
Abstract
Background:
Psychosocial factors significantly influence lifestyle changes in adults with hypertension. However, research focusing specifically on these factors in young- and middle-aged adults—especially those newly diagnosed within the first 5 years—is limited.
Purpose:
This cross-sectional study aimed to examine the relationship between psychosocial factors guided by Social Cognitive Theory (perceived stress, self-efficacy, outcome expectancy, and functional and workplace support), physical activity, and blood pressure in young- and middle-aged Thai adults with hypertension.
Methods:
The analysis encompassed 400 adults with hypertension (Mage = 47.98 years; SD = 7.66), with nearly 60% being female from 25 primary care settings in a Thai province. Confirmatory factor analysis validated latent variables, followed by structural equation modeling with maximum likelihood and robust standard errors to analyze direct and indirect effects on physical activity and blood pressure.
Results:
Findings highlight self-efficacy in physical activity as a significant predictor of moderate-to-vigorous physical activity, while functional support correlated with reduced systolic blood pressure. Moderate-to-vigorous physical activity mediated the relationship between self-efficacy or functional support and systolic blood pressure. Hypertension duration (diagnosis ≤12 months vs >12 months) moderated the relationship between moderate-to-vigorous physical activity or functional support and diastolic blood pressure.
Conclusions:
Our research presents a new, theory-driven perspective on how psychosocial factors could affect blood pressure levels through physical activity among younger adults newly diagnosed with hypertension. Nurses can leverage this insight by providing education to enhance confidence and engage patients’ social networks in supporting their participation in physical activity, thereby improving blood pressure management.
Keywords
Hypertension is a significant global health issue, particularly impacting Asian countries. 1 Projections by the World Health Organization suggest that by 2050, over 40% of adults will have hypertension, leading to an annual death toll exceeding 10 million without effective interventions. 2 Notably, lower-middle-income countries, including Thailand, bear a disproportionately higher burden of hypertension. 3 The prevalence of hypertension has risen sharply, especially affecting young- and middle-aged Thai adults aged 18 to 55 years. 4
Timely lifestyle modifications are crucial for effective blood pressure (BP) control, particularly within the first 5 years of hypertension diagnosis. 5 Synthesizing evidence from a systematic review and meta-analysis of 43 studies underscores that regular physical activity, such as moderate-to-vigorous intensity, is more effective than other lifestyle modifications among adults with hypertension in middle-income countries for controlling BP and preventing mortality related to high BP. 6 Nevertheless, young- and middle-aged Thai adults with hypertension show a lower propensity for adopting this behavior than their older counterparts. 7
Social Cognitive Theory posits bidirectional associations between personal factors (beliefs and thoughts) and external factors (social environment) in driving behavioral change. 8 Self-efficacy, perceived stress, and outcome expectancy represent critical personal factors within Social Cognitive Theory, while social support assumes significance as an external environmental factor. 8 Among younger adults with hypertension in Western and Middle Eastern countries, these Social Cognitive Theory factors have emerged as substantial determinants of recommended lifestyle behaviors for BP management, such as physical activity. 9 However, the state of science on the impact of psychosocial constructs on physical activity behaviors and systolic/diastolic BP remains largely unclear, particularly for young- and middle-aged Thai adults who are newly diagnosed with hypertension. Young- and middle-aged adults, part of the Sandwich Generation, may struggle with increasing stressors; due to their young ages, they may be less likely to worry about the consequences of hypertension given competing societal/familial role demands. 10
Therefore, our study aimed to explore the relationships between Social Cognitive Theory-based constructs and physical activity, as well as their impact on systolic/diastolic BP, specifically focusing on individuals diagnosed with hypertension for 5 years. We also investigated the moderation effects of hypertension diagnosis duration on these relationships via group comparison modeling. An explicit understanding can inform the development of effective interventions that can improve BP management, ultimately enhancing overall well-being among young- and middle-aged adults with hypertension in Thailand.
Methods
Design
This study, conducted from April 17 to July 28, 2023, employed a cross-sectional design to examine the correlation between psychosocial factors, as guided by Social Cognitive Theory, physical activity, and BP among young- and middle-aged adults with hypertension residing in Thailand.
Study Setting and Sampling
A total of 400 participants aged between 18 and 55 years were recruited from 25 primary care settings in the Songphinong district, Suphanburi province, Thailand, which accounted for 64% of the total adults with hypertension in the Suphanburi province. 11 The sample size estimation was completed using the A-Priori Sample Size for Structural Equation Models program. The study’s parameter values were based on the following: (a) anticipated small effect size = 0.30, (b) desired statistical power level = 0.9, (c) number of latent variables (=7), (d) number of observed variables (=11), and (e) probability level of .01. A minimum sample size of 257 would achieve a desired statistical power of 90%. We oversampled by about 30% to account for the potential nonresponse rate, missing data, and significant covariates that need to be included in additional mediation or moderation analyses. Thus, our sample size of 400 was considered sufficient to examine the above-mentioned objectives.
Inclusion and Exclusion Criteria
The inclusion criteria were that an individual: (a) was diagnosed with primary hypertension within the past 5 years as documented in their medical record; (b) was between 18 and 55 years of age; (c) was able to read and communicate in the Thai language; (d) held a job of greater than or equal to 20 hours per week; and (e) was willing to have their BP measured at least twice in a same visit. We excluded individuals who: (a) had documented physical disabilities or cognitive/psychological impairments; (b) had a diagnosis of coronary heart diseases (ie, heart failure, ischemic heart disease); or (c) were pregnant.
Measures
Demographic characteristics
A demographic survey developed by the primary investigator in the Thai language was used to assess participants’ demographic characteristics. The survey consisted of 12 items: (1) age, (2) sex, (3) duration of hypertension (in months), (4) height (in centimeters), (5) weight (in kg), (6) personal monthly income, (7) educational level, (8) marital status, (9) smoking status, (10) alcohol drinking status, (11) occupation, and (12) working hours per week.
Physical activity
The International Physical Activity Questionnaire—Short Form (Thai version), which consisted of 7 items, was used to assess the amount of time spent each day performing vigorous-, moderate-, and low-intensity activity over the previous 7 days with good reliability (α = 0.96). 12 The calculation process involved computing total MET-minute (Metabolic equivalent) scores for each type of physical activity by applying the coding instructions, which entailed the multiplication of minutes, days, and MET levels (3.5 for low-intensity, 4 for moderate, 8 for vigorous). The summation of moderate and vigorous MET-minute scores constituted the metric for moderate-to-vigorous physical activity. A higher MET-minute score corresponded to a higher level of physical activity.
Blood pressure
Participants’ systolic and diastolic BP were independently obtained after 5 minutes of rest with the Omron HEM-907 electronic sphygmomanometer, which had been calibrated according to the manufacturer’s guidelines prior to data collection. Measurements were taken by registered nurses, who were trained and had their BP measurement technique verified for accuracy in accordance with the American Heart Association protocols. 13 More specifically, systolic/diastolic BP was measured at 2 distinctive times (2 minutes apart) to minimize random errors. If the difference between these 2 readings exceeded 5%, a third measurement would be taken, consistent with recommendations for minimizing measurement variability with the American Heart Association protocols. 13 Finally, the 2 closest readings were averaged to represent the systolic and diastolic BP.
Psychosocial factors
All Social Cognitive Theory-based psychosocial measures related to physical activity in the Thai version had demonstrated good reliability and validity (see Table 1). These measures were transculturally translated from the original English version into Thai as part of our previous study on psychometric properties (Suriyawong et al, unpublished data). Details of the original measures are provided below.
Detailed Information About Selected Psychosocial Measures in Thai Versions.

Abbreviations: α: Cronbach’s alpha; ω: McDonald’s omega coefficient; AVE: average variance extracted; CVI: content validity index; PA: physical activity; r: correlation coefficient.
Suriyawong et al, unpublished data.
The Self-Efficacy for Hypertension Treatment Adherence Scale, 14 consisting of 6 items, was adapted to assess the confidence levels of adults with hypertension in adhering to physical activity despite facing various barriers. Participants rated their confidence levels on a 7-point scale, ranging from 1 (not confident) to 7 (very confident). The total score for this subscale ranged from 6 to 42, with higher scores indicating greater self-efficacy in adhering to physical activity recommendations.
The Outcome Expectancies of Behavioral Change Scale, comprised of 2 domains, 15 was selected to evaluate the perceptions of younger adults with hypertension regarding the positive and negative consequences associated with physical activity adherence in this study. The scale consists of 8 items and utilizes a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The total possible score for outcome expectancy in physical activity ranges from 8 to 56, with a higher sum score indicating a greater level of perceived outcome expectancy. The 2 domains of outcome expectancy encompass positive and negative subscales, reflecting participants’ perceptions of the beneficial or adverse outcomes resulting from their engagement in physical activity. A higher score signifies a heightened perception of positive or negative outcome expectancy.
The Perceived Stress Scale is comprised of 2 domains, including (1) perceived distress and (2) coping ability. 16 The scale consists of 10 items rated on a 5-point Likert scale, ranging from 0 (never) to 4 (very often), assessing how frequently individuals have experienced specific thoughts or feelings in the past month. Individual scores range from 0 to 40 with higher scores indicating higher perceived stress. Prior research conducted among young adults demonstrated satisfactory reliability (α = 0.85) and concurrent validity (r = 0.60) of this scale. 16
The Social Support for Exercise Behavior Scale, a 5-item measure developed by Sallis et al, 17 was employed in this study to assess participants’ perceptions of functional support from family or peers in relation to physical activity adherence. Using a scale ranging from 1 (never) to 5 (very often), participants were asked to indicate the extent to which each item accurately reflected the support they received from their family or peers to maintain a physical activity routine. The total score was computed by summing the scores for each item. Higher scores indicated a stronger perception of functional support for engaging in physical activity adherence.
The Workplace Support for Health Scale developed by Kava et al 18 was used to evaluate participants’ perceptions of coworker and supervisor support in promoting a healthier lifestyle, particularly regarding physical activity. Responses on the 5-item scale were rated on a 5-point Likert scale, ranging from 1 (totally disagree) to 5 (totally agree). The total sum score ranged from 5 to 25, with higher ratings indicating stronger workplace support for a healthy lifestyle.
Data Collection
Recruitment for the study commenced after obtaining approval from the Michigan State University Institutional Review Board (ID: STUDY00009017). Prior to completing the paper-and-pencil questionnaires and BP assessments, participants were required to provide written consent. Participants who completed all aspects of data collection received compensation of approximately $10.
The primary investigator meticulously reviewed the medical records to purposefully select eligible participants. Subsequently, the primary investigator directly contacted them via phone calls and/or extended invitations in-person to participate in the study.
During the screening phone call, inclusion and exclusion criteria were used to determine participants’ eligibility. Once eligibility was confirmed and verbal consent was obtained, the primary investigator scheduled in-person data collection appointments within 1 week. The in-person data collection took place in a private counseling room at a primary care setting, and participants’ systolic/diastolic BP were assessed.
Data Analysis
Descriptive analyses were conducted using the Statistical Package for Social Sciences (SPSS 28; IBM Corp, Armonk, NY, USA). Pearson’s chi-squared tests were performed to examine the relationships between the demographic factors and BP management status. All variables, particularly outcome variables, were evaluated for their normal distributions using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Percentage and pattern of missing data were analyzed using Little’s Missing Completely at Random Test. A missing pattern appeared to be random (χ2 = 1941.116, df = 1176, P = .071) and with less than 1% of missing values noted. Multiple imputations (10 data sets) were conducted using Mplus (Muthén & Muthén, Los Angeles, CA, USA) to maximize the use of all available data.
Mplus version 8.7 was used to examine the relationships among psychosocial determinants, physical activity, and BP management (systolic and diastolic BP) simultaneously. Four global fit indices were used to estimate the model fit (both measurement and structural model), 19 including chi-square/degree of freedom ratio (χ²/df ratio ≤3), root mean square error of approximate (RMSEA <0.08), comparative fit index (CFI), and the Tucker-Lewis index (TLI ≥0.95). The minimum value for printing the modification index greater than 10.00 was used to consider model modification to increase the parsimony of the model. 20
Using the Mplus IND function, we performed a mediation analysis to explore the mediating effect of moderate-to-vigorous physical activity, and low-intensity physical activity. The 5000 BC bootstrap method and BC bootstrapping of the 95% confidence intervals (CIs) for indirect effects were used to test the significance and degree of the mediation effect. 20
We utilized the DIFFTEST procedure within Mplus to determine moderation effects between subgroups. The investigation focuses on examining the moderating effects of hypertension diagnosis duration (≤12 months vs >12 months), building upon the significant relationships previously identified using the final structural equation modeling. Our moderation analysis was initiated with the most constrained model (the nested model), wherein initial assumptions held all pathways to be equal across the groups of hypertension duration model. Gradually, pathways were selectively relaxed one by one, enabling the examination of group difference in path coefficients and the evaluation of changes in chi-squared values (∆χ2).
Results
Participants
Table 2 provides an overview of the participants’ characteristics. The study included a total of 400 participants, of whom 58.8% were female; the mean age of participants was 47.98 years (SD = 7.66). Nearly 50% were employed in general labor. In addition, more than half of the participants (56.8%) worked more than 40 hours per week. Pearson’s chi-squared tests also revealed significant correlations between demographic variables and BP status.
Participant Demographics (N = 400).

Abbreviations: DBP: diastolic blood pressure; SBP: systolic blood pressure
Measurement Model
The final model’s fit was good with the following indices: χ2/df = 1.86, RMSEA = 0.048 (90% CI = 0.043, 0.053), CFI = 0.952, and TLI = 0.947. All standardized factor loadings were statistically significant (P < .001) and exceeded 0.6 (see Table S1). Furthermore, examining the proposed correlations between variables within these models revealed a range of low-to-moderate correlations (0.25-0.55) (see Table S2).
Structural Model
The initial model showed a good fit to the data based on 4 global fit indices (χ2/df = 1.84, RMSEA = 0.050 [90% CI = 0.046, 0.055], CFI = 0.943, TLI = 0.935). All factor loadings in both models were significant (P < .001) and above 0.60 (ranged from 0.71 to 0.95). No further modifications were needed.
The final model explained variance in physical activity and BP: 22.8% for moderate-to-vigorous physical activity, 4.6% for low-intensity physical activity, 38.4% for systolic BP, and 18.4% for diastolic BP. Self-efficacy and functional support in physical activity (P < .001) were significantly associated with moderate-to-vigorous activity. Self-efficacy in physical activity was related to systolic (β = −0.18, P = .012) and diastolic BP (β = −0.32, P < .001). Functional support in physical activity (β = −0.24, P < .001) and perceived stress (β = −0.17, P = .011) were associated with systolic BP. Moderate-to-vigorous physical activity showed a small association with systolic (β = −0.25, P < .001) and diastolic BP (β = −0.14, P = .008) (see Figure 1).
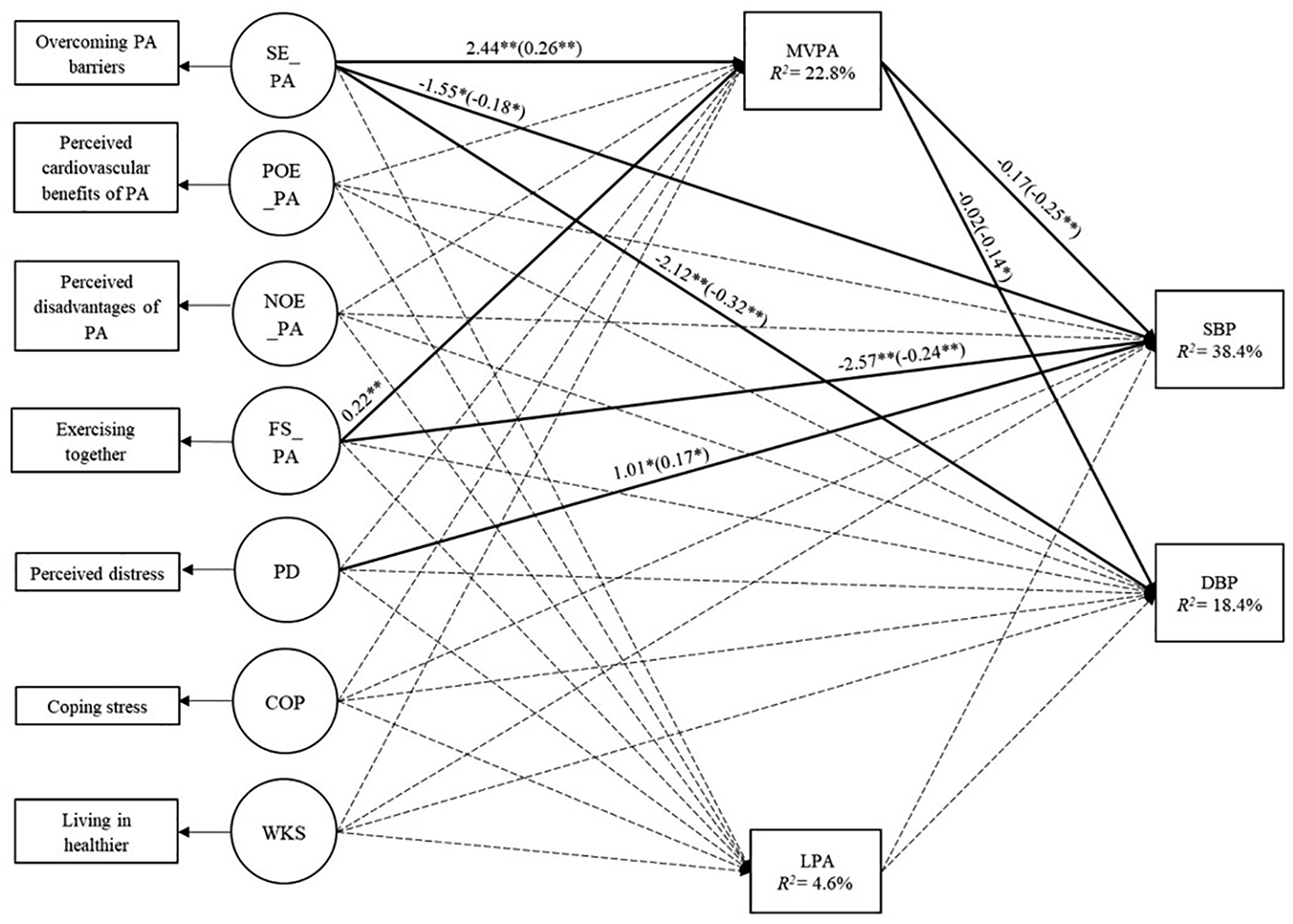
Final physical activity structure model of Thai young- and middle-aged adults with hypertension (N = 400). Solid lines indicate statistically significant paths. Dotted lines indicate a nonstatistically significant path. Standardized coefficients are presented in parentheses.
Mediation Analysis
The association of self-efficacy in physical activity (indirect effect = −0.050, P = .005) and functional support in physical activity (indirect effect = −0.031, P = .046) with systolic BP were partially mediated by moderate-to-vigorous physical activity (see Table 3). Moderate-to-vigorous physical activity also partially mediated the relationships between self-efficacy in physical activity and diastolic BP (indirect effect = −0.031, P = .037).
Mediation Effects of Physical Activity on Young- and Middle-Aged Adults With Hypertension on Psychosocial Factors and Blood Pressure (N = 400).

Standardized path coefficients for indirect effects obtained from Mplus IND function. Statistically significant difference path across groups is shown in bold.
Abbreviations: DBP: diastolic blood pressure; FS_PA: functional support in physical activity; LPA: low-intensity physical activity measured by metabolic equivalents score; MVPA: metabolic equivalents score spent by moderate-to-vigorous physical activity; SE_PA: self-efficacy in physical activity; PD: perceived distress; SBP: systolic blood pressure.
P < .05. **P < .001.
Moderation Analysis: Group Comparison
We observed substantial correlations between self-efficacy in physical activity and both moderate-to-vigorous physical activity (∆χ2 = 7.424, P = .006) and diastolic BP (∆χ2 = 3.878, P = .049), particularly in the group with a shorter duration of hypertension (≤12 months) (see Table 4). Similarly, a distinct stronger association between functional support and moderate-to-vigorous physical activity (∆χ2 = 4.173, P = .041) was observed for the shorter duration group.
Moderating Effect of HTN Duration on Path Coefficients: A Comparison between HTN Duration ≤12-month and >12-month groups.

Chi-squared difference values obtained from Mplus DIFFTEST function. Statistically significant difference path across groups is shown in bold.
Abbreviations: β: standardized beta coefficient; CFI: comparative fit index; DBP: diastolic blood pressure; FS_PA: functional support in physical activity; HTN: hypertension; MVPA: moderate-to-vigorous intensity physical activity measured by metabolic equivalents score; PD: perceived distress; RMSEA: root mean square error of approximate; SBP: systolic blood pressure; SE: standard error; SE_PA: self-efficacy in physical activity; TLI: Tucker-Lewis index.
P < .05. **P < .001.
Discussion
Our analysis highlighted that self-efficacy for physical activity demonstrated a moderate correlation with moderate-to-vigorous physical activity (r = 0.26), in contrast to findings from a Middle Eastern study with young adults with hypertension that showed higher strength of association (r > 0.30). 21 This divergence may be attributed to cultural and social contextual discrepancies, including social norms, as seen in the study by Nahari et al, where intrapersonal and interpersonal factors, including social norms, significantly influenced physical activity in Arab Americans. 22 This variation may be due to the well-documented role of social norms in shaping perceptions of suitable or acceptable physical activity. 23 For instance, if there is a cultural inclination toward gentler forms of physical activity, such as traditional Thai dances, these activities might be more socially endorsed and preferred among Thai adults with hypertension. Thus, the observed differences in the strength of association could reflect how social factors, including cultural beliefs, shape the preferences and physical activity behavior of adults with hypertension in different cultural contexts.
The role of perceived stress did not emerge as a significant predictor on these Thai adults’ physical activity. The absence of this significant relationship may be attributed to the predominantly blue-collar occupations of over 50% of the participants, such as farming and general labor. Despite the physical demands of these occupations, the reported physical activity does not seem strongly influenced by perceived stress levels. This suggests that individuals in strenuous work environments may distinguish between work-related physical activity and intentional engagement in structured activities.
Outcome expectancy stands as a relatively underexplored construct within the framework of Social Cognitive Theory. Our study, however, failed to establish its significance in the model. In contrast, an Iranian study involving 176 middle-aged adults (mean age = 49.54 years) with hypertension (mean duration = 51.23 months) found a significant association between positive outcome expectancy and increased engagement in physical activity. 21 This discrepancy might stem from the fact that our sample was slightly younger (mean age = 47.98 years) and had a shorter duration of hypertension diagnosis (mean duration = 32.73 months). It is possible that individuals experiencing hypertension for less than a year perceived their health condition as less severe, resulting in limited concern about potential complications arising from elevated BP.
Functional support in physical activity displayed a significant association with moderate-to-vigorous physical activity, consistent with an earlier study involving young adults with hypertension. 24 However, no significant correlations were observed between workplace support and low- or moderate-to-vigorous intensity physical activity. It may be that an essential factor to consider is the influence of occupation as a potential confounder in this relationship. The distinctive characteristics of blue-collar jobs, involving physical exertion, exposure to hazards, and specific workplace demands, 25 could lead to varied interpretations of workplace support. Notably, in this present study, the majority of participants held blue-collar positions (approximately 70%: farmers and general laborers). In the review of 40 studies by Smith et al, occupation notably influenced the promotion of moderate-to-vigorous physical activity at workplaces, with greater advancements observed among white-collar than blue-collar workers. 26 Drawing a parallel to the Thai context, the Thai Labour Standard TLS 8001-2020 embodies the principles of corporate social responsibility and aims to foster an environment characterized by employee acceptance, equitable treatment, suitable remuneration, and, notably, workplace safety. 27 It is possible that the perceived level of support for adopting recommended lifestyle behavior is relatively lower among Thai employees, potentially influencing the discernible impact on physical activity.
Our study unveiled significant associations of self-efficacy in physical activity, functional support in physical activity, and perceived stress with systolic BP. These associations are consistent with previous studies in adults with hypertension. For instance, a study in Sweden with middle-aged men found that enhancing self-efficacy in physical activity was associated with physiological benefits in lowering systolic BP. 28 Similarly, functional support was linked to reduced systolic BP in older adults, 29 and a study of middle-aged Chinese adults found an association between functional support and improved systolic and diastolic BP. 30 This relationship may be explained by an indirect mechanism through increased recommended lifestyle behaviors, such as physical activity, as suggested by Social Cognitive Theory. In addition, our model explained a higher variance than a previous study that investigated the relationship between psychosocial factors, such as functional support (from family and others), and cardiovascular outcomes such as high BP (either systolic or diastolic BP greater than 140 or 90 mmHg, respectively) in adults with hypertension in the United State (mean age = 48.7; R2 = 19%). 29
Significant indirect effects of self-efficacy in physical activity and functional support in moderate-to-vigorous physical activity on systolic BP emerged when these psychosocial factors were mediated by moderate-to-vigorous physical activity. Comparing these 2 psychosocial factors, self-efficacy in physical activity exhibited a slightly larger indirect effect than functional support in physical activity. In the existing literature within electronic databases, some evidence consistently confirms the direct effect with a moderate relationship between self-efficacy in physical activity (β = 0.35) 28 and functional support in physical activity (β = 1.78) 31 and systolic BP in young and middle-aged adults with hypertension. However, limited research delves into the indirect effect of moderate-to-vigorous physical activity on the relationship between these 2 psychosocial factors and systolic or diastolic BP.
Our findings highlight the potential importance of hypertension duration, especially among younger individuals with hypertension. Those with a hypertension duration of less than 12 months appear to exhibit higher levels of moderate-to-vigorous physical activity, which may support progress toward BP management goals. This analysis suggests that individuals in the <12-month hypertension duration group may experience more favorable outcomes in physical activity levels, possibly facilitated by higher self-efficacy or functional support in physical activity. Furthermore, our observations indicate that these individuals could demonstrate better diastolic BP management status, potentially linked to self-efficacy in physical activity, than those with a hypertension duration >12 months. However, as this study is correlational, further research is necessary to establish causation and explore underlying mechanisms.
Limitations
Our study purposefully targeted young- and middle-aged adults who had been diagnosed with hypertension within 5 years, resulting in a fairly homogeneous population in terms of age. Additionally, participants with chronic conditions such as coronary heart disease or heart failure were excluded. This skewed representation in terms of age, comorbidities, and hypertension duration could potentially affect how widely our findings can be applied, especially to populations with diverse age ranges, comorbidities, and durations of hypertension. It is important to note that our study heavily relied on self-report measures to assess psychosocial factors and physical activity. It is crucial to recognize that self-report measures might inadvertently introduce response biases or recall errors, potentially compromising the accuracy of the collected data.
Although our study was designed to examine the effect of pathway coefficients among groups categorized diagnosis duration, it is worth noting that the sample size within each group is relatively small (fewer than 100 participants per group). This inherent limitation could potentially limit the statistical power needed to detect subtle nuances. Moreover, our analyses did not account for whether participants were taking antihypertensive medication or their adherence to prescribed regimens. This omission may influence the interpretation of our findings.
Implications for Policy and Practice
Policymakers can utilize these findings to launch policies in primary care settings, ensuring that young- and middle-aged adults recently diagnosed with hypertension receive sufficient counseling or education to increase their confidence in adopting or maintaining recommended lifestyle behaviors for BP management, such as moderate-to-vigorous physical activity, within public health policies and programs.
The nuanced moderating effect of hypertension duration on the relationship between self-efficacy in physical activity and engagement in moderate-to-vigorous physical activity presents a strategic opportunity for nursing interventionists. Customizing intervention strategies to align with individual hypertension duration, particularly for those recently diagnosed within the first year, holds the potential to significantly enhance the efficacy of interventions. Ultimately, this approach can lead to a more effective promotion of increased moderate-to-vigorous physical activity engagement, particularly in comparison with individuals whose hypertension duration exceeds 1 year.
Nurses can initiate conversations centering on self-efficacy during patient interactions, providing a platform for working collaboratively with their patients to formulate tangible objectives and offering essential guidance to navigate these obstacles. By anchoring these dialogues in the psychosocial realm of self-efficacy, nurses can exert transformative influence over the spectrum of moderate-to-vigorous physical activity, which may ultimately translate into enhanced BP control. The recognition of the substantial influence of functional support from family and peers on both moderate-to-vigorous physical activity and systolic BP unveils a pathway for nurses to cultivate symbiotic collaborations. Thus, nurses can actively advocate for such family involvement, illuminating pathways through which family members or peers can catalyze heightened participation in moderate-to-vigorous physical activity—whether through mutual encouragement or shared activity endeavors. This synergy, forged between nurses, patients, and their support networks, stands poised to usher in a holistic transformation in hypertension management, underscoring the integral role of collaborative efforts for nurturing comprehensive well-being.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251326847 – Supplemental material for Examining the Relationship Among Social Cognitive Theory-Based Constructs, Physical Activity, and Blood Pressure in Young- and Middle-Aged Adults Living With Hypertension
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251326847 for Examining the Relationship Among Social Cognitive Theory-Based Constructs, Physical Activity, and Blood Pressure in Young- and Middle-Aged Adults Living With Hypertension by Wachira Suriyawong, Tsui-Sui Annie Kao, Lorraine B. Robbins, Jiying Ling and Leapetswe Malete in Western Journal of Nursing Research
Footnotes
Acknowledgements
We express our heartfelt thanks to all participants for their voluntary involvement. Special appreciation goes to Dr Panawat Sanprakhon and Dr Eakachai Kantawong for his invaluable coordination of data collection.
Author Contributions
WS spearheaded conceptualization, methodology development, data collection, cleaning, and analysis, as well as crafting the initial draft. TAK supervised data-related tasks, contributed to methodology, and participated in manuscript work. LR, JL, and LM offered feedback on design, result interpretation, and finalized draft reviews.
Data Availability Statement
The data supporting this study’s findings can be obtained from the first author, Wachira Suriyawong, upon a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Midwest Nursing Research Society Foundation, Sigma Theta Tau Alpha Psi Chapter, and the Graduate School Dissertation Completion Fellowship at Michigan State University.
Ethical Considerations
This study received ethics approval from the Michigan State University Institutional Review Board (ID: STUDY00009017). Participants were provided with comprehensive information about the research and given the opportunity to ask questions before providing written informed consent. Participation was entirely voluntary, with the assurance that individuals could withdraw from the study at any point without any penalties.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.