
Abstract
Background:
Working for extended hours in a physically and mentally demanding profession has subjected nurses to occupational fatigue. Limited evidence exists about nurse fatigue and alertness changes throughout shift work and their relationship with medication errors and near misses.
Purpose:
The purposes of this study were to: (1) assess the relationship between nurses’ fatigue and alertness, (2) evaluate nurses’ fatigue and alertness changes throughout their shift, and (3) examine the relationship between nurses’ fatigue, alertness, and medication errors and near misses.
Methods:
This prospective study is part of a larger mixed-method study. Fatigue and alertness data from 14 work and non-workdays were collected from a convenience sample of 90 nurses. A wearable actigraph (ReadibandTM) was used to measure alertness, while ecological momentary assessment (EMA) using text messaging was used to measure nurses’ fatigue.
Results:
A 1-unit increase in fatigue was associated with a 1.06-unit reduction in nurses’ alertness score (β = –1.06, 95% CI: [–1.33, –0.78], p < .01). Night-shift nurses experienced a 31-point reduction in alertness from the start to the end of the work shift. Nurses’ fatigue, but not alertness, was associated with medication errors and near misses (OR = 1.26, 95% CI [1.07, 1.48], p = .01).
Conclusion:
Initiating fatigue mitigation measures during mid-shift, especially for night-shift nurses, may be a viable option to mitigate fatigue and alertness deterioration among nurses and to maintain patient safety. The multifaceted nature of fatigue, as captured by EMA, is a stronger predictor of medication errors and near misses than device-measured alertness.
Keywords
“Do no harm” is one of the main ethical principles guiding the clinical practice for nurses and all health care professionals. However, medical errors are ranked as the third leading cause of death in the United States, and medication errors are among the most frequently occurring errors.1,2 These findings suggest many healthcare professionals, including nurses, are failing to maintain the “do no harm” promise to their profession and patients. Nurses function at the point of care and assume a major role in intercepting errors before reaching their patients. 3 To perform this role effectively, nurses must be well-rested and alert. However, being rested and alert is challenging due to the nursing shortage, which has greatly increased since the novel coronavirus disease 2019 (COVID-19) pandemic. 4 As of 2022, the nursing vacancy rate stood at 17%, representing a 7.1-point increase from the previous year. 4 To maintain 24/7 nursing care, most hospitals will continue relying on extended work hours, 12-hour shifts, rotating shifts, and even mandatory overtime in the near future. It is anticipated that these ongoing extended work requirements will have a negative impact on nurses’ fatigue and alertness, and may potentially affect patient safety outcomes, such as medication errors and near misses. However, few studies have evaluated these relationships.
Fatigue and Alertness Among Nurses
The terms fatigue and sleepiness are sometimes used interchangeably. Although the 2 are related and could co-occur, they represent different constructs. 5 Occupational fatigue is defined as a general sense of tiredness and exhaustion that is intensified by excessive work demands and inadequate recovery.5,6 Fatigue can be classified based on its nature as physical, mental, or global, and based on its duration into acute or chronic.5-9 In this study, we used self-rated global fatigue, defined as a general feeling of diminished energy to perform the required tasks resulting from prolonged physical and mental fatigue. 8 As we move forward, we will use the term fatigue to refer to occupational fatigue. Sleepiness, on the other hand, is defined as the tendency to fall asleep. 5 Regardless of the conceptual difference, poor sleep quality is among the most common causes of nurse fatigue, decreased alertness, and sleepiness.5,10-16 The relationship between sleep and fatigue is supported by multiple studies, including our previous work.10-16 However, there are limited studies conducted to evaluate the relationship between fatigue and alertness.
Nurse fatigue has been examined in many studies. Working in a mentally and physically demanding profession and complex work environment has subjected nurses to extreme fatigue.17-20 Multiple studies have evaluated predictors of nurse fatigue and its relationship with various nurse and patient outcomes. These studies have consistently linked nurse fatigue to a range of negative outcomes, such as drowsy driving,21-23 decision regret, 13 medication errors, 5 turnover intentions, 24 needlestick injuries, 25 sickness absences,26,27 and nurses’ mental health. 28
Although scholars have proposed that fatigue may diminish nurses’ alertness,8,10,14-16 empirical evidence exploring this relationship remains limited. One notable study by Min and colleagues 16 used wearable wrist actigraphy (Readiband) to measure alertness, and ecological momentary assessment (EMA) to measure fatigue at the beginning and end of shift work. The study findings revealed a significant correlation between fatigue at the beginning of the day shift and the subsequent decline in alertness. 16 This study, however, was conducted in Korea where nurses commonly work rotating 8-hour shifts, and did not capture fatigue variation throughout the shift.
Despite the breadth of research on nurse fatigue, a comprehensive understanding of how fatigue and alertness fluctuate during nurses’ shifts is still lacking. Furthermore, few studies have evaluated the relationship between fatigue and medication errors, 5 and the relationship between fatigue, alertness, medication errors, and near misses has not been thoroughly explored. This gap in the literature highlights the need for more studies to understand these relationships.
Purpose
A recent systematic review examining the relationship between nurse fatigue and patient outcomes identified a limited number of longitudinal studies that evaluated patterns of nurse fatigue and its consequences. 19 Thus, more longitudinal or prospective studies are needed to identify patterns of nurse fatigue and alertness throughout the shift to add knowledge about fatigue. Improved understanding in this area could provide some insights about the appropriate time to deliver fatigue mitigation interventions (eg, taking a break). Therefore, the purposes of this study were to: (1) assess the relationship between nurses’ fatigue and alertness, (2) evaluate changes in nurses’ fatigue and alertness throughout their shift work, and (3) examine the relationship between nurses’ fatigue, alertness, and medication errors and near misses.
Methods
Design, Setting, and Sample
This prospective observational study was part of a larger mixed-method study. The parent study aimed to evaluate predictors of nurse fatigue and examine if inter-shift recovery moderates the relationship between nurses’ fatigue and patient safety outcomes (medication errors and near misses). Data for the parent study were collected from 8 conveniently selected sites in the Midwest. All sites were located within a 120-mile radius of the principal investigators’ (PI) academic institution. The parent study included 3 consecutive phases; this article reports on one arm of the study’s second phase.
The sample for the selected arm consisted of 111 nurses working in 7 randomly selected general, critical care, emergency department, and behavioral health units, all from one academic medical center that was part of the parent study. The units were strategically selected to reflect the various specialties within the study site. Because some participants were missing some text messaging or wearable data, the final sample consisted of 90 participants. Nurse managers, advanced practice nurses, agency nurses, and float pool nurses were excluded from the study. A full description of the parent study setting, and sample are described elsewhere. 12
Measures
Ecological momentary assessment using text messaging was used to measure nurses’ self-rated fatigue. Ecological mo-mentary assessment involves collecting data over multiple time points to capture behaviors, emotions, and experiences from participants while in their naturalistic environment, such as at home or work setting.29,30 This method of repeatedly collecting data in real-time minimizes participants’ recall bias and allows researchers to effectively discern how context influences the behavior under study.29,30 Ecological momentary assessment has been used successfully to collect behavioral health data (eg, smoking, drinking, stress, physical activities, eating behaviors) from nurses, physicians, patients, and healthy individuals.31-36 The frequency, duration, and time interval between EMA data collection points are selected by the investigator, based on feasibility and potential subject burden.29,30
To avoid multiple interruptions to the nurses’ workflow, the PI decided to collect data 4 times every day over a 14-day period during work and non-workday days. The first text was sent 30 minutes before the beginning of the shift, the last text was sent 30 minutes after the end of the shift, and the middle 2 texts were sent at equal intervals during the shift. The leadership group of the participating units approved the proposed plan. The texting platform was designed and built for the study by collaborators at the College of Engineering. Before starting the data collection, the study PI and 4 research assistants enrolled as subjects in the texting platform and tested the system for a month. Each text prompted nurses to rate their fatigue using a 11-point Likert-type scale. The scale ranged from not fatigued at all (0) to extremely fatigued (10). In addition, participants received 2 texts at the end of their workdays to indicate if they had a medication error or near miss. Participants answered using a dichotomous scale of yes (1) or no (0) to indicate their answers.
A commercially available actigraphy wearable device, Fatigue Science ReadiBandTM (Fatigue Science, Vancouver, Canada; fatiguescience.com), was used to measure nurses’ alertness. The ReadiBandTM captures 5 sleep and awake parameters: (1) minutes in bed, (2) minutes asleep, (3) sleep latency, (4) sleep efficiency, and (5) awake after sleep onset. These parameters were processed by the Sleep, Activity, Fatigue, and Task Effectiveness (SAFTETM) biomathematical model to yield a predicted alertness score. The SAFTE© model and the ReadiBandTM have been validated in laboratory settings through controlled trials.37-39 The ReadiBand has an overall accuracy rate of 93% compared with another common method, polysomnography. 39 The predicted alertness scores range from 0 to 100, with high scores indicating good alertness. Alertness scores of 80 and above indicate a low risk of error.37-39 Alertness scores of 70% to 80% indicate an elevated risk of accidents/errors, with a decline in reaction time; and scores below 70% indicate a very high risk of accidents/errors with a significant decline in reaction time.37-39
Procedures
After obtaining the required University of Iowa Institutional Review Board’s (IRB# 201503758) approval, the study PI attended all the monthly staff meetings for all the participating units. Nurses were informed that their participation in the study was voluntary and that they could withdraw from the study at any point. The PI’s Institutional Review Board approved the request to waive the informed consent signature. After the study introduction meetings, the PI distributed the study packages to the nurses’ mailboxes. The packages contained the survey for the first phase of the study, a cover letter detailing elements of the informed consent, an invitation to participate in the second phase of the study, and a pre-stamped return envelope. To encourage participation and improve the response rate, weekly reminder flyers were distributed in the participating units over a 3-week period.
Nurses who completed the study survey and were interested in the second phase of the study completed the invitation form and included their phone number and a convenient time to call. One of the study research team members called all participants to obtain their 14-day schedule, entered the schedule into a texting platform, and then scheduled a time to deliver the ReadiBandTM. At the agreed-upon time, the research team member met with each study participant, delivered the ReadiBandTM, answered any questions, and asked about a good date and time to collect the ReadibandTM. Because the SAFTE© model requires 72-hour sleep data to calculate the alertness score, the participants were instructed to wear the ReadiBandTM on their non-dominant wrists starting 3 days before receiving the first fatigue text message. After 17 days of wearing the ReadibandTM (including 14 days of receiving the text messages and wearing the ReadibandTM), one of the research team members met with each participant to collect the ReadibandTM. After completing the data collection, each participant received a $90 compensation check and a $10 bonus if they responded to at least 75% of the fatigue text messages. We achieved an approximately 95% text messaging completion rate using the described compensation approach.
Statistical Analysis
R Studio Version 4.2.2 software (R Core Team) 40 was used to analyze the study data. To assess the relationship between nurses’ fatigue and alertness (aim 1), a repeated measures correlation was used to analyze the relationship between self-reported fatigue (0-10) assessed by EMA and alertness reported by the ReadibandTM. The ReadibandTM reports an alertness score every minute. To compare the 4 measures of self-reported fatigue with alertness, the minute-by-minute data at the time of self-reported and rolling alertness averages from the previous 5 minutes, 1 hour, and 4 hours were also compared with the participants’ self-reported fatigue at those time points. A mixed linear model was used to quantify the relationship between alertness and fatigue scores with a random intercept and slope to account for the repeated measures. Since the rolling averages were highly correlated with the minute-by-minute alertness score, only the minute-by-minute alertness score (ie, the alertness score at the time the self-reported fatigue score was collected) was used in the mixed linear model.
To evaluate changes in nurses’ fatigue and alertness throughout their shift work (aim 2), a mixed-model controlling for repeated measures was used to compare changes in the alertness scores and self-reported fatigue throughout each shift. Sex, age, marital status, education, and having a child at home were controlled for as covariates. The type of shift (day or night) was included in the model. An interaction term was included to examine how changes throughout a shift might vary between day and night shifts. Shifts starting at 7 pm, 11 pm, 5 pm, 3 pm, and 2 pm were coded as night shifts. Our analyses were conducted using 1207 and 840 observations from day and night shifts, respectively.
To examine the relationship between nurses’ fatigue, alertness, and medication errors, and near misses (aim 3), 2 univariable mixed logistic models were used to determine the relationship between having a medication error or near miss and alertness or fatigue. Medication errors and near misses were coded as a dichotomous outcome (Yes/No), and the minute-by-minute alertness scores (model 1) or fatigue scores (model 2) were the independent predictors. The odds ratio and confidence intervals were calculated from the resulting model.
Results
Sample Description
Of the 90 participants, the majority were female (90%) with a mean age of 30.6 (SD: 10.0) years old. On average, the participants had 6.2 years of nursing experience (SD: 7.7) and 3.8 years of experience in their unit (SD: 5.4). In terms of education, 78% of the nurses had a bachelor’s degree, followed by a master’s degree (10%), and an associate degree (11%). Regarding the type of unit, the largest percentage of participants worked in critical care (41%), followed by pediatrics (35%), with the smallest percentage of participants (3%) working in medical-surgical units. Slightly more than half of the participants (54.9%) started their shift at 7 am, followed by 34.3% who started at 7 pm. Most nurses (83.3%) worked a 12-hour shift, with a smaller proportion of nurses (12.3%) working an 8-hour shift (Table 1).
Nurses’ Demographics and Shift Characteristics (N = 90).
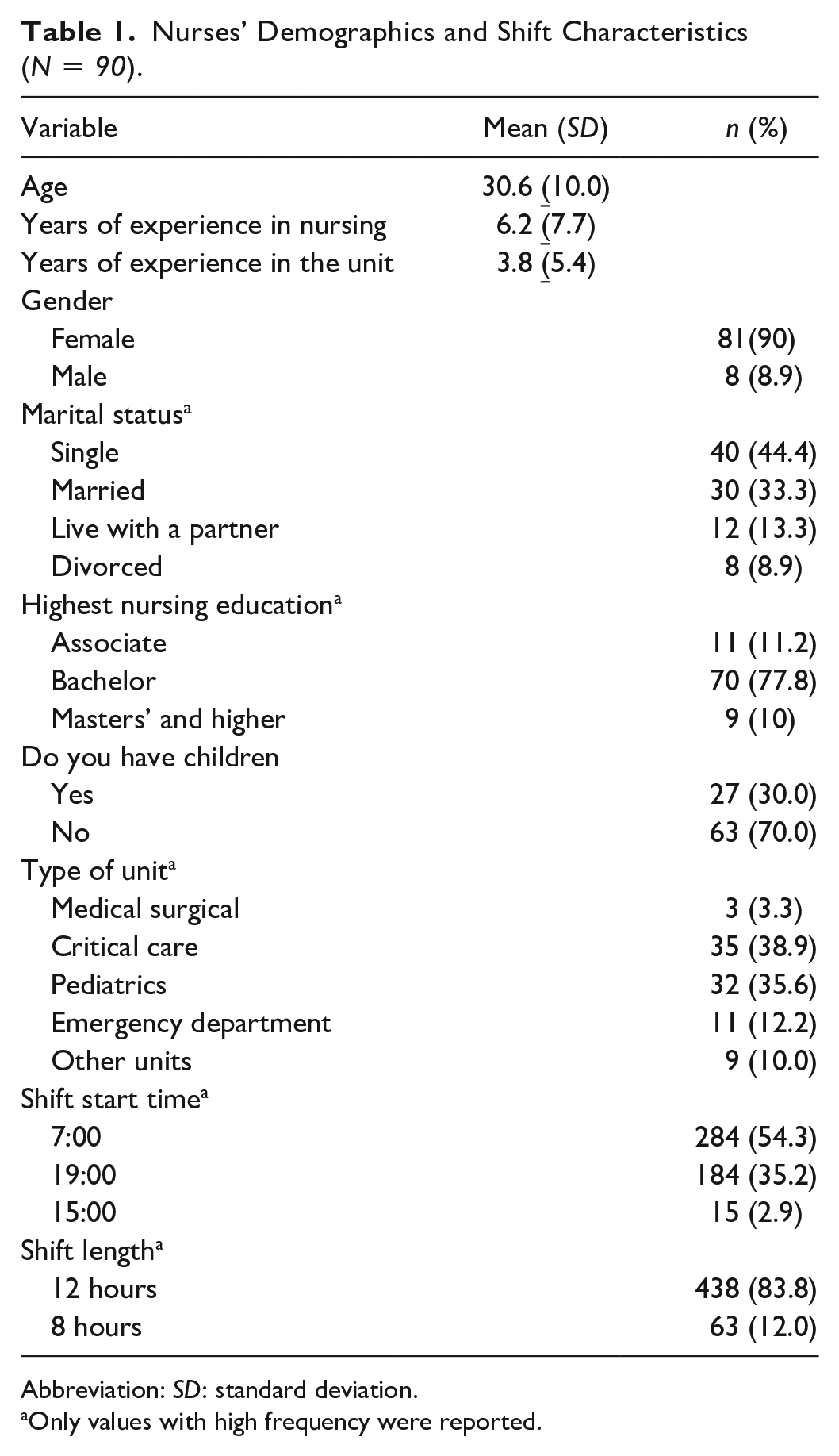
Abbreviation: SD: standard deviation.
Only values with high frequency were reported.
Relationship Between Nurses’ Self-Rated Fatigue and Objective Alertness Scores
To examine the relationship between EMA self-reported fatigue and the alertness score, we matched 4295 observations (including work and non-workdays) of concurrent EMA self-reported fatigue and ReadibandTM alertness scores among the 90 individual nurses. The EMA self-reported fatigue score was inversely associated with the corresponding minute alertness score (rrm = –0.28, 95% CI: [–0.31, –0.25], p < .001). A significant relationship was also observed between fatigue and alertness in the mixed linear model (β = –1.06, 95% CI: [–1.33, –0.78], p < .001), such that, a 1-unit increase in fatigue was associated with a 1.06-unit reduction in nurses’ alertness score.
Change in Nurses’ Alertness Throughout the Shift Work
We collected 2047 observations from 90 participants who worked day or night shifts. For alertness, a significant interaction effect across the work shift was observed among night-shift nurses (β = –7.86, 95% CI: [–8.45, –7.22], p < .001) but not among day-shift nurses (β = –0.12, 95% CI: [–0.32, 0.55], p = .55). The beginning of shift alertness scores were 16 points higher among night-shift nurses compared with day-shift nurses (β = 16.31, 95% CI: [14.5, 17.9], p < .001). Night-shift nurses experienced a 31-point reduction in alertness scores from the start to the end of the work shift, which was not observed among day-shift nurses (Figure 1).
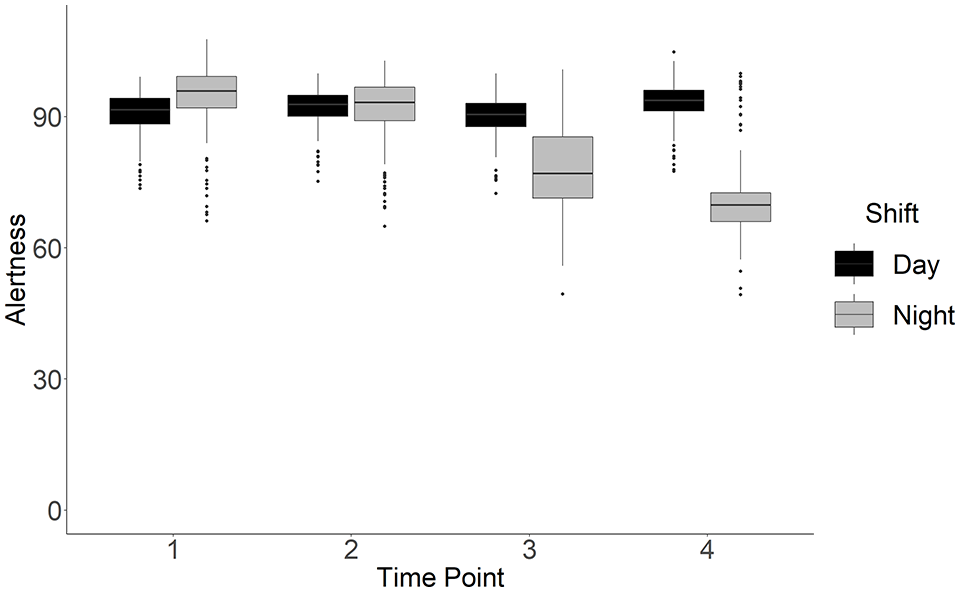
Nurses’ alertness scores (measured by the Readiband) during the day and night shifts.
Change in Nurses’ Fatigue Throughout the Shift Work
We observed a significant main effect for time (β = 0.37, 95% CI [0.23, 0.50], p < .001) and an interaction between shift and time (β = 0.37, 95% CI [0.19, 0.55], p < .001). Specifically, fatigue scores increased +1.48 points over the course of a given shift among day-shift nurses and +2.96 points among night-shift nurses. Compared with day-shift nurses, night-shift nurses reported lower fatigue scores at the beginning of their shift (β = –0.56, 95% CI [–1.06, –0.08], p = .009), but the greater increase in fatigue during the night shift mitigated this difference by the second time point (Figure 2).
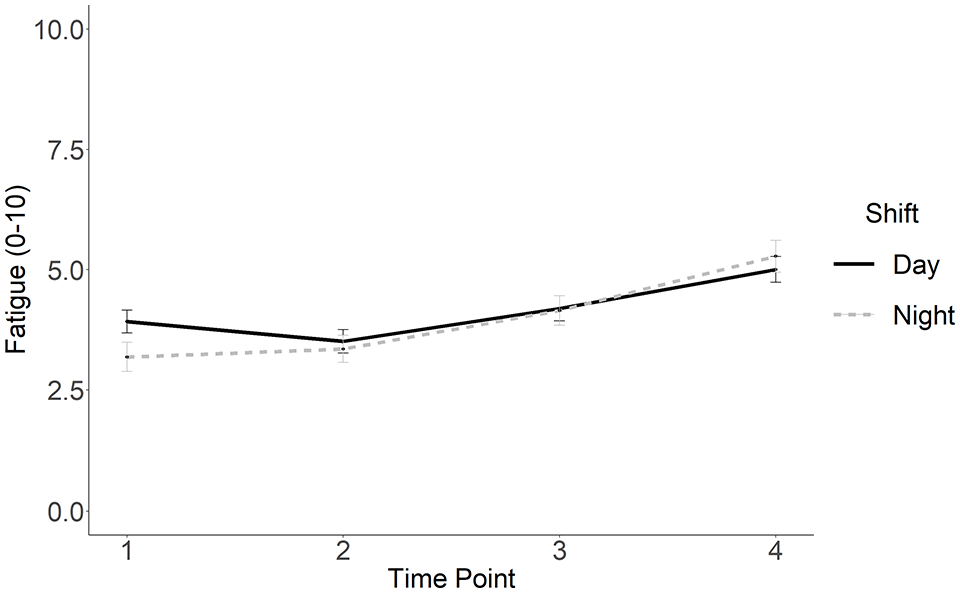
Nurses’ self-reported fatigue during the day and night shifts.
Nurses’ shift length (8, 10, or 12 hours) had no significant relationship with either fatigue or alertness. However, the timing of the shift (AM vs PM) was found to be associated with both alertness and fatigue, but this result should be interpreted with caution because we did not have an adequate representation of the different shift lengths.
Predicting Near Misses and Medical Errors
A total of 88 of 90 participants provided complete EMA data for medication errors and near misses. This included 455 shifts in which nurses reported having 17 near misses and 5 medication errors. Because of the small number of reported errors, we combined medication errors and near misses. In univariable mixed effect logistic models, the risk of near misses or medication errors was not associated with alertness (OR = 1.00, 95% CI [0.99, 1.00], p = .65) but was positively associated with self-reported fatigue (OR = 1.26, 95% CI [1.07, 1.48], p = .01). For every 1-unit increase in self-reported fatigue (eg, 2-3 of 10), there was a 25% increase in the odds of medication errors and near misses.
Discussion
This study aimed to assess the relationship between nurses’ fatigue and alertness, evaluate changes in fatigue and alertness throughout nurses’ shift work, and examine the relationship between nurses’ fatigue, alertness, and medication errors and near misses. To the best of our knowledge, this study is the first to evaluate the relationship between nurses’ fatigue and alertness and to measure fatigue and alertness concurrently. While most studies on nurse fatigue have proposed that fatigued nurses have compromised alertness as manifested by a slow reaction time, this relationship has not been adequately examined. The findings of our study support the proposed relationship between fatigue and alertness, such that increased fatigue among nurses was associated with a decline in alertness.
Our study also concurrently assessed fatigue and alertness multiple times throughout all shifts, which provides a rigorous estimation of the relationship between fatigue and alertness. Although we did not find a similar study to help interpret this result, this result may be supported by previous studies showing a relationship between nurses’ fatigue, especially after the night shift, car accidents and near accidents, injuries, and decision regret.13,41 We can presume that these negative outcomes could be attributed to the nurses’ diminished attention. A decline in nurses’ attention at the end of the shift has been supported in previous work.42-44
Although night-shift nurses started their shift with higher alertness and less fatigue than day-shift nurses, their alertness declined, and their fatigue increased significantly over the course of the shift. These changes in fatigue and alertness among night-shift nurses were not observed in day-shift nurses. This result could be because night-shift nurses managed to get a longer night’s sleep and some rest before starting their shift, unlike day-shift nurses who must wake up early to go to work. This interpretation is supported by the work of Ganesan and colleagues in 2019, who noted that compared with day-shift nurses, night-shift nurses had longer sleep hours, particularly before their first night shift. 41 However, as the night shift progressed, the nurses experienced increased fatigue and a deterioration in their alertness levels; this result was not evident among day-shift nurses. This result is aligned with previous work showing high mean fatigue scores among night-shift nurses,10,13,14 which could be attributed to being awake for a long time and working against their circadian rhythm. Furthermore, the night shift usually has fewer patient care activities, so that, nurses are more sedentary, which could decrease alertness. 42 In contrast, most active patient care activities and rounds occur during the day shift, 42 so that, nurses are more active and mentally engaged, which could increase their alertness. The decline in nurses’ alertness during the night shift has also been reported in other studies.41,43
Despite the significant inverse relationship between fa-tigue and alertness, nurse fatigue, but not alertness, was significantly associated with medication errors and near misses. This counterintuitive result could be attributed to the multifaceted nature of fatigue.5-10 Nurses’ alertness is a mental state, and the alertness score was calculated using sleep metrics. In contrast to the alertness score, when nurses self-reported their fatigue level, they responded to their perceived overall feeling, including their physical and mental fatigue. Thus, their fatigue score captured various aspects of fatigue. Thus, we could infer that medication errors and near misses are not only attributed to nurses’ alertness level but also to the nurses’ overall physical and mental state. From another perspective, fatigue was measured using a subjective self-report measure, so that, some nurses may have overestimated or underestimated their fatigue level. The absence of a relationship between nurses’ alertness and errors was noted in an earlier work where there was no association between nurses’ level of vigilance and increased risk of errors. 44
Overall, these findings may suggest that self-reported measures of fatigue may be more valid measures to evaluate the relationship between fatigue and medication errors than wearable objective measures. While future research is needed to confirm this finding, our findings suggest using EMA to measure nurses’ self-reported fatigue at work appears to be a feasible, acceptable, and useful strategy to inform interventions designed to prevent fatigue-induced medication errors. Because fatigue is measured in real-time, it has the added advantage of avoiding recall bias that could be associated with the frequently used fatigue measures. Future studies testing optimal fatigue prevention intervention among nurses are needed.
Strengths and Limitations
There are a few limitations to report. This study was conducted in one Midwestern hospital with a small sample size, so that, we cannot generalize the study results. It is possible that medication errors and near misses were underreported, which is consistent with prior studies and our previous work. 45 The underreporting of medication errors and near misses limits our ability to confirm the relationship between medication errors and fatigue. Fatigue was measured using a self-report measure. However, using EMA to measure fatigue over time could account for possible recall bias; and many fatigue studies have used daily logs and self-report measures to evaluate nurses’ fatigue. Despite these limitations, this study is one of few studies to (1) use an objective measure to capture nurse alertness, (2) use EMA to evaluate nurse fatigue at multiple points throughout the shift, and (3) evaluate the relationship between fatigue and alertness. Another strength is that we collected medication error data at the end of the shift rather than asking nurses to recall if they had an error during the previous day or week. This approach accounts for possible recall bias. Although the final sample consisted of 90 participants, this number is slightly larger than previous studies that have evaluated nurse alertness using wearable devices.
Conclusion and Implications for Future Research
Nurse fatigue has long been considered an important issue. However, with the ongoing nursing shortage, this issue is prevalent and is likely to continue in the near and possibly long-term future. Consistent with earlier work linking nurse fatigue to negative patient outcomes, the results of this study supported the relationship between nurse fatigue and medication errors and near misses. New to the literature is the empirical evidence supporting the significant relationship between nurse fatigue and the decline in nurses’ alertness. However, the counterintuitive relationship between nurses’ alertness and medication errors and near misses requires further investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the National Council State Board of Nursing (R91013) and the Healthier Workforce Center of the Midwest (HWCM). HWCM is supported by cooperative agreement no. U19OH008868 from the Centers for Disease Control and Prevention (CDC)/National Institute for Occupational Safety and Health (NIOSH).