
Abstract
Background:
Professional standards and the Codes of Ethics from the International Council of Nurses and American Nurses Association are frameworks driving professional practice and are linked to positive patient and nursing outcomes.
Objective:
To describe qualitative themes extracted from narrative responses on how nurses’ personal values influence nursing care and converge with quantitative results assessing personal values, professional values, and the practice environment, a key component of nurse satisfaction and subsequent care quality.
Methods:
A convenience sample of nurses across 19 sites within a large nonprofit healthcare system was surveyed. Quantitative measures included the Short Schwartz’s Value Survey for personal values, the Nurses Professional Values Scale-3 for professional values, and the Practice Environment Scale of the Nursing Work Index, assessing practice settings. Concurrently, nurses were asked, “How do your values influence the care you provide?” Responses were examined using a descriptive qualitative method for thematic analysis.
Results:
The sample included qualitative (n = 408) and quantitative (n = 671) responses. Six qualitative themes emerged: patient-centered care, professionalism/integrity of practice, advocacy, dissonance, golden rule/ethics of reciprocity (religiosity), and perseverance. Themes converged with the mean personal values of achievement, self-direction, universalism, benevolence, tradition, and conformity, and diverged with hedonism, security, and stimulation. All professional values factor means and work environment subscale means converged.
Conclusions:
Findings highlight convergence and divergence between qualitative and quantitative responses from nurses, offering new insights into the themes of dissonance, perseverance, and religiosity. The findings present valuable opportunities to enhance recruitment and retention strategies.
Prior to the COVID-19 pandemic, the global nursing workforce faced a shortage of 5.9 million nurses. 1 This shortfall was exacerbated by COVID-19 with many nurses leaving the profession altogether, primarily attributed to personal and system responses, stress, burnout, and higher workloads.1,2 Additionally, evidence suggests that up to 1 million more registered nurses plan to leave the profession or retire, pushing the shortfall to 7 million. 1 By 2030, it is estimated that worldwide shortages will be widespread, with an anticipated gap of 13 million nurses. 1 The escalating workforce crisis highlights an urgent need to examine how nurses’ morals and ethics are impacted by the practice environment, increasing workload, stress, and burnout.
The International Council of Nurses has a Code of Ethics guiding ethical values, responsibilities, and professional standards for nurses. 3 This global framework informs the American Nurses’ Association (ANA) Code of Ethics and Interpretive Statements, serving as a guide for nursing practice in the United States.4,5 Despite the importance of the Code of Ethics as a guide for practice, research on the ethical aspects of nursing care and how personal and professional values are potentially compromised in current healthcare environments remains limited.6,7 What is known is that ethical dilemmas arise from relatively common practice occurrences including end-of-life decision making, conflicts with the care team or family, and organizational constraints contributing to moral distress and burnout.8,9 In one systematic review, 10 burnout was associated with negative outcomes including poor patient safety and quality of care, satisfaction, and reduced organizational commitment.
Background
For nurses, personal and professional values as well as the practice environment are evolving with advancements in healthcare, technology, and societal expectations. The identity of a nurse is a blend of individual, professional, and contemporary values influencing nursing practice. 11 A nurse’s personal values directly impact care by shaping the environment through decisions and subsequent actions; however, values, while more universal in nature, can differ in priority and importance among individuals and groups. According to Schwartz’s Theory of Basic Human Values, 12 personal values may be influenced by sociocultural background, education, and organizational factors. 13 Despite being somewhat unique to each individual, personal values play a critical role in shaping the nursing profession and ultimately quality of care provided.
In parallel, strong professional values increase practice fulfillment and retention. 11 Nurses contributing to the profession maintain a sense of belonging and are more likely to remain in practice. 14 Similarly, nurses’ social values and professional quality of life are linked to retention and organizational tenure. 15 The association of a strong professional identity supported by values and ethical standards also plays a role in nurses’ choice to remain in the profession.14,16 Professional identity impacts quality and safety in patient care, 17 while nursing practice, work environment, and patient satisfaction are all influenced by professional values. 18 Values are essential for retention, practice, and quality of care—as the profession is defined not only by its actions but also by the manner in which those actions are performed. 19 The Professional Values Model connects personal and professional values with nursing care quality, enhancing nurse self-awareness as well as job and patient satisfaction through holistic, person-centered care. 20 Values, beliefs, and ethics are commonly recognized as key defining characteristics of health professions. 19 In nursing, professional identity also encompasses knowledge, values, ethics, and personal and group identity. 19
Nursing quality is influenced by the care nurses provide directly to patients, as well as the conditions of the work environment. According to the ANA, quality care is the degree to which nursing services increase positive outcomes and are consistent with current knowledge and evidence. 21 The environment is influenced by multiple factors impacting a nurse’s ability to practice and deliver high quality care.22,23 Worldwide, the practice environment is recognized as a strong contributor to organizational, nurse, and patient outcomes, 24 highlighting the relationship between environment and quality of care. A healthy work environment is also strongly associated with nursing satisfaction and subsequent retention. 23 As such, it is becoming increasingly imperative to further examine personal and professional values alongside nursing care quality in an effort to recruit and maintain an engaged professional nursing workforce.
The interconnectedness of personal and professional values and nursing care quality is supported by the study’s theoretical model, the Professional Values Model. 20 Within the model, 3 basic concepts influence each other: individual values, professional values, and nursing care quality including nurse and patient satisfaction. Because work environments are strongly linked to nurse satisfaction, the practice setting plays a crucial role in care quality. The model is useful across different care environments and is intended to evaluate both patient and nurse experiences of care. 20 However, as workforce dynamics shift, model components can change over time.
Purpose
The purpose of this secondary analysis was to explore the alignment between nurses’ qualitative feedback regarding the impact of their values on care provided, with quantitative survey results concerning personal and professional values and the practice environment, a key component of nurse satisfaction and subsequent care quality. The research aims include: (1) describing qualitative themes emerging from responses to the question, “how do your values influence the care you provide?” and (2) examining possible convergence or divergence with (a) personal values of power, achievement, hedonism, stimulation, self-direction, universalism, benevolence, tradition, conformity, and security; (b) professional values of caring, activism, and professionalism; and (c) practice environment, a component of nurse satisfaction and care quality (nursing participation in hospital affairs; foundations for quality of care; manager ability, leadership, and support of nurses; staffing resource adequacy; and collegial nurse-physician relations).
Methods
Design
This secondary analysis utilized a convergent mixed-methods design. Qualitative and quantitative data were simultaneously collected via survey with narrative responses, analyzed separately, and subsequently merged. 25 Quantitative survey data assessed nurses’ personal values, professional values, and nursing care quality, with an open-ended question for qualitative analysis. The narrative free text response to the question, “how do your values influence the care you provide?” was examined using a basic, descriptive qualitative methodological approach. 26
Study Setting and Sampling
Data for this secondary analysis were drawn from responses to a survey examining values and nursing care quality. In the parent study, a convenience sample was obtained from registered nurses (RNs) engaged in direct patient care across 19 Midwest regional sites of a healthcare system. Responses were drawn from hospitals and ambulatory care centers designated as Magnet (n = 9), on the journey to Magnet (n = 7), or those not actively pursuing Magnet designation (n = 3).
Inclusion and exclusion criteria
For this secondary analysis, all qualitative responses were included whether all quantitative questions were answered or left blank. For the parent study, screening for inclusion/exclusion was done with branching questions via Microsoft Forms. Inclusion criteria were RNs engaged in direct patient care (hands-on, face-to-face contact with patients for the purpose of care delivery at least 50% of full-time equivalent employment). Exclusion criteria were agency and travel nurses, advance practice providers, nurse leaders, nursing students, certified nursing assistants or other unlicensed assistive personnel, and RNs not engaged in direct patient care (50% of full-time equivalent or more).
Instruments
Personal values
In the parent study, the Short Schwartz’s Value Survey (SSVS), freely available in the public domain, was administered to examine personal values. The SSVS is a 10-item, self-reported tool using a Likert scale (0-opposed to my principles to 8-of supreme importance), measuring values of power, achievement, hedonism, stimulation, self-direction, universalism, benevolence, tradition, conformity, and security. The SSVS has demonstrated good validity and reliability (Cronbach’s alpha: 0.71-0.78). 27 For this analysis, mean scores for each value were compared with qualitative themes. Self-ratings below 4 (4 = important) indicated that the value was not important to nurses, while ratings of 4 or higher signified importance. In this study, the SSVS had good internal consistency (Cronbach’s alpha: 0.77).
Professional values
The professional values of nurses were measured with the Nurses Professional Values Scale-3© (NPVS-3). 28 Permission was obtained to use this 28-item scale with self-report Likert responses from 1 (not important) to 5 (most important). A total score is calculated by summing numeric responses (ranging from 28 to 140) with higher sums indicating a stronger orientation to professional values. The NPVS-3© does not have subscales, but does contain 3 factors: caring, activism, and professionalism. 28 Caring (10 items) focuses on commitment to patient as an individual, family, group, community, or population. Activism (10 items) includes components of the profession impacting health policy, promoting health diplomacy, and maintaining integrity. Finally, professionalism (8 items) captures responsibility for work environment, personal and professional growth/authority, and responsibility for practice. The NPVS-3© scale validity and reliability has been established (Cronbach’s alpha: 0.94). 28 Mean scores of the 3 factors (caring, activism, professionalism) were compared with themes. For mean scores <3 (neutral response), the professional value was interpreted as not important to nurses with values ≥3 as important. In this study, the instrument’s Cronbach’s alpha indicated excellent internal consistency (0.95).
Nursing care quality
The practice environment, a key component of nurse satisfaction and subsequent care quality, was measured with the Practice Environment Scale of the Nursing Work Index (PESNWI).22,29 This tool evaluates factors in the work setting that impact job satisfaction, stress levels, and patient outcomes, providing an overall measure of nursing care quality. This scale is the most commonly used instrument to measure nursing practice environment and has been validated for use across the United States and worldwide. 23 Nurses were asked to indicate the extent to which each item is present in their current job (1: strongly disagree to 4: strongly agree). This 31-item instrument, developed for direct care nurses, has 5 subscales (participation in hospital affairs; quality of care; manager ability, leadership, and support; staffing and resource adequacy; and collegial nurse-physician relationships).22,29 Reliability coefficients (measure and subscales) ranged from 0.77 to 0.82 and 0.82 to 0.96, respectively. 23 Subscale scores were used for comparison with qualitative themes, with mean scores ≤2.5 interpreted as disagree and >2.5 as agree. In this study, Cronbach’s alpha was 0.94.
Qualitative data
A basic qualitative descriptive methodological approach was used to analyze responses to the free text question, “When thinking about your specific work setting, how do your values influence the care you provide?” This approach is the method of choice when seeking to describe a phenomenon, focusing on questions of who, what, and where, of events or experiences. 26 Following Sandelowski’s framework, analysis aimed to capture a descriptive summary of the data. In this case, the phenomenon of interest is nurses’ described values and the influence on care.
Data Collection and Analysis
This secondary analysis utilized data from the parent study (October 17, 2022-November 30, 2022). In the original study, participants were recruited via email, flyers, and by site shared governance representatives. The anonymous survey was conducted via Microsoft Forms, reached through an electronic link and/or QR code with submission of responses indicating implied consent for participation. The quantitative and qualitative data were analyzed and interpreted separately and then combined during interpretation. This approach is consistent with convergent mixed-methods design. 25 Joint display of merged results occurred after initial analyses.
Quantitative
Descriptive statistics were used to explain participant characteristics, role, work settings, length of time as a nurse, and other demographics. For scales, measures of reliability were calculated (Cronbach alpha coefficient). Mean values of each of the 10 items in the SSVS values of power, achievement, hedonism, stimulation, self-direction, universalism, benevolence, tradition, conformity, and security were calculated. Similarly, mean scores of NPVS-3© factors and PESNWI subscales were compared to qualitative themes.
Qualitative
A basic qualitative descriptive approach was employed to analyze for codes in data from the open-ended question, “When thinking about your specific work setting, how do your values influence the care you provide?” 26 This question, deeply rooted in individual experiences and perceptions of values and the work environment, guided analytical exploration. Narrative responses were analyzed for key themes using qualitative content analysis, with responses initially coded and grouped into thematic categories. Each member of the research team was provided foundational training on this descriptive approach. The team collaboratively coded an initial set of 15 responses to establish a consistent framework. Then, all 6 members independently coded the remaining responses using qualitative content analysis. The principal investigator compared codes across members to identify broader thematic patterns. The team reconvened to ensure confirmability, discussing and refining 6 final themes through consensus. Once themes were established, the dataset was re-examined to identify supporting quotes. The team worked together to finalize themes, definitions, and quotes until full agreement was reached, with each member verifying the final results to ensure alignment with their individual analyses.
Rigor and validity
Multiple strategies were employed to ensure rigor of the qualitative analysis. Prior to beginning the analysis, the team engaged in discussions on setting aside personal bias and implemented bracketing techniques to reduce subjective influence. Four dimensions of rigor criteria (credibility, dependability, confirmability, and transferability) were systematically addressed. 30 Credibility was established through data triangulation, with 2 researchers independently interpreting and comparing results. Additionally, all research team members validated final themes, supporting quotes, and definitions. Dependability, which closely aligns with reliability, was addressed by having all 6 research team members review and analyze qualitative data independently. Confirmability of the analysis was met by each team member recording additional notes during independent analysis. Finally, transferability was enhanced with a large sample size across 19 sites, with varying sizes and patient populations served.
The parent study received non-human subjects research approval with no oversight needed from the Institutional Review Board (IRB) at a large non-profit healthcare system. For this secondary analysis, a non-human subjects’ determination was obtained. In the original study, nurses across the sites were invited to participate in the study via emails and flyers and were assured the study was voluntary, anonymous, and with no impact on employment. Filling out the survey was considered implied consent with a waiver approved by the IRB.
Results
Sample Characteristics
A sample of 671 nurses answered the quantitative portion of the survey and 408 responded to the qualitative free-response field. The majority of respondents were female (n = 616, 91.8%), with ages between 22 to 70 years with a mean age of 41.1 (SD = 11.9). Participants had between 0 to 46 years of nursing experience with a mean of 14.2 years (SD = 11.6) and a majority possessed a bachelor’s degree in nursing (n = 480, 71.5%). Full sample demographics are reported in Table 1.
Sample Demographic Characteristics (N = 671).

Abbreviations: ADN: associate degree in nursing; BSN: bachelor of science in nursing; DNP: doctor of nursing practice.
Quantitative Results
Personal values
Means and standard deviations for each of the 10 SSVS values were calculated. The values of achievement (M = 5.06, SD = 1.78), self-direction (M = 5.97, SD = 1.57), universalism (M = 5.50, SD = 1.91), benevolence (M = 6.93, SD = 1.31), tradition (M = 5.10, SD = 1.82), and conformity (M = 5.06, SD = 1.89) converged with qualitative themes (Table 2). The values of hedonism (M = 4.39, SD = 2.12), stimulation (M = 4.50, SD = 1.75), and security (M = 5.74, SD = 1.68) diverged, meaning that despite mean scores greater than 4, indicating importance, the values were not congruent with any of the qualitative themes. The value of power (M = 3.15, SD = 1.76) did not converge or diverge with themes.
Joint Display of Mixed-Methods Results.

Abbreviations: NPVS-3, Nurses Professional Values Scale-3; SSVS, Short Schwartz’s Value Survey.
Personal values of hedonism (M = 4.39 SD = 2.12), stimulation (M = 4.50, SD = 1.75), and security (M = 5.74, SD = 1.68) diverged.
Professional values
The total mean score for NPVS-3© was 108.56 (SD = 17.05), out of a range of 28 to 140. The factors and associated mean scores were caring (M = 4.47, SD = 0.47), activism (M = 3.77, SD = 0.74), and professionalism (M = 3.78, SD = 0.59). The mean scores for the factors of caring, activism, and professionalism all converged with qualitative themes (Table 2). There was no divergence in professional values, meaning that all mean score indications were in alignment with qualitative theme definitions.
Nursing care quality
The overall mean score on the PESNWI was 2.82 (SD = 0.46). The mean scores of the 5 subscales were nurse participation in hospital affairs (M = 2.76, SD = 0.52); foundations for quality of care (M = 2.88, SD = 0.42); manager ability, leadership, and support of nurses (M = 2.88, SD = 0.66); staffing and resource adequacy (M = 2.43, SD = 0.69); and collegial nurse-physician relationships (M = 3.06, SD = 0.57). All subscales’ mean scores converged with at least 1 theme, with the foundations for quality of care converging with 3 themes.
Qualitative Results
The qualitative free text responses from the survey question “how do your values influence the care you provide?” were analyzed with a descriptive approach and resulted in 6 themes: advocacy, dissonance, golden rule/ethos of reciprocity (religiosity), patient centered care, perseverance, professionalism/integrity of practice. Once identified, themes were conceptually defined from the literature and supported with participant quotes. Figure 1 visually depicts the 6 qualitative themes and how they influence nursing care, alongside personal, professional, and nursing care quality convergence.
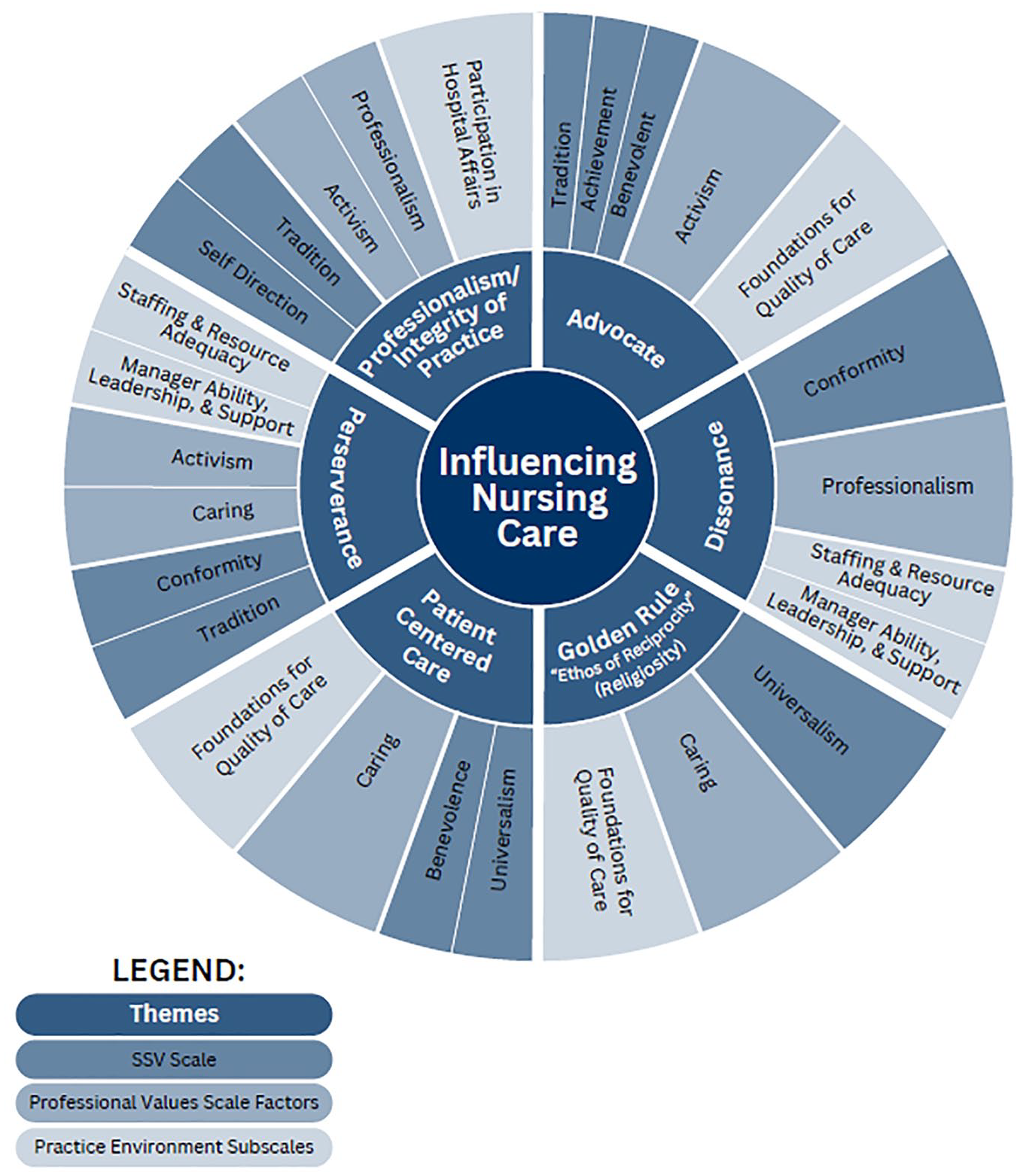
Factors influencing nursing care.
Theme 1: Advocacy
Participants answered that values aid in “advocacy for my patient” (150) and in some instances “advocating for their wishes for them” (365). Nursing advocacy is “promoting patient safety and quality care which includes the following: protecting patients, being patients’ voice, provision of quality care and interpersonal relationship as well as educating patients.”31(p.1124) The theme of advocacy extended beyond patient care to “having a good working relationship with peers and physicians” (96). In some cases, this was advocating on behalf of the patient in interprofessional communication or collaboratively advocating to “do the best thing for the patient” (96).
Theme 2: Dissonance
There was a disconnect between nurses’ perceptions of nursing care quality and clinical care. This dissonance highlights “nurses’ beliefs about how things should be, in contrast with the reality of how things are.”32(pp.3-4) Conflict was associated with safety, “due to violence and threats against staff” (287) from patients/family. Or during pandemic times, “due to staffing and bed availability it often feels we are falling short” (240). A commonality was not having adequate time “to truly connect with our patients” (228). The phrases strive and try to provide the best care emerged, alluding to participants intentions not aligning with perceived outcome, thus resulting in feelings of falling short despite best efforts.
Theme 3: Patient-centered care
Participants described the need to “respect my patients fully” (338) and acknowledged the “individual right to decide what is best for themselves” (16). This aligns with the Institute of Medicine’s 33 definition of patient-centered care, which includes qualities of compassion, empathy, respect and responsiveness to the needs, values, and expressed desires of each individual patient. Since this seminal work, the definition has expanded to “patient and family preferences, values, cultural traditions, and socioeconomic conditions are respected.” 34 This expansion was evident in participant responses with “care for patients and families from diverse ethnic and socioeconomic groups” (197). Additionally, respondents cited the need to separate their own personal values to allow for patient autonomy and “unbiased care” (95).
Theme 4: Golden rule/“ethos of reciprocity” (religiosity)
Participants frequently stated specifically the “golden rule” or “how I would want myself and my family treated?” (280). The phrase “like family” in the responses was repeated and utilized with application. The golden rule “guides people to choose for others what they would choose for themselves.” 35 This is a direct application of the ethos of reciprocity for care providers. Both have religious undertones and connect to Christianity and the Sermon on the Mount with the phrase “do unto others as you would have them do unto you.” Moreover, nurses linked the care they provide with their religiosity, most frequently citing Christianity.
Theme 5: Perseverance
Participants reported “the ability to continue on and move forward.” Courage is the essential component of perseverance, or “having the drive and fortitude to continue to move forward in a world of constant change requires self-awareness and the capacity to sustain a passion for the future.”36(p.49) References to the pandemic’s impact on healthcare staff and environment were present. Despite challenging times and situations, participants reported the ability to adjust and “prioritize my timeline at work” (185).
Theme 6: Professionalism/integrity of practice
Many respondents focused on upholding the “professionalism of nursing” (261). The literature defines nursing professionalism “as providing individuals care based on the principles of professionalism, caring, and altruism.”37(p.1) Interestingly, responses with professionalism frequently also stated “compassion.” Correspondingly, integrity of practice emerged alongside professionalism. Integrity is “to balance personal expectations, professional concerns and practice realities to retain a sense of intactness as both an individual and a professional.”38(p.743) Integrity responses focused on providing the “best possible care” (183).
Discussion
The results of this mixed-methods study highlight nurses’ quantitative responses on personal values, professional values, and the practice environment, a key component of nurse satisfaction and subsequent care quality converging with the themes of advocacy, dissonance, patient-centered care, golden rule/“ethos of reciprocity” (religiosity), perseverance, and professionalism/integrity of practice. Correspondingly, there was convergence across all professional values and nursing care quality. While there was divergence with the personal values of hedonism, security, and stimulation, suggesting that while nurses report these personal values as “important,” they do not necessarily influence the care they provide to patients. Interestingly, power did not appear in qualitative data and the mean score for power fell under “not important” to clinical nurses.
The Professional Values Model, the framework for this study, asserts the dynamic interplay between individual values, professional values of nurses, and nursing care quality, converging to influence nursing job satisfaction and patient outcomes, while serving as a foundation for addressing ethical dilemmas and decision making. 20 What is novel is the recognition that there are additional components potentially influencing nursing care including the role of practice dissonance, a desire to persevere regardless of circumstance, and religiosity. While religiosity may be indirectly linked to one’s individual values, the desire to persevere may exemplify a commitment to excellence, transcending personal or professional beliefs, suggesting that moral resilience is a critical, yet underappreciated dimension of care delivery. 39 Even under distress, nurses continue to try to provide optimal care.
The themes of advocacy and dissonance were demonstrated as participants expressed that they “tried,” or “strived,” alluding to a sense of feeling determined but describing that they fell short. This disconnect between the nurse, patient, and work/care environment suggests ongoing dissonance in the practice environment with potential impact on nursing care quality. Nurses verbalized the importance of providing patient-centered care, but also describe the clinical environment as a barrier. The challenges of maintaining satisfactory nurse/patient ratios, delivering high-quality care, while contending with a dwindling number of nurses and budget constraints present significant issues for nurses and leaders. 40 Providing care that does not “measure up” to how they or their family member should be treated results in nurse’s feeling cognitive dissonance. However, there is evidence suggesting that a supportive work environment that fosters caring while providing support to manage emotions improves self-efficacy and decreases emotional dissonance. 41 Moreover, creating and sustaining healthy work environments may produce positive outcomes for patients and nurses. 42 Healthy work environments are associated with lower negative nurse and patient outcomes, and higher patient satisfaction. 43 Thus, to potentially improve nursing care quality and avoid dissonance, it is essential that leaders and nurses set realistic expectations and employ evidence-based healthy work environment strategies.
The theme of dissonance may be heightened as a direct result of nurses’ reporting a desire to go beyond the requirements of duty, and “treat patient like family” no matter the cost. These supererogatory acts are beneficial but not expected as part of an individual or organization’s moral obligations. 44 In contrast, it could be argued that supererogatory acts cause harm or cost to the individual performing them. 45 Notably, the COVID pandemic may have increased visibility and the desire to perform supererogatory acts for healthcare workers, especially nurses. While providing patient-centered care is important and emerged as a theme, it is essential to maintain balance to avoid unrealistic expectations. Yet in today’s healthcare environment, with an increased focus on nurse wellness and patient satisfaction, these actions and expectations may indirectly harm nurses’ physical and/or mental well-being.
Interestingly, the theme of religiosity emerged, which may be associated with physical and mental health. Nurses frequently utilize religious or spiritual coping techniques to manage work stressors. 46 Some nurses may have been called to the profession out of an intrinsic motivation or desire, as a means of fulfilling one’s purpose in life, and/or the desire to help others 47 which may subtly reflect religious or spiritual beliefs. Many of the responses in this study focused specifically on Christianity; however, unbiased support of nurses’ spiritual or religious beliefs may play a role in supporting well-being and retention efforts. Furthermore, evidence supports that religion, and spirituality may aid in reducing burnout through improved well-being. 48 Most organizations already have spiritual support services in place for patients and families but have not expanded their services to staff. Healthcare leaders and organizations should consider targeted spiritual programming for nurses. Keeping this in mind, if nurses’ moral values are addressed in daily practice, they are more fulfilled and likely to remain in the profession and role. 11
This study highlighted nurses’ perseverance and professionalism/integrity of practice. The ability to persevere is dependent on many individual factors including adapting to change. Change fatigue is a well-known concept in business and intensified for healthcare professionals during the pandemic. The pandemic increased the need to constantly and rapidly incorporate changes in clinical practice as well as increasing workload. 49 Mitigation recommendations for change fatigue include building and measuring resilience in staff, optimizing change management practices, and optimizing political agency through nurses’ voice and influence. 49 Professionalism/integrity of practice is also promoted when professional (shared) governance infrastructure is present. Governance allows nurses to question practice changes while defining and demonstrating the impact of the profession. Empowering nurses can assist in avoidance of change fatigue, offering an environment that optimizes perseverance. 49 Perseverance is 1 of 3 foundational elements needed to maintain resilience for nurse leaders. 36 Similarly, clinical nurses need resilience strategies to continually adapt to the ever-changing healthcare environment and subsequent competing priorities.
Strengths of this study include that it was multisite across a Midwest region, with a large sample size for both quantitative and qualitative analysis. Additionally, the mixed-methods approach showed convergence and divergence, allowing for greater interpretation of the data. This study had several limitations. First, the majority of respondents were female, and although this is common in nursing research, values may differ between sexes, age groups, and religious/spiritual beliefs. The survey was voluntary, capturing responses from nurses who chose to participate. Quantitative measures were all self-reported, with the care environment being utilized as an indirect measure of nursing care quality, which is supported in literature, but is a recognized limitation. Finally, values that influence care are specific to clinical nurses only and do not extend to the numerous other roles nurses may have within healthcare settings.
This mixed-methods study evaluating personal values, professional values, and nursing care quality provides quantitative and qualitative insights into the nursing workforce. The 6 themes converged with professional values and nursing care quality subscales. There was also convergence with the personal values of benevolence, achievement, tradition, conformity, universalism, self-direction, and divergence with hedonism, stimulation, and security. This congruence highlights opportunities for healthcare systems and leaders to evaluate current workforce well-being, recruitment, and retention programs or strategies supporting the personal and professional values of nurses.
Future research addressing how dissonance, perseverance, and religiosity influence the nursing practice environment is warranted. The inclusion and prioritization of religious or spiritual support can aid in promoting personal and professional values in healthcare work environments. Results provide new insights into the use and application of the Professional Values Model. Healthcare organizations and nursing leaders need to explore the interconnected of these constructs and test value-based interventions to build a supported professional nursing workforce.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.