention developers should take into account that caregivers’ expression of their intention to perform a behavior is the closest determinant of an individual’s behavior and is determined by their attitudes toward the intended behavior, subjective norms, and their perception regarding whether they can control their behavior.35,36 Health care providers and researchers can aim to improve caregivers’ attitude to managing their sleep disturbance by emphasizing the benefits of the behavior change, facilitating support for caregivers from loved ones, and through assigning achievable tasks over a given period of time. 37 These efforts may increase the caregivers’ intention to participate in the recommendations of CBTI. While caregivers may be motivated to improve their sleep due to emotional and physical repercussions of the sleep disturbance, they may have caregiving and other responsibilities that are interfering with their intention. The Health Action Process Approach recognizes that intention may not lead to action, so it proposes action and coping planning to assist caregivers with developing plans regarding how they would put the practice into action and identify how they would overcome obstacles to putting the plans into action.36,38,39 Health care providers can support caregivers as they develop these plans and researchers can develop tailored caregiver sleep interventions using these frameworks.
Caregiving precipitated sleep disturbance for the changed and dissatisfied profile caregivers. In both categories, these caregivers have developed habits such as sleeping outside of the bedroom, inconsistent sleep-wake schedules, or lying in bed worrying which all perpetuate their insomnia symptoms but have not yet started taking steps to manage their sleep. This group of caregivers along with caregivers who fall within the changed but satisfied profile may not be ready to engage in behavioral interventions to improve their sleep but may still be open to education about how to prevent worsening of their sleep. These caregivers may benefit from anticipatory guidance regarding when they may need to seek additional support for their sleep changes and from education about CBTI principles. Health care providers can also specifically assess their sleep pattern to be able to identify any change in the caregivers’ sleep patterns during future provider visits and when intervention may be needed.
The findings of this study reinforce the importance of asking caregivers targeted clinical sleep questions to evaluate their risk and appropriateness for behavioral treatment. For example, general questions about sleep in this population may not reveal meaningful changes in sleep quality or impairment. Instead, asking specifics about perceived changes in and subjective distress about sleep patterns with caregiving (e.g., sleep onset latency, number of awakenings, reasons for awakening, frequency of early awakenings, naps, daytime consequences) may more sensitively identify and direct at-risk caregivers to intervention. Moreover, there is an inherently subjective (vs. objective) nature of both sleep disturbance and caregiver burden, supporting the importance of using both objective and subjective measures of these constructs in clinical evaluation. 40
While study findings offer promising implications for the clinical evaluation and treatment of caregivers of PLwD, these results warrant interpretation in the context of the study’s limitations. First, qualitative research operates as an inherently subjective exercise that typically uses small samples. 41 However, the coding process included best practices for mitigating bias, including reflective memoing, audit trailing, and third-party discrepancy management. 42 Further, prior research illustrates the utility of semi-structured interviews in identifying unique health issues facing adults, as well as for developing health promotion programs.43-45 Purposive and convenience sampling methods can produce selection bias and either over- or under-represent particular groups within a sample. For example, the current sample only included caregivers of persons with Alzheimer’s disease, and we had no Hispanic participants. Notwithstanding, the study captured other important sources of diversity in terms of age, stage, years of caregiving, and caregivers’ place of residence. The interviews were conducted after caregivers participated in the primary study for 6 months so it is possible that the intervention content to which participants were exposed could have affected their responses or perceptions. Topics such as meditation or relaxation (discussed in the intervention) or exercise (discussed in the control) could improve caregivers’ sleep patterns and perceptions; however, most caregivers interviewed still experienced some insomnia symptoms. This suggests that even with receipt of the intervention, which could have improved their sleep, sleep disturbance was still present among these caregivers. Notably, sleep was not a topic discussed within the intervention or the control group sessions. Finally, it is reasonable to deduce that caregivers may have been providing care for many years and there is a concern that caregivers may not remember their satisfaction with sleep prior to becoming caregivers.
Chronic poor sleep has appreciable immediate and long-term consequences (e.g., increased risk for developing cognitive impairment) that can affect caregiving. 46 Notwithstanding, no study to date has conceptualized, described, and proposed a framework with which to identify and describe caregivers’ sleep profiles with caregiving. Findings point to important subjective changes in sleep-related quality and distress among caregivers as well as potential reservoirs of resilience among an at-risk group. This research provides formative data and one such initial guiding framework. Routine, specific, and sensitive screening of sleep concerns among this population before—as well as ongoing evaluation throughout caregiving—can help to detect, treat, and prevent sleep problems in this at-risk group. Finally, future research should further refine these profiles, identify their caregiver-specific features, and evaluate their utility in predicting treatment appropriateness and response.
Footnotes
Author Note
Glenna S. Brewster: 1520 Clifton Road, Room 256, Atlanta, GA 30322, P: (404) 712-9164, Email:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Glenna S. Brewster was supported in part by grants from the National Institute on Aging (R01AG054079, PIs: Hepburn/Griffiths; K23AG070378, PI: Brewster), the PRIDE Institute with funding from the National Heart, Lung, and Blood Institute (R25HL105444, PI: Jean-Louis/Ogedegbe), and the Alzheimer’s Association (2019-AARDG-643440). Dr Fayron Epps was supported by an award from the National Institute on Aging (K23AG065452). Dr Kalisha Bonds Johnson was supported by a T32 postdoctoral fellowship awarded to Emory University from the National Institute of Nursing Research (T23NR012715, PIs: Dunbar/Song).