
Abstract
Background:
The absence of primary care providers’ participation in school health care may require close collaboration between school health teachers and parents. This study explores maternal perspectives on obstacles and improvements in partnerships with school health teachers of children with type 1 diabetes.
Methods:
Participants were recruited using purposive sampling through an online type 1 diabetes self-help group in South Korea. Twenty-two mothers whose children were aged between 7 and 13 and had been diagnosed with type 1 diabetes at least 1 year ago were included. Individual interviews were conducted based on a semi-structured interview guide from February to June 2019. Qualitative data were analyzed using inductive content analysis comprising open coding, coding sheets, grouping, categorization, and abstraction.
Results:
Mothers recognized obstacles in eight categories and improvements in nine categories under institutional, interpersonal, and intrapersonal aspects of the partnership with school health teachers. Respondents recognized insufficient legal coverage and guidelines, and also health teacher shortage and workload as obstacles in the institutional dimension. Mothers perceived building trust, compromising to balance responsibilities, and constant and open communication as improvements in the interpersonal dimension. They recognized practical competency and tailored care for ordinary school life as school health teacher-related improvements.
Conclusions:
The findings indicate that school health teachers should compromise to balance responsibilities to improve partnerships with parents in the school health care setting. Institutional improvements, such as establishing robust laws and clear guidelines and increasing the number of school health teachers, should be prioritized.
Keywords
Type 1 diabetes (T1D) is a primary chronic condition in children and adolescents that requires lifelong self-management. In 2021, 1.2 million children and adolescents suffered from T1D, and 149 500 were newly diagnosed. Europe has the highest incidence of childhood diabetes, occurring in 300 000 children and adolescents annually. 1 The parents of children with T1D face a variety of challenges in managing their child’s diabetes. They struggle to protect their children in an ever-changing environment. 2 Most qualitative studies on parents’ experiences of caring for children with T1D have been conducted with mothers, which relates to mothers shouldering the main caring responsibilities in diabetes care. 3 Similarly, in South Korea, mothers are mainly in charge of daily diabetes management, 4 and they are more actively involved in school health care (SHC) for their children’s chronic disease than fathers. 5 Mothers reported higher parental burden and emotional stress than fathers did. 6 They experience concerns about SHC because children spend considerable time in school. Children with T1D need periodic blood glucose tests, insulin administration, and adequate ability to cope with sudden hypoglycemia or hyperglycemia at school. Some mothers of young children attend the school daily to administer or supervise insulin for their child with T1D. 7
The European framework for school health services requires that school health professionals coordinate an individual care plan that harmonizes the medical needs in school, 8 although the laws and policies of SHC for children with chronic diseases vary from country to country. 9 Collaborative partnerships between parents and school staff foster child-centered supportive care in the United Kingdom, the United States, and Australia.7,10,11 Specifically, the school nurse, who is the only medical personnel available to manage children’s health, educate children in self-care, and empower children, 12 is of utmost importance for a safe and successful school life. In addition, parental engagement and participation in creating their child’s individualized care plan is crucial.13,14 Families living in areas with difficult access to hospitals have strong demand for family-school partnerships. 15 Parental participation in SHC and partnerships with stakeholders are related to the child’s self-management. 16 In this context, communication and cooperation between parents and the school nurse are crucial for effective diabetes care in the school setting. 13
Some developed countries have effective laws and policies pertaining to the SHC of chronically ill children, and primary care providers (PCPs), school nurses, school professionals, and families cooperate accordingly. 17 However, in certain countries, the SHC of children with T1D in terms of daily health management (i.e., blood glucose testing and insulin administration) is highly dependent on parents.18,19 Even in South Korea, policies for SHC are not well addressed. One-third of children with diabetes perform blood glucose testing by themselves at school, and over 30% self-administer insulin in their school bathroom. 20 Due to the absence of a systematic linkage between SHC and public medical services—in particular, the absence of PCPs’ participation in SHC—the action plans or individual care plans for chronically ill children in schools are insufficient.
In South Korea, school nurses are called school health teachers (SHTs). SHTs must have a registered nurse license and pass a national qualification examination to become full-time SHTs working in public schools. The legal roles of SHTs, such as health screening, emergency treatment, vaccination, and the management of chronically ill children, are similar to those of school nurses in other countries. The roles of teacher and nurse have been emphasized in SHC, such as teaching 12 hours of health classes per week. Emergency medications, such as glucagon or epinephrine which can be administered by SHTs, have been implemented in hypoglycemic or anaphylactic shock situations since December 2021; however, there is no specific scope of health care for children with diabetes or the role of SHTs to maintain stable blood glucose levels of these children in school. 21 In SHC, excluding PCPs may require close collaboration between SHTs and parents in caring for children with T1D. However, studies regarding the perceptions of stakeholders in SHC on the partnership between SHTs and parents are limited. Identifying obstacles and facilitators regarding SHC partnerships can provide important implications for the development of SHC in countries where PCPs’ involvement in SHC is limited, such as South Korea. This study examined maternal perspectives on partnership with SHTs for children with T1D. Accordingly, we proposed the following research question:
Methods
Study Design
This study employed an inductive directed content analysis. 22 The authors verified this qualitative methodology using the Consolidated Criteria for Reporting Qualitative Research checklist. 23
Participants
Participants were recruited using purposive sampling through an online self-help group for parents of children with T1D in South Korea. Before recruitment, the primary researcher introduced the study purpose, process, and implications in a meeting with the president of the self-help group and its members. Mothers whose children with T1D were aged between 7 and 13 years and had been diagnosed with T1D for at least 1 year were included. Initially, 22 mothers volunteered to participate in the interview through the self-help group and none dropped out. The chairperson of the self-help group provided information about the research in the members-only group chat room to recruit participants. The participants were sampled until the responses to the research question reached saturation. 24
Ethical Considerations
The Research Ethics Review Committee of Daegu Haany University, to which the researcher was formerly affiliated, approved this study (DHUMC-D-19002-PR0-01). Participants commenced the study after receiving an explanation of the study purpose and method and providing written informed consent.
Data Collection
The researcher personally contacted the applicants to participate in the study and conducted the interviews after setting a preferred interview date and location. Individual interviews were conducted with the participants; they lasted for a mean (±SD) of 57.6 (±11.7) minutes and were carried out once from February to June 2019. Most interviews occurred at the participants’ homes, but if this was unfeasible a rented private space near the home was used temporarily to conduct interviews.
The interviews were recorded with the participants’ consent, and field notes were written. All recorded content was transcribed and transferred to NVivo software (Release 1.2, QRS International) for analysis. The interviews were based on a semi-structured interview guide and conducted by the primary author. Key questions included what difficulties mothers were experiencing in working with the SHT and what they thought needed to be improved to work effectively with the SHT to support their child. No pilot interviews were conducted. When the contents were deemed saturated, data collection was terminated. If the participants requested a transcript of the recording, it was mailed to them. The interviewer was a Korean woman in her mid-40s with 16 years of clinical experience as a registered nurse and clinical nurse specialist in a pediatric critical care setting. The interviewer had completed qualitative research classes in graduate school, had experience in another qualitative research study, and in addition, learned qualitative data collection practices and analysis methods through participating in workshops, including NVivo workshops for coding.
Data Analysis
The collected data were analyzed according to the inductive approach to qualitative content analysis procedures suggested by Elo and Kyngäs, comprising open coding, coding sheets, grouping, categorization, and abstraction. 22 For data analysis, the researchers repeatedly read the transcripts to find important sentences or phrases, grasped the meaning, and created codes using NVivo. Open codes about meaning units were applied as labels by 2 authors. Conflicting opinions were discussed until a consensus was reached. Similar codes were formulated and grouped into subcategories, and these subcategories were further integrated into categories.
Methodological Considerations
To verify credibility, suitable meaning units were classified based on the similarities and differences, representative quotations were presented, intercoder agreement was checked to seek the experts’ approval of the codes and categories, 25 and 3 participants reviewed the validity of the subcategories; no changes were made after the review. 26 Peer researchers conducted investigator triangulation to make decisions related to coding, analysis, and interpretation with labeling regarding the abstraction process by condensing a suitable meaning unit in the texts. 27 To facilitate transferability, describing in detail the SHC-related environmental aspects in South Korea and the data analysis process was significant. For securing dependability, the researchers verified whether the codes, subcategories, and categories were similarly achieved several months after the first analysis. 26
Results
Participant Demographics
Twenty-two mothers of children with T1D were interviewed (Table 1). The participants identified obstacles and improvements in the factors under the institutional, interpersonal, and intrapersonal (mother- and SHT-related) dimensions that must be addressed to improve partnership with SHTs for children with T1D (Table 2). Eight main categories, 45 subcategories, and 110 codes emerged (see Supplementary file). There were 39 codes for obstacle factors, but 71 codes for improvement factors, and mothers expressed more perspectives on improvements than on obstacles.
Participant Demographics (N = 22).
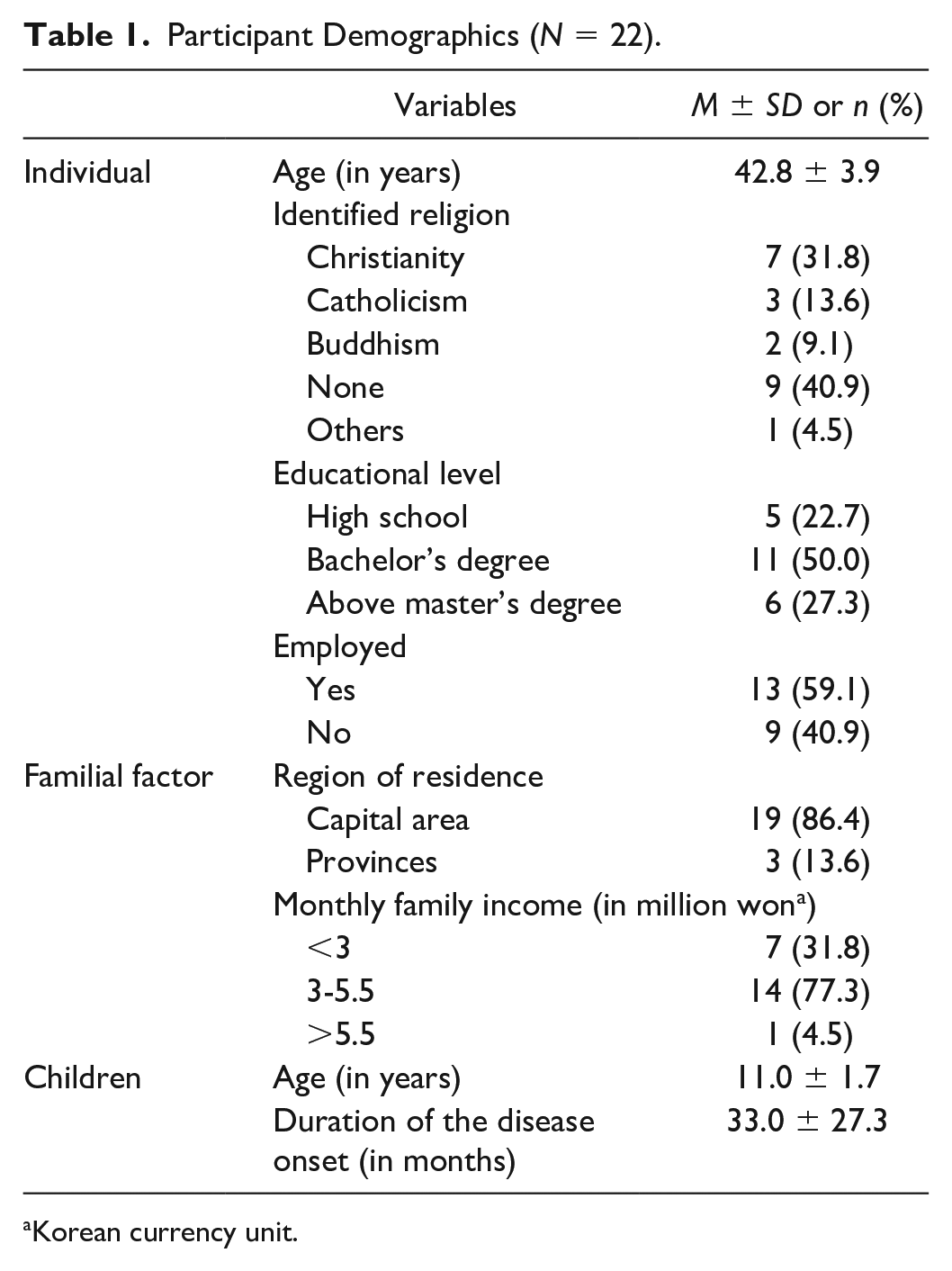
Korean currency unit.
Categories of Obstacles and Improvements in Partnership with School Health Teachers.
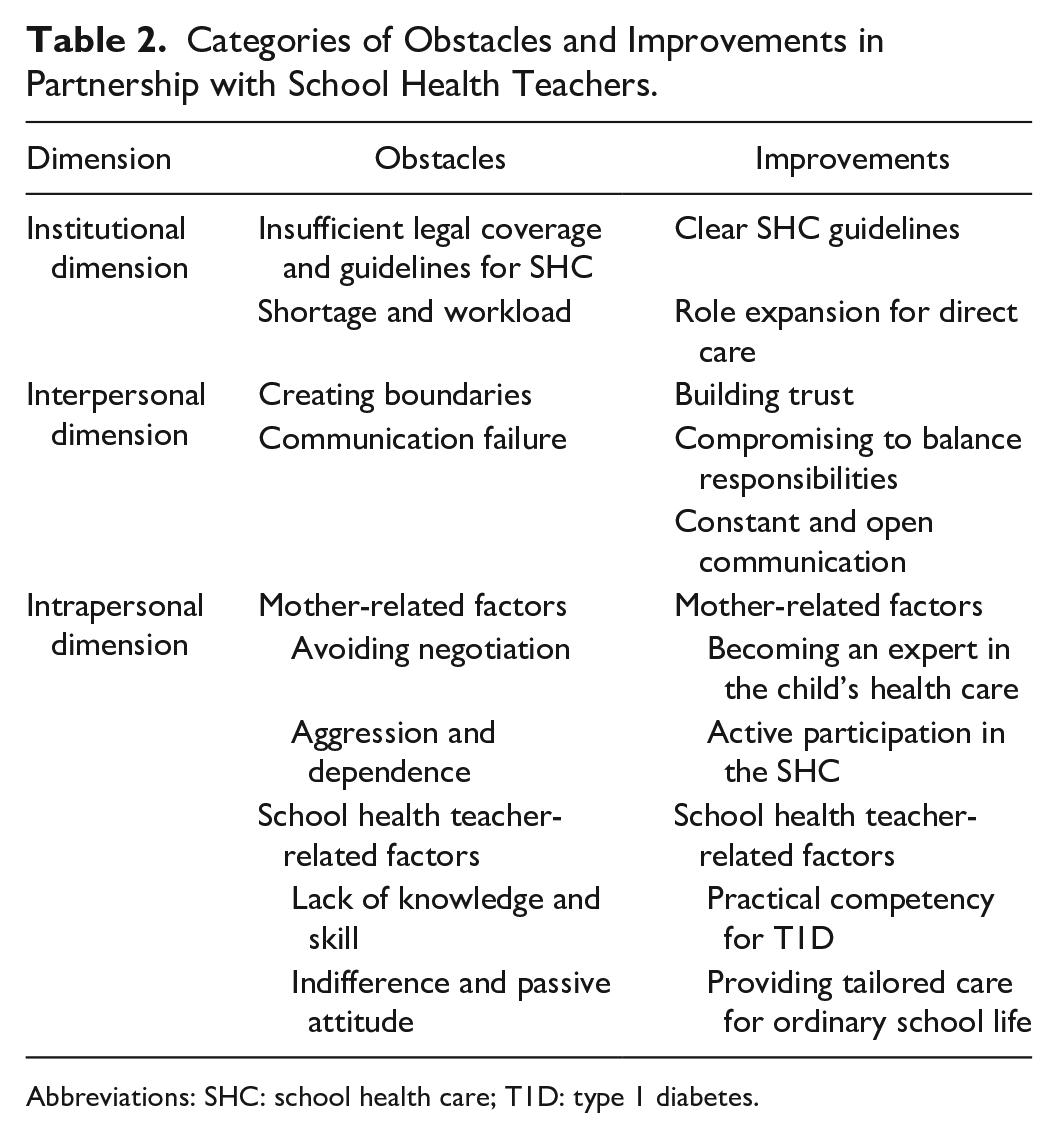
Abbreviations: SHC: school health care; T1D: type 1 diabetes.
Institutional Dimension
Institutional obstacles
Insufficient legal coverage and guidelines for school health care
The Korean School Health Act does not stipulate the specific scope of school health teachers’ responsibilities in managing chronic diseases other than first aid. The law only allows them to provide first aid, including medication, to students whose lives are in danger due to conditions such as hypoglycemic shock or anaphylactic shock. While the Enforcement Decree of the School Health Act (Article 23) presents “management of patients found to have diseases” as a duty of SHTs, it does not specify the extent of “disease management” either. The participants were aware of the inadequacy of the School Health Act, owing to the absence of specific rules for SHC for children with T1D or for the scope of SHTs. Mothers emphasized that the absence of the SHTs’ legal responsibility for routine blood glucose tests or insulin injections in schools makes it difficult to cooperate with SHTs on daily routine SHC. Since SHTs were only legally permitted to administer glucagon injections in emergency situations, mothers had to rely on SHTs’ good intentions to manage T1D for their children at school.
Since SHC for children with chronic diseases has not been systemized and the content has not been specified based on laws and guidelines, the SHT should decide on the level of collaboration according to their convictions, resulting in a situation where the quality of care cannot be guaranteed. If the guidelines are vague and incomplete due to the lack of legal justification, confusion will inevitably arise for SHTs and parents, and responsibilities will be unclear. This lack of clarity has led to limited cooperation between parents and SHTs. Specifically, some participants pointed out obstacles such as ineffective health surveys, lack of preemptive preparation, and lack of records or handover regarding diabetes care in school. Some mothers recognized that absence of rules for field trips and exclusion from after-school classes leads to discrimination of children:
I believe that the role of the school health teacher is limited to providing space beside the health office and storing items because they cannot even perform a blood glucose test. (Mother03) I told the school in advance when my child would be admitted to the school, but the school was not prepared for anything. (Mother14)
Shortage and workload
Participants pointed out the burden of work for SHTs. That is, the problem of assigning 1 SHT to many children led the SHT to make less effort at building partnerships. Mothers were aware that an SHT has a considerable amount of routine work, such as immediate nursing interventions for children who visit the health office due to sudden health problems, a large volume of paperwork, and lectures in health class. They recognized that SHTs remain too busy to continuously manage children with chronic diseases because 1 SHT has to take care of up to 1000 or 2000 students in a school and deal with unexpected situations like sudden injuries or acute illnesses:
There are insufficient school health teachers. There are things that school health teachers should do to take care of the children, and they also teach the fifth-grade classes as subject teachers. (Mother03) There were many cases where the school health teacher was absent from the office. Although the health office’s door was open when the school health teacher was giving a lesson, there was no school health teacher to give the child an injection. (Mother04)
Institutional improvements
Clear SHC guidelines
The participants mentioned that clear guidelines for SHC established by the Ministry of Education for children with chronic diseases would strengthen the partnership. It was believed that establishing a structured SHC process at the school level using comprehensive guidelines could create a supportive and safe SHC environment. Participants thought that preemptive preparation before admission, a tight-knit network among school professionals, and regular meetings between school professionals and parents could facilitate close cooperation among schools and families. For example, the details included education and training policies for school professionals, the development of a supportive environment such as the provision of a safe insulin injection place, and rules for class exceptions, such as permission to drink juice in class when hypoglycemia occurs. Moreover, respondents emphasized that the comprehensive standards to create a safe school environment for diabetes care should be included in the guidelines in detail:
“A kid with diabetes came in!” Suddenly something happened at school. It’s not like this, but a manual should be provided to the school as a policy. (Mother02) If the Ministry of Education provides guidelines, aspects of certain responsibilities, such as the scope of the school’s accountability, will become clear. If such requirements are well met, I will unquestionably expect school health teacher and demand it too. (Mother07)
Role expansion for direct care
Some participants expressed the need for expanded role descriptions for SHTs who become more actively involved in their child’s care to help improve partnerships with the SHTs. It is necessary to create an environment where SHTs can focus on children’s nursing care through being more involved in diabetes care and reducing their existing workload. Mothers said that robust legal support should be provided for more aggressive direct care for children with T1D in school. Establishing a formal scope of responsibility for a wider scope of physical care, such as the administration of insulin injections by SHTs, was considered necessary for partnership:
“How about installing an app address so that the school health teacher can occasionally see the child’s blood glucose trend on the computer monitor?” I talked about that with my husband. (Mother11) I think it would be better if the school health teachers would perform more healthcare-related work and eliminate certain administrative tasks. (Mother20)
Interpersonal Dimension
Interpersonal obstacles
Creating boundaries
The participants perceived that the SHT, by clearly specifying their limited role, could not accept any further demands, which the mothers expressed as “drawing a line.” Creating boundaries, that is, the overly strict attitude of the SHT toward demands beyond their legal responsibility, hinders cooperation. This renders it difficult to balance the needs and roles of both parties through negotiations of the SHT’s responsibilities. The preliminary explanation of what is not legally specified and the SHT’s unconditional refusal of roles not described by law were obstacles to partnership:
In our case, the school health teacher drew a line initially; thus, I did not make any requests. Since I am a full-time housewife, I thought that I could do it myself, and I have done so since the beginning. (Mother09) Whenever I visit, she tells me “Mother, I will not give your child injections.” She talks about rules first. Mothers would not make unreasonable requests. We do not even want injections. (Mother15)
Communication failure
The mothers mentioned that they experienced a lack of contact, unidirectional communication, and missed information as barriers to partnership. Participants experienced interpersonal conflict when they did not accept each other and when they considered opposing views regarding the role and responsibilities of the SHC. The communication failure worsened the relationship with the SHT. The participants considered it an obstacle to cooperation when there was no contact from the SHT or the SHT did not answer parents’ calls and when the other party did not respond or did not accept a request:
Since the school health teacher only listens to what I have to say and reacts to it, I don’t think it contributes to discussions about the child or character of the child. The school health teacher says, “Oh, is that so?” or “Ah, yes.” The conversation ends in such a manner. (Mother10) When the school health teacher was on vacation, she went away without saying anything. “Mom, the school health teacher wasn’t there.” There were gaps in our child’s healthcare. (Mother16)
Interpersonal improvements
Building trust
The participants recognized that building a basic relationship of trust is important for successful cooperation between SHTs and parents. They recognized that mutual confidence and respect were necessary for a trusting relationship. Since the relationship with the SHT is reciprocal and is influenced by the SHT’s attitude or behavior, it is necessary to maintain mutual empathy and politeness. In particular, the respondents thought that speaking carefully and being polite when communicating or making requests was more important than anything else:
Saying, I trust that the school health teacher will take good care of my child, so I’m not worried and asking What is the school health teacher doing? are very different. (Mother06) We need consideration and respect for each other. We need to cooperate with each other and help each other. (Mother17)
Compromising to balance responsibilities
The participants recognized that the process of balancing roles by adjusting to each other’s needs is important to harmoniously meet the children’s optimal health care goals. It is necessary to recognize accurately what can be reasonably demanded of an SHT and what parents should strive for in terms of a child’s SHC, considering the contextual situation of the SHC. Some parents wanted to get as much help as possible from an SHT, but most parents were concerned that some parents had made unreasonable requests of the SHT to manage their children’s health care, or depended unduly on the SHT as they were aware of the institutional limitations of SHC. They believed that these compromises related to a shared responsibility between parents and SHTs and their common plans would enhance the child’s self-care competency and enable a healthy school life:
Parents have to go to school every day. However, when an unexpected situation arises, such as when the data transmission of continuous glucose monitoring is cut off or when the sensor is disconnected, I think that the help of the school health teacher should be sought first. (Mother12) I think that the school health teacher should take care of the child to some extent, but that the parents should not completely depend on the school health teacher to manage the child’s health. (Mother19)
Constant and open communication
Smooth communication between SHTs and parents would ensure that children with chronic diseases have a smooth school life. The mothers said that establishing a trusting relationship through smooth communication is essential for a cooperative relationship. For communication, periodic contact and regular and official meetings with the SHT are needed. They said it is necessary to share information with each other through continuous or frequent contact, and some mothers said that the SHT serves as a bridge between the family and the school and between the family and the homeroom teacher. It was recognized that an open mind, that is, a willingness to listen to or accept different ideas or opinions, should precede effective communication between both parties:
What I hope is that the school health teacher will give me a phone call and communicate with me at least once during the semester. (Mother13) I believe that we need to talk often to be able to communicate. The most important thing is that something should be communicated—whether we discuss it in-person or over the phone—rather than making decisions alone. (Mother21)
Intrapersonal Dimension
Mother-related obstacles
Avoiding negotiation
Some mothers performed SHC for their children alone, without the aid of an SHT. Avoidance of negotiation and taking solitary actions for their children were related to low expectations of SHC quality and the perception that children’s health care in school is the parents’ responsibility. It was believed that care coordination by the SHT is impossible under the current circumstances. Some participants expressed that their children’s SHC was “my job” and tended to perform it alone as much as possible because they thought it would be burdensome for the SHTs. In addition, the child’s tendency to depend on the mother rather than the SHT was a factor limiting cooperation:
“How will I take responsibility if something goes wrong?” However, unless you overdose the insulin, it is unlikely that it will happen. Thus, parents have to decide. (Mother06) It’s not that I don’t trust the school health teacher, but after seeing the situation in the health office for a month, I have come to the conclusion that it is absolutely not something the school health teacher can manage. (Mother07)
Aggression and dependence
Some mothers mentioned that their aggression and dependence were a defense mechanism against the rejection of the mothers’ requests that restricted cooperation. One mother said that parents’ past experiences of being treated unfairly or discriminated against in relation to their children’s health care during kindergarten or the primary school years could indicate aggression or dependence, which hinders cooperation with the SHT. If negotiations or shared responsibilities were not achieved, some mothers skipped communication with the SHT and used civil complaints, but these methods actually weakened cooperation:
If mothers are treated unfairly or if they do not accept this appropriately through such a bad experience, they will be unable to open their heart to others or will become dependent on someone. (Mother08) It seems that mothers are constantly attacking because of defense mechanisms. However, if the other party does not accept it, the relationship worsens and it seems to create a deeper conflict. (Mother17)
Mother-related improvements
Becoming an expert in the child’s health care
Participants believed that understanding the current operating status of the SHC and recognizing its institutional limitations must be prioritized. Participants recognized that they should become experts in T1D management and SHC. Several mothers said that the use of a continuous glucose monitor or insulin pump made reliance on school staff unnecessary.
One mother mentioned awareness of the environment surrounding SHC and the legal scope of the role of the SHT—an objective view rather than one appealing to emotions. Some mothers also mentioned the importance of the role of a self-help group in acquiring professional knowledge related to SHC and sought peace of mind through psychological counseling:
The best thing was that we had a meeting at the SugarTree [online self-help group] to learn about preparations before school admission. I didn’t know what to ask of the school or how to deliver the child’s condition before that. It was helpful to learn to write a letter to the school health teacher before school admission. (Mother02) For chronically ill children, their parents need to study considerably about the latest information or trends. I think that the mothers do not have the required knowledge, and they cannot manage the child’s blood glucose appropriately; thus, they want an school health teacher to manage it, which does not seem to work anymore. (Mother08)
Active participation in SHC
The participants recognized that active participation in SHC was a factor in improving collaboration with the SHTs. Most respondents desired to fill in the gaps in SHC by participating in delegated care for their children. They anticipated that the school staff would focus on their children through their efforts. The mothers actively participated in their children’s SHC and played the role of a strong guardian for their children until the latter became psychologically independent and wanted independent self-care. The mothers taught their children self-care precautions, such as preparing insulin and low-glycemic snacks at school:
I always provide that information. I always say “Hello” even to the janitor. I tell it to the school guardians as well. Thus, if my child falls down or experiences an emergency while playing, they can take immediate action on the playground. (Mother18) My child can self-inject; nevertheless, honestly, I still want to look after him. From a parent’s viewpoint, self-injection immediately after onset is extremely unfortunate. Thus, I want to do as much as I can. (Mother22)
School health teacher-related obstacles
Lack of knowledge and skills for managing type 1 diabetes
Most participants reported SHTs’ inadequate competence, such as insufficient knowledge about T1D and its management, including dealing with devices, practical skills, and lack of communication and interpersonal skills. They said that SHTs’ lack of knowledge about children’s chronic diseases could negatively affect communication with parents. This lack of practical ability among SHTs made them feel burdened and fearful of caring for children with T1D, which in turn made it difficult to cooperate with parents. Some respondents also cited a lack of understanding of diabetes management skills and how to interact with their child as a factor undermining cooperation:
That is inaccurate knowledge. school health teachers who are uninformed about type 1 diabetes seem to be overburdened by care for children. (Mother12) The school health teacher was very afraid of the injection because she had not given the injection and did not have much clinical experience. (Mother21)
Indifference and passive attitude
The mothers expressed that the SHT’s passive attitude and indifference were barriers to their partnership. They perceived that there was no information on T1D due to the SHT’s lack of enthusiasm in caring for their children and indifference to their children’s diseases. The bureaucratic, rigid, and passive attitude of the SHT was also a factor in limiting cooperation with the mothers. In addition, the mothers perceived that failing to assist their children’s self-care or provide them with supportive care was an intrapersonal obstacle for the SHT:
The school health teacher was businesslike and rigid. “Oh, I should just do it alone” I thought. (Mother10) The school health teacher does not even carry out basic precautions such as waiting for the child to fully administer the insulin; hence, the school health teacher does not care altogether. (Mother20)
School health teacher-related improvements
Practical competency for type 1 diabetes
Improvement factors recognized by most mothers regarding SHT included enhancement of the SHTs’ competencies, such as knowledge and practical skills. They mentioned that SHTs should be knowledgeable about T1D management and possess communication and interpersonal skills. Mothers believed that the practical ability to cope with real situations without embarrassment to enable SHTs to perform prompt and critical nursing management in an emergency was important. With the recent increasing use of devices such as continuous glucose monitoring in diabetes care, demands were made for SHTs to understand the new diabetes management technologies. They recognized that SHTs’ professional, active, and responsible attitude is required to achieve a safe school life for children with chronic diseases, along with the development of these practical competencies for T1D. Respondents said that the welcoming and comfortable attitude of mothers during visits was a factor that facilitates partnerships, besides a sense of duty as an SHT:
As a medical professional, the school health teacher must have an active attitude, and a lot of intense training will be needed to cope with emergency situations. (Mother05) I hope that the school health teacher would like to gain some knowledge about diabetes management mechanisms, such as [continuous glucose monitoring app’s] screen correction value, blood glucose trends, and how to charge and replace the battery. (Mother18)
Providing tailored care for ordinary school life
Participants recognized that more individualized physical and psychological nursing and self-care education are needed to strengthen partnerships. Even if direct injection by the SHT is not possible due to legal issues, mothers wanted the SHT to monitor self-injection to ensure that the medication was administered correctly and safely. Mothers believed that SHTs should reinforce children’s self-care. Furthermore, they stated that psychological support for children and their parents is required to enable successful disease management. They wanted SHTs to show some interest in ensuring their child’s seamless school life without discrimination and the negative impact of diseases. Specifically, respondents thought it most important for their children to maintain good relationships with their peers and be with them in school. Therefore, they also wanted the SHT to educate their children’s peers on T1D so that the peers would not make fun of or ridicule their children due to misunderstanding T1D. In terms of psychological support for their children, the mothers believed that the SHT’s warm-hearted and thoughtful attitudes, attention, and consideration were needed. Some respondents indicated that advocating for children, such as by protecting privacy, providing appropriate places to perform injections, and requiring the SHT to accompany children on field trips, was necessary to strengthen partnerships:
It is to provide psychological support to the child. There is practically nothing to help. Since it is a space without a mother, the school health teacher acts instead of a mother. (Mother01) Later, the school health teacher taught my child because he now has a knack for it. “Hey A, now that you have a high blood glucose level, how much insulin do you need to release? Is it two (units)? That’s right.” I truly liked that the school health teacher educated the child. (Mother15)
Discussion
This study explored maternal perspectives on the partnership between the mothers of children with T1D and SHTs. First, as predicted, the mothers identified that institutional obstacles and improvements should be prioritized to improve cooperation with SHTs. Korean mothers recognized this absence and the need for a new SHC system to implement such a written action for managing chronic conditions at school. This finding is in line with studies conducted in Spain, Saudi Arabia, and Ireland, wherein parents recognized legal and policy issues as barriers to SHC for children with T1D.18,19 The mothers recognized the need for SHTs’ active involvement and responsibilities through legal enforcement. Similar to this finding, a previous synthesis study recommended a robust and supportive legal system to provide an adequate workforce to cope with children with T1D. 28 The most complicated issue in SHC partnerships is between SHTs and parents’ concerns the prescription of insulin doses; the possibility of undesirable events occurring, such as medication errors or hypoglycemia due to medication, and the issue of liability in case of such events is also a concern. Increasing the legal responsibility of active SHTs, such as for administering injections, entails the problem of adding responsibilities to the official duties of SHTs without increasing staff or adjusting the workload. To solve this problem in the current SHC context, SHTs and parents should understand each other’s positions first. Based on this understanding, a reasonable method should be devised. It is necessary to prepare detailed guidelines and increase the number of SHTs to strengthen the direct care role of SHTs. Even if the improvements recognized by parents have been resolved, the task of preparing a system for communication between the child’s pediatric endocrinologist and SHT in the SHC context remains; that is, the medical record sharing, a reporting system, and the medical fee.
Regarding interpersonal aspects, establishing a trusting relationship is a well-recognized element of the partnership between SHTs and families. Compared with previous studies on attributes of partnership in nursing29,30 and in SHC for children with chronic health conditions, 31 the compromising to balance responsibilities category, under interpersonal aspects, relates to negotiation, shared responsibility, and parental participation. Although the Korean School Health Act has been improving gradually, the issues regarding medication prescriptions and responsibilities remain unresolved. Parents who did not know the limitations of the school medical system in detail requested injections and routine testing from the SHT. Korean mothers recognized SHTs’ rejection of health care tasks, such as insulin administration and blood glucose testing, as an obstacle and expressed that “the SHTs drew a line.” Thus, unresolved laws, policies, and institutional problems eventually caused interpersonal conflicts. This situation contrasts with the legal guidelines in the United Kingdom, which stipulate that if a child cannot self-administer the medication at school, administration should be performed by the school staff with the written consent of the parent and the principal. 11
Despite the poor and confusing SHC-related legal and institutional circumstances, many Korean mothers have been dedicated to participating in SHC, cooperating with SHTs, and finding unique ways to take care of their children’s health and maintain their children’s safety and well-being in school. This action is seen as an effort to overcome institutional limitations and maintain relational balance. This finding is in line with a meta-ethnographic synthesis that found diabetes care at school is negotiated on an individual basis, which is challenging for diabetes nurses, parents, and schools. 28 The mothers in the present study have attempted to ensure that their children experience ordinary school life while maintaining a trusting relationship with SHTs and fulfilling their responsibilities regarding SHC. They may participate considerably more in care than the health or homeroom teachers do. In addition, the mothers recognized that the SHTs were the only school health partners who could take care of their children in an emergency and be trusted, even if the latter were not legally responsible for direct nursing care or had minimal involvement in SHC. If an improvement is not made in the foundational process of Korea’s SHC system, including legislation, policies, and schools, it is predicted that the mothers’ role in balancing the responsibilities will remain important.
Two-way communication is also a critical factor in the partnership between parents and SHTs in implementing SHC. 32 If it is impossible to produce a written care plan—a so-called 504 plan, according to an individualized diabetes management plan or a health care provider’s order as in the United States—close communication between the SHTs and parents is essential. Some parents in the present study gave up negotiating for cooperation in SHC and performed their children’s diabetes care independently without the help of an SHT. Otherwise, aggressive or excessive reliance on SHTs also hindered cooperation. In a previous study, parents’ depression or anxiety led to more maladaptive coping strategies such as avoidance and distraction. 33 In an environment where individualized SHC is created for a child, parents will also try to cooperate through negotiation and sharing of responsibilities.
Regarding intrapersonal aspects, the expertise of the other party, parental participation, and the SHTs’ competencies for T1D are critical attributes of a partnership. 34 Most parents of children with T1D attempt to reduce uncertainty by seeking information, joining support groups, and turning to technology. Lack of knowledge and misunderstanding about T1D in society affect the daily lives of parents and children. 35 For example, in a recent study Korean SHTs’ knowledge on hypoglycemia management was 9.6 out of 14 points, and this knowledge was a factor influencing diabetes management competency. 36 In a UK survey, 42% of school nurses were confident in diabetes care; this was lower than the 70% for asthma and 58% for epilepsy care. 37 Among school nurses in Poland, the rate of correct responses regarding TD1 knowledge was 46.7%, with the lowest rates for insulin pump (36.5%), nutrition (37.4%), and insulin and glucagon (37.9%). 38 As such, the literature on the lack of confidence and knowledge about T1D among SHTs supports our participants’ perceptions and concern about SHTs’ competencies for T1D. At a point in time when continuous glucose monitoring and artificial pancreas systems are universal, the SHT’s competence with using these devices is required. 39 Conducting educational programs for faculty and staff could enhance their knowledge and self-efficacy. 40 Mothers suggested enhancing the peer awareness of T1D in school. Some SHTs are working to raise peer awareness of T1D, but school support is needed to prevent the stigma of children with T1D. Parents believed that the SHT could serve as an advocate for ordinary school life. SHTs should compromise with parents to maintain a balance in SHC responsibilities, which include monitoring, assisting, educating about the child’s self-care, and providing psychological support.
This study has several limitations. First, the research was introduced to a self-help group, and active members of an online self-help group became the study participants which may result in nonrepresentative views. In addition, in this research, the primary caregivers for children with T1D were their mothers, thus limiting the generalizability of this study’s results.
Conclusions
Although the participants of this study identified barriers and enhancements similar to those found in prior studies, they were struggling to maintain their child’s safe school life and recognized the importance of balancing responsibilities. To improve partnerships with parents in SHC for children with T1D, institutional improvements, such as enacting robust laws for SHC, establishing clear guidelines, and increasing the number of SHTs, should be prioritized. It is necessary to share the improvements perceived by the parents in this study through self-help groups and to continue the SHTs’ education process. This strategy would enhance SHTs’ understanding of their cooperation with parents. This is especially needed to help explore their expertise in terms of children’s health care and balance the responsibilities until improved SHC-related legislation and guidelines are established. In addition, SHTs need to communicate that they are willing to do their best to collaborate with parents. This study’s findings regarding mothers’ perceptions can facilitate conceptual analysis, tool development, and future intervention development in SHC for children with T1D.
Supplemental Material
sj-docx-1-wjn-10.1177_01939459231193725 – Supplemental material for School Health Teachers as Partners in Diabetes Caring: Maternal Perspectives
Supplemental material, sj-docx-1-wjn-10.1177_01939459231193725 for School Health Teachers as Partners in Diabetes Caring: Maternal Perspectives by Ju-Yeon Uhm and Mi-Young Choi in Western Journal of Nursing Research
Footnotes
Acknowledgements
The authors express deepest gratitude to the 22 mothers of SugarTree who sincerely participated in the interview.
Author Contributions
Study design: J-YU and M-YC. Data collection: J-YU. Data analysis: J-YU and M-YC. Manuscript writing and revisions: J-YU and M-YC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) funded by the Korea government Ministry of Science and ICT (MSIT) (NRF-2018R1C1B5086063).
Ethical Approval
The study design was approved by the Research Ethics Review Committee of Daegu Haany University (DHUMC-D-19002-PRO-0l).
Informed Consent
All study participants provided informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.